
Abstract
Purpose of Review
To summarize both the research on and effects of physical activity tailoring in people with arthritis.
Recent Findings
Physical activity is an essential disease management strategy for people with arthritis. However, participation rates are low which may be due to generalized approaches to supporting physical activity behavior change. Tailored physical activity approaches involve the use of assessment to shape individualized intervention strategies to change physical activity. The effectiveness of tailored physical activity interventions in the general population is mixed, likely as a result of suboptimal tailoring methods, and the effectiveness in arthritis populations is unknown.
Summary
We identified 24 unique assessment factors and 23 intervention strategies used in tailored physical activity interventions for people with osteoarthritis, inflammatory arthritis, or fibromyalgia. Health professionals should conduct comprehensive patient characteristics, physical, and psychosocial assessments to select the optimal physical activity prescription and strategies to deliver it. While more research is needed to refine methods for optimal tailoring of physical activity interventions for people with arthritis, health professionals should familiarize themselves with factors to consider for tailoring, collaborate with their patients on decisions about tailoring their physical activity, and adapt tailoring approaches as required over time to optimize physical activity participation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Physical activity, defined as any voluntary bodily movement that is produced by skeletal muscles and requires energy expenditure [1], is an essential component of successful disease self-management in people with arthritis. Extant research shows that it can improve pain, function, and quality of life [2, 3], and is safe for people with osteoarthritis (OA) and inflammatory arthritis (IA) [4]. Six million people currently live with arthritis in Canada, and this number is projected to reach 10.4 million by 2042 [5]. Among older adults, arthritis often coexists with frailty, which poses a greater risk of falls [6, 7], increased morbidity, physical dependence, and hospitalization [8, 9]. Physical activity can prevent the progression of frailty [10, 11], partly by mitigating the effects of arthritis [2, 3] and the progression of concomitant conditions such as cardiovascular disease [12] and type 2 diabetes [13].
Physical activity is beneficial during all phases of chronic disease management, from primary prevention through rehabilitation and ongoing care. However, only 49% of adults aged 18–79 in Canada engage in enough physical activity to meet the World Health Organization recommendations [14]. Among people with arthritis, physical activity participation is even lower than the general population [15,16,17]. Introducing physical activity to this population is challenging as their ability to engage in activities can be affected by their symptoms, their health status (including comorbidities), or other external factors.
Both clinicians and academics have identified the lack of precision in physical activity prescription and promotion as a limitation to supporting health behavior change. In a cohort of 172 people with OA and IA who were eligible for physical activity intervention studies [18, 19], Feehan et al. [20•] identified four distinct activity profiles based on the average time participants spent daily sleeping, sitting, and walking in different intensities. Their findings suggest that a range of individualized strategies may be required to help people achieve their optimal balance between activity and rest [21•].
Physical Activity Tailoring
If we want to improve physical activity participation among people with arthritis, we need to move away from a one-size-fits-all approach and toward a personalized approach. We define “physical activity tailoring” as a process whereby health professionals use patient assessments to shape a personalized strategy to support an active lifestyle [22•], taking into account the patient’s characteristics, preferences, needs, and context [23]. When a health professional is tailoring physical activity interventions, they assess individual factors (e.g., physical activity history, fitness, psychosocial factors) and health status (e.g., disease activity, symptoms) by inquiry, observation, physical examination, and/or monitoring. They then use this information to design the “what” (e.g., activity type, frequency, and intensity) and “how” to deliver the prescription (e.g., a combination of behavior change techniques (BCT), who delivers, using what mode of delivery) [24] to support individuals to engage in those activities. The purpose of this review is to first summarize the research on the use of physical activity tailoring in people with OA, IA, and related conditions (e.g., fibromyalgia). Secondly, we report the effectiveness of different tailoring strategies on physical activity behavior in this population.
Methods
Search Strategy and Literature Screening
The systematic review protocol has been registered at PROSPERO (https://www.crd.york.ac.uk/prospero/; Registration CRD42020215513). We followed the PRISMA guidelines and searched the PROSPERO database for similar reviews before commencing this review. This review was co-developed with people living with arthritis and health professionals (KT, AMH). We also consulted with the Arthritis Patient Advisory Board, a group of advocates who bring their personal experiences and expertise with arthritis to research decision-making. Their involvement included shaping the research question, refining the data extraction, reviewing the findings, and identifying priority topics for discussion.
The search strategy was developed with an experienced research librarian. The search was conducted in June 2020 and updated in May 2022. We searched five electronic bibliographic databases including PubMed, PsycINFO, CINAHL, Embase (Ovid), and MEDLINE (Ovid). Our search included terms for tailoring, physical activity, and arthritis. See Online Resource: Fig. 1 for a sample search strategy. In addition, we hand-searched reference lists of included articles and conducted forward citation searching.
Eligible articles (1) were original studies, (2) included people with arthritis and related conditions, (3) included a tailored intervention to promote physical activity participation, and (4) included a measure of physical activity behavior. Articles were excluded when either (1) the intervention did not include an assessment or a form of assessment for tailoring, and (2) the article was written in a language other than English.
We transferred all the retrieved articles from each bibliographic database to Covidence (www.covidence.org; Veritas Health Innovation, Melbourne, Australia) for screening, and removed all duplicate articles. Two reviewers (SR, AS) screened all articles by their titles and abstracts and then reviewed the full articles for those that appeared to be eligible. A third reviewer (JM) mediated any discrepancies. JM and DH completed the updated search following the same procedure.
Data Extraction and Analysis
We developed a data extraction form in consultation with Arthritis Patient Advisory Board members. Two reviewers (SR and AS) were trained by an experienced researcher (JM) and pilot-tested the data extraction with 10% of the papers for calibration. One reviewer (SR) extracted data from the remaining articles and a second reviewer (AS) checked them. The following information was extracted: study details, intervention details, change in physical activity behavior, and tailoring factors (timing, frequency, and content of assessments, who or what conducted the assessment and delivered intervention components, which assessments were explicitly paired with tailored intervention components).
We summarized the study and intervention characteristics in descriptive statistics. For each included study, we mapped the assessment and tailoring strategies used (Fig. 1). One experienced reviewer (JM) coded the tailored intervention strategies for BCTs using the 93 Behaviour Change Technique Taxonomy version 1 (BCTTv1) [24]. The BCTTv1 has previously demonstrated support for good inter-coder and test–retest reliability [25].

