
Abstract
Objectives
This manuscript aims to understand the association between self-rated health and ethnic-racial characteristics (i.e., skin color, self-ascription, and Indigenous language) in the context of the Mexican population.
Design
Logistic regression analyses, using the 2019 PRODER (N = 7187)—a representative survey at the national level. We centered the analysis on two measures of skin color: the interviewer assessment of color skin (that has been used in previous studies), and the ITA scale, a measure constructed from optical digital colorimeter readings (a novel method in ethnoraciality studies in Mexico, included in the PRODER survey).
Results
In comparison to the interviewer’s assessment of skin color, the ITA score shows a significant association with self-rated health, even in the presence of individual conditions, sociodemographic traits, and life-course events. In contrast, ethnic-racial self-ascriptions and speaking of an Indigenous language do not show any statistical associations.
Conclusion
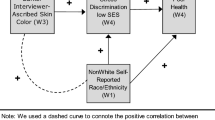
Contrary to previous research, our results suggest a positive association between skin color and self-rated health, when the former is assessed with the colorimeter readings; it means that those with lighter color skin are more prone to report a better health perception. It has methodological implications in the way skin color is observed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Self-rated health refers to the perceptions, experiences, and values that individuals have concerning their health situation [1]. Perception of health is a subjective experience that incorporates the interaction between individuals and their sociocultural world [2]; thus, it relates to physical, emotional, and subjective well-being dimensions [3]. It mirrors objective conditions of health, although the perception of own health does not have to be confirmed by medical staff or biomedical indicators [1, 4, 5]. Besides, it mostly represents physical health problems and, less frequently, mental conditions [6]. Self-rated health has also been extensively associated with several health indicators and outcomes [4]. More specifically, it has been related to morbidities and the demand for public health services [1] and mortality and the increased risk of premature death [3]. Moreover, poor perceptions of health have been linked to social isolation, negative life events, depression, and stress [7].
Despite these associations, self-rated health is a relevant indicator by itself, considering subjective perspectives of life can predict the health behaviors and lifestyles of individuals and communities [3, 6]. In addition, since it is a measure included in many studies, it has demonstrated its comparability, validity, and conceptual robustness in different contexts [3, 8]. In turn, it has been used to describe and compare the health conditions of several populations and groups [3]. This last attribute is particularly useful in the analysis of the distribution of health disparities between advantaged and disadvantaged individuals. For instance, several studies indicate that the incidence and prevalence of diseases and health patterns are unequally distributed according to social stratification categories, such as gender, race, ethnicity, age, education attainment, or socioeconomic conditions [7,8,9]. However, in the case of race and ethnicity, understanding of the relationship between them and health and health perception remains incomplete [9].
In Mexico, ethnoracial differences are an important dimension in the configuration of social structure and stratification [10], although, in the field of health perception, a little-studied one. Regarding social structures, ethnicity and race have proven to impact the distribution of economic, social, and cultural resources, and the access to social and market services and goods (such as access to healthcare), contributing to the making of hierarchies where some groups are excluded from opportunities (see, e.g., [11,12,13,14,15]. Furthermore, the “ethnoracial” adjective defines the lack of boundaries between ethnic and racial attributes [16]. In the case of Mexico, notions of ethnicity and race are blurred as a result of the narrative of Mestizaje [17], a state project that originated at the beginning of the last century, which pursued the homogeneity of the Mexican population, and therefore, the assimilation of Indigenous and African Mexican populations into the (more dominant) Mestizo society. As a result, during the rest of the twentieth century, ethnic and racial differences were sidestepped, turning the Indigenous and Afro-Mexican identities into residual categories [18] and marginalized groups, despite in 2020 they represent 9.4% and 2.0% of the Mexican population, respectively [19]. In the last decades, various social and political movements have advocated for the recognition of Indigenous and Afro-Mexican peoples, as well as for the fulfilment of their rights, leading to a constitutional and public acknowledgment of these populations.
Despite these advancements, the Mestizaje discourse has obscured the general categories of “ethnic group” and “race,” and thus, Mexicans are little familiar with the terms and avoid their use as forms of classification and social self-identification [18]. Still, people do identify some common traits in more specific categories (e.g., Indigenous or Afro-Mexicans). For instance, those who identify themselves as “Black” or “White” expose as their main argument for self-ascription racialized physical traits, such as physical attributes or skin color, whereas those who identify themselves as “Indigenous” and “Mestizos” focus on the family origin and language, culture, traditions, and customs [18]. It implies that considerations on race and ethnicity are being determined, in part, by physical characteristics, and in other, by cultural aspects. In any case, “ethnoracial” categories can be simultaneously determined by (1) other’s perceptions; (2) self-perceptions, and (3) random genetic composition. This suggests that no category is exclusively composed of one criterion, and thus, the ethnicity and race concepts are multidimensional—i.e., comprised of multiple indicators or dimensions.
In this vein, several scholars have pointed out the necessity to observe and measure dimensions such as skin color, self-ascription, color of physical features (e.g., eye color, hair color), characteristics of physical features (hair texture, nose shape, eye shape, body density, height, weight), language, or regional origin, among others, as multi-composing dimensions of ethnoracial ascriptions. If we consider the fragility or ambiguity of the concepts of race and ethnicity for Mexicans, the inclusion of these different dimensions and indicators could be central in the evaluation of socioeconomic inequalities in relation to ethnoraciality. In fact, most prior studies related to ethnoracial traits have relied on one-dimension indicators (e.g., phenotypical markers) or external criteria (i.e., assessment of interviewers) and not on multifaceted indicators or self-ascribed identities [20]. It follows that it is not only pertinent to include different dimensions of ethnoraciality but also to measure them in alternative ways. For example, skin color usually has been observed through the interviewer’s or the interviewee’s assessment, but not with measurements non-based on appreciations (e.g., optical devices), which can be less subject to social bias. This is important in the observation of race and ethnicity, considering the lack of logical consistency of ethnoracial categories that may be partially explained by other’s perceptions of appearance or identification.
