
Abstract
Objectives
This study examines the association between morbidity (i.e., chronic health conditions) and self-rated health (SRH) with the aim of testing the within-group and across-group validity of SRH across nine ethnic groups: non-Latinx White, Mexican, Puerto Rican, Cuban, African American, Afro-Caribbean, Chinese, Filipino, and Vietnamese Americans. In addition, we assess whether acculturation (i.e., nativity, years of US residency, language of interview) and health-related factors (e.g., mental disorder) account for ethnic distinctions in SRH.
Design
Data are from the National Survey of American Life (NSAL) and the National Latino and Asian American Study (NLAAS) (N = 8338). Weighted proportions and means for SRH and chronic conditions are reported. Ordered logistic regression analysis is used to determine ethnic group patterns in SRH.
Results
Despite evidence of within-group validity of SRH for each ethnic group, our results seriously challenge the across-group validity of SRH. For example, Chinese and Vietnamese respondents report lower SRH despite having fewer chronic conditions relative to non-Latinx Whites. Moreover, Mexican Americans report fewer chronic health problems but lower SRH compared to non-Latinx Whites. Acculturation factors (e.g., language of interview) partially explain the Mexican–White difference in SRH. Among Chinese Americans, completing an interview in English is associated with higher SRH relative to those who completed an interview in Chinese.
Conclusion
These findings have implications for health disparities research that uses SRH as the dependent measure. Studies that compare the health profiles of diverse ethnic groups should use the SRH measure with caution, as SRH does not align with ethnic patterns of morbidity.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Self-rated health (SRH) is one of the most commonly used health measures in social science and health services research [1]. Given its significant association with both mortality and morbidity [2], it is heralded as a reliable health measure. Furthermore, SRH is frequently used in studies to ascertain racial and ethnic health disparities [3, 4]. A general assumption is that SRH and chronic conditions are inversely correlated, and this correlation is similar across ethnic groups. In other words, SRH is presumably rated more favorably under the condition of experiencing fewer physical health ailments. Yet emerging research demonstrates that ethnic patterns for subjective health measures like SRH do not always align with objective health measures [5, 6]. Consequently, despite its prominence in the literature, the construct validity of this measure has recently been called into question [5, 7,8,9,10,11].
The underlying issues for understanding the paradoxical incongruence between subjective and objective measures across ethnic groups are rooted in challenges with the within-group and across-group validity of the SRH measure. Prior research suggests that the “presumption of cross-cultural uniformity of assessment” can be rife with challenges to validity across ethnic groups [12]. The primary aim of the current study is to investigate whether health patterns by ethnicity are aligned for objective (i.e., morbidity) and subjective (i.e., SRH) health assessments. Challenges to the use of SRH across ethnic groups may reflect actual between-group variations in health, differences in evaluations or reporting styles, or language translation effects. Therefore, our second objective is to examine the extent to which acculturation (i.e., nativity, years of US residency, language of interview) and health-related factors (e.g., mental disorder) account for ethnic distinctions in SRH. Using nationally representative US data from the Collaborative Psychiatric Epidemiology Surveys (CPES), we contribute to the extant literature by evaluating the construct validity of SRH within and across nine ethnic groups: non-Latinx Whites, African Americans, Afro-Caribbeans, Mexicans, Cubans, Puerto Ricans, Chinese, Filipino, and Vietnamese Americans. To our knowledge, this is the first study to assess the comorbidity-SRH relationship, as well as acculturation and health-related mechanisms, across such a diverse racial and ethnic sample. This research has implications for health disparities research that utilizes SRH as a dependent outcome, which renders the across-group validity of SRH critical to ascertain.
Background
Racial and Ethnic Differences in Self-rated Health
Black and Latinx individuals tend to rate their health more negatively than non-Latinx Whites. Numerous studies demonstrate that even after adjusting for influential factors such as socioeconomic status, a greater proportion of Blacks report fair/poor health than non-Latinx Whites [13,14,15,16,17]. Shetterly et al. [18] find that Latinx Whites are approximately twice as likely to rate their health as fair/poor compared to non-Latinx Whites, and similar results have been replicated with more recent samples [5, 8, 13]. Notably, there is much ethnic and nativity heterogeneity within the Black and Latinx populations in terms of health [15, 19, 20]. African Americans report significantly worse SRH than Caribbean-born Blacks in the USA [20]. Similarly, some Latinx subgroups, such as Puerto Ricans and Dominicans, are more likely to self-report ill health than Mexicans and other Latinxs [15, 21]. When race and ethnicity are considered simultaneously, divergent results emerge. For example, Puerto Ricans are more likely to report fair/poor health (25.1%) than both non-Latinx Blacks (24.3%) and non-Latinx Whites (12.6%), but Mexican Americans (21.7%) and Cuban Americans (17.1%) are less likely to do so [15]. Overall, these findings demonstrate that both race and ethnicity impact individuals’ health and health perceptions.
Research less frequently examines racial and ethnic group differences in SRH among Asians. Existing findings are mixed, with some studies demonstrating a SRH advantage among Asians compared to non-Latinx Whites [19] but others indicating that Asians exhibit less positive SRH compared to non-Latinx Whites [8, 22, 23]. Yet when disaggregated into ethnic groups, Chinese, Filipino, Korean, and Vietnamese individuals are less likely to report excellent/very good health and more likely to report fair/poor health compared to non-Latinx Whites [8]. Ahmmad, Wen, and Li [23] similarly found that all of the eight Asian subgroups in their study exhibited lower SRH relative to non-Latinx Whites. Hence, SRH patterns for Asian Americans are varied but emerging evidence suggests Asians in general experience an SRH disadvantage compared to non-Latinx Whites.
Racial and Ethnic Patterns in Morbidity
Chronic physical health conditions (e.g., diabetes, heart disease, stroke) disproportionately befall some historically marginalized ethnic groups, while other minority ethnic groups experience lower risk for health problems vis-à-vis non-Latinx White Americans. Black Americans experience higher prevalence of most chronic physical health problems compared to their non-Latinx White counterparts [24]. Recent work examines ethnic heterogeneity within the Black population, finding that Black Americans of Caribbean descent also experience more chronic conditions, on average, compared to non-Latinx Whites [25].
Though Black–White physical health disparities are longstanding, the physical health profiles of Latinx and Asian Americans are more variegated. Evidence from the Latinx epidemiological paradox literature suggests that despite economic and social disadvantages, Latinxs, on average, experience relatively fewer chronic health problems such as cardiovascular disease [26, 27]. This pattern is paradoxical given the strong and enduring association between socioeconomic status and health [28]. However, there is substantial ethnic variation in these patterns, with Puerto Ricans exhibiting more health problems relative to Mexican Americans and Cuban Americans [29, 30]. The Latinx epidemiological paradox also does not extend to all health outcomes. Although Latinxs exhibit a mortality advantage, they concomitantly experience elevated rates of specific types of morbidity and disability compared to non-Latinx Whites [27, 31]. Specifically, Latinxs are disadvantaged in terms of diabetes [27] and depressive, metabolic, and inflammatory risk [31], which indicates that observed health patterns are not exclusively paradoxical. That is, socioeconomic disadvantage and stress exposure contribute to health profiles for Latinxs similar to non-Latinx Blacks for some health indicators [31].
