
Abstract
The majority of end-stage kidney disease patients are treated with haemodialysis (HD). Starting HD can pose physical, social, and psychological challenges to patients, and mortality rates within the first 6 months are disproportionately high, with intensive HD regimens implicated as a potential factor. Starting HD with an incremental approach, taking residual kidney function (RKF) into account, potentially allows for a gentle start with reduced dialysis intensity. Dialysis intensity (session time or frequency) can then be proportionally increased as RKF reduces. This approach to starting HD has been reported in observational studies to result in better patient self-reported health quality of life and reduced costs, and now several definitive randomised controlled trials are underway comparing an incremental approach to the conventional thrice weekly paradigm. Physician concerns over the risk of inadequate dialysis, with consequent increased emergency admissions, and practical challenges of how to estimate RKF and implement incremental dialysis have impeded widespread adoption. Addressing these challenges is paramount to increasing the uptake of incremental HD. Careful patient selection lies at the heart of a successful incremental HD programme. Generally, patients with a residual urea clearance of > 3 ml/min/1.73 m2 can be considered suitable for starting with incremental HD provided they comply with fluid intake, salt and other dietary recommendations. Calculating RKF from regular interdialytic urine collections and appropriately adjusting sessional HD clearance targets are practical and conceptual challenges. In this report we aim to disentangle these complexities and provide a step-by-step guide for patient selection and adjusting dialysis sessional targets.
Graphical abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The number of patients with end-stage kidney disease continues to increase world-wide, and the majority of patients are treated by haemodialysis (HD). While HD is life-sustaining for many patients with kidney failure, it can be burdensome and is associated with physical, social, and psychological challenges. In the 6 months after HD initiation, mortality rates are disproportionately high, with the abrupt transition to intensive thrice-weekly HD regimens being implicated [1]. Increased availability and access to dialysis services has led to many patients now starting dialysis while still having some residual kidney function (RKF), which may persist for many months or even years. Retention of RKF is associated with improved outcomes including control of blood pressure, anaemia, nutrition, increased middle molecule clearance and survival benefit [2,3,4,5,6]. More intensive HD can accelerate loss of RKF [7], whereas a more gradual dialysis start may potentially be protective [8, 9].
Incremental HD utilises RKF to reduce dialysis intensity, minimising session frequency or duration below what would be considered standard therapy of 4 h thrice weekly. Haemodialysis can be initiated at lower intensity, even starting from once a week dialysis, and incrementally increased according to individual need as RKF reduces. This is in contrast to palliative dialysis with reduced session frequency or duration and no incremental intention. Numerous observational and two feasibility randomized control trials (RCTs) have demonstrated that incremental HD can mitigate some of the burdens, harms, and costs of conventional initiation [10]. Various definitive trials are underway internationally. The IHDIP trial is investigating the safety of once weekly HD initiation [11]. The REAL LIFE trial is planned to investigate preservation of RKF by incremental HD, and also involves HD frequency as low as once a week [12]. The TWOPLUS trial is planned as a non-inferiority study of incremental dialysis with primary composite outcome of all-cause hospitalizations, emergency department visits, or death (ClinicalTrials.gov ID NCT 05828823). The US INCHVETS study (ClinicalTrials.gov ID NCT05465044) will examine health-related quality of life in incremental HD compared to thrice weekly HD. The Australian INCH-HD study will determine the impact of twice weekly HD initiation on the kidney-specific component of KDQOL-SF [13].
Despite the potential benefits, incremental HD adoption remains low, in part due to practical challenges of performing incremental HD and physician concern regarding risks of underdialysis. We aim to provide a practical guide for safe incremental HD implementation and guidance on patient selection.
Practical ways to perform incremental dialysis
Patient selection
One of the basic determinants of patient selection for Incremental HD is RKF. Substantial data from observational and feasibility prospective studies support incremental HD in patients with a renal urea clearance (KrU) > 3 ml/min/1.73 m2 body surface area and a urine output of > 500 ml/day [9, 14,15,16]. It may be possible to identify patients with a KrU > 3 ml/min with a β2 microglobulin blood test but this approach has not been applied in safety studies [17].