Tailoring checklist: summary of tailoring methods and considerations used across studies
Appraisal of the Evidence
We assessed the quality of the studies with the Cochrane Risk of Bias (ROB) tool (for randomized controlled trials, RCTs) [26], and the Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I; for non-RCTs) [27]. When interpreting overall risk of bias for randomized controlled trials, we did not consider blinding of participants given the challenge of blinding in a physical activity intervention. Random sequence generation, blinding of outcome assessment, incomplete outcome data, and other bias domains were prioritized in the overall Cochrane ROB appraisal.
Results
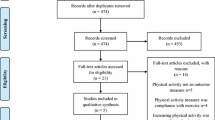
The systematic search retrieved 2121 records; of those, 257 passed the title and abstract screening. After the full-text screening, 78 articles (from 39 studies) were included (Online Resource File 1: List of Included Studies), with a total of 13,626 participants (individual study sample size varied from 3 to 8894 participants) (Online Resource Fig. 2: PRISMA Flow Diagram). The primary reasons for exclusion were (1) not an original article (n = 99), (2) did not measure physical activity behavior (n = 30), and (3) did not conduct a tailored intervention (n = 13). For the complete data extraction, see Open Science Framework Repository: https://osf.io/t7ybv/.
Study Characteristics
Of the 39 total studies identified (Table 1), 31 were randomized controlled trials [18, 19, 28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56]. Twelve studies were categorized as low risk of bias [18, 39,40,41, 44, 49, 51, 52, 54, 55, 57, 58], 13 as moderate risk of bias [28,29,30, 32, 35, 37, 38, 42, 50, 53, 56, 59, 60], and 14 as high risk of bias [19, 31, 33, 34, 36, 43, 45,46,47,48, 61,62,63,64] (Online Resource: Table 1 and 2). The mean age of participants varied from 48 to 72 years old. Twenty-three studies reported on physical activity tailoring in participants with OA [19, 28, 29, 31, 34, 35, 37, 42,43,44,45, 47, 48, 50,51,52,53, 56,57,58, 62,63,64], 13 in participants with IA [18, 30, 32, 33, 38, 40, 41, 46, 49, 54, 55, 59, 60], and 3 in participants with fibromyalgia [36, 39, 61] (Table 1). The disease duration of study participants ranged from 1.75 to 20 years.
Intervention Details
The interventions employed in the studies lasted from 19 days to 2 years. Twenty-eight interventions were delivered in-person, while the rest (n = 11) were delivered remotely (e.g., via app, telephone, website) (Table 2). Most interventions (n = 31) were delivered by a health professional (physiotherapist, occupational therapist, nurse, physician, exercise physiologist). Providers who delivered interventions were variably trained in counseling, motivational interviewing, autonomy-supportive strategies, behavior change techniques, exercise prescription, stages of change, patient-practitioner collaboration, effective communication, and brief action planning.
Changes in Physical Activity Participation
Of the 39 studies, 27 demonstrated significant improvements in at least one measure of physical activity over time [18, 19, 28,29,30,31,32, 35, 36, 38, 40, 42,43,44,45,46,47,48,49,50,51,52, 55, 56, 58, 59, 63]. Sixteen interventions demonstrated significant improvements in physical activity in comparison to control groups [19, 28,29,30, 35, 40, 42, 44,45,46,47,48,49,50,51,52], though 4 of those interventions were appraised as having a high risk of bias.
Tailoring Methods
Figure 1 summarizes the tailoring methods and considerations used across the studies and provides a checklist to guide decision-making. The majority of studies conducted assessments throughout the intervention (n = 29), at baseline only (n = 2), or used both baseline and repeated assessments throughout the intervention (n = 8). Assessment was conducted by a human (n = 30), technology/device (n = 5), both (n = 3), or was not reported (n = 1). Both the interventionist and participant (n = 26), only the interventionist (n = 9), technology/device and participant (n = 3), or all of the above (n = 1) decided which tailored intervention components were delivered based on the assessment.
Interventionists and patients shared decision-making responsibility for the tailoring of the intervention in 10/12 interventions that demonstrated significant differences between groups in favor of the tailored intervention in at least one outcome of physical activity behavior (excluding high risk of bias studies). In all the effective interventions, assessments to inform tailored approaches were reassessed at multiple time points. The remainder of tailoring methods did not demonstrate consistent patterns across effective, low-moderate risk studies. See Online Resource: Table 3 for the full tailoring characteristic data extraction.
Assessment Factors and Intervention Strategies used in Tailoring
Figure 1 contains a summary of assessment and intervention factors used for tailoring across the included studies (labeled as “tailoring options”). Online Resource: Figs. 3 and 4 contain the assessment and intervention factors employed by each study. A total of 24 unique assessment factors and 23 intervention strategies for tailoring were used across the studies. The most commonly used assessment factors were past physical activity (n = 22), disease symptoms (n = 16), physical function (n = 14), fitness (n = 14), goals (n = 14), barriers (n = 13), and confidence (n = 11). The most commonly used tailored intervention strategies were goal setting (n = 27), physical activity prescription (n = 24), and problem solving (n = 17).
Among the low-moderate risk of bias interventions that demonstrated significant differences between groups’ physical activity behavior in favor of the tailored intervention, the assessment factors were barriers, confidence, demographics, disease symptoms, fitness, goals, mood, motivation, needs, past physical activity, physical function, and preferences (activity type, setting, general/not defined). The tailored intervention strategies included behavior change techniques (action planning, body changes, goal setting, environmental context and resources, information about health consequences, instructions on how to perform the behavior, problem solving, reinforcement), intervention dose, provider, and physical activity equipment, options, and prescription.
Discussion
This review provides a summary of tailoring methods used to date in physical activity interventions for people with arthritis. The evidence suggests that assessments to guide tailoring should be made repeatedly over time and that the health professional and the patient should make decisions together about tailoring. Health professionals may be able to select more appropriately tailored intervention strategies if they assess factors such as patient characteristics (e.g., demographics, disease symptoms, physical function), barriers (e.g., needs, confidence, motivation), and physical activity readiness and preferences (e.g., physical activity history, fitness, goals). Such strategies may include tailoring behavior change techniques (e.g., action planning, problem solving, provision of resources), the frequency of using these techniques, exercise prescriptions, and who should deliver the intervention.