Generally, Asian Americans experience fewer chronic health conditions compared to non-Latinx Whites [32]. However, ethnic nuances are also relevant for Asian Americans [33]. Generally, the most health advantaged Asian ethnic groups include Chinese, followed by Japanese, Korean, Vietnamese, and Southeast Asians [33, 34]. In contrast, Filipinos, Pacific Islanders, and South Asians experience more chronic health conditions such as diabetes, hypertension, and cardiovascular disease compared to non-Latinx Whites and other Asian populations [33]. These divergent health trends reveal the importance of researching individuals as socially located in ethnic groups rather than in broad and heterogeneous racial categories alone.
The Paradox: Incongruent Ethnic Patterns for Morbidity and Self-rated Health
A growing body of literature seeks to confirm whether the morbidity-SRH association is reflected across diverse ethnic groups that have distinct cultural orientations, beliefs, and practices. These studies confirm that ethnic patterns for subjective health measures like SRH do not always map onto objective health measures such as morbidity and mortality. For example, Latinxs report lower SRH, on average, despite experiencing fewer chronic conditions relative to non-Latinx Whites [5, 6]. Huh, Prause, and Dooley [6] find a similar disjuncture between morbidity and SRH patterns for Asian Americans relative to non-Latinx Whites, although they do not disaggregate the sample by ethnic group. Erving [25] reports relatively worse SRH among Chinese and Vietnamese Americans, but simultaneously fewer chronic health problems compared to non-Latinx White Americans. Similarly, Assari and Lankarani [35] demonstrate that BMI is a weaker predictor of SRH for Chinese and Vietnamese respondents than it is for other Asians, Latinxs, non-Latinx Blacks, and non-Latinx Whites. This empirical conundrum for Latinx and Asian ethnic groups merits additional investigation, as it has implications for the conclusions drawn from quantitative studies examining ethnic disparities in health using SRH as the dependent measure.
A similar quandary arises for SRH among Black Americans. Though SRH is a predictor of mortality [2], the SRH-mortality association is weaker for Blacks compared to non-Latinx Whites. That is, SRH better predicts mortality for Whites than for Blacks, which implies that Blacks and Whites evaluate their health differently [11]. For instance, Blacks may assess their health more optimistically than other racial groups despite experiencing more chronic conditions on average [7, 36]. Other research suggests that Blacks may appraise their health more negatively than Whites, as evidenced by older Blacks (aged 70–79 years) reporting lower SRH at comparable health statuses [17]. Nevertheless, it is largely unknown at present if the weaker SRH-mortality association for Blacks compared to non-Latinx Whites extends to the relationship between SRH and morbidity.
Factors Influencing Self-rated Health Evaluations Across Ethnic Groups
Generally speaking, socioeconomic factors such as higher education and income are associated with better SRH [16, 18]. Other sociodemographic factors associated with SRH include gender, age, and marital status [3]. These widely accepted determinants of health importantly contribute to self-evaluations of health. Nevertheless, prior research suggests ethnic nuances in the specific factors that influence how individuals evaluate their health [5, 17, 35, 37]. Variation in SRH across ethnic groups could indicate actual between-group disparities in health, differences in evaluation or reporting style, or language translation effects. Because of our interest in unique factors impacting SRH across ethnic groups, here, we focus on acculturation-related factors, translation issues, and mental health problems as possible mechanisms.
First, acculturative factors such as generational status and length of time in the USA influence SRH. Overall, first-generation immigrants rate their health more positively than second- and third-generation immigrants [15, 19, 20, 30, 38], although some studies find the opposite [5] or no association [39]. The effects of duration of residence as an acculturative factor are also mixed, with various studies revealing a negative [14, 15, 19, 38] or no association between length of US residency and SRH [40]. For instance, recent Asian immigrants (0–4 years since migrating) are significantly less likely to report fair/poor physical SRH compared to US-born Asians [41]. As this example illustrates, the studies that demonstrate significant findings using nationally representative samples generally indicate that later-generational status and increased length of US residency are detrimental for SRH. While foreign-born individuals report better health than US-born individuals, this immigrant health advantage declines with length of US residency, a pattern that aligns with the notion of unhealthy assimilation [42].
Second, language of interview affects personal health evaluations [3, 5, 9, 10, 21, 43]. That language influences SRH may reflect issues related to both survey administration and acculturation. For example, Sanchez and Vargas [9] find that differences in wording for the “fair” (regular versus mas o menos) SRH response in Spanish-translated surveys bias this measure for Latinxs. Accordingly, disparities in SRH between respondents based on language of interview may indicate inaccuracies in the translation of the measure. Conducting the interview in a language other than English may also be indicative of lower levels of acculturation, which, in turn, is associated with underlying variations in norms, attitudes, and behaviors. Research on Asian and Latinx populations find that reporting good English proficiency is associated with higher ratings of SRH [40, 41, 44]. Thus, evidence suggests that interviews not conducted in English may bias the SRH measure due to translation issues and/or cultural differences in evaluation or reporting styles.
Third, psychological and emotional problems might adversely affect how individuals evaluate their health [43, 45]. In other words, individuals experiencing psychological distress or mental disorders may assess their self-rated physical health negatively. For example, Angel and Guarnaccia [43] show that depressive affect is associated with lower SRH for both Mexican and Puerto Rican Americans. Depressive symptomology is also associated with decreased SRH among a sample of Black and White respondents [17]. Finch and colleagues [46] find that depression accounts for 43% of the association between discrimination and SRH, which indicates that depression is a crucial mechanism through which discrimination operates, particularly for Latinxs. Notably, there may be ethnic differences in how non-physical factors impact personal health assessments, whereby social, emotional, and/or spiritual well-being may affect Latinxs’ and Asians’ SRH to a greater extent than non-Latinx Whites’ evaluations [8, 47]. This trend may partially explain the tendency of Latinxs and Asian Americans to report low SRH on average [5, 8]. At the same time, research suggests that the SRH of non-Latinx Whites, non-Latinx Blacks, and Cubans more strongly reflect the presence of diagnosed psychological disorders relative to Asian and other Latinx groups [45]. Although most previous studies of SRH include depression or depressive symptoms when accounting for psychological well-being, other mental disorders may also affect SRH. Thus, in addition to depression, we incorporate a more comprehensive measure of mental health by including other mood (e.g., bipolar disorder), anxiety, and substance use disorders.
The Current Study
Though SRH is a consistent predictor of morbidity and mortality in the general population, recent research calls into question whether the construct validity of SRH is reflected across diverse populations. Ethnicity is a critical social status characterized by linguistic, cultural, and social distinctions that potentially influence how individuals evaluate their health. To assess the within-group and across-group validity of SRH, we use nationally representative data to examine the association between morbidity and SRH across diverse ethnic groups in the USA. Previous studies examine the morbidity-SRH relationship [48, 49] or racial and/or ethnic differences in SRH [8, 13, 14, 18, 38]. Researchers rarely evaluate physical health indicators and racial and/or ethnic differences in SRH simultaneously and even then, only for limited racial and ethnic populations [6, 17]. We extend prior research by assessing the comorbidity-SRH relationship across nine ethnic groups, drawing attention to ethnic diversity within broader racial categories that are often studied homogeneously. For example, among Asian Americans, we examine the validity of SRH for Chinese, Filipino, and Vietnamese Americans, three of the largest ethnic groups within the US Asian population [50]. In addition, we investigate the roles that acculturation and health-related factors play in ethnic variations in SRH. Given the pervasiveness of SRH in social science empirical research, study results have implications for future research on racial and ethnic health disparities.
