
Abstract
The implementation of a sensory feedback system is particularly important in upper limb prosthesis to improve closed-loop control and prosthesis acceptance. Restoring the touch sensations of individual fingers becomes critical in increasing the sense of embodiment of the artificial limb. Vibrotactile feedback appears as a feasible route to provide useful sensory feedback to prosthesis users. Most studies evaluate the stimulation of the forearm as a potential location of the sensory feedback system. However, it is also necessary to evaluate the stimulation of the upper arm to provide feedback to above-elbow amputees. In this work, the ability of 30 able-bodied subjects to discriminate vibrotactile stimulations in the biceps was evaluated. Particularly, experiments were conducted to evaluate their ability to discriminate different stimulation sites and different stimulation patterns. Stimulation sites were associated to tactile feedback from individual fingers of a virtual hand whereas simulation patterns were associated to potential grasping configurations of the hand. To compare the results, the same experiments were performed on the forearm. The results showed that subjects discriminated finger’s tactile feedback with about 94% average accuracy and grasping pattern feedback with about 85% average accuracy. The special acuity observed in the upper arm suggests that vibrotactile stimulation may also provide suitable feedback for restoring tactile sensation in above elbow amputees.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Over the years, various types of upper limb prostheses have been developed for restoring the motor function allowing prosthetic users to perform tasks that otherwise would be impossible [1]. However, surveys and workshops centered on prosthetic user needs revealed that there still are several limitations significantly affecting the acceptance of modern prosthesis [2, 3]. One of the main limitations is the lack of an appropriate feedback system for restoring the sensory function. For this reason, in the last years researchers increased the amount of studies focused on understanding the natural sensory feedback system and on determining appropriate alternatives for providing artificial sensory information to the users [4,5,6,7].
Direct nerve stimulation through implanted microelectrodes was proposed as an interface to provide natural sensory feedback to amputees [8]. Arrays of microelectrodes are surgically placed in direct contact with stump nerves corresponding to the afferent pathway. Proper stimulation through these electrodes can cause amputees to perceive real touch and proprioceptive sensations referred to their phantom hand. Clinical trials showed that this feedback modality helped amputees to improve object manipulation tasks and increase self-confidence [9,10,11]. Implementing a neural stimulation device that works outside the laboratory is a complex engineering challenge that may require decades to be accomplished.
In current prosthesis, the short-term realization of sensory feedback requires unobtrusive, comfortable and easy-to-implement alternatives. Different non-invasive feedback systems were proposed in the literature to close the loop in myoelectric prosthesis by delivering sensory information to subjects. Grasping force is the most common variable coded to feedback because it is difficult to assess through vision. Hand aperture, object stiffness, slippage, and finger position are other sensory variables transferred to users for improving their ability to control the prosthesis. Sensory information is typically provided through interfaces based on mechanotactile, electrotactile and vibrotactile stimulation [12,13,14]. Sensory feedback through mechanotactile stimulation is referred to as modality-matching feedback due to the fact that the sensory variable measured in the prosthesis is coded and transferred to the subject in the same modality. For example, the grasping force is transferred to the subject as force by applying pressure on the skin using servomotors [14]. This sensory substitution method provides more intuitive feedback than vibro- and electrotactile feedback; however, it is more burdensome and may be difficult to integrate into a prosthetic device.
Sensory feedback through vibro- and electrotactile stimulations is referred to as modality-mismatching feedback due to the fact that the sensory variable measured in the prosthesis is coded and transferred to the subject in a different modality. For example, either an electric current or a mechanical vibration is applied on the subject’s skin to code information about grasping force [6]. Electrotactile stimulation consists in delivering electric current to the surface of the skin through either single or multichannel electrodes [15,16,17,18]. Sensory information is conveyed by an independent modulation of the stimulation parameters, i.e. pulse width, amplitude and frequency of the pulse and stimulus location [19,20,21]. The implementation of electrotactile interfaces on myoelectric prosthesis is suitable due to their low power consumption, fast response and compact design. The limitation of this approach is that the perceived sensations may become uncomfortable to the user. It also represents an interference to electromyography (EMG) signal recording, which may strongly affect the control of the myoelectric prosthesis [22].
