
Abstract
Geographic barriers to accessing timely and appropriate primary health care services have been identified as significant social determinants of health that contribute to the growing health inequities among Hispanic and Latino immigrants in the United States. The purpose of this study was to examine the geographic factors that serve as barriers to healthcare access for Hispanic and Latino immigrants in the southern community of Louisville, Kentucky. Accessibility to healthcare services was examined using spatial analysis techniques, a Geographic Information System and geographic data from the U.S. Census Bureau and the Louisville and Jefferson County Information Consortium. Results from this study indicated that physical location, socioeconomic factors, distance, and transportation served as barriers to accessing healthcare services. Findings provide significant implications for future research and policy-based interventions focused on eliminating geographic barriers and promoting social and health equity for the underserved.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Despite being one of the largest and fastest growing immigrant populations in the United States, Hispanic and Latino immigrant (HLI) populations experience disproportionately greater health disparities as a result of limited access to healthcare services. Access to healthcare services among HLIs has been shown to vary across the U.S., depending on the geographic location and physical characteristics of the residential environment [1, 2]. Variations in access have been identified in several midwestern and southern regions of the U.S., where local agencies are unable to adequately meet the unique healthcare needs of growing HLI populations [3–7]. Differences in availability and access to healthcare services have also been observed in rural communities experiencing growth in HLI populations, where further limitations in access relative to geospatial factors exist [8, 9]. These findings provide evidence of physical segregation of HLI groups, which leads to social isolation from mainstream community and resources [10]. Harari et al. explored healthcare experiences of recent Latino immigrants in Midwest communities in which 48 % of HLIs reported feeling social isolation, and lack of strong social and information networks [7]. Additionally, it was found that segregated HLI communities located in the outskirts, bordering metropolitan areas usually, have limited availability of and access to healthcare services. Living in isolated communities increases travel time to access services and demands the need for transportation, which serve as additional access barriers.
Limited literature on healthcare access among HLIs warrants further research, especially in southern, inland states like Kentucky where the increasing demands of growing immigrant populations continue to overwhelm current health and social service infrastructures [5, 11–13]. Geographic location serves as a factor for healthcare disparities as populations residing in central states, inner-cities, and rural areas have the highest need for improved quality and access to healthcare services [14]. The National Health Disparities Report found that populations residing in inner-city and rural areas of south-central states like Kentucky are at increased risk for receiving poorer quality of, and access to, healthcare [14]. As an inner-city area in the predominantly rural state of Kentucky, Louisville serves as a prime location to assess health and healthcare access disparities among HLIs. Although it has been identified that immigrants experience difficulties in accessing services in Louisville and surrounding regions, there is limited demographic and health-related data on foreign-born populations, specifically on HLIs, which further impedes the development of strategies to overcome barriers to access. Therefore, the purpose of this study was to examine the geographic factors that serve as barriers to healthcare access for HLIs in Louisville, Kentucky.
Methods
Setting
The setting for the study was Louisville, the largest metropolitan city in Kentucky that has experienced a recent influx of HLIs [11]. According to the Migration Policy Institute, Kentucky is one of the top ten states with the fastest growing foreign-born population [15]. Roughly 50,000 immigrants represent countries from Latin America (38.9 %), Asia (32.4 %), Africa, (15 %), and Europe (16.5 %). Hispanics and Latinos are one of the fastest growing immigrant subgroups in Louisville representing 4 % of the total population [13, 16]. The Hispanic population in Louisville has almost doubled in size since 2000 from an estimated 12,370 to 23,715 in 2010 [17]. Existing data indicated that Louisville has a large concentration of HLI predominantly residing in distinct neighborhood areas such as South Central Louisville and South Louisville [18] (See Fig. 1).

Hispanic and Latino population by census tract in Louisville, with neighborhood boundaries
Statistics on local HLIs are inaccurate and underrepresented because they do not account for undocumented immigrants. Difficulties in obtaining accurate estimates on HLIs and undocumented immigrants have become a local as well as national issue [13, 19]. According to the latest estimates by the Urban Institute, in 2000, 18 % of the Louisville immigrant community was undocumented, with the vast majority representing Mexico and other Latin American countries [5]. Despite immigration reform and stricter border enforcement policies, this number has continued to rise in Louisville.