Are Tailored Physical Activity Interventions Effective for People with Arthritis?
Overall, tailored interventions appear to be effective in improving physical activity participation among people with arthritis. However, we were unable to determine whether they are more effective than generic interventions given the lack of studies comparing the use of these approaches in this population. Meta-analyses have shown that tailored interventions demonstrate only small effects [65] or have demonstrated smaller effects than generic interventions for changing physical activity behavior in the general population [66]. However, select reviews and randomized controlled trials have supported the use of tailored interventions in improving physical activity behavior and demonstrated medium- to large-sized effects [67]. Well-defined moderators of physical activity behavior also signal the value of tailored interventions [68, 69]. Taken together, we argue that comparing the effectiveness of tailored vs. non-tailored interventions is premature without evidence for optimizing tailoring methods [22•]. Our summary of tailoring methods used across studies and recommendations for effective strategies is a step toward improving our understanding of optimal tailoring approaches. Further research is needed to define how tailoring approaches can be refined before quantifying or comparing its value in physical activity interventions. Therefore, while it is unclear whether tailored physical activity interventions are more effective than generic interventions among people with arthritis, our review notes the common use of certain tailored approaches in studies with effective interventions, which may indicate the importance of taking into account a patient’s characteristics, physical abilities, and psychosocial needs in client-centered care.
How do Health Professionals Learn to Tailor?
There is likely room for both systematic and humanistic approaches to tailoring. The Behaviour Change Wheel is one example of a systematic approach using evidence- and consensus-based links to tailor behavior change techniques to identified barriers [70]. The questions and checklist provided in this review may also help health professionals and researchers strategically plan tailoring in a systematic fashion. A key finding of this review is that a tailored physical activity intervention strategy has more chance of success if the health professional and patient collaborate on how to structure it. None of the included studies reported details of the decision-making process, possibly because the collaboration with patients was more intuitive than systematic (i.e., following a distinct procedure). Many health professionals are already tailoring strategies instinctively by employing aspects of motivational interviewing (compassion, acceptance, partnership, evocation) and principles of shared decision-making (e.g., situation diagnosis, option clarification, deliberation of patient preferences) [71, 72•]. Another point of consideration is that none of the included interventions mentioned self-tailoring, where patients alone decide on the intervention strategies and how they are tailored. Self-tailoring stems from the concept of self-management, whereby patients use self-management skills, decision-making skills, and problem-solving skills to apply knowledge to themselves as appropriate [73]. Collaborating with and equipping patients to self-tailor may be another tailoring strategy that benefits both health professionals’ workload and patient outcomes. As the literature for optimal physical activity tailoring strategies among patients with arthritis builds, it is important to consider not only “what” we tailor, but “how” and “with whom” we tailor.
Limitations and Future Directions
We acknowledge that this review has certain limitations. First, most studies did not provide enough detail for their tailoring methods to be reproducible. Therefore, the coding we conducted produced broad categories for tailoring, but important nuances like specific questions to ask or specific assessment tools to use are missing. Second, the checklist in Fig. 1 is a compilation of tailoring options that were included across the studies in this review and is not an exhaustive list. Furthermore, it is challenging to single out effective components of complex interventions as they likely intertwine and overlap. We encourage researchers and health professionals to build on our list and use principles of evidence-informed practice to decide with their patients which tailoring options are best suited for them [74]. Lastly, given the heterogeneity of the included tailoring approaches and limitations in study reporting, we were unable to define explicit links between assessments and strategies (i.e., if X finding is determined from the assessment, then Y strategy should be implemented). In the future, the specific links between assessment factors and tailored intervention strategies should be explored and more clearly defined.
Conclusion
Physical activity is a complex behavior that is influenced by demographic, physical, and psychosocial factors. Health professionals and researchers who want to move beyond generic interventions and increase physical activity participation among people with arthritis may benefit from using tailored approaches that involve patients in the decision-making process, can adapt to each patient’s changing needs over time, and are based on a broad range of relevant assessment factors. While much more work is needed to develop and refine methods for optimal tailoring, health professionals can start by familiarizing themselves with their options for tailoring and take a patient-centered approach to guide their decision-making and help more people with arthritis to be physically active.
References and Recommended Reading
Papers of particular interest, published recently, have been highlighted as: • Of importance
Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 1985;100:126–31.
Fransen M, McConnell S, Harmer AR, Van der Esch M, Simic M, Bennell KL. Exercise for osteoarthritis of the knee: a Cochrane systematic review. Br J Sports Med. 2015;49:1554–7.
Juhl C, Christensen R, Roos EM, Zhang W, Lund H. Impact of exercise type and dose on pain and disability in knee osteoarthritis: a systematic review and meta-regression analysis of randomized controlled trials. Arthritis Rheumatol. 2014;66:622–36.
Quicke JG, Foster NE, Thomas MJ, Holden MA. Is long-term physical activity safe for older adults with knee pain?: a systematic review. Osteoarthr Cartil. 2015;23:1445–56.
Badley EM, Wilfong JM, Zahid S, Perruccio AV. The status of arthritis in Canada: national report. Toronto: Arthritis Community Research and Evaluation Unit (ACREU); 2019.
Iijima H, Shimoura K, Aoyama T, Takahashi M. Low back pain as a risk factor for recurrent falls in people with knee osteoarthritis. Arthritis Care Res. 2021;73:328–35.
Stanmore EK, Oldham J, Skelton DA, O’Neill T, Pilling M, Campbell AJ, Todd C. Risk factors for falls in adults with rheumatoid arthritis: a prospective study. Arthritis Care Res. 2013;65:1251–8.
Fried L, Tangen C, Walston J, Newman A, Hirsch C, Gottdiener J, Seeman T, Tracy R, Kop W, Burke G, McBurnie M. Frailty in older adults: evidence for a phenotype. J Gerontol. 2001;56:M146-156.
Veronese N, Maggi S, Trevisan C, Noale M, De Rui M, Bolzetta F, Zambon S, Musacchio E, Sartori L, Perissinotto E, Stubbs B, Crepaldi G, Manzato E, Sergi G. Pain increases the risk of developing frailty in older adults with osteoarthritis. Pain Med. 2017;18:414–27.