Vibrotactile stimulation comprise mechanical stimulation of fast adapting mechanoreceptors (Type I and II) using different types of actuators, i.e. linear electromagnetic actuators, rotary electromagnetic actuators and non-electromagnetic actuators [23]. In the field of prosthetics, the sensory information measured in the prosthesis is transferred to the user by modulating amplitude and frequency of vibration, which in some cases cannot be controlled independently. Arrays of coin vibration motors were placed on the forearm both circumferentially and longitudinally to study and determine appropriate stimulation parameters in terms of stimulus modulation and stimulation sites [24]. These motor distributions were used to study different coding strategies to feedback information about level of grasping force [25, 26], hand aperture [27], object slippage [28] and object stiffness [29]. Experiments conducted on able-bodied subjects and amputees showed that vibrotactile feedback improved their performance on virtual grasping and holding tasks [27]. Additionally, a study demonstrated that providing vibrotactile stimulation to phantom finger sites on the residual limb can improve the ability of amputees to discriminate multiple feedback sites [30]. Finally, the usage of a single C2 tactor was investigated as alternative to coin-shaped motors to provide vibrotactile feedback [31]. This is a more complex type of stimulator that allows certain independence in the control of the amplitude and frequency of vibrations. Experiments on able-bodied subjects suggested that the modulation of vibration amplitude provides superior grasping force feedback during virtual object manipulation tasks [31] Additionally, an appropriate training on vibrotactile feedback is required to increase the ability of subjects to perform object manipulation tasks [32, 33].
The reviewed literature shows that most of the works are focused on vibrotactile feedback for transradial amputees. However, it is also interesting to understand how transhumeral amputees or people with elbow disarticulation would perform with vibrotactile feedback. The objective of this study was to determine the ability of subjects to recognize vibrotactile feedback applied to the surface of their biceps. Specifically, the effectiveness of stimulating the upper arm was compared with respect to the forearm. The methodology consisted of experiments conducted on able-bodied subjects to evaluate their ability to discriminate different stimulation sites (spatial coding) and different stimulation patterns (spatial and amplitude coding). Stimulation sites were associated to tactile feedback from individual fingers of a virtual hand, whereas simulation patterns were associated to potential grasping configurations of the hand. Results of the experiments indicated that the ability of subjects to discriminate stimulation sites was significantly higher than their ability to discriminate stimulation patterns. Additionally, no statistically significant differences were found in discrimination accuracy between upper arm and forearm. Providing tactile feedback about the sensory state of individual fingers is particularly important as it could help amputees to increase the sense of embodiment of the prosthesis, and hence the functionality of the prosthetic hand could be increased.
2 Methods
2.1 Vibrotactile feedback
Non-invasive vibrotactile stimulation was provided using coin-shaped vibration motors having a diameter of 10 mm and a thickness of 3.4 mm (Precision Microdrives Ltd, UK). Their main advantages are the low costs and the small size and weight, allowing an unobtrusive and simple mounting into a prosthetic socket [25]. An array of three coin motors was located on the anterior part of the biceps at a fixed distance from the elbow, using a custom-made fabric sleeve. Motors were positioned following a diagonal line with a separation between motors of 4 cm in the proximal-distal direction and 4 cm in the lateral-medial direction (Fig. 1, top). Literature showed that subjects can accurately discriminate vibrotactile stimuli, for different orientations of the stimulator array in the forearm, when the distance between stimulators is about 4 cm [34]. The array of motors was later placed on the subject’s forearm to compare the discrimination abilities at both locations (Fig. 1, bottom). Each motor in the array provided information about the sensory state of a specific finger on a virtual hand. Sites S1, S2, and S3 (Fig. 1) were associated to the sensory state of the thumb, index and middle fingers, respectively. In this study, two sensory states (ON/OFF) were simulated on each site. In the ON condition (i.e. finger in contact with an object), the motors were activated to produce 1 s of constant vibration at approximately 225 Hz. In the OFF condition (i.e. no feedback) the motors were turned off.

