
Abstract
Sleep disturbances are common in neurodegenerative disease and impair quality of life. People with Alzheimer’s disease (AD) develop daytime hypersomnia and nighttime insomnia. These symptoms likely result from circadian rhythm disruption due to reduced zeitgeber input, suprachiasmatic nucleus dysfunction, and melatonin alterations. In Parkinson’s disease (PD), various sleep disorders, such as insomnia, hypersomnia, and REM sleep behavior disorder (RBD) are often seen. These problems are related to neurodegeneration of brain structures influencing sleep and wake states, circadian rhythm dysfunction, and motor and non-motor symptoms. RBD can precede PD motor symptoms by several years, and it represents a window of opportunity to treat the disease process when a disease-modifying therapy for PD becomes available in the future. Effective treatments for sleep disturbances in AD and PD are limited. Deeper understanding of sleep and circadian dysfunction is necessary to develop treatments that improve quality of life and potentially alter the degenerative course.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Over the past few decades, sleep and circadian rhythm dysfunction in neurodegenerative diseases has been increasingly recognized. In this review, we discuss the types of sleep disorders in the two most common neurodegenerative diseases: Alzheimer’s disease and Parkinson’s disease (Table 1).
Alzheimer’s Disease
Sleep disturbances are quite common in dementia, particularly Alzheimer’s disease (AD). These and secondary agitation, in fact, are the primary impetus in institutionalizing older individuals with cognitive decline, as family members are unable to take care of them at night. Nocturnal exacerbation of delirium or “sundowning” is a well-recognized entity in dementia and is often associated with sleep disturbances. Sundowning is characterized by agitation, confusion, and irritability as natural lights begin to fade in the evening and at night. Daytime hypersomnia and nighttime insomnia are the most common sleep complaints with dementia. The association between disturbed sleep and cognitive decline is bidirectional and complex.
Circadian rhythm sleep disorders (CRSD) are common in this cohort and can manifest with both the excessive daytime sleepiness and poor sleep continuity at night. The most common circadian rhythm sleep-wake disorder to affect this group is irregular sleep-wake disorder. It is also the most disabling of sleep disorders in AD. Parasomnias, such as rapid eye movement (REM) sleep behavior disorder (RBD), have rarely been reported in AD but have a more significant association with α-synucleinopathies. There may also be a slightly increased risk of sleep disordered breathing, particularly obstructive sleep apnea (OSA) presumably secondary to degeneration of central respiratory control areas in the brainstem.
This article will focus mainly on the CRSD, primary Irregular Sleep Wake Disorder (IRSWD). As these are by far the most common, and their unique pathophysiology in AD requires specialized multidisciplinary approach to treatment, which may improve both insomnia and daytime sleepiness.
Pathophysiology of CRSD in AD
The circadian sleep-wake rhythms are controlled by the suprachiasmatic nucleus (SCN), the master clock or the pacemaker that resides in the hypothalamus. Even with normal aging, the SCN degenerates resulting in earlier awakenings and less consolidation of nocturnal sleep [1]. The disturbances of circadian rhythms, as well as fragmentation of sleep at night, are more pronounced in AD. In fact, dampened circadian rhythm amplitude and delayed acrophase (the time period during which the circadian process is most active) in otherwise healthy older adults is a risk factor for developing AD within the following 5 years with an odds ratio of 1.57 (95 % CI 1.10–2.26) [2]. Due to a variety of reasons, people with AD have less exposure to light, the primary zeitgeber (time givers or external stimuli that reset the internal clock). Furthermore, the impact of light on their sleep-wake rhythms is dampened due to multiple factors including age-related yellowing of the cornea and cataracts [3] and degeneration of the retinal ganglionic cells [4]. These cells project through the retinohypothalamic tract to the SCN, providing the pathway on how light can influence the sleep-wake cycle and entrain to follow the 24-h day rather than the slightly longer intrinsic rhythm [5]. AD patients are also more likely to spend more time indoors and be less physically active than their healthy counterparts, further limiting their exposure to natural light [6]. Reduced natural light and daytime physical activity result in institutionalized elderly having more disturbed sleep-wake cycles than their community-dwelling counterparts [7].
The release of melatonin, a hormone secreted by the pineal gland under the control of the SCN, is used to regulate circadian fluctuations. CSF melatonin levels decrease with normal aging, and they become even lower in AD; its onset is earlier, and its peak becomes irregular. This is presumably due to SCN degeneration, as the pineal gland is not affected by AD pathology [8]. In addition, the degeneration of the nucleus basalis of Meynert, a major source of cholinergic input, can further affect sleep-wake rhythms [9]. The dysfunction of the SCN and the related retinohypothalamic tract, alteration of melatonin levels, and significantly reduced exposure to zeitgebers lead to CRSD in dementia and AD in particular, and they can cause both excessive daytime sleepiness and nighttime insomnia.
The more severe the underlying cognitive decline, the more disrupted sleep becomes, but genetic predispositions also play a role in sleep disturbances in AD. Melatonin and its decline in secretion may be the link between AD and sleep disturbances. Melatonin inhibits β-amyloid aggregation and toxicity and inhibits tau protein hyperphosphorylation [10]. It is also a potent antioxidant that may prevent cell death [11]. Dysfunction in melatonin levels leads to circadian desynchrony. Degeneration of the hippocampus commonly occurs in AD. Its plasticity, presumably due to its connections through the SCN, is influenced by light, melatonin and circadian gene manipulation [12]. Hence, another potential mechanism by which dementia may be linked to sleep-wake disturbances.
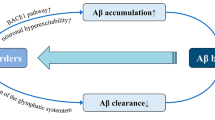
In animal models, β-amyloid increases during wakefulness and is cleared from the brain during sleep through the lymphatic system [13]. With sleep deprivation, there is a further increase in β-amyloid levels [14]. It is unclear whether the fluctuations of the β-amyloid levels are directly under the control of circadian system, or if they are indirectly influenced by circadian control of the sleep-wake cycle.
Sleep Architecture Changes and Other Sleep Disorders in AD
Most but not all sleep-wake abnormalities in AD are due to circadian rhythm disturbances. There are also sleep architecture changes which are the same as seen in the healthy elderly population but much more pronounced in severity. As mentioned above, RBD has been rarely described in AD, as the latter is a tauopathy, and RBD is usually associated with α-synucleinopathies. Sleep disordered breathing, particularly OSA, is more common in AD than can be explained by age alone. OSA worsens cognitive decline in AD and positive airway pressure therapy partially improves cognition [15]. Lastly, restless legs syndrome (RLS), although not more prevalent in AD, can disturb sleep and worsen “sundowning”. In addition, depending on the degree of dementia, establishing the diagnosis based on symptomatology can be challenging [16, 17].
