
Abstract
This study investigated the short-term effects of exposure particulate matter (PM10) in Zabol, Iran, from 2013 to 2015. The concentrations of PM10 recorded from 2013 to 2015 were given as the input to the software (AirQ 2.2.3) developed by the World Health Organization (WHO) to estimate the attributed proportion of the health effects and the number of excess cases related to total mortality (TM), cardiovascular mortality (CM), respiratory mortality (RM), hospital admissions due to cardiovascular disease (HACD), and hospital admissions due to respiratory disease (HARD). According to the data, 73 days during 2013–2014 and 144 days during 2014–2015 in Zabol exceeded the National Ambient Air Quality Standards (NAAQS) guideline limits. This finding indicates the impact of the windy period on the ambient air condition of Zabol’s airshed. Moreover, the number of excess cases attributed to TM, CM, RM, HACD, and HARD per 100,000 people was estimated as 182, 96, 18, 94, and 243 individuals during 2013–2014. However, these values increased by about 50% during 2014–2015. This significant level of health effects of PM10 on the residents of Zabol necessitates urgent controlling/management actions to reduce dust storms in this region.
Graphic abstract

Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
One of the most critical environmental risks for human life is air pollution, which threatens human health through acute and chronic effects. According to the World Health Organization (WHO) statistics, about 800,000 people die annually due to respiratory and cardiovascular diseases and lung cancer caused by air pollution throughout the world (WHO 2014). Various air pollutants affect human health, among which fine particles or particulate matters (PMs) can be mentioned, which can penetrate the body through the pulmonary system (Marzouni et al. 2016). Also, as proved in many studies, PMs pose several adverse effects on the cardiovascular and respiratory systems (Khaniabadi et al. 2017; Zallaghi et al. 2014; Naddafi et al. 2012; Jeong 2013).
Various PMs affect health differently due to their different size, concentration, and chemical composition (Marzouni et al. 2016). Hence, PMs are classified based on their size. For instance, PM2.5 and PM10 describe the inhalable particles that their diameters are equal to or smaller than 2.5 µm and 10 µm, respectively. PM2.5 is generally produced by mechanical and physical processes, such as dust resuspension and material smashing and eroding (Marzouni et al. 2016). Generally, PMs might affect almost all urban airsheds, but in a wide range of levels depending on location, climate, transportation, and energy consumption patterns (Marzouni et al. 2016). In recent decades, PM levels have increased in many parts of the world, including Iran, due to the increased frequency of severe dust storms. The increase in PM level can be justified by their capability to travel longer distances during dust storms. Besides, they can carry toxins, influenza viruses, and several pathogenic and non-pathogenic microorganisms, e.g., Mycobacterium, Brucella, Aspergillus, Cladosporium, Coxiella Burnetti, Actinomycetes, Clostridium perfingens, and Bacillus (Khaniabadi et al. 2017).
A case study conducted in Kermanshah, Iran (Marzouni et al. 2016), in 2011 showed that 7.6, 11, 15.1, 13.5, and 7.6% of total mortality (TM), cardiovascular mortality (CM), respiratory mortality (RM), hospital admission for respiratory diseases (HARD), and hospital admission for cardiovascular diseases (HACD), respectively, were caused by short-term exposure to PM10. Also, Goudarzi et al. (2014) attributed about 17% of the total RM, CM, and HARD cases in Ahvaz, Iran, to PM10. On the other hand, a study revealed that frequent dust storms in Zabol, Iran, are due to the high frequency and intensity of northwestern winds (Rashki et al. 2012). Such winds blow 120 days per year, making the summers of Zabol windy and dusty. Hence, storms originate from the lakebeds covering the surrounding villages. Most prevailing winds in this region start from north and northwest and pass over the lakebed of Hamoon (Jamalizadeh et al. 2008). Since the Hamoon lake is dried, the winds can transport airborne PMs and salt particles to Zabol. Such a condition makes Zabol one of the worst cities of Iran regarding the pollution by atmospheric PM10. Therefore, its PM level exceeds the national air quality standards in many days of the year. WHO has introduced Zabol as the most air-polluted city in the world due to its dust storms (Rahnama and Rajabpour 2017; Soleimani and Amini 2017). To improve the atmospheric condition of Zabol and reduce the health effects of PM, these effects should be modeled and studied.