Materials and Methods
We draw data from the National Survey of American Life (NSAL) and the National Latino and Asian American Study (NLAAS) [51]. These surveys are a part of a larger national data collection effort designed to provide first-time national health estimates for ethnically diverse populations. NSAL and NLAAS are included in the publicly available Collaborative Psychiatric Epidemiology Surveys (CPES). CPES includes three data sources that were merged and harmonized by the principal investigators [51]. The data were collected between 2001 and 2003, providing national probability samples of several understudied minority ethnic groups in the USA. Despite the “age” of the data, NSAL and NLAAS remain critical and authoritative sources of information regarding the social determinants of health for ethnically diverse groups in the USA. For example, NSAL remains a premier source illuminating the health profiles of Afro-Caribbeans in the US context [52].
NSAL focuses on the US Black population, and is the first national probability study of Blacks of immediate Caribbean descent [53]. All respondents were 18 years of age and older. A total of 6082 face-to-face interviews were completed and consisted of 1621 Afro-Caribbeans, 3570 African Americans, and 891 non-Latinx Whites. All interviews were conducted in English. In the NSAL, African Americans were persons who self-identified as Black but did not report Caribbean ancestry. Afro-Caribbean were persons who self-identify as Black and answered affirmatively to any of the following inclusion criteria: (1) they were of West Indian or Caribbean descent, (2) they were born within a Caribbean area country, or (3) they had parents or grandparents who were born in a Caribbean area country (e.g., Jamaica, Haiti, Trinidad/Tobago). Interviews lasted an average of 2 h and 20 min, and the overall response rate was 72%.
With a focus on Latinx and Asian Americans, NLAAS consists of adults 18 and over residing in households in the coterminous US, Alaska, and Hawaii. A total of 4649 interviews were completed, which included Mexican, Puerto Rican, Cuban, Chinese, Filipino, Vietnamese, Other Latino, and Other Asian respondents. Interviews were conducted in English, Spanish, Chinese, Tagalog, and Vietnamese [54], and lasted an average of 2 h and 35 min. The response rate was 73% [55].
This analysis includes nine ethnic groups: non-Latinx Whites, African Americans, Afro-Caribbeans, Mexicans, Puerto Ricans, Cubans, Chinese, Filipinos, and Vietnamese. In our analysis, we use non-Latinx Whites as the reference category for two reasons. First, this decision is consistent with previous epidemiological research documenting racial disparities in health [56, 57]. Second, Whites are the most socially privileged (with regard to race) and have, on average, the greatest access to valued societal resources [58, 59]. Nevertheless, we recognize the importance of evaluating non-White ethnic group differences in health and advocate for future research to document these patterns. Data collection for both data sources were approved by the IRB at University of Michigan. The authors also received IRB approval for secondary data analysis of NSAL and NLAAS through their institution.
Measures
The dependent measure is self-rated health (SRH): response categories included Poor (= 1), Fair (= 2), Good (= 3), Very good (= 4), and Excellent (= 5). Although prior research tends to dichotomize SRH [60, 61], we analyzed the morbidity-SRH association using all five categories to capture subtleties between the categories. The key dependent measure is an index count of physical health conditions ranging from 0 to 4 or more conditions [62]. Respondents were queried if they had ever been professionally diagnosed with any of the following nine physical conditions: arthritis, asthma, cancer, chronic lung disease, diabetes, heart disease/heart trouble, high blood pressure, stroke, and ulcer. These health conditions were selected because they (1) have relatively high prevalence in the general population, (2) are associated with increased mortality risk/disability and are generally chronic in nature, and (3) are available in both datasets. Furthermore, previous research shows that a summary count of physical conditions is a more parsimonious measure for understanding broad dimensions of health as opposed to focusing on a single health measure [63]. The count measure was truncated at four conditions, as only 1.8% of respondents reported more than four conditions.
We included two factors that researchers most commonly use to capture acculturation [64]. First, nativity/length of US residency included the following categories: US-born (reference), less than 5 years, 5 to 10 years, 11 to 20 years, and more than 20 years living in the USA. Second, language of interview distinguished between those who completed the interview in English (= 1) compared to interview completion in a different language (i.e., Spanish, Vietnamese, Chinese, or Tagalog).
To assess whether mental health influenced SRH, as previous studies indicate [17, 43], we controlled for if a mental disorder (= 1) was experienced within the past 12 months. The World Mental Health Survey Initiative version of the World Mental Health Composite International Diagnostic Interview (WMH-CIDI) was used to assess psychiatric disorders based on criteria established in DSM-IV [65]. Mental disorders assessed included major depressive disorder (MDD), major depressive episode, dysthymic disorder, bipolar disorders 1 and 2, agoraphobia, panic disorder, social phobia, generalized anxiety disorder (GAD), post-traumatic stress disorder (PTSD), alcohol abuse, alcohol dependence, drug abuse, and drug dependence.
Though primarily interested in mental health problems, we included several measures of other health and healthcare factors known to affect SRH and morbidity [16, 48, 66, 67]. Health insurance coverage is a dichotomous measure (yes = 1) [19]. Morbid obesity was constructed using respondents’ reporting of their height and weight (BMI ≥ 40). To assess physical functioning, respondents were asked to report whether they experienced difficulty with mobility due to health problems in the last 30 days (yes = 1) [7, 39]. Bed days assessed the number of days in the past month respondent was in bed for half the day or more due to health or substance abuse problems [16].
All regression models controlled for sex, age, region of residence, number of children in the household, relationship status, and socioeconomic status, as is standard in studies examining SRH [14, 16, 19]. Sex distinguished between males and females (= 1). Age is a four-category variable: 18 to 34 years (reference), 35 to 49 years, 50 to 64 years, and 65 years and older. Region compared individuals residing in the South (= 1) to other regions. The number of children under the age of 18 living in the household ranged from 0 to 4 or more. Relationship status distinguished among married or cohabiting (reference), never married, and formerly married (i.e., divorced/separated/widowed). Three measures captured socioeconomic status (SES): annual household income, employment status, and education. Annual household income is a continuous measure, ranging from $0 to $200,000 or more (top-coded), and measured in increments of $10,000s. Employment status distinguished among those employed (reference), unemployed, and not currently in the labor force. Education included less than high school (reference), high school diploma/some college, and college graduate.
Missing Data
Collectively, the original sample size for NSAL and NLAAS included 10,731 respondents. Due to the inability to identify specific ethnic origin, Other Latinxs (n = 797) and Other Asians (n = 467) were excluded from the analysis. Next, listwise deletion was conducted, and we retained 88% of the original sample. Respondents were most likely to be missing on past month sick bed days (6%) and difficulty with mobility (7%), two critical health indicators that are likely to be related to SRH. The restricted sample is 8338.
Analysis Plan
We first present descriptive statistics for SRH and the count of chronic physical conditions by ethnicity (Table 1). Wald tests were conducted to assess significant differences in health measures between Non-Latinx Whites and each ethnic minority group. Next, the bivariate association between SRH and chronic conditions (Table 2) is assessed three ways: (1) Spearman correlations, (2) crosstabs between the number of chronic conditions by each SRH category, and (3) mean SRH scores by each number of chronic conditions.
