
Abstract
Objectives
A disproportionate number of individuals with autism spectrum are unable to transition into independent living during adulthood, compromising the ability to experience autonomy and exert self-determination. Over the past 30 years, there has been an increasing trend to incorporate technology into educational and behavioral interventions, including those to target daily living skills.
Methods
In order to inform practice and identify needs for future research, we conducted a systematic review of peer-reviewed published research evaluating the effectiveness of an intervention incorporating electronic technology to improve daily living skills among adults with autism spectrum. We extracted data regarding participants, daily living skills targeted, intervention characteristics, and outcomes. Additionally, we evaluated each case against What Works Clearinghouse single-case design standards.
Results
Through a systematic database search and ancillary searches, we identified 27 studies with 49 participants. Interventions supported by electronic technology were most commonly used to improve meal preparation and housekeeping tasks. Across most applications, technology was utilized within the antecedent portion of an intervention, most commonly used with video modeling or video prompting interventions. Surprisingly, few studies took place in the participants’ place of residence.
Conclusions
Evidence suggests there is great potential for incorporating technology into daily living skill interventions; however, more research is warranted to realize the full benefits of this approach.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Daily living skills are a critical domain of adaptive behavior necessary for age-appropriate, independent functioning and for transitioning independently into adulthood (Baker et al., 2021; Smith, Greenber, et al., 2012; Smith, Maenner, et al., 2012). Further, the development of daily living skills is essential to promote autonomy, encourage self-determination, and improve one’s quality of life (Bal et al., 2015; Cruz-Torres et al., 2020). According to Sparrow et al. (2005), the daily living skill domain encompasses three sub-domains including personal (i.e., eating, dressing, hygiene, cleanliness), domestic (i.e., household chores, meal preparation), and community skills (i.e., time management, money management, use of transportation). Development of the skills required for independent day-to-day functioning can be challenging for individuals on the autism spectrum and thus lifelong support with activities related to daily living is required (Bal et al., 2015; Krauss et al., 2005). The National Longitudinal Survey of Transition-2 (NLTS-2; Newman et al., 2011) reports only 17% of autistic adults live independently. Given the role that the acquisition of daily living skills plays in an individual’s successful transition to adult life, such as improving quality of life and decreasing dependence on others, the effective identification and implementation of evidence-based practices targeting the development of daily living skills is necessary (Delano, 2007; Wertalik & Kubina, 2018).
The lack of daily living skills can contribute to a decreased sense of self-worth, self-confidence, and life satisfaction and, thus, lead to the development of learned helplessness (Perez-Fuster et al., 2019; Peterson et al., 1993; Vermeulen, 2013). Ideally, daily living skills are taught to autistic individuals well before graduation, regardless of plans after graduation. Hendricks and Wheman (2009) reported a vast majority of autistic individuals experience challenges in acquiring these skills that are essential to independent functioning, thus hindering integration into the community after graduation and contributing to an increased dependence on others. In order to address these difficulties, researchers have turned to employing technology-supported instruction based on findings of high effectiveness (Ayres & Langone, 2005; Shukla-Mehta et al., 2010). These technology-supported instructions may be delivered via computer, cellular phone, or tablet and include the use of video modeling and prompting, audio cuing, and picture prompts. Further, the rapid advancements in technology and the widespread use of mobile devices have led to an increased use of electronic technology among individuals with intellectual and developmental disabilities (Ayres et al., 2013). The use of electronic technology to improve educational outcomes for individuals on the autism spectrum has many potential benefits. Technology today often comes in the form of handheld devices that are portable for easy use at home and in the community. Moreover, the ubiquitous use of technology in today’s society ensures that technology support blends seamlessly into one’s environment, without stigma (Cihak et al., 2007).
Some previous reviews have summarized literature on this topic. Mechling and Gustafson (2008) summarized literature from 1986 to 2006 regarding the use of high-tech and low-tech applications for teaching cooking skills to persons with ASD. Palmen et al. (2012) conducted a literature review of behavioral interventions to improve adaptive skills, which were defined as social interactions or daily living skills among high-functioning young adults with autism. Additionally, Palmen and colleagues set their parameters to any behavioral intervention (e.g., prompting, task analysis) and not specifically targeting technology like the current review. den Brok and Sterkenburg (2015) reviewed the literature from 1996 to 2011 on the utilization of technology to support skill attainment across daily living skills, vocational skills, and transitioning between tasks among individuals with ASD and/or intellectual disabilities. While the den Brok and Sterkenburg (2015) results included studies with adult participants with ASD, this was not the specific focus of the review. Moreover, the search was conducted 10 years ago. With the fast-paced advancements in technology, an updated review is warranted. Further, Gardner and Wolfe (2013) conducted a systematic review of literature published between 2005 and 2013 that focused on video modeling and video prompting interventions to teach individuals with ASD daily living skills. Of the 13 studies reviewed, the age ranges of individuals with ASD were 6 to 41 years. Additionally, the review was limited to video modeling and prompting, as opposed to a comprehensive review of all technology-supported interventions.
The purpose of this review is to identify and summarize the characteristics of participants, interventions, technology, and outcomes among studies that implemented technology-supported intervention to teach daily living skills to autistic adults. We aim for the summary of literature to provide practical guidance for utilizing electronic technology in teaching daily living skills to autistic adults as well as inform future research.
Method
Participants
Studies for this review were selected based on five criteria: (a) the inclusion of participants, aged 18 years or older, with a diagnosis of autism; (b) the dependent variable was an observational measure of a daily living skill; (c) the implementation of a behavioral intervention involving the use of electronic technology; (d) the article was published in English; and (e) the article was published in a peer-reviewed journal. A study was included if authors reported participant diagnosis of autism, autism spectrum disorder, Asperger syndrome, or pervasive developmental disorder-not otherwise specified (PDD-NOS). Further, if a study included participants both with and without an autism spectrum diagnosis, or both adults and children, the study was only included if data could be extracted for those autistic adult participants. We placed no restrictions upon participants’ level of functioning. We utilized the definition of daily living skills as age-appropriate, self-care behaviors that facilitate independent living (Smith, Greenber, et al., 2012; Smith, Maenner, et al., 2012); therefore, studies that directly targeted skills that were essential for independent living, such as self-care, cooking, and cleaning, were included. Although communication, social, academic, and motor skills certainly facilitate independent living, we excluded studies that targeted these skills without an obvious impact on independent living. For example, a study that improved conversation skills between peers would be excluded, but one that facilitated asking for assistance in locating specific items at the grocery store would be included. Finally, electronic technology was any assistive technology (Individuals with Disabilities Education Act [IDEA], 2004) that was powered by battery or electricity, such as computers, tablets, or television.
