
Abstract
Background
Historically, Blacks and Hispanics have had lower opioid-involved overdose death rates in Connecticut (CT). We examined if a shift has taken place where rates of Black fatal overdoses have now surpassed Whites in the state.
Methods
Drug overdose fatality rates were calculated by number of deaths per year per 100,000 population from 2012 to 2019 in Connecticut. Measures were by race (White, Hispanic, Black, and Asian or Pacific Islander), age groups, and types of drugs, including fentanyl, heroin, cocaine, and other opioids. Poisson regression was used to test the interactions (race × age); joinpoint regression analysis was used to evaluate trend lines of fatality rate by racial/ethnic group within each age group with a significance level of p < 0.05.
Results
Drug overdose fatality rates in CT from 2012 to 2019 showed a significant increase for all races combined, estimated 3.6 deaths per 100,000 population per year. For Whites, overdose deaths were 4.6 per year from 2012 to 2017 with no change from 2017 to 2019. The overdose fatality rate for Hispanics was 3.0 and for Asian or Pacific Islanders 0.6 per year from 2012 to 2019. For Blacks, the death rates were statistically flat between 2012 and 2014; however, from 2015 to 2019, this group saw the largest average increase of 6.0 overdose deaths per 100,000 population each year. By 2019, the overdose fatality rate was higher in Blacks than in Whites, (39 vs. 38 per 100,000, respectively). Further, Blacks ages 50 years and over reported the highest overdose fatality rates among all race/age groups, an increase of 8.5 deaths per 100,000 population since 2014.
Conclusions and Relevance
Connecticut is a microcosm of the opioid overdose trend in the New England region of our country. The majority of overdose deaths in CT involved illicit drugs, fentanyl, heroin, and cocaine, rather than prescription drugs. Blacks 50-years-old and over showed the fastest growing overdose death rates. Opioid deaths are now shifting to the Black community, creating an urgent public health crisis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The opioid epidemic has been declared a US national public health emergency [1]. The ongoing epidemic has shifted from prescription opioid-involved overdoses beginning in the 1990s to heroin-involved overdose in 2010 and then to synthetic opioid-involved overdoses in 2014 [2, 3]. With the recent introduction of synthetic opioids, such as illicitly manufactured fentanyl, the USA has observed an increase in opioid-related overdoses and deaths [1]. In 2017, 58.9% of the overdose deaths were linked to synthetic opioids [4]. In 2018, opioid fatality overdoses increased six-fold to 47,000 deaths when compared to the number of opioid-involved deaths in 1999 [5].
Opioid-involved overdose deaths have unprecedentedly increased among minorities, especially Blacks and Hispanics [4, 6,7,8,9,10,11,12,13]. Recent publications have shown a temporal trend in racial/ethnic disparities of opioid-involved overdose deaths since 1999 [4, 7, 8, 10,11,12]. The growth of opioid deaths among Blacks has started outpacing Whites [7], while the opioid deaths among Hispanics is still lower when compared to Whites. [4, 8] Similarly, recent studies on short-term trends (years 2015 to 2017 and 2017 to 2018) evidenced widening racial ethnic gaps in opioid overdose fatalities by identifying complex health disparities in high-risk subgroups [4, 9, 11, 14, 15], such as Black older women and men. Black women and men 50 years old and over presented the fastest growing opioid overdose fatality rates when compared to other races and age groups [4, 8, 9, 11]. Due to the complex patterns of opioid-involved overdose deaths within subgroups, more research is warranted to comprehensively examine temporal trends by age and racial/ethnic groups.
Geographically, the northeast region of the USA, including Connecticut (CT), has been a hotspot for opioid/fentanyl overdoses [16, 17]. Following the national trends in drug overdose fatalities, generally, almost all populations began to rise with the introduction of synthetic opioids; in Whites, a 79% increase per year was observed and in Blacks a 107% increase per year was observed [4, 18]. Furthermore, the use of heroin and its mortality rates in minorities and Whites have also recently begun to converge [17]. Specifically, from 2014 to 2015, CT had statistically significant increases in drug overdose death rates [16]. In 2016, there were 917 accidental drug-related deaths in CT alone. Of these deaths in the past year, 75% were male, 78% White/non-Hispanic, 94% involved opioids (along with other substances), 30% involved cocaine, 28% involved alcohol, and 28% involved benzodiazepines [19]. The typical profile for an overdose victim in CT in 2016 was a non-Hispanic White male between the ages of 30 and 59 who used opioids, such as heroin/fentanyl and other substances, and overdosed that day along with one or two other people [19].
