
Abstract
Child undernutrition is a global health problem, with one in every four children being stunted. Children who are stunted, wasted, or underweight are more likely to have long-term health effects, including infant and under-five mortality, than those who are not. Although prior studies examined the determinants and the effects of stunting, less is known about the spatial inequality of child undernutrition in developing countries. Using the nationally representative data from the 2010/2011 and 2015 Demographic Health Survey, the paper estimated the spatial inequality and determinants of undernutrition among under-five children in Zimbabwe. The analysis carried out using thematic maps and Pooled OLS analysis. Found that spatial inequality and spatial autocorrelation in stunting, wasting, and underweight exist in Zimbabwe; hotspots and coldspots in undernutrition were present in 2010 and 2015. Aridity, number of wet days, skilled worker availability, precipitation, perception of distance to the health facility, and women’s education in the cluster were associated with child undernutrition. Therefore, policies to reduce inequality and child undernutrition should be need-based, that is, the clusters and districts with high child undernutrition should be prioritised. Policymakers should consider factors contributing to child nutrition to ensure that children have healthy adult lives and well-being through a healthy early life, enabling proper physical and cognitive development.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
Child undernutrition is a global health challenge that burdens developing countries highly (Bloss et al., 2004; Khor, 2003; Martorell & Young, 2012). According to Bredenkamp et al. (2014) and Govender et al. (2021), child undernutrition is a major contributor to infant and child mortality in most developing countries. Undernutrition is associated with 45% of under-five mortality globally (WHO, 2022), increased healthcare costs, reduced productivity, and reduced living standards (Bredenkamp et al., 2014). Literature shows that child undernutrition deters children from attaining their full potential in terms of physical and cognitive development (Ahmed et al., 2021; Ali et al., 2022; Tamir et al., 2022; Usman & Kopczewska, 2022). This is associated with worsened educational attainment, compromised adulthood health outcomes and increasing poverty (Bredenkamp et al., 2014; Govender et al., 2021). Undernutrition has long-lasting economic and developmental effects on households, societies and countries.
Child undernutrition is measured using stunting, wasting and underweight of children under the age of five (Govender et al., 2021; Mgongo et al., 2017; Ntenda & Chuang, 2018; Wolde et al., 2015). According to WHO (2022), almost a quarter of children under five were stunted, whilst approximately a tenth of the children were wasted in 2022. Undernutrition is associated with low socioeconomic status, poor maternal health and nutrition, and inappropriate intake of nutrients in the early years (Mgongo et al., 2017; Tette et al., 2015; Vitolo et al., 2008) as well as mother’s education, child’s gender and age, marital status, food security, birth weight and geographic location (Amir-ud-Din et al., 2021; Sartorius et al., 2020; Seferidi et al., 2022). Regionally, child nutrition is associated with food security, perception of distance to the health facility, geographical location, women’s education and climate factors (Govender et al., 2021; Ntenda & Chuang, 2018; Tamir et al., 2022).
Despite the efforts to reduce child undernutrition, Zimbabwe faces a high prevalence of child undernutrition when the country grapples with economic and political challenges (Sisimayi et al., 2021). For instance, 27% of under-five children were short for their age, 3% were thin for their height, and 8% were thin for their age in 2015 (ZIMSTAT & ICF International, 2016a, 2016b). Over the years, child undernutrition has been prevalent in Zimbabwe, affecting people and regions differently, particularly in rural and poor populations (Lukwa et al., 2020; Sisimayi et al., 2021).
Existing literature investigated the individual-level factors affecting child nutrition (Bloss et al., 2004; Bredenkamp et al., 2014; Chowdhury et al., 2020; Frongillo et al., 1997; Girma et al., 2019; Seferidi et al., 2022; Tette et al., 2015; Wolde et al., 2015; Yayo Negasi, 2021). Although previous studies established the factors affecting child nutrition, less is known about the regional-level determinants of and spatial inequality in undernutrition (Amir-ud-Din et al., 2021; Jouzi et al., 2023; Sartorius et al., 2020). Specifically for Zimbabwe, most studies focused on socioeconomic inequalities and individual effects of stunting (Lukwa et al., 2020; Marume et al., 2022; Matema, 2021). A few studies have explored health outcomes and service availability through spatial analysis in Zimbabwe. For example, Chazireni (2015) examines spatial inequalities and temporospatial variations in health conditions and reports that health conditions are poor and the health system is characterised by severe spatial inequalities. Musuka et al. (2021) focus on the association between diarrhoea episodes and seeking treatment, and find that several factors, such as wealth quintiles, are associated with seeking treatment. Given the limited literature on spatial inequality in undernutrition in Zimbabwe, this study builds upon this existing evidence by focusing on spatial inequality and the cluster-level factors determining child undernutrition in Zimbabwe, a critical area to detect regions excessively affected by undernutrition. This allows for targeted interventions to address inequalities in child health and well-being.
Understanding the spatial information on child undernutrition will enhance policy-making and resource allocation to those who need it most. This analysis reveals unprecedented and significant district heterogeneity in child undernutrition in Zimbabwe, which is vital for ensuring the effective and efficient use of scarce resources by directing them to the districts in need. Addressing these spatial differences is crucial in eliminating differences in education and labour market outcomes—and, ultimately, poverty and inequality in adulthood. The analysis is critical as Zimbabwe still grapples with a high prevalence of child undernutrition when inequality is at the centre of Vision 2030.
2 Methods
2.1 Data Sources
The study used data from the Zimbabwe Demographic Health Survey (DHS). The DHS is collected every five years in Zimbabwe, and six DHS have been collected so far from 1988 up to 2015. The dataset was collected from all the country’s provinces to represent the overall population. The DHS was collected using the two-stage sampling technique, where the enumeration areas were selected first, and households were allocated into their respective enumeration areas. The data was collected from both rural and urban areas. The survey gathers information on fertility, child and maternal mortality, child and maternal health outcomes, breastfeeding, anaemia and household characteristics. The children’s questionnaire was used to determine spatial inequality in child undernutrition since it comprises information on stunting, wasting and underweight.
