
Abstract
Cardiovascular disease (CVD) is one of the most serious health issues and the leading cause of death worldwide in both developed and developing countries, including Brazil. However, CVD mortality rates are not uniformly distributed across the country. Brazil is marked by important regional differences resulting from socioeconomic inequality and limited access to health services. Mortality varies in a number of dimensions including age, sex, race, socioeconomic status, educational level and geography/space. Geographic inequalities in mortality in Brazil appear to be greater than other countries in Latin America. Given the spatial distribution of causes and heterogeneity of deaths from cardiovascular disease in Brazil, both at macro and micro levels, the goal of this paper is to evaluate the spatial patterns of deaths from CVD in the adult population (over 30 years of age), by sex, in Brazilian micro-regions from 1996 to 2015. Our main contribution was to study an important cause of death in small areas (micro-regions), taking into consideration space, as a proxy of socioeconomic conditions, access to health care and social norms that might affect CVD, as an important variable to understand changes in the CVD mortality.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Cardiovascular disease (CVD) is one of the most serious health issues and the leading cause of death worldwide in both developed and developing countries (Roth et al. 2017a, b). However, levels, the rates and the risk of mortality in all populations depend on several factors such as, age structure, income (GDP), education, behavior, climate, access to health services, and epidemiological conditions (Timaeus 1993; Lopez et al. 1995, 2006a, b; Vallin and Meslé 2004; Jerrett et al. 2005; Marmot 2010; WHO 2014).
The absolute number of deaths from CVD and circulatory diseases is increasing at the global level (Lozano et al. 2012; Roth et al. 2015) and in the last twenty-five years increased from 12,334,351.16 to 17,273,017.16. In 1990 the deaths from CVD represented 26.50% of all causes of deaths, whereas in 2015 the burden of cardiovascular mortality represented about 31.90%. In the same period, the neoplasms, which are the second leading cause of death worldwide, increased from 12.25 to 16.16%. Meanwhile, diarrhea, lower respiratory tract infection, and other common infectious diseases (the third largest cause of mortality) decreased from 17.36 to 9.02% (IHME 2017). In Brazil the deaths from CVD represent the leading cause of death in the population. While the number of deaths from CVD increased from 258,338.97 in 1990 to 363,474.38 in 2015, the percentage has remained fairly stable, 28.89% and 28.82%, respectively (IHME 2017).
However, regional disparities in the distribution of health-disease patterns among countries are very important (Reddy and Yusuf 1998; Yusuf et al. 2001a, b; WHO 2014; Roth et al. 2015). While some low-income countries still show the occurrence of communicable diseases (diarrhea, lower respiratory, HIV/AIDS, tuberculosis and other common infectious diseases), in others, especially developed countries and those at an advanced stage of the epidemiologic transition process, the prevalence of chronic non-communicable diseases (NCDs) is observed, in particular, cancers and cardiovascular diseases. Also, in several Latin American and South Asian countries, there is still a high prevalence of infectious diseases and rapid increase of chronic diseases (Frenk et al. 1996).
These regional disparities also apply to sub-national populations within a specific country. Therefore, regardless of the level of development, stage of the epidemiological transition, or age composition, the fact is that the geographical variation in cardiovascular mortality is not uniform within the country (Reddy and Yusuf 1998; Lotufo 2000; Yusuf et al. 2001a, b; Mansur et al. 2002; Dyakova et al. 2008; Asaria et al. 2012; Nowbar et al. 2014; Rasella et al. 2014; Barbieri et al. 2015; Guimarães et al. 2015; Borges 2017; Brant et al. 2017; Chen et al. 2017; Roth et al. 2017; Baptista et al. 2018).
In Brazil, CVD mortality rates are not uniformly distributed across the country (Borges 2017; Baptista et al. 2018). Brazil is marked by important regional differences resulting from socioeconomic inequality and limited access to health services (Souza et al. 2018). Due to the spatial distribution of causes and spatial heterogeneity of mortality in general, and more specifically, of cardiovascular disease in Brazil, at both a macro and micro level, the goal of this paper is to identify and to analyze the spatial patterns of deaths from cardiovascular disease in the adult population (over 30 years of age), by sex, in Brazilian micro-regions from 1996 to 2015. We will use a combination of demographic techniques and spatial autocorrelation methods to investigate temporal and spatial evolution of cardiovascular diseases in the country.
Levels of mortality by cardiovascular diseases are far from homogeneous across subpopulations in Brazil. The experience of the country as a whole does not necessarily reflect the experience of individual subgroups or population subgroups. Mortality varies in a number of dimensions including age, sex, race, socioeconomic status, educational level and geography/space. Geographic inequalities in adult mortality in Brazil appear to be greater than other countries in Latin America. Along with varying mortality levels, regions within Brazil also have vastly different experiences in terms of environmental exposures, disease control, medical treatment and care, and behavioral risk (Fenelon 2013; Brant et al. 2017; França et al. 2017; Roth et al. 2017; Baptista et al. 2018).
We use spatial statistical analysis to identify recent patterns of CVD mortality in Brazil and also discuss possible future trends in the country (Hecht 2014). In general, mortality studies in Brazil focus on the whole country, specific areas, or the states. There are very few studies dealing with smaller areas, but there has been an increase in interest in these approaches in recent years (Roth et al. 2017; Schmertmann and Gonzaga 2018; Lima and Queiroz 2014). Therefore, by using spatial analysis of mortality from cardiovascular diseases, we want to know where these deaths occur, how they relate to other variables (sex, age, among others), what it all means, and what actions we could take. “That’s why whenever we look at maps, we inherently start turning them into instruments for making decisions” (Hecht 2014).
