
Abstract
The purpose of this study was to compare and evaluate the inter-joint coordination between the hips and lumbar spine in both male and female skilled golfers during the downswing phase. Six infrared MCAM2 cameras were used for capturing each participant’s swing motion. In order to evaluate the inter-joint coordination, kinematic data and continuous relative phase (CRP) were obtained during downswing phase. The lead hip-lumbar spine CRP in male golfers showed a typical parabola pattern with a minimum value at around 60% of the downswing phase. On the other hand, the CRP between the lead hip and lumbar spine of female golfers barely changed from the initial to middle downswing stages, and increased at the later stage. Male golfers typically used their lead hip more than their lumbar spine during the early downswing, while the rotational contribution of the lumbar spine and lead hip in female golfers were comparable until the middle of the downswing phase. These findings result from the opposite rotation of the lumbar spine for even the early downswing phase due to the muscular and articular flexibility of female golfers. This study has the potential to help develop gender-specific coaching materials for the improvement of swing skills.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
The golf swing is a complex movement involving the entire body and multiple joints [1], with high coordination characteristics between the joints and between the segments of the human body [2, 3]. Male professional golfers use their lower limb joint more to compensate the deficiency of the muscle flexibility of their upper body compared to the female golfers. On the other hand, female golfers have a greater rotation of pelvis and upper torso than the male golfers to improve the golf swing performance [4]. Additionally, women golfers had twice as many wrist injuries as the men golfers based on the epidemiological data [5], and this difference was associated with the weaker kinetic chain consisted of neuromuscular and articular joint system of human body [6]. In general, the swing outcomes of male professional golfers differ to those of female professional golfers due to the differences in the physical features [7] and basic swing mechanics between men and women [6, 8]. Swing outcomes are commonly evaluated using the clubhead velocity at impact and the driving distance of the ball [9, 10], and the rotational biomechanics has an important role in improving swing performance [11]. During the golf swing, the stored energy by coiling at the top of the backswing is rapidly released and the high impulse is transferred to the club and ball during the downswing, leading to increased driving distance of the ball [12, 13]. From a biomechanical perspective, understanding of the proper swing mechanisms of both male and female professional golfers during downswing provides gender-specific information to improve swing skill and prevent golf injury [8].
The axial rotational movement during a golf swing is controlled the lumbar spine and hip joints that are connected to the trunk, pelvis, and thigh segments [14]. The relative rotation between the pelvis and upper torso at the top of the backswing, which is defined as the ‘x-factor’, represents the fully eccentric loading condition of the trunk muscles, and these muscles perform concentric shortening during the downswing. Finally, this mechanism allows the player to produce increased power which can then be transferred to the clubhead [15]. In addition, the kinematic difference between male and female professional golfers can be observed in the hips and lumbar spine during the golf swing due to the difference in their swing mechanisms. According to previous publications, female professional golfers exhibited higher absolute range of motion (ROM) and movement variability of the pelvis and trunk [1, 4, 6]. These studies mainly focused on the kinematics of the trunk, thorax, and pelvis, and no research has been carried out on the evaluation of compensatory mechanisms or coordination between joints controlled by the neuromuscular system. Swing performance is affected not only by the trained movement of each segment and joint but also by the sequence or phase differences between neighboring joints [2, 14, 16].
