
Abstract
Adverse sexual and reproductive health outcomes resulting from risky sexual behaviours (RSB) among young adults disproportionately affect them and contribute to an increased burden of sexually transmitted diseases. Existing research in sub-Saharan Africa, has yielded contrasting findings on the factors associated with the sexual behaviour of young people. This paper presents a comprehensive examination of the geographical distribution and socio-demographic determinants of RSB among young people in Nigeria, focusing on three primary outcomes: unprotected sex, multiple sexual partners, and early sexual debut. This study used cross-sectional data from the 2018 Nigeria Demographic and Health Survey on young adults aged 15–24 years. Descriptive and inferential statistics, including Bayesian multivariate shared component spatial modelling were used to assess geographical and socio-demographic factors influencing RSB. Males in the North-West region exhibited a high prevalence of unprotected sex and early sexual debut while unprotected sex was more prevalent among females in the South–South region. Furthermore, individuals in the South-South and Central regions consistently showed a higher likelihood of engaging in all three indicators of RSB. Individuals who were employed as well as rural residents had an increased risk of early sexual debut and multiple sexual partners. Furthermore, mobile phone and internet access were found to impact RSB. These findings offer insights into the geographic distribution and socio-demographic determinants of RSB among young people, highlighting the need for tailored interventions. These insights can inform the development of targeted interventions, education programs, and policies to reduce the prevalence of RSB.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Background
Sexually transmitted infections (STIs) pose a significant public health concern globally, with a particular impact on young people aged 15–24 (Visalli et al., 2014). This age group represents a crucial demographic in terms of sexual health, as it is characterised by physical and emotional changes, increasing sexual activity, and important life transitions (Arain et al., 2013; World Health Oragnization (WHO), 2023). STIs, including Human Immunodeficiency Virus (HIV) and Acquired Immunodeficiency Syndrome (AIDS), have a disproportionately high prevalence and incidence among young people, particularly in developing countries (Aral et al., 2006). This places them at considerable risk of immediate health complications and long-term consequences (Azene et al., 2022).
In many parts of the world, young people lack adequate sexual education, access to healthcare services, and resources for practising safe sexual behaviours (Janighorban et al., 2022). This contributes to the alarming prevalence of STIs within this age group. For instance, in 2019, young people aged 15–24 accounted for approximately 2 out of every 7 new HIV infections, with approximately 460,000 new HIV infections reported among this age group (UNAIDS, 2021). Additionally, factors such as peer pressure, experimentation, and a lack of awareness about the importance of protection during sexual activity can further exacerbate the risk of contracting infections (Ochen et al., 2019; Raheel et al., 2013). Adverse sexual and reproductive health outcomes, including HIV, sexually transmitted infections (STIs), unsafe abortion, early marriage, and sexual violence, disproportionately affect young people and contribute to an increased burden of disability-adjusted life-years (Mokdad et al., 2016). These outcomes have both immediate and long-term implications across various aspects of their lives(Azene et al., 2022). The primary vulnerability stems from their engagement in risky sexual behaviours (RSB), such as having multiple sexual partners, early sexual debut, and unprotected sex, resulting in over one million new STIs daily worldwide(Ochen et al., 2019; World Health Organization (WHO), 2023).
The situation is particularly challenging in low-and middle-income countries where resources for healthcare, education, and sexual health services are often limited (Church et al., 2010). These countries face socioeconomic challenges that hinder comprehensive STI prevention and control efforts (Aral et al., 2006). As a result, STIs, including HIV and AIDS, continue to spread among young people in these regions (Aral et al., 2006). Existing research on the sexual behaviour of young people in sub-Saharan Africa, has identified various factors associated with these behaviours in young people, which vary by gender (Adedini et al., 2021; Amo-Adjei & Tuoyire, 2018; Odimegwu & Somefun, 2017; Yaya & Bishwajit, 2018). Some studies have indicated that increased socioeconomic status reduces the risk of early sexual debut among young women, whereas the opposite holds true for young men (Amo-Adjei & Tuoyire, 2018; Odimegwu & Somefun, 2017). In addition, while a low level of education was reported to increase the risk of early sexual debut in females, it had an opposite effect on males (Amo-Adjei & Tuoyire, 2018). Furthermore, lack of parental supervision was a predictor of sexual debut in males (Marston et al., 2013). Previous studies conducted in Nigeria have consistently reported low condom and contraceptive usage among young people (Adedini et al., 2018; Ajayi & Okeke, 2019; Tenkorang, 2022), as well as multiple sexual partners (Yaya & Bishwajit, 2018) and early sexual debut (Alawode et al., 2021; Yaya & Bishwajit, 2018). A meta-analysis conducted across 26 countries identified males, those who are educated to secondary and above, those living in urban areas and from the middle to highest wealth index as risk factors for RSB (Berhan & Berhan, 2015). In contrast, some studies have identified females (Eyeberu et al., 2023; Eze et al., 2022), and those residing in rural areas at increased risk of RSB (Eze et al., 2022). Also, contrasting evidence suggests that young people with higher education are less likely to engage in early sexual intercourse (Adedini et al., 2018; Fatusi & Blum, 2008). Other factors include having access to mass media such as TV, mobile, newspaper, and internet use (Asekun-Olarinmoye et al., 2014; Eyeberu et al., 2023; Omisore et al., 2022). Furthermore, regional disparities in sexual behaviour among young people in Nigeria have been observed, particularly regarding the timing of first sexual intercourse between individuals in the northern and southern regions, highlighting the influence of geographic and cultural factors on sexual and reproductive health behaviour (Amoyaw & Luginaah, 2017).
Addressing these issues requires a multi-pronged approach, including comprehensive sex education, increased access to affordable and confidential healthcare services, promoting safe sexual practices, and reducing the stigma associated with STIs (Desrosiers et al., 2020). Additionally, efforts to empower young people with accurate information and tools to protect themselves are essential in combating the high prevalence and incidence of STIs among individuals aged 15–24, both globally and especially in developing countries (Starrs et al., 2018). However, to ensure the efficacy of proposed interventions, it is important to assess the dependencies between the multiple variables that interplay to cause a high level of engagement in RSB among young adults and the correlates and geographical context of RSB. This will help to promote better geographically targeted intervention programs.