Procedures
Database Search
We conducted a four-step search procedure. First, in September 2020, we conducted a systematic search of the following electronic databases: Education Research Information Clearing House (ERIC), Academic Search Complete, PsychArticles, PsychINFO, Education Research Complete, and Psychology and Behavioral Sciences Collection. Although we expected that most studies would have been published in the last 30 years, coinciding with the increased availability of technology, we were unable to pinpoint the exact date in which technology that could be incorporated into interventions to improve daily living skills were available on the market. In order to be certain to identify the earliest uses of electronic technology to promote daily living skills, we did not restrict the search by year of publication. The search was restricted to English language publications and search terms were entered using the Boolean operators and truncation across three categories: autism, daily living, and technology. The autism search terms included autism, Asperger syndrome, PDD, and pervasive developmental delay. The daily living search terms included daily living, DLS, chore, adaptive skill, life skill, hygiene, meal, cook, shop, money management, self-care, time management, and grooming. Finally, the technology terms included technology, tablet, video, iPad, computer, phone, iPhone, TV, and DVD.
The electronic database search identified 619 articles for possible inclusion in the review. Authors first reviewed the title and abstract of each article and recorded which of the five inclusion criteria the article failed to meet. For example, the database search identified Shic and Goodwin (2015), but a review of the abstract clarified this was an introduction to a special issue rather than an empirical evaluation of an intervention. As a result, the author recorded that it failed to meet the following criteria: (a) adults with autism spectrum served as participants, (b) the dependent variable was an observational measure of a daily living skill, and (c) the implementation of a behavioral intervention involving the use of electronic technology. After screening title and abstracts, the authors reviewed the full text of the remaining articles, recording which of the five inclusion criteria each study met or failed to meet.
Each of the three authors applied the inclusion criteria in the method described above to two-thirds of the studies identified in the database search. This ensured that two authors independently applied the inclusions criteria to each of the 619 articles. That is, the first and second author both independently applied the inclusion criteria to one-third of the identified studies, the first and third authors both applied the inclusion criteria to another one-third of the studies, and the second and third authors both applied the inclusion criteria to the remaining one-third of studies.
Interrater reliability was calculated by dividing the number of agreements by total number of studies identified and multiplying by 100 to obtain a percentage. Interrater agreement was 93%. All disagreements were resolved via discussion. In some cases, disagreements were a result of an oversight by one of the two authors and a quick discussion highlighted such oversight. The majority of the remaining disagreements involved the determination of a dependent variable as a daily living skill. For example, two authors disagreed about the inclusion of Baumgart and VanWallenghem (1987) who taught participants to read site words affiliated with the grocery store. One author originally categorized sight-word reading grocery-store words as a daily living skill, but the other did not. We discussed the information regarding the dependent variable that was presented in the article along with our operational definition of daily living skills and ultimately agreed that this dependent variable failed to meet our definition. Specifically, because the words were being taught with no application of that skill to actual grocery shopping, we determined that it failed to meet the criteria.
Ancillary Searches
Next, we conducted a hand search of the journal in which most studies identified in the electronic database search were published (i.e., Education and Training in Autism and Developmental Disabilities). We searched all volumes dated 2000 and later, which dated five years prior to the oldest study identified in the electronic database search. This search resulted in the identification of no additional articles. Afterward, we conducted an author search for the author with the most publications among those identified in the electronic database search (i.e., Linda Mechling). One additional study was identified. Lastly, the references of the studies meeting these criteria were reviewed to identify additional studies for possible inclusion, and thus resulted in the identification of two additional studies. See Fig. 1 for a summary of the search process.

Flowchart of systematic search of studies to be included for synthesis
Measures
Data from 27 included studies are summarized according to (a) participant characteristics, (b) daily living skills, (c) intervention characteristics, and (d) outcome measures. Participant characteristics that were extracted include the sex, age, diagnosis, and race and/or ethnicity of each participant. Data extracted regarding daily living skills summarized the targeted skill (e.g., food preparation, laundry, grooming). Intervention characteristics that were extracted include (a) implementer, (b) setting, (c) electronic technology device utilized, (d) how electronic technology was incorporated into an intervention, and (e) treatment fidelity. Outcome measures that were extracted included data regarding (a) generalization, (b) maintenance, and (c) social validity.
Two independent experimenters independently conducted data extraction on 37% of the included studies. An agreement was counted if both authors recorded the same item. Interrater reliability was calculated by dividing the total number of agreements among the items by the total number of items scored and multiplied by 100. Mean agreement across studies was 84% (range 65–100%). All instances of disagreements were discussed until a consensus was reached.
Data Analyses
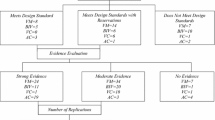
Of the 27 included studies, one study did not include an experiment, rather two case studies. All of the 26 remaining studies employed single-case research designs, which contained 57 single-case experiments. We rated each experiment against the What Works Clearinghouse Single-Case Design Standards (WWC, 2020). Each experiment was assigned a rating of meet standards, meets standards with reservations, or does not meet standards.
In order to meet standards, an experiment had to meet four design criteria. First, the raw data must be available in graphical or tabular form to allow for visual analysis (WWC, 2020). Second, the experimenter systematically manipulated the independent variable. Third, interobserver agreement (IOA) was measured in at least 20% of each condition and met a minimum threshold of 80% agreement or 0.60 Cohen’s Kappa. Fourth, if an alternating treatment design was employed with a third condition, residual treatment effects were determined to be unlikely. If an experiment failed to meet any of these four criteria, then it was rated as does not meet standards. If an experiment met these four criteria, they were rated based on specific design standards. If an ABAB design contained at least four phases with at least 5 data points per phase, it was rated as meet standards. If an ABAB design contained at least four phases with 3–4 data points, it was rated as meet standards with reservations. For a multiple-base or multiple-probe design to meet standards, it must include at least 6 phases with at least 5 data points per phase. If the design contained 6 phases with 3–4 data points, it was rated as meet standards with reservations. Multiple-probe designs must meet additional criteria. To meet standards, at least three initial baseline sessions overlapped vertically and at least three sessions were conducted just prior to the introducing the intervention. If only 1–2 baseline sessions overlapped and/or 1–2 sessions were conducted just prior to introducing the intervention, the experiment was rated as meet standards with reservations. Finally, for an alternating treatment design to meet standards, there must have been at least five data points per condition with no more than two consecutive data points per condition. If an alternating treatment design contained at least 4 data points per condition with no more than two consecutive data points per condition, it was rated as meet standards with reservations.
We rated any experiment in which the effect of a technology-supported intervention on a daily living skill was measured. Many articles contained multiple experiments. Some articles containing multiple experiments with a single participant in which the effects of one independent variable was measured on two or more dependent variable (e.g., Bouck et al., 2016). Other studies contained multiple experiments in which the effects of two or more technology-supported interventions were evaluated. For example, Mechling et al. (2013) used an alternating treatment design to compare the effects of commercially available video prompts and custom-made video prompts on the completion of cooking recipes among one adult participant with autism. Although conducted within a single alternating treatment design comparing three conditions (commercially available video prompts, custom-made video prompts, and a control condition), we evaluated the experiment comparing commercially available video prompts to a control condition and the experiment comparing custom-made video prompts to a control condition separately.