Management
The discovery of melatonin dysfunction in AD led to a handful of trials with exogenous melatonin for sleep-wake disturbances in AD, and the results have been equivocal. Singer et al. ran the largest double-blind placebo-controlled randomized clinical trial. They randomized 157 subjects to either placebo, 10 mg of immediate release melatonin and 2.5 mg of controlled release melatonin. There were no differences in sleep parameters among the groups both objectively using actigraphy and subjectively using caretaker reports [18•]. A randomized placebo-controlled crossover trial with 6 mg of melatonin failed to demonstrate any actigraphic sleep parameters in 45 subjects with AD [19]. Lastly Gehrman et al., again using actigraphy, found no improvement in either sleep parameters or daytime agitation in 41 patients with AD who were randomized to either placebo, 8.5 mg of regular melatonin or to 1.5 mg of delaed release melatonin [20]. Asayama et al., however, using actigraphy demonstrated modest decrease in nighttime activity with 3 mg of melatonin vs. placebo in a group of 20 subjects with AD. There were no significant changes in daytime naps, overall sleep duration or quality [21]. When added to bright light therapy, 3 mg of melatonin was shown to be slightly more effective in improving actigraphic sleep parameters both at night and during the day than bright light alone in 50 subjects with AD [22]. Lastly, another trial comparing placebo, dronabinol, and melatonin showed only modest reduction in nighttime activity in the melatonin arm without any impact on agitation or other actigraphic sleep parameters or neuropsychological function [23].
Phototherapy
Several small trials have evaluated the benefits of bright light therapy. Neither the intensity nor the duration of the light has been standardized among reports. Morning bright light therapy (usually ≥2500 lx), or even 30 lx of blue light, improves nighttime sleep, daytime wakefulness, and reduces evening agitation [5]. A plan of high intensity light exposure during the day and low intensity at night, improving visual conditions during wakefulness, and nightlights to reduce falls can improve daytime alertness, consolidate sleep and decrease the incidence of sundowning [24].
Behavioral Modifications
A combined treatment of sleep hygiene, daytime exercise and nighttime environment modification has been shown effective in improving sleep-wake cycles both in AD patients and cognitively normal elderly population and in community dwellers and geriatric institutionalized. These include (a) daily exercise, 30 min in duration, preferably outdoors; (b) decreasing time spent in bed during the day and limiting naps to about 30 min before 1 P.M.; (c) maintaining a quiet and low lit bedroom at night; and (d) avoiding stimulating medications close to bedtime [25•]. Finally, sedative hypnotics, dopamine agonists, cholinesterase inhibitors and other medications for symptomatic management of AD sleep-wake complaints should be used with caution given their side effect profile (i.e., dizziness, bradycardia, and insomnia).
Parkinson’s Disease
Parkinson’s disease (PD) is the second most common neurodegenerative disease and affects 1 % of the general population over age 60 years [26]. Clinical manifestations include bradykinesia, rigidity, tremor, and shuffling gait. PD can be divided into subtypes, such as tremor predominant, characterized by significant resting tremor, or postural instability gait dysfunction (PIGD), which involves a greater severity of gait disorder, falls, and freezing of gait. The pathological hallmark of PD is Lewy bodies, comprised of intraneuronal α-synuclein inclusions in the substantia nigra, a source of dopaminergic neurotransmission.
Although much focus has been on motor symptoms, non-motor symptoms of PD, such as sleep dysfunction have been recognized as major contributors to impaired quality of life [27]. Sleep dysfunction is extremely common in PD, affecting 60-98 % during their course of the disease [28, 29]. A variety of sleep disorders can arise in this population, with the most common being insomnia, hypersomnia, and REM sleep behavior disorder (RBD).
Insomnia
Insomnia, typically sleep fragmentation, is the most common sleep complaint in PD, affecting 60-80 % of the PD population [30, 31]. Sleep fragmentation is a significant contributor to impaired quality of life [32, 27] and is associated with hypersomnia and fatigue [33], impaired attention and executive function [34], and depression [32]. It also increases caregiver burden, particularly if the patient needs assistance when awake [35]. Polysomnographic characteristics confirm lower sleep efficiency, greater wake after sleep onset, and less slow wave sleep and stage REM sleep in PD patients compared to age-matched controls [36].
There are several causes of insomnia in PD, and often multiple co-exist in an individual patient. Nocturnal motor symptoms, such as tremor, akinesia, and pain, and non-motor symptoms including nocturia, depression, and hallucinations, are associated with sleep disruption in PD [33]. Recently, other causes more intrinsic to the disease have been examined.
There is increasing evidence that sleep dysfunction in PD can be related to the disease process, including neurodegeneration of brainstem sleep centers [37]. Furthermore, dysfunction of dopaminergic nuclei may play a role given that dopamine is involved in controlling sleep and wake. Dopamine in the ventral tegmental area and substantia nigra interact with key nuclei such as the raphe nuclei, locus ceruleus, hypothalamus, basal forebrain, and thalamus, which are involved in mediating sleep and wake states [38]. In rats, lesion experiments involving the substantia nigra pars compacta, a key area of degeneration in PD, lead to increased wakefulness during the normal rest period as well as the active period [39•]. The degree of the lesion correlates with the amount of wakefulness. These results indicate that dopaminergic input from the substantia nigra is part of a pathway with other basal ganglia structures, specifically the caudoputamen and globus pallidus externa, that influence sleep and wake states. Dopaminergic medications increase sleep efficiency [36], and although this effect may be due to improvement of nocturnal motor symptoms, these medications can also cause excessive sleepiness [40].
Increasing evidence indicates that circadian rhythm dysfunction may underlie some of these sleep disturbances in PD. Studies using wrist actigraphy show decreased daytime activity and increased nighttime activity, indicating low amplitude of the rest-activity rhythm [41, 42]. Furthermore, those with lower amplitude and less interdaily stability of the rest-activity rhythm have more severe disease and hallucinations [42]. Other rhythms in other such as core body temperature [43], melatonin [44•], blood pressure [45], and cortisol [46] are also to be altered. The mechanism of circadian alterations is not clear but may include alterations in light exposure [47–49] and dysfunction in the SCN [50].
