
Abstract
Purpose
Patients submitted to curative surgery for non-functioning pancreatic neuroendocrine neoplasms (NF-PanNENs) exhibit a variable risk of disease relapse. Aims of this meta-analysis were to estimate the rate of disease recurrence and to investigate the risk factors for disease relapse in patients submitted to curative surgery for NF-PanNENs.
Methods
Medline/Pubmed and Web of Science databases were searched for relevant studies. A meta-regression analysis was performed to investigate the source of recurrence rate heterogeneity. Pooled hazard ratios (HRs) and 95% confidence intervals (95% CI) were used to assess the effect of each possible prognostic factor on disease-free survival.
Results
Fifteen studies, involving 2754 patients submitted to curative surgery for NF-PanNENs, were included. The pooled rate of disease recurrence was 21% (95% CI 15–26%). Study quality (Odds ratio, OR 0.94, P = 0.016) and G3-PanNENs rate (OR 2.18, P = 0.040) independently predicted the recurrence rate variability. Nodal metastases (HR 1.63, P < 0.001), tumor grade G2-G3 (G1 versus G2: HR 1.72, P < 0.001, G1 versus G3 HR 2.57, P < 0.001), microvascular (HR 1.25, P = 0.046) and perineural (HR 1.29, P = 0.019) invasion were identified as significant prognostic factors. T stage (T1-T2 versus T3-T4, P = 0.253) and status of resection margins (R0 versus R1, P = 0.173) did not show any significant relationship with NF-PanNENs recurrence.
Conclusion
Disease relapse occurs in approximately one out of five patients submitted to curative surgery for NF-PanNENs. Nodal involvement, tumor grade, microvascular and perineural invasion are relevant prognostic factors, that should be taken into account for follow-up and for possible trials investigating adjuvant or neoadjuvant treatments.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Pancreatic neuroendocrine neoplasms (PanNENs) account for approximately 2–3% of all pancreatic tumors [1]. Despite being still regarded as rare lesions, their incidence has dramatically increased over the last three decades due to the widespread use of high-quality imaging techniques [1, 2]. Non-functioning (NF) PanNENs represent the vast majority of these lesions and span a wide range of aggressiveness, including both slow-growing tumors with an indolent biological behaviour and aggressive neoplasms presenting at an advanced stage with local invasion and/or distant metastases [3].
Surgery represents the backbone for the curative treatment of localized NF-PanNENs [4,5,6]. Moreover, surgical management has been reported to be associated with a survival benefit also in the presence of resectable or potentially resectable liver metastases [7, 8]. The recurrence rate within 5 years after curative surgery has been reported between 10 and 40% [9,10,11]. Postoperative follow-up plays a pivotal role for the early detection of disease recurrence and its timing should be tailored according to the presence of tumor features of aggressiveness [12]. A number of clinic-pathological features, including presence of symptoms, tumor size and grade, nodal metastases, perineural and microvascular invasion, have been investigated as possible predictors of disease relapse after surgery [13,14,15,16,17]. Furthermore, several retrospective series have developed accurate nomograms that could be of help in predicting the risk of recurrence and consequently in tailoring the follow-up scheme [18,19,20]. Nevertheless, the features at high-risk for postoperative recurrence are still matter of debate and there is much uncertainty regarding the optimal strategy and timing of surveillance after surgery [4, 5].
The aims of this systematic review and meta-analysis were: (i) to estimate the rate of disease recurrence and (ii) to identify the risk factors for disease relapse in patients submitted to curative surgery for NF-PanNENs.
Methods
The present study was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) statement [21].
Eligibility criteria
Prospective and retrospective cohort studies fulfilling the following PICOTS criteria [22] were considered eligible for the present study:
-
1.
Population (P): patients submitted to surgical resection with curative intent (R0-R1) for NF-PanNENs;
-
2.
Index prognostic factors (I): T stage (T1-T2 versus T3-T4), N stage (N0 versus N +), tumor grade (G1 versus G2, G1 versus G3), resection margin status (R0 versus R1), microvascular invasion (no versus yes), perineural invasion (no versus yes);
-
3.
Comparator prognostic factor (C): none;
-
4.
Outcome (O): disease recurrence after curative surgery;
-
5.
Timing (T): at any time during post-surgical follow-up;
-
6.
Setting (S) and role: estimate of recurrence rate and identification of prognostic factors based on which a tailored follow-up schedule could be developed.
Studies were included if either recurrence rate or Kaplan–Meier curve representing disease-free survival (DFS) were provided. Multivariate hazard ratios (HRs) and 95% confidence intervals (CI) were required to enter the meta-analysis on each prognostic factor. Studies comprising both functioning and non-functioning PanNENs were included only if a sub-analysis for NF-PanNENs was performed. Review articles without original data and small case series including less than ten patients were excluded. Studies analysing secondary recurrences or comprising patients submitted to palliative surgical resection (R2) were excluded as well.
Information sources
A systematic review of the literature was conducted following the recommendations for systematic reviews in surgery provided by Goossen et al. [23]. The MEDLINE/PubMed and Web of Science databases were searched for eligible articles, without any language, publication date, or publication type restriction. The last electronic search was performed on December 28, 2020. The PubMed function “related articles” was used with the aim to expand the search. The reference list of all potentially eligible studies was screened to minimize the retrieval bias. The corresponding authors of two included studies were contacted to retrieve additional information.