Prior to rating each experiment, the second author provided training to the first and third authors. Training consisted of reviewing written materials, modeling, and jointly evaluating two randomly selected articles containing 4 experiments. After training, two independent experimenters assessed 26 experiments (46%) against WWC standards. The experimenters assigned identical ratings to 21 of the 26 experiments (81%). Disagreements among the remaining five were resolved via discussion.
We visually analyzed the experiments that met standards, with or without reservations according to the WWC guidelines (WWC, 2020). Visual analysis was conducted collectively among all three authors who had graduate-level training in single-case design. First, the authors evaluated data within a phase, specifically the level, trend, and variability. Next, the authors evaluated data cross phases by examining the immediacy of effect, overlap of data compared to previous phase, and consistency of data in similar phases (e.g.., consistency among baseline phases). Authors used this within and across phase evaluation to determine the number of demonstrations of an effect. Experiments with three demonstrations of an effect and no demonstrations of a non-effect were rated as having a strong effect. Those with three demonstrations of an effect and one demonstration of a non-effect were rated as having a moderate effect. An experiment without at least three demonstrations of an effect was rated as having no effect.
Results
A total of 27 studies were identified and included in the systematic review. Across the 27 included studies, an electronic technological device was utilized to teach daily living skills for 49 adults on the autism spectrum.
Participant Characteristics
From the 27 studies, 49 participants received daily living skills training utilizing a technology-supported intervention. Most participants were males (n = 39; 80%). The participants’ age ranged from 18 to 41 years, with most participants between 18 and 29 years (n = 38; 78%). Only 11 participants (22%) were aged 30 years or older.
The majority of participants (n = 31; 63%) had two or more comorbid diagnoses. In addition to an autism spectrum diagnosis, 19 participants (39%) had one additional diagnosis, nine participants (18%) had two additional diagnoses, and three participants (6%) had three or more additional diagnoses. Of the comorbid diagnoses, intellectual disability (n = 29; 94%) and speech impairment (n = 7; 23%) were the most common. One participant each had the following comorbid diagnoses: attention-deficit/hyperactivity disorder (ADHD), hearing impairment, epilepsy, Williams syndrome, hypothyroidism, psychotic disorder not specified, mood disorder, and behavior disorder.
Race and ethnicity were not reported for the majority of participants (n = 44; 90%). Among the five participants in which race and/or ethnicity was reported, three participants were White, one participant was Asian American, and one participant was Hispanic.
Daily Living Skill Characteristics
Some participants received training on skills across multiple daily living skill domains (n = 16; 33%). Nonetheless, the most common domain of skills taught were meal preparation (n = 23; 47%) and housekeeping (n = 22; 45%). For example, Cannella-Malone et al. (2006) compared the effectiveness of video modeling and video prompting for teaching participants to set the table (meal preparation) and put away groceries (housekeeping). During video prompting sessions, the participants were oriented toward the computer and the trainer stated, “Watch this.” A short video segment of the step to be completed was followed by an opportunity to complete that step and then returning to watch the next video segment. Video modeling consisted of similar procedures, but the participants viewed a video of the entire task, as opposed to viewing steps one at a time, and then were given the opportunity to complete the task. While both video modeling and prompting resulted in improvements in daily living skills, Canella-Malone and colleagues found video prompting to be the superior technique to teach these skills.
Other daily living skills were targeted, but with less frequency. These include community skills such as shopping (n = 8; 16%) and washing or folding laundry (n = 8; 16%). The skill domains of time management, healthcare management (e.g., scheduling doctor appointments), leisure time and recreation, and mobility and transportation (e.g., riding the bus) were targeted with two participants each. Finally, one participant received instruction to learn money management and hygiene skills. A complete list of the targeted skill domains is listed in Table 1.
Intervention Characteristics
The majority of intervention sessions took place in a school setting (e.g., high school, university campus; n = 18; 37%) or within a vocational or day habilitation center (n = 17; 35%). For example, Pérez-Fuster et al. (2019) taught four adults with autism spectrum and intellectual disability to wash dishes and complete a load of laundry within the day habilitation center which they attended. When instructed to perform a daily living task, the participant would select the correct task from a menu presented on a tablet. After selection, audio and picture prompts for the selected tasks were delivered via the tablet and an LED light within the day habilitation center was illuminated to indicate the correct location for performing the targeted task. Intervention was implemented in a community setting for six participants (12%), in a residential facility for four participants (8%), and in the homes of four participants (8%). The setting in which two participants received intervention were not clearly reported.
A researcher implemented intervention for the majority of participants (n = 37; 76%). Teachers (n = 4; 8%), clinical therapists (n = 2; 4%), life coaches (n = 2; 4%), and a parent (n = 1; 2%) also served as implementers. The implementer was not reported for three participants (6%). Fidelity of implementation was reported for just over half of all participants (n = 25; 51%). When reported, treatment fidelity results were at or above acceptable levels for all participants.
The most common technology device utilized to teach daily living skills was a tablet (n = 23; 47%). Among articles published after the introduction of the iPad into the technology market in 2010, a tablet was utilized with more than three-fourths of participants (n = 20; 80%). Gardner and Wolfe (2019) utilized a tablet to deliver video priming and video prompting to teach three autistic adults to wash the dishes. Researchers positioned the tablet near the sink and instructed participants to watch a video demonstrating the entire process of dish washing. Next, they instructed participants to watch a second series of video segments, each segment depicting a single step of the dish washing task analysis. After watching each video segment, researchers instructed participants to complete that same step. A computer (n = 19; 39%) was the second most widely utilized technological device for intervention. Although television (n = 4; 8%), cellular phones (n = 3; 6%), and radio with headsets (n = 2; 4%) were utilized, it was infrequently.
For the most part, technology was incorporated into the antecedent component of the intervention. The most frequently implemented technology-supported intervention was video modeling or video prompting (n = 39; 80%). For example, Aldi et al. (2016) used a tablet to provide point-of-view video modeling to teach two participants meal preparation, laundry, and housekeeping skills. The participants watched the entire video model and were then instructed to complete the task.
Technology was also utilized to deliver audio prompts (n = 6; 12%). For example, Bouck et al. (2016) compared the efficacy of audio prompts delivered via an audio recorder and written instructions to teach participants how to conduct price comparison of groceries (e.g., $1.64 vs $1.66 vs $1.69).