Yamada M, Arai H, Sonoda T, Aoyama T. Community-based exercise program is cost-effective by preventing care and disability in Japanese frail older adults. J Am Med Dir Assoc. 2012;13:507–11.
Kidd T, Mold F, Jones C, Ream E, Grosvenor W, Sund-Levander M, Tingström P, Carey N. What are the most effective interventions to improve physical performance in pre-frail and frail adults? A systematic review of randomised control trials. BMC Geriatr. 2019;19:184.
Higueras-Fresnillo S, Cabanas-Sánchez V, Lopez-Garcia E, Esteban-Cornejo I, Banegas JR, Sadarangani KP, Rodríguez-Artalejo F, Martinez-Gomez D. Physical activity and association between frailty and all-cause and cardiovascular mortality in older adults: population-based prospective cohort study. J Am Geriatr Soc. 2018;66:2097–103.
Hayashino Y, Jackson JL, Hirata T, Fukumori N, Nakamura F, Fukuhara S, Tsujii S, Ishii H. Effects of exercise on C-reactive protein, inflammatory cytokine and adipokine in patients with type 2 diabetes: a meta-analysis of randomized controlled trials. Metabolism. 2014;63:431–40.
Canadian Health Measures Survey: Activity Monitor Data, 2018–2019. Ottawa: Statistics Canada; 2021.
Wallis JA, Webster KE, Levinger P, Taylor NF. What proportion of people with hip and knee osteoarthritis meet physical activity guidelines? A systematic review and meta-analysis. Osteoarthr Cartil. 2013;21:1648–59.
Vancampfort D, Koyanagi A, Ward P. Chronic physical conditions, multimorbidity and physical activity across 46 low- and middle-income countries. Int J Behav Nutr Phys Act. 2017;14:6.
Vancampfort D, Stubbs B, Koyanagi A. Physical chronic conditions, multimorbidity and sedentary behavior amongst middle-aged and older adults in six low- and middle-income countries. Int J Behav Nutr Phys Act. 2017;14:147.
Li LC, Feehan LM, Xie H, Lu N, Shaw C, Gromala D, Aviña-Zubieta JA, Koehn C, Hoens AM, English K, Tam J, Therrien S, Townsend AF, Noonan G, Backman CL. Efficacy of a physical activity counseling program with use of a wearable tracker in people with inflammatory arthritis: a randomized controlled trial. Arthritis Care Res. 2020;72:1755–65.
Li LC, Feehan LM, Xie H, Lu N, Shaw CD, Gromala D, Zhu S, Aviña-Zubieta JA, Hoens AM, Koehn C, Tam J, Therrien S, Townsend AF, Noonan G, Backman CL. Effects of a 12-week multifaceted wearable-based program for people with knee osteoarthritis: randomized controlled trial. JMIR mHealth uHealth. 2020;8:e19116.
• Feehan LM, Lu N, Xie H, Li LC. Twenty-four hour activity and sleep profiles for adults living with arthritis: habits matter. Arthritis Care Res. 2020;72:1678–86. A cross-sectional cohort from two randomized controlled trials among people with arthritis demonstrating the potential for tailoring based on 24-h activity-sleep profiles.
• Li LC, Feehan LM, Hoens AM. Re-thinking physical activity promotion during COVID-19 pandemic: focus on a 24-hour day. J Rheumatol. 2021;48:1205–7. An editorial on changing how we promote physical activity by balancing activities across a 24-h day and considering inequities in physical activity promotion.
• Ma JK, Floegel TA, Li LC, Leese J, De Vera MA, Beauchamp MR, Taunton J, Liu-Ambrose T, Allen KD. Tailored physical activity behavior change interventions: challenges and opportunities. Transl Behav Med. 2021;11:2174–81. Defines tailored physical activity interventions and research priorities in this area.
Kreuter MW, Strecher VJ, Glassman B. One size does not fit all: the case for tailoring print materials. Ann Behav Med. 1999;21:276–83.
Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, Eccles MP, Cane J, Wood CE. The Behavior Change Technique Taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med. 2013;46:81–95.
Michie S, Wood CE, Johnston M, Abraham C, Francis JJ, Hardeman W. Behaviour change techniques: the development and evaluation of a taxonomic method for reporting and describing behaviour change interventions (a suite of five studies involving consensus methods, randomised controlled trials and analysis of qualitative data). Health Technol Assess. 2015;19:1–188.
Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, Savović J, Schulz KF, Weeks L, Sterne JAC. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928.
Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, Henry D, Altman DG, Ansari MT, Boutron I, Carpenter JR, Chan A-W, Churchill R, Deeks JJ, Hróbjartsson A, Kirkham J, Jüni P, Loke YK, Pigott TD, Ramsay CR, Regidor D, Rothstein HR, Sandhu L, Santaguida PL, Schünemann HJ, Shea B, Shrier I, Tugwell P, Turner L, Valentine JC, Waddington H, Waters E, Wells GA, Whiting PF, Higgins JP. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919.
Bossen D, Veenhof C, Van Beek KE, Spreeuwenberg PM, Dekker J, De Bakker DH. Effectiveness of a web-based physical activity intervention in patients with knee and/or hip osteoarthritis: randomized controlled trial. J Med Internet Res. 2013;15:e257.
Allen KD, Arbeeva L, Callahan LF, Golightly YM, Goode AP, Heiderscheit BC, Huffman KM, Severson HH, Schwartz TA. Physical therapy vs internet-based exercise training for patients with knee osteoarthritis: results of a randomized controlled trial. Osteoarthr Cartil. 2018;26:383–96.
Thomsen T, Aadahl M, Beyer N, Hetland ML, Loppenthin K, Midtgaard J, Christensen R, Ostergaard M, Jennum PJ, Esbensen BA. The efficacy of motivational counselling and SMS reminders on daily sitting time in patients with rheumatoid arthritis: a randomised controlled trial. Ann Rheum Dis. 2017;76:1603–6.
Brandes M, Wirsik N, Niehoff H, Heimsoth J, Mohring B. Impact of a tailored activity counselling intervention during inpatient rehabilitation after knee and hip arthroplasty - an explorative RCT. BMC Musculoskelet Disord. 2018;19:209.