The treatment of insomnia in PD can be challenging, because it requires identifying which of the myriad of underlying causes are contributing to the disorder. Treatment should be targeted toward identified potential underlying causes. For nocturnal motor symptoms, addition of a dopaminergic therapy at night, such as with dopamine agonists [51, 52] or controlled release levodopa [53], can improve sleep [36]. Additionally, underlying depression, nocturia, and hallucinations should be addressed. However, if such factors are not present, or response of insomnia to their treatment is not adequate, other means to address insomnia should be sought. Although treatment of insomnia in PD can be similar to that of older adults, hypnotic therapy should be carefully considered if the patient has higher risk of falls or has cognitive impairment. Only a few strategies have been assessed specifically in the PD population. Doxepin, which is anti-histaminergic at low doses, given at a dose of 10 mg at bedtime, was shown to improve the symptoms of insomnia compared to placebo, though objective improvements by actigraphy were not seen [54]. In that same study, cognitive behavioral therapy (CBT) for 90 min weekly for 6 weeks, in combination with bright light therapy (30 min daily), also improved insomnia symptoms by some but not all self-reported measures [54]. Circadian rhythm-based therapies have potential to improve insomnia. One large retrospective [55] and one small prospective study [56] using bright light exposure before bedtime showed improvement in insomnia symptoms. Melatonin administration 3 mg [57] and 5 mg given at night [58] improved self-reported sleep quality and quantity, but these changes were not objectively observed with PSG [57] or actigraphy [58].
Hypersomnia
Self-reported hypersomnia is a common complaint in PD, affecting up to 50 % [59, 60]. Hypersomnia is independent of age, disease duration, disease severity, depression, and RBD but is associated with sleep-disordered breathing [61, 59, 62]. In a group of 30 unselected PD patients, 37 % have severe hypersomnia based on a mean sleep latency of less than 5 min on the multiple sleep latency test (MSLT), typical of people with narcolepsy [62]. However, a larger study of 134 unselected patients with PD found that only 13 % had a mean sleep latency of less than 8 min [59]; however, that group had a less dopaminergic therapy than the earlier study. In those who complain of sleepiness, the frequency of severe hypersomnia (mean sleep latency <5 min on MSLT) is much higher at 50 %. In addition, 39 % had stage REM sleep in at least two naps, a finding typical of narcolepsy [61]. These patients with a “narcolepsy-like phenotype” were sleepier than those with less than two naps with stage REM sleep. Furthermore, one neuropathological study of 11 PD patients found a greater loss of hypothalamic orexinergic neurons compared to controls, and this change correlated with disease severity [63]. A recent study has also shown that PD patients with stage REM sleep during the day are sleeper than those without daytime REM sleep [64]. Although objective and self-reported sleepiness (using Epworth sleepiness scale >10) correlate, the strength of this association is variable, suggesting that some patients are not aware of how sleepy they are [61, 59, 62].
Sleep attacks, described as an irresistible or sudden sleepiness with our without warning signs, have also been described in up to 43 % people with PD [65, 66]. This is a particularly dangerous symptom as 21 % report sleep attacks when driving [66]. Sleep attacks are associated with dopaminergic therapy, particularly dopamine agonists but also levodopa, and is predicted by older age, longer disease duration and severity, male sex, and poor self-reported sleep quality, though the Epworth sleepiness scale was poorly predictive [67, 65]. The strongest effect of dopamine agonists on sleep attacks occurred in younger men (age <70 years) [65]. Some dopamine agonists appear to lower orexin-A levels, and this could be a potential mechanism by which they cause sleep attacks [68].
Hypersomnia in PD has several potential causes and is often multifactorial. Levodopa therapy appears to be associated with hypersomnia [61], though not all studies have noted this finding [59, 62]. Sleep disordered breathing, particularly OSA, is associated with hypersomnia in PD but can also cause hypersomnia in older adults without PD [59, 62]. However, patients with PD do not appear to be at higher risk and may actually be at lower risk for OSA than controls [69, 70]. A less explored potential cause of hypersomnia in PD is circadian rhythm disruption. A recent study showed that patients with PD have lower serum melatonin secretion amplitudes than controls and was more prominent in those with hypersomnia [44•]. Low melatonin secretion was confirmed in patients with early PD, in addition to altered rhythms in cortisol secretion and clock gene Bmal1 expression [71]. Furthermore, dopaminergic therapy appears to alter circadian alignment between the melatonin and sleep-wake rhythms [72•].
Treatment of hypersomnia requires identification of potential underlying causes, but the hypersomnia is often persistent. Unfortunately, no therapy has been shown to consistently improve hypersomnia in PD. Several small trials of modafinil with daily doses ranging 200–400 mg improves self-reported hypersomnia [73–76], though most of them have shown only modest benefit, and two studies did not show improvement [77, 78]. Furthermore, modafinil does not affect objective sleepiness [79, 74, 78]. Neither doxepin [54] nor CBT combined with bright light therapy improved subjective sleepiness in a group of PD patients [54]. In one open-label study, sodium oxybate improved subjective sleepiness and fatigue, but it can cause dizziness and nocturia [80]. Given the relationship between circadian dysfunction and hypersomnia, development of circadian-based approaches to address this troublesome symptom is needed. Only one study examining the effect of melatonin (5 and 50 mg) on hypersomnia, but a significant effect on subjective sleepiness was not demonstrated [58].
REM Sleep Behavior Disorder
RBD is a parasomnia characterized by dream enactment behavior, such as screaming, flailing, punching, or jumping out of bed, by history or documented during stage REM sleep and the finding of REM sleep without atonia (RSWA) on PSG [81]. The behaviors are often violent but can be non-violent, such as singing, smiling, and laughing. Somnambulism is rare in RBD, as the eyes are closed, and there is no awareness of the environment. The dream enactment can result in injuries to the patient or bedpartner [82]. Idiopathic RBD is more common in men with an age of onset of approximately 62 years [83].
