
Abstract
Fostering skills in research is important for medical schools. This scoping review examined undergraduate curricular structures devoted to research training and their outcomes. For the sixty papers meeting inclusion criteria, descriptive statistics and a thematic analysis were conducted. Forty (67%) articles described US programs, with 30 (50%) being mandatory. Timing of research training was variable across included studies with the majority (58%) describing embedded longitudinal curricula. Reported benefits included enhanced knowledge, improved research and writing skills, clarity around career plans, and mentoring relationships. There are many curricular structures for undergraduate research training, but no high-quality evidence to support particular designs.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Physician-scientists are trained to focus on health research and clinical care delivery. Their translational perspective helps bring research findings into the clinic and develop key research questions nested in clinical experience [1, 2]. As far back as 1999, there have been concerns raised about declining numbers of physician-scientists and a series of recommendations proposed to reverse this trend [3]. Medical school training is frequently recommended as part of the solution: “medical schools (should) create an environment that attracts, fosters, and rewards students committed to research” [3]. In 2010, the Future of Medical Education in Canada (FMEC) published its report for undergraduate medicine with 10 key recommendations, including: “…research interests and skills must be developed to foster a new generation of health researchers.” One strategy endorsed in this document was to “Support existing and new programs that integrate research training with medical education” [4]. In 2016, the Association of Faculties of Medicine of Canada (AFMC) was even more explicit in their recommendations for training future physician-scientists, recommending (a) integrated MD-PhD and MD-MPH professional training programs be established or restored, (b) the creation of a national training strategy for physician-scientists, and (c) encouragement and support for graduate students committed to a career in research [5].
These recommendations prompt an important question: Should research training be restricted to students with self-declared research interest prior to starting medical school? Many of the AFMC’s practical recommendations are focused on identifying a small number of students with pre-existing research interest [4].This assumes that students without this interest prior to medical training will not develop it at a later stage and that research training is unnecessary for students who do not have an explicit research career goal. Participation in research projects during medical school is associated with increased interest in future research involvement, suggesting that exposure to research can stimulate interest and alter career goals and questioning of these assumptions [6]. Examining training structures in undergraduate medical education and their reported outcomes is the first step in understanding how best to foster interest and competence in clinical research, an essential step in the process of choosing a research-focused career goal.
It is unclear what an optimal undergraduate research curriculum looks like. Effective teaching of research skills is resource-intensive, and it is a challenge to create student research experiences with the limited time of research-focused faculty members. There are increased demands for medical schools to teach their students more clinical topics with higher complexity, so the delivery of optimally designed research training will require challenging decisions from medical educators. What should be dropped to fit it in? What amount of exposure to research training achieves adequate skills to prepare students for residency? Is the preferred outcome an increased number of physician-scientists or enhanced student satisfaction and research-related skills? Which strategy yields the highest number of graduates with research careers: a large amount of research training focused on a minority of students, a small amount of training for all, or both? Given these broad questions, we conducted a scoping review to examine the current landscape and identify existing curricular structures for research training within undergraduate medicine and to evaluate best practices for training undergraduate medical students in clinical research.
Methods
The review was performed using PRISMA scoping review guidelines [7]. With the support of a health sciences librarian, a search strategy was developed to identify papers describing undergraduate medical educational curricula focused on teaching research skills. Medline and Embase databases were searched between 1996 and 2019 using keywords such as “Research,” “Research/Ed,” “Medical Education,” “Curriculum.” The review was restricted to English-language articles. Reference lists of included papers were reviewed to identify additional citations. Titles and abstracts were screened, and potentially relevant articles were reviewed in duplicate (JP and HM) for eligibility.
To be eligible for inclusion, articles had to contain a description of the curriculum and identify undergraduate medical students as the target learners. Articles that examined postgraduate research education were excluded. Data abstraction from the included papers was performed in duplicate and discrepancies were resolved through consensus (JP and HM). Quantitative data was obtained where possible, and an emergent thematic analysis was undertaken on available qualitative data.