Search
The search was conducted using medical subject headings (MeSH) in combination with free text words. The search strategy used in MEDLINE/PubMed was the following: (Pancreatic Neuroendocrine Neoplasm OR Pancreatic Neuroendocrine Neoplasms OR Pancreatic Neuroendocrine Tumor OR Pancreatic Neuroendocrine Tumors OR Pancreatic Neuroendocrine Tumour OR Pancreatic Neuroendocrine Tumours OR Pancreatic Endocrine Tumor OR Pancreatic Endocrine Tumors OR Pancreatic Endocrine Tumour OR Pancreatic Endocrine Tumours OR Pancreatic Endocrine Neoplasm OR Pancreatic Endocrine Neoplasms OR Adenoma, Islet Cell OR Adenomas, Islet Cell OR Islet Cell Adenomas OR Islet Cell tumor OR Islet Cell Tumors OR Tumor, Islet Cell OR Tumors, Islet Cell OR Island Cell Tumor OR Island Cell Tumors OR Tumor, Island Cell OR Tumors, Islands Cell OR Apudoma OR Carcinoma, Islet Cell OR Carcinomas, Islet Cell OR Islet Cell Carcinoma OR Islet Cell Carcinomas OR Islet Cell Tumor, Malignant) AND (Disease-Free Survival OR Disease Free Survival OR Survival, Disease-Free OR Survival, Disease Free OR Recurrence OR Relapse).
Study selection
All the records identified through the literature search strategy were screened by two investigators (VA and GG), independently. Titles and abstracts were initially reviewed to remove duplicates and select relevant publications. If the abstract suggested relevance, the full-text paper was assessed for eligibility in accordance with the predefined inclusion criteria.
When multiple articles were published by the same study group and overlapping study periods were reported, either the most recent or the most relevant study was selected to avoid duplication of data. Since two eligible studies [18, 24] had a partially overlapping study population (n = 39) and the authors had access to the database related to the publication by Partelli et al. [24], a new survival analysis was performed excluding the overlapping patients from the above-mentioned study. Two series with a minimal, but not quantifiable cohort overlap, were considered as two independent studies [13, 25]. Two studies by Zhou et al. [26, 27] analysed an almost completely overlapping population. For this reason, patients included in these two series were described as a single study cohort [26, 27].
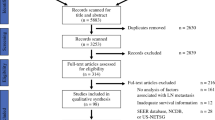
The final decision on eligibility was reached by consensus between the two screening authors (VA and GG). Any disagreement regarding inclusion criteria was solved through discussion or by consulting a third author (SP). Detailed information regarding the screening process are provided in the PRISMA flow diagram (Fig. 1).

PRISMA flow diagram illustrating study selection
Data collection process
Data were extracted from the selected articles using a piloted extraction form by both the screening authors (VA and GG), independently. Extracted data were then compared and any discrepancies were solved through discussion. A third author (SP) was consulted to reach a final consensus and confirm the data, when necessary.
Data items
Data were sought for general information (first author, year of publication, study type and design, study period, institution and country, number of participants), inclusion and exclusion criteria, demographics of study participants (gender and age) and follow-up details (recurrence rate, median follow-up and lost rate). Disease recurrence was defined as local recurrence at the pancreatic resection site, newly identified pathological lymph nodes or development of distant metastases. Clinic-pathological characteristics considered as possible predictors of disease recurrence were: T stage (T1–T2 versus T3–T4) and N stage (N0 versus N +) defined according to European Neuroendocrine Tumor Society (ENETS) or to American Joint Committee on Cancer (AJCC) (8th edition) classifications [28, 29], tumor grade (G1 versus G2 and G1 versus G3) defined according to the 2010/2017 World Health Organization (WHO) classification [30, 31], status of resection margins (R0 versus R1), presence of microvascular and perineural invasion.
Risk of bias in individual studies, summary measures, and synthesis of results
The qualitative assessment of the studies was carried out based on the methodological index for non-randomized studies (MINORS) [32]. All categorical variables were reported as frequencies and percentages, while continuous variables were presented as means with standard deviations. A dedicated statistical algorithm was used to calculate the mean and standard deviation in studies that presented median and interquartile range [33, 34]. The results were reported as pooling proportion of the recurrence rate, together with a 95% CI. When the recurrence rate was not reported, a dedicated software was used to obtain the crude number of events from Kaplan–Meier curves (GetData Graphical Digitizer@). We also extracted the HRs of multivariate prognostic models predicting DFS, when reported. The HRs together with a 95% CI were converted in logarithimc form and analyzed using a random effect model. The results were reported as cumulative HRs and 95% CI and as fictitiuos median DFS time units. The last measure was calculated assuming that: (1) the hazard rates of the group with lower risk was equal to 1, corresponding to a median DFS of 0.7 fictitious time units. The hazard rate for the group with higher risk was calculated following this formula:\(Median DFS=\frac{\mathrm{ln}(2)}{Hazard rate}\)
The meta-analysis was carried out in line with recommendations from the Cochrane Collaboration and Meta-analysis of Observational Studies in Epidemiology guidelines [35, 36] and the Mantel–Haenszel random-effects model was used to calculate effect sizes [37].
