
Abstract
Despite the greatest onset and increased frequency of suicidal or self-harm behavior occurring in adolescence, most youth affected do not receive professional care. Family-based intervention offers a promising treatment for this population, however, there is much to learn about the barriers and facilitators to effective care and the tailoring of treatment necessary to meet youth and family needs. Such insights can be sourced from a growing qualitative literature reporting the views of young people and their caregivers affected by suicidality and self-harm. This systematic review analyzes qualitative research to synthesize the perspectives of these youth and their caregivers about their needs for and experiences of professional help. Following a search of 4 databases, 35 studies were analyzed using Consensual Qualitative Research methods. Barriers to effective care were identified at individual, family, and systems levels. Young people and their caregivers experienced fractured relationships and overwhelming emotions that impeded engagement, increased young people’s distress and suicidality, and reduced parenting efficacy. Systemic barriers to care included insufficient, fragmented, and inaccessible services, and stigmatizing or dismissive responses from healthcare providers. In contrast, effective professional care was timely, non-judgmental, collaborative, and included separate and joint sessions for youth and caregivers to address their individual needs and foster relationship repair. This review’s findings support the value of family-based treatment that pro-actively addresses stigma and highlight the need for increased services that are structured to facilitate therapeutic engagement from crisis through recovery.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Despite decades of prevention programs, rates of youth suicide and self-harm remain alarmingly high (Curtin, 2020), and most young people affected by suicidal behavior do not receive professional care (Rowe et al., 2014). Clinical trials show family-based treatment to be a promising intervention for youth suicidal behavior (Glenn et al., 2019; Iyengar et al., 2018) however, to increase treatment engagement and improve the tailoring of professional care, it is crucial to develop a greater understanding of the experiences and views of youth and their caregivers affected by suicidal or self-harm behavior. The present study addresses this research gap by systematically reviewing the qualitative literature to synthesize the perspectives of this population on professional care needed or experienced.
Youth self-harm and suicide rates are at concerning levels despite prevention efforts (Curtin, 2020). Suicide is the second leading cause of death for youth in the USA (Center for Disease Control, 2020; Ivey-Stephenson et al., 2020) and internationally (World Health Organization, 2019). As the greatest onset and increased frequency of self-harm and suicidal behavior occur in adolescence, prevention and treatment at this developmental stage are crucial (Valencia-Agudo et al., 2018). Across different samples and contexts, between 10.5% (Kokkevi et al., 2012) and 17% (Liu et al., 2018) of adolescents report having attempted suicide, and self-reported youth self-harm ranges from 17% (Swannell et al., 2014) to 31.3% (Aggarwal et al., 2017), thus representing a significant proportion of young people. Among high school youth surveyed in the USA, 7.4% said they had attempted suicide at least once during the previous 12 months, and up to 26.1% had made a suicide plan (Kann et al., 2018). Health intervention for young people affected by self-harm or suicidal behavior is imperative to relieve associated health, social, and educational burdens (Glenn et al., 2019), and because these youth are at the most significant risk of subsequent suicide death (Liu et al., 2018; Olfson et al., 2018).
However, most youth affected by suicidal behavior do not receive mental health treatment (Michelmore & Hindley, 2012; Rowe et al., 2014). Youth self-report studies found only 30% to 45% of those who had attempted suicide subsequently accessed professional support (Slovak & Singer, 2012; Wu et al., 2010). Youth with mental health problems generally have low help-seeking rates (Velasco et al., 2020), and young people with more severe suicidal symptoms are less likely to seek help than those with milder mental health concerns (Armiento et al., 2014; Berger et al., 2013). Among suicidal or self-harming youth who do access treatment, up to half drop out prematurely (Brent et al., 2013; Glenn et al., 2015). Therefore, increasing engagement and treatment retention are essential priorities for the prevention of youth suicide and self-harm (Ougrin et al., 2015).
Family-based treatment is a promising intervention for youth affected by suicidal behavior. Although clinical trials of treatments for suicidal adolescents are mostly small-scale and with a single site (Glenn et al., 2019; Zalsman et al., 2016), systematic reviews of such trials identify several characteristics common to promising treatments. These characteristics include mandated family or caregiver involvement in treatment (Calear et al., 2016; Iyengar et al., 2018), a focus on enhancing the coping skills of youth and caregivers (Glenn et al., 2019), strengthening youth-caregiver relationships (Brent et al., 2013; Glenn et al., 2015), the delivery of treatment over several weeks or more (Glenn et al., 2019), and having higher intensity treatment at the start of care (Brent et al., 2013). Of promising treatments, only adapted Dialectical Behavior Therapy-Adolescent (DBT-A), incorporating strong family systems elements and the aforementioned characteristics, has been independently replicated (Glenn et al., 2019; Iyengar et al., 2018). Notably, some interventions were only effective for reducing suicidal or self-harm behavior when family or parent components were added (Calear et al., 2016; Glenn et al., 2015), and family-based treatment appears to be associated with higher levels of treatment engagement (Curtis et al., 2018; Iyengar et al., 2018).
Extensive research into the role of family relationships and attachment with caregivers in youth suicidality provides theoretical support for family-based treatment (Ewing et al., 2015). Supportive connections with caregivers and family contribute to resilience, and improvements in this attachment relationship have been associated with sustained reductions in suicidal behavior (Czyz et al., 2012). Family dynamics that are predictive of suicidal events include family conflict (Wagner & Wagner, 2012), low cohesion and family stress (Ewing et al., 2015), poor parent–child connection (Cruz et al., 2014), and family-related loneliness (Giletta et al., 2012). Given the empirical and theoretical support for family-based treatment, it is important to examine the professional care needed and experienced through a family systems lens, considering both youth and caregiver perspectives.
There is a growing qualitative literature reporting the views of young people and their caregivers affected by suicidal behavior, including rich data about their emotional experience, the caregiver-youth relationship, access to effective care, and their perspectives on professional help. This literature presents an opportunity to address the gaps in knowledge about treatment approaches that engage young people and their families affected by suicidal behavior or self-harm (Ougrin et al., 2015). Previous systematic reviews of the qualitative literature concerning young people affected by suicidal or self-harm behavior have highlighted the significance of family influences for suicidality and recovery (Grimmond et al., 2019; Lachal et al., 2015), that some youth describe their self-harm relationally, as attempting to communicate or connect (Stänicke et al. 2018), the need for more research on youth experiences of professional care (Lindgren et al., 2018), the impact of shame as a barrier to accessing help (Curtis et al., 2018; Grimmond et al., 2019), and potential benefits of intervention to improve caregiver-youth communication and support (Curtis et al., 2018). However, there is a gap in the research with a lack of studies focusing specifically on family-based treatment experienced or wanted or examining the qualitative literature from a family intervention lens.
Current Study
It is crucial to listen to the voices of young people and their caregivers affected by suicidal or self-harm behavior to better understand their needs and drive appropriate professional care however, systematic reviews to date have not examined the available qualitative literature from a family intervention perspective, despite the promising support for family-based treatment. The present study addresses this gap by systematically reviewing and synthesizing qualitative research reporting the views of young people and their caregivers affected by suicidal or self-harm behavior from a family systems lens to inform how to increase engagement and improve the tailoring of treatment to meet their individual and family needs. To this end, the study considers how young people and their caregivers describe their experience of suicidality and self-harm, the challenges they faced individually and within the context of family relationships, their views on professional help needed, barriers and facilitators to accessing effective help, and helpful or unhelpful aspects of intervention experienced.
Method
The procedure for searching, selecting, appraising the quality, and synthesizing the findings was based on the ENTREQ statement’s steps (Tong et al., 2012) and the Consensual Qualitative Research (CQR) approach (Hill, 2012). CQR involves multiple researchers in all research stages and analysis, with the data being discussed together until a consensus is reached about the findings. Transparency between the raw data and the conclusions drawn is facilitated by extracting direct quotes and describing each theme’s prominence in the presentation of the data.