2 Background
Câmara et al. (2004) argues that understanding the spatial distribution of data from phenomena occurring in space constitutes today a great challenge for the elucidation of central issues in several areas of knowledge. Demography has begun to use and seek more and more the help of spatial analysis as a way of understanding and explaining some of the issues present in the core of this science (Langford and Unwin 1994; Messner and Anselin 2004; Sampson and Morenoff 2004; Weeks 2004; Jerrett et al. 2005; Castro 2007; Yang et al. 2009; Journal of Spatial Demography 2013). Weeks (2004) and Castro (2007) argue that space is a crucial element in demographic studies. Demography is inherently a spatial science because it almost always deals with human populations in a defined geographic region (Weeks 2004). Demographers, as well as geographers and others, often try to measure how “everything is related to everything else”Footnote 1 by looking at connections between pairs of locations or entities. However, spatial analysis has still played a small role in the development of demographic theory. According to Weeks (2004), there are several reasons for this, including the recent character of many spatial statistical approaches, and the fact that many people studying Demography do not “belong” to geography and therefore were not encouraged to think spatially. However, even in geography, few are those who study population and who adopt spatial approaches that go beyond measures of movement of people from one place to another or comparisons of demographic trends between different regions. The author complements and affirms that “demography is not only spatial, but it is also by nature interdisciplinary”. Raymer et al. (2018) argue that spatial demography should focus on studying population dynamics and change across space. We argue that this paper contributes to the field by studying mortality differentials by cardiovascular disease over time and across space in a less developed country.
In recent years, there has been an increasing interest in identifying regional differences in mortality across and within countries. Barbieri et al. (2015) analyze regional adult mortality trends in the US from 1959 to 2004. They show that the decline of mortality at the end of the 1960s was unexpected, but also generalized and driven by the decline of CVD mortality. In the same direction, Roth et al. (2017) estimate age-standardized mortality rates from CVD among US counties between 1980 and 2014 and find extensive spatial disparity. They observe large differences across counties in rates of mortality from ischemic heart disease and stroke. They also find smaller differences for other diseases such as myocardial disease, atrial fibrillation, aortic and peripheral arterial disease, rheumatic heart disease, and endocarditis. Asaria et al. (2012) examine the trends in age-standardized CVD mortality in all 7932 electoral districts in England between 1982 and 2006. The results indicate that at the national level the “CVD mortality declined by about two-thirds for men and women aged 30–64 years between 1982 and 2006 and by over one-half for those aged > 65 years”. At the level of electoral districts, the age-standardized CVD mortality declined in most districts, but in 186 of them this rate increased for women aged over 65 years. The drop was more pronounced where the initial mortality was higher. Finally, Yusuf et al. (2001a, b)describe the variations in CVD by specific region of the world or ethnic group (European origin, Japanese, Chinese, South Asians, Hispanics, Aboriginal Populations and Blacks of African Origin—Africa, West Indies, US). They explore information about differences in the age-standardized mortality rates among men and women, risk factors and prevention, and point out that cardiovascular disease is a health problems across countries and that there is a strong correlation between urbanization and increases in the risk of cardiovascular related mortality.
In Brazil the studies of cardiovascular diseases that adopt a demographic and spatial approach are still scarce (Baptista et al. 2018). In general, the focus is on epidemiological and public health aspects and the studies target the entire country, major geographic regions (Southeast, Northeast, etc.), or very specific counties (Souza et al. 2001; Mansur et al. 2002; Ishitani et al. 2006; Melo et al. 2006; Godoy et al. 2007; Rasella et al. 2014; Guimarães et al. 2015; Brant et al. 2017; Borges 2017). Therefore, there is an absence and need for studies investigating the variation of mortality from cardiovascular disease, taking both time frame and spatial factors into consideration. Borges (2017) examines health and mortality transitions across regions in Brazil. The author finds rapid decline in infant mortality across regions of the country and increase in the participation of chronic diseases. One main finding is the regional variation in the improvement of mortality from cardiovascular diseases; faster declines are observed in the Southern regions of the country. Souza and colleagues (2001) analyzed, by sex and age, the risk of death due to cardiovascular, cardiac ischemic, and cerebrovascular diseases between 1979 and 1996 in the 5 Brazilian geographic regions. The study showed that the “risk of death significantly increased in the central western region and decreased in the southeastern and southern regions of the country. In the northern region, a trend toward stability was observed, and, for some age brackets, a slight decline was seen”. In summary, there was an increase in CVD mortality in the less developed regions (Center-West, North and Northeast) and a reduction in the more developed (Southeast and South). A study also using the 5 Brazilian geographic regions was conducted by Guimarães et al. (2015), estimating mortality from ischemic heart disease and cerebrovascular disease between 1980 and 2012. The authors highlight a regional variation between proportional mortality coefficients and point out that “in general, in relation to the regions, the Southeast and the South had the highest coefficients of mortality for the two groups of diseases, and the North and Northeast regions showed the lowest rates”. Brant et al. (2017) analyzed the variations of CVD mortality rates and their peculiarities between 1990 and 2015 in Brazil and in Brazilian states. They point out that there was a reduction in mortality rates, although these have not been uniform among Brazilian states, “being higher (above 40%) in the southeastern and southern regions of the country and in the Federal District. In contrast, the lowest reductions occurred in the northern and northeastern regions”, where socioeconomic conditions are worse. The paper also highlights the differences between the sexes, where, where “mortality due to CVDs tends to reduce first among women”. Finally, Rasella et al. (2014) evaluate the possible impacts of Brazil’s Family Health Program (FHP) on CVD mortality (heart and cerebrovascular disease) throughout the first decade of this century in 1622 Brazilian municipalitiesFootnote 2 with vital statistics of adequate quality. They point out that the FHP “coverage is associated with a reduction in hospitalizations and mortality from heart and cerebrovascular disease causes in Brazil. Moreover, its effect increases according to the duration of FHP’s implementation in the municipality”. In addition, they discovered a negative association between the FHP “and mortality rates from in both unadjusted and adjusted models for demographic, social, and economic confounders”. Additionally, the implementation of the Family Health Program “increased the number of health education activities, domiciliary visits, and medical consultations” that might have positive impact on the reduction of mortality. However, population dynamics might affect the increase in the absolute number of deaths by CVD. As this cause of mortality is more specific to older age groups, as population ages one needs to know whether the reduction in mortality compensates for the change in population age structure.
Understanding the heterogeneity in the distribution of causes of deaths across regions and time in Brazil is important to developing better public health interventions and to explaining the variation and differentials in life expectancy at birth in the country, since regional differences are also reflecting difference in other risk factor such population age structure, access to health care, quality of hospital care and variations in risk behavior. The purpose of this paper is to study deaths from cardiovascular diseases in time (1996–2015) and space (micro-regions). This paper contributes to the literature by focusing on small areas of a very diverse country and taking into consideration space as an important variable to understand changes in the CVD mortality.