Location of the vibration motors in the anterior part of the biceps (top) and forearm (bottom)
2.2 Data Collection
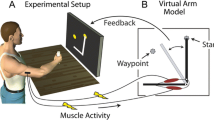
A total of 30 able-bodied subjects volunteered for this study (9 females and 21 males, mean age (SD) 27.7 (± 9.6) years). The Ethical Committee of the National University of Río Cuarto approved this study. Informed consent was obtained from all subjects included in this study. Subjects participated in an experimental session, where they were seated comfortably with the dominant arm in a resting position (Fig. 2). Subjects wore earmuffs throughout the experiment to avoid any auditory cue associated to the motor sound that could help them to discriminate vibration sites or patterns. A custom-made software application was developed to generate a vibration stimulus and its corresponding visual cue. The delay between vibrotactile and visual feedback was kept less than 300 ms to avoid a perceivable delay between both feedback conditions that may affect the results [35].

Setup of the experiment performed to evaluate the ability of subjects to discriminate different vibrotactile stimulations
2.3 Experimental Procedure
The experimental session was divided into two parts. In each part, a training period was implemented to help subjects to adapt to the system and to learn to interpret vibrotactile feedback [32]. The first part consisted in discriminating the site of a stimulus (S1, S2, and S3). It started with a training stage in which 45 vibrotactile stimuli (15 for each site) were randomly provided to the subject while he/she was looking at the computer screen for receiving visual feedback. In this part of the experiments, the visual cue was a picture of the anterior part of an open human hand in which the finger being stimulated was highlighted while the vibrotactile feedback was provided. In this stage, subjects learned to associate each finger with the corresponding stimulation site. Next, in the validation stage, a new set of 45 vibrotactile stimuli (15 for each site) was randomly provided to subjects without visual feedback. After each stimulus, subjects determined which site was stimulated and the experimenter either validated or corrected the answer. This stage allowed subjects to strengthen the finger–stimulus site association. Finally, in the testing stage, 45 vibrotactile stimuli (15 for each site) where randomly provided to the subject, who was asked to infer which finger was stimulated having neither visual nor experimenter feedback.
The second part of the experiment consisted in discriminating three different stimulation patterns associated with different grasping configurations of the virtual hand. These stimulation patterns were obtained by combining multiple stimulation sites. For lateral grasping configuration, the stimulus was presented as S1-ON, S2-OFF and S3-OFF (i.e. only the site corresponding to the thumb was stimulated). For pinch grasping, the stimulus was presented as S1-ON, S2-ON and S3-OFF (i.e. thumb and index fingers were stimulated simultaneously). Finally, cylindrical grasping was presented as S1-ON, S2-ON and S3-ON (thumb, index and middle fingers were stimulated simultaneously). In this part of the experiment, the visual cue was a set of pictures of a human hand showing each grasping configuration (see computer screen in Fig. 2). The picture frame was highlighted to indicate which grasping configuration corresponded to the stimulation pattern provided to the subject. As in the experiments for discrimination of stimulation sites, training and validation stages were implemented to help subjects to learn and reinforce the association between grasping configurations and stimulation patterns. Finally, in the testing stage subjects were asked to infer which grasping configuration was stimulated having neither visual nor experimenter feedback. A total of 45 stimuli were randomly provided to subject during each stage (15 stimuli for each pattern).
The experimental procedure described above was repeated with the vibration motors located on the anterior part of the forearm to compare the discrimination abilities of subjects at both locations.
2.4 Data Analysis
Subject’s answers for the validation and testing stages were logged into a datasheet and saved for analysis. Discrimination accuracy was the metric used to evaluate the performance of subjects in the experiments. Accuracy was defined as the number of correct answers stated by subjects divided by the total number of the presented stimuli. Balanced two-way analysis of variance (ANOVA) was performed to evaluate the differences in discrimination accuracy over the experimental conditions. In the first analysis, the arm location for the vibrotactile stimulation (biceps-vs-forearm) and the experimental stage (validation-vs-testing) were evaluated. In another analysis, the stimuli locations and the discrimination tasks (individual finger vs. grasping pattern) were the evaluated factors. Post hoc analysis on specific differences was done using the Student t test. A significance level of 5% was selected in all cases.