Selection Criteria
Following a preliminary literature review, the selection criteria were refined through an iterative process. An initial literature search for qualitative research with a primary focus on family-based treatment experiences for adolescents (12–18 years) affected by suicidal or self-harm behavior found no studies. Selection criteria were subsequently broadened as follows:
-
1.
age extended to include youth (12–25 years) or their parents/caregivers;
-
2.
studies with comments on needs or help wanted (in addition to professional help experienced); and,
-
3.
studies with participants’ views on the impact of family relationships on a young person’s suicidality or recovery.
The intersection of these selection criteria is shown in Fig. 1. Implications for policy and family-based treatment for this group are identified from the data drawn from these broadened criteria.

Selection criteria for the systematic review
Search and Selection Strategy
An exhaustive search strategy was pursued to yield a large sample of studies for review. Published research from Jan 1, 1994, to Apr 20, 2020, was searched across Medline, PsycINFO, CINAHL, and Embase. Primary search terms were combined using Boolean operators AND OR. Terms included adolescent (youth; child; young person) AND suicide (suicide attempt; self-harm; suicidal ideation; suicidal behavior) AND treatment (counseling; family therapy; family treatment; psychotherapy; risk assessment; intervention) AND qualitative experience (lived experience; perspectives; views). A complete set of search terms is contained in Supplementary Table S2.
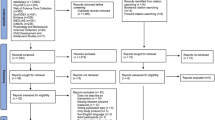
The selection process is shown in Fig. 2. A total of 4,320 items was retrieved from the initial database search. Following removal of duplicates and screening by title, 320 articles remained. A further 18 articles were added from hand searching other reviews and the reference lists of articles, resulting in 338 articles for abstract review. Ninety-six articles were included for full-text review, and of these, 35 met the selection criteria. One author (DS) conducted the screening of articles by title and abstract. Two authors (DS and IGS) independently screened articles by full text, resolving any disagreements regarding selection through discussion. Articles were excluded based on participant characteristics (e.g., age, community, or professionals’ surveys), methodology (e.g., not qualitative), the nature of publication (e.g., not written in English) and focus (e.g., lacking any comment about family relationships or help wanted or experienced).

PRISMA Flowchart
Quality Appraisal
The quality of studies was evaluated by two authors (DS and KM) using the Critical Appraisal Skills Program (CASP, 2019). The Cochrane collaboration recommends the CASP measure (Noyes et al., 2021), and it is used widely in systematic qualitative reviews (Lachal et al., 2017). No study was excluded based on its CASP ratings.
Data Analysis and Synthesis
CQR informed the analysis of qualitative studies. Two authors (DS and IGS) independently analyzed the 35 included articles, reading each in full, summarizing key themes, and recording extensive direct quotes from participants in relation to each theme. These authors then compared their initial data analysis and jointly developed a single list of themes and sub-themes with exemplar quotes. The list of themes was further refined in consultation with other authors (IS and KM), and the final themes and sub-themes are shown in Tables 2, 3, 4. The prominence of each theme is indicated using the terms recommended by the CQR method, with “General” indicating that a theme was unanimously or near-unanimously referenced; “Typical” indicating that the theme was present in the majority; and “Variant” indicating a theme with some, but less than majority agreement (Hill et al., 2005). All authors jointly conducted a higher-level analysis of the data, categorized themes into overarching domains, and discussed key findings and their implications.
Results
No articles with a primary focus on the lived experience of family-based treatment were retrieved during the literature search. Thirty-five articles met the expanded selection criteria and are shown in Table 1, incorporating the views of 342 young people and 183 caregivers across 11 countries. Studies varied in sample size (from 3 to 68 with a median of 12) and location (with 44% of studies conducted in Europe, 36% in North America, 6% in both Asia and Australia, and 3% each from Africa and Central America). The gender of participants, where specified, was overwhelmingly female (85% of youth and 86% of caregivers), as shown in Table 5 in Appendix. While many studies did not identify the participants’ racial, cultural or linguistic background, when stated, most participants were of Caucasian background, 11% of studies had Hispanic or Latina participants, 9% had participants of Asian backgrounds, and 3% (1) had Native American participants. Most studies (80%) used one-on-one interviews, while 9% used focus groups, and a further 9% used both surveys and interviews.
Overall, the studies were of good quality. All had clear aim statements, clear findings, were appropriate for qualitative methodology, and constituted valuable research. Almost all studies had research designs appropriate to their aims (97%), appropriate recruitment (89%), and appropriate data collection strategies (94%). However, only a minority of studies (29%) demonstrated consideration of the relationship between the researcher and the participants (i.e., reflexivity). The CASP ratings for each study are shown in Supplementary Table S3.
Participants’ descriptions were categorized into two major domains. The first, “Fractured Relationships”, focused on the quality of family relationships and the lived experience of suicidality or self-harm within the family systems context. Themes within this domain included reports from young people and their caregivers of overwhelming emotions and a sense of disconnection or conflict and how this contributed to the young person’s suicidality and reduced parenting efficacy. The second domain, “Professional help wanted or experienced”, focused on healthcare experiences and aspects of treatment identified as critical to engagement and recovery, or conversely, unhelpful to engagement and recovery. This domain included participants’ descriptions of professional help they had wanted or experienced, barriers to accessing support, helpful and unhelpful aspects of professional care, and family-based treatment experiences. Changes in family relationships perceived as helpful and the role of professional help in facilitating such change, if applicable, were also described. The themes in each domain and their inter-relationships are represented in Figs. 3 and 4. The themes, along with example quotes, are shown in Tables 2, 3 and 4.

Domain one: Fractured relationships

Domain two: Professional help wanted or experienced
Fractured Relationships
A general theme for youth was the experience of overwhelming emotions such as hopelessness and shame, accompanied by an acute sense of isolation and disconnection. Young people typically spoke of concealing their distress and suicidal or self-harm behavior, which further intensified their isolation. Together with a fear of adverse reactions or judgment, shame and hopelessness often impeded young people from sharing their thoughts of suicide or self-harm and asking others for help.
When discussing family relationships before treatment, young people generally felt unable or unwilling to communicate their distress or ask caregivers for support. Reasons for doing so included shame, concern about their parents’ reactions, a lack of hope that parents could or would help, and a prevailing sense of disconnection in the relationship, e.g., “Our relationship is a boat and it’s got holes in it and we’re both trying to haul out the water,” (Tingey et al., 2014, p. 1522). In addition, many young people also described a longing for support and for their distress to be acknowledged by their caregivers. They typically reported making indirect cries for help that were not heard and left them feeling misunderstood or not cared about. Some also described their suicidal behavior as attempting to resolve a relationship impasse, or seeking affirmation that others cared about them, e.g., “I wanted to try killing myself. I wanted to know if anyone would be sorry if I died or if anyone wanted me” (Sukhawaha et al., 2016, p. 337).
A variant to typical theme referenced in youth studies was young people’s experience of caregivers’ adverse responses when their suicidality or self-harm was eventually disclosed. These negative responses included being dismissed and ignored, e.g., “any time I displayed any signs of it in my home it was wrote off or I was told I was being foolish” (Bostik & Everall, 2006, p. 281), or experiencing angry, punitive, or abusive reactions. Family relationship problems were described as typically directly triggering or worsening the young person’s suicidality. Family conflict, rejection, criticism, abuse, or feeling unloved were among the reasons listed for self-harm or suicide attempts.
Overwhelming and wide-ranging emotions in response to discovering their child’s suicidality or self-harm were general themes in caregiver studies. The most cited emotions parents and caregivers reported were shame, guilt, and powerlessness, and they also described feeling shock, denial, confusion, anger, grief, and fear. These feelings, and the idea that self-harm could only happen in a sick family, made it harder for caregivers to access support from either professional or informal sources. Adverse reactions from others intensified their sense of isolation, e.g., one parent reported, “It can be very lonely… you can tell everybody, but people will then cross the road to avoid talking to you” (Ferrey et al., 2016b, p. 4). Panic, fear, and pervasive worry about the risk of future suicidal behavior were typical experiences for caregivers, impacting them personally and affecting family relationships. The young person’s suicidal behavior was typically experienced as a relationship rupture. Many caregivers expressed grief and sadness about changes in the relationship, while variant themes described by caregivers included a sense of rejection, betrayal, anger, or rage towards their child.