In the Mexican case, research that examines multiple ethnoracial dimensions is scarcer [20], despite in recent studies, it has been highlighting the need to study social inequalities and ethnoracial characteristics from intersectional and multidimensional approaches [10, 21, 22]. This perspective is necessary due to the composite nature of discrimination, life experiences, and perceptions of social well-being that cannot be explained solely by one attribute, such as belonging to one population or displaying specific racialized physical traits, which remarks the importance of measuring social and economic disparities through multidimensional views of ethnic and race. Evidence demonstrates socioeconomic inequalities between distinctive ethnic and racial populations, among them, Indigenous and African Mexicans, and those with specific phenotypes (e.g., darker skin tones). These disparities reproduce and legitimize economic, social, cultural, and political inequalities [10] and reflect on issues such as the lack of access to wealth and education [23, 24]; barriers to the labor market [24, 25]; narrow social mobility [26, 27]; everyday and major discrimination experiences [22]; interaction with government institutions [28]; and a diminished perception of subjective well-being [12].
In this way, the 2019 Project on Ethnic-Racial Discrimination in Mexico (Proyecto Sobre Discriminación Étnico-Racial en México 2019, in Spanish [PRODER 2019]) aimed to collect information on the multiple dimensions of ethnoraciality of Mexicans and their relationship to inequalities. Some important advances in this study were the utilization of several evaluations of ethnoracial traits, including external observations, as well as self-perception of interviewees and the novelty use of digital optical colorimeters in inequality studies to observe the color of skin. The employment of these electronic devices represented an addition to the study of ethnoracial traits, mostly because it helped to suppress the bias based on external assessments, such as those produced by the interviewer’s perceptions or those originating from contextual factors or social markers. Consequently, the use of multiple and distinctive assessments led to more precise analyses of the role of skin color and other ethnoracial traits on economic and social inequalities, such as has been evidenced in previous studies using the 2019 PRODER (see, e.g., [12, 17, 22, 29]).
Concerning health perception, a few studies have explored its association with ethnoracial dimensions in the context of Latin America, indicating bad and poor self-rated health in those self-ascribed as Indigenous or in any ethnic minority, or whose interviewers have reported them as having dark-skin color [1, 20, 30]. Contrary, those who self-ascribe as Whites are less prone to report bad health, in comparison to non-Whites [3]. However, in Mexico, little is known about the role of ethnic-racial traits on self-rated health. Only a few scholars have exposed that Afro-descendants, light brown, and dark brown individuals report lower health status compared to Whites [31, p. 9], but in general, the relationship with ethnic-racial attributes has been overlooked [20]. In consequence, self-rated health measurements have been not considered in the decisions of health care policies despite their theoretical and empirical importance and associations with social structures [1].
A better understanding of self-rated health, particularly among Indigenous and Afro-descendant groups or those with darker skin tones, will redress health disparities and allow the construction of relevant health policies and interventions [32]. In countries with similar economic contexts—i.e., mid and low-income ones—and with comparable historic and cultural trajectories and ethnic-racial compositions—i.e., Latin American nations—knowledge about self-rated health and distinctions of ethnoracial measurements will help to promote equity, improve access to health care, personalize healthcare for different patient groups, and advance health research and policy.
Therefore, in the current manuscript, we aim to explore the associations between self-rated health and several ethnic-racial characteristics, such as skin color, ethnic-racial self-ascription, and the speaking or understanding of an Indigenous language, in Mexico, using data from the 2019 PRODER. As noted, in comparison to previous research, we will employ a multidimensional and multi-measurement approach to the ethnic-racial traits, particularly with skin color, as well as several socioeconomic indicators related to inequalities that may account for the perception of health.
Bearing all previous exposition in mind, the research question that emerges is, how is the association between self-rated health and ethnic-racial characteristics (i.e., skin color, self-ascription, and language) in the Mexican context? The answer to this question will be helpful in the explanation of the underlying factors that compose perceptions of health, in such a context as those like Mexico. In turn, hopefully, findings from this research will be useful in the design of health policies and healthcare systems that minimize ethnoracial disparities and abolish social conditions that have been, historically, uneven.
Hypotheses
As noted, extant literature suggests the existence of a negative association between self-ascription of disadvantaged racial-ethnic categories, individuals with darker skin tones, and self-rated health. However, these relationships have been not fully explored in the context of the multiracial and multi-ethnic population in Mexico, and less from the perspective of multiple and overlapping dimensions of race and ethnicity. Thus, trying to fulfil this gap, we propose the following exploratory hypotheses:
-
H1.
Darker tones of skin color (measured by the interviewer’s assessment) will decrease the likelihood that interviewees classify themselves in the higher category of self-rated health; whereas, lighter tones of skin color will increase it.
-
H2.
Darker tones of skin color (measured by optical colorimeter readings) will decrease the likelihood that interviewees classify themselves in the higher category of self-rated health; whereas, lighter tones of skin color will increase it.
-
H3.
Indigenous and Black self-ascriptions will decrease the likelihood that interviewees classify themselves in the higher category of self-rated health; meanwhile, White self-ascription will increase the likelihood that interviewees classify themselves in the higher category of self-rated health.
-
H4.
Speaking and understanding an Indigenous language will decrease the likelihood that interviewees identified as Indigenous classify themselves in the higher category of self-rated health.