Nonetheless, limited attention has been given to the exploration of the spatial patterns (heterogeneity) of RSB among young adults at a micro-geographical level. Establishing a quantitative baseline of RSB allows for effective monitoring and evaluation of progress over time. Regions identified with extreme RSB can be monitored for improvements based on interventions applied, helping to assess the effectiveness of different strategies and policies (Mirzaei et al., 2016). Additionally, by quantifying how RSB varies spatially, policymakers and planners can identify which regions are most burdened and thus require more immediate attention or resources. This facilitates more efficient and targeted allocation of resources, ensuring that interventions are directed where they are most needed (Eryando, 2022). Furthermore, existing studies pertaining to RSB among young adults in Nigeria have so far addressed the risk factors as separate elements without considering the interactions between them and the implications for different geographical regions/ locations (Odimegwu & Somefun, 2017; Olugbenga-Bello et al., 2009; Owoaje & Uchendu, 2009; Ugoji, 2014). These studies have failed to examine the influence of geographical variations on young adults’ involvement in RSB, particularly in relation to micro-spatial scale.
This present study utilised a Bayesian multivariate spatial modelling to assess RSB among young people in Nigeria while treating age as a nonlinear variable. This approach helps in understanding the disparities in RSB across different regions and can uncover underlying factors contributing to these disparities, such as economic, environmental, or social determinants, as well as capturing the nonlinear effects of age. By mapping these patterns, the approach provides a clear visual representation of inequality, which can be a powerful tool in advocacy and policy making, particularly in settings where barriers exist in sex education for young people (Aliyu & Aransiola, 2023; Mbachu et al., 2020). The attainment of Sustainable Development Goal (3), calls for action to ensure that all people have access to reproductive health information and education by 2030, as well as the inclusion of reproductive health in national policies and programs (World Health Organization (WHO), 2019). The findings could provide valuable data to stakeholders working on young people’s sexual and reproductive health, enabling the development of evidence-based interventions to reduce RSB and its adverse effects, such as STIs, including HIV/AIDS and the prevention of unintended pregnancy.
2 Methods
2.1 Data Source
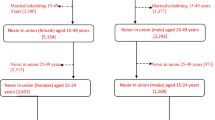
This study was conducted among young men and women aged 15–24 years in Nigeria. Data were sourced from the 2018 Nigeria demographic and health survey women’s and men’s files. The variables were recoded for uniformity and subsequently merged for analysis. The Demographic Health Survey (DHS) is a nationally representative survey that is carried out periodically, often every five years, in over 85 low- and middle-income countries worldwide. The survey collects demographic and health information from women, children and men in various households sampled. The sampling frame for the 2018 Nigeria DHS was based on the previous census conducted in 2006. Nigeria has 36 states. These states are divided into local government areas (LGAs), each containing localities, which are further segmented into enumeration areas (EAs), also called survey clusters (Fig. 1). The survey adopted a 2-staged stratified sampling approach to select respondents. The first stage was characterised by the selection of 1400 EAs chosen proportional to the size of the households within the EAs. In the second stage, a fixed number of 30 households were chosen in every cluster and this translated to 42,000 households. A total of 40,666 households were captured, showing a response rate of 99%. Within these households, 41,821 and 13,311 women aged 15–49 and men aged 15–59, respectively, were successfully interviewed, and all showed a response rate of 99%. However, for this study, only 8,884 young people with complete cases of RSB indicators comprised the sample size. Details of the sampling procedure, pretesting of the instruments and training of field staff have been published in the main report (Nigeria, 2019). The data set is publicly available at https://www.dhsprogram.com/data/dataset/Nigeria_Standard-DHS_2018.cfm?flag=0. The Nigeria boundary representation shapefiles were also used as provided by the DHS GIS/Spatial data repository database available from https://spatialdata.dhsprogram.com.

Map of Nigeria showing, A the six geopolitical regions and the 36 states plus the Federal Capital Territory, B the triangulation mesh of the study area, where the vertices serve as the base for the triangulation process discretising the continuous random field. The collected sample locations (survey cluster) are depicted as red dot points in the figure
2.2 Study Variables
2.2.1 Dependent Variable
The dependent variable for the study was RSB. It was defined based on three indicators; 1) non-condom use during most recent sexual intercourse (yes, no), 2) age at first sex (below 15, 15 or more) and 3) multiple sexual partners (1, 2 or more). The same variables have been used to measure RSB in previous studies using DHS data (Adedini et al., 2021). For the purposes of this study, non-condom use during most recent sexual intercourse has been tagged as unprotected sex and age at first sex of below 15 years has been tagged as early sexual debut.
2.2.2 Independent Variable
Fourteen independent variables were considered in this study. These were current age in years, sex (male, female), education (no formal education, primary, secondary, higher), currently working (no, yes), religion (Christians, Muslims, other), marital status (not currently married, currently married), wealth status (poorest, poorer, middle, richer, richest), residence (urban, rural) and region of residence (north-east, north-west, south-east, south-south, south-west). Other variables were internet use, Access to radio, Access to Television (TV), Access to mobile and access to newspapers which had yes or no responses. The choice of these variables was informed by the literature (Adedini et al., 2021; Amo-Adjei & Tuoyire, 2018; Odimegwu & Somefun, 2017; Yaya & Bishwajit, 2018).
2.3 Statistical Analysis
All data analyses were carried out in Stata version 14.0 and R version 4.0.2. Both descriptive and inferential analyses were employed. The descriptive analysis was used to describe the characteristics of the respondents and the prevalence of RSB using frequencies and percentages. First, a preliminary analysis of geographical variation of RSB (i.e. unprotected sex, multiple sexual partners and early sexual debut) was undertaken at the cluster level. Figure 2 revealed that RSB in Nigeria were geographically varied, therefore, a shared-component regression model that jointly analysed the spatial variation of rates of multiple outcomes with common risk factors was adapted to this data (Held et al., 2005). Furthermore, allowing for a more flexible representation of age effects, age was treated as a nonlinear variable to adequately capture its varied impact on the RSB across different age groups (Fig. 3).

