
Abstract
Objectives
Self-injurious behavior (SIB) refers to any repeated self-directed, non-suicidal, behavior that may cause or has the potential to cause physical harm to the person’s body. Behavioral interventions provide the standard evidence-based treatments for SIB by people with autism spectrum disorder (ASD) and intellectual disabilities (ID). Translating the proven effectiveness of behavioral interventions to treatment of self-injury in community settings by clinicians and caregivers has not been totally successful. The aim of the present study was to advance translational research by providing real-time telehealth consultation to a treatment team at a community-based mental health agency that provided inpatient and outpatient services to individuals with ASD and ID.
Method
The participants of this single-case experimental study were three adolescents with ASD who had been referred for services because of their increasingly unmanageable SIB both at home and at school. The telehealth consultant provided real-time assistance to the treatment team within a translational model of care in the development and implementation of a behavior support plan and an informal mindfulness-based Soles of the Feet (SoF) program.
Results
Both visual and statistical analyses demonstrated reductions in the frequency of SIB for all three adolescents, with overall clinically significant reductions only with the SoF intervention.
Conclusion
The results of this translational study suggest that telehealth consultation might be a viable technological alternative in situations which preclude face-to-face consultation. Telehealth consultation could be one method of supporting people with behavioral difficulties during pandemics, such as COVID-19.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Self-injurious behavior (SIB) in autism spectrum disorder (ASD) refers to any repeated self-directed, non-suicidal, behavior that may cause or has the potential to cause physical harm to the person’s body. SIB may take different forms across individuals, including but not limited to head banging, pinching, slapping, scratching, biting, eye poking or gouging, hair pulling, and punching self. Risk factors for SIB include severity of ASD, deficits in receptive and expressive language, comorbid genetic disorders, and changes in life events (e.g., physical illness, change in caregiver, separation from a significant person, assault from another person, change in residence, physical and sexual trauma, and various medical conditions). While its prevalence in individuals with intellectual disabilities (ID) ranges from 4 to 30% (Hoch et al., 2016), it hovers around 30% for children and adolescents with ASD (e.g., Duerden et al., 2012; Lance et al., 2014; Soke et al., 2016).
A number of treatments have been researched for either reducing or eliminating SIB in individuals with ID and ASD. Historically, in the absence of effective treatments, psychopharmacological approaches were used as default treatments for the safety of the individuals, essentially to sedate rather than treat them (Aman & Singh, 1988). Since then, research has shown that few psychotropic drugs are truly effective without concomitant adverse effects in treating SIB (Deb, 2016), perhaps with the exception of risperidone (Aman et al., 2002) and possibly aripiprazole in the short-term management of challenging behavior (VanDerwall et al., 2021). Although several trials of different medications have been undertaken, even current psychopharmacological treatments are rarely based on evidence of their purported mechanism of action for treating SIB in individuals with ID and ASD. Studies are needed that test specific hypotheses for the effects of psychopharmacology on SIB, such as the study by Singh et al. (1994) that tested if decreased dopaminergic neurotransmission leads to an increase in pica (i.e., SIB due to ingesting non-food items) in some individuals with intellectual and developmental disabilities (IDD). Although not approved by the US Food and Drug Administration (FDA) for this purpose, naloxone and naltrexone act as competitive antagonist at opioid receptor sites and thus provide a testable hypothesis for their effects on SIB. Indeed, clinical cases and a few small studies attest to the possible effectiveness of these drugs (Fischer et al., 2020) but await randomized controlled trials to establish their efficacy.
At present, behavioral interventions provide the standard evidence-based treatments for SIB in ASD. Although the evidence base varies by specific treatment procedures, overall antecedent and consequence interventions are the two most commonly used behavioral interventions. The strength of evidence for behavioral treatments has been classified based on the Kratochwill et al. (2010) criteria for evidence-based treatments (see Hoch et al., 2016). While no antecedent behavioral interventions can be rated as having strong evidence, procedures that include non-contingent reinforcement have moderate evidence. Antecedent procedures with limited evidence include manipulating motivating operation-based interventions, use of high probability instructional sequence, response blocking, and fading the use of protective equipment. In terms of consequence interventions, while no single procedure can be rated as having strong evidence, multi-component procedures with the following as the primary component meet the criteria for strong evidence: punishment-based procedures (e.g., contingent use of electric shock, aromatic ammonia, water mist, overcorrection, and protective equipment) and differential reinforcement-based procedures (e.g., differential reinforcement of other behavior, differential reinforcement of alternative behavior, functional communication training). There is moderate evidence for punishment and differential reinforcement procedures and limited evidence for extinction-based procedures and non-contingent reinforcement-based procedures when each of these procedures is used alone. However, punishment-based procedures are now not recommended for the treatment of any behavioral condition in any population for ethical reasons.
The relatively small literature on other approaches for treating SIB in individuals with ID and ASD, such as sensory integration therapy and conscious discipline, have questionable evidence for their effectiveness (Hoch et al., 2016). This means that behavioral interventions remain the treatment of choice. Even though there is good evidence for the effectiveness of behavioral interventions, there is a translational problem because the well-controlled published research has not been found to be equally effective under real world conditions when therapists are unable to control nonspecific variables that potentiate the individual’s SIB. These variables may include the individual’s private events (including emotional state); the caregivers’ stress, burnout, and compassion fatigue; and the behavior analyst’s limited experience with low frequency but high intensity SIB of individuals with ASD at the severe and profound levels of functioning. Such variables may compromise the integrity and fidelity of implementation of an otherwise well-developed behavior analytic intervention plan.