Moreover, the paper used the 2010/2011 (ZIMSTAT & ICF International, 2011) and 2015 (ZIMSTAT & ICF International, 2016b) DHS, given that they are the most recent DHS surveys with the relevant child undernutrition information at the time of the study. A total of 406 enumeration areas were included in the 2010/11 DHS data, 169 in the urban areas and 237 in the rural areas with 10 828 households. In 2015, 400 enumeration areas were selected for analysis (166 from urban areas and 234 from rural areas) with 11 196 households. More information on the data collection process and its contents can be found in the 2010/2011 and 2015 Zimbabwe DHS reports (ZIMSTAT & ICF International, 2012, 2016a).
The analysis was based on the enumeration level or cluster-level variables, including 400 clusters in 2015 and 406 clusters in 2010/11. However, some of the variables had missing information, reducing the total number of observations in the analysis. Thus, the analysis was possible for a total of 792 clusters (for both 2010/11 and 2015) instead of 806, which was initially sampled with over four thousand observations after missing observations were excluded from the analysis.
Data on climate factors affecting child undernutrition in Zimbabwe were extracted from the 2010/2011 and 2015 DHS geospatial covariate datasets. This data is extracted from raster files (images and modelled surfaces) to generate values. The vector files (polygons and points) show the clusters’ location and boundary (Mayala et al., 2018). The geospatial covariate dataset includes variables like rainfall, temperature, aridity and length of the growing season, to mention a few. According to Mayala et al. (2018), cluster geographical position coordinates used to extract the data were displaced to protect the individual’s anonymity, up to 2 km for urban and 10 km for rural clusters. In that regard, the displacement was done carefully to ensure that clusters would not overlap with the other administrative areas. Comprehensive information on data extraction can be found in the DHS program geospatial covariates dataset manual (Mayala et al., 2018).
DHS data only report information at the first administrative unit (province or region), not the second administrative unit (districts). The paper extracted the Zimbabwe subnational administrative boundaries at the second administrative unit from Human Data Exchange (2018) to identify districts from the DHS data. The geomasked cluster information from the DHS was then compared with the district data from the subnational administrative boundaries information as indicated by Wilson et al. (2020). The district data from the subnational administrative boundaries tallying with the cluster DHS data were used for the analysis. This method was proven effective in identifying the second administrative unit where the information is not provided in the DHS by Wilson et al. (2020) in their Malawi paper.
2.2 Conceptual Framework
Figure 1 shows the conceptual framework for the determinants of malnutrition. This framework acknowledges the significant role of diets and care in determining child nutrition due to an increased undernutrition burden. This framework shows different levels of undernutrition determinants, denoted as immediate (diets and care), underlying (household food security, maternal and child care and healthy environment) and enabling determinants (human, economic and financial resources). Resource availability influences the underlying determinants, which are associated with dietary intake and care received, hence determining the nutrition status of children.

Nutrition conceptual framework (adapted from (UNICEF, 2021))
Child undernutrition is measured using stunting, wasting and underweight among children under the age of five years (Govender et al., 2021; Mgongo et al., 2017; Ntenda & Chuang, 2018; Wolde et al., 2015). According to Govender et al. (2021), stunting indicates persisting failure to receive enough nutrients in children under five. This chronic condition has further implications for cognitive development and adult health outcomes. Stunted children have height-for-age z-scores less than negative two (− 2) standard deviations, while wasted children have weight-for-height z-scores below negative two (− 2) standard deviations. Wasting involves the failure to have enough nutrition for children under five, resulting in recurrent sickness and weight loss (Mgongo et al., 2017; Ntenda & Chuang, 2018). Underweight is defined as children’s weight-for-age z-scores below negative two (− 2) standard deviations. The underweight variable incorporates height-for-age and weight-for-height. Stunting, wasting, and underweight are the dependent variables in the analysis. These variables were measured as the proportions of children stunted, wasted or underweight within a cluster. The underlying, immediate and enabling determinants of undernutrition are discussed below.
Enabling factors of undernutrition include human, economic and financial resources, which are important in ensuring nutrition among children. Human resources are measured by the level of education in a specific area, that is, the knowledge and experience important in ensuring that children receive nutritional food and safe water (UNICEF, 2021). Educated women know the importance of child nutrition in reducing long-term development effects, and they will use their resources to reduce undernutrition among children. Women are primarily responsible for children’s well-being, and women’s capability to make intra-household resource allocation choices plays a vital role in averting child undernutrition (Pillai & Maleku, 2019). Since women’s capacity to make nutrition-related decisions is positively associated with their educational level, improving women’s education is significant in preventing child undernutrition (Ncube-Murakwani et al., 2020; Pillai & Maleku, 2019). Women’s education was measured as the proportion of women with secondary education and above in a cluster. Thus, the education variable indicated the proportion of educated women in the analysis. These cluster-level factors were constructed by aggregating the individual and household information at the cluster level.
Geographical location, perception of distance to the health facility, skilled health worker availability, and climate factors were used as independent variables to estimate the determinants of stunting, wasting and underweight in Zimbabwe (Govender et al., 2021; Ntenda & Chuang, 2018; Tamir et al., 2022). According to Pillai and Maleku (2019), geographical location is crucial in determining child nutrition. Mothers residing in urban areas are less likely to have stunted children than mothers residing in rural areas, owing to the availability and accessibility of prenatal and postnatal care and information on child nutrition. Most rural areas have weak access to healthcare services and environmental risks that compromise child nutrition (Govender et al., 2021; Pillai & Maleku, 2019). Geographical location is a proxy for environmental risks, health, water, and sanitation availability, as well as shared values (Govender et al., 2021). Given that the analysis was done at the cluster level, not at the household or individual level, the occupational and economic variables are a subset of development in a specific cluster, which is indicated by its rurality or urbanicity. Rural areas are primarily associated with high poverty and self-employment compared to urban areas. These variables are, therefore, captured under the rural–urban differences. Geographical location was measured as urban or rural areas, represented by one for rural areas and zero for urban areas.