The first set of regression analyses presented in Table 3 has two aims: (1) assess the morbidity-SRH association for the full sample and (2) examine ethnic patterns in SRH after adjustments for key covariates. Table 3 includes SRH as the dependent measure and uses ordered logistic regression. Model 1 includes the number of chronic conditions, ethnic groups, and the controls. Model 2 adds acculturation factors, and Model 3 adjusts for health and healthcare factors. Model 4 includes both acculturation and health factors.
The second set of regression analyses presented in Table 4 is designed to ascertain whether the morbidity-SRH association differs by ethnic group membership. Ethnicity-stratified models are run to assess the association between morbidity and SRH. Then, the suest command is used to compare the equality of coefficients across ethnic groups. This will answer the question whether the effect of chronic conditions on SRH differs across ethnic groups. Stated differently, this test is equivalent to an ethnicity-pooled model that includes a statistical interaction between ethnicity and the number of chronic conditions. To account for the complex survey design of the NSAL and NLAAS data, survey weights were used. All analyses were conducted in STATA 16.1 and were weighted using the suite of svy commands.
Results
Descriptives
Table 1 includes the means and proportions for SRH and the count of chronic conditions by ethnicity. Descriptive statistics for the independent measures and controls are available in Appendix Table 5. In terms of SRH, the mean score is 3.34 (SD = .98) for non-Latinx Whites, falling between the “good” and “very good” categories. Mexicans have significantly lower SRH, at 3.16 (SD = 1.09), while Filipinos have significantly higher SRH, at 3.55 (SD = .92). When examining proportions by each SRH category, Vietnamese (10%) have the highest prevalence of rating their health as “poor.” Relative to the other ethnic groups, Mexican, Puerto Rican, and Chinese respondents have a high proportion of rating their health as “fair”, at 30%, 23%, and 21%, respectively. This is in stark contrast to non-Latinx Whites, with 12% of respondents rating their health as “fair.” “Good” and “very good” are the modal categories for all ethnic groups. Cubans have the highest rate of reporting “excellent” health, at 25%, compared to 7% of non-Latinx Whites who rate their health as “excellent.”
For the count of chronic conditions, the mean is 1.08 (SD = 1.29) for non-Latinx Whites, while Mexican, Chinese, Filipino, and Vietnamese Americans report significantly lower mean chronic conditions. The proportion by each number of chronic conditions reveals similar patterns, with Mexican (66%), Chinese (59%), and Vietnamese (60%) respondents being the most likely to have no chronic conditions. Given that Mexicans report relatively lower SRH compared to non-Latinx Whites, this finding is counterintuitive. Furthermore, that Chinese and Vietnamese Americans have fewer chronic conditions but do not significantly differ from non-Latinx Whites in terms of SRH is also curious. African Americans and non-Latinx Whites are the most likely to have two or more conditions, at 32% and 30%, respectively. In addition, African Americans (7%), Puerto Ricans (6%), and non-Latinx Whites (6%) experience the highest rates of four or more health conditions.
Table 2 presents the bivariate association between SRH and chronic conditions. First, Spearman correlations reveal an inverse association for all nine ethnic groups. Stated differently, a higher number of chronic conditions is associated with lower SRH. Nevertheless, the correlations are largest for Cubans (− .47), Puerto Ricans (− .45), and non-Latinx Whites (− .43), and relatively weaker for Chinese (− .22), Filipinos (− .25), and Mexicans (− .25); African Americans (− .40), Vietnamese (− .40), and Afro-Caribbeans (− .38) fall in the middle. Second, crosstabs of mean conditions by SRH category confirm the inverse morbidity-SRH association within each ethnic group. Nevertheless, mean conditions by SRH categories vary across ethnicity. For example, mean chronic conditions among those reporting “fair” health is low for Chinese (.82) and Mexicans (.89) compared to non-Latinx Whites (1.88) and African Americans (1.91). For mean SRH by number of chronic conditions crosstabs, the “starting point” for SRH scores differ across ethnicity. For example, for no conditions, the mean SRH for non-Latinx Whites, Puerto Ricans, and Afro-Caribbeans is 3.73; similar “objectively healthy” Mexicans and Chinese rate SRH as 3.33 and 3.42, respectively. These bivariate results raise concerns regarding the validity of SRH across ethnic groups. Regression analysis which adjusts for potential confounding factors (e.g., language of interview, mental health) may yield explanations for these concerns. It is to this set of results that we now turn.
Regression Analysis: Across-Group Validity
In Table 3, weighted odds ratios from ordered logistic regression models predicting SRH are shown.Footnote 1 Across all four models, a higher number of chronic conditions is associated with lower SRH, further confirming the inverse association between these two commonly used health measures. We ran supplemental analyses to assess whether having each physical condition was associated with lower SRH. When each specific health condition is entered into the model (as opposed to a number of chronic conditions measure), seven of the nine health conditions were associated with lower SRH. Cancer and asthma were not statistically significant, but were in the expected direction (i.e., coefficients indicate that diagnosis of both were associated with lower SRH).
With regard to ethnic patterns in SRH, in model 1, Mexican (OR = .655, p < .01) and Chinese (OR = .494, p < .001) respondents have relatively worse SRH compared to non-Latinx Whites, while Cubans report better SRH (OR = 1.449, p < .05). In model 2, after adjusting for acculturation factors, the Chinese SRH disadvantage and Cuban SRH advantage remains while the Mexican-White SRH difference falls to non-significance. With regard to the effect of acculturation factors, compared to the US-born, recently arrived immigrants (less than 5 years; OR = 1.444, p < .01) and long-term immigrants (20 or more years; OR = 1.491, p < .01) report significantly higher SRH. This finding is inconsistent with the unhealthy assimilation hypothesis which suggests that longer US residency is associated with worse health. Nevertheless, this set of findings lend partial support for the healthy immigrant hypothesis. Completing an interview in English is associated with higher SRH (OR = 1.771, p <. 001). These results suggest that acculturation factors (i.e., length of US residency and language of interview) influence SRH, and also partially explain Mexicans’ relatively lower SRH compared to non-Latinx Whites. Only 43% of Mexican respondents were interviewed in English (see Appendix Table 5); thus, the remaining 57% who completed interviews in Spanish appear to rate their health more negatively. The implication is that SRH categories carry different connotations in Spanish and English.
In model 3 of Table 3, health and healthcare factors are included. These factors do not appear to explain SRH ethnic patterns; in fact, when adjusting for health-related factors, Vietnamese respondents emerge as having significantly lower SRH compared to non-Latinx Whites (OR = .652, p < .05). Having a past-year mental disorder is associated with lower SRH (OR = .586, p < .05), suggesting that respondents incorporate their mental health into assessing overall health. Furthermore, past month mobility difficulties (OR = .410, p < .001) and sick bed days (OR = .904, p < .001) are associated with lower SRH. In model 4, which includes adjustments for acculturation and health-related factors, the same ethnic patterns remain: Cubans report significantly higher SRH while Chinese report significantly lower SRH. However, the results from this analysis suggest that Mexicans’ relatively poorer SRH compared to non-Latinx Whites is, in part, due to acculturation factors.