Patient adherence to fluid and salt restriction and dietary advice also needs to be taken into account [15]. Inadequate volume control would necessitate a longer dialysis session or more frequent dialysis, therefore weight gain between the dialysis sessions needs to be taken into consideration when assessing suitability of the patient for incremental dialysis.
Although not usually accounted for, minimum dialysis dose to achieve toxin clearance depends on physical activity and energy expenditure. Physically active patients generating more waste products of metabolism would require more dialysis [18]. Physical activity may need to be considered when dialysing using an incremental approach by uplifting the clearance target. Older, less active patients may therefore particularly benefit from incremental dialysis.
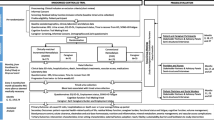
A decision aid for incremental vs conventional HD start is shown in Fig. 1.

Decision aid for incremental vs conventional HD start based on patient’s characteristics
Monitoring RKF
A standard method of measuring RKF is timed urine collection, with KrU calculated by the ratio of urea removal rate to plasma urea concentration. [19].
where KrU is expressed in ml/min. Uurea and Purea are urine and plasma concentration of urea, respectively. U vol is the urine volume in the collection interval. Collection time is typically the interdialytic interval which conventionally is taken as the interval between the first 2 dialysis sessions of the week. However, urine collection for the full interdialytic interval may be cumbersome. Several methods have been reported to estimate KrU from partial interdialytic urine collections ending before the next HD session (e.g. last 24 h of the interdialytic interval).
To calculate KrU, the steady state urea during the urine collection period is required (Purea), which is difficult to measure in intermittent dialysis. There are a few different ways to determine Purea which is most representative of steady state urea concentration. Most simply it can be expressed as the average of post- and pre-dialysis urea concentrations between the two consecutive dialysis sessions. An alternative expression of steady state urea is time-averaged urea concentration TACUrea, which requires formal urea kinetic modelling. Daugirdas et al. have reported a method of estimating TACUrea as a function of duration of urine collection within the interdialytic interval, urea reduction ratio (URR) during the dialysis session, and pre-dialysis urea concentration (before the next HD session) [20, 21]
where \(R = 1.075 - \left( {0.0038~ \times URR + 0.059} \right) \times \frac{{Duration~of~urine~collection}}{{Interdialytic~interval}}\)
URR in the equation above is the urea reduction ratio.
A similar method of calculating RKF based on full or partial interdialytic urine collection has been reported by Lindley and validated using data from the BISTRO study [22]. The method described assumes that urea generation rate remains constant during each interdialytic interval of the week and that solute reduction ratio is equal for each HD session of the week. With this method it is possible to calculate KrU using a pre- and post-dialysis urea and a partial interdialytic urine collection provided the patient records the time when the urine collection commenced. This method utilises estimation of the solute concentrations at the end of the urine collection and may provide a simplified method of RKF estimation.
Frequent interdialytic urine collection to monitor RKF is difficult from a patient’s perspective, hence there is developing interest in estimating RKF from plasma concentration of middle molecules such as β-2 microglobulin [23,24,25]. This could potentially do away with the need for interdialytic urine collection. Factors which can affect β-2 microglobulin concentration such as chronic inflammatory conditions, and some cancers need to be taken into account when estimating RKF using this method. These methods of RKF estimation have not been applied in prospective trials and their reliability is not yet established.
Adding RKF with dialysis clearance
Haemodialysis provides intermittent (sessional) clearance of uraemic toxins (Kd), whereas RKF provides continuous clearance, expressed as KrU. These entities are not equivalent, so they cannot be directly added together. Combining these two necessitates making one equivalent to the other by one of the following ways [26]:
-
a.
Convert continuous RKF clearance (KrU) to an equivalent intermittent clearance comparable to HD.
-
b.
Convert intermittent HD clearance (Kd) to an equivalent continuous clearance comparable to RKF.
Both approaches will allow simple addition of the dialysis and RKF clearances [26, 27].