3 Results
As regards the identification of stimulation sites, results showed that the average discrimination accuracy (± SD) in the validation stage in the biceps was 94.1 ± 6.2% and in the forearm was 93.7 ± 5.9%. In the testing stage, the average accuracy in the biceps was 93.9 ± 6.5% and in the forearm 92.1 ± 9.0%. ANOVA analysis showed no significant differences between the results of the experimental stages (validation and testing, p = 0.471) and between the results of arm location (biceps and forearm, p = 0.403). It also showed no significant interaction in the effects of the two factors on the discrimination accuracy (p = 0.624).
In the experiments involving the identification of stimulation patterns, subjects achieved an average accuracy in the validation stage of 84.1 ± 10.1% in the biceps and 81.3 ± 12.3% in the forearm. In the testing stage, the average accuracy in the biceps was 85.0 ± 10.9% and in the forearm 82.1 ± 11.0%. The ANOVA analysis indicated no significant differences in the discrimination accuracy between validation and testing stages (p = 0.675) and between biceps and forearm locations (p = 0.151). No significant interaction effects of experimental stage and arm location factors on the discrimination accuracy were found either (p = 0.985).
Figure 3 presents boxplots that illustrate the distribution of subject’s answers for identifying stimulation sites and stimulation patterns during the testing stage. As regards discrimination of stimulation site, 67% of the subjects obtained accuracies greater than 95% in the biceps whereas only 53% of subjects achieved more than 95% accuracy in the forearm. Although no statistically significant differences were found, the results may indicate that participants had more difficulties for discriminating stimulation sites in the forearm than in the biceps. Considering the discrimination of stimulation patterns, the average accuracy in the biceps and in the forearm dropped significantly with respect to the discrimination accuracy for stimulation site (p = 0.0003 in the biceps and p = 0.0002 in the forearm).

Boxplot that shows the distribution of the accuracy of subjects responses for individual finger and grasping pattern discrimination. Dashed line inside the box represents the mean value
A more detailed illustration of the results is presented in Figs. 4 and 5. Figure 4 shows the confusion tables generated from all subject’s answers during the testing stage of the stimulation site discrimination experiment. The main diagonal of the tables (dark gray boxes) depicts the number of correct answers over a total of 450 for each site (30 subjects and 15 stimuli per site). The remaining elements (white boxes) correspond to the incorrect answers. In both locations (biceps and forearm), the incorrect answers were mainly caused by subjects confusing adjacent sites. Site S2 (motor in the center of the array) presented the lower discrimination accuracy.

Confusion matrix showing the results for site discrimination. The last column and the last row of each matrix represent the true positive rates and the discrimination accuracy for each finger, respectively. Bottom right box represents the average accuracy

Confusion matrix showing the results for stimulation pattern discrimination. The last column and the last row of each matrix represent the true positive rates and the discrimination accuracy for each finger respectively. Bottom right box represents the average accuracy
Figure 5 shows the confusion table for the testing stage of the stimulation pattern discrimination. Also in this task, most of the incorrect answers were caused by subjects confusing “adjacent” stimulation patterns. That is, since the patterns were directly related to the number of active motors, when missing, subjects confused whether 1 or 2 motors were active or whether 2 or 3 motors were active. However, subjects hardly ever confused when 1 or 3 motors were active.
4 Discussion and Conclusion
In upper-limb prosthesis, the implementation of a sensory feedback system is extremely important to achieve an intuitive control and, most importantly, to increase the sense of embodiment of the prosthesis. Artificial tactile sensations can be generated by connecting sensors placed on the fingertips of an artificial hand to electrical/mechanical stimulators placed on the residual limb. Such actuators can be instantaneously activated, with different levels of intensity, when subjects touch and grasp objects. This will stimulate the skin’s mechanoreceptors in the residual limb inducing touch sensations in the brain as if they originated from the artificial hand. In this work, the implementation of vibrotactile feedback to restore tactile sensations on the upper arm was investigated. Particularly, the ability of subjects to identify different stimulation sites and different stimulation patterns was evaluated. An accurate discrimination of stimulation sites would help amputees to receive information about the sensory state of individual fingers of the artificial hand. This information would help them to identify which fingers are touching an object and what level of force is being applied to that object during manipulation tasks, thus increasing the prosthesis embodiment.