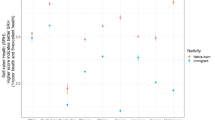
Figure 1 provides a visual depiction of ethnic differences in SRH based on estimates before (Table 3, model 1) and after (Table 3, model 4) adjusting for contributing factors. We show predicted probabilities of reporting fair or poor self-rated health, as past research tends to distinguish between fair/poor health and good/very good/excellent health [60, 61].Footnote 2 A clear pattern emerges whereby Chinese (.27) and Mexican (.22) Americans have a higher predicted probability of reporting fair or poor health compared to non-Latinx Whites (.16) in the unadjusted models. On the other hand, Cubans (.11) have a lower predicted probability of reporting fair or poor health compared to non-Latinx Whites. These patterns remain quite consistent even after adjusting for acculturation and health-related factors in the fully adjusted model.

Regression Analysis: Within-Group Validity
To assess the within-group validity of SRH, Table 4 presents results from ethnicity-stratified models to test the morbidity-SRH association within ethnic groups. First, odds ratios for the effect of chronic conditions on SRH are shown for models with controls and, second, models that adjust for health-related factors and, when appropriate, acculturation factors. For each ethnic group, more chronic conditions are associated with lower SRH. Nevertheless, the effect of chronic conditions on SRH is relatively weaker for Cuban and Vietnamese Americans when compared to non-Latinx Whites in the unadjusted and adjusted models.
Given the emphasis on SRH translation challenges for interviews conducted in Spanish, we opted to show language of interview effects by ethnic group in Table 4. Language of interview is not relevant for non-Latinx Whites, African Americans, and Afro-Caribbeans because all interviews were conducted in English for these groups. Interestingly, for Mexican (OR = 1.654, p <. 05) and Puerto Rican (OR = 2.029, p <. 01) respondents, but not Cubans, interviews conducted in English are associated with higher SRH. This suggests that less acculturated respondents (i.e., those who completed interviews in Spanish) report worse SRH. Among Asian Americans, language of interview is only significant for Chinese Americans (OR = 5.175, p < .001): Chinese respondents who completed English interviews report higher SRH compared to those who completed interviews in Chinese.
Discussion
The current study assessed ethnic distinctions in the predictive validity of self-rated health (SRH), a common health measure in social science and health services research. Our concern for validity is rooted in a growing body of research that casts doubt on the ability of SRH to capture existing racial and ethnic disparities in objective health measures (e.g., morbidity and mortality). To assess the within-group and across-group validity of SRH, we used data from the National Survey of American Life and National Latino and Asian American Study to examine the association between professionally diagnosed chronic physical conditions and SRH across nine ethnic groups in the USA. We contribute to existing research by demonstrating ethnic diversity within the broader racial categories of “Black,” “Latinx,” and “Asian” American. Our study results reveal heterogeneity within these racial groups who are often studied monolithically.
We found limited evidence of across-group validity for SRH, particularly for Mexican Americans vis-à-vis their non-Latinx White counterparts. Despite experiencing relatively fewer chronic conditions compared to non-Latinx Whites, Mexican Americans reported significantly lower SRH. In fact, 30% of Mexicans rated their health as “fair,” compared to 12% of non-Latinx Whites. Furthermore, Mexicans’ lower SRH was explained, in part, by survey administration and acculturation factors; more specifically, Mexican respondents who completed interviews in English, on average, reported relatively higher SRH. The same pattern of language effects emerged for Puerto Rican, but not Cuban, respondents. Scholars suggest that the translation of the “fair” category to regular leads Spanish language Latinx respondents to report poorer health since regular may denote a more positive meaning in Spanish than intended [9, 10]. This language effect may coalesce with cultural factors, such as the traditional social norm to avoid boasting about one’s health among some Latinx populations [18], to create artificial disparities in SRH. Interestingly, for other Latinx groups, Puerto Ricans and Cubans, there appeared to be greater consistency between SRH and morbidity. This set of findings further confirms the necessity of ethnically disaggregating the diverse Latinx category. In addition, recent research also suggests that racial identification in combination with ethnicity among Latinxs also contributes to differentiated SRH patterns [13, 14, 38]. Although the data did not allow for the differentiation of Latinx respondents by race, studies indicate that Latinx Blacks are more likely to report fair/poor health than Latinx Whites and non-Latinx Blacks and Whites [13, 14]. As such, the lack of inclusion of race could conceal health variation among Latinx populations. Future research should explore the intersections of racial identification, ethnic group membership, and nativity status among Latinx populations, and the implications of these statuses for SRH.
A second challenge to the across-group validity of SRH was found for Asian Americans: though Chinese and Vietnamese Americans had relatively fewer chronic conditions, they simultaneously reported lower SRH compared to non-Latinx Whites. In some Asian cultures in which modesty is highly valued, reporting health as “excellent” may appear particularly immodest [6] or overly optimistic [8]. Alternatively, perhaps Chinese and Vietnamese Americans are relying on co-ethnics as a reference group when evaluating their health, which could cause them to evaluate their health poorly even in the absence of health problems. Analogously, research on Asian American academic performance shows a similar disjuncture: in interviews with Chinese and Vietnamese immigrants, Lee and Zhou [68] found that because other high performing co-ethnics was their comparison group, many suffered from low self-efficacy despite having objectively high academic achievement. While the finding is specific to the educational sphere, it demonstrates a weak linkage between personal subjective evaluations (self-efficacy or self-rated health) and objective measures (academic achievement or chronic health problems). An alternative explanation for Asian Americans’ relatively lower SRH is that some Asian Americans may conceptualize health from a more holistic perspective, incorporating physical, emotional, and spiritual health; non-Latinx White Americans, however, may adopt a medical model perspective, relying primarily on medical conceptions such as pre-existing conditions and health behaviors [8]. Accordingly, an absence of chronic diseases may not signify optimal health for Asian Americans. Future research should explore the factors affecting how various ethnic groups within the Asian American population evaluate their health, especially in light of recent research demonstrating variation in the social determinants of SRH between different Asian ethnic groups [37]. Anchoring vignettes might be an insightful methodological approach [7, 69].
Beyond cultural interpretations of health, language effects may also contribute to differences in SRH between non-Latinx Whites and Asian Americans. As Kandula et al. [8] suggest, terms such as “excellent” and “fair” may not have commensurate translations in some Asian languages. This may be the case for the Chinese language given that Chinese respondents who completed English interviews reported significantly higher SRH compared to those who completed interviews in Chinese. In light of previous findings regarding the translation effects of the word “fair” in Spanish, this pattern merits further attention. Future research should investigate whether altering the words for different SRH categories systematically modifies patterns in SRH for Chinese-speaking respondents, as Sanchez and Vargas [9] found for Spanish-speakers.
Surprisingly, we did not find evidence of SRH differences between Black Americans (African American or Afro-Caribbeans) and their non-Latinx White counterparts. Prior research has indicated that Blacks might be optimistic in their ratings, as they are likely comparing themselves to their less healthy family members and peers [7]. Lee and Hicken [36 , p. 432] offered the explanation that health problems Blacks experience at disproportionately higher rates could be “simply accepted as part of life” or “seen as more manageable.” The possibility of normalization of health problems among Black Americans is an interesting hypothesis, and some qualitative research suggests that Black Americans may rely on different indicators (e.g., spirituality and social activities) when reporting their health relative to their non-Latinx White counterparts [70, 71]. Thus, despite finding similar patterns of SRH and chronic conditions in this sample of Black and non-Latinx White Americans, Black–White differences (or lack thereof) in SRH should be investigated in future research.
