
Abstract
In 2013, the Italian Society of Nephrology joined forces with Nephrocare-Italy to create a clinical research cohort of patients on file in the data-rich clinical management system (EUCLID) of this organization for the performance of observational studies in the hemodialysis (HD) population. To see whether patients in EUCLID are representative of the HD population in Italy, we set out to compare the whole EUCLID population with patients included in the regional HD registries in Emilia-Romagna (Northern Italy) and in Calabria (Southern Italy), the sole regions in Italy which have systematically collected an enlarged clinical data set allowing comparison with the data-rich EUCLID system. An analysis of prevalent and incident patients in 2010 and 2011 showed that EUCLID patients had a lower prevalence of coronary heart disease, peripheral vascular disease, heart failure, valvular heart disease, liver disease, peptic ulcer and other comorbidities and risk factors and a higher fractional urea clearance (Kt/V) than those in the Emilia Romagna and Calabria registries. Accordingly, survival analysis showed a lower mortality risk in the EUCLID 2010 and 2011 cohorts than in the combined two regional registries in the corresponding years: for 2010, hazard ratio (HR) EUCLID vs. Regional registries: 0.80 [95% confidence interval: 0.71–0.90]; for 2011, HR: 0.76 [0.65–0.90]. However, this difference was nullified by statistical adjustment for the difference in comorbidities and risk factors, indicating that the longer survival in the EUCLID database was attributable to the lower risk profile of patients included in that database. This preliminary analysis sets the stage for future observational studies and indicates that appropriate adjustment for difference in comorbidities and risk factors is needed to generalize to the Italian HD population analyses based on the data-rich EUCLID database.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Patient-oriented research [1] is a research area considered as an absolute priority by patients, health managers, health authorities and scientific societies alike. This research area encompasses observational (non-experimental) studies in the clinical scenario and general population-based studies and can be based on high quality clinical data-bases [2] or on a planned collection of specific (primary) data at community level. Over the last 20 years, major efforts have been made to establish end-stage renal disease (ESRD) and chronic kidney disease (CKD) research databases to promote patient-oriented research [3]. These databases offer great prospects for exploratory etiologic research and for prognostic studies and are precious also for comparative effectiveness studies aimed at investigating the efficacy of drug treatments prescribed to CKD and ESRD patients [4]. The success of these databases in fostering renal research is indisputable and this open, transparent scenario is expected to accelerate advancement in knowledge in clinical research in the medium term [5]. The European Renal Association − European Dialysis and Transplant Association (ERA-EDTA) registry and the national registers contributing to the main European registry are the most important sources of epidemiological information on dialysis and transplantation in Europe but these registries include very limited clinical information, e.g. the ERA-EDTA registry does not provide information about blood pressure or the main biochemical parameters or somatometric data, i.e. data of obvious relevance. The European Clinical Database (EuCliD)® was created by Fresenius Medical Care to monitor a large series of clinical indicators in dialysis centers of the European dialysis network of this provider [6]. In Italy, renal replacement therapy (RRT) is mainly managed in the public sphere, with over 600 public dialysis centers and a global dialysis population of 40,000 patients [7]. Within Italy, the Nephrocare network treats about 1,500 patients and Nephrocare centers are present in only five regions: there are 7 centers in Lombardy, 6 in Lazio, 20 in Campania, 4 in Puglia and 2 in Sicily [8].
In 2013, Nephrocare-Italy joined forces with the Italian Society of Nephrology to create an observational database including patients on file in EuCliD to allow interested investigators to carry out original clinical research, and the database was successfully established the following year. To see whether the population in this database is representative of the whole dialysis population in Italy, we compared the Nephrocare dialysis population with the population treated in public hospitals in Italy. We focused on two regions, namely Emilia-Romagna in Northern Italy and Calabria in Southern Italy, as these are the sole regions among the nineteen Italian regions which, since the inception of the registries, have systematically collected an enlarged clinical data set including standard risk factors and clinical indicators so allowing a comparison of the risk profile of these dialysis patients with that of patients in the large clinical data set of EuCliD. Herein we report the comparison of the Nephrocare population with that from the two regional registries in Italy.
Materials and methods
The protocol conformed with the ethical guidelines of our institution. Because we used standard aggregated registry data, no written informed consent was required from participants.