Recently, mindfulness-based interventions have emerged as a viable intervention that can be used as an alternative to or adjunctively with other interventions to produce behavior change in individuals with ID and ASD (Singh & Hwang, 2020). Mindfulness-based interventions have been used in three general ways to assist individuals with ASD: (1) teach mindfulness-based programs directly to the individuals so that they can achieve inhibitory control of their challenging behaviors; (2) teach mindfulness-based interventions to parents and other caregivers with the expectation that the effects will cascade or spillover to the individuals with ASD in their care; and (3) teach mindfulness-based interventions to the parents and other caregivers and the individuals with ASD in parallel so that the effects on the individuals are enhanced by the cascading and spillover effects from parental and caregiver mindfulness and also from their own mindfulness practices (Singh & Hwang, 2021).
Translational research refers to “bench-to-bedside” approaches that endeavor to harness knowledge gained from basic research to developing therapeutics for patient care (Woolf, 2008). A similar approach is beginning to emerge with regard to translating behavioral and mindfulness-based research to “patient care” by making it accessible through telehealth behavioral consultation to individuals that need these interventions. Skilled behavior analysts have used telehealth as a means of conducting stimulus preference assessments (Ausenhus & Higgins, 2019), conducting functional analyses of problem behavior (Wacker et al., 2013), delivering interventions to individuals with ID (Pellegrino et al., 2020), and teaching caregivers (including parents and teachers) to deliver well-designed behavioral programs (Fischer et al., 2017; LeBlanc et al., 2020; Tomlinson et al., 2018). During uncontrollable environmental and medical events, such as the current COVID-19 pandemic, the use of telehealth can be a saving grace for families and caregivers of children and adolescents with ASD who evince intractable SIB and aggression. The aim of the present study was to extend translational research by providing real-time telehealth consultation to a treatment team at a community-based mental health agency that provided inpatient and outpatient services to individuals with ID and ASD.
Method
Participants
Therapists
The therapists worked at a community-based mental health agency that specialized in the treatment of individuals with ID and ASD. The services were provided by a multidisciplinary team of therapists including a behavior analyst (BCBA-D), a psychiatrist with expertise in neurodevelopmental disorders, a social worker, an occupational therapist, and a registered nurse. The members had been working as a cohesive team for over 7 years and had a broad range of therapeutic skills. Clients were admitted on a short-term basis (up to 2 months) for crisis stabilization, assessment, development of a treatment plan, and initial implementation of the plan and then discharged with follow-up appointment. The discharge plans included training of therapists of the receiving residential agency, or of parents if the client was being discharged to parental care.
Clients
The clients were three adolescents with ASD. They had been referred for services by their school counselor because of increasingly unmanageable SIB both at home and at school. The school counselor had developed and implemented behavior support plans for each of the adolescents, but outcome data showed the plans were not very effective and the school district decided that they needed additional assistance with these adolescents. The school had previously used the outpatient services of the community-based mental health agency for their students with various psychological and psychiatric issues, including ASD, and found their programs to be very helpful. However, the school and the mental health agency had limited success with these three adolescents. Because of failure on successive admissions in the mental health agency’s behavioral treatment of these three adolescents, the mental health agency and school district requested telehealth consultation for the treatment of self-injury exhibited by these three adolescents who were due to be admitted as inpatients for the fourth time.
Alex (client names are pseudonyms) was a 17-year-old adolescent with ASD who functioned at the mild level of intellectual disability and had a 12-year history of self-injury. The topography of his self-injury included hitting the head, face, and other body parts. Brandon was a 19-year-old adolescent with ASD who functioned at the mild level of intellectual disability and had an 11-year history of self-injury that was sporadic at first and then occurred on a daily basis. The topography of his self-injury included arm and hand biting, and self-pinching. Charlie was a 13-year-old adolescent with ASD who functioned at the mild level of intellectual disability and had a 5-year history of self-injury. The topography of his self-injury included hitting his hand on hard objects and eye poking. The adolescents did not have any diagnosed comorbid psychiatric disorders and were not on any psychotropic medications for their self-injury. This is not surprising given that the prevalence of neuroleptic medication for behavioral issues is only 6% (Lopata et al., 2013) in higher functioning individuals with ASD, as in the present study. Their most recent functional behavior assessments based on the Questions about Behavioral Function (QABF; Paclawskyj et al., 2000) rating scale produced mixed motivations for their self-injury, with escape and non-social receiving slightly higher ratings than physical, tangibles, and attention.
Procedure
Telehealth Consultation
The school district and the mental health agency’s treatment team requested telehealth consultation for intractable self-injury of the three adolescents with ASD. Real-time consultation involved the telehealth consultant working with the treatment team that was led by the behavior analyst. The extensive experience and expertise of the treatment team’s behavior analyst resulted in the consultant being used in an advisory capacity in terms of assessing the fidelity of the team’s development, staff training, and implementation of the behavior support plan (BSP). Given the treatment team’s lack of experience in developing and implementing mindfulness-based programs, the consultant was involved in providing real-time training to the behavior analyst in mindfulness of the breath and Soles of the Feet (SoF) mindfulness-based program, and in collaborating with the behavior analyst in the training of the three adolescents in the SoF program. Training was conducted in real time via Zoom, and all baseline and outcome data were viewed through WhatsApp, which has end-to-end encryption for security.