We therefore proposed a comprehensive statistical approach to address the rise in drug overdose deaths in all populations in CT. The study was based on the most recent available CT overdose mortality data ranging from 2012 to 2019 and investigated changes over time of overdose deaths related to the use of fentanyl, heroin, and other prescription and non-prescription opioids in age-stratified racial/ethnic groups (Whites, Blacks, Hispanics, and Asian or Pacific Islanders (APIs)). The goal of the study was to analyze data regarding the extent of health disparities in overdose fatality in minority populations and to provide better-defined information regarding possible prevention and intervention strategies to decrease overdose deaths.
Methods
The study data ranged from 2012 to 2019 and focused on the accidental overdose deaths from the Connecticut Office of the Chief Medical Examiner (OCME) (https://portal.ct.gov/OCME/Statistics). Accidental deaths were defined as any deaths caused by external, violent, or accidental means and were not related to any intentional or criminal acts or suicidal intention [3]. Deaths due to drugs were identified by toxicology test and noted in the death certificate. Due to no precise mechanism to ascertain which drugs contributed to the cause of death, multiple drugs were often listed. Thus, the overdose information reported in this research is defined as the overdose involving a particular drug type. Based on the different distinct patterns of overdose history in the USA, we selected to report the overdose fatality, which involved the use of the following drugs/drug categories: fentanyl and fentanyl analogue, heroin, cocaine, and other opioids including oxycodone, oxymorphone, hydrocodone, methadone, tramadol, and morphine. In the current database, each of these drugs were determined by OCME based on the toxicity report, death certificate, as well as a scene investigation using a complex algorithm to identify every possible case (https://data.ct.gov/Health-and-Human-Services/Accidental-Drug-Related-Deaths-2012-2018/rybz-nyjw).
Racial/ethnic groups included in this study were categorized as Non-Hispanic Whites (Whites), Hispanics, Non-Hispanic Blacks (Blacks), and Non-Hispanic APIs. Due to the exclusion criteria of other racial/ethnic groups, a small number of racial/ethnic groups (e.g., American Indian or Alaska Native, other, or missing race/ethnicity) were excluded from the mortality data. The number/percent of overdose events were also excluded. Counts for such missing data ranged from 3 to 16 deaths from 2012 to 2019 in Connecticut. Age groups used for descriptive analysis included < 20, 20–34, 35–49, 50–64, and 64+.
Statistical Methods
Crude fatality rates per year per 100,000 were calculated using the number of opioid involved deaths from the CT OCME public dataset (https://portal.ct.gov/OCME/Statistics) along with the 2000 US Census from the National Center for Health Statistics (https://portal.ct.gov/DPH/Health-Information-Systems%2D%2DReporting/Population/Annual-State%2D%2DCounty-Population-with-Demographics) for the per year base population estimates for each age group and racial/ethnic group. Overall, fatality rates were generated from deaths involved with all drugs in the study. Rates (e.g., number of persons dying from an overdose relative to the number of people at risk for that group during a specified period (year)) were analyzed using Poisson regression [20] in the GENMOD procedure in SAS. The predictors were time (years between 2012 and 2019), race (White, Hispanic, Black and API), and age plus the interaction (race × age), which assessed the extent to which age modified the association of mortality and race reported in the figure legend of the trend plot. If the interaction (race × age) was significant at 0.05, joinpoint analysis was performed by race within three ages groups (20–34, 35–49, and 50+) and ages < 20 were excluded due to the small numbers of death.
Joinpoint regression models were used to evaluate trend lines and graphic displays of the relationships over time [21,22,23,24,25,26] were created using Joinpoint Trend Analysis Software [21]. To estimate changes of crude fatality rates by groups (e.g., age, race, types of drugs) over time, the algorithm tested if the slope of each regression line was statistically different from zero using a two-sided alpha level of 0.05. The regression analysis used a weighted least square (WLS) approach that uses the reciprocal of the SEs for weights. One joinpoint was used as default for 7–11 data points [21]. When a significant trend line was identified it was compared across all race groups. All p values reported in the text are from the Joinpoint analysis, except where noted.