Various models have been developed to evaluate the effect of air pollution on human health concerning epidemiologic results. The developed models have integrated the assessment of relative risk (RR), baseline incidence (BI), and attributable proportion (AP), and reported the results in terms of mortality and morbidity. One of the most popular models is AirQ software developed by the European Centre for Environmental Health of WHO, Bilthoven Division (Miri et al. 2016).
This study aims to model the morbidity and mortality due to exposure to PM10 in Zabol inhabitants using the WHO approach implemented in the AirQ 2.2.3 software.
Materials and methods
Study area
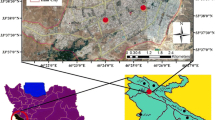
Zabol is the capital of Zabol County in Sistan and Baluchestan province, which shares a border with Afghanistan and has a total area of about 344 km2. This city is positioned in a semi-arid area with an average annual precipitation of 57.7 mm, an average relative humidity of 37%, and an average temperature of 29 °C. The population of this city was 137,722 in 2011 (Sistan and Baluchestan Governorate 2019). Figure 1 shows the location of the studied area in the Sistan and Baluchestan province.

Location of the studied area (Zabol city) in the Sistan and Balouchestan Province, in the southeast of Iran
Air pollution data collection
In the present study, the PM10 concentrations related to two time-periods of 2013–2014 and 2014–2015 were obtained from the Environmental Protection Agency of Zabol. The data were collected by the organization’s air monitoring station that measures different air pollutants, including ambient PM10 based on hourly and daily average. The processed data were given to the AirQ 2.2.3 as input.
AirQ software
The AirQ 2.2.3 software was used to estimate the health effects of exposure to PM10 in Zabol inhabitants. This model assumes an approved causal relationship between exposure to PM10 and the health effects without any confounding effect. The AP values of the health impacts, which are the fraction of health effects in a defined population associated with air pollutant exposure, were calculated as follows:
where RR(c) is the relative risk for a health effect in category c of the exposed pollutants that can be obtained based on the exposure–response functions extracted from epidemiological studies, and P(c) indicates the portion of the population in the c exposure category (Miri et al. 2016).
The rate of the health effects attributable to the exposed population was calculated using the following equation by determining the baseline incidence of the health effects:
Here, IE represents the health effect rate attributed to exposure, and I implies the baseline incidence of the health effect in the exposed population. Considering the size of the studied population, the number of excess cases of the health effects was obtained using:
where NE and N are the number of cases and population size, respectively.
Data processing and exposure assessment
RR values were obtained from the time-series studies, investigating how long-term changes affect pollutant concentration. The model used the default data provided by WHO in the library of the AirQ software due to the lack of systematic studies on the health effect of PM10 in Iran. The values of BI for TM, CM, and RM were obtained from Zabol University of Medical Sciences. For other health implications, the default values of the AirQ software were used.
The PM10 concentrations were classified at 10 µg/m3 intervals concerning their exposure categories. The annual and seasonal mean and maximum values, 98th percentile of PM10, and the number of exposure days were calculated and used as the input data for the modeling software.
Results and discussion
Based on the regulations of National Ambient Air Quality Standards (NAAQS), the annual and daily averages of PM10 concentration are, respectively, 50 and 150 µg/m3 (Hu et al. 2014). The WHO guideline recommends an annual average PM10 of 20 µg/m3 (Khaniabadi et al. 2017). These values are compared with the average, maximum, and minimum values of PM10 in regular and dusty days of Zabol, as presented in Table 1. According to this table, the average annual values of PM10 during 2013–2014 and 2014–2015 in Zabol are 156.3 and 380.7 µg/m3, respectively, which are 3.1 and 7.6 times higher than the level announced by NAAQS (i.e., 150 µg/m3). Furthermore, 73 and 144 days with daily PM10 concentrations higher than the NAAQS limit were recorded during 2013–2014 and 2014–2015, respectively. The results are compared with similar studies in Kermanshah (2011, 2012) and Ilam (2015–2016), Iran. The first study has reported 138 and 63 days of high PM10 level in 2011 and 2012, respectively (Marzouni et al. 2016), and the second has reported 180 days of high PM10 concentration during 2015–2016 (Khaniabadi et al. 2017). Though the periods are not the same, it can be stated that Zabol experiences more days with a high PM10 index compared to Kermanshah and fewer days compared to Ilam.