Converting RKF to intermittent clearance
A relatively simple way to add RKF to Kd is to convert RKF (KrU) to an equivalent per-session Kt/V to allow its addition to Kt/V from HD.
where Kd is the dialysis clearance, Td is time on dialysis, Kr is KrU from interdialytic urine collection, Tr is the mean time interval between two HD sessions, and VUrea is the volume of distribution of urea. In the above, Kt/VDialysis is calculated using either conventional spKt/Vurea or eKt/Vurea using standard methodology.
However, continuous clearance is thought to be more efficient than intermittent dialysis clearance. To account for this difference in clearance efficiencies, the interdialytic interval Tr can be adjusted. For thrice weekly and twice weekly HD, a Tr of 5500 and 9500 min may be used, respectively, with different values used for other HD frequencies [27]. The effect of enhanced efficiency of RKF is more pronounced with fewer dialysis treatments per week. Hence, the adjusted Tr value reduces for increasing HD frequency [26, 27]. Since this method calculates per session clearance, the minimum per session Kt/VTotal is different for different dialysis frequencies. For thrice weekly dialysis the minimum per session Kt/VTotal is 1.2. The target for other frequencies is not well established; for twice weekly dialysis it is ≈ 1.86 [28]. An example of how to calculate dialysis and renal clearance using this method is described in the Appendix.
In our centre we have been practising incremental dialysis for more than 20 years using this method.
Converting dialysis clearance (K d) to equivalent continuous clearance
An alternative approach is to convert Kd to its continuous equivalent, followed by the addition to KrU. There are two different methods based on this principal.
Casino–Lopez method /Fixed equivalent renal urea clearance
The Casino and Lopez method [29] is recommended by European Best Practice Guidelines [30].
In this method combined Kd and KrU are expressed as ‘equivalent renal urea clearance’ (EKR) as shown in Fig. 2. Equivalent renal urea clearance is computed as a ratio of urea generation (G) and Time averaged urea concentration normalized to 40 L which is considered to be the volume of urea distribution in an average individual, to allow comparison between different patients. The relationship between equivalent renal urea clearance, eKt/V and KRU was determined using a nomogram. The minimum adequate equivalent renal urea clearance to achieve eKt/V of 1.2 was 13 ml/min. This relationship is described as follows:

Fixed target model for equivalent renal urea clearance
Rearranging the equation minimum ekt/v to achieve equivalent renal urea clearance of ≈13 ml/min in the presence of varying KrU can be derived as follows:
These equations apply to thrice weekly dialysis. Different formulae are required for other dialysis schedules with different contributions of dialysis and renal clearance to achieve an equivalent renal urea clearance of 13 ml/min.
For twice weekly dialysis the equation derived was
With increasing HD frequency, this equation markedly inflates the effect of dialysis clearance. An example of how to calculate dialysis and renal clearance using this method is described in the Appendix.
A limitation of this method is that target equivalent renal urea clearance 13 ml/min was primarily based on dialysis clearance (ekt/V 1.2) and assumed KrU = 0ml/min. Adjusting the HD clearance in patients with a significant KrU to achieve equivalent renal urea clearance target of 13 ml/min assumes equal contribution of HD clearance and KrU. Due to the inability to correct for enhanced efficiency of native RKF, in this method equivalent renal urea clearance relies heavily on HD clearance. Hence, it is difficult to achieve target equivalent renal urea clearance with less frequent dialysis using this method. This can be overcome using the modified method reported below.
Variable equivalent renal urea clearance
Casino and Basile reported a method to adjust for higher efficiency of KrU compared to Kd. They corrected KrU to 35L (rather than 40L) since this provides a better equivalence to 1.73m2 body surface area, the usual scaling adjustment used for clearance, and introduced a concept of a variable target model, whereby equivalent renal urea clearance target (equivalent renal urea clearance from dialysis + RKF) changes with KrU, as opposed to fixed equivalent renal urea clearance target [31].
Depending on the relative equivalence of KrU compared to Kd, Casino and Basile developed maximum and minimum equivalent renal urea clearance targets [32]. The maximum equivalent renal urea clearance target considers HD initiation below KrU 6 ml/min/35L and assumes that KrU is twice as efficient as Kd. Therefore, with 1ml/min fall in KrU below 6ml/min, equivalent renal urea clearance target increases by 1 ml/min. The equation for maximum adequacy target is:
where KRUn is KrU corrected for V = 35 L (KrU × 35/V).