Results
In Connecticut, there were 6236 fatal overdoses, 175 deaths per 100,000 population from 2012 to 2019 (Table 1). About two thirds were between 20 and 49 years old, a quarter were 50 to 64 years old, and the remaining 3% were either younger than 20 or older than 65 years old. Of all overdose deaths, 78% were White, 12% Hispanic, 9% Black, and 0.7% API. Three quarters were male.
The crude annual opioid-involved fatality rate sharply increased from 2012 to 2019, with a slight pause in 2018 (Fig. 1). Fentanyl-involved crude fatality rates showed sharper increases from 2016 to 2019. Heroin involved fatality rates increased from 2012 to 2016 and slightly declined since then. For other opioids, no notable changes occurred from 2012 to 2019.

Overdose fatality per 100,000 population by types of drugs in Connecticut: 2012–2019
Racial/Ethnic Overdose Fatality Differences by Age and by Types of Drugs Involved
Overdose fatality involved with all drugs
Comparing the overdose fatality by racial/ethnic status (Fig. 2 and Supplement Table 1), the absolute increase from 2012 to 2014 was 13.8 per 100,000 population (123% increase) for Whites, 7.0 for Hispanics (91% increase), and 1.8 for APIs (16% increase). In contrast, in the last 5 years, from 2015 to 2019, for all persons, the absolute increase was 12.5 per 100,000 population (~ 50% increase since 2015), with notable increases for Hispanics at 6.4 (~ 112% increase) and Blacks at 25.4 (~ 189% increase).

Overdose fatality involved with all drug type use in Connecticut from 2012 - 2019, by racial/ethnic status per 100,000 population by Joinpoint analysis trend lines. A test for (race ´ year) interaction indicates mortality rates varied across race/ethnic group and time period 2012 to 2019 (Poisson regression analysis, (p = 0.002, χ2 = 44.2). Joinpoint analysis presents solid lines as increasing over time (p < 0.05). For Blacks and Whites, a breakpoint indicates a change in the trend of mortality. A dotted line indicates no change during that time period (p > 0.05).
Figure 2 shows the Joinpoint analysis results for drug overdose fatality rates from 2012 to 2019 by race. For the total fatality rate, there was a significant increase during this period (p < 0.05, red line) with a Joinpoint-estimated increase per year of 3.6 per 100,000 population. For Whites (purple), the estimated increase per year was 4.6 from 2012 to 2017 (p < 0.05) and flat (i.e., no change) from 2017 to 2019. For Hispanics (blue), the increase per year was 3.0 deaths during the same period (p < 0.05). APIs had the lowest fatalities of any group with 0.6 (p < 0.05). For Blacks, the rates were statistically flat between 2012 and 2014; however, from 2015 to 2019, this group saw the largest average increase of 6.0 overdose deaths per 100,000 population each year. By 2019, the overdose fatality rate among Blacks was at a similar level of Whites (39 vs. 38 per 100,000, respectively).
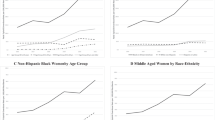
Poisson regression results of the (race × age) interaction was significant (p < 0.001). Figure 3A shows the detailed age-race Joinpoint analysis results for all drug involved overdose fatality rates from 2012 to 2019. There were significant increases after 2014 (p < 0.05, red line) with annual Joinpoint-estimated increases: 4.8 additional deaths per 100,000 population per year for individuals ages 20–34 (Fig. 3B), 6.8 for ages 35–49 (Fig. 3C), and 5.1 for ages 50 and over (Fig. 3D).

A) All-cause overdose fatality per 100,000 population by age groups from 2012 - 2019. B) Overdose fatality in age groups 20–34 by racial/ethnic status. C) Overdose fatality in age groups 35–49 by racial/ethnic status. D) Overdose fatality in age groups 50+ by racial/ethnic status. Joinpoint analysis presents solid lines as increasing over time (p < 0.05). A dotted line indicates no change during the specific period (p > 0.05).