3 Data and Methods
3.1 Study Population, Level of Analysis and Information Source
We use cause-specific mortality from cardiovascular disease from the Tenth Revision of the International Classification of Diseases (ICD-10), Chapter IX, publicly available in the Sistema de Informações sobre Mortalidade (SIM), DATASUS, which was created by the Brazilian Ministry of Health in 1975 (www.datasus.gov.br). The data are organized by sex (males and females), age (population over 30 years and in 5-year groups up to 80 years or more) and cause of death, as well as by the geographical micro-region where the deceased resided. For purposes of analysis, we use four 5-year periods 1996–2000, 2001–2005, 2006–2010 and 2011–2015. Population data organized by age and sex were obtained from the 2000 and 2010 Censuses and intercensal estimates from the Brazilian Institute of Geography and Statistics (IBGE).Footnote 3
The units of analysis are the 558 Brazilian micro-regions, as proposed by the Brazilian Institute of Geography and Statistics (IBGE). The micro-regions are statistical constructions aggregated using regional and socioeconomic similarities, i.e., geographic micro-regions do not constitute political or administrative entities. One of the advantages of using this type of unit is that their boundaries are constant throughout the research period. Thus, it was possible to monitor and study the 558 areas between 1996 and 2015. Furthermore, it is assumed that there is internal homogeneity within the micro-regions, that is, significant changes only occur on the borders.
3.2 Limitations
In Brazil, mortality studies are limited by poor data quality (Hill 1987; Luy 2010; Queiroz et al. 2017; Schmertmann and Gonzaga 2018). In addition, another common limitation of mortality studies is the underreporting of deaths available in the vital statistics of these countries (Mathers et al. 2005; Luy 2010; Lima et al. 2014; Queiroz et al. 2017). Parallel to this, Brazil is an extremely heterogeneous country with regard to social, economic, cultural and demographic dimensions. The same can be said of the great differences in the quality of vital statistics across Brazilian regions (Paes 2005; França et al. 2008; Agostinho 2009; Lima and Queiroz 2014; Queiroz et al. 2017; Schmertmann and Gonzaga 2018). As a result of this heterogeneity, the analysis requires greater attention and effort on the part of policy makers to improve and propose solutions to these issues.
In this paper, we will use estimates of underreporting of death counts produced by Lima and Queiroz (2014), specifically those using the “Adjusted Synthetic Extinct Generations (SEG-adj)” method proposed by Hill et al. (2009). Lima and Queiroz (2014) present estimates of the degree of coverage by meso-regions by using the methods of “Synthetic Extinct Generations—SEG” (Bennett and Horiuchi 1981), “General Growth Balance—GGB” (Hill 1987), and “adjusted Synthetic Extinct Generations—SEG-adj” (Hill et al. 2009). Since the literature does not indicate the best method for correction of death underreporting, we used the SEG-adj method because it is considered, in general, to be more robust than others.Footnote 4
These estimates relate to all causes of death. Thus, a strong assumption of this study is that there is no significant difference between the pattern of mortality observed in the study of these authors, using all causes of death, and the patterns in this study that refer only to those people who died from cardiovascular disease (Murray and Lopez 1996; Lopez et al. 2006a, b), i.e., the possible underreporting found in deaths from cardiovascular diseases will be fixed, taking as a basis all causes of death.
A second limitation is the quality of causes of death registration. To analyze mortality trends in the whole country, it is crucial to bear in mind the regional differences in coverage of the official health statistics system, and particularly the proportion of ill-defined deaths (França et al. 2008). Historically, the North and Northeast states have had lower coverage and worse quality of the death declarations, compared to Southeast and South states. However, since the 2000s, there has been an impressive improvement in both conditions. The better quality of mortality information in the North/Northeast changed the mortality trends radically, mainly due to non-communicable diseases. We are using data from 1996 to 2015. Several papers argue and show that the quality of information has improved since then, allowing proper comparison across regions (Guimarães et al. 2015; Borges 2017).
We are also concerned with the high percentage of unreported information found in the data from the Sistema de Informações sobre Mortalidade (SIM) on socioeconomic variables. This invalidates any analysis that intends to use variables such as income, education and race, for example. Thus, this paper will be limited to the study of demographic variables such as gender and age, which, by themselves, will make a meaningful contribution to the studies on cardiovascular mortality in Brazil (Castanho et al. 2001; Ribeiro et al. 2016; Brant et al. 2017; França et al. 2017).
3.3 Spatial Autocorrelation
The spatial autocorrelation can be calculated by global and/or local indexes of spatial association. These indexes characterize the relative distribution of events observed in different regions with the objective of finding spatial patterns or verifying if the data are randomly distributed. These two statistics are differentiated by the unit of analysis, being that the global ones consider the general spatial tendency of the events and the locals specify where the agglomerations (clusters) or extreme cases occur. In this paper, specifically, local spatial autocorrelation will be used, and local Moran’s I may be given by (Anselin 1995):
where zi and zj are deviations from the mean; the value wij is the weight assigned to areas i and j; the scalar c is the same for all locations, i.e., does not play a role in the estimate of significance. “The latter is obtained by means of a conditional permutation method, where, in turn, each zi is held fixed, and the remaining z-values are randomly permuted to yield a reference distribution for the statistic” (Anselin 1995).
The local spatial autocorrelation index allows for comparison of the values of a variable in each area with the values found in its neighbors. That is, this type of “local analysis” or “local modeling” disaggregates global statistics according to their local constituents, focusing more on local specificities than on the search for global regularities. The local indicators of spatial autocorrelation produce a specific value for each object, thus allowing the identification of clusters of objects with values of similar attributes, outliers and more than one spatial regime. For Anselin (1995), the LISA (Local Indicators of Spatial Association) must satisfy two criteria: (1) have the ability, for each observation, to indicate statistically significant spatial clusters; and (2) the property that the sum of local indicators for all regions should be proportional to the corresponding global spatial autocorrelation indicator.