RBD is a common finding in PD with about 46 % affected across the disease range [84] and is associated with greater progression of motor symptoms [85]. Some studies suggest that those with RBD are more likely to have PIGD subtype [86, 87], though others have not confirmed this finding [88, 84]. However, a quantitative analysis of the motor activity during stage REM sleep showed RSWA in patients with PD and freezing of gait compared to those without freezing of gait. Furthermore, the amount of tonic motor activity during stage REM sleep was similar to RBD; the phasic activity was elevated in PD with FOG but not as much as RBD [89]. Furthermore, RBD appears to be a strong risk factor for the development of dementia in PD, with 34 % of non-demented PD patients developing dementia over 4.4 years [90•]. A survey-based study using the RBD screening questionnaire in a large group of PD patients showed that those with high likelihood for RBD had more sleep disruption and hallucinations [91]. However, studies using this questionnaire in PD should be interpreted with caution, as the sensitivity and specificity compared to PSG are significantly lower, unless the patients are aware of RBD symptoms [92].
RBD as a Harbinger of Neurodegenerative Disease
Soon after the disorder was recognized by Schenck and colleagues, a relationship between RBD and the development of neurodegenerative disease, particularly PD and dementia with Lewy bodies, has become apparent [93]. Several studies have since confirmed increased risk of developing a neurodegenerative disease over several years [94, 83, 95–97]. Recently, Iranzo and colleagues extended their previous findings and showed that over 90 % of 174 patients with PSG-confirmed RBD develop a neurodegenerative disease at 14 years from diagnosis of RBD, with a median time to diagnosis of 7.5 years [83]. Among 172 autopsied cases with PSG-confirmed RBD, 170 had a neurodegenerative disease, with the most common clinical diagnosis being dementia with Lewy bodies (57 %) and then PD (19 %) [98•]. On pathological examination, 94 % ultimately have α-synuclein pathology, most of which was consistent with either dementia with Lewy bodies or PD [98•].
These findings have sparked a search for markers to determine which patients with RBD will develop neurodegenerative disease and when. Patients with RBD have abnormal brain metabolism and perfusion imaging patterns consistent with PD and dementia with Lewy bodies, and that these imaging modalities may be helpful to predict conversion of RBD to PD or dementia with Lewy bodies [99]. Patients with RBD and mild cognitive impairment have a greater proportion of slower waking electroencephalography (EEG) frequencies using power spectral analysis than those without mild cognitive impairment and controls. This finding suggests that the cause of the dementia is related to the EEG changes, rather than the RBD itself, and perhaps quantitative EEG analysis can be used to predict those likely to convert to dementia [100]. Identification of these at-risk patients will be important to test the ability of potential disease-modifying agents to reduce or eliminate development of neurodegenerative disease. Guidelines for clinical trials toward this aim were recently published in a consensus statement from the International RBD Study Group [101]. However, at this time no treatments have been demonstrated to slow PD progression.
Antidepressants, particularly selective serotonin reuptake inhibitors, increase the risk of RBD symptoms [102, 103]. However, in a group with RSWA related to sertraline, the typical male predominance and elder age of idiopathic RBD were not seen [103]. In addition, a quantitative analysis of the electromyography during stage REM sleep found that the RSWA in patients taking antidepressants had less total and less tonic activity in the submentalis muscle than PD patients with RBD [104]. These findings suggest that the pathophysiology of antidepressant medication-induced RBD is different from idiopathic RBD [102–104]. Other recent data suggests that the development of RBD in the setting of antidepressants may be an early signal of an underlying neurodegenerative disease [105]. RBD patients on antidepressants were found to have a higher rate of other known preclinical markers of neurodegenerative disease, such as loss of olfaction and color vision, autonomic dysfunction, and altered motor function. Although these patients did not develop a neurodegenerative disease at the same rate as those with idiopathic RBD (17 vs. 52 %) over the 8-year follow-up period, it is not clear how many of the control subjects developed neurodegenerative disease [105]. Therefore, it remains unclear if those with RBD on antidepressants are actually at higher risk of developing a neurodegenerative disease.
Treatment of RBD
Symptomatic treatment of RBD includes medications and safety precautions. However, no large randomized controlled trials have been performed in RBD. Clonazepam, a long-acting benzodiazepine, is the most commonly used medication for RBD, since it was shown to improve RBD symptoms [93]. A low dose of clonazepam (up to 1 mg) is effective in the majority of patients [106]. However, there remains a concern for this medication to worsen cognitive function in older adults. Melatonin administration of 3–15 mg can also be effective to reduce frequency and severity of self-reported RBD symptoms and even reduce the motor tone during stage REM sleep [107, 106, 108]. Furthermore, melatonin has a better adverse event profile that clonazepam with diminished potential for drug-drug interactions, an important consideration in older adults.
Some patients do not improve with clonazepam or melatonin, and other therapies are needed to address the dream enactment behavior. Ramelteon, a melatonin receptor agonist, was beneficial for RBD symptoms and reduced RSWA in two patients [109]. Rivastigmine, a cholinesterase inhibitor, improved RBD symptoms in 12 PD patients in whom melatonin and clonazepam therapy failed [110]. Finally, in a small study of 4 patients with RBD refractory to clonazepam and melatonin, a pressurized bed alarm reduced sleep-related injuries from RBD [111].
Conclusion
Sleep disturbances in AD and PD are common and result from the underlying disease process, as well as secondary to motor dysfunction, in the case of PD, or non-motor disturbances, such as low exposure to zeitgebers, mood disorders, and autonomic dysfunction. In addition, circadian rhythm dysfunction appears related to neurodegeneration, but it remains unclear whether this is a downstream effect or potential avenue to intervene in the disease process. Understanding the role of sleep and circadian function in neurodegeneration is important to improve quality of life and disability in these patients and perhaps develop therapies to alter the disease course.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
Maaskant M, van de Wouw E, van Wijck R, Evenhuis HM, Echteld MA. Circadian sleep-wake rhythm of older adults with intellectual disabilities. Res Dev Disabil. 2013;34(4):1144–51.
Tranah GJ, Blackwell T, Stone KL, Ancoli-Israel S, Paudel ML, Ensrud KE, et al. Circadian activity rhythms and risk of incident dementia and mild cognitive impairment in older women. Ann Neurol. 2011;70(5):722–32.
Thome J, Coogan AN, Woods AG, Darie CC, Hassler F. CLOCK genes and circadian rhythmicity in Alzheimer disease. J Aging Res. 2011;2011:383091.
Katz B, Rimmer S, Iragui V, Katzman R. Abnormal pattern electroretinogram in Alzheimer’s disease: evidence for retinal ganglion cell degeneration? Ann Neurol. 1989;26(2):221–5.
Hanford N, Figueiro M. Light therapy and Alzheimer’s disease and related dementia: past, present, and future. J Alzheimers Dis. 2013;33(4):913–22.