Inter-joint coordination refers to the interconnected relationship among the movements of neighboring joints [17] and provides basic information to evaluate how the central nervous system organizes various joints to achieve specific movement [18]. Continuous relative phase (CRP), considering the angles and angular velocities of neighboring joints, is generally used to evaluate inter-joint coordination [19] and applied for the evaluation of dynamic motor control, improvement of movement ability, and prevention of musculoskeletal injury during human movement such as walking and ski jumping [17, 20]. Chiu et al. (2015) compared the coordination of the lower body joints between young and old adults while ascending and descending stairs [21]. The coordination strategy in elderly people was demonstrated to be less flexible, and each joint moved less independently than the joints of young people. More recently, inter-joint coordination between the lumbar spine and hip joints in skilled male golfers was evaluated, and the relationship between this coordination pattern and performance was identified [14]. The results showed that the coordination between the lumbar spine and leading hip joints plays a critical role in improving swing speed at impact. Human movement is represented as the synergetic activities of the muscular nervous system based on the constraints of the anatomical structures, environmental effects, and various movements, and this synergy allows a human locomotor system to react simply and properly [22]. Since the redundant degrees of freedom in the neuromuscular system reduce the complexity of each joint and muscle from the central nervous system, the muscle groups of similar functions are activated at the same time [23]. Therefore, the evaluation of the coordinated movement during the complex movement such as golf swing can provide an understanding of how the central nervous system organizes each joint and how the redundant motor unit can be simplified and controlled.
Even though inter-joint coordination is a very useful parameter in biomechanics, few studies have been conducted that evaluate sports movements utilizing coordination characteristics. Specifically, the coordination between lumbar spine and hip joint during downswing is important parameter to improve golf swing performance [14], but the difference between male and female golfers has not been reported. The understanding of the rotational coordination characteristics between the hips and lumbar spine in both male and female skilled golfers during the downswing provides not only information for gender-specific training methods and injury factors but also explains of the human locomotor mechanisms controlled by the neuromuscular system. Therefore, the purpose of this study was to compare and evaluate the inter-joint coordination between the hips and lumbar spine in both male and female skilled golfers during the downswing phase using the CRP parameter. It was hypothesized that the coordination characteristics of male golfers differed from those of female golfers due to the difference of swing mechanisms.
2 Materials and Methods
2.1 Participants
Eighteen male and sixteen female golfers participated in this study. All participants were right-handed professional golfers as members of the Korea (Ladies) Professional Golf Association and had a self-reported handicap index below 0. No participant had any previous history of musculoskeletal disease and golfers who were currently experiencing pain in their joints or muscles were excluded in this experiment. All of the experiment procedures were approved by the Sungkyunkwan University Ethics Committee, and written informed consent was provided by every participant prior to the experiments. Table 1 shows the physical and swing characteristics of the participants.
2.2 Instrumentation and Experimental Procedure
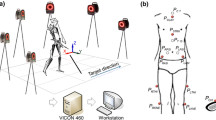
In order to mimic an actual golf environment, the experiment incorporated a swing-net and a foot mat. Six infrared MCAM2 cameras, located outside of the swing-net region, were used for capturing each participant’s swing motion at 120 Hz. The X-, Y-, and Z-axes of the global reference system were set as the left–right, forward–backward, and perpendicular directions based on the set-up posture, respectively. The target was set as the opposite direction of the X-axis of the global reference system.
A total of twelve optical markers were attached to the skin of each participant at the following locations (Fig. 1): four markers on the upper torso, including the suprasternal notch (PCLAV), xiphoid process (PSTRN), C7 (PC7), and T10 (PT10) spinous process of the notch; four markers on the pelvis, including the left and right anterior superior iliac spines (PLASI and PRASI) and posterior superior iliac spines (PLPSI and PRPSI); and four markers on each thigh segment, including the left and right surface of the thigh (PLTHI and PRTHI) and the femoral condyle (PLKNE and PRKNE). Additionally, two markers were located on the clubhead (PCH) and shaft (PCS) of the club to detect the downswing phase. The participants performed sufficient golf swing practice with their own drivers before beginning the experiments [10]. A total of three trials per participant were performed and recorded, and the average values of two selected trials based on the data quality and subjective decision of an effective shot were used for the analysis [6].

