
Abstract
The 8-item Youth Self-rated Insomnia Scale (YSIS) was developed to assess insomnia severity in the past month among youths. The YSIS has satisfactory psychometric properties in the general adolescent population. This study examined psychometric properties of the YSIS in a large sample of adolescent psychiatric patients. A total of 536 patients aged 10–19 years were consecutively recruited from the outpatient department of Shandong Mental Health Center between December 2021 and March 2022. Patients completed a structured questionnaire consisting of the YSIS scale and questions about sleep duration, nightmares, psychiatric history, depression, psychiatric and sleep medications, and demographics. Patients were diagnosed following the ICD-10 criteria. Of the participants, the mean age was 15.30 years (SD = 1.95), 61.0% were female, 60.9% were diagnosed with mood disorders, 65.7% were on antidepressants, and 49.0% were on anxiolytics or hypnotics. The mean YSIS score was 22.6 (SD = 8.07). Coefficient omega was 0.84. Exploratory factor analysis revealed one factor and two correlated residuals. The YSIS scores were significantly correlated with depression scores (r = 0.68) and significantly increased with sleep onset latency, short sleep duration, nightmare frequency, and sleep medication use. The YSIS demonstrated satisfactory internal consistency reliability, construct validity, and criteria-related validity in adolescent psychiatric patients. The YSIS appears to be a reliable and valid scale for measuring insomnia severity in adolescent psychiatric patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Insomnia is a common sleep disorder, defined as difficulty falling asleep, difficulty maintaining sleep, waking up too early, or nonrestorative sleep and daytime impairments related to these sleep symptoms [1]. Insomnia symptoms are common complaints of sleep problems in adolescents and have negative impacts on daytime functioning, quality of life, and mental and physical health [2,3,4]. The prevalence of insomnia symptoms in previous epidemiological studies in adolescents varies from 7 to 37% [5,6,7], depending on the criteria or measures used to assess one or more insomnia symptoms or insomnia disorder and the population studied [1, 8]. Despite its high prevalence and daytime impairment, insomnia in adolescents remains poorly described, underdiagnosed, and undertreated in the general clinical practice [8].
Insomnia symptoms are often measured by self-report or clinical interview in the routine clinical practice. Several self-reported measures have been developed to assess frequency and severity of insomnia symptoms in adults, such as Insomnia Severity Index (ISI), Pittsburgh Sleep Quality Index (PSQI), and Athens Insomnia Scale (AIS) [9, 10]. There are several questionnaires for evaluating sleep disturbances in pediatric population, such as Pediatric Sleep Questionnaire [11] and Children's Sleep Habits Questionnaire (CSHQ) [12].
According to both DSM-V [13] and ICSD-3 [14], Liu et al. developed the Youth Self-Rating Insomnia Scale (YSIS), an 8-item self-administered questionnaire to measure insomnia severity for adolescents during the past month [15]. The YSIS demonstrated satisfactory psychometric properties in a large community sample of Chinese adolescents (n = 11,626) [15]. Internal consistency reliability coefficient was 0.80 and 2-week test–retest reliability coefficient was 0.82. Both exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) yielded 2 factors defined as insomnia symptoms (3 items) and daytime distress or impairment (5 items). The YSIS scores were significantly correlated with short nocturnal sleep duration, depression, hypnotic use, sleep disordered breathing problems, restless legs syndrome, and daytime sleepiness.
The YSIS has been used in multiple studies and has shown satisfactory psychometric properties in the general adolescent and adult populations [16,17,18,19,20,21,22]. For example, in a study of 1794 adolescent students, Chi et al. reported that the YSIS had an internal consistency reliability coefficient of 0.91. CFA supported the construct validity of the YSIS scale, with good model-data fit (CFI = 0.974, TLI = 0.961, RMSEA = 0.077, SRMR = 0.030) [16]. In a study of 6710 college students, Tao et al. reported that the YSIS had an internal consistency reliability coefficient of 0.92. Network analysis demonstrated high correlations of insomnia symptoms assessed by YSIS with anxiety assessed by Generalized anxiety disorder scale (GAD-7) and depression assessed by Patient health questionnaire (PHQ-9) [20].