According to Table 1, the mean daily concentration of PM10 during the windy period of Zabol is higher than the values recorded for the rest of the year for both study periods. This fact highlights the severe effect of the 120 windy days on the ambient air condition of Zabol. However, the point is that the maximum PM10 concentration, i.e., 3856 µg/m3, is associated to a typical month during 2014–2015. It means that the occurrence of dust storms in this region is not limited to 120 windy days. The last point outlined in Table 1 is that the PM10 concentrations during 2014–2015 are higher than those of 2013–2014.
Figure 2 illustrates the number of dust events for normal days (PM10 < 50 µg/m3), dusty air (PM10 = 50–200 µg/m3), light dust storms (PM10 = 200–500 µg/m3), dust storms (PM10 = 500–2000 µg/m3), strong dust storms (PM10 = 2000–5000 µg/m3), and serious dust storms (PM10 > 5000 µg/m3). As this figure shows, the number of dust events experienced during 2014–2015 has increased compared to 2013–2014. In the meantime, 125 and 42 days of dust storm are reported for Ahvaz, Iran in 2013, and 2014, respectively (Maleki et al. 2016). Also, Marzouni et al. (2016) have reported 230 and 322 days of dusty air, and 91 and 17 days with light dust storms in 2011 and 2012 in Kermanshah, respectively. 164 dusty days, 16 days of light dust storm, two dust storm days, and no strong or severe dust storms are reported for Ilan during 2015–2016 (Khaniabadi et al. 2017). These values indicate fewer dust events in Kermanshah, compared to Zabol.

The occurrence of dust events from 2013 to 2015 in Zabol
Figure 3 shows the number of TM resulted from exposure to different PM10 concentrations. In this figure, each chart shows the cumulative number of excess cases related to each interval of PM10 concentration for the three risk categories. The risk categories include the upper relative risk, central relative risk, and lower relative risk separately at the confidence intervals of 95% (overestimated risk), 50% (central risk), and 5% (underestimated risk). As can be seen, the number of excess TM cases caused by short-term exposure to PM10 concentrations above 20 µg/m3 was 93 and 284 persons during 2013–2014 and 2014–2015, respectively. Among the cases, 30 and 153 people died due to the exposure to PM10 concentrations higher than 400 µg/m3 during 2013–2014 and 2014–2015, respectively. This finding reveals the concerning impact of dust storms on the health of Zabol residents during the study periods. In line with the observed deadly effect of PM10, Naddafi et al. (2012) reported 1372 extra deaths in Tehran, Iran, caused by short-term exposure to PM10 levels higher than 20 µg/m3.

Relationship between the cumulative numbers of total mortality and atmospheric PM10 concentration
The percentage of days, in which the Zabol residents were exposed to different concentrations of PM10 during 2013–2015, is depicted in Fig. 4. As can be seen, during 2013–2014, the people are more exposed to the PM10 concentration of 60–69 µg/m3, while in 2014–2015, they are more exposed to PM10 values greater than 400 µg/m3. However, in both periods, the highest percentages of excess cases of health outcomes (32.14% for 2013–2014 and 53.88% for 2014–2015) are associated with PM10 concentrations higher than 400 µg/m3. This result reflects the occurrence of more dust storms in 2014–2015, resulting in more severe and adverse health consequences compared to 2013–2014. A comparison with another study in Mazzano and Rezzato (located in an industrialized area of Northern Italy) showed that its residents were exposed to high levels of PM10 in fewer days than those of the present study (Fattore et al. 2011). According to the report of Fattore et al., the highest level of PM10 that residents of Mazzano and Rezzato were exposed to was lower than 250 µg/m3. The results of another study conducted in Sanandaj, Iran showed that the total number of days, in which the residents of the city were exposed to concentrations above 170 µg/m3 PM10, was less than 2% that is much lower than the days in which Zabol residents are exposed to high PM10 concentration.