Study populations
This study was based on data of prevalent and incident patients (index dates: 2010 and 2011) of dialysis registries of Calabria and Emilia Romagna and on data from EuCliD. The Calabria Registry of Dialysis and Transplantation (CREDIT) and the Registro Emiliano Romagnolo di Dialisi e Trapianto (RER-DT) were both established in 1994. These regional registries are affiliated with the Italian and the ERA-EDTA registries, and core data (collected once a year, at 31st December) for these regions coincide with those requested by the national and European registries. Furthermore, both regional registries collect information on comorbidities, anthropometry and other data driven by specific research projects. Both in Calabria and in Emilia-Romagna, data collection is performed via an identical web-based platform (REGDIAL©, Traccia, Matera, Italy). The Italian Nephrocare cohort includes all patients, extracted from the EuCliD platform, on treatment in the 35 Nephrocare dialysis centers at the same index dates of data collection in the two regional registries (see above). Patients in this cohort received the first dialysis treatment either in a Nephrocare center or in a public dialysis facility of the Italian health system and transferred to Nephrocare once stabilized.
Statistical methods
Demographic and clinical data in the two regional registries and in Nephrocare Italy are summarized as mean (continuous variables) or percentage (binary variables) and 95% confidence intervals (CI), and comparisons between the two groups were made by Student’s t-test, Mann–Whitney test, or Chi square test (with and without continuity correction), as appropriate. The incidence rate of mortality (and 95% CI) was calculated by considering two index dates (2010 and 2011) and compared between the two cohorts (EuCliD vs. regional registries) by univariate and multivariate Cox regression analyses. In multivariate Cox models we adjusted for age, gender, and diabetes, as well as for all relevant comorbidities differing between the EuCliD and the two regional registries’ cohorts, i.e. hypertension, liver disease, peptic ulcer, peripheral vascular disease, heart failure, chronic obstructive pulmonary disease (COPD), and valvular heart disease. In the Cox models, data were expressed as hazard ratio (HR), 95% CI and p value. Data analysis was performed by SPSS for Windows (Version 22), Chicago, Illinois, USA.
Results
The number of patients included in the two Italian regional registries and in the EuCliD database at the two index dates (2010 and 2011) are detailed in Table 1. The Emilia Romagna Registry included the highest number of prevalent and incident patients (n = 2917 and n = 661, respectively), these figures being about 3 times higher than those in Calabria and twice as high as those of the EuCliD database. The main demographic, clinical and biochemical data in these registries and in EuCliD are detailed in Table 2 and Appendix A (prevalent patients), and in Table 3 and Appendix B (incident patients).
Prevalent dialysis patients
In the index years 2010 (Table 2a) and 2011 (Table 2b), prevalent patients included in EuCliD did not materially differ from those included in Calabria and Emilia Romagna registries concerning demographic and anthropometric variables (age, proportion of males and body mass index [BMI]), dialysis vintage, or serum albumin. Among primary renal disease, hypertensive nephrosclerosis was less frequent in Calabria and diabetic nephropathy less frequent in Emilia Romagna. Hemoglobin was higher and serum phosphate lower in the EuCliD database patients, while serum calcium was lower in the Emilia Romagna registry than in the other two databases and parathormone (PTH) was higher in the Calabrian registry. Serum lipids (total cholesterol, high-density lipoprotein [HDL] cholesterol, and triglycerides), diabetes and background cerebrovascular disease were comparable in the three cohorts. The prevalence of coronary heart disease was higher in Emilia Romagna than in EuCliD, and heart failure, peripheral vascular disease and liver disease were all much more common in the Emilia Romagna and Calabria registries than in EuCliD both in 2010 and 2011, whereas fractional urea clearance (KT/V) was consistently higher in EuCliD than in the two regional registries (Table 2a, b). Of note, the prevalence of hypertension did not differ between EuCliD and the Calabria registry but it was coherently lower across the two index-years in the Emilia Romagna registry than in the other two cohorts (Table 2a, b).
As shown in Appendix A, COPD was higher in prevalent patients in the Calabria registry than in those of Emilia Romagna or the EuCliD database, and this was true both in 2010 and 2011. Dementia, valvular heart disease, peptic ulcer disease and metastatic cancers were more frequent in the Emilia Romagna and Calabria registries than in EuCliD (Appendix A).