The reliability and validity of the YSIS in psychiatric patients are unknown. This study assessed psychometric properties of the YSIS in a large sample of adolescent psychiatric patients. Our first aim was to assess the factor structure of the YSIS via factor analysis. The second aim was to assess the internal consistency reliability of the YSIS. The third aim was to assess its concurrent validity by correlating YSIS scores to sleep onset latency, sleep duration, nightmares, daytime sleepiness, depression, and sleep medication use.
Methods
Participants and procedure
This study included 536 consecutive patients aged 10–19 years, who presented to the outpatient department of Shandong Mental Health Center (a public psychiatric hospital in Jinan, the capital and largest city of Shandong Province) between December 2021 and March 2022. Patients were diagnosed following the ICD-10 criteria. Patients with severe cognitive impairment or unable to read and complete the survey by themselves were excluded.
A research clinician administered a structured questionnaire to participants to collect data. Before filling out the questionnaires, all participants were told that participation in the study was voluntary, and their answers were confidential. We asked every participant and his/her parent or guardian if he/she would like to take part in the study. Oral informed consent was obtained from participants and their parents or guardians. Only patients who agreed to participate in this study were asked to complete the questionnaire. It took approximately 15 min to complete the questionnaire. The study was approved by the Ethics Committee of Shandong Mental Health Center.
Measures
A structured questionnaire was developed to collect data about demographics, psychiatric history, current psychiatric and sleep medications, depression, insomnia, daytime sleepiness, sleep duration, and nightmares. The following measures were included in the questionnaire.
Insomnia
The YSIS is an 8-item self-rated scale to measure insomnia severity in the past month [15]. Each item is rated on a 5-point scale ranging from 1 to 5. Example items are “During the past month, how often would you say you have had trouble falling asleep?” “During the past month, how would you rate the quality of your sleep overall?” The scale score was computed by summing the item scores, with a higher score indicating a greater insomnia severity. Based on a large sample of community adolescents (n = 11,626), Liu et al. recommended that the YSIS cutoff scores were 22–25 for mild insomnia, 26–29 for moderate insomnia, and ≥ 30 for severe insomnia [15]. The YSIS has demonstrated satisfactory psychometric properties and has been used in multiple studies of insomnia in adolescents [23,24,25].
Daytime sleepiness
The Chinese adolescent daytime sleepiness scale (CADSS) was used to assess daytime sleepiness [26]. The CADSS consists of seven questions that ask about individual’s general feeling of drowsiness and dozing off at different situations during the daytime in the past month. Example items are “During the past month, how often would you say you feel sleepy during the day?” “During the past month, how often would you say you have dozed off in the morning classes?” All 7 items are rated on a Likert scale from 1 = Never to 5 = Almost every day. Summing up the item scores yields a total CADSS score ranging from 7 to 35. A higher CADSS score indicates a greater daytime sleepiness. The CADSS has satisfactory psychometric properties and has been used in multiple studies of Chinese adolescents [27,28,29,30]. The coefficient alpha with the current sample was 0.90.
Depressive symptoms
The 20-item Center for Epidemiologic Studies Depression Scale (CES-D) [31] was used to measure depressive symptoms. Participants were asked to rate how often they experienced each symptom in the past seven days: 0 = “less than 1 day”, 1 = “1–2 days”, 2 = “3–4 days”, and 3 = “5–7 days”. The CES-D contains 20 items, of which four positive affect items are reversely coded. A total score was calculated by summing the item scores, with higher scores indicating higher severity of depressive symptoms. The coefficient alpha of the scale with the current sample was 0.93.
