
Abstract
This project describes application of an evidenced-based, trauma-informed treatment framework, Attachment, Regulation and Competency (ARC), with adopted children impacted by complex trauma and their caregivers. Results demonstrate that ARC treatment was associated with significant decreases in child symptoms and caregiver stress from pre- to post-treatment, which were maintained over a 12-month follow up period. Preliminary findings contribute to an emerging empirical basis for the ARC model and are supportive of its clinical utility as a practice with adopted children. Next steps include; a) expanding study findings by conducting controlled efficacy research, b) examining the transaction between child and caregiver factors as agents of change, and c) conducting longitudinal research of children and families receiving ARC to more deeply examine impact on resiliency.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Every year in the United States, upwards of three million children experience maltreatment (U.S. Department of Health and Human Services 2015). The majority of trauma-impacted children in treatment-seeking samples have experienced multiple exposures (Briggs et al. 2012a, b; Spinazzola et al. 2005), and with increasing exposure comes increasing symptom complexity (Cloitre et al. 2009), presumably resulting from developmental trajectory disruptions across social, emotional and behavioral domains (Cook et al. 2005; D’Andrea et al. 2012). These disruptions are expressed by a range of emotional and behavioral symptoms including internalizing and externalizing problems (Manly et al. 2001), poor affect regulation, disrupted attention and concentration, negative self-image, lack of impulse control and increased aggression (Spinazzola et al. 2005), resulting in categorization with a variety of co-morbid diagnosis including mood, anxiety and disruptive behavior disorders (D’Andrea et al. 2012). Although PTSD is often used as the index diagnosis for this population, research shows it to be only the 5th most common diagnosis (Ackerman et al. 1998), while significant behavioral and academic problems (Briggs et al. 2012a, b) and / or clinically significant difficulties with affect regulation, impulse control, and attention (Spinazzola et al. 2005) are observed among upwards of 50 % of this population.
Children exposed to complex trauma may experience maltreatment and neglect of sufficient magnitude to warrant child welfare system investigation and intervention resulting in removal from their family of origin. In 2013, 239,000 children entered foster care and 51,000 children were adopted (U.S. Department of Health and Human Services 2015). Children in the child welfare system have high rates of psychiatric disorders (Garland et al. 2001), including rates of externalizing behavior problems that are two to four times that observed in the general population (Armsden et al. 2000). This is of concern because child externalizing behavior problems are associated with increased caregiver stress (Morgan et al. 2002), risk for placement disruption (James 2004; Proctor et al. 2011) and child maltreatment (Rodriguez and Green 1997), factors that are likely interrelated. Moreover, externalizing behaviors do not reduce once environmental safety is established, but either remain stable or increase over time, with increases associated with use of negative parenting strategies (Vanderfaeillie et al. 2013).
Caregiver stress is a particularly notable variable, as an important factor promoting resilience among children who have experienced complex trauma is the presence of a stable and supportive caregiver (Cook et al. 2005; van der Kolk 2005). Interpersonal support mitigates the negative impact of trauma on child functioning and supports positive adaptation and competence (Masten et al. 1999; Pynoos 1993). Clinicians who specialize in working with this population identify caregiver involvement as essential to therapy (Pond and Spinazzola 2013).
Current Complex Trauma Interventions
While a number of approaches targeting complex trauma in children and families exist (see Ford and Cloitre 2009), there are limits to their applications. Many approaches are intended primarily to ameliorate symptoms of PTSD (Cohen et al. 2006), target child / adolescent intervention in the absence of explicit caregiver supports (i.e., (DeRosa and Pelcovitz 2008), or are designed for use with young children (Lieberman and Van Horn 2008). The Attachment, Regulation and Competency (ARC; Blaustein and Kinniburgh 2010) framework is a core components intervention designed specifically to address the multi-layered diagnostic presentation observed among children who have experienced complex trauma, as well as associated caregiver difficulties. As detailed below, the central goals of the ARC framework are to (a) support caregiving systems and enhance caregiver-child relationships (“Attachment”), (b) support children in developing the skills and tolerance for managing emotional and physiological states (“Self-Regulation”), (c) build key capacities associated with resilience (“Competency”), and (d) integrate traumatic experiences including development of life narrative (“Trauma Experience Integration”). ARC treatment has an emerging evidence base and has demonstrated initial effectiveness at reducing PTSD symptoms and internalizing / externalizing behavior problems with young children (Arvidson et al. 2011), youth in residential care (Hodgdon et al. 2012), and youth included in a national treatment seeking sample (IFCMARCO 2010).
ARC Theoretical Underpinnings
The ARC treatment framework was designed to address the needs of children and families who have experienced multiple and chronic layers of adversity. Drawing from the literature on normative development and on risk and resilience, ARC targets factors that are both impacted by the experience of trauma and relevant to future resilience. ARC is organized within three broad domains comprised of 9 specific treatment targets (see Table 1).