Technology was utilized to display picture prompts for another five participants (10%). Gil et al. (2019) taught grocery shopping skills using an iPad with photographs that served as a grocery list. The participant was taught to check each task off their grocery list as they shopped. For another four participants, LED lights served as visual cues to begin a specific task in a specific location. That is, LED lights illuminated the location in which each step of the targeted task was to take place (Perez-Fuster et al., 2019).
A calendar application that delivered both text and audio prompts was implemented with two participants. The following interventions were implemented with one participant each: visual cues, augmented reality role play, and Google Maps. For one participant, Cakmak and Cakmak (2015) created an interactive animation in which the participant controlled a character created in his likeness to complete a shopping trip.
Studies that implemented virtual or augmentative reality were not a focus of this review, but are addressed within another systematic review, published in this special issue.
Outcome Measures
Maintenance was reported for almost half of the participants (n = 24; 49%). Maintenance was measured within 2 weeks of completing intervention among five participants (21%), within 3 weeks to a month for four participants (17%), within 1 to 2 months for three participants (13%), and more than 2 months for four participants (17%). The duration after which maintenance was measured was not clearly reported for the remaining eight participants (33%).
Generalization was reported for one-third of participants (n = 17; 35%). Further, generalization was most commonly measured across settings (n = 10; 59%). Generalization was measured across materials for three participants (18%), across tasks for two participants (12%), and across people for one participant. For three participants in which generalization was evaluated, specific details were not reported.
Social validity was assessed among 20 participants (41%). Among those participants for which social validity was measured, teachers completed the social validity assessments most frequently (n = 14; 70%). Nine participants themselves evaluated social validity (45%). Four caregivers (e.g., parents; 20%, three graduate students: 15%, one teaching assistant; 5%), and one residential staff member (5%) also served as social validity assessment informants.
Design Quality and Visual Analysis
We analyzed 57 experiments against the WWC Single-Case Design Standards (WWC, 2020). Among the 57 experiments, 7 (12%) met standards, 6 (11%) met standards with reservations, and 44 (77%) did not meet standards. Among the 13 experiments that met standards, with or without reservations, nine (69%) demonstrated strong evidence of a causal relationship, one demonstrated a moderate evidence (8%), and four (23%) demonstrated no evidence of a causal relationship. It is important to note that among the four experiments that failed to demonstrate evidence of a causal relationship, two evaluated a technology-supported intervention against a traditional intervention unaided by technology (Bouck et al., 2016). Similarly, Cannella-Malone and colleagues (2006) compared two technology-supported interventions, video modeling and video prompting, to a baseline condition. While the evaluation of video prompting demonstrated evidence of a causal relationship, the evaluation of video modeling did not (Cannella-Malone et al., 2006). In other words, the four experiments that failed to demonstrate evidence of causal relationship are not necessarily evidence that technology-supported interventions may not be efficacious in supporting daily living skills instruction.
Additional experiments that did not meet standards and, therefore, no evaluation of the evidence of a causal relationship was conducted, also compared technology-supported interventions to traditional interventions (i.e., without technology) rather than comparing a technology-supported intervention to a baseline condition (Bouck et al., 2017; Mechling & Gustafson, 2008). Such an evaluation makes it impossible to determine if the technology-supported intervention is effective, relatively to baseline. Future research should consider designs used by Cannella-Malone and colleagues (2006) which allows for an evaluation of effectiveness and a comparison of interventions. After baseline, but prior to implementing video modeling, Haring et al. (1987) provided a training in which they delivered least-to-most prompting and praise for correct response. This precludes the ability to determine if video modeling would have been effective without this training condition. Similarly, after the baseline phase, O’Handley and Allen (2017) conducted a video production phase in which the participant and his mother created video models. Experimenters evaluated the effect of video production prior to implementing video modeling. Although this experiment met standards and demonstrated strong evidence of a causal relationship, it is impossible to preclude if video modeling would have been effective without first participating in video production.
Discussion
Autistic adolescents often experience an improvement of independent daily living skills across their development. Unfortunately, once the adolescent reaches adulthood, this improvement plateaus or regresses (Smith, Greenber, et al., 2012; Smith, Maenner, et al., 2012). This plateau or regression is likely related to the fact that adolescents receive daily living skills supports in public high school, but when those supports are discontinued upon high school graduation, similar supports by other providers are unavailable. The rapid increase in the use of technology over the past 20 years has resulted in great benefits in teaching skills to individuals with ASD. As such, the purpose of this review was to examine the existing literature on the use of technology to teach daily living skills to autistic adults. Through a systematic search of the literature, a total of 27 intervention studies containing 49 participants were identified and reviewed. Most studies incorporated technology into the antecedent component of the intervention and used various consequence strategies that typically did not include a technological component. The types of technology, the interventions with which technology was utilized, and the daily living skills targeted for instruction varied greatly across the literature. Many interesting themes were identified across this literature synthesis.
The skills taught across the included studies varied greatly. Meal preparation and housekeeping were the most common skills taught. Yet, within each of these domains, several specific skills were represented. For example, among studies that taught meal preparation, skills included preparing specific foods (e.g., making popcorn, microwaving pizza, preparing macaroni and cheese), preparing to make a meal, and setting the table. Of the studies that targeted a cooking skill specifically, the majority targeted one or two specific foods, often snacks, rather than a full meal. While learning to prepare a single dish or snack is undoubtedly important in improving independence and autonomy, an individual may be no more able to live independently with skills to prepare only a few foods within their repertoire. Additional research should continue to explore the development of a more robust set of cooking skills.
Very few studies targeted grooming and hygiene and no study addressed dressing. This was particularly alarming for a few reasons. First, dressing, grooming, and hygiene deficits are particularly prevalent among individuals with ASD relative to those with an intellectual disability (Matson et al., 2009). Yet, few studies address this significant area of need. Second, technology-supported interventions are ideally suited for skills in which privacy would be of utmost importance, such as dressing and grooming. That is, the significant benefit of technology-supported intervention with a skill such as dressing or toileting is that it can reduce the time an implementer is needed to assist an individual in activities that are commonly completed in private. Only one study included the parent as an implementer, so it would be beneficial to explore any intervention that may assist in privately occurring skills that would allow for the reduction of intervening individuals to preserve the privacy and self-dignity of the autistic individual. This being said, the lack of studies incorporating electronic technology to promote grooming and hygiene skills should not be interpreted to mean that no such effective interventions exist. On the contrary, many efficacious interventions can be found in the existing literature (Palmen et al., 2012), but very few of those have evaluated the potential additive value of incorporating electronic technology.