Sleep duration
Sleep duration on weekdays and weekends was measured by the question “During the past month, on an average weekday/weekend day, how many hours of actual sleep did you get at night?” Sleep onset latency was measured using the question “How many minutes did it usually take you to fall asleep after you go to bed at night in the past month?” Hypnotic use was measured using the question “How often did you take medicine to help sleep?” Nightmare frequency was measured using the question “In the past month, how often did you have nightmares (emotionally intense, frightening, and vivid dreams that awoken you from sleep)?”. [32]
Statistical analysis
Means and standard deviations for continuous variables or frequencies for categorical variables were reported. Inter-item and item-total correlations were computed. Confirmatory factor analysis (CFA) was performed to evaluate the 2-factor model (i.e., insomnia symptoms and daytime distress) found in the community adolescents [15]. Exploratory factor analysis (EFA) was performed following an inadequate fit of the CFA model. Coefficient omega was computed to assess internal consistency reliability based on the chosen factor model. Analysis of covariance (ANCOVA) was performed to compare mean YSIS scores across sleep variables (hypnotic use, sleep duration, sleep onset latency, and nightmare frequency), with age and sex as covariates. Correlations were computed between YSIS scores and sleep duration, sleep onset latency, daytime sleepiness, and depression. Factor analysis was conducted in Mplus 8.7 [33]. All other statistical analyses were conducted in IBM SPSS Version 28.0.
Results
Sample characteristics
All outpatients who completed the questionnaire were included in the analysis. Of the 536 outpatients, the mean age was 15.30 years (SD = 1.95, range = 10–19) and 327 (61.0%) were female. 60.9% were diagnosed with mood disorders. 65.7% were treated with antidepressants, 49% with anxiolytics or hypnotics. 16.4% were newly diagnosed patients, 31.2% had a history of 1- 3 years, and 6.2% had a history of more than 3 years. Approximately 40% of patients had been hospitalized at least once and 11% at least twice. The mean sleep duration was 7.32 hours (SD = 1.70) on weekdays and 8.43 hours (SD = 1.92) on weekends. The median sleep onset latency was 30 min. 28% fell asleep within 15 min, 25.5% at least 60 min. See Table 1 for details.
YSIS total score and item analysis
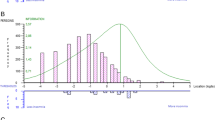
Figure 1 shows the distribution of the YSIS total scores in psychiatric outpatients. The YSIS total scores were not normally distributed (Kolmogorov–Smirnov = 0.063, p < 0.001; Shapiro–Wilk = 0.976, p < 0.001; skewness = 0.001, SE = 0.106; kurtosis = − 0.904, SE = 0.211). The YSIS total scores ranged from 8 to 40, the mean score was 22.80 (SD = 8.07), 25th, 50th, 75th, and 95th percentiles were 16, 23, 29, and 35, respectively.

The distribution of YSIS scores in adolescent patients. YSIS Youth Self-rating Insomnia Scale
Table 2 shows descriptive statistics of YSIS items. As shown in Table 2, more than half of the patients had unrefreshed sleep and more than 40% had difficulty falling asleep at least 3 times/week. Compared with other items, early morning awakening was less common (16% at least 3 times/week). The mean score for individual items ranged from 2.08 for early morning awakening to 3.46 for unrefreshing sleep.
Table 3 shows the polychoric correlations between YSIS items. All items were positively correlated with correlation coefficients ranging from 0.29 between item 5 and item 7 and 0.88 between item 1 and item 2. All items were also positively and moderately–highly corelated with the total score of all the 8 YSIS items (r = 0.65 for item 5 to 0.81 for item 1) and the total score without the item (r = 0.53 for item 5 to 0.74 for item 1).
Factor analysis and internal consistency reliability
CFA was performed to examine whether the factor structure of YSIS items in psychiatric patients was the same as that in the community adolescents (i.e., two factors with a correlated residual between item 1 and item 2) [15]. The model did not yield an adequate fit, χ2 = 179.25, df = 18, p < 0.01, RMSEA = 0.129, and CFI = 0.951. Importantly, the two factors were highly correlated (r = 0.88). We therefore proceeded with EFA. Both CFA and EFA were conducted in Mplus 8.7 based on polychoric correlations (as shown in Table 3) using unweighted least squares estimation method with both mean and variance adjustment (i.e., ULSMV).