World Health Organisation (WHO) recommends a minimum acceptable diet for children aged five and below to ensure cognitive development and healthy life during adulthood. The dietary requirement comprises different food types that offer a balanced diet to children, including legumes, dairy products, vegetables, animal products, roots, and tubers (WHO, 2023). The different food types provide a high-quality diet for both breastfed and non-breastfed children (WHO, 2023). High-quality nutrition is vital for better infant and maternal health outcomes (Marume et al., 2022). Children receiving nutritious food learn better, are more productive, and have better opportunities, improving living standards and eradicating the vicious cycle of poverty in society. These children are more likely to have undernutrition if they don’t receive the minimum acceptable diet (Sisimayi et al., 2021).
Another determinant of child nutrition is good care, which is driven by adequate services to support good nutrition for children and women (UNICEF, 2021). Good care is proxied by skilled health worker availability measured by the proportion of women who delivered at the health facility and were assisted by a health professional. According to Ntenda and Chuang (2018), undernutrition children are more likely to reside in areas with poor socioeconomic conditions and weak access to essential primary healthcare services. The perception of distance to the health facility is another determinant, defined as the proportion of women who deem distance to be a challenge when ill or sick (Ntenda & Chuang, 2018). Therefore, the perception of distance to the facility represents the individuals’ perception of distance to the health facilities, not the actual distance.
As an underlying determinant, food security is vital in ensuring improved child nutrition (Ntenda & Chuang, 2018; Shrimpton, 2020). Food security is critical in ensuring children under-five receive age-appropriate and nutrient-rich foods (UNICEF, 2021). Climate factors of child nutrition were included in the analysis, based on their effects on crop production and food security, which contribute to child undernutrition (Ahmed et al., 2021). These climate factors include aridity, daytime land surface temperature, the annual number of wet days and precipitation (Ahmed et al., 2021). Climate factors are useful for monitoring and managing drought, floods, and food security early warnings (Mayala et al., 2018). These variables were transformed using logarithms to ensure a better distribution of variables.
2.3 Estimation Technique
2.3.1 Thematic Maps
Spatial information is collected from multiple sources, and decision-makers use the consolidated spatial information to take action based on the needs. The spatial analysis enables clustering of data on undernutrition, which helps authorities understand demographic commonalities by focusing on the density of projected data points. In addition, data is presented on maps by using layers, such as heat maps or bubble charts, to facilitate visual mapping. Thematic maps were used to determine the spatial inequality in undernutrition among children in Zimbabwe. This allowed the identification of the areas prone to undernutrition in Zimbabwe. Thus unmasking the regional disparities in Zimbabwe as far as stunting, wasting and underweight are concerned.
The paper also used the Getis-ORD statistics to determine the local spatial autocorrelation in undernutrition in Zimbabwe. According to Amir-ud-Din et al. (2021) and Tobler (1979), areas close to each other are more likely to be similar than areas far from each other. A positive and significant statistic indicates hot spot-areas with high prevalence in undernutrition, whilst a negative and significant statistic shows the cold spot—areas with low prevalence in undernutrition. Hot spots are areas with high spatial clustering values, that is, areas with high undernutrition are close to areas with high undernutrition (Amir-ud-Din et al., 2021). Cold spots exist in areas with less prevalence of child undernutrition and are surrounded by areas with less prevalence of undernutrition (Amir-ud-Din et al., 2021). Areas with insignificant spatial autocorrelation statistics are considered not to be spatially clustered.
The Getis-ORD statistic is specified as follows:
where \({x}_{j}\) is the attribute value for feature j, \({w}_{i,j}\) is the spatial weight between i and j and n is the total number of features. \(\overline{X} = \frac{{\mathop \sum \nolimits_{j = 1}^{n} x_{j} }}{n} \;{\text{and}}\;S = \sqrt {\frac{{\mathop \sum \nolimits_{j = 1}^{n} x_{j}^{2} }}{n} - \left( {\overline{X}} \right)^{2} }\).
The likelihood ratio test was used to determine the appropriate model between non-spatial and spatial models. The null hypothesis was accepted, as non-spatial models were appropriate for the analysis.
2.3.2 Pooled OLS Model
Existing literature on factors affecting child undernutrition used logistic regression Bloss et al. (2004), Chowdhury et al. (2020), Ntenda and Chuang (2018), Nyarko et al. (2022) and Tamir et al. (2022). Jouzi et al. (2023) used geographically weighted regression, whilst Usman and Kopczewska (2022) used an OLS and spatial Durbin error model. However, although various quantitative methods for analysis, this paper used pooled OLS as the cluster analysis was based on two surveys. Pooled OLS is also appropriate for pooled cross-sectional data.
Pooled cross-sectional data are obtained by sampling data from a large population (Wooldridge, 2015). Pooled cross-sectional data are mainly used to evaluate policies and inform decision-making. Unlike cross-sectional data, pooled data are also widely used, as such data increase the sample size, thus providing accurate mean estimates (Wooldridge, 2015). According to Wooldridge (2015), using randomly selected observations increases the chances of getting more precise estimators and testing statistics with more power. The pooled dataset is useful in examining a stable relationship between dependent and independent variables over time.
The individual cross-sectional observations are considered linearly independent when dealing with a pooled OLS model (Wooldridge, 2010). Pooled OLS has similar assumptions to the standard OLS method; it assumes that the error term is not correlated with the explanatory variables, \(E\left({x}_{it}{\prime}{\varepsilon }_{it}\right)=0\) and error terms are not correlated with each other. The assumptions enhance the effectiveness of the model and violating them results in biased estimates. In the presence of omitted variables and when an independent variable is correlated with the error term, the estimates from pooled OLS models are biased and inconsistent (Wooldridge, 2015).