Last, we found evidence of within-group validity for SRH. In other words, for each ethnic group, SRH and chronic conditions were inversely associated. This finding is encouraging, as it suggests that studies focused on a single ethnic group will be less prone to validity concerns. Such studies can be insightful because they reveal the social correlates of SRH for a particular group. For example, Todorova and colleagues’ [72] study of SRH among Puerto Ricans revealed specific determinants of their SRH including emotional support, heavy alcohol use, and smoking, among other factors.
Despite the study’s insights, there are some limitations. First, beyond self-reported measures of health conditions (i.e., asking respondents if they have been diagnosed with a condition), health measures based on medical professional evaluation could yield a more precise measure of morbidity prevalence, particularly for groups less likely to be insured. Interestingly, Angel and Guarnaccia [43] found substantial differences between Latinxs’ ratings of their own health compared to physician evaluations, with doctors being more likely to rate respondents’ health as “excellent” or “very good,” particularly among those who took the survey in Spanish. This finding suggests a complex interplay between physician evaluation and patient self-evaluation that we were unable to capture here. In a similar vein, such evaluations could also illuminate details regarding the timing of diagnosis, treatment approach, and disease severity. Relatedly, examining the association between SRH and measures of biological risk (e.g., allostatic load) may offer a more stringent test of whether SRH maps on to objective health outcomes [61]. Second, statistical power challenges prevented us from examining ethnic, racial, age, and gender distinctions in SRH and chronic health conditions. Nevertheless, past research suggests SRH reporting styles also display racial (as previously discussed), age, and gendered patterns [13, 14, 38, 69, 73, 74]. Research indicates that the association between SRH and physical health, including functional limitations and chronic conditions, weakens with age [73, 74]. Due to sample size limitations, we were unable to conduct age-stratified analyses to account for potential aging, cohort, or survivor effects. Instead, our models included age as a covariate in order to account for differing age distributions by ethnicity. We were similarly unable to stratify analyses by gender, but account for gender in our analyses given women’s propensity for optimism when rating their health [69]. How ethnicity, race, age, gender, and nativity statuses intersect to produce differentials in SRH reporting remains an important area of empirical investigation. Third, acculturation is a dynamic process used to describe a broad range of cultural adjustments experienced by individuals who migrate to the US. Beyond the “typical” measures of acculturation used here (i.e., language of interview, length of US residency), more granular acculturation measures may aid in better specifying how acculturation processes impact the ways in which immigrants answer the SRH question in survey data. For instance, measures that capture individuals’ ethnic identity, adoption of health-related attitudes, and health behaviors may more accurately capture convergence to the host society’s culture.
Conclusion
Using data from two nationally representative samples, findings from this study reveal within-group validity of the SRH measure for nine ethnic groups in the USA. However, study results raise serious concerns regarding the across-group validity of SRH, particularly in research comparing Mexican, Chinese, and Vietnamese Americans to their non-Latinx White counterparts. We submit that SRH may be insufficient as a sole health indicator for studies seeking to assess population-based health disparities. Nonetheless, when used in tandem with other health measures (e.g., morbidity, functional limitations), SRH may yield fruitful information regarding group differences in the perceptual dimension of health not captured in objective health measures like condition-specific prevalence rates. Though SRH is a highly subjective measure, its subjectivity is not a liability. Instead, racial and ethnic patterns in SRH must be adequately contextualized given our study findings and more recent research suggesting the non-equivalence of SRH across ethnic groups. The broader implication is that health scholars should exercise caution when using SRH in studies focused on racial, ethnic, and nativity disparities in health. Furthermore, given its ubiquity in social science research, more research is needed to ascertain what specific factors affect how respondents evaluate health, and whether SRH determinants differ across ethnicity and nativity status.
Data Availability
Data are available online at the following website: https://www.icpsr.umich.edu/web/ICPSR/studies/20240/datadocumentation
Code Availability
Coding from do-files produced in STATA are available upon request.
Notes
When SRH is dichotomized (i.e., 0 = excellent/very good/good, 1 = fair/poor), as is common in the literature [60, 61], we find similar, but not identical, results. More specifically, in Model 1, Mexican, Puerto Rican, Chinese, and Vietnamese Americans have a significantly higher odds of reporting fair/poor health compared to non-Latinx Whites (at p < .01). In the fully adjusted model, Mexican and Chinese Americans are significantly more likely to report fair/poor health compared to non-Latinx Whites (at p < .01).
Predicted probabilities for all five SRH categories are available upon request. Of note, ethnic differences in predicted probability of “fair” SRH are most pronounced.
References
Krause NM, Jay GM. What do global self-rated health items measure? Med Care. 1994;32(9):930–42.
Ilder EL, Benyamini Y. Self-rated health and mortality: a review of twenty-seven community studies. J Health Soc Behav. 1997;38(1):21–37. https://doi.org/10.2307/2955359.
Benjamins MR, Hirschman J, Hirschtick J, Whiteman S. Exploring differences in self-rated health among Blacks, Whites, Mexicans, and Puerto Ricans. Ethn Health. 2012;17(5):463–76. https://doi.org/10.1080/13557858.2012.654769.
Klest B, Freyd JJ, Hampson SE, Dubanoski JP. Trauma, socioeconomic resources, and self-rated health in an ethnically diverse adult cohort. Ethn Health. 2013;18(1):97–113. https://doi.org/10.1080/13557858.2012.700916.
Bzostek S, Goldman N, Pebley A. Why do Hispanics in the USA report poor health? Soc Sci Med. 2007;65:990–1003. https://doi.org/10.1016/j.socscimed.2007.04.028.
Huh J, Prause A, Dooley DC. The impact of nativity on chronic diseases, self-rated health and comorbidity status of Asian and HIspanic immigrants. J Immigr Minor Health. 2008;10(2):103–18. https://doi.org/10.1007/s10903-007-9065-7.
Dowd JB, Todd M. Does self-rated health bias the measurement of health inequalities in U.S. adults? Evidence using anchoring vignettes from the Health and Retirement Study. J Gerontol B Psychol Sci Soc Sci. 2011;66(4):478–89. https://doi.org/10.1093/geronb/gbr050.
Kandula NR, Lauderdale DS, Baker DW. Differences in self-reported health among Asians, Latinos, and Non-Hispanic Whites: the role of language and nativity. Ann Epidemiol. 2007;17:191–8. https://doi.org/10.1016/j.annepidem.2006.10.005.
Sanchez G, Vargas E. Language bias and self-rated health status among the Latino population: evidence of the influence of translation in a wording experiment. Qual Life Res. 2016;5:1131–6. https://doi.org/10.1007/s11136-015-1147-8.
Viruell-Fuentes EA, Morenoff JD, Willaims DR, House JS. Language of interview, self-rated health, and the other Latino health puzzle. Am J Public Health. 2011;101(7):1306–13. https://doi.org/10.2105/AJPH.2009.175455.
Woo H, Zajacova A. Predictive strength of self-rated health for mortality risk among older adults in the United States: does it differ by race and ethnicity? Res Aging. 2017;39(7):879–905. https://doi.org/10.1177/0164027516637410.
Malgady RG. The question of cultural bias in assessment and diagnosis of ethnic minority clients: let’s reject the null hypothesis. Prof Psychol Res Pract. 1996;27(1):73–7. https://doi.org/10.1037/0735-7028.27.1.73.