The first primary domain, Attachment, addresses the safety and capacities of the caregiving system. Childhood complex trauma is by definition relational in nature, frequently taking place within the family, implicating the caregiver-child relationship as both context and source of traumatic stress. Traumatic experiences may both influence that relationship, and be influenced by it: in other words, significant adversity can strain and disrupt even previously healthy caregiver – child relationships, and stressed caregiver-child relationships can be a notable vulnerability factor in the response to and healing from adverse exposures. These trauma-related impacts may be complicated by numerous factors, including the frequent intergenerational experience of stress and adversity; the high percentage of trauma-impacted children placed in out-of-home care; and the individual and additive impact of the child’s stress on the caregiver’s own emotional experience. To address this, the ARC framework actively targets caregiver safety and parenting capacities, addressing caregiver regulatory abilities and resources; ability to accurately read and effectively respond to child cues; effective parenting skills; and use of routines to build rhythm and predictability.
The second domain of ARC, Self-regulation, is viewed as the core situ of impact of complex trauma (D’Andrea et al. 2012), with challenges in self-regulation capacity beginning in early childhood (Schore 2001) and continuing across development (Cicchetti and Valentino 2006; Ford 2005) . The drivers of this dysregulation are complex, and may encompass (a) the overwhelming nature of the traumatic exposures, (b) failure of the attachment system to provide adequate modeling, support, and safety, (c) the exacerbating impacts of the child’s use of maladaptive coping strategies (i.e. dissociation, self-injury, substance use), serving to increase rather than decrease dysregulation, and (d) repeated experiences of developmental challenge and stress that are often part of complex trauma experience and its aftermath. ARC simultaneously targets the child’s ability to identify, contextualize, and tolerate internal experience and the environmental resources needed to support the child in active use of those strategies.
The third domain of ARC, developmental Competency, recognizes the pernicious impact of complex trauma on developmental outcomes. In normative development, the attachment system serves as the key model and facilitating environment for the range of developmental tasks, including (a) relational communication and connection, (b) understanding of self and identity, and (c) facilitation of regulation, exploration, and cognitive approach to the world. When trauma disrupts developmental course, particularly when it occurs within or impacts the nature of the caregiving system, salient developmental tasks may be sacrificed in order to prioritize survival. The overwhelming impact of complex childhood trauma on developmental tasks is highlighted in a number of reviews (i.e., D’Andrea et al 2012) which delineate the qualitative difference between childhood- and adult-onset traumatic exposures and emphasize the need for developmentally informed interventions (R. S. Pynoos et al. 2009). Prominent within both the research base on tasks disrupted by early trauma exposure, as well as in literature emphasizing markers of resilience, are executive function capacities and development of healthy self and identity; as a result, these areas serve as primary targets for ARC intervention.
The goal of the current project was to examine the effectiveness of a structured application of the ARC model with complex trauma-exposed, adoptive children and families ages 6–12 through conducting a naturalistic treatment outcome study in an outpatient mental health clinic. We hypothesized that 16 weeks of outpatient ARC treatment would be associated with reductions in child mental health symptoms, including decreases in PTSD symptoms and internalizing and externalizing problems, as well as decreases in caregiving stress.
Method
Participants and Procedures
Data for this study was derived from clinical evaluation data of the ADOPTS Program, a federally funded, multi-site treatment program established by Bethany Christian Services. Clients served via the ADOPTS program included children ages 6 to 17 years in adoptive or pre-adoptive placement, who were referred from adoption and community mental health agencies in their area. Eligibility criteria for ADOPTS included: (a) Pre- or post-adoptive status, including placement in foster care with a plan for adoption, adoptive home (pre- and post-finalization), or long term foster care; (b) 2+ lifetime traumatic exposures; (c) functional impairment across at least two life domains (home, school and / or community); and (d) current PTSD symptoms as measured by the Clinician Administered PTSD Scale (CAPS; Blake et al. 1995). There were no formal exclusion criteria for the ADOPTS program, although some individuals were not enrolled due to diagnoses that would significantly interfere with ability to participate in the program, such as a psychotic disorder or severe developmental disability.
Clinical outcome data from a subset of 481 children and their caretakers enrolled in the ADOPTS Program were selected for use in this project. Children in the study were 6 to 12 years of age (M = 11.04, SD = 3.05) and 49.1 % were male. The sample had the following ethnic breakdown; 18.3 % African American, 2.3 % Asian, 5.2 % Biracial, 56.5 % Caucasian, 6.4 % Hispanic, 0.2 % Native American and 1.6 % Other. Children had 1–27 previous placements (M = 2.91, SD = 2.42) with current placement at time of enrollment as follows: adoptive home (60.1 %), pre-adoptive home (27.4 %), permanent or temporary foster care (4.6 %), residential (3.7 %), and placement described as “other” (3.7 %). The sample had a high rate of trauma exposure with a mean exposure of 4.93 different trauma types (SD = 2.27, range 2–13), including both acts of omission (neglect, attachment disruption, parental mental illness and substance abuse, traumatic loss) and commission (physical, sexual and emotional abuse, exposure to domestic violence and war, medical trauma, acute incidents, and “other trauma”). Exposure rates for each trauma type are provided in Table 2. The vast majority of participants 70.6 % had experienced four or more types of trauma.
