
Abstract
Background
Fluid accumulation may delay recognition of acute kidney injury (AKI) in intensive care unit (ICU) patients. This study aims to evaluate the impact of fluid balance on the incidence, time of AKI diagnosis and predictive performance for outcomes of critically ill patients.
Methods
This study included a cohort of 7696 adult ICU patients at Mayo Clinic Hospital in year 2011 with at least one serum creatinine (SCr) measured in ICU. AKI was defined based on SCr criterion for stage I of KDIGO definition. The AKI incidence and predictive performance for 60-day mortality was compared before and after SCr adjustment for fluid balance.
Results
AKI was detected in 1860 (24.2 %) before and 1947 (25.3 %) after fluid balance adjustment (P < 0.001). Patients with AKI both before and after SCr adjustment had significantly higher 60-day mortality in comparison with patients who did not develop AKI (OR 3.38; 95 % CI 2.84–4.02). The risk of 60-day mortality in patients who met AKI criteria after but not before SCr adjustment was significantly higher than patients without AKI (OR 2.00; 95 % CI 1.25–3.11). In contrast, the risk of 60-day mortality in patients who met AKI criteria before but not after SCr adjustment was similar to patients without AKI (OR 1.19; 95 % CI 0.48–2.50). The C-statistic for unadjusted and adjusted SCr to predict 60-day mortality were 0.68 and 0.70, respectively (P = 0.001).
Conclusion
Our study found that SCr adjustment for fluid balance could result in a more accurate detection of AKI cases. We suggest using fluid balance adjustment for volume overload critically ill patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Acute kidney injury (AKI) is a frequent clinical syndrome encountered in hospitalized and particularly in critically ill patients. Using the Kidney Disease, Improving Global Outcomes (KDIGO) definition for AKI [1], 1 in 5 adults worldwide experience AKI during hospitalization. In addition, the incidence of AKI occurring in patients admitted to intensive care units (ICUs) ranges from 30 to 60 % [2]. Studies have demonstrated that AKI is independently associated with both short and long-term mortality [3–6]. AKI-related mortality was reported to be as high as 23 % [7].
The KDIGO definition of AKI is based on absolute or relative changes in serum creatinine (SCr) and weight-adjusted hourly urine output, respectively. This definition has been validated to standardize the diagnosis and staging the severity of AKI [8, 9].
Serum creatinine as a surrogate marker of kidney function holds some limitations when it is used for the AKI diagnosis. Recent studies have demonstrated the dilutional effects of fluid accumulation on SCr [10, 11]. Since volume overload is very common, especially in perioperative and ICU settings [12], diluting and masking SCr increments can lead to a delay in AKI diagnosis in critically ill patients [13, 14]. Moreover, SCr dilution during fluid resuscitation may result in underestimation of the AKI severity [14]. The effect of SCr adjustment for fluid balance in early diagnosis and staging of AKI and its impact on the AKI definition predictive ability for mortality outcome in a large cohort of critically ill patients are not very well known.
This study aims (1) to evaluate and compare the incidence of AKI diagnosis and staging according to SCr criterion of KDIGO definition, before and after SCr adjustment for fluid balance and (2) to investigate the predictive performance of AKI definition for 60-day mortality in critically ill patients before and after fluid balance SCr adjustment.
Materials and methods
Study population
This was a single-center retrospective study conducted at a tertiary referral hospital. We studied all adult patients (age ≥18 years) admitted to the intensive care units (ICUs) at Mayo Clinic Hospital, Rochester, MN from January 1 to December 31, 2011. We included patients who had at least one SCr measured in the ICU. Patients with a history of stage 5 chronic kidney disease or end-stage renal disease (ESRD), patients who received any dialysis modalities within 14 days prior to the ICU admission and patients who did not provide research authorization were excluded from the study. Stage 5 chronic kidney and ESRD disease were identified based on ICD-9 code assignment, or based on estimated glomerular filtration rate (eGFR) of <15 ml/min/1.73 m2. The local Institutional Review Board approved this study.