Data
Accessibility to healthcare services was examined using spatial analysis techniques in a Geographic Information System (GIS). Geographic Information Systems are collections of hardware, software, data, and methods for visualizing, managing, and analyzing all types of geographically referenced data [20, 21]. Using ArcGIS® software and geographic data from the U.S. Census Bureau and the Louisville and Jefferson County Information Consortium (LOJIC) [22], a number of GIS products were derived to demonstrate the spatial distribution and socioeconomic makeup of HLI population in Louisville; the distribution of primary healthcare providers and facilities within the study setting; travel times of HLI populations to acquire health services; and transportation routes, among other variables. All data were open for public access, and anonymity and confidentiality were maintained through de-identification of census data and the use of geocoded data.
Choropleth mapping of demographic data obtained from the U.S. Census Bureau was used to characterize the geographic and social contexts of the HLI population in Louisville. Choropleth mapping is a thematic mapping technique where areas are classified on the values of a statistical variable and shaded proportionally in the map [23]. All data classification utilized the Jenks Natural Breaks method, which for n classes, seeks to minimize variance within classes while maximizing variance between classes [24]. Choropleth maps were produced to visualize the population of HLIs of both census tracts and zip codes; and the socioeconomic status of HLI including median household income, poverty status, educational attainment, and English language skills.
In order to better understand the spatial relationship between the HLI population and healthcare access, the locations of healthcare services were plotted by geocoding the addresses of hospitals, pharmacies, pediatricians, dentists, family health centers (federally qualified health centers), family planning services, family medicine practices, nurse practitioners, eye-care providers, general practice clinics, OBGYN practices, and internal medicine practices. These georeferenced data were then overlain in the GIS with choropleth maps of HLI population for visualization and analysis. To demonstrate real-world access of HLI populations to healthcare, a variety of network analyses were undertaken using street network data obtained from LOJIC [22]. Drive-time analysis models travel time along a street network dataset to produce polygon drive-time areas around input points were based on given drive-time numbers [21]. Drive-time maps were produced for hospitals and family health centers/free clinics at drive-time intervals of 2 min. Resulting drive-time maps were overlain with HLI population data to demonstrate the variable access to these healthcare facilities for concentrations of HLIs in Louisville. Bus route maps were also overlain with HLI population maps to help identify gaps in public transit for residential concentrations of HLIs.
Using GIS technology for the spatial analysis of data significantly strengthened this study by providing a mechanism to visually depict large amounts of census data using maps, and elucidating spatial relationships that may be obscured when observed in tabular formats alone [25]. Furthermore, GIS technology has been identified as an effective measure to evaluate patterns of primary healthcare access and to examine health inequities within various geographic settings [26, 27]. The ability of GIS to locate specific health and social service facilities assists in identifying service delivery regions and the demographic characteristics of these regions. These maps were compared and contrasted with other existing community maps to provide further insight into HLI populations that may have been underrepresented in census data.
Results
Geospatial data helped accurately identify the geographic distribution of HLIs, along with other key socioeconomic factors, such as poverty, income, education, and language that shaped both the physical and social positioning of HLI in Louisville. Using 2010 census data, the physical location of HLIs in Louisville was mapped according to census tracts in Jefferson County for this study (Fig. 1). Findings indicated that HLI populations were predominantly concentrated in southern neighborhoods of Louisville consisting of census tracts 56, 90, 120.02, 114.04, 114.05, 113.02, 110.02, 110.04, and 119.06. Surrounding census tract areas also had a high concentration of HLI and largely represented neighborhood areas of South Louisville, South Central Louisville, Buechel-Newburg-Indian Trail, and Southeast Louisville (See Fig. 1). Geospatial data and community maps indicated distinct concentrations of HLI populations by neighborhoods and census tracts in Louisville. Findings also revealed that while HLI populations were predominantly concentrated in southern regions of Louisville, these groups were also growing at an increasing rate in northeastern regions of the city.