Risk of bias across studies and additional analyses
The risk of bias across included studies was tested, measuring both the “between-study heterogeneity” and publication bias. I2 and Cochran’s Q statistics were used to assess heterogeneity [38]. In particular, the value of I2 describes the percentage of variability in point estimates due to heterogeneity rather than sampling error. When I2 was < 50%, the risk of “between-study heterogeneity” was judged as low-moderate; if I2 was ≥ 50%, the risk of “between-study heterogeneity” was considered high. The meta-regression analysis was carried out when heterogeneity was high and the result was statistically relevant [39]. The meta-regression was planned only for the primary endpoint (pooling proportion meta-analysis). The meta-regression was based on the use of maximum residual likelihood (REML) [40, 41].
The multivariate model was built using the forward stepwise model.
Firstly, we calculated the distribution of covariates in each study. Secondly, for each covariate, the following parameters were described: odds ratio (OR) with standard error (SE) and R2. The OR ± SE was related to the change of the recurrence rate: if the OR was > 0, the covariate increase produced a positive modification of the recurrence rate. On the other hand, R2 indicated the percentage of between-study variance explained by the covariate. A two-tailed P value < 0.05 was considered statistically significant. The publication bias evaluation was made using the Begg and the Egger tests [40], and a P value < 0.05 indicated a non-negligible “small-study effect”. A nonparametric “trim and fill” method was used to adjust for the publication bias. The method, a rank-based data augmentation technique, formalizes the use of funnel plots, estimates the number and the outcomes of missing studies, and adjusts the meta-analysis to incorporate the theoretical missing studies. The statistical analysis was carried out using dedicated packages for STATA version 14® (StataCorp, College Station, TX, USA).
Results
Study selection
The PRISMA flow diagram illustrating the study selection process is depicted in Fig. 1. Overall, a total of 11,030 articles were identified using the literature search strategy. Forty-three additional studies were retrieved by means of hand search. Among these, 1579 were excluded, as they were duplicates. The remaining 9494 records were screened by title and abstract for eligibility. Of these, 9194 were excluded because they were not pertinent to the field of the study or did not meet the inclusion criteria. Finally, the full texts of 300 studies were evaluated. Of these, 285 were excluded, 14 of which owing to data duplication (overlapping study cohorts). Eventually, 15 studies fulfilled the inclusion criteria and were suitable for the meta-analysis.
Study characteristics and risk of bias within studies
Fifteen retrospective observational cohort studies, involving a total of 2754 patients submitted to curative surgery for NF-PanNENs, were included [13, 18, 24, 26, 27, 42,43,44,45,46,47,48,49,50,51,52]. All the series were published between 2013 and 2020 and were conducted in nine different countries. Four of these studies were multicentric experiences [13, 18, 24, 47]. The general features and the quality assessment of the included studies are summarized in Table 1. Most of the studies (n = 9) considered only patients with localized disease, whereas six series included also metastatic patients submitted to curative surgery [26, 43,44,45, 48, 51]. Two studies considered standard resections only [46, 48], whereas another series established enucleation (but not other parenchyma-sparing resections) as exclusion criterion [13]. Partelli et al. [24] analysed a cohort selectively including patients submitted to pancreaticoduodenectomy. Six studies considered only patients with PanNENs G1-G2 [13, 18, 49,50,51,52], whereas nine experiences included also G3 neoplasms. Of these latter, only Capretti et al. [46] applied the latest WHO classification [31] distinguishing between well-differentiated PanNETs G3 and poorly differentiated pancreatic neuroendocrine carcinomas (PanNECs) G3. Inclusion and exclusion criteria of selected studies are reported in Table S1. Other clinic-pathological features are provided in Table 2 and Table S2.
Primary endpoint: recurrence rate
The pooled rate of disease recurrence (Fig. 2), calculated considering all the studies (n = 15) included in the meta-analysis, was 21% (95% CI 15–26%). Since the “between-study heterogeneity” was high (I2 92.86%, P < 0.001), a meta-regression analysis was performed (Table 3). At univariate meta-regression analysis, study quality assessed with MINORS score was significantly related to the variability of the recurrence rate (OR 0.94, SE 0.21, P = 0.033). This variable alone could explain 33% (R2) of recurrence rate variability, with a decrease in study quality producing an increase in relapse rate (Fig. S1a). The percentage of G3-PanNENs included in each study showed a trend towards an association with recurrence rate between-study variance (OR 2.31, SE 0.97, P = 0.087). This variable alone could explain 19% (R2) of recurrence rate variability, with an increase in the quote of G3 neoplasms producing an increase in the rate of disease relapse (Fig. S1b).

Forest plot of the pooled recurrence rate of patients submitted to curative surgery for nonfunctioning pancreatic neuroendocrine neoplasms (NF-PanNENs)
Multivariate meta-regression analysis showed that study quality (OR 0.94, SE 0.01, P = 0.016) and G3-PanNENs rate (OR 2.18, SE 0.73, P = 0.040) independently predicted recurrence rate variation. The final multivariable model explained 72.3% of recurrence rate variability.
Secondary endpoints: predictors of disease recurrence
A meta-analysis based on multivariate HRs and 95% CI extraction was performed to evaluate the effect of each covariate (T stage, N stage, tumor grade, resection margin status, microvascular invasion and perineural invasion) on disease recurrence (Table 4).
Three studies [13, 24, 42], including 399 patients, reported T stage dichotomized as T3–T4 versus T1–T2 [28]. The pooled HR was 1.16 (95% CI 0.90–1.50), indicating that T category was not a significant prognostic factor (P = 0.253) (Fig. 3a). The median DFS for T1–T2 and T3–T4 tumors was similar (0.7 versus 0.6 time units).