Geographical distribution of the three main outcomes (non-condom use, multiple sexual partners and early sexual debut) in the study

Estimate marginal effect of current age A unprotected sex and early sexual debut. b Unprotected sex and multiple sexual partners, C Multiple sexual partners and early sexual debut, D All three risky behaviours
2.3.1 Shared Component Model
A shared and non-shared spatial effects of non-condom use, multiple sexual partners and early sexual debut was fitted via integrated nested Laplace approximations (INLA) implemented through R-INLA, which does a full Bayesian analysis of latent Gaussian models (Lindgren et al., 2011). This method, proposed by Lindgren et al. (2011) offers an alternative to modelling Gaussian random fields, significantly reducing computational costs. It represents the continuous spatial process by discretising it into a spatial random process known as a Gaussian Markov random field (GMRF) via the SPDE technique. The regression model considers that data may be spatially correlated since data in neighbouring areas may be more similar than those farther away.
The model was formulated as follows:
Let \({Y}_{ijk}=1, i\in \left\{1,\dots ,8964\right\},\) if a respondent \(i\) from survey cluster \(j=1,\dots ,1400\) engage in RSB \(k=\text{1,2},3, (\) 1 = non-condom use, 2 = multiple sexual partners and 3 = early sexual debut), and \({Y}_{ijk}=0\) if otherwise. Therefore, \({y}_{ijk}|{p}_{ijk}\sim Binomial({n}_{ijk},{p}_{ijk})\), where \({p}_{ijk}=\text{Pr}({y}_{ijk}=1)\), is the probability that a respondent engages in any of the RSB. Assuming \(X\) is a vector of all available covariates and a logit link function transforms the covariates into probabilities expressed as:
such that
where \(\beta\) is the parameter vector for categorical variables. Through exponentiation, the continuous values derived from the model \(X\beta\), are converted into probability values. These probability values serve as the scale for the parameter \({p}_{ijk}\).
Assuming that the covariate vector consists of variables of different types, such as Δ, a collection of the categorical variables, g representing the metrical covariates, and \({U}_{jk}\) is a random effect. These covariates can be linked through the predictor \({\eta }_{jk}\), thus
where \(\alpha\) is the intercept, \(\beta\) represents the categorical covariate effect, and \(f(g)\) is the metrical covariates.
To simultaneously explore the three RSBs, the study employed a spatial shared component model as introduced by (Knorr-Held & Best, 2001) Knorr-Held and Best. This model split the random effect on a RSB \(k\) into a general burden shared across all three types of RSB and pairwise shared components. Thus, the model is:
\(g({u}_{i})\) is the latent shared component (spatial field) common to the three RSB with \({\delta }_{i}\) being a weight used to allow for a varying risk gradient of shared components for each risky behaviour \(k\).
A stochastic partial differential equation (SPDE) was employed to incorporate all the shared spatial random elements (all three and pairwise). This equation connects a continuous spatial Gaussian field to a discretely indexed Gaussian Markov random field.
where \(k>0\) is a scale parameter, \(\Delta\) is the Laplacian, \(u\epsilon {\mathbb{R}}^{d}, \alpha\) is the smoothness parameter, \(\tau\) controls the variance, \(\Psi (u)\) is a Gaussian white noise process, \(y\left(u\right)\), has a Matern (Blangiardo & Cameletti, 2015) covariance function expressed as:
where \(\parallel {u}_{i}-{u}_{j}\parallel\) is the Euclidean distance between locations \({u}_{i}\) and \({u}_{j}\in {\mathbb{R}}^{d}\) and \({\sigma }^{2}\) is the marginal variance. The term \({K}_{\lambda }\) is a modified Bessel function of the second kind and \(\lambda >0\) measures the degree of smoothness of the function (Cameletti et al., 2013). \(y\left(u\right)\) is the exact stationary solution of the SPDE.
Now, utilizing the finite elements method to approximate \(u\) by expressing it as a linear combination of a finite set of basis functions associated with nodes on a triangular mesh covering the domain of \(u\),
where \(y\left(u\right)\) is represented as a sum over basis functions weighted by zero-mean Gaussian distributed coefficients \({\omega }_{l}\). The basis functions, denoted as \({\varphi }_{l}\), are defined such that they are linear within each triangle, taking the value of 1 at their respective nodes, and 0 at all other nodes. This construction enables barycentric interpolation within each triangle, enhancing accuracy. The mesh is designed to have finer triangles near the areas of interest to improve accuracy while minimising computational costs. A Delaunay triangulation is employed to optimise the triangle shapes, preventing the formation of overly elongated triangles, which would compromise interpolation accuracy (see Fig. 1b).
Similar to Gayawan et al., (2022), \(\alpha\) and \(\beta\) were assigned a weakly informative Gaussian prior with small precision; the smooth function \(f\left(g\right)\) were modelled through a random walk of order 2 prior; the shared and non-shared spatial components are assumed to follow a Gaussian Markov random field (Cameletti et al., 2013) with a two-parameter penalised prior, type 2 Gumbel distribution prevents over-fitting especially for an over-parameterised model (Gayawan et al., 2022; Simpson et al., 2017).
The model provided smoothed relative risks (logRR) of RSB in Nigeria to stabilise regions with smaller counts and populations. The posterior means were mapped together with their 95% credibility interval.
3 Results
3.1 Socio-Demographic Characteristics of Respondents
Table 1 shows the socio-demographic characteristics of respondents. It was found that the majority (90.3%) of the respondents were females and 67.5% of the respondents were aged 20–24. About 43% of the respondents had a secondary level of education, with 7% having higher education. More than half (53.6%) were currently working, while about 57% were Muslims. Sixty six percent were currently married. About 24% were in poorer households, 68.9% were in rural areas and 28.5% were in South-East region.