In general, the fatality rates for Whites, Hispanics, and Blacks of all ages showed an increase overtime, while the fatality rate for APIs remained relatively flat. However, the fatality rate in Blacks ages 50 years and over surpassed the rates of Whites and Hispanics (8.5 deaths per 100,000 population per year) since 2014. This was the highest increase among all race–age groups.
Fentanyl-involved overdose fatality
Figure 4A shows the Joinpoint analysis results for fentanyl involved overdose fatality rates from 2012 to 2019, by age and race. After 2014, there were significant increases (p < 0.05) with annual Joinpoint-estimated increases: 8.9 additional deaths per 100,000 population per year in individuals ages 20–34, 10.0 in ages 35–49, and 4.2 in ages 50 and over (Fig. 4A).

A) Fentanyl involved overdose fatality per 100,000 population by age groups. B) Fentanyl involved overdose fatality in age groups 20–34 by racial/ethnic status. C) Fentanyl involved overdose fatality in age groups 35–49 by racial/ethnic status. D) Fentanyl involved overdose fatality in age groups 50+ by racial/ethnic status. Joinpoint analysis presents solid lines as increasing over time (p < 0.05). A dotted line indicates no change during the specific period (p > 0.05).
In general, the fatality rates for Whites, Hispanics, and Blacks of all ages showed similar increases over time, while the fatality rate for APIs remained relatively flat (Fig. 4B, 4C and 4D). Fatality rates in Whites ages 20–34 (Fig. 4B) and 35–50 (Fig. 4C) estimated the highest increases of > 11 additional deaths per 100,000 population per year. In contrast, Blacks, 50 years old and over (Fig. 4D) surpassed rates of Hispanics and Whites (additional 9.3, 6.3, and 3.4 deaths per 100,000 population per year, respectively) since 2015.
Heroin overdose fatality
Figure 5 shows the Joinpoint analysis results for heroin involved overdose fatality rates from 2012 to 2019 by age and race. There were significant increases of fatality rates by age from 2012 until 2016, estimated 2.7–4.1 per 100,000 population per year for age groups 20–34, 35–49, and 50–64 (p < 0.05), and no notable changes through 2019 (Fig. 5A).

A) Heroin involved overdose fatality per 100,000 population by age groups. B) Heroin involved overdose fatality in age groups 20–34 by racial/ethnic status. C) Heroin involved overdose fatality in age groups 35–49 by racial/ethnic status. D) Heroin involved overdose fatality in age groups 50+ by racial/ethnic status. Joinpoint analysis presents solid lines as increasing over time (p < 0.05). A dotted line indicates no change during the specific period (p > 0.05).
Regarding racial/ethnic status within each age group, Blacks and Hispanics ages 50 years old and over were the only groups with annual increases of overdose deaths from 2015 to 2019 (p < 0.05) (Fig. 5D). Blacks 50 years old and over showed a significant continuous increase of an additional 4.9 deaths per 100,000 population per year (p < 0.05), the highest increase among all race–age groups.
Cocaine and other opioid-involved overdose fatality
Supplemental Figure 1 shows the Joinpoint analysis results for cocaine-involved overdose fatality rates from 2012 to 2019 by race. There was a significant increase during all years of 1.3 per 100,000 population (p < 0.05, red line) for the total fatality rate.
Regarding racial/ethnic status, Whites and Hispanics presented a similar annual increase of about one death per 100,000 population per year from 2012 to 2019 (p < 0.05) while no changes were observed in APIs. In contrast, there were no changes in Blacks from 2012 to 2014. However, since 2014, there was a significant increase of 3.0 deaths per 100,000 per year (p < 0.05). In 2019, the fatality rate in Blacks was three times higher than that of Whites and Hispanics. Analysis by age and racial/ethnic status showed a significant increase from 2012 to 2019 in Whites and Blacks. Cocaine overdose deaths decreased over time in the older age group when compared to the younger age groups. In contrast, cocaine overdose deaths increased continuously in older Blacks, particularly in those 50 years old and over.
Supplemental Figure 2 shows data for other opioid overdose fatality rates for total and racial/ethnic status. No group met the criteria for Joinpoint change overtime (p < 0.05). Overall, other opioid use fatality rates were flat from 2012 to 2019.