Forest plots of studies showing the effect pathological factors on disease recurrence (a: T stage—T1-T2 versus T3-T4; b: N stage—N0 versus N + ; c: tumor grade—G1 versus G2; d: tumor grade—G1 versus G3; e: status of resection margins—R0 versus R1; f: microvascular invasion—no versus yes; g: perineural invasion—no versus yes)
Ten series [13, 18, 24, 27, 42, 45, 47, 49, 51, 52], including 2045 patients, evaluated N category (N0 versus N +) as prognostic variable. The pooled HR was 1.63 (95% CI 1.38–1.92), indicating that nodal involvement was a significant predictor of recurrence (P < 0.001) (Fig. 3b). The median DFS was longer in N0 tumors than in N + (0.7 versus 0.5 time units).
Nine studies considered tumor grade as prognostic variable [13, 18, 24, 27, 45, 47, 49,50,51]. Overall, 1218 patients had a PanNEN G1, 722 had a PanNEN G2 and 61 had a PanNEN G3. The pooled HR for G1 versus G2 was 1.72 (95% CI 1.41–2.10), thus indicating that G2 tumors have a significantly higher risk of recurrence compared to G1 tumors (P < 0.001) (Fig. 3c). After adjustment for publication bias, the pooled HR was 1.66 (95% CI 1.37–2.01). Four series [24, 27, 45, 47] considered also the comparison G1 versus G3. The pooled HR for G1 versus G3 was 2.57 (95% CI 1.53–4.34, P < 0.001) (Fig. 3d). The median DFS were 0.7, 0.4 and 0.3 time units for G1, G2 and G3 lesions, respectively.
Three series [13, 47, 48], including 1096 patients, considered the prognostic role of microscopic margin involvement (R0 versus R1). The pooled HR was 1.24 (95% CI 0.92–1.67) (Fig. 3e), indicating that microscopic involvement of the resection margin was not a significant prognostic variable (P = 0.173). The median DFS was similar in patients who underwent R0 and R1 resection (0.7 versus 0.7 time units).
Five studies [13, 24, 42, 47, 51], including 1405 patients, considered the prognostic role of microvascular invasion. The pooled HR was 1.25 (95% CI 1.00–1.55) (Fig. 3f), indicating that microvascular invasion was a significant predictor of disease recurrence (P = 0.046). The related median DFS were 0.7 and 0.6 time units in the absence or presence of microvascular invasion, respectively.
Seven series [13, 18, 24, 42, 47, 50, 51], including 1947 patients, considered the prognostic role of perineural invasion. The pooled HR was 1.29 (95% CI 1.04–1.60) (Fig. 3g), indicating that perineural invasion was a significant predictor of disease recurrence (P = 0.019). The median DFS in the absence or presence of perineural invasion were 0.7 versus 0.5 time units.
Heterogeneity and publication bias
Heterogeneity between studies was low-moderate (I2 < 50%) for T stage (I2 = 0%), resection margin status (I2 = 37%) and microvascular invasion (I2 = 38%). On the contrary, heterogeneity between included series was high (I2 ≥ 50%) for nodal status (I2 = 52%), tumor grade (G1 versus G2, I2 = 54%; G1 versus G3, I2 = 72%) and perineural invasion (I2 = 59%) (Table 4). No “small study effect” was observed for any of the investigated variables using both visual assessment (Fig. S2, panels a-g) and Begg and Egger tests (Table 4). HRs and 95% CI adjusted for publication bias are reported in Table 4.
Discussion
The present study comprehensively assessed the prognosis of patients submitted to curative surgery for NF-PanNENs. The analysis showed that the pooled recurrence rate after curative resection was 21% and that study quality and G3-PanNENs proportion were the main determinants of recurrence rate variability across studies. Tumor grade, nodal involvement, microvascular and perineural invasion were identified as significant predictors of disease relapse.
Radical surgical resection represents the cornerstone for the curative treatment of NF-PanNENs. However, a relevant proportion of patients still experience disease relapse during postoperative follow-up. In this regard, a number of clinic-pathological features have been investigated as possible predictors of disease recurrence. Nevertheless, the rarity of the disease and the heterogeneity in terms of study populations and follow-up length still make it challenging to extrapolate a reliable recurrence rate (10–25%) as well as to draw firm conclusions regarding the most relevant prognostic factors after NF-PanNENs curative resection [9, 10]. Therefore, an accurate stratification of the recurrence risk is currently lacking and there is no tailored follow-up strategy based on the individual risk of recurrence [4, 12].
The present meta-analysis showed that approximately one out of five patients submitted to curative surgery for a NF-PanNEN experiences a disease relapse during follow-up. This rate is higher compared to that reported in a recent meta-analysis published by Li et al. [53], who described a 13% relapse rate after curative surgery for well-differentiated PanNENs. Two main reasons can explain this divergent data: first, the present study included NF-PanNENs only, whereas Li et al. considered both NF and functioning tumors. In this regard, it has been widely reported that functioning PanNENs have a different biological behaviour and a significantly better prognosis compared to NF-PanNENs [19, 54]. Therefore, the selective inclusion of NF neoplasms represents a strength of the present study, as there are no previous meta-analyses evaluating prognostic factors on a homogeneous cohort of curatively resected NF-PanNENs. Second, also G3 neoplasms were considered in this study, while the previous experience limited the analysis to G1-G2 tumors [53]. Consistently, the rate of G3 neoplasms was identified as an independent determinant of recurrence rate variability across the included studies, with a higher rate of G3 PanNENs being associated with an increased rate of disease relapse. The other significant factor explaining recurrence rate heterogeneity was study quality (assessed with MINORS score), with higher recurrence rates in the presence of lower study quality. Of note, the presence of distant metastases was not identified as a predictor of recurrence rate variability, probably due to the low rate of M1 patients included in the present meta-analysis. The use of a meta-regression analysis to identify the main determinants of recurrence rate variability represents another strength of the present study, as it has never been performed in this setting. In addition, most of the included studies (n = 9) had a follow-up length greater than 40 months, which improves the reliability of the present findings.