Incident dialysis patients
The analysis of data of incident patients, both for 2010 (Table 3a) and 2011 (Table 3b), showed that patients in the two regional registries were quite similar concerning age, proportion of males and dialysis vintage and substantially confirmed the differences observed among prevalent patients. The proportion of hypertensive patients was consistently higher in EuCliD than in the Calabria and Emilia Romagna registries, whereas diabetic patients were more frequent in the Calabria and Emilia registries than in EuCliD. The proportion of patients with a history of liver disease, peripheral vascular disease and heart failure was higher in the Calabria and Emilia Romagna registries than in EuCliD. In 2010 and in 2011, the Emilia Romagna registry had the highest proportion of patients with coronary artery disease (Table 3a, b). In 2010, no difference was observed among the two regional registries and the EuCliD database concerning the proportion of patients with cerebrovascular disease, whereas in 2011 this comorbidity tended to be lower in EuCliD (9%) than in the other two regional registries (Calabria: 12%; Emilia Romagna: 13%). KT/V was consistently higher in EuCliD than in the other two registries both in 2010 and 2011. In parallel with data observed in prevalent patients, COPD was higher in incident patients included in the regional registries than in the EuCliD database (Appendix B). The proportion of patients with acquired immunodeficiency syndrome (AIDS), dementia, valvular heart disease, peptic ulcer, and metastatic cancers was more frequent in the regional registries than in EuCliD (Appendix B). Of note, both in 2010 and 2011, the large majority of patients (90.4 and 93.0%, respectively) were admitted to Nephrocare centers within 1 month of starting chronic dialysis.
Survival analysis
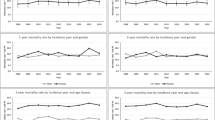
In the 2010 EuCliD cohort, 227 patients out of 1556 died over a 2-year follow-up period (13 deaths per 100 person-years [95% CI: 11–14]) and this death rate was lower than the corresponding death rate in Calabria: 767 out of 2917 patients (16 deaths per 100 person-years [95% CI: 15–18]), and in Emilia Romagna: 365 out of 1302 patients (15 deaths per 100 person-years [95% CI: 14–17]). The same analysis in the 2011 cohorts confirmed a lower mortality rate in the EuCliD cohort than in the two renal registries: EuCliD: 191 deaths among 1745 patients (12 deaths per 100 person-years [95% CI: 10–14]); Calabria: 195 deaths among 1290 patients (16 deaths per 100 person-years [9 5% CI: 14–19]); Emilia Romagna: 433 deaths among 2998 patients (16 deaths per 100 person-years [95% CI: 14–17]).
In unadjusted analyses, comparing the data for 2010 (EuCliD vs. Regional registries: HR 0.80 [95% CI: 0.71–0.90]) and 2011 (HR: 0.76 [0.65–0.90]), the death risk was 20% and 24% lower in the EuCliD cohort than in the regional registries (p < 0.001). However, the reduced death risk in the EuCliD cohort became of similar magnitude (2010 HR: 0.97 [0.84–1.13], p = 0.71; 2011 HR: 0.99 [0.81–1.21], p = 0.94) after adjustment for age, gender, diabetes as well as for all relevant comorbidities differing between the EuCliD and the two regional registries cohorts (hypertension, hepatopathy, peptic ulcer, coronary heart disease, peripheral vascular disease, heart failure, COPD, and valvulopathy), indicating that the higher burden of comorbidities and risk factors in large part explains the difference in mortality risk between the EuCliD and the two regional registries cohorts.
Discussion
The comparison of the demographic and clinical profile of the hemodialysis population of two public hospital-based regional dialysis registries with the corresponding data from the largest private hemodialysis network in Italy shows substantial similarities in demography and in the clinical parameters but a slightly higher proportion of high risk patients in the two dialysis registries than in the private network. This difference accounted for a modest difference in mortality across the public and the private networks in Italy. Overall findings in this survey show that the EuCliD clinical database adequately reflects the dialysis population in Italy and this sets the basis for future collaborative studies between the Italian Dialysis Registry and the largest clinical database of patients on regular dialysis treatment in the largest private network in Italy.