One can see that for a patient with KrU 6ml/min/35L, equivalent renal urea clearance target = 6 ml/min, this patient would not be expected to require dialysis (Fig. 3). Whereas for a patient with KrU 4ml/min, equivalent renal urea clearance target = 8ml/min an additional equivalent renal urea clearance of 4ml/min would be required from dialysis (EKRd) (Fig. 3).

Variable target model with maximum equivalent renal urea clearance target
The minimum equivalent renal urea clearance target considers dialysis initiation below KrU 4 ml/min/35L and assumes KrU is 2.5 times as efficient as Kd. Therefore, a fall of 1 ml/min in KrU below 4 ml/min would increase the target equivalent renal urea clearance by 1.5 ml/min and EKRd will need to increase by 2.5 ml/min to achieve this target (Fig. 4). The equation for minimum adequacy target is:

Variable target model with minimum equivalent renal urea clearance target
Any equivalent renal urea clearance value achieved between minimum and maximum target equivalent renal urea clearance is considered adequate (Fig. 5). Per-session eKt/V required to achieve this variable target can then be calculated for different dialysis schedules with varying KrU [33], as exemplified in the Appendix. Similarly, the per-session eKt/V required to achieve this minimum target equivalent renal urea clearance can be determined for varying dialysis schedules and KrU. An eKt/V achieved between maximum and minimum target eKt/V is considered adequate.

Variable target model adequacy map for incremental dialysis prescription with maximum and minimum equivalent renal urea clearance targets and adequacy zone
Another simplified approach to perform incremental dialysis emerged from variable target model modelling which proposed to keep eKt/V constant and change the frequency of dialysis as a function of KrU. Keeping eKt/V as 1.2, which is considered adequate dialysis sessional clearance, Casino and Basile identified the range of KrU within which 1 × weekly, 2 × weekly and 3 × weekly dialysis can be performed safely [32]. There is an ongoing pragmatic multicentre RCT to determine the efficacy and safety of incremental dialysis using a variable target model [12]. Compared to a fixed equivalent renal urea clearance target model, a variable equivalent renal urea clearance target model allows incremental dialysis to start even at once a week dialysis due to adjustment for higher efficiency of KrU.
Standard K t/V
Gotch and Leypoldt described another method of converting Kd to its continuous equivalent, expressed as standard (std) Kt/V [34, 35]. It was proposed to measure continuous equivalent of Kd from urea generation (G) and average pre-dialysis urea concentration.
This is similar to the Casino–Lopez method except that average pre-dialysis urea was used instead of time averaged urea concentration urea. This was based on the assumption that time averaged urea concentration urea is lower than the steady state urea concentration.
A weekly standard Kt/V of 2 equates to spKt/v of 1.2 for thrice weekly dialysis schedules. This method is also limited by the fact that it assumes no KrU and fixed volume of distribution [34].
Daugirdas et al. corrected the Leypoldt standard kt/v for volume changes (weekly fluid gains between dialyses) and also developed an algorithm to add renal standard Kt/v with dialysis standard Kt/v [36]. A detailed description of this method is reported in the Appendix. This method provides a reliable tool to add RKF with dialysis clearance to determine the total clearance. A UK feasibility RCT has employed this method with the calculation procedure reported in Supplementary material [9].
KDOQI 2015 guidelines suggest target weekly standard Kt/V of 2.3 with a minimum delivered dose of 2.1 using a method of calculation that includes the contributions of ultrafiltration and residual kidney function [37].
Other methods
There are other simplified methods to perform incremental HD which put less emphasis on precise measurement of RKF. Two of these methods are as follows.
KDOQI 2006 recommendations
KDOQI 2006 Haemodialysis adequacy guidelines proposed a simple way to take into account RKF to perform minimally adequate dialysis. It was recommended to reduce the target spKt/V in patients with KrU ≥ 2 ml/min [38]. The guideline recommends capping the allowed dialysis dose reduction at this level of KrU. This is a step-wise approach where patients with KRU of < 2 ml/min would dialyse to achieve normal spKt/v target and those with ≥ 2 ml/min would dialyse at the same reduced dose, even if their KrU is much higher than 2 ml/min.