Measures
-
1.
Trauma Questionnaire. Lifetime trauma exposure was assessed via a checklist (yes / no) administered to the caregiver assessing child exposure to 13 trauma types including; physical, sexual, and emotional abuse, neglect, parental substance abuse and / or mental illness, attachment disruption, acute trauma, traumatic loss, medical trauma, trafficking, exposure to war / terrorism, witnessing domestic violence and “other trauma”.
-
2.
Clinician Administered PTSD Scale (CAPS: Blake et al. 1995), a 30-item, semi structured clinical interview measuring frequency / severity of PTSD symptoms based on DSM-IV-TR criteria, was used to assess change in PTSD symptom severity from pre- to post-treatment. Frequencies (ranging from 0 = never to 4 = daily or almost daily) are summed to create an overall severity score. The CAPS is reliable and valid measure of PTSD symptoms and has been used in a wide variety of settings and populations (Weathers et al. 2001).
-
3.
Trauma Symptom Checklist for Children (TSCC; Briere 1989), is a 54 item parent-report measure assessing trauma related symptoms, including posttraumatic stress, anxiety, depression, sexual concerns, dissociation and anger among children ages 3 to 12 years of age. The TSC-C has high reliability (Briere 1989; Evans et al. 1994) and moderate levels of convergent / discriminate validity (Lanktree et al. 2008).
-
4.
Behavioral Assessment System for Children, 2nd Edition (BASC-2; Reynolds and Kamphaus 2004) is a 138 item parent report measure assessing internalizing (anxiety, depression and somatization), externalizing (hyperactivity, aggression and conduct) and other (atypicality, withdrawal) problems, as well as adaptive skills, among children ages 2 to 21. The BASC has demonstrated satisfactory internal consistency and test-retest reliability and shows concurrent and discriminate validity (Reynolds and Kamphaus 1992).
-
5.
Parenting Stress Index, Short Form (PSI-SF; Abidin 1995; Loyd and Abidin 1985), is a 36 item caregiver report measure assessing level of stress in the caregiver-child relationship, yielding a Total Stress score, as well as three subscales including Difficult Child, Parent Distress and Parent Perception of Difficult Child. The PSI has demonstrated a high degree of internal consistency, test-rest reliability and factorial validity when administered to parents of children with and without emotional and behavioral problems (Loyd and Abidin 1985).
Treatment Approach and Sequence
The ADOPTS program implemented a 16-week structured application of the ARC treatment framework designed to be used as a brief outpatient intervention with adoptive children and their families (Blaustein and Kinniburgh 2010; Kinniburgh and Blaustein 2005) that included 16 individual sessions and 6 group sessions for both children and caregivers. Weekly individual / family sessions addressed clearly delineated treatment targets, with clinicians providing specific guidance as to session goals, psychoeducational content, and intervention strategies. Topics addressed are delineated in Table 1. All clients participated simultaneously in 6-weeks of parent and child groups emphasizing psychoeducation and skill-building, and reinforcing topics addressed in individual treatment.
Master’s level practitioners in psychology, social work, or related fields provided ARC treatment to the ADOPTS participants. After receiving training in the model, clinicians received weekly supervision and monthly consultation, training, and technical assistance from one of the treatment developers. Clinicians filled out progress notes after each session, including ratings of how well they were able to implement the model’s goals for that week, as well as the degree to which they needed to make modifications to the protocol.
Data Analysis
Initial data analysis examined correlations between parent and child outcome variables (Pearson’s R) and change in diagnostic status from the pre- to post-treatment assessment (Chi Square). Multilevel regression was used to analyze all other outcome data (Singer and Willett 2003). Strengths of multilevel regression include (a) capability of handling missing data and unbalanced designs (i.e., the number of assessment points / timing of assessments can vary across participants) allowing for the inclusion of study participants who had only one data point for a given measure, (b) very efficient and powerful estimation procedures that utilize all data points available, and (c) modeling flexibility that provides multiple options for how to model time and allows for the inclusion of continuous or categorical, time invariant or time varying, predictors and covariates. For the current analyses, time was modeled as a categorical variable using dummy coded time variables (Cohen et al. 2003). This produces a model analogous to a repeated measures ANOVA, but more powerful in that it capitalizes on the many advantages of the multilevel regression approach.