Process
The telehealth consultant assisted the treatment team in implementing the procedure in real time in two phases: (1) advising on developing and implementing a BSP and (2) being closely involved in developing and implementing an informal mindfulness-based Soles of the Feet (SoF) program. Except for the details of the interventions, the general methodology was planned to be similar for both phases. In practice, the BSP was developed, implemented, and evaluated first, followed by a 2-week no-treatment period during which the treatment team, parents of the adolescents, the adolescents themselves, and the telehealth consultant discussed the next steps in adopting a non-pharmacological alternative treatment. After evaluating extant research data on likely treatment alternatives, the consensus was reached for the treatment team to implement and assess the utility of the SoF program. The strong endorsement of the SoF program by the adolescents was an important deciding factor. They particularly liked the thought of being in control of their own treatment with this positive portable self-regulation program.
Experimental Design
A multiple-baseline design across three participants was used for both the behavioral and mindfulness-based interventions (Barlow et al., 2009). This design was chosen because it has internal validity for evaluating outcomes of interventions in small samples. In addition, the behavior analyst and Registered Behavior Technicians (RBTs) had previous experience in using this research design to assess behavioral interventions with other clients.
Baseline
To minimize threats to internal validity, the adolescents were randomly assigned to one of the three baselines. During baseline, data on each adolescent’s number of self-injurious events were collected by a pool of four RBTs trained in behavioral observations. No variables were manipulated during baseline. Inpatient staff continued to use whatever clinical management techniques they were using prior to initiation of baseline data collection. Data were collected at about the same time twice daily, once in the morning and once in the afternoon, while the adolescents engaged in their routine inpatient program. Each observation session was for a period of 3 h. The same pool of four observers and observation system were utilized during baseline and intervention phases. The baseline for both BSP and SoF interventions was for 3, 5, and 8 days.
Behavior Support Plan
Following baseline data collection, the behavior analyst developed the adolescents’ BSP based on standard behavior analytic practices used in the field of IDD (e.g., Bambara & Knoster, 2009). Functional assessment data were used to generate specific and general hypotheses for the adolescents’ self-injury. Then comprehensive BSPs were developed that included the following components: modifications of setting events and antecedent conditions, teaching alternative skills, consequence interventions, and long-term supports. The plan also included strategies for training care staff on daily data collection and implementation of the programs, and schedule for periodic review of progress and revisions of the plans, as indicated by the data. The intervention was implemented for 37 days.
Mindfulness-Based Program
The consultant taught the behavior analyst a basic meditation on the breath practice (see Table 1), which is a requirement for mindfulness teachers (Carmody & Baer, 2009; McCown et al., 2010), at the termination of the BSP for the three adolescents. This training was requested by the behavior analyst so that authenticity of mindfulness practice could be initiated and later maintained when used in the absence of the telehealth consultant. Then the telehealth consultant taught the behavior analyst the basics of the SoF program. While the SoF program is simple, it takes substantial practice to use it proficiently and to teach clients with competency. Training involved verbal instructions, modeling, demonstrations, and return demonstrations. The behavior analyst’s competency was objectively rated by a rater independent of the telehealth consultant on the 40-item SoF Trainer Monitoring Checklist. Training was terminated when the behavior analyst achieved a score of 100% on the checklist. Step-by-step instructions for teaching the SoF program are presented in the Singh et al. (2011) training manual and, more recently, by Felver and Singh (2020). The behavior analyst used the earlier manual for this training. The total training time for the behavior analyst to reach competency was a total of 5 h (1 h per day for 5 days), but additional time was spent in practicing the SoF procedure to achieve fluency in teaching it to clients.
Once the behavior analyst achieved proficiency in using and teaching the SoF program, the behavior analyst took the lead in teaching the three adolescents to use it for their self-injury. The telehealth consultant provided encouragement and assistance (in vivo via telehealth), as needed. The behavior analyst essentially followed the Singh et al. (2011) instruction manual as a general guide and adapted the language and instructions aligned with each adolescent’s abilities and needs. During each training session, an adolescent was seated comfortably on a soft straight-backed chair with feet flat on the floor and hands resting gently on the thighs. The adolescent kept his eyes gently closed to increase concentration and narrow his focus to the present moment. Then, the behavior analyst provided the SoF instructions in a calm and soft voice, taking the adolescent through the steps outlined in Table 2. Once the adolescent was able to engage in the basic SoF program, the behavior analyst used the training steps outlined in the SoF instruction manual to assist the adolescent to operationalize the precursors to his rising urge to engage in self-injury and then to use the SoF program with the earliest precursor to self-injury. The behavior analyst then discussed with the adolescent how to recognize current and new precursors to his self-injury in daily life and how to use the SoF program to effectively manage his self-injury at the earliest moment of arising.
The behavior analyst taught the adolescents individually in a 30-min session, on Monday, Wednesday, and Friday during the first week of training, reduced it to 15-min per session in the second week, and met with the adolescents for 10 mins each weekday thereafter until discharge to review the data on their use of the SoF program, to respond to their questions, and to reinforce their self-management of self-injury. In addition, the inpatient staff nudged the adolescents to use the SoF program when they felt the urge to engage in self-injury. Each adolescent used the SoF program for 37 days before being discharged home to their parents. Two weeks prior to the adolescents being discharged, their parents were also taught the SoF program by the behavior analyst so that they could encourage and reinforce their children in its use at home.