The Pooled OLS model was identified as follows:
where child undernutrition was the dependent variable (stunting, wasting and underweight), \(x\) was the matrix of other independent variables (skilled delivery availability, perception of distance to health facility, women’s education, geographical location and precipitation, number of wet days, daily land surface temperature and aridity), i was the district and t was the time. \({\mu }_{i}\) was the regional-fixed effects, and \({\delta }_{t}\) represented the time-fixed effects.
The coefficients show the extent and direction in which independent variables determine child undernutrition in Zimbabwe.
3 Results
Table 1 shows the descriptive statistics for the variables used in the analysis. The number of wet days was relatively high in 2010 compared to 2015. In addition, on average, it precipitated more in 2010 than in 2015. On average, 2015 was arider than 2010, as indicated by 2.128 and 2.270, respectively. Day land surface temperature was higher in 2015 than in 2010; the land surface was cool during the day in 2010. More urban areas were included in the survey in 2010 than urban areas in the 2015 survey. The mean availability of skilled workers was higher in 2010 than in 2015. The average skilled health worker availability was more than fifty percent for both years. Around two-fifths of the respondents deemed the distance to the health facility a big challenge, and no significant difference existed between 2010 and 2015. On average, women in different districts are highly educated, as indicated in Table 1. Over three-fifths of the women in 2010 and 2015 had secondary and tertiary education in Zimbabwe. Child undernutrition was prevalent in Zimbabwe in terms of stunting, wasting and underweight. Approximately a quarter of the children under five were stunted in 2010 and 2015, with more children stunted in 2010 (0.227) than in 2015 (0.202). On average, wasting was more prevalent in 2015 (0.038) compared to 2010 (0.032). Around ten percent of the children in the survey were underweight, with more children underweight in 2010 (0.100) than in 2015 (0.078).
3.1 Spatial Inequality in Child Undernutrition
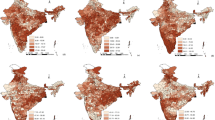
Child undernutrition varied across regions over time in Zimbabwe. Figures 2, 3, and 4 illustrate the regional disparities in stunting, wasting, and underweight.

Prevalence of stunting in Zimbabwe

Prevalence of wasting

Prevalence of underweight
Figure 2 shows the prevalence of stunting in 2010 and 2015. Stunting was more prevalent in the north-east, south-west and some western parts of the country in 2010. As indicated by the figure, these areas had more stunted children than other districts. A total of eight districts had high stunting in 2010, which are Mudzi, Lupane, Gokwe South, Gokwe Town, Mangwe, Shurugwi Town, Shurugwi rural and Marondera. Children in the central and some districts in the southern and northern parts of the country had low levels of stunting. Chiredzi, Kariba, Muzarabani, Chirumhanzu and Chikomba had the lowest stunting levels. The same thing happened in 2015; stunting varied across districts. Districts in the northern, north-west, western and some districts of the eastern parts of the country had a high prevalence of stunting. Nine districts with high stunting levels include Mangwe, Gwanda urban, Gwanda rural, Insiza, Chipinge rural, Chipinge urban, Shamva, Bindura urban and Bindura rural in 2015. Marondera rural. Marondera urban, Chikomba, Harare, Bulawayo and Umguza had less stunting prevalence in 2015. Different districts faced high stunting levels over time except for Mangwe district, which had high stunting levels in both 2010 and 2015. Chikomba had the least stunted children in 2010 and 2015.
The prevalence of wasting is illustrated in Fig. 3. This showed wasting inequalities in Zimbabwe; some districts were more affected by wasting than others. In 2010, districts in the southern, western, north-west and northeast parts of the country were mostly affected by child wasting. These include Bulilima, Bubi, Nkayi, Insiza, Chirumhanzu, Chiredzi urban, Chiredzi rural and Mutoko. Relatively a large proportion of districts are in the central, eastern, and some districts of the northern part of the country had less wasting prevalence. Furthermore, districts in the central, eastern, southeast and northeast parts had the least prevalence of child wasting in 2015. Child wasting was prevalent in the northern, north-west, western and southern parts of Zimbabwe. Areas with rampant wasting levels include Mutoko, Bulilima, Umguza, Nkayi, Matobo, Gutu and Lupane. In that regard, Bulilima, Nkayi, and Mutoko districts faced a high prevalence of wasting in 2010 and 2015.
Figure 4 illustrates underweight prevalence in Zimbabwe. The figure showed that spatial inequality in underweight exists, that is, different districts were facing different levels of child underweight. In 2010, child underweight was more prevalent in the country’s western, north-west and central parts. These districts include Bulilima, Gokwe South, Gokwe Town, Bubi, Kwekwe rural, Kwekwe urban, Redcliff, Chirumhanzu and Nyanga. Districts like Chimanimani, Chiredzi urban, Chiredzi rural, Bikita, Gutu and Insiza had low underweight prevalence in 2010. Similarly, spatial disparities were also present in 2015. Districts in the northern, north-east, north-west and western parts had more underweight children than other districts. These districts were Nyanga, Mutasa, Bulilima, Plumtree, Insiza, Chirumhanzu, Zvimba, Nkayi, Bindura urban and Bindura rural. Furthermore, Chiredzi urban, Chiredzi rural, Masvingo urban, Masvingo rural, Gutu, Chegutu urban, Chegutu rural, Kariba urban and Kariba rural had a lower prevalence of underweight in 2015. In that regard, Nyanga, Bulilima, and Chirumhanzu had high underweight prevalence in 2010 and 2015, while Chiredzi urban, Chiredzi rural, and Gutu had the lowest underweight prevalence in 2010 and 2015.