Results of the site discrimination experiments showed that subjects presented a high level of discrimination accuracy. They also showed that there were no significant differences in the accuracies observed in the biceps and in the forearm. An explanation for this may be found from a physiological point of view. Each coin motor stimulated a specific location on the skin, activating the skin’s mechanoreceptors and generating a sensory signal that travelled through afferent pathways to the somatosensory cortex that decoded the signal. The density of mechanoreceptors in the region of stimulation plays an important role in the perception of the vibrotactile stimuli and, most importantly, in the spatial resolution [36]. The density of these receptors is similar in the upper arm and the forearm [37]. This may be a possible reason for not finding significant differences in the discrimination results at both locations.
The accuracy values obtained in this study for spatial discrimination were comparable to the results observed in previous studies. In [38], authors presented an array of 5 servomotors to provide mechanotactile stimulation to the forearm of amputees and able-bodied subjects. Amputees achieved an average accuracy of 75.2% in identifying five different stimulation locations whereas able-bodied participants achieved 89.6%. In [31] and [33], vibrotactile stimulation was provided to the biceps of participants using a single actuator to determine appropriate stimulation parameters. However, the spatial acuity of subjects was not evaluated in those studies. In [20], subjects identified four movements of a prosthetic finger with 95.6% of accuracy using a multichannel electrotactile feedback system (in the forearm). In [12], two electrotactile coding schemes (spatial and mixed) were evaluated for transferring 15 levels of grasping force to the forearm of able-bodied subjects. The mixed coding (frequency and spatial) scheme presented the highest discrimination level (87%). The presented results corresponded to psychometric tests, which only evaluated the capacity of subjects to discriminate different stimulation modalities. They constitute the first step towards the development of a sensory feedback system, which would have to be evaluated on closed-loop control tasks to understand and evaluate its performance [12].
On the other hand, the ability of subjects to discriminate grasping patterns dropped significantly with respect to their ability to discriminate sites. This behavior was observed at both stimulation locations (biceps and forearm). A potential reason may be that stimulation patterns involved the activation of more than one vibration motor (sites) at the same time. A vibrotactile stimulus with 1 active motor was felt by subjects as a vibration of a pure tone whereas a stimulus with 2 or 3 active motors was felt as repeated beats due to a phase shift between motors caused by small differences in the amplitude and frequency of vibration of each motor. Such differences produced stimuli with similar amplitude that may have been hard to distinguish. As a result, subjects were able to accurately discriminate 1-motor stimuli but they presented difficulties to distinguish stimuli produced by 2 o 3 active motors.
This paper contributes to the field of prosthetics and haptics by showing that the upper arm may be a suitable location to provide vibrotactile stimulation for restoring the sense of touch. The experiments on able-bodied subjects revealed that the spatial acuity on the biceps was not significantly different with respect to the spatial acuity in the forearm, location most commonly studied in the literature. This result would help to increase the population of prosthetic users who can receive and interpret sensory feedback by including people with either transhumeral amputation or elbow disarticulation. Integrating a sensory feedback system into the upper-limb prosthesis is extremely important as it helps people to increase the functionality of their prostheses and hence reduce device abandonment [2].
During the experiments, a fixed distribution of actuators was used to stimulate different sites in the biceps of able-bodied subjects. This may constitute a limitation of this study because amputees may have a limited space in their residual for providing tactile feedback. Thus, the number and location of the actuators would depend on the physiology of the residual limb. Previous studies showed that transradial amputees may present a phantom map of the hand, which allows finding specific sites in their residual limb that correspond to the phantom fingers [30, 39]. Moreover, another study demonstrated that the stimulation of skin areas without phantom sensations could potentially help the development of phantom finger sensations in the residual limb [40]. In above elbow amputees, further studies are required to determine if they present the phantom map of the missing hand or if it can be developed with appropriate stimulation. Thus, future work will be focused on evaluating vibrotactile feedback on upper arm amputees to find potential stimulation sites for restoring tactile sensations of individual fingers. Additionally, future studies will seek to determine whether restoring individual finger sensations through vibrotactile stimulation would help subjects to improve their ability to perform daily living activities.