Figure 2 presents the geographical distribution of three main outcomes: unprotected sex, multiple sexual partners, and early sexual debut. In Fig. 2A, a high percentage of unprotected sex was observed among males in the North-West region, while in the South-South region, unprotected sex was more prevalent among females (Fig. 2D). Regarding multiple sexual partners, there was spatial variation, with South-South males showing a higher prevalence (2B). On the other hand, females in the North-East, South-South, and South-West regions had higher proportions of multiple sexual partners (2E). For early sexual debut, it was more prevalent among males in the North-West region (Sokoto) and parts of the North-East region (Gombe) (2C).
3.2 Risk Factors for Risky Sexual Behaviours
Table 2 displays the posterior mean and corresponding 95% credibile intervals (CI) for various indicators of RSB, both in pairs and all together. Young people who used the internet exhibit a higher risk of engaging in RSB: unprotected sex and early sexual debut (0.24; 95%CI = 0.09, 0.38), unprotected sex and multiple sexual partners (0.45; 95%CI = − 0.28, 0.62), early sexual debut and multiple sexual partners (0.16; 95%CI = 0.01, 0.31), and all three indicators combined (0.15; 95%CI = 0.06, 0.27). Regarding employment status, those who were employed faced an increased risk of early sexual debut and multiple sexual partners (0.12; 95%CI = 0.02, 0.21). Rural residents had a reduced risk of condom use and early sexual debut (− 0.11; 95%CI = − 0.21, − 0.01), condom use and multiple sexual partners (− 0.22; 95%CI = − 0.37, − 0.08), but an increased risk of early sexual debut and multiple sexual partners (0.14; 95%CI = 0.04, 0.24). In terms of mobile phone access, those with mobile phones had a reduced risk of condom use and early sexual debut (− 0.12; 95%CI = − 0.23, − 0.01) and early sexual debut and multiple sexual partners (− 0.13; 95%CI = − 0.25, − 0.02), but an increased risk of condom use and multiple sexual partners (pm = 0.37; 95%CI = 0.20, 0.53) compared to those without mobile phones. Those in the richest wealth quintile had a reduced risk of condom use and early sexual debut (− 0.22; 95%CI = − 0.44, − 0.01) and early sexual debut and multiple sexual partners (− 0.25; 95%CI = − 0.47, − 0.03) compared to the poorest individuals. Muslims had reduced risk of unprotected sex e and early sexual debut (− 0.28;95%CI = − 0.42, − 0.13), unprotected sex and multiple sexual partners (− 0.49;95%CI = − 0.68, − 0.30) and all three (− 0.26; 95%CI = -0.06, − 0.14) compared to Christians. Currently, married young people had a reduced risk of engaging in unprotected sex and early sexual debut (− 0.99;95%CI = − 1.12, − 0.87), unprotected sex and multiple sexual partners (− 4.79; 95%CI = − 5.02, − 4.58) and EASI and MSP (− 2.64; 95%CI = − 2.77, − 2.51).
Figure 3 presents estimates of the marginal effect of current age on pairs of RSB: condom use and early sexual debut, condom use and multiple sexual partners, multiple sexual partners and early sexual debut, and all three behaviours. The marginal estimates show a consistent risk pattern across all indicators of RSB. Specifically, as young people age, the risk of engaging in all components of RSB decreases (Figs. 3A-D).
3.3 Shared Random Effect
Figure 4 displays the map of the shared spatial random effect. It indicates that individuals in the South-South and Central regions were more likely to engage in unprotected sex and early sexual debut (Fig. 4A), as well as multiple sexual partners and early sexual debut. However, there was no distinct pattern observed for condom use and multiple sexual partners (Fig. 4B). Likewise, the pattern for all three indicators together was not very clear, but individuals in the South-South and Central regions (Benue, Kogi, Nasarawa) showed a higher likelihood of engaging in all three indicators of RSB (Fig. 4 D).

Shared spatial random effect. A Unprotected sex and early sexual debut. B Unprotected sex and multiple sexual partners, C Multiple sexual partners and early sexual debut, D All three risky behaviours
4 Discussion
This study provides valuable insights into the geographical distribution of RSB among young people in Nigeria, as well as the influence of various socio-demographic factors on these behaviours. The key outcomes examined in this study include unprotected sex, multiple sexual partners, and early sexual debut. These findings can inform public health interventions and policies aimed at reducing the prevalence of RSB among young individuals.
Most young people (86.1%) in this study had unprotected sex in their most recent sexual encounter, surpassing the prevalence of 72% in SSA and 39.5% in Ethiopia (Ali & Tadele, 2021; Ndagijimana et al., 2023). Additionally, 30% of young people had multiple sexual partners, aligning with findings from a Cameroonian study (Tarkang, 2015). However, this was lower than the 54.5% and 42% reported by Tarkang et al., 2018 and Fetene and Mekonnen., 2018, respectively (Fetene & Mekonnen, 2018; Tarkang et al., 2018). Moreover, 19.3% of young people had their first sexual experience before age 15, higher than the prevalence reported in a study conducted in Kenya, Malawi, Nigeria, Tanzania, and Uganda (Seff et al., 2021). These variations may stem from differences in cultural norms and participant demographics between the studied countries (Fetene & Mekonnen, 2018; Watsi & Tarkang, 2020). The prevalence of RSB in Nigeria may be explained by various factors. Odimegwu and Somefun., 2017, argued that Nigerian youth express masculinity and femininity through early sexual relations (Odimegwu & Somefun, 2017). Additionally, violence against young women (Kullima et al., 2015; Odimegwu & Somefun, 2017; Seff et al., 2021) and patriarchal traditions promoting child marriage, especially in the Northern regions, could contribute to these behaviours (Odimegwu & Somefun, 2017). Furthermore, this study consistently found a higher RSB than previous research (Adedini et al., 2021; Tuoyire et al., 2018). This highlights the need for gender-specific interventions, with a particular focus on young women as they are more impacted by RSB.