Fenton SAM, Veldhuijzen van Zanten JJ, Metsios GS, Rouse PC, Yu CA, Ntoumanis N, Kitas GD, Duda JL. Testing a self-determination theory-based process model of physical activity behavior change in rheumatoid arthritis: results of a randomized controlled trial. Transl Behav Med. 2021;11:369–80.
Flint-Wagner HG, Lisse J, Lohman TG, Going SB, Guido T, Cussler E, Gates D, Yocum DE. Assessment of a sixteen-week training program on strength, pain, and function in rheumatoid arthritis patients. J Clin Rheumatol. 2009;15:165–71.
Gilbert AL, Lee J, Ehrlich-Jones L, Semanik PA, Song J, Pellegrini CA, Pinto Pt D, Dunlop DD, Chang RW. A randomized trial of a motivational interviewing intervention to increase lifestyle physical activity and improve self-reported function in adults with arthritis. Semin Arthritis Rheum. 2018;47:732–40.
Hinman RS, Campbell PK, Lawford BJ, Briggs AM, Gale J, Bills C, Kasza J, Harris A, French SD, Bunker SJ, Forbes A, Bennell KL. Does telephone-delivered exercise advice and support by physiotherapists improve pain and/or function in people with knee osteoarthritis? Telecare randomised controlled trial. Br J Sports Med. 2019;54:790–7.
Ang DC, Kaleth AS, Bigatti S, Mazzuca S, Jensen MP, Hilligoss J, Slaven JE, Saha C. Research to Encourage Exercise for Fibromyalgia (REEF)-use of motivational interviewing, outcomes from a randomized-controlled trial. Pain. 2013;29:296–304.
Hoogeboom TJ, Dronkers JJ, van den Ende CH, Oosting E, van Meeteren NL. Preoperative therapeutic exercise in frail elderly scheduled for total hip replacement: a randomized pilot trial. Clin Rehabil. 2010;24:901–10.
Brodin N, Eurenius E, Jensen I, Nisell R, Opava CH, Group tPS. Coaching patients with early rheumatoid arthritis to healthy physical activity: a multicenter, randomized, controlled study. Arthritis Rheum. 2008;59:325–31.
Da Costa D, Abrahamowicz M, Lowensteyn I, Bernatsky S, Dritsa M, Fitzcharles MA, Dobkin PL. A randomized clinical trial of an individualized home-based exercise programme for women with fibromyalgia. Rheumatology. 2005;44:1422–7.
O’Dwyer T, Monaghan A, Moran J, O’Shea F, Wilson F. Behaviour change intervention increases physical activity, spinal mobility and quality of life in adults with ankylosing spondylitis: a randomised trial. J Physiother. 2017;63:30–9.
Habers GE, Bos GJ, van Royen-Kerkhof A, Lelieveld OT, Armbrust W, Takken T, van Brussel M. Muscles in motion: a randomized controlled trial on the feasibility, safety and efficacy of an exercise training programme in children and adolescents with juvenile dermatomyositis. Rheumatology (Oxford). 2016;55:1251–62.
Bennell KL, Campbell PK, Egerton T, Metcalf B, Kasza J, Forbes A, Bills C, Gale J, Harris A, Kolt GS, Bunker SJ, Hunter DJ, Brand CA, Hinman RS. Telephone coaching to enhance a home-based physical activity program for knee osteoarthritis: a randomized clinical trial. Arthritis Care Res. 2017;69:84–94.
Hoorntje A, Witjes S, Kuijer P, Bussmann JBJ, Horemans HLD, Kerkhoffs G, van Geenen RCI, Koenraadt KLM. Does activity-based rehabilitation with goal attainment scaling increase physical activity among younger knee arthroplasty patients? Results from the randomized controlled ACTION trial. J Arthroplasty. 2020;35:706–11.
Skrepnik N, Spitzer A, Altman R, Hoekstra J, Stewart J, Toselli R. Assessing the impact of a novel smartphone application compared with standard follow-up on mobility of patients with knee osteoarthritis following treatment with Hylan G-F 20: a randomized controlled trial. JMIR Mhealth Uhealth. 2017;5:e64.
Veenhof C, Koke AJ, Dekker J, Oostendorp RA, Bijlsma JW, van Tulder MW, van den Ende CH. Effectiveness of behavioral graded activity in patients with osteoarthritis of the hip and/or knee: a randomized clinical trial. Arthritis Rheum. 2006;55:925–34.
Knittle K, De Gucht V, Hurkmans E, Peeters A, Ronday K, Maes S, Vlieland TV. Targeting motivation and self-regulation to increase physical activity among patients with rheumatoid arthritis: a randomised controlled trial. Clin Rheumatol. 2015;34:231–8.
Talbot LA, Gaines JM, Huynh TN, Metter EJ. A home-based pedometer-driven walking program to increase physical activity in older adults with osteoarthritis of the knee: a preliminary study. J Am Geriatr Soc. 2003;51:387–92.
Hughes SL, Seymour RB, Campbell PK, Pollak N, Huber G, Sharma L. Impact of the fit and strong intervention on older adults with osteoarthritis. Gerontologist. 2004;44:217–28.
van den Berg MH, Ronday HK, Peeters AJ, le Cessie S, van der Giesen FJ, Breedveld FC, Vliet Vlieland TP. Using internet technology to deliver a home-based physical activity intervention for patients with rheumatoid arthritis: a randomized controlled trial. Arthritis Rheum. 2006;55:935–45.
Murphy SL, Kratz AL, Kidwell K, Lyden AK, Geisser ME, Williams DA. Brief time-based activity pacing instruction as a singular behavioral intervention was not effective in participants with symptomatic osteoarthritis. Pain. 2016;157:1563–73.
Li LC, Sayre EC, Xie H, Clayton C, Feehan LM. A community-based physical activity counselling program for people with knee osteoarthritis: feasibility and preliminary efficacy of the TRACK-OA study. JMIR mHealth uHealth. 2017;5:e86.
Li LC, Sayre EC, Xie H, Falck RS, Best JR, Liu-Ambrose T, Grewal N, Hoens AM, Noonan G, Feehan LM. Efficacy of a community-based technology-enabled physical activity counseling program for people with knee osteoarthritis: proof-of-concept study. J Med Internet Res. 2018;20:e159.