In the ‘80 s the Editors of the New England Journal of Medicine made the point that private for-profit health care delivery can perhaps provide a more efficient service to patients than not-for-profit organizations [9]. However, reservations of various kinds have been expressed about this tenet, particularly the fact that for-profit facilities may privilege shareholder returns over patients’ interests [10]. The issue was hotly debated and the concern was raised that mortality may be higher in for-profit hemodialysis facilities than in not-for profit organizations delivering the same treatment [11], a possibility which was confirmed in a meta-analysis by Devereaux et al. [12]. These considerations are of obvious relevance when setting up a collaborative effort between a for-profit dialysis provider like Nephrocare and a scientific society like the Italian Society of Nephrology that maintains a registry based mainly on not-for profit, public hospitals and dialysis centers. In this preparatory analysis, we found that the risk profile of patients in Nephrocare, although presenting a high burden of cardiovascular and non-cardiovascular comorbidities, was less severe than that in the Calabria and Emilia regional registries. Indeed, among prevalent and incident patients, peripheral vascular disease, heart failure and liver diseases and other comorbidities like dementia were higher in Emilia Romagna and Calabria than in EuCliD, and EuCliD patients had a higher Kt/V and a higher proportion of hypertensive patients than the regional registries. Along with the lower comorbidities burden, EuCliD patients had a 20–24% lower mortality risk than patients in the two regional registries. The smaller comorbidity burden in EuCliD patients in large part accounted for the lower mortality risk in these patients because appropriate adjustment for relevant comorbidities which differed between EuCliD and regional registries substantially reduced the difference in the death risk between these populations, which became largely non-significant. Another reason that could explain the better survival of Nephrocare patients might be that part of incident patients in this network are transferred to this network after disease stabilization in dialysis centers in public hospitals in Italy, suggesting that fragile patients with high early mortality [13] may be less represented in the Nephrocare network. Thus, the present survey and the associated cohort study suggest that future studies utilizing the EuCliD database may provide results generalizable to the Italian dialysis population provided that differences in baseline comorbidities with the Italian regional registries are appropriately accounted for in the same database. EuCliD is a data-rich database and this may make it possible to carry out prognostic studies and comparative effectiveness studies looking at various clinical end-points. As an example of the potential relevance of a collaboration between this database and that of the Italian Society of Nephrology, we have planned to validate in Italian hemodialysis patients—both from the EuCliD database and the two regional registries—a calculator of the risk of death in the dialysis population developed by investigators of the ARO cohort (a large cohort of European hemodialysis patients on treatment in the Fresenius dialysis network) which was externally validated in the Dialysis Outcomes and Practice Patterns Study (DOPPS) cohort [14]. Risk calculators of the kind are important not only for prognostic purposes but also for modelling the dynamics of the dialysis population at regional and national level. The accurate information about drug treatments administered to hemodialysis patients in the EuCliD database will provide an important opportunity for exploring the effectiveness of these treatments in ESRD patients and will provide relevant knowledge to refine clinical policies aimed at improving clinical outcomes in the scenario of hemodialysis patients in Italy.
A limitation of this study is the variability in demography and comorbidities among regional registries in Italy. In other words, data in the Emilia Romagna and Calabria registries may not perfectly reflect the composition and the risk profile of the overall Italian dialysis population. In conclusion, this comparative study between a for-profit hemodialysis network in Italy based on a data-rich clinical database (EuCliD) and two regional registries of the Italian Society of Nephrology shows that the risk profile of patients on treatment in this for-profit network is less severe than that in two regional registries of the Italian Society of Nephrology, and this difference almost entirely accounts for the lower mortality in the EuCliD database. Thus, it is reasonable to assume that future analyses on this data-rich database will be generalizable to the Italian hemodialysis population provided that appropriate adjustment is made for differences in comorbidities between EuCliD patients and patients treated in public hospitals in Italy.