References
Micera, S., Carpaneto, J., & Raspopovic, S. (2010). Control of hand prostheses using peripheral information. IEEE Reviews in Biomedical Engineering, 3, 48–68. https://doi.org/10.1109/RBME.2010.2085429.
Peerdeman, B., Boere, D., Witteveen, H., in ’t Veld, R. H., Hermens, H., Stramigioli, S., et al. (2011). Myoelectric forearm prostheses: State of the art from a user-centered perspective. Journal of Rehabilitation Research and Development, 48(6), 719–737.
Pylatiuk, C., Schulz, S., & Döderlein, L. (2007). Results of an internet survey of myoelectric prosthetic hand users. Prosthetics and Orthotics International, 31(4), 362–370.
Lundborg, G., & Rosén, B. (2001). Sensory substitution in prosthetics. Hand clinics, 17(3), 481–488, ix–x.
Johansson, R. S., & Flanagan, J. R. (2009). Coding and use of tactile signals from the fingertips in object manipulation tasks. Nature Reviews Neuroscience, 10(5), 345–359. https://doi.org/10.1038/nrn2621.
Antfolk, C., D’Alonzo, M., Rosén, B., Lundborg, G., Sebelius, F., & Cipriani, C. (2013). Sensory feedback in upper limb prosthetics. Expert Review of Medical Devices, 10(1), 45–54. https://doi.org/10.1586/erd.12.68.
Li, K., Fang, Y., Zhou, Y., & Liu, H. (2017). Non-invasive stimulation-based tactile sensation for upper-extremity prosthesis: A review. IEEE Sensors Journal, 17(9), 2625–2635. https://doi.org/10.1109/JSEN.2017.2674965.
Tyler, D. J. (2016). Creating a prosthetic hand that can feel. IEEE Spectrum, 53(5 (INT)), 24–29.
Ortiz-Catalan, M., Håkansson, B., & Brånemark, R. (2014). An osseointegrated human-machine gateway for long-term sensory feedback and motor control of artificial limbs. Science Translational Medicine, 6(257), 257re6–257re6. https://doi.org/10.1126/scitranslmed.3008933.
Raspopovic, S., Capogrosso, M., Petrini, F. M., Bonizzato, M., Rigosa, J., Di Pino, G., et al. (2014). Restoring natural sensory feedback in real-time bidirectional hand prostheses. Science Translational Medicine, 6(222), 222ra19–222ra19. https://doi.org/10.1126/scitranslmed.3006820.
Schiefer, M., Tan, D., Sidek, S. M., & Tyler, D. J. (2016). Sensory feedback by peripheral nerve stimulation improves task performance in individuals with upper limb loss using a myoelectric prosthesis. Journal of Neural Engineering, 13(1), 016001. https://doi.org/10.1088/1741-2560/13/1/016001.
Dosen, S., Markovic, M., Strbac, M., Belic, M., Kojic, V., Bijelic, G., et al. (2017). Multichannel electrotactile feedback with spatial and mixed coding for closed-loop control of grasping force in hand prostheses. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 25(3), 183–195. https://doi.org/10.1109/TNSRE.2016.2550864.
Kim, K., Colgate, J. E., Santos-Munne, J. J., Makhlin, A., & Peshkin, M. A. (2010). On the design of miniature haptic devices for upper extremity prosthetics. IEEE/ASME Transactions on Mechatronics, 15(1), 27–39. https://doi.org/10.1109/TMECH.2009.2013944.
Antfolk, C., Balkenius, C., Lundborg, G., Rosén, B., & Sebelius, F. (2010). A tactile display system for hand prostheses to discriminate pressure and individual finger localization. Journal of Medical and Biological Engineering, 30(6), 355–360.