Analyses were conducted using Hierarchical Linear and Non-linear Modeling (HLM6; Raudenbush et al. 2005) software using full-maximum likelihood estimation. Repeated measures were nested within clients; therefore, the Level 1 variable was time and the Level 2 variable was mean change in each outcomes measure. To determine the significance of the overall time effect, the difference in the deviance statistic (i.e., – 2 log-likelihood value) between the unconditional model (i.e., model with no predictors) and a model that includes the dummy coded time variables, was calculated. Examining change in the deviance statistic (Δdev; which follows a chi-squared distribution; Raudenbush and Bryant 2002) to determine the presence of a significant overall time effect is comparable to an omnibus F-test in ANOVA. Regression coefficients for each of the dummy coded time variables were examined to elucidate the nature of the time effect, which corresponds to conducting specific contrasts/comparisons following a significant F-test in ANOVA. To document the strength of the time effect, a R 2 value based on the amount of within-subjects variance accounted for the time variables was calculated.
Results
Child Mental Health Symptoms
-
1.
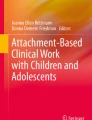
Clinician Administered PTSD Scale (CAPS). Figure 1 presents results of the analyses examining change in total CAPS severity score from pre- to post-treatment. A significant overall time effect emerged for total CAPS score (Δdev = 196.46, df = 1, p < .0001; R 2 = .47). An examination of the regression coefficients revealed a significant reduction in CAPS severity from pre- (M = 58.52) to post-treatment (M = 38.74; b = -19.84, t = -16.26, p < .001). Although not a requirement for inclusion, at the baseline assessment 75.9 % of study subjects met criteria for PTSD per the CAPS. At the post-treatment assessment, only 33.3 % of study subjects met criteria for PTSD, representing a significant change in diagnostic status (X 2 (1, N = 275) = 15.01, p < .001).
Fig. 1 
Change over time in CAPS total severity scores from pre- to post-treatment. N = 481; Overall time effect R2 = .47, P < .0001
-
2.
Trauma Symptom Checklist for Children (TSC-C). Table 3 summarizes results of the analyses examining change over time in the TSC-C subscales. A significant overall time effect emerged for: Anxiety (Δdev = 53.84, df = 2, p < .001; R 2 = .15); Depression (Δdev = 32.68, df = 2, p < .001; R 2 = .09); posttraumatic stress (PTS) scale (Δdev = 44.91, df = 2, p < .001; R 2 = .12); Dissociation (Δdev = 14.12, df = 2, p < .001; R 2 = .05); and Anger (Δdev = 37.30, df = 2, p < .001; R 2 = .10). For the Depression, PTS, Dissociation, and Anger scales, the significant reduction in symptoms from the pre- to post-treatment was maintained (i.e. did not increase or continue to decrease), throughout the follow up period. For the Anxiety scale, there was a significant reduction from pre- (M = 54.42) to post-treatment (M = 50.29; b = -4.14, t = -6.57, p < .001) that continued to decrease throughout the follow up period (M = 48.30; post versus follow-up comparison, b = -1.98, t < .05). No significant change was observed in Sexual Concerns.
Table 3 Change over time in TSC-C subscale scores from pre- to post-treatment and 12 month follow up -
3.
Behavioral Assessment System for Children (BASC). Table 4 summarizes the results of the analyses examining change over time in the BASC, by mother and father report. A significant overall time effect emerged for the following BASC scales: Father reported externalizing (Δdev = 10.21, df = 2, p < .01; R 2 = .09); mother reported externalizing (Δdev = 43.48, df = 2, p < .001; R 2 = .12); mother reported internalizing (Δdev = 27.48, df = 2, p < .001; R 2 = .06); mother reported adaptability (Δdev = 19.90, df = 2, p < .001; R 2 = .05); and mother reported adaptive skills (Δdev = 55.09, df = 2, p < .001; R 2 = .16). For all scales evincing significant change from pre- to post-treatment, change was maintained through the follow up period. Analysis of change over time in father reported internalizing symptoms, adaptability and adaptive skills revealed non-significant findings.
Table 4 Change over time in BASC subscale scores from pre- to post-treatment and 12 month follow up -
4.
Parenting Stress Index (PSI). At baseline significant positive correlations were observed between all parenting stress indicators and child internalizing and externalizing problems, but not with PTSD symptoms (See Table 5). Table 6 summarizes the results of the analyses examining change over time in the PSI, by mother and father report. A significant overall time effect emerged for the following PSI scales: mother reported Total Stress (Δdev = 24.01, df = 2, p < .001; R 2 = .06); mother reported parent distress (Δdev = 7.34, df = 2, p < .05; R 2 = .02); mother reported parent-child dysfunction (Δdev = 15.36, df = 2, p < .001; R 2 = .04); father reported perception of difficult child (Δdev = 7.33, df = 2, p < .05; R 2 = .08), and mother reported perception of difficult child (Δdev = 54.60, df = 2, p < .001; R 2 = .15). For all of the scales demonstrating a significant decrease from pre- to post-treatment, the reduction was maintained throughout the follow up period. Analyses of change over time in father reported total stress, parent distress, and parent-child dysfunction revealed non-significant findings.