Fidelity of Training
Given the extensive experience of behavior analysts in training staff to implement BSPs, no measure of fidelity of training was deemed necessary by the treatment team. However, the fidelity of the training of the behavior analyst in SoF by the telehealth consultant and the subsequent training of SoF provided by the behavior analyst to the adolescents were new and needed to be measured. Two aspects of fidelity were assessed: structural fidelity (i.e., what is being taught) and process fidelity (i.e., how the contents are being taught) (Feagans Gould et al., 2016). An additional mindfulness instructor experienced in teaching practitioners to use the SoF program was remotely present via Zoom during the training of the behavior analyst and when the behavior analyst taught the adolescents. This mindfulness instructor’s only role was to collect the fidelity data in real time. The four commonly accepted facets of fidelity of implementation (Dane & Schneider, 1998; Dusenbury et al., 2003) were adapted for monitoring the fidelity of training in the SoF program. These facets included the following: adherence (i.e., extent to which the core training components of the SoF program were taught); dosage (i.e., the number of training sessions delivered); quality (i.e., extent to which the trainer delivered the program components and contents as intended); and responsiveness (i.e., extent to which the trainer was responsive and skillfully engaged with the adolescents). The structural and process fidelity were assessed at 100% for the training of the behavior analyst by the telehealth consultant and ranged from 85 to 98% for the training of the three adolescents by the behavior analyst.
SoF Trainer
The telehealth consultant had a long-standing personal meditation practice for over 40 years, over 30 years of experience as a mindfulness teacher, and was an experienced behavior analyst at the BCBA-D level. The fidelity data collector had an on-going personal meditation practice, a 10-year history as a mindfulness instructor, but no formal training in behavior analysis.
Measures
Events and Response Definitions
In general, self-injury is any repeated self-directed, non-suicidal, behavior that may cause or has the potential to cause physical harm to the person’s body. Specifically, the universe of self-injurious behaviors of the three adolescents was defined as including hitting the head, face, and other body parts; arm and hand biting and self-pinching; and hand hitting and eye poking. Each instance of one of these behaviors was counted as a single event. A trained pool of four RBTs collected the data for 3 h in the morning and another 3 h in the afternoon. Random pairs of RBTs were scheduled to collect the data each day during the morning and afternoon shifts, with one as the primary data collector and the other as a reliability data collector. Reliability data were collected during a third of each session (i.e., an hour in the morning and an hour in the afternoon). An agreement was defined as the primary and reliability data collector recording the same self-injurious event as occurring at about the same time. Percentage of inter-rater agreement was calculated for the whole period of observation by dividing agreements by agreements plus disagreements and multiplying by 100. Agreement in each case was 100%, likely due to the very discrete nature of the target behaviors and the extensive experience of the RBTs in reliably collecting such data.
Social Validity
The 8-item Abbreviated Acceptability Rating Profile (AARP; Tarnowski & Simonian, 1992) was used to assess the social validity of the two interventions for the three adolescents. The language used in the AARP was modified to make it specific to the BSP and SoF interventions used in this translational study. The adolescents’ five treatment team members consensually rated each item on a 6-point Likert scale (i.e., 1 = strongly disagree, 2 = disagree, 3 = slightly disagree, 4 = slightly agree, 5 = agree, and 6 = strongly agree) for both interventions at the discharge conference on the day the adolescents were discharged home. Higher ratings indicate higher social validity.
The adolescents also provided social validity data from their perspective as recipients of the interventions. They rated a 5-item social validity questionnaire adapted from a previous study utilizing the SoF program (Singh et al., 2019). The five items asked questions pertaining to acceptability of the intervention, effectiveness, side effects, ease of use, and recommend the intervention to others. The adolescents independently rated each item on a 5-point Likert scale (i.e., 1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree) for both interventions on the morning of the day they were discharged home. Higher ratings indicate higher social validity.
Data Analyses
Data were analyzed visually and statistically. In visual analysis, individual participant data were graphed, and the levels of functional relation between the manipulation of the intervention (BSP or SoF) and changes in self-injury were examined. The rationale for reliance on visual analysis of data is that an intervention should produce large and consistent effects that should be visually evident to be clinically significant. However, visual analysis alone may produce differing interpretations of the significance of the data depending on the expertise of the person performing the visual analysis or if aspects of the data itself (e.g., autocorrelation in time-series data) compromise the visual analysis (Kratochwill et al., 2014). Thus, pairing the visual analysis with single-case statistical analysis strengthens data analyses in single-case experimental design studies.
Descriptive statistics including mean and range occurrence of self-injury were computed for each adolescent and overall for baselines, BSP, and SoF interventions. The differences between phases were analyzed using the novel TAU-U method that estimates non-overlap between phases while simultaneously controlling for trends within a phase (Parker et al., 2011).