Adjusting dialysis dose based on clinical and biological surveillance
The concept of ‘Dialysis adequacy’ is limited if only considered as related to uraemic toxin clearance. Dialysis adequacy reflects many other clinically relevant aspects of dialysis patient care including cardiovascular disease, renal anaemia, nutrition, fluid balance, mineral bone disorders and quality of life. Strict clinical and biological surveillance could be an alternative to complex calculations of RKF and dialysis adequacy.
Based on this concept, incremental HD could be performed in carefully selected patients until there is clinical indication to increase the dialysis frequency, such a fluid overload, hyperkalaemic events etc., irrespective of RKF and delivered dialysis dose. There is an ongoing Australian prospective RCT to test the non-inferiority of this approach in health-related quality of life[13].
Discussion
Retrospective data report the quality of life and health economic benefits of incremental HD but there are practical and conceptual barriers to its implementation. Broad clinical adaptation of incremental dialysis requires better clinician understanding of the practicalities and barriers of this approach. In this review we have explored some of the key practical aspects of incremental HD and provided a practical guide to perform incremental dialysis.
In essence, a safe way to perform incremental HD would involve frequent monitoring of RKF and addition of RKF with dialysis clearance with one the described methods. Although incremental HD can be performed solely based on clinical events without precise addition of RKF and dialysis clearance, there are safety concerns with this approach, and it requires evaluation in an ongoing clinical trial.
Frequent RKF monitoring and precise calculations require time and effort. It also requires patient education for effective concordance. All of these have additional financial implications. However, there are substantial cost savings due to reduced dialysis treatment. Vilar et al. reported health economic benefits for incremental dialysis in an incremental HD feasibility trial [16].
Patients with progressive chronic kidney disease generally spontaneously follow a low protein diet, with some centres advocating 0.6–0.8 g/kg/day, or even lower protein intakes of 0.3–0.4 g/kg/day with keto analogue supplements designed to slow the progressive loss of kidney function and for conservative management [39], whereas HD patients are recommended to eat 1.0–1.2 g/kg/day (Kidney Disease Outcome Quality Initiate (KDOQI)) [40]. Although some centres advocate continuing protein restriction when patients initiate incremental dialysis, this will depend on individual patient requirements such as body composition and physical activity [41]. As a three-hour HD session will clear much more urea, creatinine and phosphate compared to 24-h urine of end-stage kidney disease patients, protein restriction should generally be increased, with individual targets determined by trained renal dietitians, especially as incremental dialysis is more appropriate for elderly patients initiating dialysis [42]. Nonetheless, patients should generally continue a low sodium, potassium, and phosphate diet. However, initiating incremental dialysis may not provide sufficient bicarbonate to correct metabolic acidosis, and so patients may require on-going bicarbonate supplementation.
Data availability
Not applicable as there are no research data.