Materials and Methods
Study Design, Dataset, and Sample
This study is a secondary data and quantitative analysis with an exploratory and relational approach. The analysis uses data from the 2019 PRODER that aims to obtain information on the ethnic-racial characteristics of Mexicans and learn about ethnic-racial discrimination in Mexico, social inequities, and the perceptions of these issues [33].
The 2019 PRODER was a representative survey at the national level. The sampling design was probabilistic, multi-stage, and by conglomerates. Weights were calculated using sociodemographic information from the 2015 Intercensal Survey (Encuesta Intercensal 2015, in Spanish) [33]. Data were collected from 7187 face-to-face interviews with people from 25 to 64 years old, from July to October 2019, in Spanish. In addition, electronic devices, such as smartphones and digital colorimeters, were used [22, 29].
In order to test and validate the instrument of the survey and the data collection system, a pilot test was carried out, using the field procedures that would be used to collect the definitive information and capture skin images through the colorimeter.
Measurements
In this study, the outcome (i.e., dependent variable) is the self-rated health indicator. Independent variables are organized into three sets of indicators: ethnoracial characteristics (i.e., skin color assessment by the interviewer, skin color assessment by the optical colorimeter, self-ascription, and Indigenous language [only for those who self-identify as Indigenous]), individual and sociodemographic traits (i.e., age, sex, marital status, type of region, years of education, and the assets index), and life-course events (i.e., discrimination experiences and recent health events). All of them have been selected according to findings in the literature. In the next paragraphs, we describe everyone (a summary of measurements is available in Supplementary Information 1, Table S1).
Self-Rated Health
In the 2019 PRODER survey, the self-rated health perception was evaluated through the question, “How do you consider your current state of health?” The item included five categories of response: (1) very good, (2) good, (3) fair, (4) bad, and (5) very bad. Then, following literature in the field, the variable was dichotomized between (1) those who perceived good health (responses “very good” and “good”) and (0) those who perceived bad or regular health (“fair,” “bad,” and “very bad”) [20].
Skin Color Assessment by the Interviewer
In this paper, we employ the PRODER color palette, an alternative color scale designed to “capture the subtler variations in skin color, and more specifically lightness of skin, in the Mexican population” [17, p. 13]. The PRODER palette is originally based on the Pantone skin tone guide, which establishes a standard for skin color variations while guaranteeing more precise color representation in the PRODER palette. In the final part of the design, only eleven skin tones were selected, to allow comparability with previous palettes, such as the PERLA scaleFootnote 1 [34].
Bearing that in mind, in the PRODER survey, skin color was assessed by the interviewer in one item. It used the question “Based on the PRODER color scale, in what skin tone would you place the person interviewed?” Following previous research,Footnote 2 we recodified the variable into five groups, from darker to lighter tones: group 1 (from A to C color), group 2 (D and E color), group 3 (F color), group 4 (from G to H color), and group 5 (from I to K color).
Skin Color Assessment by the Optical Colorimeter
Despite the importance of the PRODER palette regarding a more accurate evaluation of the Mexican population, it does not eliminate the problems of measurement error and bias [17]. Measurements based on external appreciations, such as those using color palettes or interviewers’ assessments, are more prone to be affected by circumstantial situations or influenced by several factors, for example, clothing or socioeconomic status markers. Considering this, in the 2019 PRODER, the skin color of respondents was alternatively captured via portable digital optical colorimeters, color scanners that have their light source to measure color, and thus, are not affected by interviewers’ biases or are less influenced by measurement error.
Measures of the inside of the wrist and the back of the hand were collected, using the colorimeter, and then averaged. Data was recodified using the CIELAB color space, based on the values L*, for luminosity from 0 (black) to 100 (white), and b*, for the variations in color from blue to yellow. In turn, based on the values of L* and b*, we built a measure of skin tone termed the individual typological angle (ITA) [17]. The result, the ITA scale, is a continuous variable that ranges from darker skin tones to lighter ones.
Ethnoracial Self-Ascription and Speaking of an Indigenous Language
The 2019 PRODER survey includes four dichotomous items that asked interviewees whether they considered themselves Indigenous, Afro-Mexican (or Black), White, and Mestizo, or not (yes = 1, no = 0). In the case of the Indigenous self-ascription and speaking of an Indigenous language items, they were integrated into one variable, so, data was recoded into (a) those who do not identify themselves as Indigenous, (b) those who identify as Indigenous but do not speak an Indigenous language or their parents do not speak one, and (c) those who identify as Indigenous and speak an Indigenous language or their parents speak one. The other ascriptions were recoded into those who do not identify with the self-ascription and those who do (no = 0, yes = 1).
Individual and Sociodemographic Traits
The second group of variables covers individual and sociodemographic indicators that have been evidenced to be related to perceptions of health; thus, we employ them as control variables.
Age has been linked to the perception of health [3, 8], although the relationship remains controversial, that is, some authors suggest a better perception of health in younger individuals, while others point to older people. In any case, we measure age with a continuous variable that specifies years old turned. Sex and gender have been also evidenced to have an association with self-rated health, usually, interacting with other factors such as socioeconomic status, age, and education [1, 3, 8]. In the analysis, we employ sex as a dichotomous variable that categorizes respondents into man or woman (man = 1, woman = 2). Social capital and social support have been also related to perceptions of health because; in some way, they reflect the availability of resources for coping with future health events [7]. Thus, we include marital status as a proxy for both conditions with a variable that indicates whether the individuals are in a relationship or not (no = 0, yes = 1). The geographic area or type of region (urban or rural) influences access to health services; therefore, it has been suggested to have an influence on self-rated health [1]. Considering this, in the analysis, we include the type of region where the interviewee lives at the moment of the interview, which could be urban or rural regions (urban = 0, rural = 1). Education is another central trait in the perception of health. To some scholars, more educated individuals are more prone to report better health outcomes, probably, because of a major awareness of individual health conditions [1, 3, 8]. In the analysis, we incorporated educational attainment expressed as the standardized variable of years of education, which is an interval measure. Finally, socioeconomic status has also been evidenced to predict self-rated health [8, 35]. In this vein, we employ the assets index—a standardized and interval variable of the total number of assets, goods, and services in the household—as a proxy of socioeconomic status. The index comprises the ownership of the following items: refrigerator, iron, blender, gas or electric stove, washing machine, cable television, telephone, DVD/Blu-ray player, microwave, fan, videogame console, toaster, internet access, number of light bulbs, printer, car, property or real estate, and the number of household members divided by the number of bedrooms.