The geographic distribution of RSB revealed notable variations across regions in the study area. Specifically, the North-West region stands out with a high prevalence of unprotected sex among males, and early sexual debut is also more prevalent in this region, as well as parts of the North-East. In contrast, the South-South region exhibits a distinctive pattern where unprotected sex is more prevalent among females, and there is a higher prevalence of multiple sexual partners among South-South males. Previous studies in Nigeria also reported geographic and rural–urban variations in young people's RSB. For instance, a study found that young people in the North-East region were more likely to have multiple sexual relationships, while those in the South-West region were less likely to inconsistently use condoms (Adedini et al., 2021). These differences may be attributed to economic, social, and cultural factors in the respective regions (Amoyaw & Luginaah, 2017). This regional variation suggests the importance of tailored interventions that consider local factors and specific cultural norms. Furthermore, individuals in the South-South and Central regions consistently displayed a higher likelihood of engaging in all three indicators of RSB. This suggests that these regions might require particular attention in public health campaigns and interventions aimed at reducing RSB among young people. Furthermore, rural residents exhibited distinct patterns in risky RSB. They had reduced condom use and early sexual debut. This finding further highlights the need for region-specific interventions, as rural areas may have unique challenges and opportunities for addressing RSB among young people.
Employment status was associated with early sexual debut and multiple sexual partners, in line with previous research across select African countries (Puplampu et al., 2021). Employment may expose individuals to affluence and increase the likelihood of transactional sex, leading to a higher risk of engaging in high-risk sexual behaviours (Alsan & Cutler, 2013; Puplampu et al., 2021). However, the study also found that young people in the wealthiest quintile were less likely to engage in non-condom use or early sexual debut, consistent with a previous study (Zhang et al., 2013). This underscores the significant influence of family economic status on young people's RSB. Some scholars have argued that young people from poor family backgrounds, particularly young girls engage in RSB as a means of economic coping mechanism (Amoateng et al., 2014; Ritchwood et al., 2016). There was a reduced risk of engaging in RSB as young people age. Specifically, young people aged 15–19 were more likely to engage in RSB than those aged 20–24. This result is in line with findings from several investigations (Adedini et al., 2021; Fetene & Mekonnen, 2018). This is partly explained by the curiosity associated with the adolescence stage and the influence of peers on adolescents’ behaviour. This finding suggests that employment status can influence the sexual behaviours of young people and underscores the importance of comprehensive sexual education programs for working individuals (Adedini et al., 2021; Fetene & Mekonnen, 2018).
The study also identified internet and mobile phone usage as predictors of RSB among young people in Nigeria, aligning with previous research in SSA (Agbede et al., 2016; Onasoga et al., 2020). The observed association could be partially explained by the ease of accessing such content, the influence of social media on norms and behaviors, and the possible desensitization to risky behaviors promoted through various online channels.This suggests that mobile phones can be leveraged as a tool for delivering sexual education and prevention strategies, while also recognising the potential risks associated with mobile phone use. While the internet offers a promising platform for disseminating health information and facilitating information exchange, it also exposes young people to inappropriate sexual content and social media misuse (Onasoga et al., 2020). This suggests that increased exposure to inappropriate online sexual content may heighten the negative effects on young people's sexual behaviour (Landry et al., 2017). Furthermore, the findings indicated that Muslim youth had a lower risk of engaging in RSB compared to Christians, consistent with prior studies (Tarkang, 2015; Tarkang et al., 2019). This finding may be explained by the more conservative stance on ‘inappropriate’ sexual behaviour in the Islamic religion, discouraging behaviours such as premarital sex (Odii et al., 2020; Watsi & Tarkang, 2020). This finding highlights the need for targeted interventions that incorporate safe online practices and education to reduce the risk of engaging in RSB among internet users. Policies aimed at creating digital literacy programs that educate young people about the responsible use of internet, particularly in relation to sexual health, are crucial. Additionally, these findings suggest the importance of involving educators and parents in monitoring and guiding internet use among youths to mitigate the risks associated with these behaviors (American Psychological Association (APA), 2024).
4.1 Strength and Limitations
This study used nationally representative data, allowing for generalisation of findings to all young people in Nigeria. It also highlights the benefits of employing a trivariate additive model to combine the three RSB indicators when quantifying the marginal effects of each indicator, thus addressing potential residual dependence between outcomes given observed covariates (Gayawan et al., 2023). However, some limitations may affect generalisability of the study findings. These include potential exaggeration and underreporting of sexual activity and the number of sexual partners, influenced by social norms where men tend to exaggerate and women tend to understate their sexual behaviour (Odimegwu & Somefun, 2017). Additionally, recall bias may have influenced participants’ recall of their age of sexual debut. Furthermore, due to the cross-sectional nature of the study design, it is important to note that the findings cannot establish causal relationships.
5 Conclusion
In conclusion, this study provides valuable information about the geographical distribution of RSB and their associations with various socio-demographic factors. The findings emphasise the importance of considering socioeconomic status, religion, and marital status in designing effective interventions and awareness campaigns. These findings can inform the development of gender and region-specific interventions, education programs, and policies to reduce the prevalence of RSB among young people. Tailored strategies that consider regional and individual factors are essential for the success of such interventions. Additionally, the influence of internet use on RSB underscores the importance of integrating digital literacy and safety into sexual education programs for young people in the digital age.
References
Adedini, S. A., Babalola, S., Ibeawuchi, C., Omotoso, O., Akiode, A., & Odeku, M. (2018). Role of religious leaders in promoting contraceptive use in Nigeria: Evidence from the Nigerian urban reproductive health initiative. Global Health: Science and Practice, 6(3), 500–514. https://doi.org/10.9745/ghsp-d-18-00135
Adedini, S. A., Mobolaji, J. W., Alabi, M., & Fatusi, A. O. (2021). Changes in contraceptive and sexual behaviours among unmarried young people in Nigeria: Evidence from nationally representative surveys. PLoS ONE, 16(2), e0246309. https://doi.org/10.1371/journal.pone.0246309
Agbede, O. C., Kio, J. O., & Ajetunmobi, A. A. (2016). Analysis of the influence of the internet on sexuality education and sexual behaviour among adolescents in Nigeria universities: The case of university of Lagos. Journal of Biology, Agriculture and Healthcare, 6(16), 74–83.