Quicke JG, Foster NE, Croft PR, Ogollah RO, Holden MA. Change in physical activity level and clinical outcomes in older adults with knee pain: a secondary analysis from a randomised controlled trial. BMC Musculoskelet Disord. 2018;19:59.
Lamb SE, Williamson EM, Heine PJ, Adams J, Dosanjh S, Dritsaki M, Glover MJ, Lord J, McConkey C, Nichols V, Rahman A, Underwood M, Williams MA. Exercises to improve function of the rheumatoid hand (SARAH): a randomised controlled trial. Lancet. 2015;385:421–9.
Veldhuijzen van Zanten JJ, Fenton SAM, Rouse PC, Ntoumanis N, Osailan A, Yu C-a, Metsios GS, Kitas GD, Duda JL. Autonomous motivation, cardiorespiratory fitness, and exercise in rheumatoid arthritis: randomised controlled trial. Psychol Sport Exerc. 2021;55:101904.
Bendrik R, Kallings LV, Bröms K, Kunanusornchai W, Emtner M. Physical activity on prescription in patients with hip or knee osteoarthritis: a randomized controlled trial. Clin Rehabil. 2021;35:1465–77.
Allen K, Vu MB, Callahan LF, Cleveland RJ, Gilbert AL, Golightly YM, Griesemer I, Grimm K, Hales DP, Hu DG, Huffman K, Nelson AE, Pathak A, Rees J, Rethorn ZD, Wandishin AE. Osteoarthritis physical activity care pathway (OA-PCP): results of a feasibility trial. BMC Musculoskelet Disord. 2020;21:308.
Skou ST, Roos EM. Good Life with osteoArthritis in Denmark (GLA:D): evidence-based education and supervised neuromuscular exercise delivered by certified physiotherapists nationwide. BMC Musculoskelet Disord. 2017;18:72.
Nordgren B, Friden C, Demmelmaier I, Bergstrom G, Lundberg IE, Dufour AB, Opava CH, Group PS. An outsourced health-enhancing physical activity programme for people with rheumatoid arthritis: exploration of adherence and response. Rheumatology (Oxford). 2015;54:1065–73.
Stavropoulos-Kalinoglou A, Metsios GS, Veldhuijzen van Zanten JJ, Nightingale P, Kitas GD, Koutedakis Y. Individualised aerobic and resistance exercise training improves cardiorespiratory fitness and reduces cardiovascular risk in patients with rheumatoid arthritis. Ann Rheum Dis. 2013;72:1819–25.
Camerini L, Giacobazzi M, Boneschi M, Schulz PJ, Rubinelli S. Design and implementation of a web-based tailored gymnasium to enhance self-management of fibromyalgia. User Model User-Adap Inter. 2010;21:485–511.
O’Brien N, Philpott-Morgan S, Dixon D. Using impairment and cognitions to predict walking in osteoarthritis: a series of n-of-1 studies with an individually tailored, data-driven intervention. Br J Health Psychol. 2016;21:52–70.
Walker A, Williams R, Sibley F, Stamp D, Carter A, Hurley M. Improving access to better care for people with knee and/or hip pain: service evaluation of allied health professional-led primary care. Musculoskelet Care. 2018;16:222–32.
Lee FI, Lee TD, So WK. Effects of a tailor-made exercise program on exercise adherence and health outcomes in patients with knee osteoarthritis: a mixed-methods pilot study. Clin Interv Aging. 2016;11:1391–402.
Webb TL, Joseph J, Yardley L, Michie S. Using the internet to promote health behavior change: a systematic review and meta-analysis of the impact of theoretical basis, use of behavior change techniques, and mode of delivery on efficacy. J Med Internet Res. 2010;12:e4.
Conn VS, Hafdahl AR, Mehr DR. Interventions to increase physical activity among healthy adults: meta-analysis of outcomes. Am J Public Health. 2011;101:751–8.
Ma JK, West CR, Martin Ginis KA. The effects of a patient and provider co-developed, behavioral physical activity intervention on physical activity, psychosocial predictors, and fitness in individuals with spinal cord injury: a randomized controlled trial. Sports Med. 2019;49:1117–31.
Rhodes RE, Dickau L. Moderators of the intention-behaviour relationship in the physical activity domain: a systematic review. Br J Sports Med. 2013;47:215–25.
Bernard P, Carayol M, Gourlan M, Boiché J, Romain AJ, Bortolon C, Lareyre O, Ninot G. Moderators of theory-based interventions to promote physical activity in 77 randomized controlled trials. Health Educ Behav. 2017;44:227–35.
Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42.
Miller WR, Rollnick S. Motivatoinal interviewing: helping people change. 3rd ed. New York: Guilford Press; 2012.
• Wieringa TH, Rodriguez-Gutierrez R, Spencer-Bonilla G, de Wit M, Ponce OJ, Sanchez-Herrera MF, Espinoza NR, Zisman-Ilani Y, Kunneman M, Schoonmade LJ, Montori VM, Snoek FJ. Decision aids that facilitate elements of shared decision making in chronic illnesses: a systematic review. Syst Rev. 2019;8:121. A systematic review of shared decision-making aids, principles overlap with tailoring.
Lorig KR, Holman H. Self-management education: history, definition, outcomes, and mechanisms. Ann Behav Med. 2003;26:1–7.
Hoffmann T, Bennett S, Del Mar CB (2017) Evidence-based practice across the health professions: Elsevier. https://www.elsevierhealth.com.au/evidence-based-practice-across-the-health-professions-9780729542555.ht. Accessed Jan 2022.
Bossen D, Veenhof C, Dekker J, de Bakker D. The usability and preliminary effectiveness of a web-based physical activity intervention in patients with knee and/or hip osteoarthritis. BMC Med Inf Decis Mak. 2013;13:1–16.
Williams QI, Gunn AH, Beaulieu JE, Benas BC, Buley B, Callahan LF, Cantrell J, Genova AP, Golightly YM, Goode AP, Gridley CI, Gross MT, Heiderscheit BC, Hill CH, Huffman KM, Kline A, Schwartz TA, Allen KD. Physical therapy vs. internet-based exercise training (PATH-IN) for patients with knee osteoarthritis: study protocol of a randomized controlled trial. BMC Musculoskel Dis. 2015;16:264.