Results
Characteristics of Included Studies
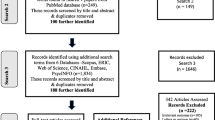
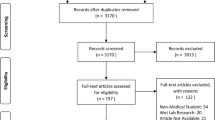
A flow chart of included studies is presented in Fig. 1. There were 169 studies identified through the literature search, and a further 38 studies identified through hand search. After removal of duplications, 112 full-texts were assessed for eligibility, and articles were excluded for reasons such as not including an undergraduate training program and a lack of description of the research curriculum. Ultimately, 60 studies were included in this review. All studies were descriptive in nature with some describing programs at a variety of medical schools around the world. There were no identified studies with analytic components or with comparator arms. An overview of the findings of the review is presented in Table 1.

PRISMA diagram
Thematic Analysis
Relevant information was extracted from the included articles under the emergent themes of structure and timing of curriculum delivery, mentorship, academic productivity, assessment methods, and program evaluation.
Theme 1: Curriculum Structures for Research Training Are Variable
Curriculum Design
There was a high degree of variability in the structure and location of curricular time devoted to research. Thirty-five institutions (58.3%) had an embedded research program throughout medical school, and eight institutions (13.3%) had a dedicated year for research [8,9,10,11,12,13,14,15]. Six institutions (10%) offered a research program in the preclinical years, four (6.7%) during the clinical years, and four (6.7%) during the summer only. Finally, only 1 institution (1.7%) offered a pre-graduation program, and program timing was unclear in 2 (3.3%) papers (Table 1). Many reports described programs where research training was delivered longitudinally, in parallel with other courses [8, 16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43]. Some programs offered varying amounts of protected time in which students could perform research and meet with mentors [12, 42]. Other programs included devoted blocks in which students had no other course obligations [9,10,11, 26, 44,45,46,47,48,49,50]. In contrast, some programs offered little to no scheduled curricular time. In these programs, students were expected to complete the components of their scholarly requirement on weekends, holidays, or during summer vacation [35, 51, 52]. The choice of enrollment in research training also varied among reports, with 30 (50%) programs being mandatory and 15 (25%) optional. Six (10%) were mandatory with an optional extension, and nine (14.8%) were by application only with limited enrollment.
Many programs reported a mixed approach, with some component of scheduled group learning followed by a longitudinal component in which students executed their research project outside of classroom time [17, 35, 37, 40]. One program design featured multiple focused blocks in which students could immerse themselves in their research without splitting attention between coursework, clinical obligations, and research [10, 26]. Another approach was to allow flexible scheduling of the research requirement [52]. Of the 8 schools providing students with a full year devoted to research, Duke University structures their medical school with a single pre-clinical year, a year of clerkship, a year of dedicated clinical research, and then another year of clinical electives [8, 9, 11]. Other programs accommodated an additional research year by extending medical school from 4 to 5 years [12, 26].
Program Duration
The total amount of time devoted to research teaching and execution was variable and frequently not reported in the literature, perhaps due to the flexibility in the courses with self-directed learning components. Of those reporting specific hour requirements, the expectation for a longitudinal research project was generally 4 + hours per week or minimum 120–160 h devoted to the project [8, 16, 40]. Full-time courses typically expected students to work on their research at least 35 h per week. Some courses were short in duration, with less than 1 month of devoted curriculum time. Shortened courses had modified expectations, with students participating in group research for a faculty-generated question and performing pre-designed lab exercises rather than developing and pursuing original ideas [43, 53, 54]. The more lengthy full-time courses (up to 12 months) typically required students to design and conduct their own research project [9, 11].
Timing of Training
Though there was some variability in the stage of training at which the scholarly components were initiated, most courses were introduced in the pre-clinical years with research components completed in either the second preclinical year, the summer thereafter or extending into early clinical training time [14, 17, 25, 40, 41]. However, some courses were initiated as late as the final year of medical school [27, 42, 45].One novel approach grouped students based on interest to undertake a shared research project over the course of 4 weeks in the final year of medical school [54].
The use of the summer months to pursue research projects was identified as a good time for students since they were not overburdened with simultaneous academic or clinical demands [51]. However, mandated use of holiday periods imposes a financial burden on students who would have otherwise sought employment. Some programs have provided guaranteed funding to students to offset this, increasing the cost of the program [35]. Some schools have a baseline research competency requirement that all students must meet prior to graduation, with additional streams for students wishing a higher degree of training and research competency [19, 27]. Some programs also allow students to expand their research and earn an MSc or PhD [11, 41].