The eight YSIS items yielded the largest eigenvalue of 4.674 and the second largest eigenvalue was 0.995, suggesting a dominant general factor. The one-factor EFA model was meaningful, however, the modification indices suggested adding two residual correlations, one was between item 1 and item 2 and the other was between item 4 and item 5. Adding the two residual correlations were meaningful because item 1 and item 2 reflect perceived sleep quality and satisfaction while item 4 and item 5 indicate maintaining sleep. Therefore, a one-factor EFA model with two residual correlations was conducted via the framework of exploratory structural equation modeling [34]. The model fitted the data reasonably well, χ2 = 87.76, df = 18, p < 0.01, RMSEA = 0.085, and CFI = 0.979. The factor accounted for 51% of total item variance. The factor loadings ranged from 0.52 for item 5 to 0.81 for item 6. Figure 2 shows the factor loadings and correlated residuals. Based on the one-factor model with two residual correlations, we computed coefficient omega [35]. The value was 0.84, indicating an adequate internal consistency reliability.

Standardized parameter estimates from factor analysis. Item 1 poor sleep quality; Item 2 sleep dissatisfaction; Item 3 Difficulty initiating sleep; Item 4 Difficulty maintaining sleep; Item 5 early morning awakening; Item 6 = Sleep insufficiency; Item 7 unrefreshing sleep; Item 8 daytime functioning impairment
Criterion-related validity
Table 4 shows the mean YSIS scores across sleep variables. Mean YSIS scores were significantly elevated in adolescents with reduced sleep duration on either weekdays or weekends, increased sleep onset latency, hypnotic use, and nightmare frequency. In addition, the YSIS scores were negatively correlated with night sleep duration on weekdays (r = − 0.364) and positively correlated with sleep onset latency (r = 0.372), daytime sleepiness scores (r = 0.576), and depression scores (r = 0.677) (all p < 0.001).
Discussion
The 8-item YSIS was developed to assess insomnia severity in the past month in adolescents. The YSIS has shown satisfactory reliability and validity in the community adolescents and has been used in multiple studies in adolescents, college students, and general population of adults [15, 18, 21]. However, the psychometric properties of the YSIS in psychiatric patients are unknown. The current study demonstrated that the YSIS had acceptable internal consistency reliability, construct validity, and criteria-related validity in a large sample of adolescent psychiatric patients (n = 536). The psychometric properties of the YSIS are summarized and discussed below.
The YSIS demonstrated satisfactory internal consistency reliability in psychiatric patients. In the current study, the coefficient omega was 0.84. All items were positively and moderately–highly correlated with each other and with the total scale score of other items. The internal consistency reliability in psychiatric patients is similar to those reported in an early study of community adolescents (omega coefficient = 0.80) [15] and recent studies of adolescents and adults (Cronbach’s alpha = 0.89–0.94) [16,17,18,19,20,21,22].
The YSIS was developed on the basis of the definitions of insomnia by ICSD-3 and DSM-V (i.e., a subjective report of insomnia symptoms and associated daytime consequences). In the community adolescents, the YSIS items measured two factors, one factor involving 3 insomnia symptoms and another factor consisting of 5 items related to insomnia distress or impairment in the community adolescents [15]. The 8 items had acceptable standardized loadings ranging from 0.50 to 0.90. The 2-factor structure has been supported by a recent study of adolescents [16]. In the current study of psychiatric patients, CFA did not support the 2 factors observed in the community adolescents [15, 16]. EFA yielded one factor, accounting for 51% of total item variance. The factor loadings of the 8 items were acceptable, ranging between 0.52 and 0.81. The findings suggest that the 8 YSIS items measure one single dimension of insomnia—insomnia severity in psychiatric adolescents.