Kaczmarek, K. A., Webster, J. G., Bach-y-Rita, P., & Tompkins, W. J. (1991). Electrotactile and vibrotactile displays for sensory substitution systems. IEEE Transactions on Biomedical Engineering, 38(1), 1–16. https://doi.org/10.1109/10.68204.
Liu, W., & Tang, H. (2005). An initial study on lip perception of electrotactile array stimulation. Journal of Rehabilitation Research and Development, 42(5), 705–713. https://doi.org/10.1682/JRRD.2005.02.0051.
Krueger, E., Da, C., Scheeren, E. M., & Nohama, P. (2014). Electrical and mechanical technologies in sensory system feedback and control: Cybernetics in physical rehabilitation. Journal of Control, Automation and Electrical Systems, 25(4), 413–427. https://doi.org/10.1007/s40313-014-0121-y.
Li, C.-M., Lee, H.-Y., Hsieh, S.-H., Wang, T.-G., Wang, H.-P., & Chen, J.-J. J. (2016). Development of innovative feedback device for swallowing therapy. Journal of Medical and Biological Engineering, 36(3), 357–368. https://doi.org/10.1007/s40846-016-0146-8.
Xu, H., Zhang, D., Huegel, J. C., Xu, W., & Zhu, X. (2016). Effects of different tactile feedback on myoelectric closed-loop control for grasping based on electrotactile stimulation. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 24(8), 827–836. https://doi.org/10.1109/TNSRE.2015.2478153.
Patel, G. K., Dosen, S., Castellini, C., & Farina, D. (2016). Multichannel electrotactile feedback for simultaneous and proportional myoelectric control. Journal of Neural Engineering, 13(5), 056015. https://doi.org/10.1088/1741-2560/13/5/056015.
Schweisfurth, M. A., Markovic, M., Dosen, S., Teich, F., Graimann, B., & Farina, D. (2016). Electrotactile EMG feedback improves the control of prosthesis grasping force. Journal of Neural Engineering, 13(5), 056010. https://doi.org/10.1088/1741-2560/13/5/056010.
Hartmann, C., Došen, S., Amsuess, S., & Farina, D. (2015). Closed-loop control of myoelectric prostheses with electrotactile feedback: Influence of stimulation artifact and blanking. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 23(5), 807–816. https://doi.org/10.1109/TNSRE.2014.2357175.
Choi, S., & Kuchenbecker, K. J. (2013). Vibrotactile display: Perception, technology, and applications. Proceedings of the IEEE, 101(9), 2093–2104. https://doi.org/10.1109/JPROC.2012.2221071.
D’Alonzo, M., Cipriani, C., & Carrozza, M. C. (2011). Vibrotactile sensory substitution in multi-fingered hand prostheses: Evaluation studies. In 2011 IEEE international conference on rehabilitation robotics (ICORR) (pp. 1–6). https://doi.org/10.1109/icorr.2011.5975477.
Pylatiuk, C., Kargov, A., & Schulz, S. (2006). Design and evaluation of a low-cost force feedback system for myoelectric prosthetic hands. Journal of Prosthetics and Orthotics, 18(2), 57–61. https://doi.org/10.1097/00008526-200604000-00007.
Cipriani, C., D’Alonzo, M., & Carrozza, M. C. (2012). A miniature vibrotactile sensory substitution device for multifingered hand prosthetics. IEEE Transactions on Biomedical Engineering, 59(2), 400–408. https://doi.org/10.1109/TBME.2011.2173342.
Witteveen, H. J., Rietman, H. S., & Veltink, P. H. (2015). Vibrotactile grasping force and hand aperture feedback for myoelectric forearm prosthesis users. Prosthetics and Orthotics International, 39(3), 204–212. https://doi.org/10.1177/0309364614522260.
Walker, J. M., Blank, A. A., Shewokis, P. A., & O’Malley, M. K. (2015). Tactile feedback of object slip facilitates virtual object manipulation. IEEE Transactions on Haptics, 8(4), 454–466. https://doi.org/10.1109/TOH.2015.2420096.