Figueiro MG, Hamner R, Higgins P, Hornick T, Rea MS. Field measurements of light exposures and circadian disruption in two populations of older adults. J Alzheimers Dis. 2012;31(4):711–5.
Meadows R, Luff R, Eyers I, Venn S, Cope E, Arber S. An actigraphic study comparing community dwelling poor sleepers with non-demented care home residents. Chronobiol Int. 2010;27(4):842–54.
Wu YH, Swaab DF. The human pineal gland and melatonin in aging and Alzheimer’s disease. J Pineal Res. 2005;38(3):145–52.
Madeira MD, Pereira PA, Silva SM, Cadete-Leite A, Paula-Barbosa MM. Basal forebrain neurons modulate the synthesis and expression of neuropeptides in the rat suprachiasmatic nucleus. Neuroscience. 2004;125(4):889–901.
Dragicevic N, Copes N, O’Neal-Moffitt G, Jin J, Buzzeo R, Mamcarz M, et al. Melatonin treatment restores mitochondrial function in Alzheimer’s mice: a mitochondrial protective role of melatonin membrane receptor signaling. J Pineal Res. 2011;51(1):75–86.
Olcese JM, Cao C, Mori T, Mamcarz MB, Maxwell A, Runfeldt MJ, et al. Protection against cognitive deficits and markers of neurodegeneration by long-term oral administration of melatonin in a transgenic model of Alzheimer disease. J Pineal Res. 2009;47(1):82–96.
Stranahan AM. Chronobiological approaches to Alzheimer’s disease. Curr Alzheimer Res. 2012;9(1):93–8.
Kang JE, Lim MM, Bateman RJ, Lee JJ, Smyth LP, Cirrito JR, et al. Amyloid-beta dynamics are regulated by orexin and the sleep-wake cycle. Science. 2009;326(5955):1005–7.
Xie L, Kang H, Xu Q, Chen MJ, Liao Y, Thiyagarajan M, et al. Sleep drives metabolite clearance from the adult brain. Science. 2013;342(6156):373–7.
Onen F, Onen H. [Obstructive sleep apnea and cognitive impairment in the elderly]. Psychol Neuropsychiatr Vieil. 2010;8(3):163–9.
Guarnieri B, Adorni F, Musicco M, Appollonio I, Bonanni E, Caffarra P, et al. Prevalence of sleep disturbances in mild cognitive impairment and dementing disorders: a multicenter Italian clinical cross-sectional study on 431 patients. Dement Geriatr Cogn Disord. 2012;33(1):50–8.
Rose KM, Beck C, Tsai PF, Liem PH, Davila DG, Kleban M, et al. Sleep disturbances and nocturnal agitation behaviors in older adults with dementia. Sleep. 2011;34(6):779–86.
Singer C, Tractenberg RE, Kaye J, Schafer K, Gamst A, Grundman M, et al. A multicenter, placebo-controlled trial of melatonin for sleep disturbance in Alzheimer’s disease. Sleep. 2003;26(7):893–901. This is the landmark study showing the futility of melatonin as a treatment for sleep disturbances in Alzheimer’s disease.
Serfaty M, Kennell-Webb S, Warner J, Blizard R, Raven P. Double-blind randomised placebo-controlled trial of low-dose melatonin for sleep disorders in dementia. Int J Geriatric Psychiatry. 2002;17(12):1120–7.
Gehrman PR, Connor DJ, Martin JL, Shochat T, Corey-Bloom J, Ancoli-Israel S. Melatonin fails to improve sleep or agitation in double-blind randomized placebo-controlled trial of institutionalized patients with Alzheimer disease. Am J Geriatric Psychiatry: Off J Am Assoc Geriatric Psychiatry. 2009;17(2):166–9.
Asayama K, Yamadera H, Ito T, Suzuki H, Kudo Y, Endo S. Double blind study of melatonin effects on the sleep-wake rhythm, cognitive and non-cognitive functions in Alzheimer type dementia. J Nippon Med Sch. 2003;70(4):334–41.
Dowling GA, Burr RL, Van Someren EJ, Hubbard EM, Luxenberg JS, Mastick J, et al. Melatonin and bright-light treatment for rest-activity disruption in institutionalized patients with Alzheimer’s disease. J Am Geriatr Soc. 2008;56(2):239–46.
Mahlberg R, Walther S. Actigraphy in agitated patients with dementia. Monitoring treatment outcomes. Z Gerontol Geriatr. 2007;40(3):178–84.
Figueiro M. A proposed 24-h lighting scheme for older adults. Light Res Technol. 2008;40(2):153–60.
Peter-Derex L, Yammine P, Bastuji H, Croisile B. Sleep and Alzheimer’s disease. Sleep Med Rev. 2015;19C:29–38. This is an up to date and comprehensive review of sleep and its disorders in Alzheimer’s disease.
de Lau LM, Breteler MM. Epidemiology of Parkinson’s disease. Lancet Neurol. 2006;5(6):525–35.
Duncan GW, Khoo TK, Yarnall AJ, O’Brien JT, Coleman SY, Brooks DJ, et al. Health-related quality of life in early Parkinson’s disease: the impact of nonmotor symptoms. Mov Disord. 2014;29(2):195–202.
Lees AJ, Blackburn NA, Campbell VL. The nighttime problems of Parkinson’s disease. Clin Neuropharmacol. 1988;11(6):512–9.
Tandberg E, Larsen JP, Karlsen K. A community-based study of sleep disorders in patients with Parkinson’s disease. Mov Disord. 1998;13(6):895–9.
Dauvilliers Y. Insomnia in patients with neurodegenerative conditions. Sleep Med. 2007;8 Suppl 4:S27–34.
Oerlemans WG, de Weerd AW. The prevalence of sleep disorders in patients with Parkinson’s disease. A self-reported, community-based survey. Sleep Med. 2002;3(2):147–9.
Avidan A, Hays RD, Diaz N, Bordelon Y, Thompson AW, Vassar SD, et al. Associations of sleep disturbance symptoms with health-related quality of life in Parkinson’s disease. J Neuropsychiatry Clin Neurosci. 2013;25(4):319–26.
Adler CH, Thorpy MJ. Sleep issues in Parkinson’s disease. Neurology. 2005;64(12 Suppl 3):S12–20.