Ajayi, A. I., & Okeke, S. R. (2019). Protective sexual behaviours among young adults in Nigeria: Influence of family support and living with both parents. BMC Public Health, 19, 1–8.
Alawode, O. A., Ogunwemimo, H., Bolorunduro, M.-E., & Awoleye, A. F. (2021). Age at sexual debut and multiple sexual partnerships among adolescents in Nigeria: An assessment of the mediating role of the knowledge of sexually transmitted infections. Adolescents, 1(4), 421–432.
Ali, R., & Tadele, A. (2021). Risky sexual behavior across extremes of wealth in sub-Saharan Africa: A meta-analysis of demographic and health surveys. Ethiopian Journal of Health Sciences, 31(1), 159.
Aliyu, T. K., & Aransiola, J. O. (2023). Parent-adolescent communication about reproductive health issues in Nigeria. SAGE Open, 13(2), 1–7.
Alsan, M. M., & Cutler, D. M. (2013). Girls’ education and HIV risk: Evidence from Uganda. Journal of Health Economics, 32(5), 863–872.
American Psychological Association (APA). (2024). Health advisory on social media use in adolescence. American Psychological Association (APA). Retrieved 18 April from
Amo-Adjei, J., & Tuoyire, D. A. (2018). Timing of sexual debut among unmarried youths aged 15–24 years in sub-Saharan Africa. Journal of Biosocial Science, 50(2), 161–177.
Amoateng, A. Y., Kalule-Sabiti, I., & Arkaah, Y. J. (2014). The effect of socio-demographic factors on risky-sexual behaviours of adolescents in the North West Province of South Africa. African Population Studies, 28(1), 487–498.
Amoyaw, J. A., & Luginaah, I. (2017). Residential spaces and timing of first sexual intercourse among never-married youths in Nigeria. Archives of Sexual Behavior, 46, 1939–1948.
Arain, M., Haque, M., Johal, L., Mathur, P., Nel, W., Rais, A., Sandhu, R., & Sharma, S. (2013). Maturation of the adolescent brain. Neuropsychiatric Disease and Treatment, 9, 449–461. https://doi.org/10.2147/ndt.S39776
Aral, S. O., Over, M., Manhart, L., & Holmes, K. K. (2006). Sexually transmitted infections. In Jamison, D. T., Brennan, J.G., Measham, A. R., Alleyne, G., Claeson, M., Evans, D. B., Jha, P., Mills, A., Musgrove, P., (Eds.), Disease control priorities in developing countries. (2nd ed.). The International Bank for Reconstruction and Development / The World Bank. https://www.ncbi.nlm.nih.gov/books/NBK11734/
Arije, O., Udoh, E., Ijadunola, K., Afolabi, O., Aransiola, J., Omoregie, G., Tomori-Adeleye, O., Ukeme-Edet, O., Fajemisin, O., & Titus, R. (2023). Combination prevention package of interventions for reducing vulnerability to HIV among adolescent girls and young women in Nigeria: An action research. PLoS ONE, 18(1), e0279077.
Asekun-Olarinmoye, O. S., Asekun-Olarinmoye, E. O., Adebimpe, W. O., & Omisore, A. G. (2014). Effect of mass media and Internet on sexual behavior of undergraduates in Osogbo metropolis, Southwestern Nigeria. Adolescent Health, Medicine and Therapeutics, 5, 15–23.
Azene, Z. N., Tsegaye, L., Gebriel, M. W., Tadesse, A., Tadele, A., Aynalem, G. L., Andualem, Z., & Taye, B. T. (2022). Risky sexual practice and associated factors among youth preparatory students in Gondar City. Northwest Ethiopia. Frontiers in Public Health, 10, 843359. https://doi.org/10.3389/fpubh.2022.843359
Berhan, Y., & Berhan, A. (2015). Is higher risk sex common among male or female youths? SAHARA-J: Journal of Social Aspects of HIV/AIDS, 12(1), 106–115.
Blangiardo, M., & Cameletti, M. (2015). Spatial and spatio-temporal Bayesian models with R-INLA. John Wiley & Sons.
Cameletti, M., Lindgren, F., Simpson, D., & Rue, H. (2013). Spatio-temporal modeling of particulate matter concentration through the SPDE approach. AStA Advances in Statistical Analysis, 97(2), 109–131. https://doi.org/10.1007/s10182-012-0196-3
Church, K., De Koning, K., Hilber, A. M., Ormel, H., & Hawkes, S. (2010). Integrating sexual health services into primary care: An overview of health systems issues and challenges in developing countries. International Journal of Sexual Health, 22(3), 131–143.
Desrosiers, A., Betancourt, T., Kergoat, Y., Servilli, C., Say, L., & Kobeissi, L. (2020). A systematic review of sexual and reproductive health interventions for young people in humanitarian and lower-and-middle-income country settings. BMC Public Health, 20(1), 666. https://doi.org/10.1186/s12889-020-08818-y
Eryando, T. (2022). Spatial analysis for enhancing the use of health data availability from different sources to help the decision-making process. Kesmas: Jurnal Kesehatan Masyarakat Nasional (National Public Health Journal), 17(3), 165–168.
Eyeberu, A., Lami, M., Bete, T., Yadeta, E., Negash, A., Balcha, T., Sertsu, A., Birhanu, B., Alemu, A., Meseret, F., & Getachew, T. (2023). Risky sexual behavior and associated factors among secondary school students in Harari regional state: Multicenter study. International Journal of Africa Nursing Sciences, 18, 100520.
Eze, I. I., Mbachu, C. O., Ndubuisi, M. N., Agu, I. C., Ezumah, N., & Onwujekwe, O. (2022). Prevalence and sociodemographic determinants of risky sexual behavior among unmarried adolescents in Southeast Nigeria. International Journal of Medicine and Health Development, 27(2), 176–184.