Borrell LN, Crawford ND. Race, ethnicity, and self-rated health status in the Behavioral Risk Factor Surveillance System Survey. Hisp J Behav Sci. 2006;28(3):387–403. https://doi.org/10.1177/0739986306290368.
Borrell LN, Dallo FJ. Self-rated health and race among Hispanic and Non-Hispanic adults. J Immigr Minor Health. 2008;10:229–38. https://doi.org/10.1007/s10903-007-9074-6.
Cho YW, Frisbie P, Hummer RA, Rogers RG. Nativity, duration of residence, and the health of Hispanic adults in the United States. Int Migr Rev. 2004;38(1):184–211. https://doi.org/10.1111/j.1747-7379.2004.tb00193.x.
Dowd JB, Zajacova A. Does the predictive power of self-rated health for subsequent mortality risk vary by socioeconomic status in the US? Int J Epidemiol. 2007;36(6):1214–21. https://doi.org/10.1093/geronb/gbr050.
Spencer M, Schulz R, Rooks R, Albert S, Thorpe R Jr, Brenes G, et al. Racial differences in self-rated health at similar levels of physical functioning: an examination of health pessimism in the Health, Aging, and Body Composition Study. J Gerontol B Psychol Sci Soc Sci. 2009;64(1):87–94. https://doi.org/10.1093/geronb/gbn007.
Shetterly S, Baxter J, Mason L, Hamman R. Self-rated health among HIspanic vs Non-Hispanic White Adults: the Sna Luis Valley Health and Aging Study. Am J Public Health. 1996;86(12):1798–801. https://doi.org/10.2105/ajph.86.12.1798.
Acevedo-Garcia D, Bates LM, Osypuk TL, McArdle N. The effect of immigrant generation and duration on self-rated health among US adults 2003–2007. Soc Sci Med. 2010;71(6):1161–72. https://doi.org/10.1016/j.socscimed.2010.05.034.
Griffith DM, Johnson JL, Zhang R, Neighbors HW, Jackson JS. Ethnicity, nativity, and the health of American Blacks. J Health Care Poor Underserved. 2011;22(1):142–56. https://doi.org/10.1353/hpu.2011.0011.
Santos-Lozada A, Martinez M. How have you been? Or ¿Como estás?: does language of interview influence self-rated health among Hispanic subgroups? J Immigr Minor Health. 2018;20(4):766–75. https://doi.org/10.1007/s10903-017-0606-4.
Howell J, Emerson MO. So what 'should' we use? Evaluating the impact of five racial measures on markers in social inequality. Soc Race Ethn. 2017;3(1):14–30. https://doi.org/10.1177/2332649216648465.
Ahmmad Z, Wen M, Li K. Self-rated health disparities among Asian Americans: mediating roles of education level and household income. J Immigr Minor Health. 2020. https://doi.org/10.1007/s10903-020-01051-0.
Brown TH, O'Rand AM, Adkins DE. Race-ethnicity and health trajectories: tests of three hypotheses across multiple groups and health outcomes. J Health Soc Behav. 2012;53(3):359–77. https://doi.org/10.1177/0022146512455333.
Erving CL. Gendered tri-racial stratification and health disparities. Soc Sci Res. 2020;88-89. https://doi.org/10.1016/j.ssresearch.2020.102427.
Markides K, Coreil J. The health of Hispanics in the Southwestern United States: an epidemiological paradox. Public Health Rep. 1986;101(3):253–65.
Cunningham SA, Ruben JD, Narayan KM. Health of foreign-born people in the United States: a review. Health Place. 2008;14(4):623–35. https://doi.org/10.1016/j.healthplace.2007.12.002.
Phelan JC, Link BG, Tehranifar P. Social conditions as fundamental causes of health inequalities: theory, evidence, and policy implications. J Health Soc Behav. 2010;51:S28–40. https://doi.org/. https://doi.org/10.1177/0022146510383498.
Erving CL. Physical-psychiatric comorbidity: patterns and explanations for ethnic group differences. Ethn Health. 2018;23(6):583–610. https://doi.org/10.1080/13557858.2017.1290216.
Zsembik B, Fennell D. Ethnic variation in health and the determinants of health among Latinos. Soc Sci Med. 2005;61(1):53–63. https://doi.org/10.1016/j.socscimed.2004.11.040.
Boen CE, Hummer RA. Longer-but harder-lives? The Hispanic health paradox and the social determinants of racial, ethnic, and immigrant-native health disparities from midlife through later life. J Health Soc Behav. 2019;60(4):434–52. https://doi.org/10.1177/0022146519884538.
National Center for Health Statistics (NCHS). Health, United States, 2015: with special feature on racial and ethnic health disparities. Hyattsville; 2016. https://www.ncbi.nlm.nih.gov/books/NBK367640/. Accessed 27 May 2020.
Gordon NP, Lin TY, Rau J, Lo JC. Aggregation of Asian-American subgroups masks meaningful differences in health and health risks among Asian ethnicities: an electronic health record based cohort study. BMC Public Health. 2019;19(1):1551. https://doi.org/10.1186/s12889-019-7683-3.
Zhao B, Jose PO, Pu J, Chung S, Ancheta IB, Fortmann SP, et al. Racial/Ethnic differences in hypertension prevalence, treatment, and control for outpatients in Northern California 2010-2012. Am J Hypertens. 2015;28(5):631–9. https://doi.org/10.1093/ajh/hpu189.
Assari S, Lankarani MM. Demographic and socioeconomic determinants of physical and mental self-rated health across 10 ethnic groups in the United States. Int J Epidemiol Res. 2017;3(12):185–93. https://doi.org/10.15171/ijer.2017.02.
Lee H, Hicken MT. Death by a thousand cuts: The health implications of Black respectability politics. Souls. 2016;18(2-4):421–45. https://doi.org/10.1080/10999949.2016.1230828.
Assari S, Kumar A. Social determinants of physical self-rated health among Asian Americans; comparison of six ethnic groups. Societies. 2018;8(24). https://doi.org/10.3390/soc8020024.
Marquez-Velarde G, Jones NE, Keith VM. Racial stratification in self-rated health among Black Mexicans and White Mexicans. SSM Popul Health. 2020;10:2–8. https://doi.org/10.1016/j.ssmph.2019.100509.
Erosheva E, Walton EC, Takeuchi DT. Self-rated health among foreign- and U.S.-born Asian Ameircans: a test of comparability. Med Care. 2007;45(1):80–7. https://doi.org/10.1097/01.mlr.0000241114.90614.9c.
Kimbro RT, Gorman BK, Schachter A. Acculturation and self-rated health among Latino and Asian immigrants to the United States. Soc Probl. 2012;59(3):341–63. https://doi.org/10.1525/sp.2012.59.3.341.
Zhang W, Ta V. Social connections, immigration-related factors, and self-rated physical and mental health among Asian Americans. Soc Sci Med. 2009;68(12):2104–12. https://doi.org/10.1016/j.socscimed.2009.04.012.
Anetecol H, Bedard K. Unhealthy assimilation: Why do immigrants converge to American health status levels? Demography. 2006;43:337–60. https://doi.org/10.1353/dem.2006.0011.
Angel R, Guarnaccia PJ. Mind, body, and culture: somatization among Hispanics. Soc Sci Med. 1989;28(12):1229–38. https://doi.org/10.1016/0277-9536(89)90341-9.