The statistical approach proposed by Jacobson and Truax (1991) was used to examine if reductions in self-injury as a result of BSP and SoF interventions were clinically significant. Jacobson et al. (1984) “propose[d] that a change in therapy is clinically significant when the client moves from the dysfunctional to the functional range during the course of therapy” (p. 340). That is, clinically significant change is evident when the post-treatment average behavior rate falls outside of two standard deviations from the average of dysfunctional population toward functionality. This is the most applicable approach in the case of self-injury due to the difficulty in establishing population norms for individuals with ASD. We estimated the cut-off point for clinical significance based on combined baseline data of all three adolescents. To enhance precision of estimating clinical significance, we computed 95% confidence intervals (CI) around individual and group average daily frequency of self-injury pre- and post-intervention. Clinical significance for the adolescents and overall for each intervention (BSP and SoF) was determined by considering 95% CI.
Results
Visual Analysis
Figure 1 presents the daily frequency of self-injury for each of the adolescents during baseline and intervention with BSP. The frequency of self-injury during baseline averaged to 13.67 (range 12 to 15) for Alex, 7.2 (range 5 to 9) for Brandon, and 10.13 (range 7 to 13) for Charlie. During the intervention, the frequency of self-injury averaged to 12.43 (range 5 to 17) for Alex, 6.14 (range 2 to 10) for Brandon, and 9.76 (range 2 to 14) for Charlie.

Frequency of self-injury during baseline and BSP intervention
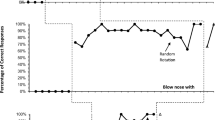
Figure 2 presents the daily frequency of self-injury for each of the adolescents during baseline and intervention with SoF. The frequency of self-injury during baseline averaged to 14.0 (range 13 to 16) for Alex, 9.6 (range 9 to 11) for Brandon, and 10.38 (range 9 to 13) for Charlie. During the intervention, the frequency of self-injury averaged to 3.81 (range 0 to 11) for Alex, 3.92 (range 0 to 12) for Brandon, and 4.62 (range 0 to 13) for Charlie.

Frequency of self-injury during baseline and SoF intervention
Non-overlap Analysis
Table 3 shows the TAU-U coefficients together with standardized (Z) scores indicating no significant differences in SIB between baseline and the BSP intervention, while significant reductions of self-injury for all three adolescents and overall were evident with the SoF intervention (TAU-U range between − 0.84 and − 1).
Clinical Significance
Overall clinically significant reduction of self-injury was observed with the SoF intervention but not with the BSP intervention (Table 3). Specifically, the SoF intervention produced clinically significant improvements in two adolescents (Alex and Brandon), while the average daily number of self-injurious events (4.62) for the third adolescent (Charlie) was below the established cut-off point of 5.40 for clinical significance with only marginal overlap of 95% CI of 1.21 computed as follows (4.62 + 1.21 = 5.83 > 5.40).
Social Validity
The treatment team members consensually rated the social validity of the BSP and SoF interventions on the last day of the adolescents’ inpatient stay before they were discharged home to their parents. The eight items were rated on a 6-point scale, with higher ratings indicating higher social validity (see Table 4). The total score was 27 for BSP and 48 for SoF, indicating greater social validity for the SoF program.
The adolescents individually rated the social validity of the two interventions on the last day of their inpatient stay. The five items were rated on a 5-point scale, with higher ratings indicating higher social validity (see Table 5). Across the three adolescents, the total summed rating for acceptability was 5 for BSP and 18 for SoF, effectiveness 3 for BSP and 18 for SoF, side effects 8 for BSP and 18 for SoF, ease of implementing the intervention 8 for BSP and 14 for SoF, and recommend for use by others 3 for BSP and 18 for SoF. The total summed rating for social validity was 27 for BSP and 86 for SoF, indicating greater social validity for the SoF program.
Discussion
This translational study was designed to provide real-time telehealth consultation to a treatment team at a community-based mental health agency that provided inpatient and outpatient services to individuals with ID and ASD. Telehealth consultation is an important technological advance over face-to-face consultation during the time of COVID-19 pandemic especially for those needing urgent assistance but are working under lockdown conditions. In addition, real-time telehealth services can provide one viable way of reducing mental health care inequity by extending timely services to those with limited resources, those unable to access primary care, or those living in rural areas where specialist services are unavailable. Individuals who have cell phones or can access computers could take advantage of telehealth services in real time when the need is most urgent. Having a family member who engages in severe self-injury or physical aggression toward their caregivers provides good examples of the necessity for telehealth services when other community-based services are unavailable.
There is an emerging research based on the use of telehealth technology in delivering services that include the behavior analytic and mindfulness-based programs for individuals with IDD. For example, as reported by Lee et al. (2015), behavioral consultation in telehealth had its beginnings in the mid-1990s. Wacker et al. (2016) have provided an evidence-based model for using behavioral telehealth services in the community. Furthermore, current research evidence indicates that behavioral telehealth services cover intake, assessment, development, and implementation of BSPs in clinical, school, home, and residential settings, and are not only effective and efficient but also cost-effective (Fischer et al., 2017; Wacker et al., 2016). Although not nearly as extensive as behavioral telehealth services, telehealth mindfulness-based services for individuals with IDD and their caregivers are just emerging (e.g., Myers et al., 2018; Singh et al., 2017).