Thematic maps were also used to demonstrate socioeconomic factors of HLIs such as levels of poverty, income, education, and language. In 2012, the USDHHS estimated the poverty level at $23,050 (annual income) for a family of four [28]. The U.S. Census Bureau estimated that from 2007 to 2010, an average of 17.5 % of residents in Louisville were living below the poverty level [29]. Additionally, 41 % of Hispanics and Latinos in Louisville had incomes below the poverty level [13]. Analysis revealed that HLIs living in poverty were primarily concentrated in census tracts 56 and 90, but were also located in census tracts 112.02, 91.05, 119.01, 119.06, 115.05, and 110.02 (Fig. 2a). Census tracts 56 and 90 are located in the neighborhoods of South Louisville and South Central Louisville (Fig. 1).

Indicators of socioeconomic status for Hispanic and Latino population in Louisville, KY
Figure 2b shows the distribution of HLIs in Louisville based on median household income. It must be noted that this thematic map was developed using American Community Survey data from 2005 to 2009 and census tract boundaries for HLIs based on 2000 census data, due to insufficient 2010 census data on this measure. Geospatial analysis revealed that the majority of HLIs with household incomes below $26, 509 resided in census tracts 56, 90, 91.03, 119.04, 119.06, 114.06, 110.02, and 115.05 (Fig. 2b). As indicated in Fig. 3, these census tracts also have a larger number of HLIs living below the poverty level. South Louisville, Fairdale, Buechel-Newburg-Indian Trail, and parts of Highview-Okolona neighborhoods represented the areas with the lowest levels of income among HLIs (See Fig. 1). Generally, HLIs with higher levels of income were shown to reside predominantly in Fern Creek, Jefferson town, and Northeast Jefferson neighborhoods. Therefore, HLIs with low levels of income and those living below the poverty level were primarily concentrated in southern regions of Louisville as indicated by geospatial analysis that revealed distinct physical demarcations of these populations within identified areas.

Distribution of healthcare facilities for Hispanic and Latino population in Louisville
Geospatial analysis revealed that distribution of HLIs in Louisville also varied according to levels of educational attainment (Fig. 2c). Figure 2c shows the percentage of the total Hispanic populations (18 years and older) with educational attainment of a bachelor’s degree or higher. Findings revealed that census tracts with the lowest levels of educational attainment among HLI males and females were scattered across the city, but were generally located in previously identified southern regions of Louisville. Hispanic and Latino immigrants residing in eastern regions of Louisville were more likely to have a bachelor’s degree, and HLIs living in southern regions of Louisville were less likely to have a bachelor’s degree. The distribution of educational levels was shown to correspond with income and poverty maps, indicating that areas with less-educated HLIs also had a significant number of HLIs with incomes below the poverty level.
Language was another demographic characteristic that was shown to geographically vary across Louisville. Interpretation of data revealed variations in English language skills among HLIs (Fig. 2d). Significantly, concentrations of HLIs in southern regions of Louisville were more likely to speak English not well or not at all. Roughly 20 % to 40 % of HLIs residing in census tracts 56, 90, 114.04, 114.06, and 118 did not speak any English at all. Census tracts and neighborhoods with lower levels of English proficiency corresponded to highly concentrated HLI census tracts with lower income and educational levels and higher levels of poverty.
Access to Healthcare Services
Geospatial factors that served as barriers to healthcare access included physical access to healthcare facilities, traveling distance, and transportation. The distribution of hospitals significantly diminished in the southern regions of Louisville with higher concentrations of HLIs (Fig. 4). There were no hospitals located in major populated census tracts in South Louisville, Fairdale, Buechel-Newburg-Indian Trail, and Highview-Okolona areas, which were also identified as impoverished regions of the city (Fig. 4). However, several hospitals were clustered in major populated census tracts in downtown regions and eastern areas of the city, where HLI populations were identified to have higher levels of income, education, and English proficiency levels.