As examples of local indicators of spatial autocorrelation, we have the Cluster Map and Moran scatter plot (local Moran’s I statistic). The Cluster Map presents sites with local statistical significance of Moran “with the significant locations color coded by type of spatial autocorrelation” (Anselin 2005). The red color represents what is called high–high, that is, observations with values above the average, with their neighbors also above the average. It will occupy the first quadrant in the Moran scatter plot. Already those below the average, with their neighbors in the same situation, are in the third quadrant (low–low) and are represented by the blue color. Both high–high and low–low are considered spatial clusters, thus defined as positive local spatial autocorrelation (Anselin 2005). The second (low–high) and fourth (high-low) quadrants of the Moran scatter plot are occupied, respectively, by observations with values below the average surrounded by neighbors with values above the average (light blue color) and places with values above the average surrounded by neighbors with low values (pink color). These two are regarded as spatial outliers, hence, defined as negative local spatial autocorrelation. If there is no spatial autocorrelation, the observations will be randomly distributed.
To implement this methodology, we used GeoDa software. This generated the LISA indicators, through Univariate Local Moran’s I, which were mapped. In the software, a neighborhood structure between the micro-regions called Queen was also defined. This criterion correlates the micro-regions with their neighbor independent of their direction. The level of significance used in this paper was 1%. In other words, this is the percentage of error likely to say that the spatial distribution is not random. Data is publicly available, but we provide full access to all estimates used in this paper on GitHub (https://github.com/blanza).
4 Results
The methodology used in this paper shows us how an analysis based on the verification of the existence of spatial autocorrelation can clarify the relative distribution of the observed events in space. In the next figures, we present Lisa Cluster maps for all periods of analysis. In each figure, we identify the correlation between cardiovascular disease deaths and the clusters with high or low mortality due to cardiovascular diseases found in Brazil during the study period. Cluster detection is an important tool because it can help to identify factors associated with cardiovascular disease. We also highlight the connection between the Moran scatter plot and the Lisa Cluster maps.
Anselin (1996) points out that the “Moran scatter plot consists of a plot with the spatially lagged variable on the y-axis and the original variable on the x-axis. The slope of the linear fit to the scatter plot equals Moran’s I”. Moran’s I gives a global statistic. So, it is known that there is clustering going on in the research area, but we do not know exactly where or how. To investigate further, one can make a Local Indicators of Spatial Association (LISA). This test not only tests for regional clustering, it can also show the presence of significant spatial clusters or outliers by micro-region. In addition, the Moran scatter plot provides an allocation of spatial association into four classes (high–high, low–low, low–high and high-low), “corresponding to the location of the points in the four quadrants of the plot”. These classes are relative to the mean of the variable, which is the center of the graph, and should not be interpreted in a consummate sense. “It is important to keep in mind that there is a difference between a location (and its spatial lag) being in a given quadrant of the plot, and that location being a significant local cluster or spatial outlier” (Anselin 2005).
The Moran’s I result (Figs. 1 and 2) showed that there was spatial dependence in all periods and for both sexes. The first period (1996–2000) showed the highest Moran’s I values (0.7413 for male and 0.7057 for female). In the next two periods (2001–2005 and 2006–2010) Moran’s I values decreased for both sexes. However, in the last period Moran’s I values increased again (0.550041 and 0.505538 for male and female, respectively).

Moran scatter plot for deaths from cardiovascular diseases in the adult population, males, micro-regions, Brazil—5-year periods 1996–2000(top left), 2001–2005(top right), 2006–2010(bottom left) and 2011–2015(bottom right)

Moran scatter plot for deaths from cardiovascular diseases in the adult population, females, micro-regions, Brazil—5-year periods 1996–2000(top left), 2001–2005(top right), 2006–2010(bottom left) and 2011–2015(bottom right)
For better understanding of the Moran scatter plot, we use women (Fig. 2) for the period 1996–2000 (top left) as an example. The plot shows a linear fit through the point cloud. The slope of this line corresponds to Moran’s I = 0.705775 and p value = 0.01. To avoid distorting the data, we can see that both axes have the same units. Thus, the points in the graph are somewhat balanced, because it is rendered as a square. The CVD mortality rates are on the horizontal axis, and their spatially lagged counterparts on the vertical axis. Note that the CVD mortality rate values have been standardized, where the mean is 0 and the standard deviation is 1. Similarly, the spatial lag is computed for those standardized values. We can see still that the shape of the point cloud is determined by the presence of some outliers. One observation (micro-region of Amapá—first quadrant) is as large as 4 standard deviational units above the mean. “Finally, we can select points in each of the quadrants (highlighted by the dashed lines) and identify locations in the map associated with each of the four types of spatial autocorrelation” (Anselin 2005).
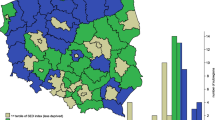
In parallel to this, the LISA function is very useful because it can create the global statistics in graphic form along with the local statistics. Figure 3, focusing on males, and Fig. 4, on females, the high–high spatial clusters, that is, micro-regions with high CVD mortality rates, with neighboring micro-regions in the same situation, generally have the same spatial pattern, although in lesser quantity (micro-regions) for women. Initially (1996–2000), these clusters were concentrated in the Southeast (São Paulo, Rio de Janeiro and Minas Gerais) and Southern (Rio Grande do Sul, Santa Catarina and Paraná) regions. Later (2001–2005), the clusters move to the Center-West (Mato Grosso do Sul and Mato Grosso, in particular) and North (Pará and Tocantins) regions, although the state of Rio de Janeiro (Southeast) still presents a concentration of high–high clusters. In the following periods (2006–2010 and 2011–2015), clusters are concentrated in the North (Pará and Tocantins) and Northeast (Maranhão and Piauí) regions, with some representation still in the Center-West (male population in 2006–2010) and Amapá in the last period (men). It is observed, therefore, that during the period there was a reduction in the high–high spatial clusters. Brant et al. (2017) argues that socioeconomic improvements and health policies are important factors explaining the observed variation across regions and over time in the country. Socioeconomic status was also an important factor to explain the deaths from CVD in studies in Australia (Bagheri et al. 2015) and Strasbourg, France (Kihal-Talantikite et al. 2017). In both, the authors show that populations with high risk for CVD trend to concentrate in economically deprived areas.