The results of this study also validate the prognostic role of several clinic-pathological features. The presence of nodal involvement was confirmed to be associated with a poorer DFS, with nine out of ten series agreeing about the significant prognostic role of nodal metastases. Only Gong et al. [51] reported a discordant result, possibly due to low study quality and missing data regarding nodal status in 10% of cases [51]. The present data are concordant with those reported by previous meta-analyses considering resected PanNENs regardless of functional status [53, 55]. Moreover, a recent meta-analysis by Tanaka et al. found a significant association between nodal involvement and decreased survival outcomes in patients with resected NF-PanNENs, highlighting a non-negligible rate of nodal metastases (10%) also in small (< 2 cm) and G1 NF-PanNENs [56]. Based on these findings, an oncological resection with lymphadenectomy seems justified to properly stage patients submitted to surgery for NF-PanNENs and to accurately stratify their risk of disease relapse. Of note, also patients with small NF-PanNETs showing features of aggressiveness (i.e., presence of symptoms, dilation of main pancreatic duct/bile duct) should be managed by formal resection with lymphadenectomy. On the other hand, parenchyma-sparing resections can be considered as a valid option for selected patients with indolent NF-PanNETs ≤ 2 cm, when a conservative management cannot be pursued (i.e., for patient’s choice).
Consistently with previous reports [53, 55], also tumor grade was identified as a relevant predictor of DFS, with G2 and G3 neoplasms having an increasingly higher risk of disease relapse compared to G1 tumors. Indeed, G2 tumors represent a large fraction of PanNENs and include both aggressive and indolent neoplasms encompassing a wide range of Ki67 [10, 15]. Therefore, the between-study heterogeneity hereby reported might be explained by different distributions of Ki67 within the G2 category. The risk of recurrence was even higher in patients with G3 PanNENs, who were also identified as those experiencing the earliest disease relapse (0.3 versus 0.7 time units for G1 tumors). This evidence strengthens the need for a closer postoperative follow-up schedule, based on high-quality morphological and functional imaging, for patients with high-grade neoplasms [20]. However, the number of patients with G3 PanNENs included in the present meta-analysis was pretty low, and no analysis stratified by cell differentiation was performed. Therefore, further assessments distinguishing between G3 PanNETs and PanNECs are now required to draw firm conclusions on this aspect.
Finally, also microvascular and perineural invasion were identified as significant prognostic factors, suggesting that these features should be routinely assessed and systematically reported. This evidence, which is in line with previous findings [16, 17], supports the hypothesis that vessels and nerves could represent a route of metastatic spread and should be consequently regarded as indicators of an aggressive biological behaviour [10]. On the other hand, T stage and status of resection margins did not show any significant relationship with recurrence at pooled analysis. Li et al. reported a similar finding for tumor size, but recognized positive resection margins as a significant risk factor for disease relapse [53]. Of note, in the present meta-analysis, only three studies were considered for the evaluation of these features and sample size was consequently limited. The reason explaining the low number of series available for T stage analysis is that only homogeneous studies applying either the ENETS classification or the AJCC classification 8th edition were considered as eligible [13, 24, 42]. Also, T1–T2 neoplasms may comprise patients with small PanNETs that were not managed conservatively due to the presence of aggressiveness features. Therefore, a selection bias towards aggressive small PanNETs being treated by surgery might explain the lack of a significant association between T stage and disease relapse. Regarding resection margin status, it is currently matter of debate whether R1 resection represents an independent predictor of poorer DFS. In this regard, a recent study showed that re-resection of an initially positive surgical margin to achieve a R0 resection did not improve survival outcomes in patients with PanNENs [57].
The present meta-analysis has several limitations. First, all the included studies are retrospective and this might lead to biases in the collection and reporting of data. Second, inclusion criteria vary across the studies and this represents a relevant source of heterogeneity. In particular, several series considered also metastatic patients submitted to curative surgery. However, the low number of M1 PanNENs prevented from performing a separate analysis to investigate this factor as predictor of disease relapse. Third, most of the included studies applied the 2010 WHO classification for tumor grade, without distinguishing between well- and poorly differentiated G3-PanNENs [30]. Also, the inclusion of series adopting either the 2010 or the 2017 WHO classifications led to a variable categorization (G2 or G1) of patients with Ki67 proliferative index comprised between 2 and 3%. Fourth, there are other relevant prognostic factors, including presence of symptoms, necrosis and DAXX/ATRX status, that were not analysed due to the limited number of series assessing these parameters. Also, the number of harvested lymph nodes could not be evaluated as predictor of disease relapse, due to heterogeneous reporting and lack of data stratified according to the type of surgical resection. Fifth, the number of studies that could be included in the evaluation of T stage and resection margin status is limited, which leads to a decreased reliability of these results. In addition, there is variability in terms of multivariate regression model construction, and this could partially explain the high heterogeneity of the pooled HRs observed for several prognostic factors. Last, fictitiuos median DFS time units, calculated from HRs, were used to estimate the time to disease recurrence for each prognostic factor, as median DFS expressed in months were not available in most of the included studies.