Table 5 Correlation matrix: parenting stress and child internalizing, externalizing and PTSD symptoms Table 6 Change over time in PSI subscale scores from pre- to post-treatment and 12 month follow up

Discussion
Although an increasing body of research emphasizes the need to consider the impact of developmental trauma across domains of functioning (D’Andrea et al. 2012), a limited number of studies to date have examined outcomes for trauma-impacted youth broadly, beyond diagnostic classification. This study examined the effectiveness of a structured implementation of a components based intervention for trauma-impacted children and families-- the Attachment, Regulation and Competency (ARC) Framework-- among a sample of adopted children with histories of complex trauma whose diagnostic presentation included, but was not limited to, posttraumatic stress. In this sample, the average presenting youth had a history of exposure to four layers of adversity in early childhood; three living transitions prior to adoptive placement; clinically significant posttraumatic stress symptoms; clinically significant parent-reported externalizing symptoms; and low levels of adaptive functioning. Moreover, the average caregiver was experiencing clinically significant levels of reported stress.
Findings indicate that 16 weeks of individual and group based ARC treatment was associated with improvement in both child and caregiver functioning. Changes in child symptoms included reductions in internalizing, externalizing, posttraumatic stress, depression, anxiety, anger and dissociative symptoms from pre- to post-treatment gains, which were maintained over a 12-month follow up period. Youth also demonstrated change in PTSD diagnosis. These results are consistent with the extant literature on child-trauma interventions demonstrating that short-term, trauma-focused treatments can substantially decrease PTSD. Beyond PTSD, ARC showed promise for reducing externalizing behavioral problems, which is particularly important considering that in real-world settings, externalizing behaviors – acting out, oppositionality, and aggression – are a driving force in child mental health service referral, and at its extreme, of placement instability (James 2004; Proctor et al. 2011).
ARC treatment was also associated with improved caregiver functioning: namely, significant reductions in caregiver perception of child difficulty, as well as on all measured domains of maternal reported stress. This finding is notable in light of recent research demonstrating that caregiver perceptions directly impact child PTS symptoms and internalizing and externalizing behaviors and also are mediated by changes in child emotion regulation (Muller et al. 2013), indicating that caregiver perceptions are an important intervention target as they influence both child symptomatology and self-regulatory capacity.
Also of importance were the strong and significant correlations between caregiver stress variables and youth internalizing and externalizing symptoms at the pre-treatment assessment. Strikingly, the same relation between caregiver stress and child PTSD symptoms was not observed, indicating that while addressing PTSD symptoms is presumably crucial for youth functioning, it may not be sufficient for adequately addressing the transactional interplay between youth and caregiver functioning that characterizes developmental trauma.
As notable as where change was observed, is where it was not observed. A challenge of the treatment outcome research is to both adequately measure the complex presentation of youth and families as they exist in the real world, and to realistically assess what treatment can – and cannot – address within the context of a measurable intervention. The nature of treatment outcome studies frequently requires brief treatment periods, highly controlled protocols, and constraints on client presentation. A naturalistic study utilizing a brief intervention offers a starting point for examining the potential effectiveness of an intervention with a real-world population, while providing some controls over treatment approach and course. In addition, this approach offers the opportunity to examine the limits of shorter-term treatment for children and families impacted by complex trauma. In the current outcome evaluation, although statistically significant change was seen in child externalizing symptoms during the 16-week period under measurement, the absolute shift was not clinically significant. Further, while caregiver perceptions shifted, actual experience of stress continued with less abatement. So while short-term ARC treatment was associated with reductions in PTSD and showed promise for ameliorating broader domains of child and caregiver functioning, it was insufficient to fully address all reported challenges. This may suggest that increasing complexity in youth presentation, history, and family system requires longer-term treatment than is typically measured in treatment outcome research.
One important implication of this study is that it is not sufficient to simply measure diagnostic presentation. By examining presence and level of PTSD alone, youth in this sample show remarkably positive outcomes in a 16-week treatment period. When expanding assessment of outcome to include broader symptom presentation, adaptive functioning, and caregiver functioning, it is clear that although these complex youth and families are demonstrating positive and meaningful progress, there remains work to be done.
Beyond reducing pathology, an important goal of the ARC framework is to support resilient outcomes in youth through actively developing strengths and competencies. Even within this brief intervention period, ARC treatment was associated with improvement in caregiver-reported child adaptability and adaptive functioning. This is notable given that a presumed goal for all trauma-impacted youth is not just less bad, but more good.