In the community adolescents, the YSIS had shown good criterion validities as assessed by significant correlations with short sleep duration, daytime sleepiness, and anxiety/depression [15]. Significantly higher YSIS scores were also found in those adolescents who slept less, had sleep disordered breathing and restless legs syndrome, and used hypnotics than those who did not [15]. In the current study of psychiatric patients, the mean YSIS scores were significantly elevated in patients with reduced sleep duration on either weekdays or weekends, increased sleep onset latency, hypnotic use, and nightmare frequency. The YSIS score was negatively correlated with night sleep duration on weekdays and positively correlated with sleep latency, daytime sleepiness score, and depression score. All the concurrent associations between YSIS and short sleep duration, nightmare frequency, daytime sleepiness, and depression support the validity of YSIS for assessing insomnia severity in adolescent psychiatric patients.
The mean YSIS total score was 3.5 points higher in outpatients (22.60 ± 8.07) than in community adolescents (19.12 ± 6.20) [15]. Using cutoffs of the YSIS in community adolescents [15], more than half of psychiatric outpatients had mild-severe insomnia symptoms and 23% had severe insomnia. Higher mean YSIS score and prevalence of insomnia symptoms in psychiatric patients are expected and support the validity of the YSIS used to measure insomnia severity in psychiatric patients.
Although this is a large study to assess psychometric properties in psychiatric patients, the following limitations need to be considered when interpreting the findings. First, the study did not include insomniac patients. The psychometric properties of the YSIS for clinical use need to be assessed in clinical samples of adolescents with insomnia. Second, the measures used to validate the YSIS such as sleep duration, nightmares, depression, and daytime sleepiness were all self-reports. Objective assessments are needed to measure sleep duration, sleep quality, and daytime sleepiness in future studies. Third, although the sample size is large, all patients were recruited from one single mental health center, it is unknown if the findings could be generalized to adolescent patients from other mental health institutions. Further research is needed to include patients from other mental health institutions. In addition, physical conditions that may affect sleep, such as chronic pain, cough, and itching were not considered in this analysis.
Despite the study limitations, the YSIS demonstrated satisfactory internal consistency reliability, construct validity, and criteria-related validity in adolescent psychiatric patients. Although further research is needed, the findings from the current study suggest that the YSIS is a reliable and valid scale for measuring insomnia severity in adolescent psychiatric patients.
Abbreviations
- AIS:
-
Athens Insomnia Scale
- ANCOVA:
-
Analysis of covariance
- CADSS:
-
Chinese adolescent daytime sleepiness scale
- CFA:
-
Confirmatory factor analysis
- CSHQ:
-
Children’s Sleep Habits Questionnaire
- EFA:
-
Exploratory factor analysis
- GAD-7:
-
Generalized anxiety disorder scale
- ISI:
-
Insomnia Severity Index
- PHQ-9:
-
Patient health questionnaire
- PSQI:
-
Pittsburgh Sleep Quality Index
- YSIS:
-
Youth Self-rated Insomnia Scale
References
Roth T. Insomnia: definition, prevalence, etiology, and consequences. J Clin Sleep Med. 2007;3:S7-10.
Liu X, Buysse DJ. Sleep and youth suicidal behavior: a neglected field. Curr Opin Psychiatry. 2006;19:288–93. https://doi.org/10.1097/01.yco.0000218600.40593.18.
Owens J. Insufficient sleep in adolescents and young adults: an update on causes and consequences. Pediatrics. 2014;134:e921–32. https://doi.org/10.1542/peds.2014-1696.
Zhang J, Chan NY, Lam SP, Li SX, Liu Y, Chan JW, et al. Emergence of sex differences in insomnia symptoms in adolescents: a large-scale school-based study. Sleep. 2016;39:1563–70. https://doi.org/10.5665/sleep.6022.
Gradisar M, Gardner G, Dohnt H. Recent worldwide sleep patterns and problems during adolescence: a review and meta-analysis of age, region, and sleep. Sleep Med. 2011;12:110–8. https://doi.org/10.1016/j.sleep.2010.11.008.