Discussion
Overdose fatalities involving the use of fentanyl in CT reported here are parallel with what has occurred in the USA [16, 27,28,29,30]. Since 2014, the USA has experienced a drug overdose epidemic characterized by a shift in mortality from heroin-related to synthetic opioid-related, primarily illicitly manufactured fentanyl [16, 26,27,28,29,30]. Fentanyl and fentanyl analogues are easily and cheaply manufactured and are considerably more profitable to dealers/distributors than heroin [27]. Fentanyl is often added to or sold as heroin in many geographic regions of the USA [27]. Since 2015, higher levels of fentanyl mortality (> 100%) have been reported in Black and Hispanic populations as compared to Whites. Historically, these minority groups had lower opioid-involved overdose death rates [4]. A study by Lippold and colleagues reported 60% of opioid-involved overdose deaths in US metropolitan areas in 2017, with synthetic opioids reaching 70% of all opioid-involved overdose deaths among Blacks, 54.2% among Whites, and 56.0% among Hispanics [4]. Recently, an increase in synthetic opioid-involved overdose deaths has been observed in Black populations between the ages of 45 and 54 (19.3 to 41.9 per 100,000 population) and between ages 55 and 64 years (21.8 to 42.7 per 100,000 population) [4]. Further, a recent report stated that compared to all other populations, Blacks/African Americans had the highest increase in overdose death rates involving synthetic opioids like fentanyl and fentanyl analogs [31, 32]. Our analysis echoes the US fatal overdoses during the same period and shows a steady, sharp increase of overdose fatalities in all racial/ethnic groups (White, Black, and Hispanic), particularly in older Blacks ages 50 and over, in CT. Deaths involving fentanyl use exceeded those involving heroin use in CT.
Policy initiatives to expand drug overdose treatments should target reduction of opioid use disorder in Connecticut [33]. In recent years, Connecticut has been expanding medication-assisted treatments including buprenorphine, extended-release naltrexone, and other FDA-approved medications, adding care management and peer supports and other harm reduction initiatives, and targeting at-risk populations (https://www.samhsa.gov/grants-awards-by-state/ct/discretionary/all/details?page = 34; https://portal.ct.gov/DMHAS/Programs-and-Services/Opioid-Treatment/Opioid-Treatment). However, in general, small portions of those with addiction who need treatment actually received it at a specialty facility (https://www.whitehouse.gov/wp-content/uploads/2020/02/2020-NDCS-Treatment-Plan.pdf). Increases in overdose fatalities with the use of heroin and cocaine were observed in CT [16, 17]. There are limited resources to treat individuals with cocaine and heroin addiction and people of color are usually the ones who have less access to adequate treatment, such as medication-assisted treatment [34]. Thus, health disparities in treating heroin and cocaine addictions has been further enlarged.
The overdose fatality trends from 2012 to 2019 in Connecticut reflect similar trends observed in the USA [4, 7,8,9,10,11,12,13,14, 30, 32,33,34,35]. Understanding racial and ethnic health disparities can shine a light on the increase in overdose fatalities involving fentanyl and polydrug use in CT. It is important to understand the root causes that underlie previous and current drug-specific sub-epidemics (e.g., opioids, cocaine), as well as both supply and demand factors (supply factors—lower prices, increased potency; demand factors—despair, loss of purpose, and dissolution of communities) to merge and drive mortality in an exponential trajectory [36].
Further, our data support and are consistent with previous study findings of the rise of fentanyl-involved deaths, as well as the increase in other illicit drug use (heroin and cocaine) in the Black population [4,5,6,7,8,9,10,11,12,13,14]. However, there is a lack of detailed drug fatality data on identifying annul trends for these specific high-risks groups. In our study, we showed that older Blacks, ages 50 and over, in CT, showed the sharpest increase in heroin-involved fatalities overall. We also showed that there has been an increase in this group for cocaine fatalities since 2012 and fentanyl since 2015. Future policies and interventions to prevent overdose fatalities with specific targeted substances involved should target this group. In recent years, Connecticut has expanded resources including harm reduction to populations in need; however, as a top priority, further investigation and policy may be needed to study the older Black population. Health providers and community outreach programs should be informed about this current highest risk group. In the end, the overall implication of this study demonstrates that further data are required to study higher risk subgroups and risk factors by age and race, particularly in different geographic regions.