Reduced parenting efficacy was a general theme. The discovery of their child’s suicidality or self-harm shattered caregivers’ confidence in parenting, and they felt unsure about how to help their son or daughter. A loss of trust and ease in the relationship was fueled by pervasive worry about future suicidal behavior. Parents typically felt they were “walking on eggshells” and being hypervigilant to maintain safety and supervision (Oldershaw et al., 2008, p. 142). Caregivers also discussed problems navigating normal adolescent-parent conflict and setting limits. Fear about possible future self-harm led some to oscillate between being overly lenient or restrictive.
Parents’ psychological, family, or socio-economic struggles intensified their sense of powerlessness, e.g., one mother reported, “I can’t do anything to save her in the role of a mom because of I am powerlessness, alcoholic, and poor mom” (Sukhawaha et al., 2016, p. 338), while others spoke of their dismay or despair when their attempts to support their youth seemed to have no positive impact. Another general theme for caregivers was problems in communication with their young person. They found it hard to initiate conversation and felt unsure about what to say and how to give the young person space while maintaining the active supervision and support necessary to be confident that their child was safe. Parents’ own emotional reactions, particularly anxiety, hurt, or anger, typically made it harder to keep the focus on supporting their child, e.g., one parent spoke of “yelling and screaming at her to stop (self-harming)” (Kelada et al., 2016, p. 3407), while other parents spoke about minimizing communication with their young person to avoid emotional or frustrated communication.
Descriptions of Help Wanted or Experienced
There were three main sub-themes explored within participants’ descriptions of the professional help they received or reported wanting to have received. These included the barriers they experienced in accessing effective care, what they described as being effective in the care they received, and the distinct needs of youth and caregivers.
Barriers to Effective Care
Young people and their caregivers typically had problems accessing professional help. Systemic barriers to care included a lack of services or information about how to access services, stigma concerning youth suicidal or self-harm behavior, and the impact of healthcare providers’ stigmatizing responses. Many caregivers and youth said they did not know where and how to get help. A general lack of information about suicidal or self-harm behavior and that it was a problem that could be helped, contributed to this. One parent said, “I got lost, like I was completely on my own trying to figure out who I should get her into…I didn’t feel like there was a good resource” (Kelada et al., 2016, p. 3412).
The impact of shame and fear of judgment was typically experienced as a barrier to professional help. One young person described feeling exposed and vulnerable at the point of help-seeking, “It was really scary... you feel like everybody knows what you’re being there for... it’s like sitting in the waiting room of a doctor’s office and they didn’t give you a gown... just like a total walk of shame.” (Murray & Wright, 2006, p. 159). Adverse or dismissive reactions from health professionals were variant to typical themes. Some youth felt looked down on or judged by some healthcare staff, particularly when seeking help in hospital emergency departments, e.g., “(the clinicians) just look at you with utter disgust like you’re some monster” (Owens et al., 2016, p. 288). They felt staff ignored their needs and treated them as attention-seekers who diverted resources from other patients with more “legitimate” emergency healthcare needs, and they did not feel listened to or understood. Caregivers similarly reported not being included in professional care and feeling judged or blamed by healthcare staff.
Not getting enough help, having to wait for treatment, or receiving fragmented care were typical themes in unhelpful care experienced by youth and caregivers. Some spoke of waiting weeks or months after the suicidal crisis before being offered services. Others commented on not having enough help due to infrequent appointments and a lack of support outside of scheduled sessions.
Fragmentation in the provision of care was another barrier to effective treatment. A typical theme in youth studies was that care involved seeing many different clinicians rather than having the chance to engage with a consistent treating team. This was exemplified in the experience of one young person who felt they had “seen, over the past three years, “about 20 different” counselors, psychiatric nurses, and doctors” (Storey et al., 2005, p. 73). Similarly, young people and caregivers noted problems with coordination between acute and ongoing treatment and falling between the gaps in the referral criteria of available services, leading to them receiving insufficient or fragmented care. One mother stated, “So what are we all doing here? While you’re batting referrals back and forth, I’ve got a child who is cutting herself, becoming more isolated and withdrawn” (Stewart et al., 2018, p. 81).
A lack of transparency from health professionals and being excluded from treatment decisions were typical to general themes. Some youth reported a lack of openness from health professionals, particularly about diagnoses and treatment planning, while a variant youth theme concerned not having enough say about inpatient care, psychotherapy, or pharmacotherapy. Caregivers also described being excluded from treatment planning and intervention even when they had actively instigated it. Despite being given little or no information by treating health professionals about their child’s difficulties, caregivers were expected to be responsible for monitoring the young person’s wellbeing and safety.
Effective Professional Care
When discussed, effective care was typically described as timely and flexible. Helpful, professional support was available as frequently as needed, with clear avenues for crisis support outside scheduled sessions. The crucial nature of relationships with health professionals in facilitating engagement and helpful care was a general theme. Youth and caregivers typically highlighted the importance of open, trusting, and collaborative relationships with health professionals. Being listened to and feeling accepted by clinicians who took time and care to get to know them and understand their concerns was a similarly recurrent theme. As one young person reported, “It (therapy) was beneficial because it was somebody I could come and talk to, and somebody I got familiar with, and somebody I felt comfortable with for the first time.” (Murray & Wright, 2006, p. 161). The benefits of having a say in treatment planning and reviewing progress were also typical themes in both youth and caregiver studies.
Youth and Caregiver Needs
Helpful, professional care was comprehensive and focused on the distinct youth, caregiver, and family-related needs. Young people and caregivers typically wanted individual sessions for themselves, and some interventions focused on joint or relationship work. Caregivers spoke of the need for space and support to manage their own emotions before they felt ready for family therapy. Separate sessions for caregivers were also important for specific advice and guidance on supporting their child and responding to their distress in an emotionally attuned yet containing manner. Interestingly, some young people expressly wanted their caregivers to have individual treatment and felt relieved when this occurred, e.g., one young person noted, “I think that it changed my mom quite a bit; I think my mom started doing different measures of releasing her stress, or even her depression, instead of bottling it up. I think she (the clinician) helped her to do something in a different way, I don’t know but I think she (the clinician) helped our family quite a bit” (Murray & Wright, 2006, p. 160). Youth studies also typically highlighted the importance for young people of having individual sessions, with space to reflect with a clinician who they experienced as caring about them, e.g., “I really had that sense that she honestly did care about me and how I was doing, and she genuinely did want to help me and didn’t mind listening to me when I did talk and if I was blabbing on about something she just sat there and listened” (Bostik & Everall, 2007, p. 88).
Improving the relationship between young people and their parents was identified as a critical aspect of the intervention and a general theme across youth and caregiver studies. For some youth, improved connection with caregivers was identified as the most critical factor in their recovery, e.g., one young woman said, “I realized after I hit rock bottom. I’m not in it alone. I have my mom. My mom loves me” (Holliday & Vandermause, 2015, p. 172). Therapy that fostered dialogue and helped young people talk to their parents about their feelings and support needs, or discuss issues with less conflict, was beneficial and a typical youth theme. Preparation before joint sessions and having choices about these appointments’ focus and timing were also important for young people. While some wanted health professionals to speak to their caregivers on their behalf, others said they wanted their therapist to help them speak to their parents and expressed relief in having joint sessions with a supportive therapist actively involved in these conversations. However, in contrast, two young people reported feeling coerced into family sessions where they felt exposed to family members and burdened by hearing about their parents’ concerns (variant theme).