Li SX, Chan NY, Man Yu MW, Lam SP, Zhang J, Yan Chan JW, et al. Eveningness chronotype, insomnia symptoms, and emotional and behavioural problems in adolescents. Sleep Med. 2018;47:93–9. https://doi.org/10.1016/j.sleep.2018.03.025.
Chung KF, Kan KK, Yeung WF. Assessing insomnia in adolescents: comparison of Insomnia Severity Index, Athens Insomnia Scale and Sleep Quality Index. Sleep Med. 2011;12:463–70. https://doi.org/10.1016/j.sleep.2010.09.019.
Yuksel D, Kiss O, Prouty DE, Baker FC, de Zambotti M. Clinical characterization of insomnia in adolescents—an integrated approach to psychopathology. Sleep Med. 2022;93:26–38. https://doi.org/10.1016/j.sleep.2022.03.010.
Buysse DJ, Ancoli-Israel S, Edinger JD, Lichstein KL, Morin CM. Recommendations for a standard research assessment of insomnia. Sleep. 2006;29:1155–73.
Moul DE, Hall M, Pilkonis PA, Buysse DJ. Self-report measures of insomnia in adults: rationales, choices, and needs. Sleep Med Rev. 2004;8:177–98. https://doi.org/10.1016/S1087-0792(03)00060-1.
Chervin RD, Hedger K, Dillon JE, Pituch KJ. Pediatric sleep questionnaire (PSQ): validity and reliability of scales for sleep-disordered breathing, snoring, sleepiness, and behavioral problems. Sleep Med. 2000;1:21–32.
Owens JA, Spirito A, McGuinn M. The Children’s Sleep Habits Questionnaire (CSHQ): psychometric properties of a survey instrument for school-aged children. Sleep. 2000;23:1043–51.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Arlington: American Psychiatric Publishing; 2013.
American Academy of Sleep Medicine. The international classification of sleep disorders (ICSD-3). Darien: AASM; 2014.
Liu XC, Yang YY, Liu ZZ, Luo YC, Fan F, Jia CX. Psychometric properties of Youth Self-Rating Insomnia Scale (YSIS) in Chinese adolescents. Sleep Biol Rhythms. 2019;17:339–48. https://doi.org/10.1007/s41105-019-00222-3.
Chi X, Liang K, Chen ST, Huang Q, Huang L, Yu Q, et al. Mental health problems among Chinese adolescents during the COVID-19: the importance of nutrition and physical activity. Int J Clin Health Psychol. 2021;21:100218. https://doi.org/10.1016/j.ijchp.2020.100218.
Lu C, Chi X, Liang K, Chen ST, Huang L, Guo T, et al. Moving more and sitting less as healthy lifestyle behaviors are protective factors for insomnia, depression, and anxiety among adolescents during the COVID-19 pandemic. Psychol Res Behav Manag. 2020;13:1223–33. https://doi.org/10.2147/PRBM.S284103.
Wang D, Chen H, Zhai S, Zhu Z, Huang S, Zhou X, et al. Is returning to school during the COVID-19 pandemic stressful? A study on immediate mental health status of Chinese college students. J Affect Disord. 2021;287:261–7. https://doi.org/10.1016/j.jad.2021.03.035.
Zhang J, Mi L, Zhao J, Chen H, Wang D, Ma Z, et al. The Moderating role of lifestyle on insomnia in home quarantine college students during the COVID-19 epidemic. Front Psychiatry. 2022;13:830383. https://doi.org/10.3389/fpsyt.2022.830383.
Tao Y, Hou W, Niu H, Ma Z, Zhang S, Zhang L, et al. Centrality and bridge symptoms of anxiety, depression, and sleep disturbance among college students during the COVID-19 pandemic—a network analysis. Curr Psychol. 2022. https://doi.org/10.1007/s12144-022-03443-x.
Geng F, Li S, Yang Y, Zou J, Tu L, Wang J. Trauma exposure and posttraumatic stress disorder in a large community sample of Chinese adults. J Affect Disord. 2021;291:368–74. https://doi.org/10.1016/j.jad.2021.05.050.