To combat the opioid epidemic crisis properly in the USA and CT, a better understanding regarding opioid use and the effects by age and race and ethnicity will be necessary [32, 33]. Focusing on the population as a whole can cause inaccurate interpretation of data, such as an underestimation of the effect of the opioid crisis on each racial/ethnic population. Throughout the years, the opioid epidemic has shifted drastically from prescription misuse in the White population to now heroin and illicit drugs, such as fentanyl, affecting both the White and Black communities [17, 32, 33 ]. A better understanding on the opioid epidemic by age and race is necessary, and this in turn will allow for a better design of access strategies to treat people who would not normally receive the proper help, such as people in large metropolitan areas with low income or lack of insurance [37]. One strategy can include the ease of access to resources such as naloxone distribution and medication assisted treatment for higher risk groups.
The findings in this study are subject to several limitations. First, drug-related causes of deaths in CT are not only based on toxicology reports but also from death certificates and scene investigations. The drug classification used in this analysis was not based on ICD-10 codes but was ascertained directly from the CT OCME databases. Second, variability of the quality and completeness of toxicological testing in death certificate data has been noted [38,39,40], even though CT is classified as having “very good to excellent reporting” by the CDC [41]. Incompleteness in data reporting may affect the generalizability of the results. Third, the data used in this study do not include overdoses classified as relating to intentional acts (or undetermined intent). Issues in the classification of injury intent for drug poisoning incidents in death certificate data can be problematic [42], particularly since the extent of these classification issues vary by race/ethnicity [43]. Given these issues, a more accurate representation would be to include all drug overdose mortality, regardless of intent. We suggest that for future studies both types of overdose information be included (accidental and intentional). Fourth, as a secondary data analysis, the ability to justify some important risk factors of substance abuse such as stress is limited and would be beneficial for future studies.
Despite some limitations, strengths of this study include the use of detailed drug category data, 2019 data, to illustrate and understand the racial/ethnic differences in overdose fatalities. The age-stratified analyses also provide detailed racial/ethnic disparities in specific drug-involved overdose fatalities over time.
In summary, we found increased rates of opioid use and overdoses in Blacks ages 50 years and over in CT, which is a microcosm of the Northeast region in our country [33]. The data point to the fact that opioid-involved deaths may be shifting to the Black community. We believe that it is critical for addiction treatments in Black communities and other historically oppressed groups mirror that of White communities. Treatments such as naloxone and medication-assisted treatments should be culturally competent to specifically address the needs of people of color, particularly in the older Black population (50-years-old and over) in CT.
References
Santoro TN, Santoro JD. Racial bias in the US opioid epidemic: a review of the history of systemic bias and implications for care. Cureus. Published online 2018. https://doi.org/10.7759/cureus.3733
Centers for Disease Control and Prevention. 2019 Annual Surveillance Report of Drug-Related Risks and Outcomes — United States Surveillance Special Report. Centers for Disease Control and Prevention, U.S. Department of Health and Human Services. https://www.cdc.gov/drugoverdose/pdf/pubs/2019-cdc-drug-surveillance-report.pdf. Accessed July 5, 2020.
Ahmad FB, Rossen LM, Sutton P. Provisional drug overdose death counts. National Center for Health Statistics. Published 2010. https://www.cdc.gov/nchs/nvss/vsrr/drug-overdose-data.htm. Accessed November 5, 2020.
Lippold KM, Jones CM, Olsen EOM, Giroir BP. Racial/ethnic and age group differences in opioid and synthetic opioid-involved overdose deaths among adults aged ≥18 years in metropolitan areas – United States, 2015–2017. MMWR Morb Mortal Wkly Rep. Published online 2019. 10.15585/mmwr.mm6843a3
Centers for Disease Control and Prevention. Opioid overdose: data analysis and resources. https://www.cdc.gov/drugoverdose/data/analysis.html. Accessed October 6, 2020
Substance Abuse and Mental Health Services Administration. The opioid crisis and the Black/African American population: an urgent issue. Publication No. PEP20-05-02-001. Office of Behavioral Health Equity. Substance Abuse and Mental Health Services Administration. https://store.samhsa.gov/sites/default/files/SAMHSA_Digital_Download/PEP20-05-02-001_508%20Final.pdf. Accessed October 1, 2020.