LISA cluster map for deaths from cardiovascular diseases in the adult population with direct standardization data, males, micro-regions, Brazil—5-year periods 1996–2000 (a), 2001–2005 (b), 2006–2010 (c) and 2011–2015 (d)

LISA cluster map for deaths from cardiovascular diseases in the adult population with direct standardization data, females, micro-regions, Brazil—5-year periods 1996–2000 (a), 2001–2005 (b), 2006–2010 (c) and 2011–2015 (d)
We find that low–low spatial clusters, that is, micro-regions with low CVD mortality rates, with neighboring micro-regions in the same situation, seem to move “clockwise” to high–high spatial clusters. In the period 1996–2000, the low–low spatial clusters are concentrated in the North (Amazonas and Pará) and Northeast (Maranhão, Piauí, Ceará, Rio Grande do Norte, Paraiba, Pernambuco, Alagoas, Sergipe and Bahia) regions. In a way, the pattern described above repeats for the period 2001–2005, although in some states of the Northeast the cluster representativeness decreases. Already in the period 2006–2010 the low–low spatial clusters are grouped basically in the states of Amazonas (North), Bahia (Northeast) and Minas Gerais (Southeast). Finally, in the last period (2011–2015) the clusters are still concentrated in the states of Amazonas (North), Bahia (Northeast), Minas Gerais and São Paulo (Southeast), Rio Grande do Sul and Santa Catarina (South). These are gains that need to be carefully considered, since they may be related to the under-enumeration of death when declared in the census or underreporting of deaths available in the vital statistics of these states, especially because, for the most part, they are socioeconomically poor regions within the states themselves.
Regarding spatial outliers (low–high and high-low), they are the negative spatial autocorrelation (Anselin 2005), i.e., they imply that the rates for CVD mortality tend to be dissimilar from their neighboring areas; these do not present a spatial configuration over the analyzed period when adopted a level of significance of 1%. Already in the micro-regions where it reads “not significant” (without color/white), the spatial dependence, from a geographic perspective, was not significant for the current selection of the p value, i.e., 0.01 in our paper.
5 Discussion
The study of demographic and epidemiological changes in any population depends directly on the quality of mortality information (Paes 2007; França et al. 2008; Lima et al. 2014). In Brazil one of the main constraints to adult mortality studies is the underreporting of the basic events in the available vital statistics. Thus, to obtain adequate estimates of the level and pattern of mortality, it is essential to evaluate and, when necessary, correct the quality of death information (Luy 2010). In the case of regions within the country, there are also significant differences in the quality of vital statistics (Agostinho 2009; Queiroz and Lima 2011; Queiroz et al. 2017; Schmertmann and Gonzaga 2018), due to the heterogeneity of the mentioned aspects, which highlights the need for greater attention and effort on the part of policy makers to propose and improve on solutions to these issues. In this sense, our first task was to use estimates of underreporting of deaths counts, from 1980 to 2010 by small areas, produced by Lima and Queiroz (2014), to obtain adequate estimates of the level and pattern of mortality to the Brazilian micro-regions and then study the pattern of CVD mortality over time and space.
In a second stage, we use spatial analysis models to verify the existence of spatial autocorrelation that could help to understand the relative distribution of the observed events in space. The results show that there was a decrease in high–high spatial clusters—micro-regions with high CVD mortality rates, with neighboring micro-regions in the same situation—for both men and women over the period analyzed in the micro-regions of both the Southeast and South regions, notably the most developed regions of the country. We speculate that new information regarding the fall in cardiovascular mortality rates can be explained in part by the improvement in education and health conditions of the population, in premature diagnoses regarding cardiovascular risks and in the search for a better quality of life (Ribeiro et al. 2012; Rasella et al. 2014). On the other hand, the micro-regions of the Center-West, North and Northeast regions, in general, have seen an increase in mortality rates over the years. We hypothesize that the explanation for this may be contrary to the aspects mentioned for micro-regions located in the Southeast and South regions, but it is also necessary to consider the increase in life expectancy of the populations of these regions, the increase in the prevalence of cardiovascular risk factors, as well as the improvement of their death registration and vital statistics, as highlighted by Mathers et al. (2005), França et al. (2008), Luy (2010), Freire et al. (2014).
However, we consider that there is still an important and significant variation in deaths from cardiovascular diseases in time and space due to the country’s state of development, represented by regional, socioeconomic or epidemiological disparities, by improvements in the access to and quality of health services in the last decades, and risk factors, taking into account the increase in the life expectancy of the average Brazilian (Ribeiro et al. 2012; Rasella et al. 2014).
Souza et al. (2001) and Guimarães et al. (2015) analyzed the deaths from CVD, more specifically mortality from ischemic heart disease and cerebrovascular disease, for the five Brazilian geographic regions. They highlight a regional variation observed in the country. While Souza et al. (2001) show that between 1979 and 1996 there was an increase in CVD mortality in the less developed regions (Center-West, North and Northeast) and a reduction in the more developed (Southeast and South), Guimarães et al. (2015) point out that “in general, in relation to the regions, the Southeast and the South had the highest coefficients of mortality for the two groups of diseases, and the North and Northeast regions showed the lowest rates” between 1980 and 2012. This information maintains temporal and spatial consistency with our findings, although the periods, especially the study by Souza et al. (2001), are not similar. However, these studies are important to maintain temporal continuity with our analysis, since they allow us to visualize the trajectory of CVD mortality over the last 35 years in Brazil, albeit at a more macro spatial level. Borges (2017) finds that changes in CVD mortality have had an important impact in reducing overall mortality levels for females in the Southern regions of the country, but benefited older adults in all regions. Malta et al. (2014) argues that improvements in life conditions and public health programs played a significant role in the reduction of CVD mortality.
Brant et al. (2017) analyzed the variations of CVD mortality rates and their peculiarities between 1990 and 2015 in Brazil and in Brazilian states. They point out that there was a reduction in mortality rates, although these have not been uniform among Brazilian states, “being higher (above 40%) in the southeastern and southern regions of the country and in the Federal District. In contrast, the lowest reductions occurred in the northern and northeastern regions”, where socioeconomic conditions are worse. The authors also highlight the differences between the sexes, where “mortality due to CVDs tends to reduce first among women”.