References
Lukowsky LR, Kheifets L, Arah OA, Nissenson AR, Kalantar-Zadeh K (2012) Patterns and predictors of early mortality in incident hemodialysis patients: new insights. Am J Nephrol 35(6):548–558
Vilar E, Wellsted D, Chandna SM, Greenwood RN, Farrington K (2009) Residual renal function improves outcome in incremental haemodialysis despite reduced dialysis dose. Nephrol Dial Transplant 24(8):2502–2510
Chandna SM, Farrington K (2004) Residual renal function: considerations on its importance and preservation in dialysis patients. Semin Dial 17(3):196–201
Menon MK, Naimark DM, Bargman JM, Vas SI, Oreopoulos DG (2001) Long-term blood pressure control in a cohort of peritoneal dialysis patients and its association with residual renal function. Nephrol Dial Transplant 16(11):2207–2213
Penne EL, van der Weerd NC, Grooteman MP, Mazairac AH, van den Dorpel MA, Nubé MJ et al (2011) Role of residual renal function in phosphate control and anemia management in chronic hemodialysis patients. Clin J Am Soc Nephrol 6(2):281–289
Wang AY, Sea MM, Ip R, Law MC, Chow KM, Lui SF et al (2001) Independent effects of residual renal function and dialysis adequacy on actual dietary protein, calorie, and other nutrient intake in patients on continuous ambulatory peritoneal dialysis. J Am Soc Nephrol 12(11):2450–2457
Daugirdas JT, Greene T, Rocco MV, Kaysen GA, Depner TA, Levin NW et al (2013) Effect of frequent hemodialysis on residual kidney function. Kidney Int 83(5):949–958
Kaja Kamal RM, Farrington K, Busby AD, Wellsted D, Chandna H, Mawer LJ et al (2019) Initiating haemodialysis twice-weekly as part of an incremental programme may protect residual kidney function. Nephrol Dial Transplant 34(6):1017–1025
Murea M, Patel A, Highland BR, Yang W, Fletcher AJ, Kalantar-Zadeh K et al (2022) Twice-weekly hemodialysis with adjuvant pharmacotherapy and transition to thrice-weekly hemodialysis: a pilot study. Am J Kidney Dis 80(2):227-40e1
Caton E, Sharma S, Vilar E, Farrington K (2022) Impact of incremental initiation of haemodialysis on mortality: a systematic review and meta-analysis. Nephrol Dial Transplant 38(2):435–446
Deira J, Suárez MA, López F, García-Cabrera E, Gascón A, Torregrosa E et al (2019) IHDIP: a controlled randomized trial to assess the security and effectiveness of the incremental hemodialysis in incident patients. BMC Nephrol 20(1):8
Casino FG, Basile C, Kirmizis D, Kanbay M, van der Sande F, Schneditz D et al (2020) The reasons for a clinical trial on incremental haemodialysis. Nephrol Dial Transplant 35(11):2015–2019
The INCremental dialysis to improve Health outcomes in people starting Haemodialysis (INCH-HD) study: a randomised controlled trial. https://aktn.org.au/inch-hd. Accessed 17 Nov 2023
Obi Y, Streja E, Rhee CM, Ravel V, Amin AN, Cupisti A et al (2016) Incremental hemodialysis, residual kidney function, and mortality risk in incident dialysis patients: a cohort study. Am J Kidney Dis 68(2):256–265
Rhee CM, Ghahremani-Ghajar M, Obi Y, Kalantar-Zadeh K (2017) Incremental and infrequent hemodialysis: a new paradigm for both dialysis initiation and conservative management. Panminerva Med 59(2):188–196
Vilar E, Kaja Kamal RM, Fotheringham J, Busby A, Berdeprado J, Kislowska E et al (2022) A multicenter feasibility randomized controlled trial to assess the impact of incremental versus conventional initiation of hemodialysis on residual kidney function. Kidney Int 101(3):615–625
Vilar E, Boltiador C, Wong J, Viljoen A, Machado A, Uthayakumar A et al (2015) Plasma levels of middle molecules to estimate residual kidney function in haemodialysis without urine collection. PLoS ONE 10(12):e0143813
Sridharan S, Vilar E, Davenport A, Ashman N, Almond M, Banerjee A et al (2017) Scaling hemodialysis target dose to reflect body surface area, metabolic activity, and protein catabolic rate: a prospective, cross-sectional study. Am J Kidney Dis 69(3):358–366
Chin AI, Depner TA, Daugirdas JT (2017) Assessing the Adequacy of Small Solute Clearance for Various Dialysis Modalities, with Inclusion of Residual Native Kidney Function. Semin Dial 30(3):235–240
Daugirdas JT (2016) Estimating Time-averaged Serum Urea Nitrogen Concentration during Various Urine Collection Periods: A Prediction Equation for Thrice Weekly and Biweekly Dialysis Schedules. Semin Dial 29(6):507–509
Obi Y, Kalantar-Zadeh K, Streja E, Daugirdas JT (2018) Prediction equation for calculating residual kidney urea clearance using urine collections for different hemodialysis treatment frequencies and interdialytic intervals. Nephrol Dial Transplant 33(3):530–539
Lindley E, Keane D, Belcher J, Fernandes Da Silva Jeffcoat N, Davies S. Monitoring residual kidney function in haemodialysis patients using timed urine collections: validation of the use of estimated blood results to calculate GFR. Physiol Meas. 2022;43(8).