Zhang L, Tao Y, Hou W, Niu H, Ma Z, Zheng Z, et al. Seeking bridge symptoms of anxiety, depression, and sleep disturbance among the elderly during the lockdown of the COVID-19 pandemic—a network approach. Front Psychiatry. 2022;13:919251. https://doi.org/10.3389/fpsyt.2022.919251.
Zhang Y, Wang D, Zhao J, Chen XY, Chen H, Ma Z, et al. Insomnia and other sleep-related problems during the remission period of the COVID-19 pandemic: a large-scale survey among college students in China. Psychiatry Res. 2021;304:114153. https://doi.org/10.1016/j.psychres.2021.114153.
Zhang L, Yang Y, Luo Y, Liu ZZ, Jia CX, Liu X. A longitudinal study of insomnia, daytime sleepiness, and academic performance in Chinese adolescents. Behav Sleep Med. 2022;20:798–808.
Huang L, Liang K, Jiang W, Huang Q, Gong N, Chi X. Prevalence and correlates of mental health problems among Chinese adolescents with frequent peer victimization experiences. Children (Basel). 2021;8:403. https://doi.org/10.3390/children8050403.
Liu XC, Yan YY, Liu ZZ, Che H, Fan F, Jia CX. Psychometric assessment of the Chinese adolescent daytime sleepiness scale (CADSS). Sleep Biol Rhythms. 2017;15:9.
Liu XC, Yang YY, Liu ZZ, Chen H, Fan F, Jia CX. Psychometric assessment of the Chinese adolescent daytime sleepiness scale (CADSS). Sleep Biol Rhythms. 2017;15:207–16.
Wang ZY, Liu ZZ, Jia CX, Liu X. Age at menarche, menstrual problems, and daytime sleepiness in Chinese adolescent girls. Sleep. 2019. https://doi.org/10.1093/sleep/zsz061.
Liu X, Liu ZZ, Wang ZY, Yang Y, Liu BP, Jia CX. Daytime sleepiness predicts future suicidal behavior: a longitudinal study of adolescents. Sleep. 2019. https://doi.org/10.1093/sleep/zsy225.
Hu T, Wang Y, Lin L, Tang W. The mediating role of daytime sleepiness between problematic smartphone use and post-traumatic symptoms in COVID-19 home-refined adolescents. Child Youth Serv Rev. 2021;126:106012. https://doi.org/10.1016/j.childyouth.2021.106012.
Radloff LS. The CES-D scale: a self report depression scale for research in the general population. Appl Psychol Meas. 1977;1:385–401.
Liu X, Liu ZZ, Liu BP, Jia CX. Nightmare frequency and psychopathological problems in a large sample of Chinese adolescents. Soc Psychiatry Psychiatr Epidemiol. 2022;57:805–16. https://doi.org/10.1007/s00127-022-02224-y.
Muthén LK, Muthén BO. Mplus user’s guide (version 8th). Muthén & Muthén, Los Angeles; 1998–2022.
Asparouhov T, Muthén B. Exploratory structural equation modeling. struct Equ Model. 2009;16:397–438.
Green SB, Yang Y. Reliability of summed item scores using structural equation modeling: an alternative to coefficient alpha. Psychometrika. 2009;74:155–67.
Acknowledgements
The authors would like to thank all adolescent psychiatric patients and their parents for their voluntarily participating in this study.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Conceived and designed the study: LH, XCL, YY. Data collection: ZW, LH. Analyzed the data: XCL, LH, YY. Wrote the paper: LH, XCL, YY. Revision and final decision: LH, XCL, YY, ZW.
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Ethical approval
This study was approved by the ethics committee of the Shandong Mental Health Center in China.
Informed consent
Informed consent was obtained from all individual participants and their parents included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Hu, L., Wang, Z., Yang, Y. et al. Psychometric properties of the Youth Self-rated Insomnia Scale (YSIS) in adolescent psychiatric patients. Sleep Biol. Rhythms 22, 103–111 (2024). https://doi.org/10.1007/s41105-023-00487-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41105-023-00487-9