In our study the high–high spatial clusters also show this tendency by showing a smaller number of micro-regions in every 5-year period when compared to men. More interestingly, we observed a clock-wise change in the regional profile of high–high clusters over time. In the early period (1996–2000) of analysis, there was a concentration in the Southern part of the country that moved to the interior of the northeast in the last period (2011–2015).
6 Conclusion
Our main contribution was to study an important cause of death in small areas (micro-regions). This helps to understand the dynamics of the health transition in Brazil in a recent period of time and has positive impacts on public health policies. Our results are in line with others that focus on states or major regions of the country, but we provide results for small regions. Mortality by cardiovascular diseases are related to population age structure, health conditions, institutional factors, the environment and the socioeconomic situation to which the population is exposed. Brazil is marked by large socioeconomic differences with strong relations to regional diversities. These relations offer possibilities for targeted public interventions, but at the same time present challenges, which a country of continental dimensions cannot avoid. Brazilian health-system planning needs an understanding of the absolute burden of cardiovascular disease and the effect of population aging. For example, regions with a declining incidence of cardiovascular diseases may still need to invest heavily in health promotion and treatment given trends in population age structure that might increase the number of deaths from this specific cause. In recent years, the decline in CVD is very related to the decline in risk factors by the individuals that are associated to policies such as tobacco control and better preventive care to high blood pressure (França et al. 2017; Brant et al. 2017). However, quality of hospital care plays an important role in the declining trend and there are large regional differences in the quality (Brant et al. 2017; Ribeiro et al. 2016).
The results might help to investigate associated factors that can explain recent changes in mortality by cardiovascular diseases, and other causes, and to understand regional differences in life expectancy and health status across regions in Brazil. Regional trends of early mortality by cardiovascular diseases should be carefully analyzed, seeking a better definition of the strategies for the realities of different regions of the country. In addition, this study serves as a powerful stimulus to integrate spatial analysis and demography in the study of mortality, in this specific case, CVD mortality. The knowledge and analysis of the variations in deaths from cardiovascular diseases in time and space is of fundamental importance to promote actions with regard to health, and to propose and plan public health policies in a localized and effective way.
Notes
Tobler’s First Law of Geography (1970) states that: “Everything is related to everything else, but near things are more related than distant things”.
In 2010 there were 5565 municipalities in Brazil.
IBGE. http://www.ibge.gov.br.
References
Agostinho, C. S. (2009). Estudo sobre a mortalidade adulta, para Brasil entre 1980 e 2000 e Unidades da Federação em 2000: uma aplicação dos métodos de distribuição de mortes. In Tese de Doutorado. Tese (Doutorado em Demografia)–Centro de Desenvolvimento e Planejamento Regional (p. 243). Universidade Federal de Minas Gerais, Belo Horizonte.
Anselin, L. (1995). Local indicators of spatial association—LISA. Geographical Analysis, 27, 91–115.
Anselin, L. (1996). The moran scatterplot as an ESDA tool to assess local instability in spatial association. In Manfred Fischer, Henk Scholten, & David Unwin (Eds.), Spatial analytical perspectives on GIS in environmental and socio-economic sciences (pp. 111–125). London: Taylor and Francis.
Anselin, L. (2005). Exploring spatial data with GeoDa: a workbook. Revised version April 21, 2018. In Center for spatially integrated social science. University of Illinois, Urbana-Champaign. Available in: http://www.csiss.org.
Asaria, P., Fortunato, L., Fecht, D., Tzoulaki, I., Abellan, J. J., Hambly, P., et al. (2012). Trends and inequalities in cardiovascular disease mortality across 7932 English electoral wards, 1982–2006: Bayesian spatial analysis. International Journal of Epidemiology, 41(6), 1737–1749.
Bagheri, N., et al. (2015). Community cardiovascular disease risk from cross-sectional general practice clinical data: a spatial analysis. Preventing Chronic Disease, 12, 140379.
Baptista, E. A., Queiroz, B. L., & Rigotti, J. I. R. (2018). Decomposition of mortality rates from cardiovascular disease in the adult population: a study for Brazilian micro-regions between 1996 and 2015. Revista Brasileira de Estudos de População. https://doi.org/10.20947/s102-3098a0050
Barbieri, M., Ouellette, N., Andreeva, M., Riffe, T., & Vinant, C. (2015). The cardiovascular revolution in the United States: a geographic analysis. Presented at the Annual Meeting of the Population Association of America, San Diego, California, May 2–4. https://paa2015.princeton.edu/papers/153514
Bennett, N. G., & Horiuchi, S. (1981). Estimating the completeness of death registration in a closed population. Population Studies, 47(2), 207–221.
Borges, G. M. (2017). Health transition in Brazil: regional variations and divergence/convergence in mortality. Cadernos de Saúde Pública, 33(8), E00080316.
Brant, L. C. C., Nascimento, B. R., Passos, V. M., Duncan, B. B., Bensenõr, I. J., Malta, D. C., et al. (2017). Variations and particularities in cardiovascular disease mortality in Brazil and Brazilian states in 1990 and 2015: estimates from the global burden of disease. Revista Brasileira de Epidemiologia., 20, 116–128.
Câmara, G., Monteiro, A. M., Druck, S., & Carvalho, M. S. (2004). Análise espacial e geoprocessamento. In G. Câmara, A. M. Monteiro, S. Druck, & M. S. Carvalho (Eds.), Análise espacial de dados geográficos. Distrito Federal: Planaltina.
Castanho, V. S., Oliveira, L. S., Pinheiro, H. P., Oliveira, H. C., & De Faria, E. C. (2001). Sex differences in risk factors for coronary heart disease: a study in a Brazilian population. BMC public health, 1(1), 3.
Castro, M. C. (2007). Spatial demography: an opportunity to improve policy making at diverse decision levels. Population Research and Policy Review, 26(5–6), 477–509.
Chen, W. W., Gao, R. L., Liu, L. S., et al. (2017). China cardiovascular diseases report 2015: a summary. Journal of Geriatric Cardiology: JGC, 14(1), 1–10. https://doi.org/10.11909/j.issn.1671-5411.2017.01.012.
Dyakova, M., Shipkovenska, E., Dyakov, P., Dimitrov, P., & Torbova, S. (2008). Cardiovascular risk assessment of bulgarian urban population: cross-sectional study. Croatian Medical Journal, 49(6), 783–791.