Table 2 shows the hot spots and the cold spots that existed in 2010 and 2015 concerning stunting, wasting and underweight. Z-scores with values of at least 1.96 represent hot spots, while z-scores less than or equal to 1.96 show cold spots in child undernutrition. Five stunting hot spots were identified in 2010, and three hot spots in 2015. The stunting hot spot districts in 2010 were Marondera rural, Marondera urban, Lupane, Mangwe and Matobo, whilst Bindura rural, Bindura urban and Chirumhanzu were hotspots in 2015. Moreover, Gweru urban and Bubi were the cold spot districts in 2015 and 2010, respectively. Concerning wasting, Beitbridge rural, Beitbridge urban, Nkayi and Bubi districts were deemed hot spots in 2010, whilst Nkayi was the only hot spot in 2015. Nkayi remained the wasting hot spot district over the years. Shurugwi and Gweru districts were wasting cold spots in 2010, and there were no cold spot districts in 2015 for wasting. Focusing on child underweight, Chirumhanzu was the only hot spot district in 2015, with no hot spot in 2010. Chimanimani and Chipinge urban were the underweight cold spot districts in 2010, and no cold spot districts in 2015. Chirumhanzu, therefore, was the hot spot for both stunting and underweight in 2015.
Table 3 illustrates the Pooled OLS model results for three different equations: stunting, wasting and underweight. As indicated in Table 3, aridity significantly increased child stunting, whilst skilled health workers’ availability, women’s education, and precipitation significantly reduced child stunting. Distance, daily land surface temperature, number of wet days, and location were insignificantly affecting child stunting. Surprisingly, only skilled worker availability significantly increased child wasting. Precipitation, skilled health worker availability and women’s education were negative and significantly determined child underweight, whereas aridity was positive and significantly contributed to child underweight. Moreover, perception of distance to the facility, number of wet days, location and daily land surface temperature were insignificant in determining the child’s weight.
Understanding the macroeconomic and political implications of child undernutrition is of utmost importance in Zimbabwe, particularly as the data was collected during a macroeconomic and political instability period. From 2009 to 2013, the country was under a government of national unity (GNU), a period characterised by relative stability compared to the periods before and after. Including a GNU variable in the analysis, representing whether the child was born in 2009–2013 or not, was a robustness check. These results, presented in Table 4 in the Appendix, were consistent with those in Table 3. However, as indicated in Table 4, the GNU variable was insignificantly associated with child undernutrition (stunting, wasting, and underweight).
4 Discussion
Child undernutrition is a critical concern, as it directly impacts the health and well-being of every child. Ensuring optimal nutrient intake in the early years is a key strategy for long-term health benefits. This research delves into the spatial distribution of stunting, wasting, and underweight in Zimbabwe, aiming to shed light on the inequality and the contributing factors.
The paper found that spatial inequality in child undernutrition exists in Zimbabwe. These results are consistent with findings from prior literature (Ahmed et al., 2021; Ali et al., 2022; Amir-ud-Din et al., 2021; Haile et al., 2016; Ntenda & Chuang, 2018; Sartorius et al., 2020; Usman & Kopczewska, 2022). Districts in the western and northeast parts of the country had a higher prevalence of child undernutrition than other districts on average. For instance, twelve districts in the north-east, south-west and western parts of the country had a high prevalence of child stunting in 2010 and 2015. Districts in the north-east, southern and western had more wasted children: Bulilima, Bubi, Nkayi, Insiza, Chirumhanzu, Chiredzi, Mutoko, Matobo, Gutu and Lupane. Nyanga, Mutasa, Bulilima, Plumtree, Insiza, Chirumhanzu, Zvimba, Nkayi and Bindura had a high underweight prevalence. The areas in the western parts of the country consume less protein and iron-rich food regardless of being one of the livestock-rearing areas and having dietary diversity, contributing to undernutrition, hence contributing to spatial inequality in the country (Food & Nutrition Council of Zimbabwe, 2018). Moreover, these areas have more women who are less educated than other areas, which is associated with high prevalence of undernutrition (Food & Nutrition Council of Zimbabwe, 2018). Spatial differences in child undernutrition might led to differences in education and labour market outcomes—and, ultimately, poverty and inequality. Understanding these spatial differences in child stunting is crucial not only for policy-making and public health intervention (Ahmed et al., 2021) but also has significant practical implications by improving nutrition education and healthcare access. This analysis revealed unprecedented and significant district heterogeneity in child undernutrition in Zimbabwe, which is vital for ensuring the effective and efficient use of scarce resources by directing them to the districts in need. Moreover, the results highlighted the trends in child undernutrition in different districts and significant factors that can be addressed to tackle the problem. In addition to that, the paper also contributes to the existing literature by providing more insights into spatial inequality in child undernutrition in developing countries.
Hot spots in child undernutrition also exist in Zimbabwe, which is in line with prior literature (Ali et al., 2022; Amir-ud-Din et al., 2021; Haile et al., 2016; Tamir et al., 2022). This was in line with Jouzi et al. (2023) paper, which indicated stunting hotspots in the north-east part of Zimbabwe. The districts with a high prevalence of child undernutrition tend to receive less rainfall and are more likely to face drought. These are generally known as lowland areas associated with erratic and unreliable rainfall. This, therefore, has a negative implication on agricultural production and food security that tends to affect child undernutrition.
Aridity and precipitation affect child undernutrition in Zimbabwe. Aridity increases child undernutrition, whilst precipitation decreases child undernutrition. Children residing in more arid clusters are more stunted than those in less arid clusters. An increase in aridity increases stunting and underweight by 0.283 and 0.261, respectively, while an increase in precipitation and the number of wet days tend to reduce child underweight by 0.306 and 0.227, respectively. This is in line with Usman and Kopczewska (2022) paper, which found that climate variability is associated with child stunting in Pakistan and Ahmed et al. (2021) in Ethiopia. Climate fluctuations are associated with low precipitation, high temperatures and more arid areas, further affecting crop production and food security (Ahmed et al., 2021). Agriculture is the backbone of Zimbabwe, the economy and many individuals rely on agricultural outputs (Jouzi et al., 2023; Lukwa et al., 2020). Given that most of the farmers depend on rain-fed agriculture, climate variability affects crop and livestock production (Jouzi et al., 2023), hence reducing the diversity in diet intake and less nutritious food, which compromises child health (Ahmed et al., 2021; Usman & Kopczewska, 2022).