References
Laine C, Davidoff F (1996) Patient-centered medicine. A professional evolution. JAMA 275:152–156
Zoccali C (2001) The importance of large, high quality clinical databases in nephrology. J Nephrol 14:89–93
Shlipak M, Stehman-Breen C (2005) Observational research databases in renal disease. J Am Soc Nephrol 16:3477–3484
Winkelmayer WC, Liu J, Kestenbaum B (2011) Comparative effectiveness of calcium-containing phosphate binders in incident U.S. dialysis patients. Clin J Am Soc Nephrol 6:175–183
Chang TI, Winkelmayer WC (2012) Comparative effectiveness research: what is it and why do we need it in nephrology? Nephrol Dial Transplant 27:2156–2161
Marcelli D, Kirchgessner J, Amato C et al (2001) EuCliD (European Clinical Database): a database comparing different realities. J Nephrol 14(Suppl 4):S94–S100
Alloatti S, Strippoli GF, Buccianti G et al (2008) Current structure and organization for renal patient assistance in Italy. Nephrol Dial Transplant 23:1323–1329
http://www.nephrocare.com/dialysiscentres.html?tx_fkclinicfinder_pi1%5Bloc%5D = 5&cHash = d28b0432d290402e4408b7281bac1d83. Accessed 6 May 2016
Relman AS, Rennie D (1980) Treatment of end-stage renal disease: free but not equal. N Engl J Med 303:996–998
Woolhandler S, Himmelstein DU (1999) When money is the mission–the high costs of investor-owned care. N Engl J Med 341:444–446
Nissenson AR, Owen WF (2000) Ownership of dialysis facilities and patients’ survival. N Engl J Med 342:1054-5-6
Devereaux PJ, Schünemann HJ, Ravindran N et al (2002) Comparison of mortality between private for-profit and private not-for-profit hemodialysis centers: a systematic review and meta-analysis. JAMA 288:2449–2457
Nordio M, Limido A, Maggiore U et al (2012) Survival in patients treated by long-term dialysis compared with the general population. Am J Kidney Dis 59:819–828
Floege J, Gillespie IA, Kronenberg F et al (2015) Development and validation of a predictive mortality risk score from a European hemodialysis cohort. Kidney Int 87:996–1008
Acknowledgements
Collaborators for the Calabrian and Emilian Dialysis and Transplantation Registries Workgroups
Andreoli D., Ascoli G., Barreca E., Bovino M., Bruzzese V., Candela V. (deceased), Caruso F., Chiarella S., Cianfrone P., D’Agostino F., D’Anello E., Ferrari L., Figoli D., Fornaciari C., Franco C., Galati D., Grandinetti F., Gullo M., Lo Gozzo D., Lucisano S., Mancuso F., Mannino M.L., Marsico M.L., Martire V., Mazza G., Mazza B., Mellace A., Messina A., Pisani A., Plutino D., Policastro M., Pugliese A., Reina A., Santangelo M., Sapio C., Scicchitano R., Sellaro A., Tramontana D., Vardè C., Zingone F.
Collaborators for the Emilian Dialysis and Transplantation Registries Workgroups
Dalmastri V., Rapanà R., Giovannone C., Giudicissi A., Russo G., Zambianchi L., Lucchi L., David S., Gerra D., Ballocchi S., Isola E., Stefani A., Flachi M., Mencarelli F.
Author contributions
The proposal of of a joint effort for creating a shared data base for clinical research in the Italian dialysis population was originally formulated by A Di B, SS, FC (by Nephrocare and Fresenius Medical Care) and GBC (President of the Italian Society of Nephrology in 2013–2014) who then involved AS and CZ into the project. All these investigators contributed to the planning of the present study. MP,CA, PC, CM and AV assembled and validated the study database. GD and GT made the statistical analysis and MP,CA, EA and PC callaborated into this analysis. MP, GT and CZ prepared the first draft of the paper which was then revised and integrated by AS and SS and the final version was read and approved by all investigators.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflict of interest
CA, PC and SS are Fresenius Medical Care employees, AdiB and FC are Nephrocare Italy employees. The other authors have no conflict to declare.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
No written informed consent was required from participants, because standard aggregated registry data were used.
Additional information
Collaborators of the Calabrian and Emilian Dialysis and Transplantation Registries Workgroups are listed in “Acknowledgment”.
Rights and permissions
About this article

Cite this article
Postorino, M., Amato, C., Mancini, E. et al. A comparative study of the risk profile of hemodialysis patients in a for profit network and in two regional registries of the Italian Society of Nephrology. J Nephrol 31, 119–127 (2018). https://doi.org/10.1007/s40620-016-0372-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40620-016-0372-8