Stavitsky K, Neargarder S, Bogdanova Y, McNamara P, Cronin-Golomb A. The impact of sleep quality on cognitive functioning in Parkinson’s disease. J Int Neuropsychol Soc. 2012;18(1):108–17.
Pal PK, Thennarasu K, Fleming J, Schulzer M, Brown T, Calne SM. Nocturnal sleep disturbances and daytime dysfunction in patients with Parkinson’s disease and in their caregivers. Parkinsonism Relat Disord. 2004;10(3):157–68.
Ferreira T, Prabhakar S, Kharbanda PS. Sleep disturbances in drug naive Parkinson’s disease (PD) patients and effect of levodopa on sleep. Ann Indian Acad Neurol. 2014;17(4):416–9.
Braak H, Del Tredici K, Rub U, de Vos RA, Jansen Steur EN, Braak E. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol Aging. 2003;24(2):197–211.
Rye DB. The two faces of Eve: dopamine’s modulation of wakefulness and sleep. Neurology. 2004;63(8 Suppl 3):S2–7.
Qiu MH, Yao QL, Vetrivelan R, Chen MC, Lu J. Nigrostriatal Dopamine Acting on Globus Pallidus Regulates Sleep. Cereb Cortex. 2014. This experimental study in rats showed that the dopaminergic neurons in the substantia nigra is part of a pathway through the basal ganglia that influences sleep and wake state control. These results link key areas of degeneration in Parkinson’s disease to insomnia and hypersomnia.
Kaynak D, Kiziltan G, Kaynak H, Benbir G, Uysal O. Sleep and sleepiness in patients with Parkinson’s disease before and after dopaminergic treatment. Eur J Neurol. 2005;12(3):199–207.
van Hilten B, Hoff JI, Middelkoop HA, van der Velde EA, Kerkhof GA, Wauquier A, et al. Sleep disruption in Parkinson’s disease. Assessment by continuous activity monitoring. Arch Neurol. 1994;51(9):922–8.
Whitehead DL, Davies AD, Playfer JR, Turnbull CJ. Circadian rest-activity rhythm is altered in Parkinson’s disease patients with hallucinations. Mov Disord. 2008;23(8):1137–45.
Zhong G, Bolitho S, Grunstein R, Naismith SL, Lewis SJ. The relationship between thermoregulation and REM sleep behaviour disorder in Parkinson’s disease. PLoS One. 2013;8(8):e72661.
Videnovic A, Noble C, Reid KJ, Peng J, Turek FW, Marconi A, et al. Circadian melatonin rhythm and excessive daytime sleepiness in Parkinson disease. JAMA Neurol. 2014;71(4):463–9. The results of this cross-sectional study showed that circadian melatonin rhythm is blunted in Parkinson’s disease, and that this relates to hypersomnia in these patients.
Stuebner E, Vichayanrat E, Low DA, Mathias CJ, Isenmann S, Haensch CA. Twenty-four-hour non-invasive ambulatory blood pressure and heart rate monitoring in Parkinson’s disease. Front Neurol. 2013;4:49.
Hartmann A, Veldhuis JD, Deuschle M, Standhardt H, Heuser I. Twenty-four-hour cortisol release profiles in patients with Alzheimer’s and Parkinson’s disease compared to normal controls: ultradian secretory pulsatility and diurnal variation. Neurobiol Aging. 1997;18(3):285–9.
Turner PL, Mainster MA. Circadian photoreception: ageing and the eye’s important role in systemic health. Br J Ophthalmol. 2008;92(11):1439–44.
Van Someren EJ. Circadian and sleep disturbances in the elderly. Exp Gerontol. 2000;35(9–10):1229–37.
Rutten S, Vriend C, van den Heuvel OA, Smit JH, Berendse HW, van der Werf YD. Bright light therapy in Parkinson’s disease: an overview of the background and evidence. Parkinsons Dis. 2012;2012:767105.
Kudo T, Loh DH, Truong D, Wu Y, Colwell CS. Circadian dysfunction in a mouse model of Parkinson’s disease. Exp Neurol. 2011;232(1):66–75.
Pahwa R, Stacy MA, Factor SA, Lyons KE, Stocchi F, Hersh BP, et al. Ropinirole 24-hour prolonged release: randomized, controlled study in advanced Parkinson disease. Neurology. 2007;68(14):1108–15.
Poewe WH, Rascol O, Quinn N, Tolosa E, Oertel WH, Martignoni E, et al. Efficacy of pramipexole and transdermal rotigotine in advanced Parkinson’s disease: a double-blind, double-dummy, randomised controlled trial. Lancet Neurol. 2007;6(6):513–20.
Lima MM. Sleep disturbances in Parkinson’s disease: the contribution of dopamine in REM sleep regulation. Sleep Med Rev. 2013;17(5):367–75.
Rios Romenets S, Creti L, Fichten C, Bailes S, Libman E, Pelletier A, et al. Doxepin and cognitive behavioural therapy for insomnia in patients with Parkinson’s disease—a randomized study. Parkinsonism Relat Disord. 2013;19(7):670–5.
Willis GL, Moore C, Armstrong SM. A historical justification for and retrospective analysis of the systematic application of light therapy in Parkinson’s disease. Rev Neurosci. 2012;23(2):199–226.
Willis GL, Turner EJ. Primary and secondary features of Parkinson’s disease improve with strategic exposure to bright light: a case series study. Chronobiol Int. 2007;24(3):521–37.
Medeiros CA, Carvalhedo de Bruin PF, Lopes LA, Magalhaes MC, de Lourdes Seabra M, de Bruin VM. Effect of exogenous melatonin on sleep and motor dysfunction in Parkinson’s disease. A randomized, double-blind, placebo-controlled study. J Neurol. 2007;254(4):459–64.
Dowling GA, Mastick J, Colling E, Carter JH, Singer CM, Aminoff MJ. Melatonin for sleep disturbances in Parkinson’s disease. Sleep Med. 2005;6(5):459–66.
Cochen De Cock V, Bayard S, Jaussent I, Charif M, Grini M, Langenier MC, et al. Daytime sleepiness in Parkinson’s disease: a reappraisal. PLoS One. 2014;9(9):e107278.
Ondo WG, Dat Vuong K, Khan H, Atassi F, Kwak C, Jankovic J. Daytime sleepiness and other sleep disorders in Parkinson’s disease. Neurology. 2001;57(8):1392–6.
Arnulf I, Konofal E, Merino-Andreu M, Houeto JL, Mesnage V, Welter ML, et al. Parkinson’s disease and sleepiness: an integral part of PD. Neurology. 2002;58(7):1019–24.