Discussion
There is a growing qualitative literature reporting on the views of young people and their caregivers affected by suicidal behavior, though past systematic reviews have not specifically examined this through the lens of family therapy intervention, a promising treatment approach. It is vitally important to understand more about the experience of these youth and their caregivers as adolescence is a time of increased onset and frequency of suicidal and self-harm behavior, and most youth do not receive professional care. This systematic review examined the available qualitative literature and identified a range of individual, family, and systemic barriers to treatment, including overwhelming emotions, in particular shame, and disconnection experienced by young people and their caregivers that contributed to their isolation and made it harder to seek help. Systemic barriers included a lack of available services, professional care experienced as fragmented and poorly coordinated, inadequate information about how to access care, and stigmatizing or dismissive responses from healthcare providers. This review supports family-based interventions and highlights the importance of carefully tailoring treatment to the varied and dynamic needs of youth and their caregivers within direct therapeutic processes and at broader policy and systems levels to improve engagement in effective care and outcomes for youth suicidal behavior.
Family Relationships
The core themes identified in this review underscore the importance of attending to family relationships to reduce the risk of suicidal or self-harm behavior and promote recovery. Young people’s descriptions highlighted the role of poor family relationships in contributing to suicidal behavior (e.g., Gulbas et al., 2019) and the positive potential of relationship repair and supportive relationships with caregivers (e.g., Hausmann-Stabile et al., 2018). This is consistent with previous qualitative reviews (Curtis et al., 2018; Grimmond et al., 2019) and research identifying poor attachment/family relationships as risk factors for suicidal behavior and, conversely, supportive relationships as related to resilience and recovery (Ewing et al., 2015). Before recovery, most young people felt unable or unwilling to seek support from their caregivers about their distress or suicidality, feeling disconnected, isolated (Holliday & Vandermause, 2015), rejected, or abused (Zayas et al., 2010). Despite this, a prominent theme in youth accounts was the importance of improved connection with caregivers (e.g., Bostik & Everall, 2007; Wadman, Vostanis, et al., 2018). These findings are consistent with, and strengthen support for, family-based treatments involving relationship repair and enhancing the protective potential of caregiver-youth relationships (Brent et al., 2013; Glenn et al., 2019).
Improving Engagement in Effective Care
Improving engagement in professional care is a critical suicide prevention priority, given that most young people with suicidal ideation or self-harm behavior do not access or complete professional treatment (Rowe et al., 2014). The experience of youth and their caregivers described in this article highlighted barriers to engagement at individual, family, and systems levels. At individual and family levels, overwhelming emotions, shame, isolation, and fractures in family relationships impeded help-seeking. This is consistent with previous research that identified worthlessness, self-loathing, and shame as hindering youth help-seeking (Grimmond et al., 2019), and shame and guilt as impeding help-seeking by caregivers (Curtis et al., 2018).
Also consistent with previous research (Lindgren et al., 2018), a lack of knowledge about self-harm or suicidal behavior, and confusion about the availability or usefulness of professional help, curtailed access to both informal support and professional treatment. Many caregivers reported that they were previously unaware of self-harm and did not know how to get help (Kelada et al., 2016). Young people noted that, while there are “posters all around school (for smoking) …there are actually more people who self-harm than smoke or drink. Have an assembly about self-harming” (McAndrew & Warne, 2014, p. 575). This lends support for increased public education about self-harm and suicidal behavior, as has also been suggested in previous research (Grimmond et al., 2019; Lindgren et al., 2018).
Society-based stigma about self-harm (Mitten et al., 2016), coupled with dismissive or stigmatizing healthcare providers’ responses, were systems-level barriers to professional care. Young people who had self-harmed or were suicidal and their caregivers reported feeling dismissed or judged across healthcare settings (Hausmann-Stabile et al., 2018, Kelada et al., 2016), particularly in hospital emergency departments (Owens et al., 2016). These themes are similar to the negative professional care experiences of adults who self-harm (Lindgren et al., 2018) and highlight the critical importance of the quality of relationships with health professionals in facilitating engagement in effective care.
Finally, consistent with previous research, a fundamental systemic barrier to effective care engagement was the lack of available services (Grimmond et al., 2019; Lachal et al., 2015). Waitlists (Rissanen et al., 2009a), being turned away from services (Stewart et al., 2018), and insufficient or fragmented care were all identified as issues (Keladaet al., 2016; Wadman, Vostanis, et al., 2018). Problems in getting help after a crisis, difficulties in transitions between services, and the lack of consistent care providers also contributed to fragmented care experiences (Stewart et al., 201; Storey et al., 2005). This is consistent with research into the implementation of youth suicide prevention programs that found that services could be difficult to navigate, poorly coordinated, and sometimes have duplicated and overlapping elements alongside significant gaps in service (Arnautovska et al., 2013).
These findings provide essential direction regarding policy, the structuring of services, and the skills needed at the level of intervention and practice. Fundamentally, the need for increased specialized, integrated, accessible services is highlighted. Such services should provide timely (Brent et al., 2013), sustained (Glenn et al., 2019), and tailored treatment to meet individual and family needs. Youth and caregivers valued developing a trusting and collaborative relationship with a therapist or therapeutic team rather than seeing multiple clinicians from different services (e.g., Gulbas et al., 2019). Continuity and cohesive planning in the delivery of treatment and structuring of youth mental health services is therefore recommended. Services should have cohesive linkages with crisis or inpatient mental health services and hospital emergency departments to improve continuity of care and engagement in community treatment after emergency presentations and should foster transitions of care between settings that are mindful of building trust and therapeutic engagement (Storey et al., 2005).
Psychoeducation and stigma reduction programs are essential to improve access to professional care. Broader strategies to improve mental health literacy and raise awareness about suicidality and self-harm are crucial for reducing stigma and improving treatment access. Promising results from school-based programs that aimed to increase young people’s willingness to seek help for depression (Velasco et al., 2020) strengthen the case for similar programs focused on suicidal or self-harm behavior. Likewise, it is critical that health professionals actively consider and address the sense of stigma, shame, and fear of judgment that young people and their caregivers experience so as to facilitate engagement in treatment. Staff at initial engagement points within the health system may not be mental health therapists and may therefore lack pertinent sophistication in response skills to the hidden shame of young people and caregivers. As emergency department care can have a pivotal role in facilitating treatment engagement for this population, training for these clinicians about self-harm and the shame and stigma young people and families experience is signposted by client experience and warrants urgent attention (Hodgson, 2016; Owens et al., 2016). Given caregivers’ role in instigating and accessing help for their young person (Curtis et al., 2018), and the importance of family-based treatment for recovery (Glenn et al., 2019), it is important that such potential service engagement points do not convey judgment or stigma towards these caregivers.
Tailoring of Treatment
This qualitative synthesis highlights the importance of carefully tailoring treatment to meet the distinct needs of youth and caregivers affected by self-harm and suicidal behavior, from their initial self-harm experiences through to recovery. Contact with professional care often begins in the context of a suicidal or self-harm crisis, such as a suicide attempt, or with the disclosure of suicidal ideation or behavior to a third party, and represents a personal and relationship crisis for both the young person and their caregivers. At that time, the young person is dealing with their suicidal thoughts and feelings, and any physical aftermath of the self-harm, in addition to grappling with the fact that their self-harm and suicidal struggle are now visible to others, with the accompanying sense of shame and attendant anxiety that this may entail (Beekrum et al., 2011; Orri et al., 2014). Before treatment, most youth were reluctant to reveal their distress or suicidality to their caregivers. Consequently, at the outset of professional intervention, youth may be unwilling or strongly ambivalent about having caregivers involved, despite struggling to manage their suicidal feelings independently and wanting to be accepted and supported by their family (Holliday & Vandermause, 2015; Wadman, Vostanis, et al., 2018).
It is essential to recognize that discovering the young person’s suicidal or self-harm behavior is also a crisis for caregivers. This systematic review showed that caregivers experienced wide-ranging and overwhelming emotions and all had various struggles in coming to terms with their child’s self-harm (e.g., Byrne et al., 2008; Ferrey et al., 2016a) consistent with previous qualitative research (Curtis et al., 2018; Lachal et al., 2015). These struggles may contribute to some caregivers responding in emotionally uncontained or conversely dismissive or avoidant ways to their young person, neither of which were experienced as helpful by youth (Curtis et al., 2018). Therefore, the context of the initial discovery of self-harm or suicidal event calls for sensitive and nuanced professional care to meet the immediate needs of youth and caregivers and set a foundation for ongoing treatment.