Theme 2: Faculty Mentorship Influences Student Experience and Career Direction
Mentoring Structures
Faculty supervision and mentoring (defined as guidance from an experienced researcher) was commonly reported in descriptions of research training programs. Fifty-one (85%) papers indicated some form of mentorship, three (5%) reported none, and six (10%) were unclear (Table 1). Programs incorporated faculty mentorship through individualized (39%) or small groups of < 15 students (8%). At least one program used multiple mentors, where both faculty and peer mentors facilitated small groups and provided individual student guidance [22]. In some centers, faculty were chosen for their commitment to mentorship, research productivity, and access to resources to ensure student success—a strategy that may have contributed to high student-reported satisfaction [8, 44]. At Stanford University’s Medical School, a curricular change in 2003 added an in-depth structured mentorship experience which incorporated “near-peer” mentors (students who have recently completed the research program) to advise incoming students about pros and cons of various scholarly concentrations [8].
Benefits of Mentoring
Surveys of graduates indicated that having a research mentor was valuable to their learning and increased their enthusiasm for research and desire to continue a career in academic medicine [8, 44]. Following the implementation of a curricular research program with a focus on faculty mentors at Vanderbilt University, the proportion of graduating students reporting high value from their research experience at graduation increased from 45.3% in 2000 to 94.5% in 2009 [35].The same graduates placed a higher value than the national average on the importance of faculty mentoring in the AAMC exit survey (84.3% vs. 70.4%) [35]. Many students continued to work with their mentor even after the completion of their research program, confirming the potential for these relationships to develop into lengthy collaborations [44, 55]. The level of dedication from a mentor (measured by frequent interaction with mentee and productivity) was correlated with the mentee’s increased scholarly success, facilitated their career selection, and developed the mentee’s confidence in their work [55]. Finally, a neurology-focused undergraduate mentorship program built around the values of accessibility, support, skill set-orientation, and feedback cycles saw a large increase in the number of students entering neurology residencies at the Boston University School of Medicine from the 2011–2014 period compared to the 2006–2010 period [32].
Challenges of Mentoring
There are challenges in creating mentorship opportunities for students: offering faculty mentoring within an educational program is resource and time-intensive, especially when faculty must balance clinical, research, and teaching obligations. Individual assessments by 1-on-1 mentors can lead to inconsistencies in student assessment [8]. Not all mentoring relationships work well, and problems have been well documented such as poor communication, a lack of commitment to the relationship from either party, and a mentor that is inexperienced [56, 57]. Successful mentoring requires willing faculty with institutional commitment for support, faculty development, and incentive structures [56].
Theme 3: Program Length Is Associated with Increased Student Academic Output
Academic productivity increased with the duration of time devoted to research. In one paper, a longer 21-week experience compared to shorter 17- and 13-week experiences was associated with a higher number of first-author publications (203/584,35% vs 80/329,24% vs 21/68,31%, p < 0.005); however, the magnitude of difference was small and the point of diminishing returns unclear [47]. Additionally, these observations suffer from selection bias, where students interested in research seek out training programs with research as a major focus. The time commitment to take research activities to publication is not trivial, and these schools use research intent and motivation as part of their selection criteria [40].
At Duke’s year-long research curriculum, about two-thirds of students in the program published at least one peer-reviewed paper [9].Ticknor et al. reported that 23% of students who participated in their 5-year longitudinal research track received competitive awards to support their medical school research and 87% produced peer-reviewed products from their research [26]. Students enrolled in prolonged research-intensive programs were more likely to receive research awards and attend conferences than students from previous years without this focus [26, 34].
Although the quality of the published research is poor (descriptive studies) and fraught with selection bias, there is a consistent association with length of time and academic productivity for students in dedicated research training programs.
Theme 4: Student Assessment Was Primarily Through Assignments or Presentations
A majority 51/60 (85%) of research training programs assessed students through written assignments, oral or poster presentations, manuscripts, or some combination. Nine programs (15%) were unclear regarding their assessment methods. Nineteen programs (31.7%) specifically required a written assignment. The requirements for written assignments varied between programs and often depended on the length of their respective research curriculum. For programs taking place over a shorter amount of time such as the summer, preparation of an abstract was sufficient for milestone completion [44]. For longer programs, including ones that had an ongoing embedded thread or a dedicated research year, a complete literature review or manuscript was required [47, 48]. Eight (13.3%) programs were assessed only through a presentation, either in the format of a poster or oral presentation. Finally, 24 (40%) programs employed more than one method of assessment.