A variety of technological devices were implemented across the included studies. The unique interface of the ever-growing technology selections continues to grow with different ways in which individuals may learn. Increasing text size, images, and audio and video commands (Holland & Holland, 2014) are among the most common. Though the cost of technology can vary, the mobility, accessibility, globalization, and supports they offer are endless and becoming more common in everyday life (e.g., ordering food, using transportation, housekeeping tasks, paying bills) while methods without the use of technology are slowly becoming less frequently used. Unsurprisingly, a tablet was the most common device implemented, likely due to its portability and availability. Interestingly, cellular phones were rarely utilized, despite smart phones sharing many of the same capabilities as a tablet. Perhaps the larger screen size of a tablet was more appealing, particularly in implementation of video prompting and visual schedules. Yucesoy-Ozkan et al. (2018) found that the use of a video prompting via smartphone to have higher effectiveness and efficiency than video prompting via tablet for teaching leisure skills to four participants with intellectual disabilities. Perhaps the same may be true for teaching daily living skills to adults with autism spectrum; more research is warranted.
The vast majority of studies included in the review implemented video modeling or video prompting. This was expected because daily living skills typically consist of multi-step behavior chains, making video modeling or prompting an obvious selection. Additional research should continue to explore lesser-evaluated uses of technology such as smartphone or tablet applications, audio prompts, videoconferencing, visual schedules, and augmented or virtual reality to teach daily living skills. The efficacy of smartphone and tablet applications such as a calendar, alarm clock, maps, and others designed specifically for users with their day-to-day activities should be evaluated specifically among autistic adults.
Another interesting pattern among the included studies is that very few were conducted within the natural environment. A staggering 72% of participants were taught daily living skills at school or at day habilitation centers only. Additionally, studies conducted within the school and day habilitation centers only reported generalization for 7 of the 35 participants (20%) Therefore, it is impossible to know if the daily skills learned within the school or day habilitation setting transferred to the participants’ home setting, where the skills would be most useful. If instruction is not to take place in the setting in which the participant will utilize the skills, the planning for generalization of the newly acquired skills at the onset of intervention will aide in improving long-term generalization and maintenance among participants with autism spectrum (Neeley et al., 2016). Planning and implementing daily living skills in the environment in which the skill will be utilized is essential to success and should be incorporated and evaluated in future research. Slightly under half of all studies reported maintenance of skills, ranging from 1-week post-intervention to 3 months after the conclusion of the intervention. Neeley et al. (2016) found that few studies reported generalization and maintenance of functional living skills and unfortunately, our review found no change in this trend.
The results of this review offer guidance to practitioners interested in incorporating technology into instructional practices for adults with autism spectrum. Due to the substantial evidence of its efficacy, practitioners should consider implementing video modeling and video prompting to teach daily living skills. Moreover, practitioners should feel comfortable utilizing tablets, computers, smartphones, and other electronic devices into daily living skill instruction. Though technology may not always be additive to outcomes of some privately occurring skills such as bathing, it should not be interpreted as evidence that these skills have not been addressed in some aspect (Palmen et al., 2012). Selection of intervention components should reflect what is most feasible to teach the daily living skill(s). Finally, despite a scarcity of research conducted in natural environments, practitioners should consider conducting instruction in natural environments due to some evidence of its effectiveness (e.g., Bouck et al., 2017) and the known benefits of natural environments promoting generalization (Neeley et al., 2016).
Despite the apparent benefits of incorporating electronic technology into interventions to improve daily living skills, incorporation is not always seamless. The use of many technological devices requires full functioning sensory abilities, specific fine or gross motor skills, and/or prerequisite skills. For example, audio cues are likely ineffective for individuals with hearing impairments. Likewise, individuals with poor fine motor control may not have the ability to navigate video prompts or applications on a tablet. In other words, electronic technology cannot be blanketly incorporated into all daily living interventions. Similarly, many individuals may need to first develop prerequisite skills to use electronic technology and realize the potential benefits such as turning devices on and off and navigating through a device in order to access a particular feature, such as finding and opening an application on a tablet prior to using it. Pretraining on how to navigate the technological device to be utilized should be considered for potentially greater success. Cullen, Alber-Morgan, et al. (2017) conducted preintervention training with their participants by practicing the use of the iPad and MyPicsTalk application until participants demonstrated eight key aspects of usage (e.g., swiping, navigating to specified application to be used, and turning device on and off). Similarly, Gil and colleagues (2019), conducted pretraining with all participants consisting of their ability to operate simple functions of the iPad (e.g., turn on and swipe) and use of the application (e.g., pressing the touch screen to check off items). Participants had to demonstrate their ability to navigate the iPad with 100% accuracy for a minimum of one session before moving into the intervention phase. Lastly, Kellems et al. (2018) employed iPad training prior to intervention by implementing one-on-one model-led-test procedures of accessing the Keynote program on the iPad and how to open the correction presentation containing all of the videos needed. All participants had prior experience navigating an iPad, thus only requiring one training session to reach mastery criteria for three of the participants, and three total training sessions for the remaining participant before entering intervention phases. Training components prior to intervention has become more common in the recent years and should be taken into consideration prior to implementation.
Limitations and Future Research- Reduce
Several limitations of this review are noted. First, it is likely that only studies in which interventions were successful at improving daily living skills were published, leading to a potential publication bias. Therefore, it is possible that the positive outcomes of the included studies are not representative of effects to be experienced in real-life implementation of technology-supported interventions. Second, since technology is abundantly utilized by many, it is possible that additional studies utilized technology, but this was not a key feature of the study. If so, technology-related terms were not identified as a keyword; therefore, not identified in the database search. Additionally, because only one study explored a parent implemented intervention within the home setting, further research should be done within this area. Also, video-based components are appropriate tools when working with a variety of individuals with autism spectrum, but developers of video instruction should give special attention to how adequately the videos are and that not one video sequence can be successful for all autistic adults and should be individualized as needed. Finally, the term daily living skills has a variety of definitions and was used loosely within some studies. Moreover, not all studies which were measuring a daily living skill, utilized the term daily living skills. To account for studies that may have identified a skill more specifically (e.g., cooking, grooming), but not broadly as a daily living skill, we incorporated specific skill keywords in our electronic database search (e.g., meal, cooking, shopping, grooming). However, with daily living skills representing a broad spectrum of skills, it is quite possible that our search did not include all terms necessary to identify all studies evaluating daily living skills.
Several factors associated with daily living skill interventions utilizing technology for autistic adults continue to be under-researched. First, future research should explore the benefits of incorporating technology into daily living skills typically completed in private such as grooming and hygiene behaviors. While we anticipate technology-supported interventions to be effective, we also anticipate that they may reduce the need to intervening individuals to be present during privately occurring activities (e.g., using the toilet). This should be further explored.
Second, future research should evaluate the generalization of daily living skills taught in situations that do not reflect the natural setting (e.g., school, day habilitation centers). It is quite possible that the use of technology may promote generalization as a common stimuli across settings if the technological devices is utilized both in the training and application settings (Stokes & Baer, 1977).
Third, future research should explore the efficacy of teaching natural change agents to utilize technology-supported interventions to improve daily living skills. We hypothesize that the incorporation of technology may serve to reduce the decision-making responsibility of an implementing natural change agent (e.g., roommate, parent). Future research should continue to explore this possibility and identify best practices to incorporate technology to improve daily living skills in natural settings.