Data collection
Clinical characteristics, demographic information, and laboratory data were collected using manual and automated retrieval from institutional electronic medical records. The baseline SCr was defined as the minimum SCr measured within 6 months before the index admission. If outpatient SCr was not available, the first SCr measured at hospital admission was used. The eGFR was derived by using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation [15]. Chronic kidney disease (CKD) was defined as a calculated eGFR <60 ml/min/1.73 m2. The severity of illness at ICU admission was evaluated using the Acute Physiology and Chronic Health Evaluation (APACHE) III score [16], and Sequential Organ Failure Assessment (SOFA) score [17]. Admission weight was measured within 24 h of ICU admission, using digital weight scale. The cumulative fluid balance was defined as the difference in total fluid intake and output starting from ICU admission. The fluid balance at the time of each SCr measurement was calculated and used for SCr adjustment.
Assessment of AKI using serum creatinine before and after adjustment of fluid balance
We identified and staged AKI solely based on the SCr criterion of the KDIGO definition [1]. AKI was defined as an increase in SCr in the ICU of ≥0.3 mg/dL or relative change of ≥50 % from the baseline. The AKI diagnosis time was defined as the time of the first SCr to meet SCr criterion. We repeated diagnosis and staging of AKI before and after adjusting each SCr for fluid balance. The following formula was used to adjust SCr for fluid balance [13, 14].
when correction factor = 1 + [cumulative fluid balance (L)/(admission body weight (kg) × 0.6)].
Clinical outcomes
The primary outcome was all-cause mortality at 60 days following the index ICU admission. We reviewed all patients’ vital status by reviewing registration and electronic medical records. In patients whose vital status at 60 days after ICU admission was unknown, the Social Security Death Index was used [18].
Statistical analysis
All continuous variables were reported as medians with interquartile ranges (IQR). All categorical variables were reported as counts with percentages. In the event of missing information, data was not imputed. For patients with multiple ICU admissions, only the first ICU admission during the study period was included in the analysis. The difference in the AKI diagnosis based on SCr before and after adjustment for fluid balance was assessed using a McNemar’s test. The difference in the time-to-AKI diagnosis based on adjustment of SCr was assessed using a paired t test. The agreement of AKI diagnosis and staging before and after SCr adjustment was assessed using Cohen’s weighted kappa coefficient with linear weight between AKI stages. According to the result of AKI diagnosis before and after SCr adjustment, we classified patients into 4 groups: (1) patients who had AKI both before and after SCr adjustment, (2) patients who had AKI after but not before SCr adjustment, (3) patients who had AKI before but not after fluid adjustment and (4) patients who did not have AKI both before and after fluid adjustment. We adjusted odd ratios (ORs) for pre-specified confounders, including age, ICU type, APACHE III scoreand fluid balance in ICU to assess 60-day mortality among the first three groups using the last group as a reference group. The association between AKI stages and 60-day mortality was assessed using a logistic regression analysis. The predictive performance of the SCr criterion, based on SCr adjustment, for 60-day mortality was assessed by C-statistics; after which we compared their performances using DeLong’s test. We performed the subgroup analysis based on ICU type and tertile of total fluid balance in ICU. A two-sided P value of <0.05 was considered statistically significant. All analyses were performed using JMP statistical software (version 9.0, SAS, Cary, NC).
Results
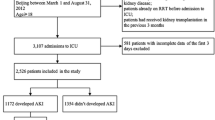
During the study period, 9277 critically ill patients were admitted to the ICU. Of these, 1581 were excluded: 532 had ESRD, or received dialysis within 14 days prior to ICU admission, 498 had no research authorization, 194 aged <18 years, and 357 had no measured SCr values in the ICU. A total of 7696 patients were analyzed. The clinical characteristics of these patients at the ICU admissions and their outcomes are summarized in Table 1. The median age was 65 years (IQR 55–77); 58 % were men and 27 % had CKD. The median fluid balance in ICU was 1515 ml (IQR −96 to 3770).
AKI diagnosis and staging before and after adjustment for fluid balance
Using unadjusted SCr, AKI occurred in 1860 (24.2 %) of the patients, with 16.6, 4.2, and 3.4 % in maximum AKI stage 1–3, respectively. Using adjusted SCr for fluid balance, AKI occurred in 1947 (25.3 %) patients with 16.7, 4.6, and 4.0 % in maximum AKI stage 1–3, respectively. Accordingly, using adjusted SCr for fluid balance, more AKI cases were identified in comparison with unadjusted SCr (P < 0.001) (Table 2).