The integration of mandatory assignments into research training programs provided students with practical advantages. Students were often able to turn their required coursework into a publication or presentation at a conference [10, 44]. Completion of assignments allows students to receive feedback on the research design, methods, and critical appraisal skills they develop throughout the program, increasing their competence in these tasks. Some programs address the challenge of limited time and faculty for student assessment through the implementation of research days, where many students come together to present their research to faculty in poster or oral presentation format [9, 40, 42].
Theme 5: Program Evaluation Data Are Scarce and of Poor Quality
Research training programs were variably evaluated. No papers described a formal program evaluation process. Seventeen (28.3%) articles described programs that were evaluated using some form of student feedback [8, 10, 12,13,14, 18, 22, 34, 35, 38, 40, 43,44,45, 49, 54, 58]. Most programs collected student feedback through regular course evaluation activity, while four programs used specifically designed student questionnaires [35, 44, 54, 58]. The results capture various aspects of student experiences in their research training programs, including self-reported improvement in research skills, perceived value of research training, interest in continuing to pursue research in their clinical career, and overall satisfaction with experience [12, 34, 49]. Though students reported overall high levels of satisfaction with embedded research training, some felt that it was difficult to balance research along with their other demanding coursework [34, 55]. Exposure to a research elective increased students’ self-reported interest in a research-focused career [49]. Eighteen (30%) programs evaluated their research program by collecting data on academic productivity [8, 10, 14,15,16, 25, 26, 28, 30, 32, 39, 47, 48, 50, 55, 59,60,61]. Most programs measured “productivity” by looking at academic output in the form of peer-reviewed publications, abstracts, and presentations; however, this was variable and frequently self-reported by students. One (1.7%) program incorporated only faculty-level feedback into their evaluation [36]. Finally, 15 (25%) programs did not mention any method of evaluating their research program or were unclear regarding the method(s) used [9, 17, 21, 23, 27, 29, 37, 42, 46, 51, 53, 62].
Overall, students report high satisfaction with their programs and increased knowledge of what a career in research entails [8, 44]. In addition, students felt that participating in a formal research curriculum improved their knowledge of research design and critical appraisal [22, 49]. Conducting research allowed students to become more engaged in specific clinical disciplines, ultimately improving their knowledge in the field and giving them greater confidence in career decisions [8, 24, 44, 49].
Faculty supervision forms an integral part of research training programs; however, faculty feedback data on these programs is scarce. One survey indicated that a majority of supervisors found medical students to be a valuable resource to their research team and were willing to continue supervising students [12].
Discussion
There are numerous perceived benefits of research training programs during undergraduate medicine. The most common reported benefit was enhanced academic productivity during medical school [11, 14, 25, 34, 41, 47].This was seen across research training programs with variable duration and intensity: longitudinal programs supported the completion of manuscripts by trainees, while shorter summer programs succeeded in supporting students to complete research abstracts or poster presentations [19]. Increased academic productivity also contributed to the research portfolio of students’ curriculum vitae (CV), which can inform selection criteria for residency programs and may improve residency match results [16]. While assessing academic productivity (if clearly defined) may be an objective method of evaluating research training programs, this outcome does not capture other benefits of research training such as improved critical appraisal skills and the integration of evidence into clinical practice.
Research training is recognized as important for students who do not intend to pursue research after medical school. This review of the literature revealed many benefits of mandatory research training programs that extend beyond research skills and productivity. Students felt they had an enhanced understanding of clinical specialties through participation in research, which assisted them with their career decisions [9, 49]. Conducting research in a particular field necessitates a deeper understanding of relevant clinical and basic science concepts [18, 54]. Medical students appear to benefit from some rudimentary research training, regardless of future career plans. Basic research training programs should be offered routinely to all medical students.