Fatusi, A. O., & Blum, R. W. (2008). Predictors of early sexual initiation among a nationally representative sample of Nigerian adolescents. BMC Public Health, 8, 1–14.
Fetene, N., & Mekonnen, W. (2018). The prevalence of risky sexual behaviors among youth center reproductive health clinics users and non-users in Addis Ababa, Ethiopia: A comparative cross-sectional study. PLoS ONE, 13(6), e0198657.
Gayawan, E., Egbon, O. A., & Adegboye, O. (2023). Copula based trivariate spatial modeling of childhood illnesses in Western African countries. Spatial and Spatio-Temporal Epidemiology, 46, 100591.
Gayawan, E., Orunmoluyi, O. S., & Adegboye, O. A. (2022). Geostatistical patterns of comorbidity of diarrhea, acute respiratory infection, and stunting among under-five children in Nigeria. Mathematical Population Studies, 29(2), 58–72. https://doi.org/10.1080/08898480.2021.1942654
Held, L., Natário, I., Fenton, S. E., Rue, H., & Becker, N. (2005). Towards joint disease mapping. Statistical Methods in Medical Research, 14(1), 61–82. https://doi.org/10.1191/0962280205sm389oa
Janighorban, M., Boroumandfar, Z., Pourkazemi, R., & Mostafavi, F. (2022). Barriers to vulnerable adolescent girls’ access to sexual and reproductive health. BMC Public Health, 22(1), 2212. https://doi.org/10.1186/s12889-022-14687-4
Knorr-Held, L., & Best, N. G. (2001). A shared component model for detecting joint and selective clustering of two diseases. Journal of the Royal Statistical Society Series A: Statistics in Society, 164(1), 73–85.
Kullima, A., Mairiga, A., Gadzama, G., Kawuwa, M., Yusuph, H., & Bako, B. (2015). Seroprevalence of HIV and other sexually transmitted infections (STI’s) among commercial sex workers using lime/lemon juice for vaginal douching. Tropical Journal of Obstetrics and Gynaecology, 32(2), 114–118.
Landry, M., Turner, M., Vyas, A., & Wood, S. (2017). Social media and sexual behavior among adolescents: Is there a link? JMIR Public Health and Surveillance, 3(2), e7149.
Lindgren, F., Rue, H., & Lindström, J. (2011). An explicit link between Gaussian fields and Gaussian Markov random fields: The stochastic partial differential equation approach. Journal of the Royal Statistical Society Series B: Statistical Methodology, 73(4), 423–498.
Marston, M., Beguy, D., Kabiru, C., & Cleland, J. (2013). Predictors of sexual debut among young adolescents in Nairobi’s informal settlements. International Perspectives on Sexual and Reproductive Health, 39(1), 22.
Mbachu, C. O., Agu, I. C., Eze, I., Agu, C., Ezenwaka, U., Ezumah, N., & Onwujekwe, O. (2020). Exploring issues in caregivers and parent communication of sexual and reproductive health matters with adolescents in Ebonyi state. Nigeria. BMC Public Health, 20(1), 1–10.
Mirzaei, M., Ahmadi, K., Saadat, S.-H., & Ramezani, M. A. (2016). Instruments of high risk sexual behavior assessment: A systematic review. Materia Socio-Medica, 28(1), 46.
Mokdad, A. H., Forouzanfar, M. H., Daoud, F., Mokdad, A. A., El Bcheraoui, C., Moradi-Lakeh, M., Kyu, H. H., Barber, R. M., Wagner, J., Cercy, K., Kravitz, H., Coggeshall, M., Chew, A., O’Rourke, K. F., Steiner, C., Tuffaha, M., Charara, R., Al-Ghamdi, E. A., Adi, Y., & Murray, C. J. (2016). Global burden of diseases, injuries, and risk factors for young people’s health during 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet, 387(10036), 2383–2401.
Ndagijimana, E., Biracyaza, E., & Nzayirambaho, M. (2023). Risky sexual behaviors and their associated factors within high school students from Collège Saint André in Kigali, Rwanda: An institution-based cross-sectional study. Frontiers in Reproductive Health, 5, 1029465.
Nigeria, I. (2019). Nigeria Demographic and Health Survey 2018. Abuja, Nigeria, and Rockville. In NPC and ICF Maryland.
Ochen, A. M., Chi, P. C., & Lawoko, S. (2019). Predictors of teenage pregnancy among girls aged 13–19 years in Uganda: A community based case-control study. BMC Pregnancy and Childbirth, 19(1), 211. https://doi.org/10.1186/s12884-019-2347-y
Odii, A., Atama, C. S., Igwe, I., Idemili-Aronu, N. J., & Onyeneho, N. G. (2020). Risky sexual behaviours among adolescent undergraduate students in Nigeria: Does social context of early adolescence matter? The Pan African Medical Journal, 37, 188–188.
Odimegwu, C., & Somefun, O. D. (2017). Ethnicity, gender and risky sexual behaviour among Nigerian youth: An alternative explanation. Reproductive Health, 14, 1–15.
Olugbenga-Bello, A., Adebimpe, W., & Abodunrin, O. (2009). Sexual risk behaviour among in-school adolescents in public secondary schools in a Southwestern City in Nigeria. International Journal of Health Research, 2(3), 243–251.
Omisore, A., Oyerinde, I., Abiodun, O., Aderemi, Z., Adewusi, T., Ajayi, I., Fagbolade, T., & Miskilu, S. (2022). Factors associated with risky sexual behaviour among sexually experienced undergraduates in Osun State. Nigeria. African Health Sciences, 22(1), 41–50.
Onasoga, O., Aluko, J., Adegbuyi, N., Filade, O., & Shittu, H. (2020). Influence of social media use on sexual behaviour of undergraduate students in Ilorin, Kwara State. Nigeria. Interdisciplinary Journal of Education, 3(2), 112–122.
Owoaje, E. T., & Uchendu, O. C. (2009). Sexual risk behaviour of street youths in south west Nigeria. East African Journal of Public Health, 6(3), 274–279.