In conclusion, the present study found that disease recurrence is not a rare event, as it occurs in approximately 20% of patients submitted to curative surgery for NF-PanNENs. Nodal involvement, tumor grade G2–G3, microvascular and perineural invasion were identified as the most relevant risk factors for disease relapse. Moreover, patients with G3 PanNENs were identified as the group experiencing the earliest disease relapse. These findings might represent the cornerstone for the establishment of a tailored follow-up schedule. In addition, the accurate stratification of patients’ risk could be useful for designing future trials investigating adjuvant treatments for PanNENs. Prospective studies are needed to confirm the validity of the present findings and assess their implications in the clinical practice.
Availability of data and material
All the data generated or analysed during this study are included in the manuscript or in the supplementary material.
Code availability
Not applicable.
References
Kuo EJ, Salem RR (2013) Population-level analysis of pancreatic neuroendocrine tumors 2 cm or less in size. Ann Surg Oncol 20:2815–2821. https://doi.org/10.1245/s10434-013-3005-7
Dasari A, Shen C, Halperin D et al (2017) Trends in the incidence, prevalence, and survival outcomes in patients with neuroendocrine tumors in the United States. JAMA Oncol 3:1335–1342. https://doi.org/10.1001/jamaoncol.2017.0589
Sandvik OM, Søreide K, Gudlaugsson E et al (2016) Epidemiology and classification of gastroenteropancreatic neuroendocrine neoplasms using current coding criteria. Br J Surg 103:226–232. https://doi.org/10.1002/bjs.10034
Falconi M, Eriksson B, Kaltsas G et al (2016) ENETS consensus guidelines update for the management of patients with functional pancreatic neuroendocrine tumors and non-functional pancreatic neuroendocrine tumors. Neuroendocrinology 103:153–171. https://doi.org/10.1159/000443171
Howe JR, Merchant NB, Conrad C et al (2020) The north American neuroendocrine tumor society consensus paper on the surgical management of pancreatic neuroendocrine tumors. Pancreas 49:1–33. https://doi.org/10.1097/MPA.0000000000001454
Partelli S, Bartsch DK, Capdevila J et al (2017) ENETS consensus guidelines for standard of care in neuroendocrine tumours: surgery for small intestinal and pancreatic neuroendocrine tumours. Neuroendocrinology 105:255–265. https://doi.org/10.1159/000464292
Cloyd JM, Wiseman JT, Pawlik TM (2020) Surgical management of pancreatic neuroendocrine liver metastases. J Gastrointest Oncol 11:590–600. https://doi.org/10.21037/jgo.2019.11.02
Andreasi V, Muffatti F, Guarneri G et al (2020) Surgical principles in the management of pancreatic neuroendocrine neoplasms. Curr Treat Options Oncol 21:48. https://doi.org/10.1007/s11864-020-00736-w
Souche R, Hobeika C, Hain E, Gaujoux S (2020) Surgical management of neuroendocrine tumours of the pancreas. J Clin Med 9:2993. https://doi.org/10.3390/jcm9092993
Pulvirenti A, Pea A, Chang DK, Jamieson NB (2020) Clinical and molecular risk factors for recurrence following radical surgery of well-differentiated pancreatic neuroendocrine tumors. Front Med 7:385. https://doi.org/10.3389/fmed.2020.00385
Singh S, Chan DL, Moody L et al (2018) Recurrence in resected gastroenteropancreatic neuroendocrine tumors. JAMA Oncol 4:583–585. https://doi.org/10.1001/jamaoncol.2018.0024
Singh S, Moody L, Chan DL et al (2018) Follow-up recommendations for completely resected gastroenteropancreatic neuroendocrine tumors. JAMA Oncol 4:1597–1604. https://doi.org/10.1001/jamaoncol.2018.2428
Partelli S, Gaujoux S, Boninsegna L et al (2013) Pattern and clinical predictors of lymph node involvement in nonfunctioning pancreatic neuroendocrine tumors (NF-PanNETs). JAMA Surg 148:932–939. https://doi.org/10.1001/jamasurg.2013.3376
Birnbaum DJ, Gaujoux S, Cherif R et al (2014) Sporadic nonfunctioning pancreatic neuroendocrine tumors: prognostic significance of incidental diagnosis. Surgery (United States) 155:13–21. https://doi.org/10.1016/j.surg.2013.08.007
Genc CG, Falconi M, Partelli S et al (2018) Recurrence of pancreatic neuroendocrine tumors and survival predicted by Ki67. Ann Surg Oncol 25:2467–2474. https://doi.org/10.1245/s10434-018-6518-2
Nanno Y, Toyama H, Otani K et al (2016) Microscopic venous invasion in patients with pancreatic neuroendocrine tumor as a potential predictor of postoperative recurrence. Pancreatology 16:882–887. https://doi.org/10.1016/j.pan.2016.06.008
Zhou H, Wang Y, Guo C et al (2021) Microscopic invasion of nerve is associated with aggressive behaviors in pancreatic neuroendocrine tumors. Front Oncol 11:630316. https://doi.org/10.3389/fonc.2021.630316
Genç CG, Jilesen AP, Partelli S et al (2018) A new scoring system to predict recurrent disease in grade 1 and 2 nonfunctional pancreatic neuroendocrine tumors. Ann Surg 267:1148–1154. https://doi.org/10.1097/SLA.0000000000002123