Lommel LL, Chen JL. The relationship between self-rated health and acculturation in Hispanic and Asian adult immigrants: a systematic review. J Immigr Minor Health. 2016;18(2):468–78. https://doi.org/10.1007/s10903-015-0208-y.
Assari S. Psychiatric disorders differently correlate with physical self-rated health across ethnic groups. J Pers Med. 2017;7(4):6. https://doi.org/10.3390/jpm7040006.
Finch BK, Hummer RA, Kol B, Vega WA. The role of discrimination and acculturative stress in the physical health and Mexican-origin adults. Hisp J Behav Sci. 2001;23(4):399–429. https://doi.org/10.1177/0739986301234004.
Finch BK, Hummer RA, Reindl M, Vega WA. Validity of self-rated health among Latino(a)s. Am J Epidemiol. 2002;155(8):755–9. https://doi.org/10.1093/aje/155.8.755.
Wolinsky FD, Miller TR, Malmstrom TK, Miller JP, Schootman M, Andresen EM, et al. Self-rated health: changes, trajectories, and their antecedents among African Americans. J Aging Health. 2008;20(2):143–58. https://doi.org/10.1177/0898264307310449.
Molarius A, Janson S. Self-rated health, chronic diseases, and symptoms among middle-aged and elderly men and women. J Clin Epidemiol. 2002;55(4):363–70. https://doi.org/10.1016/S0895-4356(01)00491-7.
Hoeffel EM, Rastogi S, Kim MO, Shahid H. The Asian population: 2010. United States Census Bureau. 2012. https://www.census.gov/library/publications/2012/dec/c2010br-11.html. Accessed 5 June 2020.
Heeringa SG, Wagner J, Torres M, Duan N, Adams T, Berglund P. Sample designs and sampling methods for the Collaborative Psychiatric Epidemiology Studies (CPES). Int J Methods Psychiatr Res. 2004;13:221–40. https://doi.org/10.1002/mpr.179.
Taylor RJ, Chatters LM, Taylor HO. Race and objective social isolation: older African Americans, Black Caribbeans, and Non-Hispanic Whites. J Gerontol B Psychol Sci Soc Sci. 2019;74(8):1429–40. https://doi.org/10.1093/geronb/gby114.
Jackson JS, Torres M, Caldwell CH, Neighbors HW, Nesse RM, Taylor RJ, et al. The National Survey of American Life: a study of racial, ethnic and cultural influences on mental disorders and mental health. Int J Methods Psychiatr Res. 2004;13:196–207. https://doi.org/10.1002/mpr.177.
Alegría M, Takeuchi D, Canino G, Duan N, Shrout P, Meng XL, et al. Considering context, place and culture: the national Latino and Asian American study. Int J Methods Psychiatr Res. 2004;13:208–20. https://doi.org/10.1002/mpr.178.
Pennell BE, Bowers A, Carr D, Chardoul S, Cheung GQ, Dinkelmann K, et al. The development and implementation of the National Comorbidity Survey Replication, the National Survey of American Life, and the National Latino and Asian American Survey. Int J Methods Psychiatr Res. 2004;13:241–69. https://doi.org/10.1002/mpr.180.
Dressler WW, Oths KS, Gravlee CC. Race and ethnicity in public health research: models to explain health disparities. Annu Rev Anthropol. 2005;34:231–52. https://doi.org/. https://doi.org/10.1146/annurev.anthro.34.081804.120505.
Williams DR. Miles to go before we sleep: racial inequities in health. J Health Soc Behav. 2012;53(3):279–95. https://doi.org/10.1177/0022146512455804.
Feagin JR. Racist America: roots, current realities, and future reparations. New York: Routledge; 2014.
Jung MK. Beneath the surface of white supremacy: denaturalizing U.S. racisms past and present. Stanford: Stanford University Press; 2015.
Chandola T, Jenkinson C. Validating self-rated health in different ethnic groups. Ethn Health. 2000;5(2):151–9. https://doi.org/10.1080/713667451.
Santos-Lozada A, Howard J. Using allostatic load to validate self-rated health for racial/ethnic groups in the United States. Biodemography Soc Biol. 2018;64(1):1–14. https://doi.org/10.1080/19485565.2018.1429891.
Anderson G. Chronic care: Making the case for ongoing care. Robert Wood Foundation. 2010. https://www.rwjf.org/en/library/research/2010/01/chronic-care.html. Accessed 20 May 2020.
Farmer M, Ferraro KF. Are racial disparities in health conditional on socioeconomic status. Soc Sci Med. 2005;60(1):191–204. https://doi.org/10.1177/0164027507311155.
Abraído-Lanza AF, Armbrister AN, Flórez KR, Aguirre AN. Toward a theory-driven model of acculturation in public health research. Am J Public Health. 2006;96(8):1342–6. https://doi.org/10.2105/AJPH.2005.064980.
American Psychiatric Association (APA). Diagnostic and statistical manual of mental disorders (DSM-IV). 4th ed. Washington, DC; 1994.
Bailis DS, Segall A, Chipperfield JG. Two views of self-rated general health status. Soc Sci Med. 2003;56(2):203–17. https://doi.org/10.1016/s0277-9536(02)00020-5.
Phillips LJ, Hammock RL, Blanton JM. Predictors of self-rated health status among Texas residents. Prev Chronic Dis. 2005;2(4):A12.
Lee J, Zhou M. The Asian American achievement paradox. New York: Russell Sage Foundation; 2015.
Grol-Prokopczyk H, Freese J, Hauser RM. Using anchoring vignettes to assess group differences in general self-rated health. J Health Soc Behav. 2011;52(2):246–61. https://doi.org/10.1177/0022146510396713.
Ilder EL, Hudson SV, Leventhal H. The meanings of self-ratings of health: a qualitative and quantitative approach. Res Aging. 1999;21(3):458–76. https://doi.org/10.1177/0164027599213006.
McMullen CK, Luborsky MR. Self-rated health appraisal as cultural identity process: African American Elders’ health and evaluative rationales. Gerontologist. 2006;46(4):431–8. https://doi.org/10.1093/geront/46.4.431.
Todorova ILG, Tucker KL, Pescador Jimenez M, Lincoln AK, Arevalo S, Falcon LM. Determinants of self-rated health and the role of acculturation: implications for health inequalities. Ethn Health. 2013;18(6):563–85. https://doi.org/10.1080/13557858.2013.771147.
Idler E, Cartwright K. What do we rate when we rate our health? Decomposing age-related contributions to self-rated health. J Health Soc Behav. 2018;59(1):74–93. https://doi.org/10.1177/0022146517750137.
Schnittker J. When mental health becomes health: age and the shifting meaning of self-evaluations of general health. Milbank Q. 2005;83(3):397–423. https://doi.org/10.1111/j.1468-0009.2005.00407.x.
Funding
The first author was supported by a Ford Foundation Postdoctoral Fellowship and Woodrow Wilson Career Enhancement Fellowship.
Author information
Authors and Affiliations
Contributions
Both authors contributed to the study conception and design. Data analysis was performed by the first author. Both authors contributed to the writing of the manuscript and approved the final manuscript.
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Appendix
Rights and permissions
About this article

Cite this article
Erving, C.L., Zajdel, R. Assessing the Validity of Self-rated Health Across Ethnic Groups: Implications for Health Disparities Research. J. Racial and Ethnic Health Disparities 9, 462–477 (2022). https://doi.org/10.1007/s40615-021-00977-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40615-021-00977-x