Puplampu, A. E., Afagbedzi, S., Dery, S., Puplampu, D. A., & Guure, C. (2021). Determinants of higher-risk sexual behavior in some selected African countries. Scientifica, 2021(1), 8089293.
Raheel, H., Mahmood, M. A., & BinSaeed, A. (2013). Sexual practices of young educated men: Implications for further research and health education in Kingdom of Saudi Arabia (KSA). Journal of Public Health, 35(1), 21–26.
Ritchwood, T. D., Hughes, J. P., Jennings, L., MacPhail, C., Williamson, B., Selin, A., Kahn, K., Gómez-Olivé, F. X., & Pettifor, A. (2016). Characteristics of age-discordant partnerships associated with HIV risk among young South African women (HPTN 068). Journal of Acquired Immune Deficiency Syndromes, 72(4), 423.
Seff, I., Steiner, J. J., & Stark, L. (2021). Early sexual debut: A multi-country, sex-stratified analysis in sub-Saharan Africa. Global Public Health, 16(7), 1046–1056.
Simpson, D., Rue, H., Riebler, A., Martins, T. G., & Sørbye, S. H. (2017). Penalising model component complexity: A principled, practical approach to constructing priors. Statistical Science, 32(1), 1–28.
Starrs, A. M., Ezeh, A. C., Barker, G., Basu, A., Bertrand, J. T., Blum, R., Coll-Seck, A. M., Grover, A., Laski, L., Roa, M., Sathar, Z. A., Say, L., Serour, G. I., Singh, S., Stenberg, K., Temmerman, M., Biddlecom, A., Popinchalk, A., Summers, C., & Ashford, L. S. (2018). Accelerate progress—sexual and reproductive health and rights for all: Report of the Guttmacher—Lancet—Commission. The Lancet, 391(10140), 2642–2692. https://doi.org/10.1016/S0140-6736(18)30293-9
Tarkang, E. E. (2015). Sexual risk behaviours of high school female learners in Mbonge subdivision of rural Cameroon. The Pan African Medical Journal, 20, 49–49.
Tarkang, E. E., Lutala, P. M., & Dzah, S. M. (2019). Knowledge, attitudes and practices regarding HIV/AIDS among senior high school students in Sekondi-Takoradi metropolis, Ghana. African Journal of Primary Health Care and Family Medicine, 11(1), 1–11.
Tarkang, E. E., Pencille, L. B., Dadah, E., Nzegge, M. M., & Komesuor, J. (2018). Highly prevalent at-risk sexual behaviours among out-of-school youths in urban Cameroon. Pan African Medical Journal, 30(1), 254.
Tenkorang, E. Y. (2022). Condom use and HIV/AIDS among young people in Edo State. Nigeria. Youth & Society, 54(3), 501–522.
Tuoyire, D. A., Anku, P. J., Alidu, L., & Amo-Adjei, J. (2018). Timing of first sexual intercourse and number of lifetime sexual partners in sub-Saharan Africa. Sexuality & Culture, 22, 651–668.
Ugoji, F. (2014). Determinants of risky sexual behaviours among secondary school students in Delta State Nigeria. International Journal of Adolescence and Youth, 19(3), 408–418.
UNAIDS. (2021). Young people and HIV. https://www.unaids.org/sites/default/files/media_asset/young-people-and-hiv_en.pdf
Visalli, G., Picerno, I., Vita, G., Spataro, P., & Bertuccio, M. P. (2014). Knowledge of sexually transmitted infections among younger subjects of the city of Messina (Sicily). Journal of Preventive Medicine and Hygiene, 55(1), 17–22.
Watsi, L., & Tarkang, E. E. (2020). Demographic determinants of risky sexual behaviours among senior high school students in the Hohoe municipality, Ghana. PAMJ-Clinical Medicine, 2(81).
World Health Organization (WHO). (2019). Sustainable development goals. World Health Organization. Retrieved 25 October from https://www.who.int/sdg/targets/en/
World Health Organization (WHO). (2023). Sexually transmitted infections (STIs). World Health Organization (WHO). Retrieved 21 October from https://www.who.int/news-room/fact-sheets/detail/sexually-transmitted-infections-(stis)
World Health Oragnization (WHO). (2023). Adolescent health. World Health Organization (WHO). Retrieved 21 Oct from https://www.who.int/health-topics/adolescent-health#tab=tab_1
Yaya, S., & Bishwajit, G. (2018). Age at first sexual intercourse and multiple sexual partnerships among women in Nigeria: A cross-sectional analysis. Frontiers in Medicine, 5, 171.
Zhang, X.-D., Temmerman, M., Li, Y., Luo, W., & Luchters, S. (2013). Vulnerabilities, health needs and predictors of high-risk sexual behaviour among female adolescent sex workers in Kunming. China. Sexually Transmitted Infections, 89(3), 237–244.
Author information
Authors and Affiliations
Contributions
Conceptualization: Abdul-Aziz Seidu, Faith O. Alele, Bunmi S. Malau-Aduli, Oyelola Adegboye; Methodology: Abdul-Aziz Seidu, Faith O. Alele, Bunmi S. Malau-Aduli, Oyelola Adegboye; Formal analysis and investigation: Abdul-Aziz Seidu, Olamide Seyi Akeboi, Oyelola Adegboye; Writing—original draft preparation: Abdul-Aziz Seidu, Oyelola Adegboye; Writing—review and editing: Abdul-Aziz Seidu, Faith O. Alele, Bunmi S. Malau-Aduli, Oyelola Adegboye; Supervision: Bunmi S. Malau-Aduli.
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that there is no conflict of interest.
Ethical Approval
No ethical approval required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Seidu, AA., Alele, F.O., Akeboi, O.S. et al. Bayesian Multivariate Spatial Modelling of Risky Sexual Behaviour Among Young People in Nigeria. Spat Demogr 12, 4 (2024). https://doi.org/10.1007/s40980-024-00125-z
Accepted:
Published:
DOI: https://doi.org/10.1007/s40980-024-00125-z