Getting help when it was most needed, access to intensive treatment, and crisis support were identified as necessary for youth and parents alike (e.g., Wadman, Vostanis, et al., 2018), and this aligns with clinical findings supporting front-loaded treatment (Brent et al., 2013). Young people and their caregivers also valued transparency and collaboration in treatment planning. Given that both youth and caregivers may be in crisis at the start of treatment, such care planning must extend beyond a surface-level list of treatment goals to address the complex and conflicting emotions experienced by young people and their caregivers and be revised over time according to their changing needs. These distinct and dynamic needs also have important implications for the role of individual or joint sessions for youth and caregivers.
Individual and Joint Sessions
The qualitative synthesis showed that both youth and caregivers needed significant individual support and that the majority wanted assistance from therapists to improve youth-caregiver communication. Both spoke about the value of independent preparatory work before conjoint sessions (e.g., Humensky et al., 2017) and the importance of therapists’ role as mediators in family sessions (e.g., Hausmann-Stabile et al., 2018). Impacting on the timing of conjoint work was the essential role for therapists in deconstructing indirect or miscued communication, e.g., young people seeking parental connection through self-harm (Beekrum et al., 2011) or parents seeking to express love for their child through “scolding” and criticism (Sukhawaha et al., 2016). Therapists must take an active role in facilitating relationship repair, consistent with the clinical treatment trials that showed benefits of relationship-focused work in which therapists scaffold and support such attachment repair (Diamond et al., 2016).
Individual sessions for caregivers were important to process their emotional reactions to regroup and remain regulated and prioritize their child’s support needs (Raphael et al., 2006). Caregivers also wanted specific and concrete psychoeducation, support, and direction. Such caregiver support may need to be quite detailed to help them problem-solve new and challenging parenting dilemmas, such as how to respond to their child’s suicidal ideation or self-harm in the moment (Dempsey et al., 2019), when and how to access emergency care, and how to maintain parenting limits and monitor the young person’s safety while fostering warmth and trust in the relationship (Byrne et al., 2008; Hughes et al., 2017). In addition, caregivers will likely benefit from individual professional support and psychoeducation focused on emotion coaching because responding to their young person’s distress and self-harm in an emotionally attuned way, showing genuine care and concern without “overreacting”, appears to be experienced as helpful for most youth (Curtis et al., 2018; Wadman, Vostanis, et al., 2018).
While highlighting the crucial role of family-based treatment, the qualitative accounts synthesized here show that a model embracing relationship repair in joint sessions should not be rigidly imposed. A couple of young people described feeling coerced into family sessions where they felt exposed and criticized (Storey et al., 2005), while other youth highlighted the importance of having choices about their care and joint sessions with parents. Therapists should not force young people to participate in family therapy. However, it is important therapists explore the young person’s doubts, fears, and expressed and unexpressed attachment wishes and actively incorporate practical support to empower young people to have more positive connections with their caregivers should they so wish. Thus, careful and collaborative planning of individual and joint sessions is essential for both youth and caregivers.
Strengths-Based Framework
The findings lend support for a strengths-based focus in work with both caregivers and young people. Young people spoke of the adverse effects of feeling judged and the need for acceptance and validation from mental health professionals to foster their sense of agency and self-worth. At the same time, parents reported that their feelings of failure, shame, and loss of parenting efficacy were exacerbated when they felt dismissed or judged by healthcare providers. Importantly, even when youth identified critical, abusive, or other negative caregiver behaviors, many still identified relationship repair and bonding with caregivers as vital to their recovery. This is highly salient for practice delivery. Therapists need to address the caregiver’s problematic behavior, affirming the young person’s need for safety and support. However, this needs to be located within a strengths-based framework and contribute to building upon any available points of positive caregiving. Treatments should focus on helping parents to understand their young person’s self-harm within a therapeutic framework that seeks to rebuild parental presence, confidence, and connection (Asarnow et al., 2015; Diamond et al., 2010), and build on parenting strengths (Pineda & Dadds, 2013).
Implications for Policy and Practice
Several critical considerations have emerged from this review. First, the findings lend strong support to the implementation of family-based treatments for this population. However, this evidence is tempered by adjacent evidence that people in this relationally fragile context need to receive responses characterized by considerable finesse. Practice responses need to be tailored and multi-modal, incorporating individual support and active therapeutic intervention to scaffold communication and relationship repair in joint sessions. Second, this review’s results cast an illuminating light on the need for treatments to be strengths-focused and, in particular, to encompass a sophisticated and nuanced appreciation of the operations of stigma and shame. Within a range of overwhelming emotions, shame was cited most frequently by both parents and young people, contributing to their isolation and distress, and was sometimes exacerbated by problems accessing treatment or stigmatizing responses from health professionals. Although both young people and their caregivers may engage in unhelpful behaviors, these must be addressed within a non-judgmental strengths-focused framework. Third, this review highlights the importance of attachment across the developmental life span. Despite adolescence being a time of increased independence, secure attachment and relationship repair with caregivers were important for the youth affected by suicidal behavior in reducing their isolation and shame, increasing their coping, and ultimately decreasing their suicidality.
At a policy level, prevention and intervention programs that include both youth and caregivers and address stigma as barriers to accessing help are highlighted. To this end, policies should improve mental health literacy and training for mental health professionals and other professionals who may be gatekeepers to treatment. Importantly, increased funding of comprehensive youth mental health services that provide multi-modal individual and family treatment with young people and caregivers is strongly indicated. Lack of appropriate services, long waitlists, and fragmented care were identified as unhelpful professional care experiences. These problems can only be addressed by the increased provision of integrated and affordable services that prioritize fostering therapeutic relationships with youth and their caregivers.
Limitations
Several limitations in this systematic review and synthesis should be noted. Most importantly, none of the studies had a primary focus on family treatment experience, and research explicitly examining this is needed. In addition, the participants included in the studies are not representative of all youth affected by suicidality and self-harm or their caregivers. For example, the perspectives of young people who died by suicide or those who declined to participate in qualitative studies are not represented, while those who disengaged from treatment are under-represented. Although the analysis incorporates both young people and parents/caregivers, no study paired their responses or included therapist experiences to provide a triangulated perspective about the same treatment. Male participants were under-represented, both for youth and caregivers. As shown in Table 1, the studies were mainly from Western nations, although several studies had participants from minority groups. Most studies did not report the LGBTQI + identity of participants. Also, studies with a specific adolescent focus were so few that the selection criteria were broadened to include young people aged 12 to 25 years. Therefore, further research is required to explore family-based treatment experiences, the unique needs of youth and their caregivers across different developmental periods and subgroups, and to develop a deeper understanding of the pathways into the fractured relationships and the repairing of those relationships.
Conclusion
Most youth and their caregivers affected by suicidality or self-harm do not access professional care. This systematic qualitative review identified that access to effective professional care was hampered by the psychological and relationship impact of the young person’s suicidality and self-harm, the operation of shame and stigma, a lack of awareness about professional help, and insufficient, fragmented, and poorly coordinated services. In contrast, effective professional care was facilitated by a timely, strengths-focused treatment that engaged both young people and their caregivers and fostered open, collaborative, and trusting therapeutic relationships. The review’s findings lend strong support for family-based intervention incorporating individual and joint sessions and emphasize that professional care should be tailored to meet youth and their caregivers’ distinct and dynamic needs from the initial disclosure of suicidal or self-harm behavior through recovery. Barriers to effective care must be addressed through increased youth mental health services that provide timely and integrated care from crisis intervention through community treatment and a concerted effort to promote public education about youth suicidal and self-harm behavior to reduce stigma, particularly for staff at potential engagement points. As the quality of therapeutic relationships was crucial to youth and their caregivers for engagement and effective intervention, this lived experience should inform direct clinical practice and the design and delivery of suicide prevention and treatment programs.