Locations of optical markers attached to the human body
2.3 Data Analysis
High frequency noise was removed from each marker trajectory by filtering noise using a Butterworth low-pass filter with a cut-off frequency of 10 Hz [24, 25]. Based on the data from the markers attached to the clubhead, the downswing phase between the top of the backswing and the impact events were calculated. The top of the backswing was determined as the point at which the speed of the clubhead marker was zero and the impact event was set as the lowest point of the Z-axis of the clubhead marker after the top of the backswing [2]. The downswing duration of each participant was normalized by 100% using the cubic spline technique.
In order to calculate the rotational angle of the lumbar spine and the location of each hip and knee joint, anatomical reference systems for the upper torso, pelvis, and each thigh segment were developed based on previous studies [26,27,28]. Additionally, the rotational angular velocities of each joint were calculated using the numerical differentiation method and 100% normalization process.
CRP values were calculated to evaluate the inter-joint coordination between the hips and the lumbar spine. The angles of each joint were normalized between the scale of − 1 and 1, and angular velocities were divided by the maximum value of the absolute angular velocity [17]. The normalized angle and angular velocity were plotted on a phase graph as the horizontal and vertical axes, respectively, and the phase angle was calculated. The phase angle was defined as the angle between the straight line from the origin to each data point and the positive horizontal axis (Eq. 1).
where θ and ω are the normalized angular displacement and velocity, respectively. The CRP was calculated from the difference of phase angle between the two neighboring joints. A CRP value close to 0 or 360° implies that the two adjacent joints move in the same direction, while CRP data near 180 or − 180° indicate that the two adjacent joints move in opposite directions. The calculation procedures of joint center, kinematic modeling and CRP were described in the previous study [14].
The mean absolute relative phase (MARP) was calculated to understand the entire coordination pattern of the adjacent joints [21]. The MARP values close to 0° indicate that the two neighboring joints rotate in the same direction (In-phase). In addition, the deviation phase (DP), calculated as an average standard deviation of CRP data, was extracted to evaluate the stability of the organized neuromuscular system in human motor control. The high DP value implies a more flexible coordination strategy between two neighboring joints, while low DP values represent relatively stable and typical control mechanisms of neuromuscular system [29].
2.4 Statistics
The average and standard deviations from the angle and angular velocity of the lumbar spine and hip joints were measured for each participant during the downswing phase. Additionally, coefficient of multiple correlation was used to evaluate the similarity of the lumbar and both hip kinematics between male and female golfers [30]. A Shapiro–Wilk test was used to evaluate the normality of each variable. The MARP and DP difference between the lead hip–lumbar spine and the trail hip–lumbar spine was evaluated using a paired t test, and the difference between male and female golfers was evaluated suing the Wilcoxon test or the Student t-test based on the data normality. The significant level was set as 0.05, and all statistics were analyzed using the Statistical Package for the Social Sciences (SPSS) program (SPSS ver. 15, SPSS Inc., Chicago, IL, USA).
3 Results
Significant statistical differences of physical and golf swing characteristics between the male and female pro-golfers were observed, except for the parameters of age and handicap score (Table 1). Specifically, the clubhead speed at impact in males was about 4 m/s greater than that of female golfers (p = 0.035) and the duration of downswing phase was 60 ms less than that of the female golfers (p < 0.01).
Different patterns of angular displacement of the lumbar spine during downswing were demonstrated between male and female professional golfers (Fig. 2a, b). Specifically, the coefficient of multiple correlation of the lumbar spine was observed the lowest similarity with r = 0.57 among all kinematic patterns (Table 2). The rotation difference between the trunk and pelvis of male golfers in the initial stage of the downswing phase increased compared to that of the female golfers. However, this difference decreased to less than 20° during the end stage of the downswing phase. For angular velocity of the lumbar spine, increased rotation was observed in the male compared to the female golfers from the middle to the end stage of the downswing phase. The patterns of the angle and angular velocity during the entire downswing phase of the lead hip joint appeared to be similar regardless of gender (Fig. 2c, d). The difference of angle between the male and female golfers was observed in the trail hip joints (average difference within ± 9°), but patterns of the angular velocities appeared to be similar for male and female golfers during the downswing phase (Fig. 2e, f). The overall summary of kinematics is presented in Table 3. The patterns of the ROM, average, and peak angular velocities of each joint showed similar values except for the lumbar spine joint. Male golfers demonstrated higher ROM values by about 7° (p < 0.01) and higher peak angular velocity by 80°/s than female golfers (p < 0.01).