Poryazova R, Benninger D, Waldvogel D, Bassetti CL. Excessive daytime sleepiness in Parkinson’s disease: characteristics and determinants. Eur Neurol. 2010;63(3):129–35.
Thannickal TC, Lai YY, Siegel JM. Hypocretin (orexin) cell loss in Parkinson’s disease. Brain. 2007;130(Pt 6):1586–95.
Bliwise DL, Trotti LM, Juncos JJ, Factor SA, Freeman A, Rye DB. Daytime REM sleep in Parkinson’s disease. Parkinsonism Relat Disord. 2013;19(1):101–3.
Korner Y, Meindorfner C, Moller JC, Stiasny-Kolster K, Haja D, Cassel W, et al. Predictors of sudden onset of sleep in Parkinson’s disease. Mov Disord. 2004;19(11):1298–305.
Paus S, Brecht HM, Koster J, Seeger G, Klockgether T, Wullner U. Sleep attacks, daytime sleepiness, and dopamine agonists in Parkinson’s disease. Mov Disord. 2003;18(6):659–67.
Ferreira JJ, Desboeuf K, Galitzky M, Thalamas C, Brefel-Courbon C, Fabre N, et al. Sleep disruption, daytime somnolence and ‘sleep attacks’ in Parkinson’s disease: a clinical survey in PD patients and age-matched healthy volunteers. Eur J Neurol. 2006;13(3):209–14.
Asai H, Hirano M, Furiya Y, Udaka F, Morikawa M, Kanbayashi T, et al. Cerebrospinal fluid-orexin levels and sleep attacks in four patients with Parkinson’s disease. Clin Neurol Neurosurg. 2009;111(4):341–4.
da Silva-Junior Jr FP, do Prado GF, Barbosa ER, Tufik S, Togeiro SM. Sleep disordered breathing in Parkinson’s disease: a critical appraisal. Sleep Med Rev. 2014;18(2):173–8.
Zeng J, Wei M, Li T, Chen W, Feng Y, Shi R, et al. Risk of obstructive sleep apnea in Parkinson’s disease: a meta-analysis. PLoS One. 2013;8(12):e82091.
Breen DP, Vuono R, Nawarathna U, Fisher K, Shneerson JM, Reddy AB, et al. Sleep and circadian rhythm regulation in early Parkinson disease. JAMA Neurol. 2014;71(5):589–95.
Bolitho SJ, Naismith SL, Rajaratnam SM, Grunstein RR, Hodges JR, Terpening Z, et al. Disturbances in melatonin secretion and circadian sleep-wake regulation in Parkinson disease. Sleep Med. 2014;15(3):342–7. This cross-sectional study links dopaminergic therapy in Parkinson’s disease with increased melatonin secretion and circadian misalignment. Medicated patients with PD had higher melatonin secretion and longer phase angle between dim light melatonin onset and habitual sleep onset than unmedicated patients, who were not different from controls.
Adler CH, Caviness JN, Hentz JG, Lind M, Tiede J. Randomized trial of modafinil for treating subjective daytime sleepiness in patients with Parkinson’s disease. Mov Disord. 2003;18(3):287–93.
Hogl B, Saletu M, Brandauer E, Glatzl S, Frauscher B, Seppi K, et al. Modafinil for the treatment of daytime sleepiness in Parkinson’s disease: a double-blind, randomized, crossover, placebo-controlled polygraphic trial. Sleep. 2002;25(8):905–9.
Lokk J. Daytime sleepiness in elderly Parkinson’s disease patients and treatment with the psychostimulant modafinil: a preliminary study. Neuropsychiatr Dis Treat. 2010;6:93–7.
Tyne HL, Taylor J, Baker GA, Steiger MJ. Modafinil for Parkinson’s disease fatigue. J Neurol. 2010;257(3):452–6.
Lou JS, Dimitrova DM, Park BS, Johnson SC, Eaton R, Arnold G, et al. Using modafinil to treat fatigue in Parkinson disease: a double-blind, placebo-controlled pilot study. Clin Neuropharmacol. 2009;32(6):305–10.
Ondo WG, Fayle R, Atassi F, Jankovic J. Modafinil for daytime somnolence in Parkinson’s disease: double-blind, placebo-controlled parallel trial. J Neurol Neurosurg Psychiatry. 2005;76(12):1636–9.
Trotti LM, Bliwise DL. Treatment of the sleep disorders associated with Parkinson’s disease. Neurotherapeutics. 2014;11(1):68–77.
Ondo WG, Perkins T, Swick T, Hull Jr KL, Jimenez JE, Garris TS, et al. Sodium oxybate for excessive daytime sleepiness in Parkinson disease: an open-label polysomnographic study. Arch Neurol. 2008;65(10):1337–40.
American Academy of Sleep Medicine. International classification of sleep disorders. 3rd ed. Darien: American Academy of Sleep Medicine; 2014.
McCarter SJ, St Louis EK, Boswell CL, Dueffert LG, Slocumb N, Boeve BF, et al. Factors associated with injury in REM sleep behavior disorder. Sleep Med. 2014;15(11):1332–8.
Iranzo A, Fernandez-Arcos A, Tolosa E, Serradell M, Molinuevo JL, Valldeoriola F, et al. Neurodegenerative disorder risk in idiopathic REM sleep behavior disorder: study in 174 patients. PLoS One. 2014;9(2):e89741.
Sixel-Doring F, Trautmann E, Mollenhauer B, Trenkwalder C. Associated factors for REM sleep behavior disorder in Parkinson disease. Neurology. 2011;77(11):1048–54.
Bugalho P, Viana-Baptista M. REM sleep behavior disorder and motor dysfunction in Parkinson’s disease—a longitudinal study. Parkinsonism Relat Disord. 2013;19(12):1084–7.
Kumru H, Santamaria J, Tolosa E, Iranzo A. Relation between subtype of Parkinson’s disease and REM sleep behavior disorder. Sleep Med. 2007;8(7–8):779–83.
Postuma RB, Gagnon JF, Vendette M, Charland K, Montplaisir J. REM sleep behaviour disorder in Parkinson’s disease is associated with specific motor features. J Neurol Neurosurg Psychiatry. 2008;79(10):1117–21.