The present study extended this line of research by providing real-time telehealth consultation for both behavioral and mindfulness-based interventions for the same set of clients with ASD whose treatment team needed assistance with their intractable self-injury. In this case, assistance was provided by a telehealth consultant within a translational model of care in which two evidence-based interventions were successively evaluated by the treatment team using a single-case experimental design. This telehealth consultation incorporated the “bench-to-bedside” medical model (Woolf, 2008) to fast track evidence-based intervention to improve inpatient care for three adolescents with ASD. First, the telehealth consultant assisted the treatment team’s behavior analyst to evaluate the effectiveness of a well-formulated BSP based on functional assessment and positive behavior support principles. This intervention was not very successful for a number of possible reasons, although the treatment team noted that the BSP did not tap into contingencies that may have been affected by the adolescents’ emotional dysregulation. Furthermore, it should be remembered that like any evidence-based intervention, even well-designed and implemented behavior analytic plans may be ineffective for non-specific reasons. Second, the telehealth consultant taught the behavior analyst a basic meditation practice that, with consistent practice over time, will enhance their embodiment of mindfulness. An unintended benefit of this training could be that the behavior analyst’s embodied mindfulness might cascade or spill over to others, including other clients, who have no personal practice of meditation (see Singh & Hwang, 2021). Third, the telehealth consultant enabled the behavior analyst and treatment team to develop and implement with fidelity the SoF intervention that was successful in significantly reducing the adolescent’s self-injury within 37 days, with every expectation that with continued practice the adolescents will eventually eliminate this behavior.
The treatment team was able to include several niceties in the evaluation of their intervention efforts, suggesting curiosity and openness to enhancing the quality of their clinical work. First, they followed the telehealth consultant’s usual practice of developing, implementing, and documenting treatment at a level that is publishable in a medium-to-high impact journal, regardless of whether it is submitted for publication. Working at this standard raises the bar for their daily clinical work and motivates them to keep abreast of relevant research literature. Second, they contextualized their clinical interventions within a single-case experimental design across participants so that they could intensively investigate the effects of two interventions on the adolescents. Third, given that they used a multiple-baseline design, they were careful to randomly assign the adolescents to the baselines to minimize threats to internal validity. Fourth, in terms of pre-intervention training, they collected data for both structural fidelity (i.e., what is being taught) and process fidelity (i.e., how the contents are being taught). While they considered collecting fidelity data on the adolescents’ implementation of the SoF program, practical limitations precluded it because the SoF program is essentially a manipulation of private events that control overt behavior (i.e., self-injurious events). Fifth, they collected inter-rater agreement data on the occurrence of the adolescents’ SIB, an ubiquitous practice in research studies that is rare in daily clinical work. Sixth, they augmented visual analysis of outcome data with statistical analyses—the TAU-U—and statistically evaluated the clinical significance of the behavior change. Finally, they collected social validity data from the treatment team members and from the adolescents themselves.
Limitations and Future Research
The outcomes of this study should be considered in the context of its limitations. This translational study was occasioned by the need to provide effective intervention when the usual evidence-based treatments failed. Thus, the choice of a single-case experimental design was appropriate given that only three adolescents needed the intervention. However, a limitation of single-case experimental designs is that they are internally valid only—we know that when these three adolescents with ASD learned to use SoF contingent on the precursors of their self-injury, the frequency of their self-injury decreased substantially—but not externally valid—we do not know if this intervention would be effective for other adolescents with ASD who engage in self-injury. Furthermore, mindfulness-based programs for individuals with ASD have been found to be effective primarily with those that function at higher cognitive levels, thus limiting the generalizability of these findings to only this population.
The use of the TAU-U statistic, which is increasingly used in single-case experimental design studies (Parker et al., 2011), clearly indicated significant reductions in self-injury with the use of the SoF program with all three adolescents with ASD. This mirrored the traditional visual analysis, thus providing a measure of reliability of interpretation of the behavior change. However, clinically significant difference was statistically evident for only two of the three adolescents when 95% CIs were accounted for based on the Jacobson and Truax (1991) index. This might be explained by higher variability of data for the third adolescent that inflated the estimated CI. However, even on this index, clinically significant changes were evident across the three participants at the group level. Thus, caution should be exercised when extrapolating from statistical analyses of clinical significance in the absence of population norms for the target behavior that is required when using this index.
Another reason for being cautious is that the findings are based on one telehealth consultant working with a specific behavior analyst, with a particular treatment team, at one mental health agency. Numerous non-specific variables were probably in play (e.g., experience of the telehealth consultant as a behavior analyst and a mindfulness teacher, motivation of the mental health agency behavior analyst to learn and practice mindfulness, an enlightened treatment team, and a mental health agency transparent of its own limitations) that may not be replicable in other contexts and with other professionals and mental health agencies. Furthermore, the motivation of the treatment team to succeed was very high, given that successful intervention was urgently needed for the safety of the adolescents (and in maintaining the reputation of the team as being clinically effective). In addition, the novelty of the SoF program may have contributed somewhat to its effectiveness given that informal mindfulness-based programs are the treatments du jour in the field of IDD at present. The use of mindfulness-based programs with children and adolescents, with and without IDD, has increased exponentially over the last decade (Singh & Singh Joy, 2021), and their effectiveness and efficacy continues to be researched and demonstrated across a variety of health, mental health, and educational domains.
This study may be heuristic for further exploration of translational research that takes an evidence-based intervention and translates it into everyday treatment by regular clinicians. While the SoF program is an evidence-based intervention for various emotion regulation problems of individuals with ID and ASD, it has not seeped into the fabric of daily clinical practice of experienced clinicians. Of course, this is not surprising given the gap of about 20 years between research and its translation into everyday practice. Further translational research may shorten this time period. Another consideration for further research is that the real-time telehealth consultation used in the present study might be eminently applicable during pandemics, such as in the era of COVID-19. It could serve two purposes—providing immediate care for those in need of such services and in researching optimal ways for using telehealth to implement and disseminate evidence-based interventions into the community.