There are no data available to support the adoption of any particular research training structure. In general, students expressed greater interest in pursuing research or an academic career immediately following the completion of a research training program [8, 21, 24, 26, 35, 44, 49]. The intensity and duration of programs seem to play a role in shaping students’ future interest in research. For example, 80% of students who participated in a 2-year research program had ambitions to pursue a PhD [12]. However, selection bias is a concern since students who enroll in an optional research program that prolongs their education are likely to be more interested in a career path that involves research. The only article in this review that looked at downstream career outcomes came from Duke University, which reported that 15–20% of graduates in the year-long scholarly experience went on to pursue academic careers [11]. Long-term data from other programs are needed to know whether research training programs outside of MD/PhD or MD/MPH programs are associated with careers in academic medicine or as a clinician-scientist.
The ideal timing and duration of a medical school research course is unclear, and there are a variety of different approaches. Introduction of the didactic components of the research process is well-suited to the first year of medical school, providing students with the foundational knowledge necessary to begin the critical enquiry process. However, initiating the development of a research question too early may tie a student to a project poorly aligned with their academic or clinical interests, which may not emerge until later in their training [35]. The optimal design will also depend on whether students are expected to undergo the lengthy process of planning a research question and performing data collection. An interesting solution is to devote curricular time for students to investigate a focused area and plan a research question, with an option to carry the research forward. This allows motivated students to continue research, while other students use their time for other ventures, though at the expense of missing the learning opportunities associated with data collection and analysis [39]. The optimal training program duration remains unclear [47, 54]. Program length should be sufficient to produce scholarly output and allow effective mentorship, however, not so long and time-intensive that students lose interest or are unable to complete the program requirements [8].
Effective faculty mentors enhance student learning, increase interest in research as a career and scholarly output during medical school and under ideal circumstances, and form lasting relationships with their mentees that continue after medical school graduation. However, the faculty time commitment required is substantial, and not all mentors are beneficial to the student experience. An optimal medical school curriculum would include incentives for faculty mentoring of a small number of selected students, offered within a structured environment that provides institutional support for faculty development [26, 63].
Perceived challenges identified across research training programs include both the financial and faculty resources required to ensure the creation and sustainability of a beneficial program [8, 12, 35, 38, 46, 51]. Other challenges identified were a lack of time for students to complete research endeavors to the level expected by faculty mentors, as well as student interest in the project [22, 34]. Finally, while good mentorship is beneficial, having enough faculty participation is key to a successful program in order to not over-burden individual mentors [16, 23, 25, 38, 52, 62].
Conclusion
This scoping review has shown that academic productivity is associated with increasing program length, that students found benefits from research programs in addition to increased academic productivity, and that faculty mentorship is a key component to successful research training with benefits that transcend research productivity. Challenges with incorporating a research program in medical school include time and resource demands, and the difficulty students experience when balancing research with coursework. Further research should evaluate the long-term impact of incorporating a research program in undergraduate medical programs, including success in developing future academic clinicians and clinician-scientists. This could be in the form of clearly defined student research outputs, the number of graduating physicians creating or contributing to research, and the outcomes from sustained incorporation of mentorship in research education.
References
Lander B, Hanley GE, Atkinson-Grosjean J. Clinician-scientists in Canada: barriers to career entry and progress. PLoS One. 2010;5(10).
Yin C, Steadman PE, Apramian T, Zhou TE, Ishaque A, Wang X, et al. Training the next generation of Canadian clinician-scientists: charting a path to success. Clin Invest Med. 2017;40(2):E95-e101.
Rosenberg L. Physician-scientists–endangered and essential. Science. 1999;283(5400):331–2.
AFMC. The future of medical education in Canada (FMEC): a collective vision for MD education. 2010. https://www.afmc.ca/wp-content/uploads/2022/10/2010-FMEC-MD_EN.pdf. Accessed 8 Nov 2022.
AFMC. A re-envisioning of health research in Canada- AFMC position paper on research. 2016. https://www.afmc.ca/wpcontent/uploads/2022/10/AFMC_Research_Position_Paper_EN.pdf. Accessed 8 Nov 2022
Amgad M, Man Kin Tsui M, Liptrott SJ, Shash E. Medical student research: an integrated mixed-methods systematic review and meta-analysis. PloS One. 2015;10(6):e0127470–e.
PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Annals of Internal Medicine. 2018;169(7):467–73.
Laskowitz DT, Drucker RP, Parsonnet J, Cross PC, Gesundheit N. Engaging students in dedicated research and scholarship during medical school: the long-term experiences at Duke and Stanford. Acad Med. 2010;85(3):419–28.