Angles and angular velocities of lead hip, trail hip and lumbar spine in male and female golfers during downswing
Figure 3 demonstrates the average CRP patterns between the lead hip and lumbar spine and between the trail hip and lumbar spine during the downswing phase. The lead hip-lumbar spine CRP in male golfers showed a typical parabola pattern with a minimum value at around 60% of the downswing phase. On the other hand, the CRP between the lead hip and lumbar spine of female golfers barely changed from the initial to middle downswing stages, and increased at the later stage (Fig. 3a). The trail hip-lumbar spine CRP appeared as an almost straight line for male golfers and as an irregular pattern with almost negative values for female golfers (Fig. 3b).

CRP plot between lead hip and lumbar spine and between trail hip and lumbar spine in male and female golfers during downswing
The MARP and DP values in the lead hip and lumbar spine of male golfers during downswing appeared to be lower than those of the female golfers (Fig. 4a, b). For the detailed phases of the downswing, male golfers demonstrated significantly lower values at all stages (initial, middle, and final downswing phases) compared to female golfers (Table 4). Similar to the relationship between the lead hip and lumbar spine, MARP and DP in the trail hip-lumbar spine of male golfers was lower than those of female golfers (p < 0.01). The MARP in male golfers was observed to have lower values at the initial and final stages of the downswing phase. The DP values of male golfers showed a lower value at the initial and final stages of the downswing phase compared to those of the female golfers (p < 0.01). Additionally, both groups appeared to have high MARP values for the lead hip-lumbar spine compared to the trail hip-lumbar spine, while a significant difference of DP values between the lead hip-lumbar spine and the trail hip-lumbar spine was observed in male golfers (p < 0.01).

MARP and DP of hips–lumbar spine coordination in male and female golfers in a complete downswing phase
4 Discussion
The patterns of the rotational angles of the lead and trail hip during the downswing were similar in the male and female skilled golfers, and the ROM, average, and peak angular velocities did not show statistical difference. However, the patterns of the rotation angles between the male and female groups somewhat differed, and the male golfers showed greater ROM and peak angular velocity values than those of the female golfers (Fig. 2 and Table 3). Compared to female golfers, the male golfers may have less flexibility related to the trunk and pelvis rotation. This might be due to the greater suppleness of female golfers and the increased coiling of the trunk and pelvis segments observed during the backswing; these rotations still appeared at the impact stage. Horan et al. (2010) reported that the female golfers had a larger trunk and pelvis rotation than the male golfers, which corresponds to our results [8]. Another study reported that the pelvis of male golfers rotated less in a complete golf swing cycle due to their poor muscular and articular flexibility [4]. The greater ROM values of the male golfers during the downswing are due to their improved strength of physical structures related to the increased physiological cross-sectional areas of muscles [7, 31]; this allows high peak angular velocity of the lumbar spine at the impact stage.