Pulvirenti A, Javed AA, Landoni L et al (2019) Multi-institutional development and external validation of a nomogram to predict recurrence after curative resection of pancreatic neuroendocrine tumors. Ann Surg. https://doi.org/10.1097/SLA.0000000000003579
Zaidi MY, Lopez-Aguiar AG, Switchenko JM et al (2019) A novel validated recurrence risk score to guide a pragmatic surveillance strategy after resection of pancreatic neuroendocrine tumors: an international study of 1006 patients. Ann Surg 270:422–433. https://doi.org/10.1097/SLA.0000000000003461
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol 62:1006–1012. https://doi.org/10.1016/j.jclinepi.2009.06.005
Riley RD, Moons KGM, Snell KIE et al (2019) A guide to systematic review and meta-analysis of prognostic factor studies. BMJ 364:k4597. https://doi.org/10.1136/bmj.k4597
Goossen K, Tenckhoff S, Probst P et al (2018) Optimal literature search for systematic reviews in surgery. Langenbeck’s Arch Surg 403:119–129. https://doi.org/10.1007/s00423-017-1646-x
Partelli S, Javed AA, Andreasi V et al (2018) The number of positive nodes accurately predicts recurrence after pancreaticoduodenectomy for nonfunctioning neuroendocrine neoplasms. Eur J Surg Oncol 44:778–783. https://doi.org/10.1016/j.ejso.2018.03.005
Landoni L, Marchegiani G, Pollini T et al (2019) The evolution of surgical strategies for pancreatic neuroendocrine tumors (Pan-NENs): time-trend and outcome analysis from 587 consecutive resections at a high-volume institution. Ann Surg 269:725–732. https://doi.org/10.1097/SLA.0000000000002594
Zhou B, Zhan C, Wu J et al (2017) Prognostic significance of preoperative gamma-glutamyltransferase to lymphocyte ratio index in nonfunctional pancreatic neuroendocrine tumors after curative resection. Sci Rep 7:13372. https://doi.org/10.1038/s41598-017-13847-6
Zhou B, Deng J, Chen L, Zheng S (2017) Preoperative neutrophil-to-lymphocyte ratio and tumor-related factors to predict lymph node metastasis in nonfunctioning pancreatic neuroendocrine tumors. Sci Rep 7:17506. https://doi.org/10.1038/s41598-017-17885-y
Rindi G, Kloppel G, Alhman H et al (2006) TNM staging of foregut (neuro)endocrine tumors: a consensus proposal including a grading system. Virchows Arch 449:395–401. https://doi.org/10.1007/s00428-006-0250-1
Brierley J, Gospodarowicz MK, Wittekind C (eds) (2017) AJCC cancer staging manual, 8th edn. Wiley, Oxford
Bosman FT, Carneiro F, Hruban RH, Theise ND (eds) (2010) WHO classification of tumours of the digestive system, 4th edn. IARC Press, Lyon
Lloyd RV, Osamura RY, Kloppel G, Rosai J (eds) (2017) WHO classification of tumours of endocrine organs, 4th edn. IARC Press, Lyon
Slim K, Nini E, Forestier D et al (2003) Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg 73:712–716. https://doi.org/10.1046/j.1445-2197.2003.02748.x
Hozo SP, Djulbegovic B, Hozo I (2005) Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol 5:13. https://doi.org/10.1186/1471-2288-5-13
Wan X, Wang W, Liu J, Tong T (2014) Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol 14:135. https://doi.org/10.1186/1471-2288-14-135
Clarke M, Horton R (2001) Bringing it all together: lancet-cochrane collaborate on systematic reviews. Lancet (London, England) 357:1728. https://doi.org/10.1016/S0140-6736(00)04934-5
Stroup DF, Berlin JA, Morton SC et al (2000) Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis of observational studies in epidemiology (MOOSE) group. JAMA 283:2008–2012. https://doi.org/10.1001/jama.283.15.2008
Mantel N, Haenszel W (1959) Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst 22:719–748. https://doi.org/10.1093/jnci/22.4.719
Hoaglin DC (2016) Misunderstandings about Q and “Cochran’s Q test” in meta-analysis. Stat Med 35:485–495. https://doi.org/10.1002/sim.6632
Higgins JPT, Thompson SG (2002) Quantifying heterogeneity in a meta-analysis. Stat Med 21:1539–1558. https://doi.org/10.1002/sim.1186
Egger M, Davey Smith G, Schneider M, Minder C (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ 315:629–634. https://doi.org/10.1136/bmj.315.7109.629
Thompson SG, Sharp SJ (1999) Explaining heterogeneity in meta-analysis: a comparison of methods. Stat Med 18:2693–2708. https://doi.org/10.1002/(sici)1097-0258(19991030)18:20%3c2693::aid-sim235%3e3.0.co;2-v
Jiang Y, Bin JJ, Zhan Q et al (2015) Impact and clinical predictors of lymph node metastases in nonfunctional pancreatic neuroendocrine tumors. Chin Med J (Engl) 128:3335–3344. https://doi.org/10.4103/0366-6999.171427
Sallinen V, Haglund C, Seppanen H (2015) Outcomes of resected nonfunctional pancreatic neuroendocrine tumors: do size and symptoms matter? Surgery 158:1556–1563. https://doi.org/10.1016/j.surg.2015.04.035