Exposure days (%) of Zabol residents to different concentrations of PM10
The results of the employed model, including the obtained BI, RR, and AP values and the number of annual excess cases related to short-term exposure to PM10 levels higher than 10 µg/m3, are presented in Table 2. According to the modeling results, the percentages of TM, CM, RM, HACD, and HARD caused by short-term exposure to PM10 concentrations above 10 μg/m3 are 8.81%, 9.46%, 13.54%, 10.51%, and 9.46%, respectively during 2013–2014. In the meantime, the values of TM, CM, RM, HACD, and HARD during 2014–2015 are 13.74%, 14.69%, 20.53%, 16.23%, and 14.69%, respectively. These percentages can be compared with the AP values reported about short-term exposure to PM10 by Fattore et al. (2011), including 3.7% and 4.1% CM and 5.3 and 5.9% RM for the residents of Mazzano and Rezzato, respectively.
According to Table 2, the AP percentages of all studied health impacts are higher during 2013–2014 compared to 2014–2015, which might be due to the higher PM10 concentrations, more dust events, and more days with PM10 levels exceeding 150 μg/m3 during 2014–2015 compared to 2013–2014 (Table 1; Fig. 2). In consistence with this statement, a significant relationship has been observed between respiratory diseases and dust storms in a study about the health effects of dust storms in Kermanshah, Iran (Marzouni et al. 2016). In general, it is known that the most frequent dust storms in Southwest Asia occur in the Sistan Basin, in which Zabol is also located (Alizadeh-Choobari et al. 2014). The large number of dust storms in this region results from blowing off the loose soil particles of the Hamoun lake by the strong 120-day winds that dominate Zabol from late spring to early autumn (May–September). These regional winds are generated due to the north–south pressure gradient between a persistent cold high-pressure system and a summertime thermal low-pressure system. This pressure gradient starts over the high mountains of Hindu Kush in northern Afghanistan towards the deserts of eastern Iran and western Afghanistan that results from sustained surface warming (Alizadeh-Choobari et al. 2014). Therefore, the higher AP values and the number of excess TM, CM, RM, HACD, and HARD cases in the present study compared with other studies can be attributed to the 120-day winds and the high frequency and intensity of dust storms in the region of study.
During 2013–2014, the number of excess TM, CM, RM, HACD, and HARD cases per 100,000 people was 182, 96, 18, 94, and 243, respectively. However, during 2014–2015, the number of these cases increased to 284, 149, 36, 144, and 378, respectively. The increase of dust storm events during 2014–2015 increased the health impacts by 50% compared to 2013–2014. The substantial increase in the number and severity of the dust storms in this region might be due to the extreme and lengthy droughts experienced from 2013 to 2015. Hosseini et al. (2014) evaluated the health effects of PM10 exposure using the AirQ model in Sanandaj, Iran, in 2013, and reported 228, 120, 23, 118, and 305 cases for TM, CM, RM, HACD, and HARD, respectively.
So far, numerous international studies have been conducted to assess the health effects of PM10 using the WHO approach implemented in the AirQ software. The results are summarized in Table 3. As this table suggests, the AP values reported by the present study for the residents of Zabol are comparable with those reported for Kermanshah (Iran) and Ahvaz (Iran). The higher AP values related to PM10 exposure in Zabol compared with other studies carried out in Sanandaj, Iran (Hosseini et al. 2014), Tehran, Iran (Naddafi et al. 2012), and Shiraz, Iran (Mohammadi et al. 2015) can be explained according to the higher mean concentration of PM10 and more days with high PM10 concentrations in Zabol.