The percentage agreement for AKI diagnosis, using the SCr before and after adjustment for fluid balance methods, was 96.6 % with a kappa of 0.91 (95 % CI 0.90–0.92). Results show that unadjusted and adjusted SCr for fluid balance both agreed in 1773 AKI cases and 5662 non-AKI cases. Using unadjusted SCr and adjusted SCr resulted in a discrepancy in AKI diagnosis in 261 cases (3.4 %). Of these 261 patients, 87 cases met the AKI diagnosis by using unadjusted SCr, but not adjusted SCr and 174 met AKI diagnosis by using adjusted SCr, but not unadjusted SCr. The percentage agreement for AKI staging, using unadjusted and adjusted SCr for fluid balance, was 94.9 % with a kappa of 0.91 (95 % CI, 0.90–0.92).
Time-to-AKI diagnosis before and after adjustment for fluid balance
We found 1773 patients developed AKI regardless of SCr adjustment for fluid balance. Adjustment did not change the time of AKI diagnosis in 1591 (90 %), expedited it in 132 (7 %), and delayed it in 50 (3 %) patients. Using adjusted SCr detect AKI significantly earlier than using unadjusted SCr with the mean difference in time-to-diagnosis of 1.5 h (95 % CI 0.6–2.4).
Risk for 60-day mortality
Of the total cohort, 10 % (n = 737) died within 60 days after ICU admission. The 60-day mortality rates after ICU admission for AKI stages by using SCr before and after adjustment for fluid balance are shown in Fig. 1. Compared to the reference group (patients without AKI both before and after SCr adjustment), the risk of 60-day mortality in patients with AKI both before and after SCr adjustment was significantly higher (OR 3.38; 95 % CI 2.84–4.02). Similarly, the risk of 60-day mortality in patients who met AKI criteria after but not before SCr adjustment was significantly increased in comparison with patients without AKI (OR 2.00; 95 % CI 1.25–3.11). In contrast, the risk of 60-day mortality in patients who met AKI criteria before but not after SCr adjustment was similar to patients without AKI (OR 1.19; 95 % CI 0.48–2.50) (Table 3; Fig. 2). The C-statistic for unadjusted and adjusted SCr to predict 60-day mortality were 0.68 and 0.70, respectively (P = 0.001).

60-day mortality rate according to acute kidney injury (AKI) stages (SCr definition)

Odds ratio of 60-day mortality in patients with or without acute kidney injury before and after SCr adjustment for fluid balance
Subgroup analysis
The clinical characteristics and outcomes of patients admitted in medical and surgical ICUare summarized in Supplemental Table 1. The subgroup analysis in medical and surgical ICU suggested SCr adjustment might impact the AKI diagnosis more in surgical ICU than medical ICU (Supplemental Table 2). There was no significant difference in AKI diagnosis before and after SCr adjustment in medical ICU (29.0 vs. 29.3 %, respectively; P = 0.49). There was significant difference in AKI diagnosis before and after adjustment in surgical ICU (19.6 vs. 21.6 %, respectively; P < 0.001). This may be due to higher total fluid balance in surgical ICU in comparison with medical ICU (2.8 vs. 1.8 L; P < 0.001). However, the use of adjusted SCr in AKI diagnosis improved the predictive performance of AKI for 60-day mortality in both medical and surgical ICU.
The subgroup analysis of fluid overload tertiles demonstrated the impact of SCr adjustment in AKI diagnosis in groups of patients with extreme negative or positive fluid balance (tertile 1 and 3) is more prominent (Supplemental Table 3).
Discussion
We report a large historical cohort study to investigate the effect of SCr values, before and after adjustment for fluid balance, on epidemiology and prognostication performance of AKI definition based on KDIGO SCr criterion. This study demonstrated that using SCr adjustment could result in early detection of more AKI cases. In addition, SCr adjustment increased the accuracy of AKI-related 60-day mortality prediction. Under-recognized AKI due to fluid overload allows underestimation of high mortality in these patients. The SCr adjustment should be done in critically ill patients, especially in those with fluid overload particularly following massive volume resuscitation.