Few studies have been carried out that evaluate lower limb kinematics and kinetics during a golf swing. In this study, it was found that the hip joint connecting the pelvis and femur has a clear role in hip rotational movement, showing significant differences between male and female golfers. For the lead hip-lumbar spine coordination, it was found that in male golfers, the lead hip has a dominant influence on the rotation at the beginning of the downswing, while in the female golfers, the lead hip and lumbar spine joints dominated the rotational movement (Fig. 3a). This gender difference can be interpreted as due to the remaining opposite side rotation of the lumbar spine of the female golfers at the beginning of the downswing, which attenuates the rotation of the lead hip joint. While this result was also observed in the male golfers, it was significant in females for up to about 40% of rotation at the initial downswing (Fig. 2a) due to the female articular and muscular flexibility. While this flexibility facilitates a smooth golf swing, the remaining excessive rotation of the opposite direction did little to contribute to increase the clubhead speed at impact. Because the rotation of the hip joint at the initial downswing has an important role in increasing the clubhead speed at impact [14], a proper hip rotation strategy as well as muscular flexibility are needed for a successful swing shot. For the coordination between the trail hip and lumbar spine, male golfers demonstrated a similar contribution for rotation, while the female golfers did not show typical coordination patterns. In addition, both groups demonstrated the different coordination characteristics between lead hip–lumbar spine and trail hip–lumbar spine (Fig. 3b). It is considered that no typical coordination strategies are made between the trail hip and lumbar spine compared to those between the lead hip and lumbar spine. In other words, various coordination strategies are available for the rotation between the trail hip and lumbar spine. Therefore, training for unskilled golfers should be provided to improve the coordination patterns between the lead hip and lumbar spine joint of skilled golfers. In particular, male golfers should focus on strengthening lower limb joint muscles due to the greater usage of lead hip joint rotation, while the practice program of female golfers includes retaining of muscle suppleness of shoulder and spine joint against excessive rotations of lumbar spine. In addition, golf coaches should recognize that less regulated movement pattern of the trail hip joint will be performed due to the flexible coordination strategies between trail hip and lumbar spine.
Out-of-phase status for inter-joint coordination between hip and lumbar spine joints was observed in the female golfers throughout the downswing phase compared to the male golfers (Fig. 4a and Table 4). This is caused by the lumbar spine rotation opposite the lead and trail hip joints at the initial stage of downswing. The difference in MARP between the lead and trail hips can be interpreted as a result of different mechanical demands in both hip joint rotations. It has been reported that the role of the lead hip differs from that of the trail hip during golf swings [13]. Complex out-of-phase coordination patterns were observed for the lead hip joint, acting as a rotation axis during the downswing, because the center of mass shifts from right (trail) to left (lead) [32, 33]. In terms of coordination variability, male golfers demonstrated a more typical and stable swing strategy than that of female golfers (Fig. 4b). Human neuromechanical processes involve three stages: localization defined as the target and end effects, motor planning, and motor execution to perform the task-based movements [34]. In golf, coordination variability has been reported to occur in the final stage of motor execution [1], and male golfers are more likely to perform a typical movement strategy in the final phase of motor execution than during localization and movement planning. On the contrary, the female group showed more flexible and various rotational coordination between the lead hip and lumbar spine.
This study only focused on evaluating the inter-joint coordination between hips and the lumbar spine during the golf downswing of male and female golfers. Because mechanical differences between male and female skilled golfers were observed to depend on various factors such as flying ball, swing club, kinematics, and kinetics of golfers, further research will be needed to identify gender-specific swing characteristics. Additionally, coordination analysis of golfers who have experienced musculoskeletal disorders of the lumbar spine or hip joints will be necessary for the evaluation of injury mechanisms as a future study.
5 Conclusions
In this study, male and female skilled golfers showed clearly different swing mechanisms from the inter-joint coordination between the hips and lumbar spine perspective. Male golfers typically used their lead hip more than their lumbar spine during the early downswing, while the rotational contribution of the lumbar spine and lead hip in female golfers were comparable until the middle of the downswing phase. This results from the opposite rotation of the lumbar spine for even the early downswing phase due to the muscular and articular flexibility of female golfers. Additionally, male golfers showed a typical and stable coordination variability, while female golfers showed more flexibility in controlling their inter-joint coordination properly during downswings. This study has the potential to help develop gender-specific coaching materials for the improvement of swing skills.
References
Horan, S. A., Evans, K., & Kavanagh, J. J. (2011). Movement variability in the golf swing of male and female skilled golfers. Medicine and Science in Sports and Exercise, 43(8), 1474–1483.