O’Connor Grochowski C, Halperin EC, Buckley EG. A curricular model for the training of physician scientists: the evolution of the Duke University School of Medicine curriculum. Acad Med. 2007;82(4):375–82.
Hunt JE, Scicluna H, McNeil HP. Development and evaluation of a mandatory research experience in a medical education program: the independent learning project at UNSW. Med Sci Educ. 2011;21(1):78–85.
Cook S, Grochowski COC, Atherton A, Laskowitz DT, Pervaiz S, Buckley EG, et al. Developing physician leaders for over 50 years: the Duke medical student research experience in the US and Singapore. Med Sci Educ. 2011;21:53–8.
Hunskaar S, Breivik J, Siebke M, Tømmerås K, Figenschau K, Hansen J-B. Evaluation of the medical student research programme in Norwegian medical schools. A survey of students and supervisors. BMC Med Educ. 2009;9(1):43.
De Silva DA, Allen JC, Krishnaswamy G, Vogel S, Cook S. Patient oriented research: the Duke-NUS medical student experience. Med Sci Ed. 2013;23:141–7.
Dekker F, Halbesma N, Zeestraten E, Vogelpoel E, Blees M, de Jong P. Scientific training in the Leiden medical school preclinical curriculum to prepare students for their research projects. Med Sci Educ. 2009;19(2S).
Blazer D, Bradford W, Reilly C. Duke’s 3rd year: a 35-year retrospective. Teach Learn Med. 2001;13(3):192–8.
Rhyne RL. A scholarly research requirement for medical students: the ultimate problem-based learning experience. Acad Med. 2000;75(5):523–4.
Schor NF, Troen P, Kanter SL, Levine AS. The Scholarly Project Initiative: introducing scholarship in medicine through a longitudinal, mentored curricular program. Acad Med. 2005;80(9):824–31.
Silverman H, Cohen T, Fridsma D. The evolution of a novel biomedical informatics curriculum for medical students. Acad Med. 2012;87(1):84–90.
Velden J, Verbeek A, Morava E, Ruijs A, Draaisma J. Integration of three different medical research projects for medical students in a Department of Pediatrics. Med Sci Educ. 2013;23:648–55.
Mitchell KD, Krane NK. Training medical students in research: the DeBakey scholars program at Tulane University School of Medicine. Med Sci Educ. 2013;23(3):385–90.
LaConte L, Johnson TA, Vari RC, Friedlander MJ. Research immersion at the virginia tech carilion school of medicine — an integrated curriculum producing scientist physicians for the future of healthcare. Med Sci Educ. 2013;23(1):122–34.
Brousseau DCH, David R. Integration of the medical college of wisconsin physician scientist pathway and summer research programs to increase medical student research skills. Med Sci Educ. 2013;23(1S):84–7.
Jacobson C, Hunter C, Wessels Q. Biomedical research at Namibia’s first school of medicine and pharmacy. Med Sci Educ. 2014;23:135–40.
Colmenares C, Bierer SB, Graham L. Impact of a 5-year research-oriented medical school curriculum on medical student research interest, scholarly output, and career intentions. Med Sci Educ. 2013;23:88–91.
Bahner I, Somboonwit C, Pross S, Collins R, Saporta S. Teaching science through biomedical research in an elective curriculum. Med Sci Educ. 2014;22:143–6.
Ticknor C, Bierer SB, Colmenares C, Hull AL. A comprehensive research curriculum to prepare physician-investigators: design, implementation and early outcomes. Med Sci Educ. 2011;21:67–77.
Aronson JF, Valbuena GA, Hellmich MR, Asimakis GK. Translational research track for medical students: developing interprofessional collaborative competencies for translational research. Med Sci Educ. 2011;21(1):63–6.
Boninger M, Troen P, Green E, Borkan J, Lance-Jones C, Humphrey A, et al. Implementation of a longitudinal mentored scholarly project: an approach at two medical schools. Acad Med. 2010;85(3):429–37.
Green EP, Borkan JM, Pross SH, Adler SR, Nothnagle M, Parsonnet J, et al. Encouraging scholarship: medical school programs to promote student inquiry beyond the traditional medical curriculum. Acad Med. 2010;85(3):409–18.
George P, Green EP, Park YS, Gruppuso PA. A 5-year experience with an elective scholarly concentrations program. Med Educ Online. 2015;20:29278.