Benninger DH, Michel J, Waldvogel D, Candia V, Poryazova R, van Hedel HJ, et al. REM sleep behavior disorder is not linked to postural instability and gait dysfunction in Parkinson. Mov Disord. 2010;25(11):1597–604.
Videnovic A, Marlin C, Alibiglou L, Planetta PJ, Vaillancourt DE, Mackinnon CD. Increased REM sleep without atonia in Parkinson disease with freezing of gait. Neurology. 2013;81(12):1030–5.
Anang JB, Gagnon JF, Bertrand JA, Romenets SR, Latreille V, Panisset M, et al. Predictors of dementia in Parkinson disease: a prospective cohort study. Neurology. 2014;83(14):1253–60. This cohort study showed that REM sleep behavior disorder was associated with a very high risk of developing dementia over a 4.4 year follow up period.
Poryazova R, Oberholzer M, Baumann CR, Bassetti CL. REM sleep behavior disorder in Parkinson’s disease: a questionnaire-based survey. J Clin Sleep Med. 2013;9(1):55–9A.
Stiasny-Kolster K, Sixel-Doring F, Trenkwalder C, Heinzel-Gutenbrunner M, Seppi K, Poewe W, et al. Diagnostic value of the REM sleep behavior disorder screening questionnaire in Parkinson’s disease. Sleep Med. 2014;16(1):186–9.
Schenck CH, Bundlie SR, Ettinger MG, Mahowald MW. Chronic behavioral disorders of human REM sleep: a new category of parasomnia. Sleep. 1986;9(2):293–308.
Gaenslen A, Wurster I, Brockmann K, Huber H, Godau J, Faust B, et al. Prodromal features for Parkinson’s disease—baseline data from the TREND study. Eur J Neurol. 2014;21(5):766–72.
Iranzo A, Tolosa E, Gelpi E, Molinuevo JL, Valldeoriola F, Serradell M, et al. Neurodegenerative disease status and post-mortem pathology in idiopathic rapid-eye-movement sleep behaviour disorder: an observational cohort study. Lancet Neurol. 2013;12(5):443–53.
Pont-Sunyer C, Hotter A, Gaig C, Seppi K, Compta Y, Katzenschlager R, et al. The Onset of Nonmotor Symptoms in Parkinson’s disease (The ONSET PD Study). Mov Disord. 2014;30(2):229–37.
Schenck CH, Bundlie SR, Mahowald MW. Delayed emergence of a Parkinsonian disorder in 38% of 29 older men initially diagnosed with idiopathic rapid eye movement sleep behaviour disorder. Neurology. 1996;46(2):388–93.
Boeve BF, Silber MH, Ferman TJ, Lin SC, Benarroch EE, Schmeichel AM, et al. Clinicopathologic correlations in 172 cases of rapid eye movement sleep behavior disorder with or without a coexisting neurologic disorder. Sleep Med. 2013;14(8):754–62. This clinico-pathological series of 172 patients illustrates the strong link between REM behavior disorder and α-synucleinopathies.
Holtbernd F, Gagnon JF, Postuma RB, Ma Y, Tang CC, Feigin A, et al. Abnormal metabolic network activity in REM sleep behavior disorder. Neurology. 2014;82(7):620–7.
Rodrigues Brazete J, Montplaisir J, Petit D, Postuma RB, Bertrand JA, Genier Marchand D, et al. Electroencephalogram slowing in rapid eye movement sleep behavior disorder is associated with mild cognitive impairment. Sleep Med. 2013;14(11):1059–63.
Schenck CH, Montplaisir JY, Frauscher B, Hogl B, Gagnon JF, Postuma R, et al. Rapid eye movement sleep behavior disorder: devising controlled active treatment studies for symptomatic and neuroprotective therapy—a consensus statement from the International Rapid Eye Movement Sleep Behavior Disorder Study Group. Sleep Med. 2013;14(8):795–806.
Frauscher B, Jennum P, Ju YE, Postuma RB, Arnulf I, Cochen De Cock V, et al. Comorbidity and medication in REM sleep behavior disorder: a multicenter case-control study. Neurology. 2014;82(12):1076–9.
Zhang B, Hao Y, Jia F, Tang Y, Li X, Liu W, et al. Sertraline and rapid eye movement sleep without atonia: an 8-week, open-label study of depressed patients. Prog Neuropsychopharmacol Biol Psychiatry. 2013;47:85–92.
McCarter SJ, St Louis EK, Sandness DJ, Arndt K, Erickson M, Tabatabai G, et al. Antidepressants Increase REM Sleep Muscle Tone in Patients with and without REM Sleep Behavior Disorder. Sleep. 2014.
Postuma RB, Gagnon JF, Tuineaig M, Bertrand JA, Latreille V, Desjardins C, et al. Antidepressants and REM sleep behavior disorder: isolated side effect or neurodegenerative signal? Sleep. 2013;36(11):1579–85.
McCarter SJ, Boswell CL, St Louis EK, Dueffert LG, Slocumb N, Boeve BF, et al. Treatment outcomes in REM sleep behavior disorder. Sleep Med. 2013;14(3):237–42.
Kunz D, Mahlberg R. A two-part, double-blind, placebo-controlled trial of exogenous melatonin in REM sleep behaviour disorder. J Sleep Res. 2010;19(4):591–6.
McGrane IR, Leung JG, St Louis EK, Boeve BF. Melatonin therapy for REM sleep behavior disorder: a critical review of evidence. Sleep Med. 2015;16(1):19–26.
Nomura T, Kawase S, Watanabe Y, Nakashima K. Use of ramelteon for the treatment of secondary REM sleep behavior disorder. Intern Med. 2013;52(18):2123–6.
Di Giacopo R, Fasano A, Quaranta D, Della Marca G, Bove F, Bentivoglio AR. Rivastigmine as alternative treatment for refractory REM behavior disorder in Parkinson’s disease. Mov Disord. 2012;27(4):559–61.
Howell MJ, Arneson PA, Schenck CH. A novel therapy for REM sleep behavior disorder (RBD). J Clin Sleep Med. 2011;7(6):639–44A.
Compliance with Ethics Guidelines
Conflict of Interest
Roneil Malkani and Hrayr Attarian declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is part of the Topical Collection on Sleep and Neurological Disorders
Rights and permissions
About this article

Cite this article
Malkani, R., Attarian, H. Sleep in Neurodegenerative Disorders. Curr Sleep Medicine Rep 1, 81–90 (2015). https://doi.org/10.1007/s40675-015-0016-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40675-015-0016-x