Beak, S. H., Choi, A., Choi, S. W., Oh, S. E., Mun, J. H., Yang, H., et al. (2013). Upper torso and pelvis linear velocity during the downswing of elite golfers. Biomedical Engineering Online, 12(1), 13.
Choi, A., Sim, T., & Mun, J. H. (2016). Improved determination of dynamic balance using the centre of mass and centre of pressure inclination variables in a complete golf swing cycle. Journal of Sports Science, 34(10), 906–914.
Egret, C. I., Nicolle, B., Dujardin, F. H., Weber, J., & Chollet, D. (2006). Kinematic analysis of the golf swing in men and women experienced golfers. International Journal of Sports Medicine, 27(6), 463–467.
McCarroll, J. R., & Gioe, T. J. (1982). Professional golfers and the price they pay. Physician and Sportsmedicine, 10, 54–70.
Zheng, N., Barrentine, S. W., Fleisig, G. S., & Andrews, J. R. (2008). Swing kinematics for male and female pro golfers. International Journal of Sports Medicine, 29(12), 965–970.
Jobe, F. W., Perry, J., & Pink, M. (1989). Electromyographic shoulder activity in men and women professional golfers. American Journal of Sports Medicine, 17(6), 782–787.
Horan, S. A., Evan, K., Morris, N. R., & Kavanagh, J. J. (2010). Thorax and pelvis kinematics during the downswing of male and female skilled golfers. Journal of Biomechanics, 43(8), 1456–1462.
Sinclair, J., Currigan, G., Fewtrell, D. J., & Tralor, P. J. (2017). Biomechanical correlates of club-head velocity during the golf swing. International Journal of Performance Analysis in Sport, 14(1), 54–63.
Choi, A., Joo, S. B., Oh, E., & Mun, J. H. (2014). Kinematic evaluation of movement smoothness in golf: Relationship between the normalized jerk cost of body joints and the clubhead. Biomedical Engineering Online, 13(1), 20.
Meister, D. W., Ladd, A. L., Butler, E. E., Zhoa, B., Rogers, A. P., Ray, C. J., et al. (2011). Rotational biomechanics of the elite golf swing: Benchmarks for amateurs. Journal of Applied Biomechanics, 27(3), 242–251.
Myers, J., Lephart, S., Tsai, Y. S., Sell, T., Smoliga, J., & Jolly, J. (2008). The role of upper torso and pelvis rotation in driving performance during the golf swing. Journal of Sports Sciences, 26(2), 181–188.
Mun, F., Suh, S. W., Park, H. J., & Choi, A. (2015). Kinematic relationship between rotation of lumbar spine and hip joints during golf swing in professional golfers. Biomedical Engineering Online, 14(1), 41.
Choi, A., Lee, I. K., Choi, M. T., & Mun, J. H. (2016). Inter-joint coordination between hips and trunk during downswings: Effects on the clubhead speed. Journal of Sports Science, 34(20), 1991–1997.
Horton, J. F., Lindsay, D. M., & Macintosh, B. R. (2001). Abdominal muscle activation of elite male golfers with chronic low back pain. Medicine and Science in Sports and Exercise, 33(10), 1647–1654.
Keogh, J. W., & Hume, P. A. (2012). Evidence for biomechanics and motor learning research inmproving golf performance. Sports Biomechanics, 11(2), 288–309.
Lu, T. W., Yen, H. C., & Chen, H. L. (2008). Comparisons of the inter-joint coordination between leading and trailing limbs when crossing obstacles of different heights. Gait & Posture, 27(2), 309–315.
Scholz, J. P. (1990). Dynamic pattern theory-some implications for therapeutics. Physical Therapy, 70(12), 827–843.
Sung, P. S. (2014). A kinematic analysis for shoulder and pelvis coordination during axial trunk rotation in subjects with and without recurrent low back pain. Gait & Posture, 40(4), 493–498.