Study Limitations
Results of this study must be interpreted within the existing limitations. ARC treatment in this study was delivered via a semi-structured but naturalistic approach taking place in the at times “messy” world of outpatient treatment centers. A major limitation of the current study was the lack of a control group, making it possible that the gains observed in the study sample were due simply to the passage of time or the presence of intervention in general. In addition, there were fewer controls over treatment administration than might exist in a more structured setting (i.e. strict fidelity monitoring via taping of sessions), which likely resulted in greater variability in treatment across clinicians. The lack of blind raters represents a third major limitation, as all evaluators were aware of treatment status and therefore, may have been biased in their ratings. Results, therefore, are most comparable to those derived from program-level evaluation, and while promising, should be interpreted within this limitation. However, it is notable that the effect size for PTSD symptom reduction from pre- to post-treatment as measured by the CAPS for ARC was large (Cohen’s D = 1.88) in this study and comparable to what has been observed in a randomized control trial comparing a treatment-as-usual (TAU) control group to Trauma Focused CBT (TF-CBT) with a similar sample and treatment delivery context, which showed a lower effect size for the TAU group (Cohen’s D = 0.88) and comparable effect size for the TF-CBT intervention group (Cohen’s D = 1.49; Jensen et al. 2014). Finally, information on caregiver socioeconomic status and child community violence exposure was not collected.
Future Directions
Future evaluations of ARC treatment would benefit from use of an active comparison group in order to more definitively demonstrate that ARC surpasses the results that might be anticipated from treatment as usual. While the current study makes a strong initial case for the potential effectiveness of ARC, randomized controlled studies are needed to establish its efficacy. Future studies will need to more carefully evaluate this framework both in comparison to other trauma-informed approaches for this population, as well as using raters blind to treatment status.
Another promising area for further study is examination of the transactional nature of caregiver and child distress, as well as bi-directional influence of changes in functioning. Results of this study suggest that ARC treatment influenced multiple layers of the family system. Examination of the ways that shifts in caregiver functioning influence child symptoms, and vice versa, will aid in delineating further the role of child and caregiver factors on treatment impact. Of particular interest, given that caregiver perception of child behavior was a salient point of change for adults, is direct evaluation of caregiver attributions and understanding of youth behavior, and ways these influence caregiver distress, caregiver skill set, and child functioning.
Additionally, examination of factors that may serve to moderate the impact of ARC treatment on client outcomes would provide valuable information that may ultimately aid in the targeting of ARC interventions. Relevant variables may include child gender, caregiver relationship, and timing / sequencing of treatment targets. Moreover, understanding how trauma specific factors, such as the number, developmental timing and / or chronicity of trauma exposure influences treatment response or length of treatment needed would help to guide the decision making of practitioners regarding allocation of therapeutic resources.
Ultimately, a primary goal in evaluation of this (or any) treatment approach is the real-world meaning for the children and families benefiting from it. Particularly relevant for the population under study is the stability and permanency of placement, an outcome in regard to which ARC has demonstrated initial effectiveness (Arvidson et al. 2011). As is common for young people impacted by multiple adversities, youth in this sample had experienced numerous prior placements, and demonstrated many of the behaviors that lead to vulnerability to placement disruption; placement disruption, in turn, is associated with its own very real and long-term life consequences that go beyond and add onto the original experiences of adversity. It is a central goal, therefore, of the authors to examine longitudinally not just whether ARC is able to ameliorate symptoms and support functioning in the immediate aftermath of intervention, but also whether this in turn leads to the systemic changes crucial to supporting long-term resilient outcomes.
References
Abidin, R. R. (1995). Parenting Stress Index (PSI) manual (3rd ed.). Charlosttesville: Pediatric Psychology Press.
Ackerman, P. T., Newton, J. E. O., McPherson, W. B., Jones, J. G., & Dykman, R. A. (1998). Prevalence of post traumatic stress disorder and other psychiatric diagnoses in three groups of abused children (sexual, physical, and both). Child Abuse and Neglect, 22(8), 759–774.
Armsden, G. C., Pecora, P. J., Payne, V. H., & Szatkiewicz, J. P. (2000). Children placed in long-term foster care: an intake profile using the child behavior checklist / 4-18. Journal fo Emotional and Behavioral Disorders, 8, 49–64.
Arvidson, J., Kinniburgh, K., Howard, K. I., Spinazzola, J., Strothers, H., Evans, M., et al. (2011). Treatment of complex trauma in young children: developmental and cultural considerations in applications of the ARC intervention model. Journal of Child and Adolescent Trauma, 4, 34–51.
Blake, D. D., Weathers, F. W., Nagy, L. M., Kaloupek, D. G., Gusman, F. D., Charney, D. S., et al. (1995). The development of a clinician-administered PTSD scale. Journal of Traumatic Stress, 8(1), 75–90.