Life-Course Events
The third set of independent variables includes occurrences that have been referred to in the literature as relevant determinants of perceptions of health, such as discrimination experiences and recent health events. This is particularly more noticeable in the case of discrimination, which has been related to health and perceptions of health in contexts of ethnic-racial diversity [36].
The discrimination indicator specifies whether the respondent has lived discrimination ever in his/her life or not. This is a dichotomous variable that has been built from two scales incorporated in the 2019 PRODER survey: the Everyday Discrimination Scale (EDS) and the Major Discrimination Scale (MDS).Footnote 3 Both scales have been overly validated and widely used in studies related to discrimination experiences; thus, we integrated them into the analysis, in the form of one single item.
The last variable is the discomfort-illness item that asked, “How long ago was the last time you suffered any pain, discomfort, illness, or accident that prevented you from performing your daily activities?” Responses were recoded into three categories, (1) never or did not have, (2) more than 1 year ago, and (3) less than 1 year ago.
Data Analysis Procedures
Several tests were performed to analyze the relationship between self-rated health and ethnic-racial characteristics. First, univariate analyses were run. For categorical variables, absolute and relative frequencies were calculated; while for interval variables, the mean, standard deviation, variance, skewness, and kurtosis were estimated. After, logistic regression models were performed. This technique allows for exploring the effect of each independent variable on the probability of the event occurring [37, p. 180]. Besides, to further interpretation, we calculated odds ratios. These can be used to estimate how an independent variable influences the dependent variable (refer to Supplementary Information 2 for logistic regression and odds ratios equations).
To test hypotheses, we build two groups of models. Each group is differentiated in the measurement of skin color. In the first one, we employed the assessment by the interviewer using the PRODER palette; whereas, in the second group, models included the measurement of skin color based on the colorimeter readings (i.e., the ITA scale).
Accordingly, in the first group, we developed three models. In model 1, we tested the association between self-rated health and ethnic-racial characteristics (skin color assessment by the interviewer, self-ascription, and speaking of an Indigenous language). In model 2, along with previous variables, we included age, sex, marital status, area of residence, education, and the assets index (i.e., the individual and sociodemographic traits). In model 3, we added to model 2 those variables related to life-course events (i.e., discrimination experiences and illness or discomfort).
In the second group, we also proposed three models. In model 4, we estimated the association between self-rated health and ethnic-racial characteristics (the ITA scale, self-ascription, and speaking of an Indigenous language). In model 5, besides variables in model 4, age, sex, marital status, area of residence, education, and the assets index were incorporated. In model 6, along with those variables in model 5, we integrated discrimination experiences and illness or discomfort indicators. Besides, odds ratios and measures of goodness-of-fit (Pearson goodness-of-fit and the Hosmer–Lemeshow tests) were calculated for the six models. Expansion factors were used for all estimations.
Results
Descriptive Statistics
According to the analysis, most respondents reported good health (74.8%), while fewer of them indicated bad health (25.3%). Concerning the assessment of skin color using the PRODER palette, respondents are distributed as follows: from tones A to C, 13.5%; tones D and E, 33.6%; tones F, 16.7%; tones G and H, 25.8%; and tones I to K, 10.4%. As noted, most interviewees are categorized into the middle tones of the scale, from D to H colors (76.1%). In the case of the ITA scale, the mean is − 0.11, the standard deviation is 0.96, the minimum value is − 4.61, and the maximum is 3.54.
In regard to ethnic-racial self-ascription, 38.2% identify as Indigenous, of which 17.1% do not speak an Indigenous language and 21.1% speak one or his/her parents are speakers of one. Regarding Black self-ascription, only 2.9% identify with this category, 60.8% with the Mestizo self-ascription, whereas 8.0% with the White group.
Concerning sociodemographic traits, most respondents are women (52.4%). The mean age is 41.3 years (standard deviation = 11.54, minimum age = 25 years old, maximum = 64 years old) and the mean of years of education is 9.6 years (standard deviation = 4.3, minimum = 0 years of education, maximum = 22 years), which is equivalent to secondary education. Other variables are summarized in Table 1.
Logit Results
Table 2 shows the logit results of the first group of models—i.e., those with the skin color variable assessed by the interviewer using the PRODER scale. The three models are statistically significant (p < 0.001) and show pseudo r2 from 0.02 (model 1) to 0.13 (model 3).
As observed in Table 2, in model 3, after adjusting for individual and sociodemographic characteristics—i.e., age, sex, marital status, area of residence, education, and the assets index—and life-course events—discrimination experiences and recent health events (illness or discomfort)—we found that none of the skin color measurement groups and the self-ascription categories show significant relationships. Considering age (p < 0.001), education (p < 0 0.001), assets (p < 0.001), and the occurrences of life-course events have statistically significant associations (p < 0.01 and p < 0.001) for discrimination categories, and (p < 0.001 and p < 0.001) for the illness’ ones, it suggests that the hypothesized association between skin color (assessed by the interviewer), self-ascriptions, language, and self-perception of health could be fully explained by individual and sociodemographic traits and individual negative life experiences.