Model limitations
This study has employed the protocol introduced by WHO for studying the effects of atmospheric air pollution on human health by modeling the individual effect of each pollutant implemented in AirQ software. Like any other model, this model has some limitations. First, AirQ assumes that the data introduced to the software represent the average exposure data of the studied population. However, using the air pollution monitoring data recorded by just one station does not seem sufficient for Zabol, which experiences dusty air and many dust storms throughout the year. Also, the data obtained from specific sampling points may not represent the average exposure data of the Zabol residents.
Consequently, to have a more representative data, more air monitoring stations should be installed, and/or mobile air sampling stations should be used at different areas within and around the city. The second limitation is the lack of data about the Zabol inhabitants, which affects the RR estimation, considerably. Since there is no evidence for different responses to air pollution between target and evidentiary populations, the mortality effect estimated from the evidentiary data is acceptable.
Conclusion
This study simulated the health impacts of PM10 pollution in Zabol, Iran, using the model recommended by the WHO and implemented in the AirQ 2.2.3 software. The average annual levels of PM10 during 2013–2014 and 2014–2015 were 3.126 and 7.614 times higher than the limit determined by NAAQS, respectively. According to the results, the 120-day winds in this region affect the outdoor air quality of Zabol, considerably. Health impacts (TM, CM, RM, HACD, and HARD) attributable proportions to PM10 were estimated using the model introduced by WHO. Results showed that the health impacts attributable proportions reported in the present study for the population of Zabol are much higher than those reported for Sanandaj, Tehran, and Shiraz in Iran.
Consequently, urgent actions are required to alleviate the huge negative health impacts of PM10 on the Zabol's residents by reducing the concentration of PM10 in this region. Furthermore, it seems that one air pollution monitoring station is not adequate for the city of Zabol, which experiences dusty air and many dust storms throughout the year. Therefore, more air monitoring stations should be installed, or mobile stations should be used to gain a better understanding and evaluate the adverse health impacts of PM10 more accurately. Also, dust sampling and analysis can be considered as a handy tool for determining the origin and transportation paths of the particulates to help politicians and decision-makers to develop appropriate management strategies. Eventually, such data can help to develop suitable procedures for controlling pollutants through stabilizing sandy soils and preventing soil erosion.
References
Al-Hemoud A, Al-Dousari A, Al-Shatti A, Al-Khayat A, Behbehani W, Malak M (2018) Health impact assessment associated with exposure to PM10 and dust storms in Kuwait. Atmosphere 9(1):6
Alizadeh-Choobari O, Zawar-Reza P, Sturman A (2014) The, “wind of 120 days” and dust storm activity over the Sistan Basin. Atmos Res 143:328–341
Fattore E, Paiano V, Borgini A, Tittarelli A, Bertoldi M, Crosignani P et al (2011) Human health risk in relation to air quality in two municipalities in an industrialized area of Northern Italy. Environ Res 111(8):1321–1327
Goudarzi G, Geravandi S, Javad Mohammadi M, Ghomaishi A, Salmanzadeh S (2014) Health endpoints caused by PM10 Exposure in Ahvaz Iran. Iran J Health Safe Environ 1(4):159–165
Goudarzi G, Geravandi S, Mohammadi MJ, Vosoughi M, Angali KA, Zallaghi E, Neisi AK, Saeidimehr S, Mohammadi B (2015) Total number of deaths and respiratory mortality attributed to particulate matter (PM 10) in Ahvaz, Iran during 2009. Int J Environ Health Eng 4(1):33