Furr-Holden D, Milam AJ, Wang L, Sadler R. African Americans now outpace whites in opioid-involved overdose deaths: a comparison of temporal trends from 1999 to 2018. Addict. 2020. doi.10.11.11/add.15233.
Shiels MS, Freedman ND, Thomas D. Berrington de Gonzalez A. Trends in US drug overdose deaths in non-Hispanic black, Hispanic, and non-Hispanic white persons, 2000–2015. Ann of Intern Med. 2018;168(6):453–5.
Wilson N, Kariisa M, Seth P, Smith H, Davis NL. Drug and opioid-involved overdose deaths—United States, 2017–2018. MMWR. 2020;69(11):290–7.
Ray B, Lowder E, Bailey K, Huynh P, Benton R, Watson D. Racial differences in overdose events and polydrug detection in Indianapolis, Indiana. Drug Alcohol Depend. 2020;206:107658.
Cano M. Racial/ethnic differences in US drug overdose mortality, 2017–2018. Addict Behav. 2021;112:106625.
Lippold K, Ali B. Racial/ethnic differences in opioid-involved overdose deaths across metropolitan and non-metropolitan areas in the United States, 1999–2017. Drug Alcohol Depend. 2020;212:108059.
Kandel DB, Hu MC, Griesler P, Wall M. Increases from 2002 to 2015 in prescription opioid overdose deaths in combination with other substances 2017. Drug Alcohol Depend. 2017;178:501–11.
Barboza GE, Angulski K. A descriptive study of racial and ethnic differences of drug overdoses and naloxone administration in Pennsylvania.
Cano M. Drug Overdose deaths among US Hispanics: trends (2000–2017) and recent patterns. Subst Use Misuse. 2020;55(13):2138–47.
Kara J, Rigg M. Fentanyl continues to drive deadly overdose epidemic.
Alexander MJ, Kiang MV, Barbieri M. Trends in black and white opioid mortality in the United States, 1979–2015. Epidemiol. Published online 2018. https://doi.org/10.1097/EDE.0000000000000858
Wolfe S. The Opioid Overdose Antidote. 2017.
Stokes ME., Dvaid CS., Koch GG. Categorical data analysis using the SAS system. 2nd Edition. The SAS Institute; 2012.
National Cancer Institute, Division of Cancer Control and Population Sciences SRP. Joinpoint Trend Analysis Software. Published 2020. Accessed September 5, 2020. https://surveillance.cancer.gov/joinpoint/
Kim HJ, Luo J, Kim J, Chen HS, Feuer EJ. Clustering of trend data using joinpoint regression models. Stat Med. Published online 2014. https://doi.org/10.1002/sim.6221
Tyczynski JE, Berkel HJ. Mortality from lung cancer and tobacco smoking in Ohio (U.S.): will increasing smoking prevalence reverse current decreases in mortality? Cancer Epidemiol Biomark Prev. 2005;14(5):1182–7.
Doucet M, Rochette L, Hamel D. Incidence, prevalence, and mortality trends in chronic obstructive pulmonary disease over 2001 to 2011: a public health point of view of the burden. Can Respir J. 2016. 10.1155/2016/7518287
John U, Hanke M. Liver cirrhosis mortality, alcohol consumption and tobacco consumption over a 62 year period in a high alcohol consumption country: a trend analysis. BMC Research Notes. Published online 2015. 10.1186/s13104-015-1808-2
Kim HJ, Fay MP, Feuer EJ, Midthune DN. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med. Published online 2000. 10.1002/(SICI)1097-0258(20000215)19:3<335::AID-SIM336> 3.0.CO;2-Z
Robeznieks A. Black patients less likely to get treatment for opioid-use disorder. American Medical Association. Nov 19, 2019. https://www.ama-assn.org/delivering-care/opioids/black-patients-less-likely-get-treatment-opioid-use-disorder. Accessed 10-21-2020.
Drug Enforcement Administration. Fentanyl remains the most significant synthetic opioid threat and poses the greatest threat to the opioid user market in the United States. https://www.dea.gov/sites/default/files/2018-07/PRB-DIB-003-18.pdf. Accessed November 5, 2020.
Centers for Disease Control and Prevention. Increases in fentanyl drug confiscations and fentanyl-related overdose fatalities. https://www.cdc.gov/drugoverdose/data/fentanyl-le-reports.html. Accessed December 3, 2018.