In Table 3, we present the logit results of the second group of models, i.e., those including the ITA scale. The three models are statistically significant (p < 0.001) and show pseudo r2 from 0.02 (model 4) to 0.14 (model 6).
In model 6, after adjusting for individual and sociodemographic characteristics and the life-course event variables, the association with the ITA scale remains statistically significant, even though this coefficient is lower than in models 4 and 5 (0.16, p < 0.001). Meanwhile, no self-identification variable remains significant in model 6, in contrast to models 4 and 5. The decrease in the ITA scale coefficient and the loss of significance of self-ascription variables in the presence of control variables suggest that sociodemographic traits and life-course events could participate as mediators or moderators of the relationship with self-perceived health.
Along with coefficients, odds are also presented in Tables 2 and 3, suggesting how a change in an independent variable is associated with a change in the dependent variable. In model 6, for instance, holding all other variables constant, a lighter skin color (i.e., an increase of one standard deviation in the ITA score) implies 1.17 times higher odds of reporting good health, in comparison to bad health. Also, those individuals with higher levels of education and assets are more prone to report good health (1.05 and 1.23 times more odds per standard deviation, respectively). In contrast, a participant who experienced discomfort or illness in the previous year was 65% less likely (odds ratio = 0.35) to report good versus bad health compared to someone reporting never having a health event; while those who experienced three or more discrimination events were 50% less likely (odds = 0.50) of mentioning good health, in comparison to bad health, holding all other variables constant.
In addition, according to AIC and BIC indicators, the model with a better fit is model 6 (with the lowest values of both criteria). Finally, also measures of goodness-of-fit (Pearson goodness-of-fit and the Hosmer–Lemeshow tests) were calculated. In every model, these tests show p values above 0.05 (i.e., they are not significant), which suggests that observed data correspond to the fitted (assumed) model.
Discussion
Results show that, in the Mexican context, self-rated health is not equally associated with all ethnic-racial characteristics. After controlling for several factors related to the perception of health, the self-ascriptions of Indigenous, Black, Mestizo, and White show a null statistical association with self-rated health. Similarly, speaking or understanding an Indigenous language (both Indigenous respondents who have speaking parents and those who speak or understand an Indigenous language) does not manifest a significant association with the self-rated health indicator. Contrary, skin color, when measured by the ITA scale (in comparison to the assessment made by the interviewer), remains statistically related to perceptions of health.
In the extant literature, although the relationship between ethnic-racial ascriptions and self-rated health has been evidenced, in the case of Mexico, the association is still ambiguous or unknown. In research where self-ascriptions have been incorporated, they are superseded by skin color (or in reverse) [3, 31]. In other studies, racialized characteristics have not been included in the analysis [30], which ignores the complex nature of ethnic-racial identities. Despite this, in the study by Perreira and Telles [20], some results partially support our findings here: ethnic-racial self-ascription is not linked to self-rated health in the presence of skin color measurements, sociodemographic traits, and life-course events. However, according to Perreira and Telles [20], skin color assessed by the interviewer loses significance when adjusted with sociodemographic characteristics and life-course experiences. In other words, ethnic-racial ascription and skin color observed by the interviewer are not relevant to self-rated health when they are controlled by several individual and contextual conditions.
Contrary to these scholars, our findings indicate that there is an association between self-rated health and skin color when we measure the last with optical colorimeter readings, instead of assessments based on personal perceptions (such as those by the interviewer or the interviewee). It reminds a similar discussion in the field regarding the breach between ethnic-racial self-ascriptions and ascriptions assigned by external observers [34], which may lead to biases and inconsistencies in the evaluation of several inequalities. Regarding skin color, it has been evidenced how its measurement can be modified by economic, social, and cultural markers, such as socioeconomic status [29]. Therefore, measures based on colorimeter readings, that use digital scans and controlled lighting, are free of social biases and measurement error [17, 29], which is not the same for external and subjective assessments. In this analysis, we avoid these predispositions by employing the ITA score, which is constructed with the data from digital colorimeters (see the “Materials and Methods” section). Using these devices has proven to be a reliable method in the evaluation of skin color [39, 40]. Thereby, results show that ethnic-racial self-ascriptions and skin color assessed by the interviewer lost relevance in the presence of control variables; whereas the ITA score shows consistent associations with self-rated health in the last three models presented, even in the presence of determinant conditions.
In other words, these findings bring more evidence to the discussion of the measurement of ethnic-racial characteristics and how some conceptual and technical decisions may affect associations with social and economic disparities. This is particularly relevant, first, because in Mexico, it has been evidenced the key role of skin color in socioeconomic inequalities, in contrast to other Latin American countries [20, 34]; and second, considering the ambiguous understanding of ethnic and racial categories for the Mexicans [18], the consistency of skin color measurements allows us to suppose that we are proposing a solid measure in the explanation and evaluation of social, economic, and political inequalities.
With the ITA scale, results suggest that lighter skin colors have an increment in the likelihood that interviewees report a higher category of self-rated health, while, in those with darker skin colors, the relationship is inverse. These findings are also consistent with the literature on self-rated health [3, 31], as well as with other inequalities related to health and access to socioeconomic resources by skin color [24, 34]. Furthermore, despite it was not significant, Perreira and Telles [20] found in Mexico a negative association between darker skin color and good self-rated health, in comparison to other Latin American countries. Thus, the sum of evidence suggests that in Mexico, skin color may be a more relevant feature than ethnic-racial identity in the distribution of economic and social benefits, and thus, in the better (or worse) well-being of specific groups and individuals [41].