Hosseini G, Maleki A, Amini H, Mohammadi S, Hassanvand MS, Giahi O et al (2014) Health impact assessment of particulate matter in Sanandaj, Kurdistan, Iran. J Adv Environ Health Res 2(1):54–62
Hu J, Wang Y, Ying Q, Zhang H (2014) Spatial and temporal variability of PM2.5 and PM10 over the North China Plain and the Yangtze River Delta, China. Atmos Environ 95:598–609
Jamalizadeh M, Moghaddamnia A, Piri J, Arbabi V, Homayounifar M, Shahryari A (2008) Dust storm prediction using ANNs technique (a case study: Zabol city) 1. Proc Worldacad Sci Eng Technolo 33:529–537
Jeong SJ (2013) The impact of air pollution on human health in Suwon City. Asian J Atmos Environ 7(4):227–233
Khaniabadi YO, Daryanoosh SM, Amrane A, Polosa R, Hopke PK, Goudarzi G et al (2017) Impact of Middle Eastern Dust storms on human health. Atmos Pollut Res 8(4):606–613
Maleki H, Sorooshian A, Goudarzi G, Nikfal A, Baneshi MM (2016) Temporal profile of PM10 and associated health effects in one of the most polluted cities of the world (Ahvaz, Iran) between 2009 and 2014. Aeol Res 2:135–140
Marzouni MB, Alizadeh T, Banafsheh MR, Khorshiddoust AM, Ghozikali MG, Akbaripoor S et al (2016) A comparison of health impacts assessment for PM10 during two successive years in the ambient air of Kermanshah, Iran. Atmos Pollut Res 7(5):768–774
Miri M, Derakhshan Z, Allahabadi A, Ahmadi E, Conti GO, Ferrante M et al (2016) Mortality and morbidity due to exposure to outdoor air pollution in Mashhad metropolis, Iran. The AirQ model approach. Environ Res 151:451–457
Mohammadi A, Azhdarpoor A, Shahsavani A, Tabatabaee H (2015) Health Impacts of Exposure to PM10 on Inhabitants of Shiraz. Iran Health Scope 4(4):e31015
Mokhtari M, Miri M, Mohammadi A, Khorsandi H, Hajizadeh Y, Abdolahnejad A (2015) Assessment of air quality index and health impact of PM10, PM2. 5 and SO2 in Yazd. Iran. J Mazandaran Univ Med Sci 25(131):14–23
Naddafi K, Hassanvand MS, Yunesian M, Momeniha F, Nabizadeh R, Faridi S et al (2012) Health impact assessment of air pollution in megacity of Tehran, Iran. Iran J Environ Health Sci Eng 9(1):28
Rahnama H, Rajabpour S (2017) Identifying effective factors on consumers’ choice behavior toward green products: the case of Tehran, the capital of Iran. Environ Sci Pollut Res 24(1):911–925
Rashki A, Kaskaoutis DG, Eriksson P, Qiang M, Gupta P (2012) Dust storms and their horizontal dust loading in the Sistan region. Iran Aeolian Res 5:51–62
Sistan and Baluchestan Governorate (2019) Zabol county: Sistan and Baluchestan Governorate Web Page; Available from: https://www.sbportal.ir/fa/cities/zabol.
Soleimani M, Amini N (2017) Source identification and apportionment of air pollutants in Iran. J Air Pollut Health 2(1):57–72
WHO. 7 million premature deaths annually linked to air pollution GENEVA: WHO; 2014 Available from: https://www.who.int/mediacentre/news/releases/2014/air-pollution/en/.
Zallaghi E, Goudarzi G, Geravandi S, Mohammadi MJ (2014) Epidemiological indexes attributed to particulates with less than 10 micrometers in the air of Ahvaz City during 2010 to 2013. Health Scope 3(4):e22276
Acknowledgements
The authors appreciate Zabol University of Medical Sciences, Iran (Zbmu.1.REC.1396.155), for supporting this research.
Author information
Authors and Affiliations
Contributions
SJ, SR, and BD refined data. MM, YF, HE, RAF, and AG analyzed data. HK and MT wrote the report. SJ revised final report. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Javan, S., Rahdar, S., Miri, M. et al. Modeling of the PM10 pollutant health effects in a semi-arid area: a case study in Zabol, Iran. Model. Earth Syst. Environ. 7, 455–463 (2021). https://doi.org/10.1007/s40808-020-00874-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40808-020-00874-y