The paper also found that the availability of skilled health workers significantly reduces child stunting, wasting, and underweight in Zimbabwe. Improving skilled health worker availability in a cluster reduces child stunting by 0.077, wasting by 0.034 and underweight by 0.056. The availability of skilled workers is essential in improving children’s health outcomes, thus improving child nutrition. More skilled health workers in a cluster increase the likelihood of receiving nutritional advice and healthcare services (Shrimpton, 2020; UNICEF, 2021). Zimbabwe and is still suffering from a brain drain from health workers during the 2007 and 2008 economic crises, which exposed the health sector (Sisimayi et al., 2021). Therefore, this brain drain challenge compromises the health care services children under five receive during routine health visits, which has an implication on their nutritional status.
The perception of distance to the facility was noted to be increasing child wasting in Zimbabwe. The longer the distance to the health facility, the more children were wasted (0.021) within the same cluster. In line with Govender et al. (2021) and Ntenda and Chuang (2018) findings, distance to the health facility contributes significantly to health access and child undernutrition. Health facilities provide nutritional advice and health care services, which might not reach those who stay far away from the health facilities. Given that children are more vulnerable to diseases and they need to access health facilities frequently, long distances to the facility result in most children failing to access health services, hence increasing the probability of undernutrition and child mortality in some cases. These children also stay in areas with poor infrastructure, which worsens their access to healthcare services in times of need.
Women’s education in a cluster also significantly improves child stunting and underweight. Children born from educated mothers are less stunted and underweight than those from uneducated mothers. This is in line with the results from Malawi (Ntenda & Chuang, 2018) and Ethiopia (Fantay et al., 2019; Ali et al., 2022). Educated women are empowered to make diet intake decisions and control resources in the households and community, enhancing health care utilisation, improving hygiene and accessing relevant information for child nutrition (Ntenda & Chuang, 2018). These women do not have to wait for their husbands to make decisions regarding child nutrition and health care services utilisation, therefore, they can act on the situation before it worsens. Moreover, educated women are more cognizant of their children’s health than uneducated women (Ali et al., 2022). Ncube-Murakwani et al. (2020) noted that the Zimbabwean Ministry of Health and Child Care implemented Amalima care groups that provided nutritional training to caregivers, and this intervention resulted in a seven percent reduction in stunting in rural Zimbabwe. This shows that education and training are vital in providing nutrition messages geared towards social behavioural change.
Although the paper provides insightful information on child undernutrition, several limitations are worth noting. Several variables are associated with child undernutrition, however, the paper only focused on the demographic and socioeconomic factors due to data limitations. In addition, the DHS does not normally collect information on food intake by children, which provides information on whether undernutrition results from poor food intake, for example, sweetened or chunk foods. Further studies should investigate the temporal dynamics of food security and child undernutrition to understand better associations over time, which was impossible for this study due to data limitations.
5 Conclusion
Child undernutrition is a global health challenge, and investigating its inequality and the contributing factors is crucial to eliminating it. Eliminating child undernutrition can ensure that every child has a healthy early life through physical and cognitive development, essential for healthy adult life and well-being. In that regard, the paper noted spatial inequality in child undernutrition in Zimbabwe. Child undernutrition is also spatially dependent and is intensely clustered at the district level, as indicated by hotspots and coldspots. Climate factors, skilled worker availability, perception of distance to the facility and education were associated with child stunting and underweight.
Alleviating child undernutrition inequality is essential to attain sustainable development goals. Therefore, policies to mitigate child undernutrition should be region-based, addressing districts with high stunting, wasting and underweight. Moreover, cluster-targeted interventions should be prioritised, given that these have the potential to reduce child undernutrition by contextualising the undernutrition challenge. Policymakers should develop integrated, effective and evidence-based policies to reduce child undernutrition and ensure that every child lives a healthy life. Thus, there is a need to improve mothers’ education by providing training on food intake and service utilisation using care groups (scaling up the Amalima care groups nationwide). Amalima mainly provides supplementary feeding rations, capacity building and community-based messaging delivered through care groups, which is important in enhancing nutrition care practices in the country hence improved under-five nutrition.There is also need to ensure frequent availability of skilled health workers and health facilities, to ensure improved quality of healthcare services received. the availability of skilled health workers and health facilities. and Moreover, policymakers should adopt the climate change farming to ensure food security and diversified and balanced diets among under-five children to reduce child under-nutrition in Zimbabwe
References
Ahmed, K. Y., Agho, K. E., Page, A., Arora, A., & Ogbo, F. A. (2021). Mapping geographical differences and examining the determinants of childhood stunting in Ethiopia: A bayesian geostatistical analysis. Nutrients, 13(6), 2104. https://doi.org/10.3390/nu13062104
Ali, M. S., Alemu, T. G., Techane, M. A., Wubneh, C. A., Assimamaw, N. T., Belay, G. M., Tamir, T. T., Muhye, A. B., Kassie, D. G., Wondim, A., Terefe, B., Tarekegn, B. T., Fentie, B., Gonete, A. T., Tekeba, B., Kassa, S. F., Desta, B. K., Ayele, A. D., Dessie, M. T., & Atalell, K. A. (2022). Spatial variation and determinants of underweight among children under 5 y of age in Ethiopia: A multilevel and spatial analysis based on data from the 2019 Ethiopian demographic and health survey. Nutrition, 102, 111743. https://doi.org/10.1016/j.nut.2022.111743
Amir-ud-Din, R., Fawad, S., & Naz, L. (2021). Nutritional inequalities among under-5 children: An analysis of cross-country and within-country hotspots and cold spots in the developing world. International Journal for Equity in Health, 21, 135.