Blaustein, M., & Kinniburgh, K. (2010). Treating traumatic stress in children and adolescents: How to foster resilience through attachment, self-regulation, and competency. New York: The Guilford Press.
Briere, J. (1989). Trauma Symptom Checklist for Children (TSC-C).
Briggs, E. C., Fairbank, J. A., Greeson, J. K. P., Layne, C. M., Steinberg, A. M., Amaya-Jackson, L. M., et al. (2012). Links between child and adolescent trauma exposure and service use histories in a national clinic-referred sample. Psychological Trauma: Theory, Research, Practice, and Policy.
Briggs, E. C., Greeson, J. K. P., Layne, C. M., Fairbank, J. A., Knoverek, A. M., & Pynoos, R. S. (2012b). Treatment needs and approaches for perpetrators and victims of trauma. Journal of Child and Adolescent Trauma, 5, 1–15.
Cicchetti, D., & Valentino, K. (2006). An ecological-transactional perspective on child maltreatment: Failure of the average expectable environment and its influence on child development. In D. J. Cohen (Ed.), Developmental psychopathology, vol 3: Risk, disorder, and adaptation (2nd ed., pp. 129–201). Hoboken: John Wiley & Sons Inc.
Cloitre, M., Stolbach, B. C., Herman, J., Van der Kolk, B., Pynoos, R., Wang, J., et al. (2009). A developmental approach to complex PTSD: childhood and adult cumulative trauma as predictors of system complexity. Journal of Traumatic Stress, 22(5), 399–408.
Cohen, J., Cohen, P., West, S. G., & Aiken, L. S. (2003). Applied multiple regression / correlation analysis for the behavioral sciences (3rd ed.). Hillsdale: Erlbaum.
Cohen, J., Mannarino, A., & Deblinger, E. (2006). Treating trauma and traumatic grief in children and adolescents. New York: The Guilford Press.
Cook, A., Spinazzola, J., Ford, J., Lanktree, C., Blaustein, M., Cloitre, M., et al. (2005). Complex trauma in children and adolescents. Psychiatric Annals, 35(5), 390–398.
D’Andrea, W., Ford, J., Stolbach, B., Spinazzola, J., & Van der Kolk, B. (2012). Understanding interpersonal trauma in children: why we need a developmentally appropriate trauma diagnosis. American Journal of Orthopsychaitry, 82(2), 187–200.
DeRosa, R., & Pelcovitz, D. (Eds.). (2008). Igniting SPARCS of change: Structured psychotherapy for adolescents responding to chronic stress. New York: Routledge.
Evans, J. J., Briere, J., Boggiano, A. K., & Barrett, M. (1994). Reliability and validity of the trauma symptom check list for children in a normal sample.Unpublished manuscript.
Ford, J. D. (2005). Treatment implications of altered affect regulation and information processing following child maltreatment. Psychiatric Annals, 35(5), 410–419.
Ford, J. D., & Cloitre, M. (2009). Best practices in psychotherapy for children and adolescents. In C. Courtois & J. D. Ford (Eds.), Treating complex traumatic stress disorders: An evidence-based guide (pp. 59–81). New York: Guilford.
Garland, A. F., Hough, R. L., McCabe, K. M., Yeh, M., Wood, P. A., & Aarons, G. A. (2001). Prevalence of psychiatric disorder in youths across five sectors of care. Journal of the American Academy of Child and Adolescent Psychiatry, 40(4), 409–418.
Hodgdon, H. B., Kinniburgh, K., Gabowitz, D., Blaustein, M., & Spinazzola, J. (2012). Development and implementation of trauma-informed programming in residential schools using the ARC framework. Journal of Family Violence.
IFCMARCO (2010). Evaluation of the National Child Traumatic Stress Initiative: FY 2010 Annual Progress Report, Executive Summary.
James, S. (2004). Why do foster care placements disrupt? An investigation of reasons for placement change in foster care. Social Service Review, 78(4), 601–627.
Jensen, T. K., Holt, T., Ormhaug, S. M., Egeland, K., Granly, L., Hoaas, L. C., et al. (2014). A radonmized effectiveness study comparing trauma-focused cognitive behavioral therapy with therapy as usual for youth. Journal of Clinical Child & Adolescent Psychology, 43, 356–369.
Kinniburgh, K., & Blaustein, M. (2005). Attachment, Self-Regulation, and Competency: A comprehensive framework for intervention with complexly traumatized youth. A Treatment Manual. Boston: Author.
Lanktree, C. B., Gilbert, A. M., Briere, J., Taylor, N., Chen, K., Maida, C. A., et al. (2008). Multi-informant assessment of maltreated children: convergent and discriminant validity of the TSCC and TSCYC. Child Abuse and Neglect, 32(6), 621–625.