In an ICU setting, even a modest degree of renal injury is associated with increased in-hospital mortality [19–21]. Despite all efforts to identify the potential treatment options for AKI, prevention in at risk patients and early diagnosis of AKI still remain the main intervention to minimize further insult [22]. The limitations of SCr for AKI diagnosis are well known, since it is influenced by several variables including age, gender, muscle mass (amputation, malnutrition, muscle wasting), diet and certain medications that inhibit tubular creatinine secretion [22, 23]. Fluid resuscitation in perioperative and ICU settings is commonly utilized and it can certainly result in expanded volume of distribution of SCr and therefore its dilution.
Recently, Englberger et al. demonstrated the dilution of SCr was common within 48 h in patients after cardiac surgery with cardiopulmonary bypass [24]. In this cohort, subsequent increase in SCr were not found to be from the baseline SCr, but rather it was due to rebound increase from diluted SCr following resolution of fluid overload. Ho et al. recently conducted a study in 350 elective cardiac surgery patients and found SCr level increase of ≥10 % (<6 h postoperative) was associated with higher AKI risk [25]. Masked increase in SCr by fluid resuscitation could alleviate SCr ability to predict AKI development.
There is growing body of literature that indicates fluid accumulation can lead to the incorrect diagnosis of AKI. Macedo et al. [14], conducted a prospective cohort study in 253 critically ill patients to evaluate the effect of fluid balance on SCr and staging of AKI severity. They found 25 % of patients had delayed AKI diagnosis due to volume overload. In 9.5 % of patients, delayed diagnosis was ≥48 h. In their study, there was no difference in mortality following SCr adjustment (40 vs. 35 %, P = 0.45). Our current study conducted in the larger cohort of 7696 patients in ICUs (both medical and surgical). We confirmed that SCr adjustment could detect more AKI cases and earlier. However, the mean difference in time-to diagnosis of AKI after SCr adjustment in our study was only 1.5 h (95 % CI 0.6–2.4). The median cumulative positive fluid balance during ICU admission in our study was lower [1.5 L (IQR, 0–3.8)] than the median cumulative fluid balance of 6.5 L (IQR, 1.1–11.3) in the study by Macedo et al. [14]. This potentially explains the less delayed AKI diagnosis time.
Our study also successfully demonstrated a higher predictive performance of the AKI definition for 60-day mortality following SCr adjustment. The PICARD study demonstrated that in patients with AKI, fluid overload itself was independently associated with mortality [26]. Accordingly, we adjusted for fluid balance when we assessed the impact of SCr adjustment for fluid balance in AKI diagnosis on 60-day mortality prediction. The post hoc analysis of patients with acute lung injury enrolled in FACTT study [13] similarly showed that the mortality was similar among patients who met AKI diagnosis before or after adjustment and patients who met AKI diagnosis only after adjustment for fluid balance. Mortality was significantly lower in patients who met AKI diagnosis before, but not after SCr adjustment. Our study not only included patients with acute lung injury, we found the same relationship in all critically ill patient population.
There are several limitations to our study. First, this report is a retrospective study and inherently subjective to biases related to its design. By enrolling a very large cohort, we have attempted to mitigate these potential biases. The benefit and feasibility of adjusting SCr for fluid balance in the diagnosis of AKI need to be further studied in non-ICU setting as fluid overload is less common in non-ICU patients and data regarding daily weight and fluid intake and output are easily available nor well documented in hospital floor. Second, we did not include urine output criterion for AKI diagnosis, since an indwelling urinary catheter was not used to obtain accurate hourly urine output data for large percentage of patients in our cohort. Third, we disregarded fluid balance prior to ICU admission due to limited data and potentially imprecise record of fluid balance outside the ICUs. As our ED boarding time is very short, we believe the positive fluid balance prior to ICU admission may not be a significant factor. Fourth, our study focused on SCr dilution effect of on AKI diagnosis and staging. We did not take etiology of AKI and types of fluid into account (blood, colloid or crystalloid). Septic AKI had different pathophysiology, clinical characteristics and outcomes from non-septic AKI [27, 28]. In addition to renal ischemia, inflammation and apoptosis have implicated in pathogenesis of septic AKI. Septic AKI can occur in hemodynamically stable patients. Differences in the volume of distribution among each fluid type could potentially affect the changes in SCr in the intravascular space. In addition, chloride-rich intravenous fluid administration may have potentially contributed to some degrees of AKI [29]. Accordingly, the inclusion of AKI etiology as well as fluid type in SCr adjustment might improve accuracy of AKI diagnosis. However, adjustment for fluid balance regardless of AKI etiology and fluid type in our study is simple and likely practical in the practice. Lastly, we did not measure injury biomarkers of AKI. It would be of interest to confirm these results in a further study of critically ill patients using established early urine biomarkers of tubular injury not modulated by fluid balance including neutrophil gelatinase-associated lipocalin (NGAL) [30], renal liver-type fatty acid-binding protein (L-FABP) [31], kidney injury molecule-1 (KIM-1) [32], cell cycle arrest biomarkers [33] for the AKI diagnosis. This would potentially provide more insight into our conclusions.