Finally, future research should address many of the methodological limitations found among the included studies. The majority of experiments included in the studies of this review did not meet WWC design standards. Future research should include strong experimental designs to better evaluate the efficacy of technology-supported interventions to address daily living skills.
This review has important implications for continued research and practice. The use of technology to teach daily living skills to autistic adults is shown to be effective and should continue to be utilized and studied, across the lifespan. Teaching individuals with developmental disabilities valuable life skills through the non-stigmatizing use of technology can have a positive and immediate effect on gaining independence. Although technology-based interventions have made significant progress in the acquisition of skills, teaching of daily living skills to adults with autism spectrum should continue to be provided to help them achieve maximum independence and improve their quality of life.
References
An * indicates studies included in the review
*Aldi, C., Crigler, A., Kates-McElrath, K., Long, B., Smith, H., Rehak, K., & Wilkinson, L. (2016). Examining the effects of video modeling and prompts to teach activities of daily living skills. Behavior Analysis in Practice, 9(4), 384-388https://doi.org/10.1007/s40617-016-0127-y
Ayres, K. M., & Langone, J. (2005). Intervention and instruction with video for students with autism: A review of the literature. Education and Training in Developmental Disabilities, 40(2), 183–196. https://www.jstor.org/stable/23880090
Ayres, K. M., Mechling, L., & Sansosti, F. J. (2013). The use of mobile technologies to assist with life skills/independence of students with moderate/severe intellectual disability and/or autism spectrum disorders: Considerations for the future of school psychology. Psychology in the Schools, 50(3), 259–271. https://doi.org/10.1002/pits.21673
Baker, K., Stavropoulos, K. K. M., Baker, B. L., & Blacher, J. (2021). Daily living skills in adolescents with autism spectrum disorder: Implications for intervention and independence. Research in Autism Spectrum Disorders, 83, 101761. https://doi.org/10.1016/j.rasd.2021.101761
Bal, V., So-Hyun, K., Cheong, D., & Lord, C. (2015). Daily living skills in individuals with autism spectrum disorder from 2 to 21 years of age. Autism, 19(7), 774–784. https://doi.org/10.1177/1362361315575840
Banda, D. R., Dogoe, M. S., & Matuszny, R. M. (2011). Review of video prompting studies with persons with developmental disabilities. Education and Training in Autism in Developmental Disabilities, 46(4), 514–527. https://jstor.org/stable/24232363
Baumgart, D., & VanWalleghem, J. (1987). Teaching sight words: A comparison between computer-assisted and teacher-taught methods. Education and Training in Mental Retardation, 56–65. https://www.jstor.org/stable/23878350
Bennett, K. D., & Dukes, C. (2014). A systematic review of teaching daily living skills to adolescents and adults with autism spectrum disorder. Review Journal of Autism and Developmental Disorders, 1, 2–10. https://doi.org/10.1007/s40489-013-0004-3
*Bereznak, S., Ayres, K. M., Mechling, L. C., & Alexander, J. L. (2012).Video self-prompting and mobile technology to increase daily living and vocational independence for students with autism spectrum disorders. Journal of Developmental and Physical Disabilities, 24(3), 269-285https://doi.org/10.1007/s10882-012-9270-8
*Bouck, E. C., Satsangi, R., & Bartlett, W. (2016). Comparing a number line and audio prompts in supporting price comparison by students with intellectual disability. Research in Developmental Disabilities, 53-54, 342-357https://doi.org/10.1016/j.ridd.2016.02.011
*Bouck, E. C., Satsangi, R., & Bartlett, W. (2017). Supporting grocery shopping for students with intellectual disability: A preliminary study. Disability and Rehabilitation: Assistive Technology, 12(6), 605-613https://doi.org/10.1080/17483107.2016.1201152
Bruininks, R. H.,Woodcock, R. W., Weatherman, R. F., & Hill, B. K. (1996). Scales of Independent Behavior-revised. Itasca, IL: Rivers
*Burckley, E., Tincani, M., & Fisher, A. G. (2015). An iPad™-based picture and video activity schedule increases community shopping skills of a young adult with autism spectrum disorder and intellectual disability. Developmental Neurorehabilitation, 18(2), 131-136https://doi.org/10.3109/17518423.2014.945045
*Cakmak, S., & Cakmak, S. (2015). Teaching to intellectual disability individuals the shopping skill through iPad. European Journal of Educational Research, 4(4), 177–183. https://doi.org/10.12973/eu-jer.4.4.177
*Cannella-Malone, H., Sigafoos, J., O'Reilly, M., de la Cruz, B., Edrisinha, C., & Lancioni, G. E. (2006). Comparing video prompting to video modeling for teaching daily living skills to six adults with developmental disabilities. Education and Training in Developmental Disabilities, 41(4), 344–356. https://www.jstor.org/stable/23879661
*Chen, B. B., & Yakubova, G. (2019). Promoting independence with vocational audio and video prompting for students with ASD. TEACHING Exceptional Children, 52(2), 98-106https://doi.org/10.1177/0040059919874308
Cihak, D. F., Kessler, K. B., & Alberto, P. A. (2007). Generalized use of handheld prompting system. Research in Developmental Disabilities, 28, 397–408. https://doi.org/10.1016/j.ridd.2006.05.003
Cullen, J. M., Alber-Morgan, S., Simmons-Reed, E., & Izzo, M. V. (2017a). Effects of self-directed video prompting using iPads on the vocational task completion of young adults with intellectual and developmental disabilities. Journal of Vocational Rehabilitation, 46(3), 361–375. https://doi.org/10.3233/JVR-170873
*Cullen, J. M., Simmons‐Reed, E. A., & Weaver, L. (2017a). Using 21st century video prompting technology to facilitate the independence of individuals with intellectual and developmental disabilities. Psychology in the Schools, 54(9), 965-978https://doi.org/10.1002/pits.22056
Davies, D. K., Stock, S. E., & Wehmeyer, M. L. (2002). Enhancing independent task performance for individuals with mental retardation through use of a handheld self-directed visual and audio prompting system. Education & Training in Mental Retardation & Developmental Disabilities,37(2), 209–218. https://jstor.org/stable/23879836
Delano, M. E. (2007). Video modeling interventions for individuals with autism. Remedial and Special Education, 28(1), 33–42. https://doi.org/10.1177/07419325070280010401
den Brok, W. L. J. E., & Sterkenburg, P. S. (2015). Self-controlled technologies to support skill attainment in persons with an autism spectrum disorder and/or an intellectual disability: A systematic literature review. Disability and Rehabilitation Assistive Technology, 10, 1–10. https://doi.org/10.3109/17483107.2014.921248.