References
*References included in the systematic review are marked with an asterisk
Aggarwal, S., Patton, G., Reavley, N., Sreenivasan, S. A., & Berk, M. (2017). Youth self-harm in low- and middle-income countries: Systematic review of the risk and protective factors. International Journal of Social Psychiatry, 63(4), 359–375. https://doi.org/10.1177/0020764017700175
Armiento, J. S., Hamza, C. A., & Willoughby, T. (2014). An examination of disclosure of nonsuicidal self-injury among university students. Journal of Community & Applied Social Psychology, 24, 518–533. https://doi.org/10.1002/casp.2190
Arnautovska, U., Kolves, K., Ide, N., & De Leo, D. (2013). Review of suicide-prevention programs in Queensland: State- and community-level activities. Australian Health Review, 37(5), 660–665.
Asarnow, J. R., Berk, M., Hughes, J. L., & Anderson, N. L. (2015). The SAFETY program: A treatment-development trial of a cognitive-behavioral family treatment for adolescent suicide attempters. Journal of Clinical Child & Adolescent Psychology, 44(1), 194–203. https://doi.org/10.1080/15374416.2014.940624
Beekrum, R., Valjee, S. R., & Collings, S. J. (2011). An emic perspective on the dynamics of non-fatal suicidal behaviour in a sample of South African Indian women. South African Journal of Psychology, 41(1), 63–73. https://doi.org/10.1177/008124631104100107
Berger, E., Hasking, P., & Martin, G. (2013). ‘Listen to them’: Adolescents’ views on helping young who self-injure. Journal of Adolescence, 36(5), 935–945. https://doi.org/10.1016/j.adolescence.2013.07.011
*Bostik, K., & Everall, R. (2006). In my mind I was alone: Suicidal adolescents’ perceptions of attachment relationships. International Journal for the Advancement of Counselling, 28(3), 269–287. https://doi.org/10.1007/s10447-006-9013-6
*Bostik, K. E., & Everall, R. D. (2007). Healing from suicide: Adolescent perceptions of attachment relationships. British Journal of Guidance & Counselling, 35(1), 79–96. https://doi.org/10.1080/03069880601106815
Brent, D., McMakin, D., Kennard, B., Goldstein, T., Mayes, T., & Douaihy, A. (2013). Protecting adolescents from self-harm: A critical review of intervention studies. Journal of the American Academy of Child and Adolescent Psychiatry. https://doi.org/10.1016/j.jaac.2013.09.009
Buus, N., Caspersen, J., Hansen, R., Stenager, E., & Fleischer, E. (2014). Experiences of parents whose sons or daughters have (had) attempted suicide. Journal of Advanced Nursing, 70(4), 823–832. https://doi.org/10.1111/Jan.12243
*Byrne, S., Morgan, S., Fitzpatrick, C., Boylan, C., Crowley, S., Gahan, H., Howley, J. Staunton, D., & Guerin, S. (2008). Deliberate self-harm in children and adolescents: A qualitative study exploring the needs of parents and carers. Clinical Child Psychology and Psychiatry, 13(4), 493–504. https://doi.org/10.1177/1359104508096765
Calear, A., Christensen, H., Freeman, A., Fenton, K., Busby Grant, J., van Spijker, B., & Donker, T. (2016). A systematic review of psychosocial suicide prevention interventions for youth. European Child & Adolescent Psychiatry, 25(5), 467–482. https://doi.org/10.1007/s00787-015-0783-4
Center for Disease Control and Prevention, National Center for Health Statistics. Underlying Cause of Death 1999–2019 on CDC WONDER Online Database, released in 2020. Data are from the Multiple Cause of Death Files, 1999–2019, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program. Accessed at http://wonder.cdc.gov/ucd-icd10.html on Apr 7, 2021.
Critical Appraisal Skills Programme. (2019). CASP (Systematic Review) Checklist (online) Available at. https://casp-uk.net/casp-tools-checklists/. Date Accessed 16 Dec 2020
Cruz, D., Narciso, I., Pereira, C., & Sampaio, D. (2014). Risk trajectories of self-destructiveness in adolescence: Family core influences. Journal of Child and Family Studies, 23(7), 1172–1181. https://doi.org/10.1007/s10826-013-9777-3
Curtin, S. (2020). State suicide rates among adolescents and young adults aged 10–24: United States, 2000–2018. National Vital Statistics Reports, 69(11).
Curtis, S., Thorn, P., McRoberts, A., Hetrick, S., Rice, S., & Robinson, J. (2018). Caring for young people who self-harm: A review of perspectives from families and young people. International Journal of Environmental Research and Public Health. https://doi.org/10.3390/ijerph15050950
Czyz, E., Liu, Z., & King, C. (2012). Social connectedness and one-year trajectories among suicidal adolescents following psychiatric hospitalization. Journal of Clinical Child & Adolescent Psychology, 41(2), 214–226. https://doi.org/10.1080/15374416.2012.651998
Daly, P. (2005). Mothers living with suicidal adolescents: A phenomenological study of their experience. Journal of Psychosocial Nursing and Mental Health Services, 43(3), 22–28.
*Dempsey, S. J. A., Halperin, S., Smith, K., Davey, C. G., McKechnie, B., Edwards, J., & Rice, S. M. (2019). ‘Some guidance and somewhere safe’: Caregiver and clinician perspectives on service provision for families of young people experiencing serious suicide ideation and attempt. Clinical Psychologist, 23(2), 103–111. https://doi.org/10.1111/cp.12172
Diamond, G. S., Wintersteen, M. B., Brown, G. K., Diamond, G. M., Gallop, R., Karni, S., & Suzanne, L. (2010). Attachment-based family therapy for adolescents with suicidal ideation: A randomized controlled trial. Journal of the American Academy of Child & Adolescent Psychiatry, 49(2), 122–131. https://doi.org/10.1016/j.jaac.2009.11.002
Diamond, G. S., Russon, J., & Levy, S. (2016). Attachment-based Family Therapy: A review of the empirical support. Family Process, 55(3), 595–610. https://doi.org/10.1111/famp.12241
*Everall, R. D., Bostik, K. E., & Paulson, B. L. (2006). Being in the safety zone: Emotional experiences of suicidal adolescents and emerging adults. Journal of Adolescent Research, 21(4), 370–392. https://doi.org/10.1177/0743558406289753
Ewing, E. S. K., Diamond, G., & Levy, S. (2015). Attachment-based family therapy for depressed and suicidal adolescents: Theory, clinical model and empirical support. Attachment & Human Development, 17(2), 136–156. https://doi.org/10.1080/14616734.2015.1006384
*Ferrey, A. E., Hughes, N. D., Simkin, S., Locock, L., Stewart, A., Kapur, N., Gunnell, D. Hawton, K. (2016a). Changes in parenting strategies after a young person’s self-harm: A qualitative study. Child Adolescent Psychiatry Mental Health, 10(1). https://doi.org/10.1186/s13034-016-0110-y
*Ferrey, A. E., Hughes, N. D., Simkin, S., Locock, L., Stewart, A., Kapur, N., Gunnell, D., Hawton, K. (2016b). The impact of self-harm by young people on parents and families: A qualitative study. British Medical Journal Open. https://doi.org/10.1136/BMJ open-2015–009631
Giletta, M., Scholte, R. H. J., Engels, R. C. M. E., Ciairano, S., & Prinstein, M. J. (2012). Adolescent non-suicidal self-injury: A cross-national study of community samples from Italy, the Netherlands, and the United States. Psychiatry Research, 197(1–2), 66–72. https://doi.org/10.1016/j.psychres.2012.02.009
Glenn, C., Esposito, E., Porter, A., & Robinson, D. (2019). Evidence base update of psychosocial treatments for self-injurious thoughts and behaviors in youth. Journal of Clinical Child & Adolescent Psychology, 48(3), 357–392. https://doi.org/10.1080/15374416.2019.1591281
Glenn, C., Franklin, J., & Nock, M. (2015). Evidence-based psychosocial treatments for self-injurious thoughts and behaviors in youth. Journal of Clinical Child & Adolescent Psychology, 44(1), 1–29. https://doi.org/10.1080/15374416.2014.945211
Grimmond, J., Kornhaber, R., Visentin, D., & Cleary, M. (2019). A qualitative systematic review of experiences and perceptions of youth suicide. PLoS ONE, 14(6), e0217568. https://doi.org/10.1371/journal.pone.0217568
*Gulbas, L. E., Guz, S., Hausmann-Stabile, C., Szlyk, H. S., & Zayas, L. H. (2019). Trajectories of wellbeing among Latina adolescents who attempt suicide: A longitudinal qualitative analysis. Qualitative Health Research, 29(12), 1766–1780. https://doi.org/10.1177/1049732319837541
*Hausmann-Stabile, C., Gulbas, L., & Zayas, L. H. (2018). Treatment narratives of suicidal Latina teens. Archives of Suicide Research, 22(1), 165–172. https://doi.org/10.1080/13811118.2017.1304305
*Herrera, A., Dahlblom, K., Dahlgren, L., & Kullgren, G. (2006). Pathways to suicidal behaviour among adolescent girls in Nicaragua. Social Science & Medicine, 62(4), 805–814. https://doi.org/10.1016/j.socscimed.2005.06.055
Hill, C. E., Knox, S., Thompson, B. J., Williams, E. N., Hess, S. A., & Ladany, N. (2005). Consensual qualitative research: An update. Journal of Counseling Psychology, 52(2), 196–205. https://doi.org/10.1037/0022-0167.52.2.196
Hill, C. E. (Ed.). (2012). Consensual Qualitative Research, American Psychological Association.