Choi SH, Kim HJ, Kim SY et al (2017) Computed tomography features predictive of lymph node involvement in patients with a nonfunctioning pancreatic neuroendocrine tumor. Pancreas 46:1056–1063. https://doi.org/10.1097/MPA.0000000000000888
Bu J, Youn S, Kwon W et al (2018) Prognostic factors of non-functioning pancreatic neuroendocrine tumor revisited: the value of WHO 2010 classification. Ann Hepato-Biliary-Pancreatic Surg 22:66–74. https://doi.org/10.14701/ahbps.2018.22.1.66
Capretti G, Nappo G, Smiroldo V et al (2019) The number of metastatic lymph nodes is a useful predictive factor for recurrence after surgery for nonmetastatic nonfunctional neuroendocrine neoplasm of the pancreas. Gastroenterol Res Pract 2019:6856329. https://doi.org/10.1155/2019/6856329
Dong D-H, Zhang X-F, Lopez-Aguiar AG et al (2019) Tumor burden score predicts tumor recurrence of non-functional pancreatic neuroendocrine tumors after curative resection. HPB (Oxford) 22:1149–1157. https://doi.org/10.1016/j.hpb.2019.11.009
Feretis M, Wang T, Ghorani E et al (2019) A rational approach to postoperative surveillance for resected non-functional pancreatic neuro-endocrine tumours. Pancreatology 19:1000–1007. https://doi.org/10.1016/j.pan.2019.08.005
Izumo W, Higuchi R, Furukawa T et al (2019) Evaluation of the site and frequency of lymph node metastasis with non-functioning pancreatic neuroendocrine tumor. Eur Surg Res 60:219–228. https://doi.org/10.1159/000504410
Landoni L, Marchegiani G, Pollini T et al (2019) The evolution of surgical strategies for pancreatic neuroendocrine tumors (Pan-NENs). Ann Surg 269:725–732. https://doi.org/10.1097/sla.0000000000002594
Gong Y, Fan Z, Zhang P et al (2021) High pre-operative fasting blood glucose levels predict a poor prognosis in patients with pancreatic neuroendocrine tumour. Endocrine 71:494–501. https://doi.org/10.1007/s12020-020-02469-0
Tan Q-Q, Wang X, Yang L et al (2020) Analysis of recurrence after resection of well-differentiated non-functioning pancreatic neuroendocrine tumors. Medicine (Baltimore) 99:e20324. https://doi.org/10.1097/MD.0000000000020324
Li Y-L, Fan G, Yu F et al (2020) Meta-analysis of prognostic factors for recurrence of resected well-differentiated pancreatic neuroendocrine tumors. Neuroendocrinology. https://doi.org/10.1159/000514047
Crippa S, Zerbi A, Boninsegna L et al (2012) Surgical management of insulinomas: short- and long-term outcomes after enucleations and pancreatic resections. Arch Surg 147:261–266. https://doi.org/10.1001/archsurg.2011.1843
Gao Y, Gao H, Wang G et al (2018) A meta-analysis of prognostic factor of pancreatic neuroendocrine neoplasms. Sci Rep 8:7271. https://doi.org/10.1038/s41598-018-24072-0
Tanaka M, Heckler M, Mihaljevic AL et al (2021) Systematic review and metaanalysis of lymph node metastases of resected pancreatic neuroendocrine tumors. Ann Surg Oncol 28:1614–1624. https://doi.org/10.1245/s10434-020-08850-7
Zhang X-F, Wu Z, Cloyd J et al (2019) Margin status and long-term prognosis of primary pancreatic neuroendocrine tumor after curative resection: results from the US neuroendocrine tumor study group. Surgery 165:548–556. https://doi.org/10.1016/j.surg.2018.08.015
Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FLTA (eds) (2010) AJCC cancer staging manual, 7th edn. Springer, Lyon
Acknowledgements
The authors are grateful to Gioja Bianca Costanza Fund for supporting the PhD Scholarship of Dr. Valentina Andreasi and the Research Fellowship of Dr. Francesca Muffatti. The Authors are also grateful to the Fondazione Umberto Veronesi for supporting the Reserach Fellowship of Dr. Giovanni Guarneri. Authors thank the ERN EURACAN initiative.
Funding
None.
Author information
Authors and Affiliations
Contributions
Study concept and design: VA, CR, SP, RC, MF. Data collection: VA, GG, SP. Analysis of the data: CR, VA, GG, CI. Interpretation of the data: VA, CR, SP, GG, CI, FM, SC, RC, MF. Drafting the manuscript: VA, CR, SP, GG. Critical revision of the manuscript: all the authors.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Ethical approval
This meta-analysis is based on published studies performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki.
Research involving human participants and/or animals
As this meta-analysis is performed based on published studies, no ethical approval was required.
Consent to participate
Not applicable.
Consent for publication
As this meta-analysis is based on published studies, no patient consent for publication was required
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Andreasi, V., Ricci, C., Partelli, S. et al. Predictors of disease recurrence after curative surgery for nonfunctioning pancreatic neuroendocrine neoplasms (NF-PanNENs): a systematic review and meta-analysis. J Endocrinol Invest 45, 705–718 (2022). https://doi.org/10.1007/s40618-021-01705-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40618-021-01705-2