Ferguson, H., Myles, B. S., & Hagiwara, T. (2005). Using a personal digital assistant to enhance the independence of an adolescent with Asperger syndrome. Education and Training in Developmental Disabilities, 40(1), 60–67. https://jstor.org/stable/23879772
Ford, K., Wang, M., & Koegel, L. K. (2021). Use of videoconferencing intervention and systematic hierarchy to teach daily living skills to young adults with autism spectrum disorder. Journal of Positive Behavior Interventions, 23(2), 81–92. https://doi.org/10.1177/1098300720921214
Fukuda, H., Morishita, T., Ogata, T., Saita, K., Hyakutake, K., Watanabe, J., Shiota, E., & Inoue, T. (2016). Tailor-made rehabilitation approach using multiple types of hybrid assistive limb robots for acute stroke patients. Assistive Technology, 28, 53–56. https://doi.org/10.1080/10400435.2015.1080768
Gardner, S., & Wolfe, P. (2013). Use of video modeling and video prompting interventions for teaching daily living skills to individuals with autism spectrum disorders: A review. Research and Practice for Persons with Severe Disabilities, 38(2), 73–87. https://doi.org/10.2511/027494813807714555
*Gardner, S. J., & Wolfe, P. S. (2019). Results of a video prompting intervention package impacting dishwashing skill acquisition for adolescents with autism. Journal of Special Education Technology, 34(3), 147-161https://doi.org/10.1177/0162643418802666
*Gil, V., Bennett, K. D., & Barbetta, P. M. (2019). Teaching young adults with intellectual disability grocery shopping skills in a community setting using least-to-most prompting. Behavior Analysis in Practice, 12(3), 649-653https://doi.org/10.1007/s40617-019-00340-x
*Goodson, J., Sigafoos, J., O' Reilly, M., Cannella, H., & Lancioni, G. E. (2007). Evaluation of a video-based error correction procedure for teaching a domestic skill to individuals with developmental disabilities. Research in Developmental Disabilities, 28(5), 458-467https://doi.org/10.1016/j.ridd.2006.06.002
*Haring, T. G., Kennedy, C. H., Adams, M. J., & Pitts-Conway, V. (1987). Teaching generalization of purchasing skills across community settings to autistic youth using videotape modeling. Journal of Applied Behavior Analysis, 20, 89-96https://doi.org/10.1901/jaba.1987.20-89
Harrison, P. L., & Oakland, T. (2003). Adaptive behavior assessment system (2nd ed.). The Psychological Corporation.
Hedges, S. H., Odom, S. L., Hume, K., & Sam, A. (2018). Technology use as a support tool by secondary students with autism. Autism, 22(1), 70–79. https://doi.org/10.1177/1362361317717976
Hendricks, D. R., & Wehman, P. (2009). Transition from school to adulthood for youth with autism spectrum disorders: Review and recommendations. Focus on Autism and Other Developmental Disabilities, 24(2), 77–88. https://doi.org/10.1177/1088357608329827
*Hill, D. A., Belcher, L., Brigman, H. E., Renner, S., & Stephens, B. (2013). The apple iPad ™ as an innovative employment support for young adults with autism spectrum disorder and other developmental disabilities. Journal of Applied Rehabilitation Counseling, 44(1), 28-37https://doi.org/10.1891/0047-2220.44.1.28
Holland, J., & Holland, J. (2014). Implications of shifting technology in education. TechTrends, 58, 16–25. https://doi.org/10.1007/s11528-014-0748-3
*Horn, J. A., Miltenberger, R. G., Weil, T., Mowery, J., Conn, M., & Sams, L. (2008). Teaching laundry skills to individuals with developmental disabilities using video prompting. International Journal of Behavioral Consultation and Therapy, 4(3), 279–286https://doi.org/10.1037/h0100857
Individuals With Disabilities Education Act of 2004, 20 U.S.C. § 1400 et seq. (2004). https://uscode.house.gov/view.xhtml?path=/prelim@title20/chapter33&edition=prelim
Jarbrink, K., McCrone, P., Fombonne, E., Zanden, H., & Knapp, M. (2007). Cost-impact of young adults with high-functional autistic spectrum disorder. Research in Developmental Disabilities, 28(1), 94–104. https://doi.org/10.1016/j.ridd.2005.11.002
*Kellems, R. O., Rickard, T. H., Okray, D. A., Sauer-Sagiv, L., & Washburn, B. (2018). iPad® video prompting to teach young adults with disabilities independent living skills: A maintenance study. Career Development and Transition for Exceptional Individuals, 41(3), 175-184https://doi.org/10.1177/2165143417719078
Krauss, M. W., Seltzer, M. M., & Jacobson, H. T. (2005). Adults with autism living at home or in non-family settings: Positive and negative aspects of residential status. Journal of Intellectual Disability Research, 49(2), 111–124. https://doi.org/10.1111/j.1365-2788.2004.00599.x
Lancioni, G. (2017). Assistive technology for people with developmental disabilities. International Journal of Developmental Disabilities, 63, 187–189. https://doi.org/10.1080/20473869.2017.1331787
Matson, J. L., Dempsey, T., & Fodstad, J. C. (2009). The effect of autism spectrum disorders on adaptive independent living skills in adults with severe intellectual disability. Research in Developmental Disabilities, 30(6), 1201–1211. https://doi.org/10.1016/j.ridd.2009.04.001
*McMahon, D. D., Smith, C. C., Cihak, D. F., Wright, R., & Gibbons, M. M. (2015). Effects of a digital navigation aids on adults with intellectual disabilities: Comparison of paper map, google maps, and augmented reality. Journal of Special Education Technology, 30(3), 157–165https://doi.org/10.1177/0162643415618927
Mechling, L. C., Ayres, K. M., Foster, A. L., & Bryant, K. J. (2013). Comparing the effects of commercially available and custom-made video prompting for teaching cooking skills to high school students with autism. Remedial & Special Education, 34(6), 371-383https://doi.org/10.1177/0741932513494856
*Mechling, L. C., Ayres, K. M., Foster, A. L., & Bryant, K. J. (2015). Evaluation of generalized performance across materials when using video technology by students with autism spectrum disorder and moderate intellectual disability. Focus on Autism and Other Developmental Disabilities, 30(4), 208–221.http://dx.doi.org/https://doi.org/10.1177/1088357614528795
Mechling, L. C., & Gustafson, M. R. (2008). Comparison of static picture and video prompting on the performance of cooking-related tasks by students with autism. Journal of Special Education Technology, 23(3), 31–45. https://doi.org/10.1177/016264340802300304
*Mechling, L., & O'Brien, E. (2010). Computer-based video instruction to teach students with intellectual disabilities to use public bus transportation. Education and Training in Autism and Developmental Disabilities, 45(2), 230–241. https://www.jstor.org/stable/23879809
National Autism Center (2009) National Standards Report. Randolph, MA: National Autism Center.