Bloss, E., Wainaina, F., & Bailey, R. C. (2004). Prevalence and predictors of underweight, stunting, and wasting among children aged 5 and under in Western Kenya. Journal of Tropical Pediatrics, 50(5), 260–270. https://doi.org/10.1093/tropej/50.5.260
Bredenkamp, C., Buisman, L. R., & Van de Poel, E. (2014). Persistent inequalities in child undernutrition: Evidence from 80 countries, from 1990 to today. International Journal of Epidemiology, 43(4), 1328–1335. https://doi.org/10.1093/ije/dyu075
Chazireni, E. 2015. The temporospatial dimension of health in Zimbabwe. (March), (pp. 1–291). University of South Africa.
Chowdhury, T. R., Chakrabarty, S., Rakib, M., Afrin, S., Saltmarsh, S., & Winn, S. (2020). Factors associated with stunting and wasting in children under 2 years in Bangladesh. Heliyon, 6(9), e04849. https://doi.org/10.1016/j.heliyon.2020.e04849
Fantay Gebru, K., Mekonnen Haileselassie, W., Haftom Temesgen, A., Oumer Seid, A., & Afework Mulugeta, B. (2019). Determinants of stunting among under-five children in Ethiopia: A multilevel mixed-effects analysis of 2016 Ethiopian demographic and health survey data. BMC Pediatrics, 19(1), 1–13. https://doi.org/10.1186/s12887-019-1545-0
Food and Nutrition Council of Zimbabwe. (2018). Zimbabwe National Nutrition Survey 2018. Zimbabwe: Harare.
Frongillo, E. A., De Onis, M., & Hanson, K. M. P. (1997). Socioeconomic and demographic factors are associated with worldwide patterns of stunting and wasting of children. Journal of Nutrition, 127(12), 2302–2309. https://doi.org/10.1093/jn/127.12.2302
Girma, A., Woldie, H., Mekonnen, F. A., Gonete, K. A., & Sisay, M. (2019). Undernutrition and associated factors among urban children aged 24–59 months in North-west Ethiopia: A community based cross sectional study. BMC Pediatrics, 19(1), 1–11. https://doi.org/10.1186/s12887-019-1595-3
Govender, I., Rangiah, S., Kaswa, R., & Nzaumvila, D. (2021). Malnutrition in children under the age of 5 years in a primary health care setting. South African Family Practice, 63(1), 1–6. https://doi.org/10.4102/SAFP.V63I1.5416
Haile, D., Azage, M., Mola, T., & Rainey, R. (2016). Exploring spatial variations and factors associated with childhood stunting in Ethiopia: Spatial and multilevel analysis. BMC Pediatrics, 16(1), 1–14. https://doi.org/10.1186/s12887-016-0587-9
Human Data Exchange. 2018. Zimbabwe - Subnational Administrative Boundaries - Humanitarian Data Exchange. Available: https://data.humdata.org/dataset/cod-ab-zwe [25 July 2022].
Jouzi, Z., Nelson, S. A. C., & Leung, Y. F. (2023). Spatial heterogeneity of child malnutrition, proximity to protected areas and environmental variabilities in Zimbabwe. GeoJournal, 88(4), 3773–3789.
Khor, G. L. (2003). Update on the prevalence of malnutrition among children in Asia. Nepal Medical College Journal: NMCJ, 5(2), 113–122.
Lukwa, A. T., Siya, A., Zablon, K. N., Azam, J., & Alaba, O. (2020). Prevalence and Socioeconomic inequalities trends in child health comparing within and between group inequalities: Food insecurity and malnutrition in Zimbabwe. BMC Public Health, 20(1), 1199.
Martorell, R., & Young, M. F. (2012). Patterns of stunting and wasting: Potential explanatory factors. Advances in Nutrition, 3(2), 227–233. https://doi.org/10.3945/an.111.001107
Marume, A., Archary, M., & Mahomed, S. (2022). Dietary patterns and childhood stunting in Zimbabwe. BMC Nutrition, 8(1), 1–9. https://doi.org/10.1186/s40795-022-00607-7
Matema, R (2021). Predictors of stunting in children under 5 years of age in Zimbabwe. Available: https://scholarworks.waldenu.edu/dissertations.
Mayala, B., Fish, D. T., Eitelberg, D., & Dontamsetti, T. (2018). The DHS Program Geospatial Covariate Datasets Manual. Maryland, USA: Rockville.
Mgongo, M., Chotta, N. A. S., Hashim, T. H., Uriyo, J. G., Damian, D. J., Stray-Pedersen, B., Msuya, S. E., Wandel, M., & Vangen, S. (2017). Underweight, stunting and wasting among children in Kilimanjaro region, Tanzania; a population-based cross-sectional study. International Journal of Environmental Research and Public Health, 14(5), 1–12. https://doi.org/10.3390/ijerph14050509
Musuka, G., Dzinamarira, T., Murewanhema, G., Cuadros, D., Chingombe, I., Herrera, H., Takavarasha, F., & Mapingure, M. (2021). Associations of diarrhea episodes and seeking medical treatment among children under five years: Insights from the Zimbabwe Demographic Health Survey (2015–2016). Food Science and Nutrition, 9(11), 6335–6342. https://doi.org/10.1002/fsn3.2596
Ncube-Murakwani, P., Moyo, S. A., Maphosa, M., Dzimba, M., Dube, S. B., & Nyathi, C. (2020). Implementing care groups for improved maternal and child nutrition: Critical factors for success from the Amalima program in rural Zimbabwe. World Nutrition, 11(2), 90–107. https://doi.org/10.26596/wn.202011290-107
Ntenda, P. A. M., & Chuang, Y. C. (2018). Analysis of individual-level and community-level effects on childhood undernutrition in Malawi. Pediatrics and Neonatology, 59(4), 380–389. https://doi.org/10.1016/j.pedneo.2017.11.019
Nyarko, S. H., Bitew, F., & Amu, H. (2022). Spatial and temporal inequalities in undernutrition among non-pregnant women in Ghana: A multilevel analysis. Spatial Demography, 10(2), 193–207. https://doi.org/10.1007/s40980-020-00074-3
Pillai, V. K., & Maleku, A. (2019). Women’ s education and child stunting reduction in India. The Journal of Sociology & Social Welfare. https://doi.org/10.15453/0191-5096.4203
Sartorius, B., Sartorius, K., Green, R., Lutge, E., Scheelbeek, P., Tanser, F., Dangour, A. D., & Slotow, R. (2020). Spatial-temporal trends and risk factors for undernutrition and obesity among children (<5 years) in South Africa, 2008–2017: Findings from a nationally representative longitudinal panel survey. British Medical Journal Open, 10(4), 1–17. https://doi.org/10.1136/bmjopen-2019-034476
Seferidi, P., Hone, T., Duran, A. C., Bernabe-Ortiz, A., & Millett, C. (2022). Global inequalities in the double burden of malnutrition and associations with globalisation: A multilevel analysis of Demographic and Health Surveys from 55 low-income and middle-income countries, 1992–2018. The Lancet Global Health, 10(4), e482–e490. https://doi.org/10.1016/S2214-109X(21)00594-5
Shrimpton, R. (2020). Care groups and community-based approaches for improved maternal and child survival and development. World Nutrition, 3(11), 153–156. https://doi.org/10.26596/wn.2020113153-156
Sisimayi, C., Mupandawana, M., Mutambwa, M., Sisimayi, T., & Njovo, H. (2021). The multi-dimensional risk of stunting amongst children under five years in Zimbabwe. Zimbabwe: Harare.