Shafi T, Levey AS (2018) Measurement and Estimation of Residual Kidney Function in Patients on Dialysis. Adv Chronic Kidney Dis 25(1):93–104
Davenport A (2016) Measuring residual renal function in dialysis patients: can we dispense with 24-hour urine collections? Kidney Int 89(5):978–980
Wong J, Sridharan S, Berdeprado J, Vilar E, Viljoen A, Wellsted D et al (2016) Predicting residual kidney function in hemodialysis patients using serum β-trace protein and β2-microglobulin. Kidney Int 89(5):1090–1098
Wong J, Vilar E, Davenport A, Farrington K (2015) Incremental haemodialysis. Nephrol Dial Transplant 30(10):1639–1648
Depner TA (2005) Hemodialysis adequacy: basic essentials and practical points for the nephrologist in training. Hemodial Int 9(3):241–254
Gotch FA, Nissenson A, Fine R, Gentile D. Clinical dialysis. Chapter six: Kinetic modeling in hemodialysis Second. 1995.
Casino FG, Lopez T (1996) The equivalent renal urea clearance: a new parameter to assess dialysis dose. Nephrol Dial Transplant 11(8):1574–1581
II.3 Haemodialysis dose and residual renal function (Kr). Nephrology Dialysis Transplantation. 2002;17(suppl_7):24-.
Casino FG, Basile C (2017) The variable target model: a paradigm shift in the incremental haemodialysis prescription. Nephrol Dial Transplant 32(1):182–190
Basile C, Casino FG (2019) Incremental haemodialysis and residual kidney function: more and more observations but no trials. Nephrol Dial Transplant 34(11):1806–1811
Casino FG, Basile C (2018) A user-friendly tool for incremental haemodialysis prescription. Nephrol Dial Transplant 33(6):1046–1053
Gotch FA (1998) The current place of urea kinetic modelling with respect to different dialysis modalities. Nephrol Dial Transplant 13(Suppl 6):10–14
Leypoldt JK (2004) Urea standard Kt/V(urea) for assessing dialysis treatment adequacy. Hemodial Int 8(2):193–197
Daugirdas JT, Depner TA, Greene T, Levin NW, Chertow GM, Rocco MV (2010) Standard Kt/Vurea: a method of calculation that includes effects of fluid removal and residual kidney clearance. Kidney Int 77(7):637–644
KDOQI Clinical Practice Guideline for Hemodialysis Adequacy (2015) 2015 update. Am J Kidney Dis 66(5):884–930
Clinical practice guidelines for hemodialysis adequacy, update 2006. Am J Kidney Dis. 2006;48 Suppl 1:S2-90.
Hahn D, Hodson EM, Fouque D (2020) Low protein diets for non-diabetic adults with chronic kidney disease. Cochrane Database Syst Rev 10(10):CD001892. https://doi.org/10.1002/14651858.CD001892.pub5. (PMID: 33118160)
Ikizler TA, Burrowes JD, Byham-Gray LD, Campbell KL, Carrero JJ, Chan W et al (2020) KDOQI clinical practice guideline for nutrition in CKD: 2020 update. Am J Kidney Dis 76(3):S1-107
Hendra H, Sridharan S, Farrington K, Davenport A (2022) Determinants of active energy expenditure in haemodialysis patients. Clin Physiol Funct Imaging 42(5):303–307
Khatri P, Davenport A (2024) Dialysis for older adults: why should the targets be different? J Nephrol. https://doi.org/10.1007/s40620-023-01835-1. (PMID: 38180729)
Funding
No external funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interest
None.
Ethical approval
Not applicable, no patient data.
Informed consent to participate
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Butt, U., Davenport, A., Sridharan, S. et al. A practical approach to implementing incremental haemodialysis. J Nephrol (2024). https://doi.org/10.1007/s40620-024-01939-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s40620-024-01939-2