Neeley, L. C., Ganz, J. B., Davis, J. L., Boles, M. B., Hong, E. R., Ninci, J., & Gilliland, W. D. (2016). Generalization and maintenance of functional living skills for individuals with autism spectrum disorder: A review and meta-analysis. Review Journal of Autism and Developmental Disorders, 3(1), 37–47. https://doi.org/10.1007/s40489-015-0064-7
Newman, L., Wagner, M., Knokey, A.-M., Marder, C., Nagle, K., Shaver, D., Wei, X., with Cameto, R., Contreras, E., Ferguson, K., Greene, S., and Schwarting, M. (2011). The Post-High School Outcomes of Young Adults With Disabilities up to 8 Years After High School. A Report From the National Longitudinal Transition Study-2(NLTS2) (NCSER 2011–3005). Menlo Park, CA: SRI International.
*O'Handley, R. D., & Allen, K. D. (2017). An evaluation of the production effects of video self-modeling. Research in Developmental Disabilities, 71, 35-41
Palmen, A., Didden, R., & Lang, R. (2012). A systematic review of behavioral intervention research on adaptive skill building in high-functioning young adults with autism spectrum disorder. Research in Autism Spectrum Disorders, 6(2), 602–617. https://doi.org/10.1016/j.rasd.2011.10.001
*Pérez-Fuster, P., Sevilla, J., & Herrera, G. (2019). Enhancing daily living skills in four adults with autism spectrum disorder through an embodied digital technology-mediated intervention. Research in Autism Spectrum Disorders, 58, 54–67. https://doi.org/10.1016/j.rasd.2018.08.006
Peterson, C., Maier, S. F., & Seligman, M. E. (1993). Learned helplessness: A theory for the age of personal control. Oxford University Press.
Shic, F., & Goodwin, M. (2015). Introduction to technologies in the daily lives of individuals with autism. Journal of Autism and Developmental Disorders, 45(12), 3773–3776. https://doi.org/10.1007/s10803-015-2640-1
Shukla-Mehta, S., Miller, T., & Callahan, K. (2010). Evaluating the effectiveness of video instruction on social and communication skills training for children with autism spectrum disorders: A review of the literature. Focus on Autism and Other Developmental Disabilities, 25(1), 23–36. https://doi.org/10.1177/1088357609352901
Sharmin, M., Hossain, M. M., Saha, A., Das, M., Maxwell, M., & Ahmed, S. (2018). From research to practice: Informing the design of autism support smart technology. Proceedings of the 2018 CHI Conference on Human Factors in Computing Systems. Association for Computing Machinery, New York, NY, USA, Paper 102, 1–16. https://doi.org/10.1145/3173574.3173676
*Sigafoos, J., O'Reilly, M., Cannella, H., Edrisinha, C., de la Cruz, B., Upadhyaya, M., Lancioni, G. E., Hundley, A., Andrews, A., Garver, C., & Young, D. (2007). Evaluation of a video prompting and fading procedure for teaching dish washing skills to adults with developmental disabilities. Journal of Behavioral Education, 16(2), 93-109https://doi.org/10.1007/s10864-006-9004-z
*Sigafoos, J., O'Reilly, M., Cannella, H., Upadhyaya, M., Edrisinha, C., Lancioni, G. E., Hundley, A., Andrews, A., Garver, C., & Young, D. (2005). Computer-presented video prompting for teaching microwave oven use to three adults with developmental disabilities. Journal of Behavioral Education, 14(3), 189-201https://doi.org/10.1007/s10864-005-6297-2
*Smith, K. A., Ayres, K. A., Alexander, J., Ledford, J. R., Shepley, C., & Shepley, S. B. (2016). Initiation and generalization of self-instructional skills in adolescents with autism and intellectual disability. Journal of Autism and Developmental Disorders, 46(4), 1196-1209https://doi.org/10.1007/s10803-015-2654-8
Smith, L. E., Greenber, J. S., & Seltzer, M. M. (2012). Social support and well-being at mid-life among mothers of adolescents and adults with autism spectrum disorders. Journal of Autism and Developmental Disorders, 42(9), 1818–1826. https://doi.org/10.1007/s10803-011-1420-9
Smith, L. E., Maenner, M. J., & Seltzer, M. M. (2012). Developmental trajectories in adolescents and adults with autism: The case of daily living skills. Journal of the American Academy of Child and Adolescent Psychiatry, 51(6), 622–631. https://doi.org/10.1016/j.jaac.2012.03.001
Sparrow, S. S., Balla, D. A., & Cicchetti, D. U. (1984). Vineland adaptive behavior scales. American Guidance Service.
Stancliffe, R. T., Hayden, M. F., Lakin, K. C. (2000). Quality and content of individualized habilitation plan objectives in residential settings. Education and Training in Mental Retardation and Developmental Disabilities, 35(2), 191–207. https://www.jstor.org/stable/23879943
Stokes, T. F., & Baer, D. M. (1977). An implicit technology of generalization. Journal of Applied Behavior Analysis, 10(2), 349–367. https://doi.org/10.1901/jaba.1977.10-349
*Thomas, E. M., DeBar, R. M., Vladescu, J. C., & Townsend, D. B. (2020). A comparison of video modeling and video prompting by adolescents with ASD. Behavior Analysis in Practice, 13(1), 40-52https://doi.org/10.1007/s40617-019-00402-0
*Van Laarhoven, T., & Van Laarhoven-Myers, T. (2006). Comparison of three video-based instructional procedures for teaching daily living skills to persons with developmental disabilities. Education and Training in Developmental Disabilities, 41(4), 365-381https://doi.org/10.1177/1088357610380412
Vermeulen, P. (2013). I am special: A workbook to help children, teens and adults with autism spectrum disorders to understand their diagnosis, gain confidence and thrive (2nd ed.) London: Jessica Kingsley Publishers.
Wertalik, J. L., & Kubina, R. M. (2018). Comparison of TAGteach and video modeling to teach daily living skills to adolescents with autism. Journal of Behavioral Education, 27, 279–300. https://doi.org/10.1007/s10864-017-9285-4
What Works Clearinghouse, Institute of Education Sciences, U.S. Department of Education. (2020). What works clearinghouse: Standards handbook (Version 4.1).
Yucesoy-Ozkan, S., Gulboy, E., & Kaya, F. (2018). Teaching children with intellectual disabilities through video prompting: Smartphone vs tablet. International Journal of Early Childhood Special Education, 10(1), 32–48. https://doi.org/10.20489/intjecse.454433
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hrabal, J.M., Davis, T.N. & Wicker, M.R. The Use of Technology to Teach Daily Living Skills for Adults with Autism: a Systematic Review. Adv Neurodev Disord 7, 443–458 (2023). https://doi.org/10.1007/s41252-022-00255-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41252-022-00255-9