Concerning the speaking or understanding of an Indigenous language, findings here do not support an association with self-rated health, due to the null results in the presence of control variables. Despite in previous studies it has been demonstrated a relationship between the use of Indigenous language, well-being [42, 43], and health [44, 45], the specific link with health perceptions has not been fully explored in the case of Latin American countries or in Mexico, suggesting an additional research line in future investigations.
The varying self-rated health outcomes across ethnoracial measures carry significant implications, particularly concerning the study of inequalities. One implication is the ongoing debate about the components defining racial or ethnic factors (see, e.g., [46]). These findings, in contrast to previous research, indicate the need for further exploration in this topic. Presently, it is uncertain whether findings within specific dimensions are exclusive and applicable across others. Therefore, to assess social outcomes—such as self-rated health—it is imperative to conduct studies incorporating more comprehensive measures, beyond traditional ones, especially those derived from external assessments or observers.
Secondly, it is evident that factors constituting ethnoracial identity are not homogenous or one-dimensional. Continual refinement of conceptualization and measurement is necessary to better grasp this concept. As noted by Roth [21], different approaches to evaluating characteristics yield varied results in social and economic disparities. Regarding skin color, it remains a controversial measure necessitating diverse approaches to provide comprehensive perspectives. While these approaches may be complementary, some might offer better insights into specific inequalities than others.
There are various potential mechanisms explaining these outcomes. According to Diderichsen et al. [47], distinctive social conditions—or social determinants of health (SDH)—rely on unbalanced social relations and power. Consequently, they promote exclusion and the lack of access to certain resources according to the structuring dimensions of identities (e.g., class, race, ethnicity, skin color, gender). It means the SDH model is based on the effects of stratified social factors, through inequalities, on health that are systematically manifested in social groups [48], particularly, in those more vulnerable. Thus, it can be pointed out that ethnicity and racialized attributes are elements of social stratification, especially in societies in which these attributes are differentiating characteristics in the access to health services, exposure to risk, and other factors that worsen the quality of life and wellness, as in the case of Mexico (see, e.g., [10, 23]).
In addition, several conditions may participate as mediators in the relationship between skin color and self-rated health. In the literature, it has been evidenced the role of socioeconomic and demographic traits as determinants of health and self-rated health. In the case of negative life experiences, our findings suggest that at least one proportion of the association between skin color and self-rated health can be explained by the effect of discrimination and life-course events, which is also coherent with previous literature [36]. Similarly, results on age, assets, and education support the idea that social and economic inequalities may be relevant predictors of perceptions of health [24, 49], confirming the notions of the SDH framework. In other words, in the analysis of outcomes related to ethnic-racial traits, it is not pertinent to overlook the influence as mediators (or moderators) of several individual and social situations.
Bearing the previous exposition in mind, we can state that hypotheses 1, 3, and 4 are not supported by our findings here, due to the null results in the associations between color skin measured by the interviewer, ethnic-racial self-ascriptions, speaking of an Indigenous language, and self-rated health. In contrast, hypothesis 2 is supported by our results, because, when skin color is measured by optical instruments, individuals with darker skin colors have less probability to report better perceptions of health; meanwhile, those with lighter tones have higher probabilities to show better self-rated health.
Conclusions
In the current manuscript, findings indicate that skin color may be associated with self-rated health depending on the method to measure color: null results when measured by external interviewers, and significant associations when evaluated by digital colorimeters. It means that skin color may change the likelihood of being in a higher category of self-rated health. In the case of darker tones, this likelihood is negative, whereas, in lighter skin tones, the probability is higher. Speaking an Indigenous language does not show the same association, despite in literature, they are somewhat related. In the case of ethnic-racial self-ascription, no identity is related to perceptions of health. Considering all these variables are included in the same models, it may imply a major role of skin color in health perception, in comparison to self-ascription or language.
Our results have some implications in public policies. First, considering self-rated health mirrors current health status, the role of skin color in health needs to be taken into account in the formulation, allocation, and delivery of culturally tailored health policies, programs, and interventions. Particularly, for those individuals and communities that have been excluded by the current economic model, among them, Indigenous, Afro-Mexicans, and individuals with certain racialized features (e.g., darker skin tones), but also, by those who do not have access to social and economic resources, such as education and assets.
Second, disparities in self-rated health expose the need for public health campaigns and educational interventions aimed at sensibilizing the role of skin color, ethnicity, race, and language on social outcomes. This also applies to the clinical context, where it is mandatory the training on cultural diversity to understand and address the needs of unique patient populations.
Third, future research must account for the measurement and multidimensionality of ethnic-racial attributes, and how these dimensions may have distinctive results in social and economic inequalities, as well as in perceptions and experiences, such as the self-rated health construct. This could involve developing more nuanced measurement instruments, methodologies, and studies and surveys to capture the complexity of racial and ethnic identities and its impact on health disparities.
Finally, although the cross-sectional design of the survey does not allow causality and the sample is mostly urban and non-indigenous, the present research provides empirical and nationally representative evidence for the study of ethnic-racial disparities in health perception, in contexts like the Mexican one.
Data Availability
Data are available at https://discriminacion.colmex.mx/?page_id=4655.
Notes
The PERLA palette was developed by Telles and Martínez Casas [34] in the context of the PERLA study. One of its purposes was the measurement of skin tone in the Latin American countries. However, considering the ample ethnic and skin tone diversity in the region, it included a wide spectrum of colors that do not completely match those found in the Mexican population. In sum, the PRODER palette is a more accurate representation of the skin-tone variability in Mexico than the PERLA color palette [17].
In previous research (see, e.g., [14]), color clustering has been used to avoid nonlinearities in the association of skin color with health. For this reason and to allow comparability, we grouped the interviewer’s color assessment variable into (approximately) quintiles.
The 2019 PRODER survey uses EDS and MDS scales in their dichotomized form, where respondents indicate whether they have lived the mentioned experienced or not [38].