Tamir, T. T., Techane, M. A., Dessie, M. T., & Atalell, K. A. (2022). Applied nutritional investigation spatial variation and determinants of stunting among children aged less than 5 y in Ethiopia: A spatial and multilevel analysis of Ethiopian Demographic and Health Survey 2019. Nutrition, 103–104, 111786. https://doi.org/10.1016/j.nut.2022.111786
Tette, E. M. A., Sifah, E. K., & Nartey, E. T. (2015). Factors affecting malnutrition in children and the uptake of interventions to prevent the condition. BMC Pediatrics, 15(1), 1–11. https://doi.org/10.1186/s12887-015-0496-3
Tobler, W. R. (1979). Smooth pycnophylactic interpolation for geographical regions. Journal of the American Statistical Association, 74(367), 519–530. https://doi.org/10.1080/01621459.1979.10481647
UNICEF. (2021). UNICEF conceptual framework on maternal and child nutrition. Available: https://www.unicef.org/media/113291/file/UNICEF Conceptual Framework.pdf.
Usman, M., & Kopczewska, K. (2022). Spatial and machine learning approach to model childhood stunting in Pakistan: Role of socioeconomic and environmental factors. International Journal of Environmental Research and Public Health, 19(17), 10967. https://doi.org/10.3390/ijerph191710967
Vitolo, M. R., Gama, C. M., Bortolini, G. A., Campagnolo, P. D. B., & Drachler, M. D. L. (2008). Some risk factors associated with overweight, stunting and wasting among children under 5 years old. Jornal de Pediatria, 84(3), 251–257. https://doi.org/10.2223/JPED.1776
WHO. (2022). Nutrition. Available: https://www.who.int/health-topics/nutrition#tab=tab_2 [February 7, 2023].
WHO. (2023). WHO Guideline on the prevention and management of wasting and nutritional oedema (acute malnutrition) in infants and children under 5 years. Available: https://iris.who.int/handle/10665/376075.
Wilson, E., Hazel, E., Park, L., Carter, E., Moulton, L. H., Heidkamp, R., & Perin, J. (2020). Obtaining district-level health estimates using geographically masked location from demographic and health survey data. International Journal of Health Geographics, 19(1), 1–14. https://doi.org/10.1186/s12942-020-0198-4
Wolde, M., Berhan, Y., & Chala, A. (2015). Determinants of underweight, stunting and wasting among schoolchildren. BMC Public Health, 15(1), 1–9. https://doi.org/10.1186/s12889-014-1337-2
Wooldridge, J. M. (2010). Econometrics analysis of cross section and panel data. The MIT Press. https://doi.org/10.1515/humr.2003.021
Wooldridge, J. M. (2015). Introduction econometrics: A modern approach (5th ed.). Cengage learning. https://doi.org/10.1201/9781315215402-43
Yayo Negasi, M. (2021). Dynamics of inequality in child under-nutrition in Ethiopia. International Journal for Equity in Health, 20(1), 1–30. https://doi.org/10.1186/s12939-021-01478-3
ZIMSTAT and ICF International. (2011). Zimbabwe Demographic Health Survey 2010/11. ZWKR62FL.DTA. Rockville, Maryland, USA: Zimbabwe National Statistics Agency (ZIMSTAT) and ICF International.
ZIMSTAT and ICF International. (2012). Zimbabwe Demographic and Health Survey 2010–11. Calverton, Maryland. Available: papers2://publication/uuid/1C4DF325–60C4–461C-B2C4–132065D84E2F.
ZIMSTAT and ICF International. (2016a). Zimbabwe Demographic Health Survey 2015: Final Report. Rockville, Maryland, USA: Zimbabwe National Statistics Agency (ZIMSTAT) and ICF International. https://doi.org/10.1017/CBO9781107415324.004.
ZIMSTAT and ICF International. (2016b). Zimbabwe Demographic Health Survey 2015. ZWKR72FL.DTA. Rockville, Maryland, USA: Zimbabwe National Statistics Agency (ZIMSTAT) and ICF International.
Funding
No external funding was received for this paper.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The author declares no conflict of interest.
Ethical Approval
No ethical approval needed for this study because it used publicly available data, which is not sensitive and not linked to person or household identifiers. The present study, therefore, did not involve direct interaction with, or data gathering from human or organisational participants.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Chari, A. Spatial Inequality in Undernutrition Among Under-Five Children in Zimbabwe. Spat Demogr 12, 5 (2024). https://doi.org/10.1007/s40980-024-00126-y
Accepted:
Published:
DOI: https://doi.org/10.1007/s40980-024-00126-y