Notwithstanding these limitations, our study carries some strength as well. It is the largest cohort of patients in medical and surgical ICUs with different critical illnesses. Moreover, we adjusted every SCr value with accumulative fluid balance during ICU admission. Therefore, the findings from our study can be generalized to patients in both medical and surgical ICUs with available recorded fluid balance.
In summary, fluid management in the ICU influences SCr and the diagnosis of AKI using SCr-based definition. Using SCr adjustment not only increases its sensitivity and allows earlier diagnosis of AKI, it also provides higher predictive performance of the AKI definition for 60-day mortality when compared with unadjusted SCr method. Based on our data, we strongly suggest using fluid balance adjustment for critically ill patients with volume overload.
References
KDIGO AKI Work Group (2012) KDIGO clinical practice guidelines for acute kidney injury. Kidney Int suppl 2:1–138
Srisawat N, Kellum JA (2011) Acute kidney injury: definition, epidemiology, and outcome. Curr Opin Crit Care 17:548–555
Chertow GM, Burdick E, Honour M, Bonventre JV, Bates DW (2005) Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol 16:3365–3370
Ricci Z, Cruz D, Ronco C (2008) The RIFLE criteria and mortality in acute kidney injury: a systematic review. Kidney Int 73:538–546
Ricci Z, Cruz DN, Ronco C (2011) Classification and staging of acute kidney injury: beyond the RIFLE and AKIN criteria. Nat Rev Nephrol 7:201–208
Thongprayoon C, Cheungpasitporn W, Akhoundi A, Ahmed AH, Kashani KB (2014) Actual versus ideal body weight for acute kidney injury diagnosis and classification in critically Ill patients. BMC Nephrol 15:176
Susantitaphong P, Cruz DN, Cerda J et al (2013) World incidence of AKI: a meta-analysis. Clin J Am Soc Nephrol 8:1482–1493
Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P (2004) Acute renal failure—definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care 8:R204–R212
Mehta RL, Kellum JA, Shah SV et al (2007) Acute Kidney Injury Network: report of an initiative to improve outcomes in acute kidney injury. Crit Care 11:R31
Lassnigg A, Schmidlin D, Mouhieddine M et al (2004) Minimal changes of serum creatinine predict prognosis in patients after cardiothoracic surgery: a prospective cohort study. J Am Soc Nephrol 15:1597–1605
Koyner JL, Bennett MR, Worcester EM et al (2008) Urinary cystatin C as an early biomarker of acute kidney injury following adult cardiothoracic surgery. Kidney Int 74:1059–1069
Bellomo R, Raman J, Ronco C (2001) Intensive care unit management of the critically ill patient with fluid overload after open heart surgery. Cardiology 96:169–176
Liu KD, Thompson BT, Ancukiewicz M et al (2011) Acute kidney injury in patients with acute lung injury: impact of fluid accumulation on classification of acute kidney injury and associated outcomes. Crit Care Med 39:2665–2671
Macedo E, Bouchard J, Soroko SH et al (2010) Fluid accumulation, recognition and staging of acute kidney injury in critically-ill patients. Crit Care 14:R82
Levey AS, Stevens LA, Schmid CH et al (2009) A new equation to estimate glomerular filtration rate. Ann Intern Med 150:604–612
Knaus WA, Wagner DP, Draper EA et al (1991) The APACHE III prognostic system. Risk prediction of hospital mortality for critically ill hospitalized adults. Chest 100:1619–1636
Ferreira FL, Bota DP, Bross A, Melot C, Vincent JL (2001) Serial evaluation of the SOFA score to predict outcome in critically ill patients. JAMA 286:1754–1758