References
Agudelo S, Romero V, Giraldo A. Percepcion del estado de salud en la region central colombiana: Encuesta Nacional de Salud, 2007. Rev Salud Pública. 2012;14(6):899–911.
Giacomino E. Autopercepción de la salud en mujeres rurales de la provincia de La Pampa. La aljaba. 2006;(10):123–140. http://www.scielo.org.ar/scielo.php?script=sci_arttext&pid=S1669-57042006000100008&lng=es&tlng=es.
Szwarcwald C, Damacena GN, de Souza Júnior PRB, de Almeida WdS, de Lima LTM, Malta DC, Stopa SR, Vieira MLFP, Pereira CA. Determinants of self-rated health and the influence of healthy behaviors: results from the National Health Survey, 2013. Rev Bras Epidemiol. 2015;18(2):33–44. https://doi.org/10.1590/1980-5497201500060004.
Altman C, Van Hook J, Hillemeier M. What does self-rated health mean? Changes and variations in the association of obesity with objective and subjective components of self-rated health. J Health Soc Behav. 2016;57(1):39–58. https://doi.org/10.1177/0022146515626218.
Malat J, Timberlake JM. County-level unemployment change and trends in self-rated health. Sociol Focus. 2013;46(1):25–46. https://doi.org/10.1080/00380237.2013.740990.
Krause N, Jay GM. What do global self-rated health items measure? Med Care. 1994;32(9):930–42. https://doi.org/10.1097/00005650-199409000-00004.
Idler E, Benyamini Y. Self-rated health and mortality: a review of twenty-seven community studies. J Health Soc Behav. 1997;38(1):21–37. https://doi.org/10.2307/2955359.
Ballesteros M, Krause M. Interseccionalidad en el estado de salud autopercibido de la población argentina (2005–2018). Rev Latinoam Poblac. 2022;(16). https://revistarelap.org/index.php/relap/article/view/12.
Roberts W, Martinez LM, Kauffman S. Racial/ethnic disparities in self-rated health: the mediating role of social trust. Sociol Focus (Kent, Ohio). 2010;43(4):349–368. https://doi.org/10.1080/00380237.2010.10571383.
Solís P, Güémez B, Lorenzo V. Por mi raza hablará la desigualdad: Efectos de las características étnico-raciales en la desigualdad de oportunidades en México, CDMX: OXFAM México; 2019.
Reyes-Martinez J. Cultural participation and subjective well-being in Latin America: does ethnic-racial ascription matter?. Sci Ann Econ Bus. 2021;(68):53–70. https://doi.org/10.47743/saeb-2021-0031.
Reyes-Martínez J. The association between ethnic-racial characteristics and subjective well-being: a perspective considering social inequalities. Submitted for publication, n.d.
Solís P, Krozer A, Arroyo C, Güémez B. Discriminación étnico-racial en México: una taxonomía de las prácticas. In: La métrica de lo intangible: del concepto a la medición de la discriminación. Zepeda J. Luna T. 2019. https://www.conapred.org.mx/wp-content/uploads/2022/07/MetricadeloIntangible_2019_Ax.pdf#page=56.
Flores R, Telles E. Social stratification in Mexico: disentangling color, ethnicity, and class. Am Sociol Rev. 2012;77(3):486–94. https://doi.org/10.1177/0003122412444720.
Reyes-Martínez J. Cultural participation and subjective well-being of Indigenous in Latin America. Appl Res Qual Life. 2022;17(2):635–54.
Cordano D. La discriminación étnico-racial y los centros de formación docente. Debates en Sociología. 1992;17:31–53.
Solís P, Güémez B, Campos R. Skin tone and inequality of economic outcomes in Mexico: a comparative analysis using optical colorimeters and color palettes, Sociol Race Ethnic. 2023:1–44. https://doi.org/10.1177/23326492231217232.
Solís P, Reyes-Martínez J. Categorias etnorraciales. In: De tez humilde: Características etnorraciales, discriminación y desigualdad social en México. Submitted for publication, n.d.
INEGI. Presentación de resultados. Censo de Población y Vivienda 2020. n.d. Available: https://www.inegi.org.mx/contenidos/programas/ccpv/2020/doc/Censo2020_Principales_resultados_ejecutiva_EUM.pdf.
Perreira K, Telles EE. The color of health: skin color, ethnoracial classification, and discrimination in the health of Latin Americans. Soc Sci Med. 2014;1982(116):241–50. https://doi.org/10.1016/j.socscimed.2014.05.054.
Roth. The multiple dimensions of race. Ethnic Racial Stud. 2016;39(8):1310–38. https://doi.org/10.1080/01419870.2016.1140793.
Solís P, Reyes-Martínez J. Discriminación percibida, características étnico-raciales y género. In: Interseccionalidad: Teoría antidiscriminatoria y análisis de casos. Universidad Autónoma Metropolitana; 2023. Manuscript subbmited for publication.
Trejo G, Altamirano M. The Mexican color hierarchy: how race and skin tone still define life chances 200 years after independence. In: The double bind: the politics of racial and class inequalities in the Americas. Washington, DC, American Political Science Association; 2016, pp. 3-16.
Villarreal A. Stratification by skin color in contemporary Mexico. Am Sociol Rev. 2010;75(5):652–78. https://doi.org/10.1177/0003122410378232.
Cano J, Mason P. Acculturation and the labor market in Mexico. IZA J Labor Policy. 2016;5(1). https://doi.org/10.1186/s40173-016-0077-6.
Campos R, Rivas C. El color de piel de los representantes de elección popular en México. Documento de trabajo. Proyecto sobre Discriminacion Étnico Racial en México (PRODER). 2020.