Chang RW, Semanik PA, Lee J, Feinglass J, Ehrlich-Jones L, Dunlop DD. Improving physical activity in arthritis clinical trial (IMPAACT): study design, rationale, recruitment, and baseline data. Contemp Clin Trials. 2014;39:224–35.
Ehrlich-Jones L, Mallinson T, Fischer H, Bateman J, Semanik PA, Spring B, Ruderman E, Chang RW. Increasing physical activity in patients with arthritis: a tailored health promotion program. Chronic Illn. 2010;6:272–81.
Hinman RS, Lawford BJ, Campbell PK, Briggs AM, Gale J, Bills C, French SD, Kasza J, Forbes A, Harris A, Bunker SJ, Delany CM, Bennell KL. Telephone-delivered exercise advice and behavior change support by physical therapists for people with knee osteoarthritis: protocol for the telecare randomized controlled trial. Phys Ther. 2017;97:524–36.
Skou ST, Odgaard A, Rasmussen JO, Roos EM. Group education and exercise is feasible in knee and hip osteoarthritis. Dan Med J. 2012;59:A4554.
Skou ST, Simonsen ME, Odgaard A, Roos EM. Predictors of long-term effect from education and exercise in patients with knee and hip pain. Dan Med J. 2014;61:A4867.
Bennell KL, Egerton T, Bills C, Gale J, Kolt GS, Bunker SJ, Hunter DJ, Brand CA, Forbes A, Harris A, Hinman RS. Addition of telephone coaching to a physiotherapist-delivered physical activity program in people with knee osteoarthritis-a randomised controlled trial protocol. BMC Musculoskelet Disord. 2012;13:246.
Witjes S, Hoorntje A, Kuijer PP, Koenraadt KL, Blankevoort L, Kerkhoffs GM, van Geenen RC. Does Goal Attainment Scaling improve satisfaction regarding performance of activities of younger knee arthroplasty patients? Study protocol of the randomized controlled ACTION trial. BMC Musculoskelet Disord. 2016;17:113.
Witjes S, Hoorntje A, Kuijer PP, Koenraadt KL, Blankevoort L, Kerkhoffs GM, van Geenen RC. Goal setting and achievement in individualized rehabilitation of younger total and unicondylar knee arthroplasty patients: a cohort study. Arch Phys Med Rehabil. 2018;100:1434–41.
Veenhof C, Dekker J, Bijlsma JW, van den Ende CH. Influence of various recruitment strategies on the study population and outcome of a randomized controlled trial involving patients with osteoarthritis of the hip or knee. Arthritis Rheum. 2005;53:375–82.
Pisters MF, Veenhof C, Schellevis FG, Twisk JW, Dekker J, De Bakker DH. Exercise adherence improving long-term patient outcome in patients with osteoarthritis of the hip and/or knee. Arthritis Care Res. 2010;62:1087–94.
Pisters MF, Veenhof C, Schellevis FG, De Bakker DH, Dekker J. Long-term effectiveness of exercise therapy in patients with osteoarthritis of the hip or knee: a randomized controlled trial comparing two different physical therapy interventions. Osteoarthr Cartil. 2010;18:1019–26.
Hughes SL, Seymour RB, Campbell RT, Huber G, Pollak N, Sharma L, Desai P. Long-term impact of Fit and Strong! on older adults with osteoarthritis. Gerontologist. 2006;46:801–14.
Hughes SL, Seymour RB, Campbell PK, Desai PM, Huber G, Chang RW. Fit and Strong!-bolstering maintenance of physical activity among older adults with lower-extremity osteoarthritis. Am J Health Behav. 2010;34:750–63.
Desai PM, Hughes SL, Peters KE, Mermelstein RJ. Impact of telephone reinforcement and negotiated contracts on behavioral predictors of exercise maintenance in older adults with osteoarthritis. Am J Health Behav. 2014;38:465–77.
Murphy SL, Lyden AK, Smith DM, Dong Q, Koliba JF. Effects of a tailored activity pacing intervention on pain and fatigue for adults with osteoarthritis. Am J Occup Ther. 2010;64:869–76.
Murphy SL, Lyden AK, Clary M, Geisser ME, Yung RL, Clauw DJ, Williams DA. Activity pacing for osteoarthritis symptom management-study design and methodology of a randomized trial testing a tailored clinical approach using accelerometers for veterans and non-veterans. BMC Musculoskelet Disord. 2011;12:177.
Murphy SL, Smith DM, Lyden AK. Type of activity pacing instruction affects physical activity variability in adults with symptomatic knee or hip osteoarthritis. J Phys Act Health. 2012;9:360–6.
Schepens SL, Braun ME, Murphy SL. Effect of tailored activity pacing on self-perceived joint stiffness in adults with knee or hip osteoarthritis. Am J Occup Ther. 2012;66:363–7.
Clayton C, Feehan L, Goldsmith CH, Miller WC, Grewal N, Ye J, Yoo JY, Li LC. Feasibility and preliminary efficacy of a physical activity counseling intervention using Fitbit in people with knee osteoarthritis: the TRACK-OA study protocol. Pilot and Feasibility Stud. 2015;1:30.
Foster NE, Healey EL, Holden MA, Nicholls E, Whitehurst DG, Jowett S, Jinks C, Roddy E, Hay EM. A multicentre, pragmatic, parallel group, RCT to compare the clinical and cost-effectiveness of three physiotherapy-led exercise interventions for knee osteoarthritis in older adults-the BEEP trial protocol (ISRCTN: 93634563). BMC Musculoskelet Disord. 2014;15:254.
Esbensen BA, Thomsen T, Hetland ML, Beyer N, Midtgaard J, Loppenthin K, Jennum P, Ostergaard M, Sorensen J, Christensen R, Aadahl M. The efficacy of motivational counseling and SMS-reminders on daily sitting time in patients with rheumatoid arthritis: protocol for a randomized controlled trial. Trials. 2015;16:23.
Thomsen T, Aadahl M, Beyer N, Hetland ML, Loppenthin K, Midtgaard J, Christensen R, Esbensen BA. Motivational counselling and SMS-reminders for reduction of daily sitting time in patients with rheumatoid arthritis: a descriptive randomised controlled feasibility study. BMC Musculoskelet Disord. 2016;17:434.