Hodgson, K. (2016). Nurses’ attitudes towards patients hospitalised for self-harm. Nursing Standard, 30(31), 38–44. https://doi.org/10.7748/ns.30.31.38.s44
*Holliday, C., & Vandermause, R. (2015). Teen experiences following a suicide attempt. Archives of Psychiatric Nursing, 29(3), 168–173. https://doi.org/10.1016/j.apnu.2015.02.001
*Hughes, N. D., Locock, L., Simkin, S., Stewart, A., Ferrey, A. E., Gunnell, D., Kapur, N., & Hawton, K. (2017). Making sense of an unknown terrain: How parents understand self-harm in young people. Qualitative Health Research, 27(2), 215–225. https://doi.org/10.1177/1049732315603032
*Humensky, J. L., Gil, R. M., Mazzula, S., Diaz, S., & Lewis-Fernández, R. (2017). Life is precious: Views of adolescents and their mothers on methods to reduce suicidal behavior in Latinas. Journal of School Nursing, 33(6), 426–433. https://doi.org/10.1177/1059840517722590
Ivey-Stephenson, A. Z., Demissie, Z., Crosby, A. E., et al. (2019). Suicidal ideation and behaviors among high school students—youth risk behavior survey, United States. MMWR Supplement, 69(1), 47–55. https://doi.org/10.15585/mmwr.su6901a6
Iyengar, U., Snowden, N., Asarnow, J. R., Moran, P., Tranah, T., & Ougrin, D. (2018). A further look at therapeutic interventions for suicide attempts and self-harm in adolescents: An updated systematic review of randomized controlled trials. Front Psychiatry, 9, 583. https://doi.org/10.3389/fpsyt.2018.00583
Kann, L., McManus, T., Harris, W. A., Shanklin, S. L., Flint, K. H., Queen, B., Lowry, R., Chyen, D., Whittle, L., Thornton, J., Lim, C., Bradford, D., Yamakawa, Y., Leon, M., Brener, N., & Ethier, K. (2018). Youth risk behavior surveillance — United States, 2017. MMWR Surveillance Summaries, 67(8), 1–114. https://doi.org/10.15585/mmwr.ss6708a1
*Kelada, L., Whitlock, J., Hasking, P., & Melvin, G. (2016). Parents’ experiences of nonsuicidal self-injury among adolescents and young adults. Journal of Child and Family Studies, 2016(25), 3403–3416. https://doi.org/10.1007/s10826-016-0496-4
*Keyvanara, M., & Haghshenas, A. (2011). Sociocultural contexts of attempting suicide among Iranian youth: A qualitative study. East Mediterranean Health Journal, 17(6), 529–535. https://doi.org/10.26719/2011.17.6.529
Kokkevi, A., Rotsika, V., Arapaki, A., & Richardson, C. (2012). Adolescents’ self-reported suicide attempts, self-harm thoughts and their correlates across 17 European countries. Journal of Child Psychology and Psychiatry, 53(4), 381–389. https://doi.org/10.1111/j.1469-7610.2011.02457.x
Lachal, J., Orri, M., Sibeoni, J., Moro, M., & Revah-Levy, A. (2015). Metasynthesis of youth suicidal behaviours: Perspectives of youth, parents, and health care professionals. PLoS ONE. https://doi.org/10.1371/journal.pone.0127359
Lachal, J., Revah-Levy, A., Orri, M., & Moro, M. R. (2017). Metasynthesis: An original method to synthesize qualitative literature in psychiatry. Front Psychiatry. https://doi.org/10.3389/fpsyt.2017.00269
Lindgren, B. M., Svedin, C. G., & Werkö, S. (2018). A systematic literature review of experiences of professional care and support among people who self-harm. Archives of Suicide Research, 22, 173–192.
Liu, X., Huang, Y., & Liu, Y. (2018). Prevalence, distribution, and associated factors of suicide attempts in young adolescents: School-based data from 40 low-income and middle-income countries. PLoS ONE. https://doi.org/10.1371/journal.pone.0207823
*McAndrew, S., & Warne, T. (2014). Hearing the voices of young people who self-harm: Implications for service providers. International Journal of Mental Health Nursing, 23(6), 570–579. https://doi.org/10.1111/inm.12093
*McDonald, G., O’Brien, L., & Jackson, D. (2007). Guilt and shame: Experiences of parents of self-harming adolescents. Journal of Child Health Care, 11(4), 298–310. https://doi.org/10.1177/1367493507082759
Michelmore, L., & Hindley, P. (2012). Help-seeking for suicidal thoughts and self-harm in young people: A systematic review. Suicide and Life-Threatening Behavior, 42(5), 507–524. https://doi.org/10.1111/j.1943-278X.2012.00108.x
*Mitten, N., Preyde, M., Lewis, S., Vanderkooy, J., & Heintzman, J. (2016). The perceptions of adolescents who self-harm on stigma and care following inpatient psychiatric treatment. Social Work in Mental Health, 14(1), 1–21. https://doi.org/10.1080/15332985.2015.1080783
*Murray, B. L., & Wright, K. (2006). Integration of a suicide risk assessment and intervention approach: The perspective of youth. Journal of Psychiatric & Mental Health Nursing, 13(2), 157–164. https://doi.org/10.1111/j.1365-2850.2006.00929.x
Noyes, J., Booth, A., Cargo, M., Flemming, K., Harden, A., Harris J., Garside, R., Hannes, K., Pantoja, T., & Thomas, J. (2021). Chapter 21: Qualitative evidence. In: JPT Higgins, J Thomas, J Chandler, M Cumpston, T Li, MJ Page, VA Welch (Eds.). Cochrane handbook for systematic reviews of interventions version 6.2 (sections 21.1–21.16). Cochrane. www.training.cochrane.org/handbook
*Oldershaw, A., Richards, C., Simic, M., & Schmidt, U. (2008). Parents’ perspectives on adolescent self-harm: A qualitative study. British Journal of Psychiatry, 193(2), 140–144. https://doi.org/10.1192/bjp.bp.107.045930
Olfson, M., Wall, M., Wang, S., Crystal, S., Bridge, J. A., Liu, S. M., & Blanco, C. (2018). Suicide after deliberate self-harm in adolescents and young adults. Pediatrics. https://doi.org/10.1542/peds.2017-3517
*Orri, M., Paduanello, M., Lachal, J., Falissard, B., Sibeoni, J., & Revah-Levy, A. (2014). Qualitative approach to attempted suicide by adolescents and young adults: The (neglected) role of revenge. PLoS ONE, 9(5), e96716. https://doi.org/10.1371/journal.pone.0096716
Ougrin, D., Tranah, T., Stahl, D., Moran, P., & Asarnow, J. R. (2015). Therapeutic interventions for suicide attempts and self-harm in adolescents: Systematic review and meta-analysis. Journal of the American Academy of Child & Adolescent Psychiatry, 54(2), 97–107. https://doi.org/10.1016/j.jaac.2014.10.009
*Owens, C., Hansford, L., Sharkey, S., & Ford, T. (2016). Needs and fears of young people presenting at accident and emergency department following an act of self-harm: Secondary analysis of qualitative data. British Journal of Psychiatry, 208(3), 286–291. https://doi.org/10.1192/bjp.bp.113.141242