Mullan JR, Weston KM, Rich WC, McLennan PL. Investigating the impact of a research-based integrated curriculum on self-perceived research experiences of medical students in community placements: a pre- and post-test analysis of three student cohorts. BMC Med Educ. 2014;14(1):161.
Zuzuárregui JR, Hohler AD. Comprehensive opportunities for research and teaching experience (CORTEX): a mentorship program. Neurology. 2015;84(23):2372–6.
Wolfson RK, Alberson K, McGinty M, Schwanz K, Dickins K, Arora VM. The impact of a scholarly concentration program on student interest in career-long research: a longitudinal study. Acad Med. 2017;92(8):1196–203.
Smith FG, Harasym PH, Mandin H, Lorscheider FL. Development and evaluation of a research project program for medical students at the University of Calgary Faculty of Medicine. Acad Med. 2001;76(2):189–94.
Gotterer GS, O’Day D, Miller BM. The emphasis program: a scholarly concentrations program at Vanderbilt University School of Medicine. Acad Med. 2010;85(11):1717–24.
MacDougall M, Riley SC. Initiating undergraduate medical students into communities of research practise: what do supervisors recommend? BMC Med Educ. 2010;10(1):83.
Strom BL, Kelly TO, Landis JR, Feldman HI. The center for clinical epidemiology and biostatistics of the Perelman School of Medicine at the University of Pennsylvania: an organizational model for clinical research in a school of medicine. Acad Med. 2012;87(1):60–5.
Ghias K, Siddiqui R, Ahmed R. Research as a pedagogical approach in undergraduate medical education: an experience. Med Sci Educ. 2014;23:119–21.
Duggan E, Doran K, O’Flynn S, O’Tuathaigh CMP. Providing research opportunities for medical students: challenges and opportunities. Med Sci Educ. 2013;23(1):99–107.
Obrador GT. Development of the research competency in the curriculum of a Mexican Medical School. Med Sci Educ. 2013;23(1):154–8.
van Eyk HJ, Hooiveld MH, Van Leeuwen TN, Van der Wurff BL, De Craen AJ, Dekker FW. Scientific output of Dutch medical students. Med Teach. 2010;32(3):231–5.
Cichoskikelly E. Using research as a tool for reinforcing basic sciences in the clinical years: description of a fourth year teaching/research requirement at the University of Vermont College of Medicine. Med Sci Educ. 2014;21:59–62.
Hodsdon W, Nygaard C, Zwickey H. The sugar study: a monograph for in-class research with medical students. Med Sci Ed. 2014;23:159–64.
Jeste DV, Halpain MC, Trinidad GI, Reichstadt JL, Lebowitz BD. UCSD’s short-term research training programs for trainees at different levels of career development. Acad Psychiatry. 2007;31(2):160–7.
Zier K, Coplit LD. Introducing INSPIRE, a scholarly component in undergraduate medical education. Mt Sinai J Med. 2009;76(4):387–91.
Zier K, Stagnaro-Green A. A multifaceted program to encourage medical students’ research. Acad Med. 2001;76(7):743–7.
Dyrbye LN, Davidson LW, Cook DA. Publications and presentations resulting from required research by students at Mayo Medical School, 1976–2003. Acad Med. 2008;83(6):604–10.
Dokter C, Sergent S, Willyerd G. Public health research in a study abroad medical service. Med Sci Educ. 2013;23(1):165–9.
Houlden RL, Raja JB, Collier CP, Clark AF, Waugh JM. Medical students’ perceptions of an undergraduate research elective. Med Teach. 2004;26(7):659–61.
Peacock JG, Warner LL, Drozdowicz LB, Martin BA, Suresh R, Denzer BJ, et al. Curricular flexibility in the pre-clinical years promotes medical student scholarship. Med Sci Ed. 2013;23(1):92–8.
Rosenblatt RA, Desnick L, Corrigan C, Keerbs A. The evolution of a required research program for medical students at the University of Washington School of Medicine. Acad Med. 2006;81(10):877–81.
Pfarr CM, Bramblett D, Osborne D, Trott A, Balsiger H, Coue M, et al. A laboratory for education in molecular medicine: a dedicated resource for medical student research. Med Sci Educ. 2013;23(1):108–18.