Fenelon, A. (2013). Geographic divergence in mortality in the United States. Population and development review, 39(4), 611–634.
França, E. B., et al. (2008). Evaluation of cause-of-death statistics for Brazil, 2002–2004. International Journal of Epidemiology, 37(4), 891–901.
França, E. B., et al. (2017). Cause-specific mortality for 249 causes in Brazil and states during 1990–2015: a systematic analysis for the global burden of disease study 2015. Population Health Metrics, 15(1), 39.
Freire, F. H. M. A., Souza, F. H., Queiroz, B. L., Lima, E. E. C., & Gonzaga, M. R. (2014). Tabelas de sobrevivência para os municípios brasileiros em 2010: análise espacial do padrão e nível de mortalidade. In Encontro nacional de estudos populacionais: População, Governança e Bem-Estar, 24 a 28 de novembro de 2014/São Pedro, SP: ABEP, 2014.19. São Pedro, São Paulo. https://www.abep.org.br/publicacoes/index.php/anais/article/viewFile/2122/2078
Frenk, J., Bobadilla, J. L., & Lozano, R. (1996). The epidemiological transition in Latin America. Adult Mortality in Latin America, 123, 485–496.
Global Burden of Disease Collaborative Network. (2017). Global burden of disease study 2016 (GBD 2016) Results. Seattle, United States: Institute for Health Metrics and Evaluation (IHME). Available from http://ghdx.healthdata.org/gbd-results-tool.
Godoy, M. F., Lucena, J. M., Miquelin, A. R., Paiva, F. F., Oliveira, D. L., Augustin Junior, J. L., et al. (2007). Mortalidade por doenças cardiovasculares e níveis socioeconômicos na população de São José do Rio Preto, Estado de São Paulo, Brasil. Arquivos Brasileiros de Cardiologia, 88(2), 200–206.
Guimarães, R. M., et al. (2015). Regional differences in cardiovascular mortality transition in brazil, 1980 to 2012. Revista Panamericana de Salud Pública, 37(2), 83–89.
Hecht, L. (2014). Understanding the power of spatial analysis. Available from https://blogs.esri.com/esri/esri-insider/2014/10/17/understanding-the-power-of-spatial-analysis/. Access in: June 26, 2018.
Hill, K. (1987). Estimating census and death registration completeness. Asian and Pacific Census Forum, 1(3), 8–13.
Hill, K., You, D., & Choi, Y. (2009). Death distribution methods for estimating adult mortality: sensitivity analysis with simulated data errors. Demographic Research, 21(9), 235–254.
Ishitani, L. H., et al. (2006). Desigualdade social e mortalidade precoce por doenças cardiovasculares no Brasil. Rev Saúde Pública, 40(4), 684–691.
Jerrett, M., et al. (2005). Spatial analysis of air pollution and mortality in Los angeles. Epidemiology, 16(6), 727–736.
Journal of Spatial Demography (2013). Available from: http://spatialdemography.org/. Access in: March 03, 2014.
Kihal-Talantikite, W., et al. (2017). Developing a data-driven spatial approach to assessment of neighbourhood influences on the spatial distribution of myocardial infarction. International Journal of Health Geographics, 16, 017–0094.
Langford, M., & Unwin, D. J. (1994). Generating and mapping population density surfaces within a geographical information system. Cartographic Journal, 31, 21–25.
Lima, E. E. C., & Queiroz, B. L. (2014). Evolution of the deaths registry system in Brazil: associations with changes in the mortality profile, under-registration of death counts, and ill-defined causes of death. Cadernos de Saúde Pública (ENSP. Impresso), 30, 1721–1730.
Lima, E. E. C., Queiroz, B. L., & Sawyer, D. (2014). Método de estimação de grau de cobertura em pequenas áreas: uma aplicação nas microrregiões mineiras. Cadernos Saúde Coletiva (UFRJ), 22, 409–418.
Lopez, A. D., et al. (1995). Adult mortality in developed countries: from description to explanation. Oxford: Oxford University Press.
Lopez, A. D., et al. (2006a). Measuring the global burden of disease and risk factors, 1990–2001. Global Burden of Disease and Risk Factors, 1, 1–14.
Lopez, A. D., et al. (2006b). Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. The Lancet, 367(9524), 1747–1757.
Lotufo, P. A. (2000). Mortalidade pela doença cerebrovascular no Brasil. [Stroke: mortality rates in Brazil]. Rev Bras Hiperten, 7(4), 387–391.
Lozano, R., Naghavi, M., Foreman, K., et al. (2012). Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the global burden of disease study 2010. Lancet, 2012(380), 2095–2128.
Luy, M. A. (2010). Classification of the nature of mortality data underlying the estimates for the 2004 and 2006 united nations’ world population prospects. Comparative Population Studies, 35(2), 315–334.
Malta, D. C., Moura, L., Prado, R. R., Escalante, J. C., Schmidt, M. I., & Duncan, B. B. (2014). Mortalidade por doenças crônicas não transmissíveis no Brasil e suas regiões, 2000 a 2011. Epidemiol Serv Saúde, 2014(23), 599–608.
Mansur, A. P., Souza, M. F., Timerman, A., & Ramires, J. A. (2002). Trends of the risk of death due to circulatory, cerebrovascular and ischemic heart disease in 11 Brazilian capitals from 1980 to 1998. Arquivos Brasileiros de Cardiologia, 79, 269–284.
Marmot, M. (2010). Fair society, healthy lives. In M. Marmot (Ed.), Strategic review of health inequalities in England post-2010. London: Department of Health.
Mathers, C. D., Ma Fat, D., Inoue, M., Rao, C., & Lopez, A. D. (2005). Counting the dead and what they died from: an assessment of the global status of cause of death data. Bulletin of the Word Health Organization, 83(3), 171–179.
Melo, E. C. P., Carvalho, M. S., & Travassos, C. (2006). Distrituição espacial da mortalidade por infarto agudo do miocárdio no Município do Rio de Janeiro. Brasil. Cadernos de Saúde Pública, 22(6), 1225–1236.
Messner, S. F., & Anselin, L. (2004). Spatial analyses of homicide with areal data. Spatially integrated social science., 12, 127–144.