Pineda, J., & Dadds, M. (2013). Family intervention for adolescents with suicidal behavior: A randomized controlled trial and mediation analysis. Journal of the American Academy of Child & Adolescent Psychiatry, 52(8), 851–862. https://doi.org/10.1016/j.jaac.2013.05.015
*Raphael H., Clarke, G., & Kumar, S. (2006). Exploring parents’ responses to their child’s deliberate self-harm. Health Education, 106(1), 9–20. https://doi.org/10.1108/09654280610637166
Rissanen, M.-L., Kylmä, J., & Laukkanen, E. (2009). Descriptions of help by Finnish adolescents who self-mutilate. Journal of Child & Adolescent Psychiatric Nursing, 22(1), 7–15. https://doi.org/10.1111/j.1744-6171.2008.00164.x
*Rissanen, M., Kylmä, J., & Laukkanen, E. (2009b). Helping adolescents who self-mutilate: Parental descriptions. Journal of Clinical Nursing, 18(12), 1711–1721. https://doi.org/10.1111/j.1365-2702.2008.02672.x
Rowe, S. L., French, R. S., Henderson, C., Ougrin, D., Slade, M., & Moran, P. (2014). Help-seeking behaviour and adolescent self-harm: A systematic review. Australian & New Zealand Journal of Psychiatry, 48(12), 1083–1095. https://doi.org/10.1177/0004867414555718
Slovak, K., & Singer, J. B. (2012). Engaging parents of suicidal youth in a rural environment. Child & Family Social Work, 17, 212–221. https://doi.org/10.1111/j.1365-2206.2012.00826.x
Stänicke, L. I., Haavind, H., & Gullestad, S. E. (2018). How do young people understand their own self-harm? A meta-synthesis of adolescents’ subjective experience of self-harm. Adolescent Research Review, 3(2), 173–191. https://doi.org/10.1007/s40894-018-0080-9
*Stewart, A., Hughes, N. D., Simkin, S., Locock, L., Ferrey, A., Kapur, N., Gunnell, D., & Hawton, K. (2018). Navigating an unfamiliar world: How parents of young people who self-harm experience support and treatment. Child and Adolescent Mental Health, 23(2), 78–84. https://doi.org/10.1111/camh.12205
*Storey, P., Hurry, J., Jowitt, S., Owens, D., & House, A. (2005). Supporting young people who repeatedly self-harm. Journal of the Royal Society for the Promotion of Health, 125(2), 71–75. https://doi.org/10.1177/146642400512500210
*Sukhawaha, S., Arunpongpaisal, S., & Rungreangkulkij, S. (2016). Attempted suicide triggers in Thai adolescent perspectives. Archives of Psychiatric Nursing, 30(3), 334–341. https://doi.org/10.1016/j.apnu.2015.12.005
Swannell, S. V., Martin, G. E, Page, A., Hasking, P., & St John, N. J. (2014). Prevalence of nonsuicidal self-injury in nonclinical samples: Systematic review, meta-analysis and meta-regression. Suicide and Life-Threatening Behavior, 44(3), 273–303. https://doi.org/10.1111/sltb.12070
*Tingey, L., Cwik, M. F., Goklish, N., Larzelere-Hinton, F., Lee, A., Suttle, R., Walkup, J., & Barlow, A. (2014). Risk pathways for suicide among Native American adolescents. Qualitative Health Research, 24(11), 1518–1526. https://doi.org/10.1177/1049732314548688
Tong, A., Flemming, K., McInnes, E., Oliver, S., & Craig, J. (2012). Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Medical Research Methodology. https://doi.org/10.1186/1471-2288-12-181
Valencia-Agudo, F., Burcher, G. C., Ezpeleta, L., & Kramer, T. (2018). Nonsuicidal self-injury in community adolescents: A systematic review of prospective predictors, mediators and moderators. Journal of Adolescence, 65, 25–38. https://doi.org/10.1016/j.adolescence.2018.02.012
Velasco, A., Cruz, I., Billings, J., Jimenez, M., & Rowe, S. (2020). What are the barriers, facilitators and interventions targeting help-seeking behaviors for common mental health problems in adolescents? A systematic review. BMC Psychiatry. https://doi.org/10.1186/s12888-020-02659-0
*Wadman, R., Armstrong, M., Clarke, D., Harroe, C., Majumder, P., Sayal, K., Vostanis, P., & Townsend, E. (2018a). Experience of self-harm and its treatment in looked-after young people: An interpretative phenomenological analysis. Archives Suicide Research, 22(3), 365–379. https://doi.org/10.1080/13811118.2017.1355286
*Wadman, R., Vostanis, P., Sayal, K., Majumder, P., Harroe, C., Clarke, D., Armstrong, M., Townsend, E. (2018b). An interpretative phenomenological analysis of young people’s self-harm in the context of interpersonal stressors and supports: Parents, peers, and clinical services. Social Science and Medicine, 212, 120–128. https://doi.org/10.1016/j.socscimed.2018.07.021
Wagner, K., & Wagner, K. (2012). Suicidal behavior in children and adolescents. Psychiatric times, 29(2), 24.
World Health Organization. (2019). Suicide in the world. https://www.who.int/publications/i/item/suicide-in-the-world
Wu, P., Katic, B., Liu, X., Fan, B., & Fuller, C. (2010). Mental health service use among suicidal adolescents: Findings from a US National Community Survey. Psychiatric Services, 61(1), 17–24.
Zalsman, G., Hawton, K., Wasserman, D., van Heeringen, K., Arensmen, E., Sarchiapone, M., Carli, V., Höschl, C., Barzilay, R., Balazs, J., Purebl, G., Kahn, J. P., Sáiz, P. A., Lipsicas, C. B., Bobes, J., Cozman, D., Hegerl, U., & Zohar, J. (2016). Suicide prevention strategies revisited: 10-year systematic review. The Lancet Psychiatry, 3(7), 646–659. https://doi.org/10.1016/S2215-0366(16)30030-X
*Zayas, L., Gulbas, L. E., Fedoravicius, N., & Cabassa, L. J. (2010). Patterns of distress, precipitating events, and reflections on suicide attempts by young Latinas. Social Science & Medicine, 70(11), 1773–1779. https://doi.org/10.1016/j.socscimed.2010.02.013
Acknowledgements
DS conceived of the study, participated in its design, data collection, analysis, and interpretation of the data, and drafted the manuscript; IS participated in the design of the study, analysis, and interpretation of the data, and revisions to the manuscript; KM participated in the design of the study, evaluation of data quality, analysis and interpretation of the data, and revisions to the manuscript; IGS participated in the data collection, analysis and interpretation of the data, and revisions to the manuscript. All authors read and approved the final manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Appendix
Rights and permissions
About this article

Cite this article
Simes, D., Shochet, I., Murray, K. et al. A Systematic Review of Qualitative Research of the Experiences of Young People and their Caregivers Affected by Suicidality and Self-harm: Implications for Family-Based Treatment. Adolescent Res Rev 7, 211–233 (2022). https://doi.org/10.1007/s40894-021-00164-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40894-021-00164-3