Jones C, Einstein E, Compton W. Changes in synthetic opioid involvement in drug overdose deaths in the United States, 2010–2016. JAMA. 2018;319(17):1819–21. https://doi.org/10.1001/jama.2018.2844.
Scholl L, Seth P, Kariisa M, Wilson N, Baldwin G. Drug and opioid-involved overdose deaths—United States, 2013–2017. MMWR Morb Mortal Wkly Rep. 2018;67(5152):2013–7. https://doi.org/10.15585/mmwr.mm675152e1.
Substance Abuse and Mental Health Services Administration (SAMHSA). Medication-assisted treatment: statutes, regulations, and guidelines. https://www.samhsa.gov/medication-assisted-treatment/statutes-regulations-guidelines. Accessed June 10, 2020.
Spencer M, Warner M, Bastian B, Trinida J, Hedegaard H. Drug overdose deaths involving fentanyl, 2011–2016. National Vital Stat Rep 2019;68(3):1-9. https://www.cdc.gov/nchs/data/nvsr/nvsr68 nvsr68_03-508.pdf. Accessed July 30, 2020.
Substance Abuse and Mental Health Services Administration. The opioid crisis and the Black/African American population: an urgent issue. https://store.samhsa.gov/sites/default/files/SAMHSA_Digital_Download/PEP20-05-02-001_508%20Final.pdf. Accessed July 30, 2020.
Minnesota State Department of Health. Race rate disparity in drug overdose death. https://www.health.state.mn.us/communities/opioids/documents/raceratedisparity.pdf. Accessed July 30, 2020.
Jalal H, Buchanich J, Roberts M, Balmert L, Zhang K, Burke D. Changing dynamics of the drug overdose epidemic in the United States from 1979 through 2016. Sci. 2018;362(6408). https://doi.org/10.1126/science.aau1184.
Wu LT, Zhu H, Swartz MS. Treatment utilization among persons with opioid use disorder in the United States. Alcohol Depend. 2016. https://doi.org/10.1016/j.drugalcdep.2016.10.015
Ruhm CJ. Geographic variation in opioid and heroin involved drug poisoning mortality rates. Am J Prev Med. 2017;53(6):745–53.
Slavova S, Delcher C, Buchanich JM, Bunn TL, Goldberger BA, Costich JF. Methodological complexities in quantifying rates of fatal opioid-related overdose. Curr Epidemiol Rep. 2019;6(2):263–74.
Tote KM, Bradley H, Martin EG, Yucel R, Rosenberg ES. Factors associated with incomplete toxicology reporting in drug overdose deaths, 2010–2016. Ann Epidemiol. 2019;38:65–9.
Kariisa M, Scholl L, Wilson N, Seth P, Hoots B. Drug overdose deaths involving cocaine and psychostimulants with abuse potential—United States, 2003–2017. MMWW. 2019;17(68):388.
Rockett IRH, Caine ED, Connery HS, Nolte KB, Nestadt PS, Nelson LS, Jia H. Unrecognised self-injury mortality (SIM) trends among racial/ethnic minorities and women in the USA. Inj Prev. (2019).
Office of the Chief Medical Examiner CT. Connecticut Accidental Drug Intoxication Deaths. Int J Drug Policy. 2020;78:102718. http://www.ct.gov/ocme/lib/ocme/AccidentalDrugIntoxication2012-2017.pdf.16. Accessed April 6, 2018.
Rockett IRH, Caine ED, Connery HS, Nolte KB. Overcoming the limitations of ‘accident’ as a manner of death for drug overdose mortality: case for a death certificate checkbox. Inj Prev. (2020). Epub Sept 2020.
Acknowledgments
The authors would like to acknowledge support from the National Institutes of Health (NIH): NIH BUILD (TL4GM118971) for funding his work (C.T.L.).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(DOCX 695 kb)
Rights and permissions
About this article

Cite this article
Wu, Z.H., Yong, Q., Walker, J.M. et al. Fentanyl, Heroin, and Cocaine Overdose Fatalities are Shifting to the Black Community: An Analysis of the State of Connecticut. J. Racial and Ethnic Health Disparities 9, 722–730 (2022). https://doi.org/10.1007/s40615-021-01007-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40615-021-01007-6