References
Aman, M. G., & Singh, N. N. (1988). Psychopharmacology of the developmental disabilities. New York: Springer.
Aman, M. G., De Smedt, G., Derivan, A., Lyons, B., Findling, R. L., & Risperidone Disruptive Behavior Study Group. (2002). Double-blind, placebo-controlled study of risperidone in the treatment of disruptive behaviors in children with subaverage intelligence. American Journal of Psychiatry, 159(8), 1337–1346.
Ausenhus, J. A., & Higgins, W. J. (2019). An evaluation of real-time feedback delivered via telehealth: training staff to conduct preference assessments. Behavior Analysis in Practice, 12(3), 643–648.
Bambara, L. M., & Knoster, T. P. (2009). Designing positive behavior support plans (2nd ed.). Washington: American Association on Intellectual and Developmental Disabilities.
Barlow, D. H., Nock, M., & Hersen, M. (2009). Single-case experimental designs (3rd ed.). New York: Allyn & Bacon.
Carmody, J., & Baer, R. A. (2009). How long does a mindfulness-based stress reduction program need to be? A review of class contact hours and effect sizes for psychological distress. Journal of Clinical Psychology, 65, 627–638.
Dane, A. V., & Schneider, B. H. (1998). Program integrity in primary and early secondary prevention: are implementation effects out of control? Clinical Psychology Review, 18(1), 23–45.
Deb, S. (2016). Psychopharmacology. In N. N. Singh (Ed.), Handbook of evidence-based practices in intellectual and developmental disabilities (pp. 347–381). New York: Springer.
Duerden, E., Oakley, H., Mak-Fan, K., McGrath, P., Taylor, M., et al. (2012). Risk factors associated with self-injurious behaviors in children and adolescents with autism spectrum disorders. Journal of Autism and Developmental Disorders, 42, 2460–2470.
Dusenbury, L., Brannigan, R., Falco, M., & Hansen, W. B. (2003). A review of research on fidelity of implementation: implications for drug abuse prevention in school settings. Health Education Research Theory & Practice, 18(2), 237–256.
Feagans Gould, L., Dariotis, J. K., Greenberg, M. T., & Mendelson, T. (2016). Assessing fidelity of implementation (FOI) for school-based mindfulness and yoga interventions: a systematic review. Mindfulness, 7(1), 5–33.
Felver, J. C., & Singh, N. N. (2020). Mindfulness in the classroom: an evidence-based program to reduce disruptive behavior and increase academic engagement. Oakland: New Harbinger Publications.
Fischer, A. J., Clark, R., Askings, D., & Lehman, E. (2017). Technology and telehealth applications. In J. K. Luiselli (Ed.), Applied behavior analysis advanced guidebook: a manual for professional practice (pp. 135–163). San Diego: Academic Press.
Fischer, J.-F., Mainka, T., Worbe, Y., Pringsheim, T., Bhatia, K., & Ganos, C. (2020). Self-injurious behavior in movement disorders: systematic review. Journal of Neurology, Neurosurgery, and Psychiatry, 91, 712–719.
Hoch, T. A., Dzyak, C. R., & Burkhalter, B. L. (2016). Self-injury. In N. N. Singh (Ed.), Handbook of evidence-based practices in intellectual and developmental disabilities (pp. 635–676). New York: Springer.
Jacobson, N. S., & Truax, P. (1991). Clinical significance: a statistical approach to defining meaningful change in psychotherapy research. Journal of Consulting and Clinical Psychology, 59(1), 12–19.
Jacobson, N. S., Follette, W. C., & Revenstorf, D. (1984). Psychotherapy outcome research: methods for reporting variability and evaluating clinical significance. Behavior Therapy, 15(4), 336–352.
Kratochwill, T. R., Hitchcock, J., Horner, R. H., Levin, J. R., Odom, S. L., Rindskopf, D. M., & Shadish, W. R. (2010). Single-case designs technical documentation. What works clearinghouse. http://ies.ed.gov/ncee/wwc/pdf/wwc_scd.pdf.
Kratochwill, T. R., Levin, J. R., Horner, R. H., & Swoboda, C. M. (2014). Visual analysis of single-case intervention research: conceptual and methodological issues. In T. R. Kratochwill & J. R. Levin (Eds.), Single-case intervention research: methodological and statistical advances (pp. 91–125). Washington, DC: American Psychological Association.
Lance, E., York, J., Lee, L. C., & Zimmerman, A. W. (2014). Association between regression and self-injurious behaviors among children with ASD. Research in Developmental Disabilities, 35, 408–413.
LeBlanc, L. A., Lerman, D. C., & Normand, M. P. (2020). Behavior analytic contributions to public health and telehealth. Journal of Applied Behavior Analysis, 53(3), 1208–1218.
Lee, J. F., Schieltz, K. M., Suess, A. N., Wacker, D. P., Romani, P. W., Lindgren, S. D., Kopelman, T. G., & Padilla Dalmau, Y. C. (2015). Guidelines for developing telehealth services and troubleshooting problems with telehealth technology when coaching parents to conduct functional analyses and functional communication training in their homes. Behavior Analysis in Practice, 8, 190–200.