Louisville hospital locations and Hispanic and Latino population by census tract
Similar to the limited distribution of hospitals, the distribution of other healthcare providers and facilities with Spanish-speaking services such as pediatricians, dentists, family health centers, nurse practitioners, and OBGYN practices was scarce in southern regions of Louisville (Fig. 3). Figure 3 depicts the physical location of healthcare facilities that offered interpreter services targeted at Spanish-speaking patients. Pediatric and dental services were dispersed across the city; however, family health centers, OBGYNs, and nurse practitioners were concentrated in northwestern regions of the Louisville. It is important to note that although there were family health centers located in South Louisville, there were no centers located in the Buechel-Newburg-Indian Trail and Highview- Okolona, which also had a large number of HLI populations living in poverty. Additionally, there were no health services in the census tracts that were identified to have higher concentrations of HLIs living in poverty and with limited English proficiency. Discrepancies in the physical location of medical services relative to areas with significant HLI populations were indicative of limited physical access to medical services and inability of healthcare facilities to expand services for HLI populations residing in areas of need.
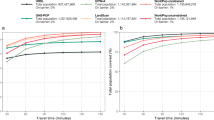
Figures 3 and 4 indicated that there were no hospitals and few family health centers conveniently located in major HLI-populated census tracts. Drive-time/distance measure maps (Figs. 5 and 6) indicated that several census tracts in southern Louisville regions were the farthest away from accessing hospital services. Figure 5 illustrated that HLIs residing in South and South Central Louisville areas had to drive an average of 4 to 8 min to access hospital services, while HLIs in Fairdale, Buechel-Newburg-Indian Trail, and Highview-Okolona areas had to drive anywhere from 6 to over 10 min to access a hospital.

Drive-time to hospitals for Hispanic and Latino population in Louisville

Drive-time to family health centers and free clinic for Hispanic and Latino population
Figure 6 indicates that drive-times to accessing family health centers were also relatively faster for HLIs residing in South and South Central Louisville and for Fairdale areas when compared with those in Buechel-Newburg-Indian Trail and Highview-Okolona neighborhoods. These findings provide evidence for the increased distance and travel time required for HLI populations in southern regions to access affordable or free medical services at family health centers or at the free clinic.
Although several healthcare facilities may have been located within southern regions of Louisville, many HLIs did not have adequate transportation to access these services. Hispanic and Latino immigrants in Louisville relied heavily on the local bus system or Transit Authority of River City (TARC) as their main means of transportation. The TARC bus system was frequently used by many community members, especially for those with low-income and living in poverty. However, findings indicated that TARC services had limited routes and schedules in highly concentrated HLI regions of southern Louisville (Fig. 7). Therefore, limited bus routes served as an additional transportation barrier to accessing health services, especially to hospitals and other medical services that were not centrally located in southern regions of Louisville.

TARC bus access for Hispanic and Latino population in Louisville
Discussion
Geospatial analysis and community maps indicated that geographic factors such as physical location, distance, and transportation played a significant role in shaping the barriers to healthcare access for HLIs living in highly concentrated southern regions of Louisville. Hispanic and Latino immigrant communities were predominantly concentrated in southern regions of Louisville, with distinct socioeconomic characteristics such as higher rates of poverty, linguistic isolation, and lower educational and income levels. Similarly, the Louisville Metro Health Equity Report indicated that southern regions of Louisville, which had the lowest life expectancy rates, also had the highest levels of poverty and crime [18]. Correspondingly, these southern regions with higher concentrations of HLIs had fewer affordable medical service facilities, such as family health centers and/or free clinics. Facilities that provided interpreter services for the Spanish-speaking population were not centrally located in areas of need, and HLIs had to travel longer distances to acquire healthcare services at these locations. Furthermore, limited bus routes and transportation served as additional barriers to accessing healthcare services for HLI communities with the highest need for affordable and linguistically competent services.