Ministério Da Saúde. Sistema de Informações sobre Mortalidade (SIM). Disponível em: http://www2.datasus.gov.br/DATASUS/index.php?area=0205 [acesso em 22 Março 2018].
Murray, C. J. L., & Lopez, A. D. (1996). Estimating causes of death: new methods and global and regional applications for 1990. In C. J. L. Murray & A. D. Lopez (Eds.), The global burden of disease: a comprehensive assessment of mortality and disability from diseases, injuries, and risk factors in 1990 and projected to 2020 (pp. 117–200). Harvard: Harvard School of Public Health.
Nowbar, A. N., Howard, J. P., Finegold, J. A., Asaria, P., & Francis, D. P. (2014). Global geographic analysis of mortality from ischaemic heart disease by country, age and income: statistics from World Health Organisation and United Nations. International Journal of Cardiology, 174(2), 293–298.
Paes, N. A. (2005). Avaliação da cobertura dos registros de óbitos dos estados brasileiros em 2000. Revista de Saúde Pública, 39(6), 882–890.
Paes, N. A. (2007). Qualidade das estatísticas de óbitos por causas desconhecidas dos Estados brasileiros. Revista de Saúde Pública, 41(3), 436–445.
Queiroz, B. L., & Lima, E. E. C. (2011). The road towards better vital registration systems: under-registration of death counts and ill-defined causes of death in Brazil. In The lancet global health metrics and evaluation conference controversies, innovation, accountability, 2011, Seattle.
Queiroz, B. L., et al. (2017). Completeness of death-count coverage and adult mortality (45q15) for Brazilian states from 1980 to 2010. Revista Brasileira de Epidemiologia, 20, 21–33.
Rasella, D., et al. (2014). Impact of primary health care on mortality from heart and cerebrovascular diseases in Brazil: a nationwide analysis of longitudinal data. BMJ, 349, 4014.
Raymer, J., Willikens, F., & Rodgers, A. (2018). Spatial demography: a unifying core and agenda for further research. Population, Space and Place. https://doi.org/10.1002/psp.2179.
Reddy, K. S., & Yusuf, S. (1998). Emerging epidemic of cardiovascular disease in developing countries. Circulation, 97(6), 596–601.
Ribeiro, A. G., Cotta, R. M. M., & Ribeiro, S. M. R. (2012). A promoção da saúde e a prevenção integrada dos fatores de risco para doenças cardiovasculares. Ciência & Saúde Coletiva, 17, 7–17.
Ribeiro, A. L. P., Duncan, B. B., Brant, L. C., Lotufo, P. A., Mill, J. G., & Barreto, S. M. (2016). Cardiovascular health in Brazil: trends and perspectives. Circulation, 133(4), 422–433.
Roth, G. A., et al. (2015). Demographic and epidemiologic drivers of global cardiovascular mortality. New England Journal of Medicine, 372(14), 1333–1341.
Roth, G. A., et al. (2017a). Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. Journal of the American College of Cardiology, 70(1), 1–25.
Roth, G. A., et al. (2017b). Trends and patterns of geographic variation in cardiovascular mortality among US counties, 1980–2014. JAMA, 317(19), 1976–1992.
Sampson, R. J., & Morenoff, J. D. (2004). Spatial (dis)advantage and homicide in Chicago neighborhoods. In M. F. Goodchild & D. G. Janelle (Eds.), Spatially integrated social science (pp. 145–170). Oxford, England: Oxford University Press.
Schmertmann, C. P., & Gonzaga, M. R. (2018). Bayesian estimation of age-specific mortality and life expectancy for small areas with defective vital records. Demography, 55(4), 1363–1388.
Souza, M. D. F. M. D., et al. (2001). Trends in the risk of mortality due to cardiovascular diseases in five Brazilian geographic regions from 1979 to 1996. Arquivos Brasileiros de Cardiologia, 77(6), 569–575.
Souza, M. D. F. M. D., et al. (2018). Changes in health and disease in Brazil and its States in the 30 years since the unified healthcare system (SUS) was created. Ciencia & Saude Coletiva, 23(6), 1737–1750.
Timaeus, I. M. (1991). Measurement of adult mortality in less developed countries: a comparative review. Population Index, 57(4), 552–568.
Timaeus, I. M. (1993). Adult mortality. In K. A. Foote, K. H. Hill, & L. G. Martin (Eds.), Demographic change in Sub-Saharan Africa (pp. 218–255). Washington (D.C.): National Academy Press.
Tobler, W. R. (1970). A computer movie simulating urban growth in the detroit region. Economic Geography, 46, 234–240.
Vallin, J., & Meslé, F. (2004). Convergences and divergences in mortality. A new approach to health transition. Demographic Research, Special Collection, 2(2), 11–44.
Weeks, J. R. (2004). The role of spatial analysis in demographic research. In M. F. Goodchild & D. G. Janelle (Eds.), Spatially integrated social science (pp. 381–399). New York: Oxford University Press.
World Health Organization—Noncommunicable Diseases (NCD) Country Profiles. (2014).
Yang, T.-C., Teng, H.-W., & Haran, M. (2009). The impacts of social capital on infant mortality in the US: a spatial investigation. Applied Spatial Analysis and Policy, 2(3), 211–227.
Yusuf, S., Reddy, S., Ôunpuu, S., & Anand, S. (2001a). Global burden of cardiovascular diseases: part I: general considerations, the epidemiologic transition, risk factors, and impact of urbanization. Circulation, 104(22), 2746–2753.
Yusuf, S., Reddy, S., Ôunpuu, S., & Anand, S. (2001b). Global burden of cardiovascular diseases: part II: variations in cardiovascular disease by specific ethnic groups and geographic regions and prevention strategies. Circulation, 104(23), 2855–2864.
Funding
Financial support from CNPq, Project “Estimating Mortality by causes in small areas in Brazil” - 421183/2018-7.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Baptista, E.A., Queiroz, B.L. Spatial Analysis of Mortality by Cardiovascular Disease in the Adult Population: A Study for Brazilian Micro-Regions Between 1996 and 2015. Spat Demogr 7, 83–101 (2019). https://doi.org/10.1007/s40980-019-00050-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40980-019-00050-6