Wentworth DN, Neaton JD, Rasmussen WL (1983) An evaluation of the Social Security Administration master beneficiary record file and the National Death Index in the ascertainment of vital status. Am J Public Health 73:1270–1274
Hoste EA, Clermont G, Kersten A et al (2006) RIFLE criteria for acute kidney injury are associated with hospital mortality in critically ill patients: a cohort analysis. Crit Care 10:R73
Coca SG, Peixoto AJ, Garg AX, Krumholz HM, Parikh CR (2007) The prognostic importance of a small acute decrement in kidney function in hospitalized patients: a systematic review and meta-analysis. Am J Kidney Dis 50:712–720
Weisbord SD, Palevsky PM (2006) Acute renal failure in the intensive care unit. Semin Respir Crit Care Med 27:262–273
Fliser D, Laville M, Covic A et al (2012) A European Renal Best Practice (ERBP) position statement on the Kidney Disease Improving Global Outcomes (KDIGO) clinical practice guidelines on acute kidney injury: part 1: definitions, conservative management and contrast-induced nephropathy. Nephrol Dial Transplant 27:4263–4272
Odden MC, Shlipak MG, Tager IB (2009) Serum creatinine and functional limitation in elderly persons. J Gerontol A Biol Sci Med Sci 64:370–376
Englberger L, Suri RM, Li Z et al (2011) Clinical accuracy of RIFLE and Acute Kidney Injury Network (AKIN) criteria for acute kidney injury in patients undergoing cardiac surgery. Crit Care 15:R16
Ho J, Reslerova M, Gali B et al (2012) Serum creatinine measurement immediately after cardiac surgery and prediction of acute kidney injury. Am J Kidney Dis 59:196–201
Bouchard J, Soroko SB, Chertow GM et al (2009) Fluid accumulation, survival and recovery of kidney function in critically ill patients with acute kidney injury. Kidney Int 76:422–427
Plataki M, Kashani K, Cabello-Garza J et al (2011) Predictors of acute kidney injury in septic shock patients: an observational cohort study. Clin J Am Soc Nephrol 6:1744–1751
Bagshaw SM, Uchino S, Bellomo R et al (2007) Septic acute kidney injury in critically ill patients: clinical characteristics and outcomes. Clin J Am Soc Nephrol 2:431–439
Yunos NM, Bellomo R, Hegarty C, Story D, Ho L, Bailey M (2012) Association between a chloride-liberal vs chloride-restrictive intravenous fluid administration strategy and kidney injury in critically ill adults. JAMA 308:1566–1572
Devarajan P (2008) Neutrophil gelatinase-associated lipocalin (NGAL): a new marker of kidney disease. Scand J Clin Lab Invest Suppl 241:89–94
Matsui K, Kamijo-Ikemorif A, Sugaya T, Yasuda T, Kimura K (2011) Renal liver-type fatty acid binding protein (L-FABP) attenuates acute kidney injury in aristolochic acid nephrotoxicity. Am J Pathol 178:1021–1032
Han WK, Bailly V, Abichandani R, Thadhani R, Bonventre JV (2002) Kidney injury molecule-1 (KIM-1): a novel biomarker for human renal proximal tubule injury. Kidney Int 62:237–244
Kashani K, Al-Khafaji A, Ardiles T et al (2013) Discovery and validation of cell cycle arrest biomarkers in human acute kidney injury. Crit Care 17:R25
Conflict of interest
None.
Ethical standards
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual subjects included in the study.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Thongprayoon, C., Cheungpasitporn, W., Srivali, N. et al. The impact of fluid balance on diagnosis, staging and prediction of mortality in critically ill patients with acute kidney injury. J Nephrol 29, 221–227 (2016). https://doi.org/10.1007/s40620-015-0211-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40620-015-0211-3