Gruis NA, Langenhoff JM. Increasing first year student s attitude and understanding towards biomedical research. Med Sci Educ. 2013;23:148–53.
DiGiovanni BF, Ward DS, O’Donnell SM, Fong C-T, Gross RA, Grady-Weliky T, et al. Process of discovery: a fourth-year translational science course. Med Educ Online. 2011;16(1):8443.
Tamariz L, Vasquez D, Loor C, Palacio A. Successful adaptation of a research methods course in South America. Med Educ Online. 2017;22(1):1336418.
Straus SE, Johnson MO, Marquez C, Feldman MD. Characteristics of successful and failed mentoring relationships: a qualitative study across two academic health centers. Acad Med. 2013;88(1):82–9.
Sambunjak D, Straus SE, Marusic A. A systematic review of qualitative research on the meaning and characteristics of mentoring in academic medicine. J Gen Intern Med. 2010;25(1):72–8.
Knight SE, Van Wyk JM, Mahomed S. Teaching research: a programme to develop research capacity in undergraduate medical students at the University of KwaZulu-Natal, South Africa. BMC Med Educ. 2016;16:61. https://doi.org/10.1186/s12909-016-0567-7.
Burge SK, Hill JH. The medical student summer research program in family medicine. Fam Med. 2014;46(1):45–8.
Hooiveld MHW, Slothouber B, Horst GJ, Kuks J, Kluin-Nelemans H. Junior Scientific Masterclass: additional science training for medical students. Med Sci Educ. 2014;21:86–90.
Cluver J, Book S, Brady K, Back S, Thornley N. Engaging medical students in research: reaching out to the next generation of physician-scientists. Acad Psychiatry. 2014;38(3):345–9.
Willis MW, Deardorff AS. Developing a research-focused learning community at one medical school. Med Sci Educ. 2011;21:98–103.
Keyser DJ, Lakoski JM, Lara-Cinisomo S, Schultz DJ, Williams VL, Zellers DF, et al. Advancing institutional efforts to support research mentorship: a conceptual framework and self-assessment tool. Acad Med. 2008;83(3):217–25.
Acknowledgements
The authors would like to thank Drs. Alyssa Louis, Meghan Brown, Shannon Meilleur and Matthew Ernst for their contributions in the early stages of this review.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This project did not collect primary data and since it was an analysis of published work, it was deemed exempt from institutional ethics requirements. There are no reproduced items from other publications or patient/personal information requiring consent for publication. Data sharing is not applicable to this study as no primary dataset was analyzed. None of the authors have any conflict of interests. This research was unfunded. All 3 authors were responsible for the review of included articles, and the drafting and revisions to the manuscript.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Appendix
Search Strategies:
-
1.
Database: Embase < 1996 to 2013 Week 35 > Search Strategy:
-
1.
medical education/ or medical school/ or residency education/ (141449)
-
2.
exp research/ (425759)
-
3.
1 and 2 (19666)
-
4.
exp curriculum development/ or exp curriculum/ (40506)
-
5.
3 and 4 (1670)
-
6.
*medical education/ or *medical school/ or *residency education/ (63210)
-
7.
exp *research/ (114115)
-
8.
6 and 7 (1781)
-
9.
4 and 8 (265)
-
10.
limit 9 to (english language and exclude medline journals) (15)
-
1.
-
2.
Database: Ovid MEDLINE(R) without Revisions < 1996 to Present with Daily Update > Search Strategy:
-
1.
Students, Medical/ (13246)
-
2.
exp Education, Medical, Graduate/ or exp "Internship and Residency"/ (28613)
-
3.
Education, Medical, Undergraduate/ (10148)
-
4.
1 or 3 (19541)
-
5.
exp Research/ed [Education] (3676)
-
6.
4 and 5 (169)
-
7.
"Curriculum"/ (29864)
-
8.
6 and 7 (57)
-
9.
2 and 5 (396)
-
10.
7 and 9 (137)
-
11.
8 or 10 (183)
-
12.
limit 11 to english language (148)
-
1.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Murray, H., Payandeh, J. & Walker, M. Scoping Review: Research Training During Medical School. Med.Sci.Educ. 32, 1553–1561 (2022). https://doi.org/10.1007/s40670-022-01679-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40670-022-01679-7