Witteveen, H. J. B., Luft, F., Rietman, J. S., & Veltink, P. H. (2014). Stiffness feedback for myoelectric forearm prostheses using vibrotactile stimulation. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 22(1), 53–61. https://doi.org/10.1109/TNSRE.2013.2267394.
Antfolk, C., D’Alonzo, M., Controzzi, M., Lundborg, G., Rosen, B., Sebelius, F., et al. (2013). Artificial redirection of sensation from prosthetic fingers to the phantom hand map on transradial amputees: Vibrotactile versus mechanotactile sensory feedback. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 21(1), 112–120. https://doi.org/10.1109/TNSRE.2012.2217989.
Stepp, C. E., & Matsuoka, Y. (2012). Vibrotactile sensory substitution for object manipulation: Amplitude versus pulse train frequency modulation. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 20(1), 31–37. https://doi.org/10.1109/TNSRE.2011.2170856.
Stepp, C. E., An, Q., & Matsuoka, Y. (2012). Repeated training with augmentative vibrotactile feedback increases object manipulation performance. PLoS ONE, 7(2), e32743.
Rombokas, E., Stepp, C. E., Chang, C., Malhotra, M., & Matsuoka, Y. (2013). Vibrotactile sensory substitution for electromyographic control of object manipulation. IEEE Transactions on Biomedical Engineering, 60(8), 2226–2232. https://doi.org/10.1109/TBME.2013.2252174.
Witteveen, H. J. B., Droog, E. A., Rietman, J. S., & Veltink, P. H. (2012). Vibro- and electrotactile user feedback on hand opening for myoelectric forearm prostheses. IEEE Transactions on Biomedical Engineering, 59(8), 2219–2226. https://doi.org/10.1109/TBME.2012.2200678.
Farrell, T. R., & Weir, R. F. (2007). The optimal controller delay for myoelectric prostheses. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 15(1), 111–118. https://doi.org/10.1109/TNSRE.2007.891391.
Cholewiak, R. W., & Collins, A. A. (2003). Vibrotactile localization on the arm: Effects of place, space, and age. Perception & Psychophysics, 65(7), 1058–1077. https://doi.org/10.3758/BF03194834.
Goldstein, E. B. (2009). The Cutaneous Sense. In Sensation and perception (8th ed., pp. 329–352). Wadsworth.
Antfolk, C., Cipriani, C., Carrozza, M. C., Balkenius, C., Björkman, A., Lundborg, G., et al. (2012). Transfer of tactile input from an artificial hand to the forearm: Experiments in amputees and able-bodied volunteers. Disability and Rehabilitation: Assistive Technology, 8(3), 249–254. https://doi.org/10.3109/17483107.2012.713435.
Grüsser, S. M., Winter, C., Schaefer, M., Fritzsche, K., Benhidjeb, T., Tunn, P.-U., et al. (2001). Perceptual phenomena after unilateral arm amputation: A pre-post-surgical comparison. Neuroscience Letters, 302(1), 13–16. https://doi.org/10.1016/S0304-3940(01)01606-8.
Chai, G., Zhang, D., & Zhu, X. (2017). Developing non-somatotopic phantom finger sensation to comparable levels of somatotopic sensation through user training with electrotactile stimulation. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 25(5), 469–480. https://doi.org/10.1109/TNSRE.2016.2580905.
Acknowledgements
This work was partially supported by a PID research grant from the Ministry of Industry, Trade, Mining and Technological Development of the province of Córdoba, Argentina. It was also partially supported by a PPI 2016–2018 research Grant from the Science and Technology Secretary, National University of Rio Cuarto. The first and third authors are supported by National Scientific and Technical Research Council (Consejo Nacional de Investigaciones Científicas y Técnicas, CONICET), Argentina.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Fontana, J.M., O’Brien, R., Laciar, E. et al. Vibrotactile Stimulation in the Upper-Arm for Restoring Individual Finger Sensations in Hand Prosthesis. J. Med. Biol. Eng. 38, 782–789 (2018). https://doi.org/10.1007/s40846-018-0374-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40846-018-0374-1