Chardonnens, J., Favre, J., Cuendet, F., Gremjon, G., & Aminian, K. (2013). Characterization of lower-limbs inter-segment coordination during take-off extension in ski jumping. Human Movement Science, 32(4), 741–752.
Chiu, S. L., Chang, C. C., Dennerlein, J. T., & Xu, X. (2015). Age-related differences in inter-joint coordination during stair walking transitions. Gait & Posture, 42(2), 152–157.
Bernstein, N. A. (1967). The coordination and regulation of movements. Oxford: Pergamon Press.
Shemmell, J., Tresilian, J. R., Riek, S., Barry, B. K., & Carson, R. G. (2005). Neuromuscular adaptation during skill acquisition on a two degree-of-freedom target-acquisition task: Dynamic movement. Journal of Neurophysiology, 94(5), 3058–3068.
Gatt, C. J., Pavol, M. J., Parker, R. D., & Grabiner, M. D. (1998). Three-dimensional knee joint kinetics during a golf swing. Influences of skill level and footwear. American Journal of Sports Medicine, 26(2), 285–294.
Choi, A., Sim, T., & Mun, J. H. (2015). Quasi-stiffness of the knee joint in flexion and extension during the golf swing. Journal of Sports Science, 33(16), 1682–1691.
Davis, R. B., Ounpuu, S., Tyburski, D., & Gage, J. R. (1991). A gait analysis data collection and reduction technique. Human Movement Science, 10(5), 575–587.
Choi, A. R., Yun, T. S., Lee, K. S., Min, K. K., Hwang, H., Lee, K. Y., et al. (2009). Asymmetric loading of erector spinae muscles during sagittally symmetric lifting. Journal of Mechanical Science and Technology, 23(1), 64–74.
Choi, A., Yun, T. S., Suh, S. W., Yang, J. H., Park, H., Lee, S., et al. (2013). Determination of input variables for the development of a gait asymmetry expert system in patients with idiopathic scoliosis. International Journal of Precision Engineering and Manufacturing, 14(5), 811–818.
Byrne, J. E., Stergiou, N., Blanke, D., Houser, J. J., Kurz, M. J., & Hageman, P. A. (2002). Comparison of gait patterns between young and elderly women: An examination of coordination. Perceptual and Motor Skills, 94(1), 265–280.
Kadaba, M. P., Ramakrishnan, H. K., Wootten, M. E., Gainey, J., Gorton, G., & Cochran, G. V. B. (1989). Repeatability of kinematic, kinetic, and electromyographic data in normal adult gait. Journal of Orthopaedic Research, 7(6), 849–960.
Abe, T., Kearns, C. F., & Fukunaga, T. (2003). Sex differences in whole body skeletal muscle mass measured by magnetic resonance imaging and its distribution in young Japanese adults. British Journal of Sports Medicine, 37, 436–440.
Okuda, I., Armstrong, C. W., Tsunezumi, H., & Yoshiike, H. (2002). Biomechanical analysis of professional golfer’s swing: Hidemichi Tanaka. Science and Golf, IV, 18–27.
Stemm, J. D., Jacobson, B. H., & Royer, T. D. (2006). Comparison of stability and weight shift among golfers grouped by skill level. Perceptual and Motor Skills, 103(3), 685–692.
Van Beers, R. J., Haggard, P., & Wolpert, D. M. (2004). The role of execution noise in movement variability. Journal of Neurophysiology, 91(2), 1050–1063.
Acknowledgements
This research was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIP) (No. NRF-2016R1A2B3009013).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Choi, A., Lee, K.Y., Lee, S. et al. Gender-Specific Kinematics for Rotational Coordination Between Hips and Lumbar Spine During Downswing. J. Med. Biol. Eng. 39, 596–604 (2019). https://doi.org/10.1007/s40846-018-0439-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40846-018-0439-1