Solís P, Güémez B, Avitia M. Autoadscripción étnico-racial en México. Reporte de la Encuesta Proder # 2. El Colegio de México. 2020. Available: https://discriminacion.colmex.mx/. Accessed 5 07 2021.
Altamirano M. Estratificación racial en el uso de servicios y programas sociales en México. Percepciones, estereotipos y sesgos implícitos. 2020. https://discriminacion.colmex.mx/wp-content/uploads/2021/01/Altamirano.-2020.-DT_4_PRODER-final.pdf.
Roth W, Solís P, Sue C. Beyond money whitening: racialized hierarchies and socioeconomic escalators in Mexico. Am Sociol Rev. 2022;1–33. https://doi.org/10.1177/00031224221119803.
Ariza-Montoya JF, Hernández-Álvarez ME. Ethnic equity in accessing health services in Bogotá, Colombia, 2007. Rev Salud Pública. 2008;10:58–71.
Ortiz-Hernandez L, Ayala-Guzman CI, Perez-Salgado D. Health inequities associated with skin color and ethnicity in Mexico. Lat Am Caribb Ethn Stud. 2020;15(1):70–85. https://doi.org/10.1080/17442222.2020.1714846.
Bombak AE, Bruce SG. Self-rated health and ethnicity: focus on indigenous populations. Int J Circumpolar Health. 2012;71(1):1853.
COLMEX. Discriminación Étnico-Racial en México. s.f. Available: https://discriminacion.colmex.mx/?page_id=4389.
Telles E, Martínez Casas R. Pigmentocracias: color, etnicidad y raza en América Latina, Fondo de Cultura Económica. 2019.
Goodman E, Huang B, Schafer-Kalkhoff T, Adler NE. Perceived socioeconomic status: a new type of identity that influences adolescents’ Self-rated health. J Adolesc Health. 2007;41(5):479–87. https://doi.org/10.1016/j.jadohealth.2007.05.020.
Cano M, Portillo AGP, Figuereo V, Rahman A, Reyes-Martínez J, Rosales R, Cano M, Salas-Wright C, Takeuchi DT. Experiences of ethnic discrimination among US Hispanics: intersections of language, heritage, and discrimination setting. Int J Intercult Relat. 2021;84:233–50. https://doi.org/10.1016/j.ijintrel.2021.08.006.
Long JS, Freese J. Regression models for categorical dependent variables using stata. 3rd ed. Statacorp LP.: Stata Press Publication; 2014.
COLMEX. s.f.-a. Available: https://discriminacion.colmex.mx/wp-content/uploads/2021/06/cuestionario_proder.pdf. Accessed 04 07 2021.
Ly BCK, Dyer EB, Feig JL, Chien AL, Bino SD. Research techniques made simple: cutaneous colorimetry: a reliable technique for objective skin color measurement. J Investig Dermatol. 2020;140(1):3–12. https://doi.org/10.1016/j.jid.2019.11.003.
Barel AO, Clarys P, Alewaeters K, Duez C, Hubinon J-L, Mommaerts M. The Visi-Chroma VC-100®: a new imaging colorimeter for dermatocosmetic research. Skin Res Technol. 2001;7(1):24–31. https://doi.org/10.1034/j.160.
Monroy-Gómez-Franco L, Vélez-Grajales R. Skin tone differences in social mobility in Mexico: are we forgetting regional variance?. J Econ Race Policy. 2020. https://doi.org/10.1007/s41996-020-00062-1.
Little S. Great Aunt Edna’s vase: metaphor use in working with heritage language families. Fam J. 2019;27(2):150–5. https://doi.org/10.1177/1066480719833417.
McCarty T, Nicholas S, Chew K, Diaz N. Hear our languages, hear our voices: storywork as theory and praxis in indigenous-language reclamation. Daedalus. 2018;147(2):160–72. https://doi.org/10.1162/DAED_a_00499.
Browne-Yung K, Ziersch A, Baum F, Gallaher G. Aboriginal Australians’ experience of social capital and its relevance to health and wellbeing in urban settings. Soc Sci Med. 2013;1982(97):20–8.
Walsh M. ‘Language is like food..’: links between language revitalization and health and well-being. In: Hinton L, Huss L, Roche L, editors. The Routledge Handbook of Language Revitalization. New York, Taylor and Francis; 2018. pp. 5–12.
Brubaker R. Ethnicity, race, and nationalism. Ann Rev Sociol. 2009;35:21–42.
Diderichsen F, Evans T, Whitehead M. The social basis of disparities in health. In: Challenging inequities in health: from ethics to action. Oxford University Press; 2001. p. https://doi.org/10.1093/acprof:oso/9780195137408.003.0002.
Diderichsen F, Andersen I, Manuel C, Andersen A-MN, Bach E, Baadsgaard M, Brønnum-Hansen H, Hansen FK, Jeune B, Jørgensen T, Søgaard J. Health inequality—determinants and policies. Scand J Public Health. 2012;40(8):12–105. https://doi.org/10.1177/1403494812457734.
Samuano F, Ortega R. Desigualdad socioeconómica en México. Percepciones y determinantes. In: Altamirano M, Flamand L, editors. Desigualdades sociales en México. Legados y desafíos desde una perspectiva multidisciplinaria. El Colegio de México; 2021.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Javier Reyes-Martínez, Iván Alcántara, and Patricio Solís. The first draft of the manuscript was written by Javier Reyes-Martínez and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Reyes-Martínez, J., Santoyo, I.A. & Solís, P. Ethnoracial Disparities in Self-Rated Health: Exploring the Impact of Skin Color and Other Ethnoracial Characteristics in Mexico. J. Racial and Ethnic Health Disparities (2024). https://doi.org/10.1007/s40615-024-02002-3
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s40615-024-02002-3