Lopata, C., Toomey, J. A., Fox, J. D., Thomeeer, M. L., Volker, M. A., & Lee, G. K. (2013). Prevalence and predictors of psychotropic use in children with high-functioning ASDs. Autism Research and Treatment, 276, 384527.
McCown, D., Reibel, D., & Micozzi, M. S. (2010). Teaching mindfulness: a practical guide for clinicians and educators. New York: Springer.
Myers, R. E., Karazsia, B. T., Kim, E., Jackman, M. M., McPherson, C. L., & Singh, N. N. (2018). A telehealth parent-mediated mindfulness-based health wellness intervention for adolescents and young adults with intellectual and developmental disabilities. Advances in Neurodevelopmental Disabilities, 2, 241–252.
Paclawskyj, T. R., Matson, J. L., Rush, K. S., Smalls, Y., & Vollmer, T. R. (2000). Questions about behavioral function (QABF): a behavioral checklist for functional assessment of aberrant behavior. Research in Developmental Disabilities, 21, 223–229.
Parker, R. I., Vannest, K. J., Davis, J. L., & Sauber, S. B. (2011). Combining non-overlap and trend for single-case research: Tau-U. Behavior Therapy, 42(2), 284–299.
Pellegrino, A. J., & DiGennaro Reed, F. D. (2020). Using telehealth to teach valued skills to adults with intellectual and developmental disabilities. Journal of Applied Behavior Analysis, 53(3), 1276–1289.
Singh, N. N., & Hwang, Y.-S. (2020). Mindfulness-based programs and practices for people with intellectual and developmental disability. Current Opinion in Psychiatry, 33(2), 88–91.
Singh, N. N., & Hwang, Y.-S. (2021). Mindfulness in intellectual and developmental disabilities. In N. N. Singh & S. D. S. Joy (Eds.), Mindfulness-based interventions with children and adolescents: Research and practice (pp. 96–118). London: Routledge.
Singh, N. N., & Singh Joy, S. D. (2021). Mindfulness-based interventions with children and adolescents: Research and practice. London: Routledge.
Singh, N. N., Ellis, C. R., Crews, W. D., & Singh, Y. N. (1994). Does diminished dopaminergic neurotransmission increase pica? Journal of Child and Adolescent Psychopharmacology, 4, 93–99.
Singh, N. N., Singh, J., Singh, A. D. A., Singh, A. N. A., & Winton, A. S. W. (2011). Meditation on the soles of the feet for anger management: a trainer’s manual. Raleigh: Fernleaf.
Singh, N. N., Chan, J., Karazsia, B. T., McPherson, C. L., & Jackman, M. M. (2017). Telehealth training of teachers to teach a mindfulness-based procedure for self-management of aggressive behavior to students with intellectual and developmental disabilities. International Journal of Developmental Disabilities, 63(4), 195–203.
Singh, N. N., Lancioni, G. E., Medvedev, O. N., Sreenivas, S., Myers, R. E., & Hwang, Y.-S. (2019). Meditation on the soles of the feet practice provides some control of aggression for individuals with Alzheimer’s disease. Mindfulness, 10(7), 1232–1242.
Soke, G. N., Rosenberg, S. A., Hamman, R. F., Fingerlin, T., Robinson, C., Carpenter, L., Lee, L.-C., Wiggins, L. D., Durkin, M. S., & DiGuiseppi, C. (2016). Prevalence of self-injurious behaviors among children with autism spectrum disorder: a population-based study. Journal of Autism and Developmental Disorders, 46, 3607–3614.
Tarnowski, K. J., & Simonian, S. J. (1992). Assessing treatment acceptance: the abbreviated acceptability rating profile. Journal of Behavior Therapy and Experimental Psychiatry, 23, 101–106.
Tomlinson, S. R. L., Gore, N., & McGill, N. G. (2018). Training individuals to implement applied behavior analytic procedures via telehealth: a systematic review of the literature. Journal of Behavioral Education, 27(2), 172–222.
VanDerwall, R., Rotta, K., Ehrhardt, K., & Poling, A. (2021). Using aripiprazole to benefit people with autism spectrum disorder: a critical appraisal. Advances in Neurodevelopmental Disorders. https://doi.org/10.1007/s41252-020-00190-7.
Wacker, D. P., Lee, J. F., Padilla Dalmau, V. C., Kopelman, T. G., Lindgren, S. D., Kuhle, J., Pelzel, K. E., & Waldron, D. B. (2013). Conducting functional analyses of problem behavior via telehealth. Journal of Applied Behavior Analysis, 46(1), 31–46.
Wacker, D. P., Schieltz, K. M., Suess, A. N., Romani, P. W., Padilla Dalmau, Y. C., Kopelman, T. G., Lee, J. F., & Lindgren, S. D. (2016). Telehealth. In N. N. Singh (Ed.), Handbook of evidence-based practices in intellectual and developmental disabilities (pp. 585–613). New York: Springer.
Woolf, S. H. (2008). The meaning of translational research and why it matters. JAMA, 299(2), 211–213.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Singh, N.N., Lancioni, G.E., Medvedev, O.N. et al. Real-Time Telehealth Treatment Team Consultation for Self-Injury by Individuals with Autism Spectrum Disorder. Adv Neurodev Disord 5, 170–182 (2021). https://doi.org/10.1007/s41252-021-00192-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41252-021-00192-z