Lieberman, A. F., & Van Horn, P. (2008). Psychotherapy with infants and young children: Repairing the effects of stress and trauma on early attachment. New York: Guilford Press.
Loyd, B. H., & Abidin, R. R. (1985). Revision of the parenting stress index. Journal of Pediatric Psychology, 10(2), 169–177.
Manly, J., Kim, J., Rogosh, F., & Cicchetti, D. (2001). Dimensions of child maltreatment and children’s adjustment: contributions of developmental timing and subtype. Development and Psychopathology, 13, 759–782.
Masten, A. S., Hubbard, J. J., Gest, S. D., Tellegen, A., Garmezy, N., & Ramirez, M. (1999). Competence in the context of adversity: pathways to resilience and maladaptation from childhood to later adolescence. Development and Psychopathology, 11, 143–169.
Morgan, J., Robinson, D., & Aldridge, J. (2002). Parenting stress and externalizing child behavior. Child Family Social Work, 7, 219–225.
Muller, R. T., Vascotto, N. A., & Konanur, S. (2013). Caregiver perceptions and expectations and child emotion regulation: a test of two mediation models predicting child psychopathology among trauma-exposed children. Journal of Child and Adolescent Trauma, 6(2), 126–141.
Pond, A., & Spinazzola, J. (2013). Residential services for children and adolescents impacted by family violence and trauma. Journal of Family Violence, 28(7), 635–638.
Proctor, L. J., Van Dusen Randazzo, K., Litrownik, A., Newton, R. R., Davis, I. P., & Villodas, M. (2011). Factors associated with caregiver stability in permanent placements: a classification tree approach. Child Abuse & Neglect, 35, 425–436.
Pynoos. (1993). Traumatic stress and developmental psychopathology in children and adolescents. In R. Pynoos (Ed.), Posttraumatic stress disorders: A clinical review (pp. 65–98). Lutherville: The Sidrun Press.
Pynoos, R. S., Steinberg, A., Layne, C., Briggs-King, E., Orstrowki, S., & Fairbank, J. (2009). DSM-V PTSD Diagnostic criteria for children and adolescents: A developmentla perspective and recommendations. Jounral of Traumatic Stress, 22(391–398).
Raudenbush, S. W., & Bryant, R. A. (2002). Heirarchical linear models: Applications and data analysis methods. Newbury Park: Sage Publications.
Raudenbush, S. W., Bryk, A., & Congdon, R. (2005). HLM 6: Hierarchical linear and nonlinear modeling [computer software and manual]. Lincolnwood: Scientific Software International.
Reynolds, C. R., & Kamphaus, R. W. (1992). BASC parent rating scales PRS-C (Ages 6-11).
Reynolds, C. R., & Kamphaus, R. W. (2004). BASC-2: Behavior assessment system for children, Second Edition Manual. Circle Pines: American Guidance Service.
Rodriguez, C. M., & Green, A. (1997). Parenting stress and anger expression as predictors of child abuse potential. Child Abuse & Neglect, 21, 367–377.
Schore, A. N. (2001). The effects of early relational trauma on right brain development, affect regulation, and infant mental health. Infant Mental Health Journal, 22(1), 201–269.
Singer, J. D., & Willett, J. B. (2003). Applied longitudinal data analysis: Modeling change and event occurence. New York: NY: Oxford University.
Spinazzola, J., Ford, J. D., Zucker, M., van, d. K., Silva, S., Smith, S. F., et al. (2005). Survey Evaluates Complex Trauma Exposure, Outcome, and Intervention Among Children and Adolescents. Psychiatric Annals, 35(5), 433–439.
U.S. Department of Health and Human Services, A. o. C., Youth and Families, (2015). Child Maltreatment 2013. from http://www.acf.hhs.gov/programs/cb/research-data-technology/statistics-research/child-maltreatment.
van der Kolk, B. A. (2005). Developmental trauma disorder: toward a rational diagnosis for children with complex trauma histories. Psychiatric Annals, 35(5), 401–408.
Vanderfaeillie, J., Van Holen, F., Vanschoonlandt, F., Robberechts, M., & Stoobants, T. (2013). Child placed in long-term family foster care: a longitudinal study into the development of problem behavior and associated factors. Children and Youth Services Review, 35, 587–593.
Weathers, F. W., Keane, T. M., & Davidson, J. R. T. (2001). Clinician-administered PTSD Scale: a review of the first ten years of research. Depression and Anxiety, 13, 132–156.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Hodgdon, H.B., Blaustein, M., Kinniburgh, K. et al. Application of the ARC Model with Adopted Children: Supporting Resiliency and Family Well Being. Journ Child Adol Trauma 9, 43–53 (2016). https://doi.org/10.1007/s40653-015-0050-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40653-015-0050-3