• Thomsen T, Aadahl M, Beyer N, Hetland ML, Loppenthin KB, Midtgaard J, Christensen R, Nielsen SM, Ostergaard M, Jennum P, Esbensen BA. Sustained long-term efficacy of motivational counseling and text message reminders on daily sitting time in patients with rheumatoid arthritis: long-term follow-up of a randomized, parallel-group trial. Arthritis Care Res. 2019;72:1560–70. A large, observer-blinded trial that demonstrates the effects of tailored motivational counseling and prompts on long-term sedentary behavior among people with rheumatoid arthritis.
Rouse PC, Veldhuijzen Van Zanten JJ, Metsios GS, Ntoumanis N, Yu CA, Koutedakis Y, Fenton SA, Coast J, Mistry H, Kitas GD, Duda JL. Fostering autonomous motivation, physical activity and cardiorespiratory fitness in rheumatoid arthritis: protocol and rationale for a randomised control trial. BMC Musculoskelet Disord. 2014;15:445.
Sjoquist ES, Almqvist L, Asenlof P, Lampa J, Opava CH. Physical-activity coaching and health status in rheumatoid arthritis: a person-oriented approach. Disabil Rehabil. 2010;32:816–25.
Sjoquist ES, Brodin N, Lampa J, Jensen I, Opava CH, group Ps. Physical activity coaching of patients with rheumatoid arthritis in everyday practice: a long-term follow-up. Musculoskelet Care. 2011;9:75–85.
Nordgren B, Friden C, Demmelmaier I, Bergstrom G, Opava CH. Long-term health-enhancing physical activity in rheumatoid arthritis - the PARA 2010 study. BMC Public Health. 2012;12:397.
Habers GE, van Brussel M, Langbroek-Amersfoort AC, van Royen-Kerkhof A, Takken T. Design of the muscles in motion study: a randomized controlled trial to evaluate the efficacy and feasibility of an individually tailored home-based exercise training for children and adolescents with juvenile dermatomyositis. BMC Musculoskelet Disord. 2012;13:108.
van den Berg MH, Ronday HK, Peeters AJ, Voogt-van der Harst EM, Munneke M, Breedveld FC, Vliet Vlieland TPM. Engagement and satisfaction with an Internet-based physical activity intervention in patients with rheumatoid arthritis. Rheumatology. 2007;46:545–52.
Hurkmans EJ, van den Berg MH, Ronday KH, Peeters AJ, le Cessie S, Vlieland TP. Maintenance of physical activity after Internet-based physical activity interventions in patients with rheumatoid arthritis. Rheumatology. 2010;49:167–72.
Heine PJ, Williams MA, Williamson E, Bridle C, Adams J, O’Brien A, Evans D, Lamb SE, Team S. Development and delivery of an exercise intervention for rheumatoid arthritis: strengthening and stretching for rheumatoid arthritis of the hand (SARAH) trial. Physiotherapy. 2012;98:121–30.
SARAH Trial Team, Adams J, Bridle C, Dosanjh S, Heine PJ, Lamb SE, Lord J, McConkey C, Nichols V, Toye F, Underwood M, Williams DA, Williamson E. Strengthening and stretching for rheumatoid arthritis of the hand (SARAH): design of a randomised controlled trial of a hand and upper limb exercise intervention – ISRCTN 89936343. BMC Musculoskelet Disord. 2012;13:230.
Williams MA, Williamson EM, Heine PJ, Nichols V, Glover MJ, Dritsaki M, Adams J, Dosanjh S, Underwood M, Rahman A, McConkey C, Lord J, Lamb SE. Strengthening And stretching for Rheumatoid Arthritis of the Hand (SARAH). A randomised controlled trial and economic evaluation. Health Technol Assess. 2015;19:1–222.
Li LC, Feehan LM, Shaw C, Xie H, Sayre EC, Aviña-Zubeita A, Grewal N, Townsend AF, Gromala D, Noonan G, Backman CL. A technology-enabled Counselling program versus a delayed treatment control to support physical activity participation in people with inflammatory arthritis: study protocol for the OPAM-IA randomized controlled trial. BMC Rheumatol. 2017;1:6–6.
Ang DC, Kaleth AS, Bigatti S, Mazzuca S, Saha C, Hilligoss J, Lengerich M, Bandy R. Research to Encourage Exercise for Fibromyalgia (REEF): use of motivational interviewing design and method. Contemp Clin Trials. 2011;32:59–68.
Kaleth AS, Saha CK, Jensen MP, Slaven JE, Ang DC. Effect of moderate to vigorous physical activity on long-term clinical outcomes and pain severity in fibromyalgia. Arthritis Care Res. 2013;65:1211–8.
Dobkin PL, Da Costa D, Abrahamowicz M, Dritsa M, Du Bergur R, Fitzcharles MA, Lowensteyn I. Adherence during an individualized home based 12-week exercise program in women with fibromyalgia. J Rheumatol. 2006;33:333–41.
Acknowledgements
We thank Charlotte Beck for helping design the search methodology.
Funding
JM was supported by a Michael Smith Foundation for Health Research Trainee Award (#17936), the Arthritis Society Post-Doctoral Fellowship (TPF-18–0209), and the Canadian Institute of Health Research Post-Doctoral Fellowship (201910MFE-430114–231890). LCL is supported by the Harold Robinson/Arthritis Society Chair in Arthritic Diseases award, the Canada Research Chair Program, and the Michael Smith Foundation for Health Research. Funding bodies did not play a role in the study collection, analysis, interpretation of the data, or writing of the manuscript. Funder websites: https://cihr-irsc.gc.ca/e/193.html; https://www.msfhr.org; https://arthritis.ca.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Jasmin K. Ma declares that she has no conflict of interest. Smruthi Ramachandran declares that she has no conflict of interest. Amrit Sandhu declares that she has no conflict of interest. Karen Tsui declares that she has no conflict of interest. Alison M. Hoens declares that she has no conflict of interest. Davin Hu declares that he has no conflict of interest. Linda C. Li declares that she has no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Osteoarthritis
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ma, J.K., Ramachandran, S., Sandhu, A. et al. Tailored Interventions for Supporting Physical Activity Participation in People with Arthritis and Related Conditions: a Systematic Review. Curr Treat Options in Rheum 8, 117–142 (2022). https://doi.org/10.1007/s40674-022-00194-5
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40674-022-00194-5