Consistent with the review of literature, geospatial analysis, and community mapping results indicated that geographic location and physical characteristics of the environment had significant effects on healthcare access for HLIs in Louisville [4, 30]. Midwest and southern regions of the U.S. with relatively newer populations of HLIs and other immigrant groups were identified in the literature as having substantially greater geospatial limitations to accessing health services, resulting in physical segregation and feelings of social isolation from mainstream society and resources [3, 6–10]. Similarly, the physical segregation of HLIs in this southern, urban community was evident in geospatial analysis, revealing that these communities were also had lower income, educational, and English proficiency levels; access to fewer health resources; longer travel times to healthcare facilities; and limited bus routes for transportation to provider locations when compared with other regions of the city.
The literature indicated that geographic location serves as a factor for healthcare disparities, especially among populations residing in central states, inner-cities, and rural areas that have the highest need for improved quality and access to healthcare services [14]. In order to assess variations in healthcare quality and access disparities across states, achievable benchmark methods that recorded the “frequency with which states perform in the top 10% of states and contribute to the achievable benchmark” were examined [14, p. 10.] Data revealed benchmark states were least often found in the East North Central, East South Central, and West South Central regions of the U.S. Kentucky and its surrounding states, which belong to the East South Central division of the U.S., fell in the third lowest quartile that represented the smallest number of benchmark measures. Within these regions, subdivisions that placed populations at further risk for receiving poorer quality of, and access to healthcare include inner-city and rural areas. Significant disparities in access to care were found among residents in large inner-cities, micropolitan areas, and noncore areas. Similarly, as an inner-city area in the south-central state of Kentucky, the geographic location of southern Louisville placed HLIs at high risks for experiencing poorer health outcomes related to the social determinants of healthcare access. Consistent with findings from previous studies examining barriers to access among HLIs in Louisville, findings from this study indicated that geospatial factors such as long distances and limited transportation were also seminal in shaping barriers to healthcare access for this population [4, 5, 30].
Research findings provided several implications for healthcare system reform in Louisville that promotes equitable access to healthcare services for HLIs. As indicated through geospatial analysis of data, few healthcare facilities and health-related services were available in southern regions of Louisville with higher concentrations of HLIs. Geospatial factors such as distance and transportation served as barriers to healthcare access indicating the need for increased presence of healthcare facilities within these underserved regions. The National Council of La Raza recommends the expansion of federally qualified health centers, free and affordable health clinics, and hospital services through charity care and other community benefits [31]. Additional facilitators to overcoming geospatial barriers to access in geographically underserved areas include the expansion of infrastructure through enhanced affordable and convenient public transportation [32]. Expanding healthcare services in these areas requires the equal distribution of healthcare providers who have the ability serve disadvantaged HLIs in culturally appropriate ways.
It is imperative to increase the presence of healthcare providers, especially advanced practice nurses and licensed primary healthcare providers, through private offices, clinics, and other healthcare facilities in underserved urban communities. Over the years, research has indicated that expanding the role of nurse practitioners has established them as a significant source of primary healthcare in community health clinics and nurse-managed health clinics across the U.S., serving over 20 million patients yearly [33]. Nurse practitioners also work in diverse healthcare settings such as physician practices, managed care facilities, retail or convenient care clinics, providing them with the ability to expand healthcare services in underserved areas. Research indicated that nurse practitioners are more likely to practice in undeserved, lower income areas and predominantly serve minorities and uninsured patients, which is indicative of their ability to promote healthcare access for disadvantaged immigrant groups such as HLIs [34–37]. Therefore, it is recommended that healthcare systems and other social systems work in collaboration to increase the presence of such clinics in southern Louisville, to improve access to vital primary healthcare services for this disadvantaged population.
This study serves as a basis for future research examining the impact of geographic location and place on healthcare access among other HLI communities, highlighting the need to further explore these phenomena on regional and national levels. Findings from this study may not be valid for other geographic regions and must be cautiously applied. Continued research on geographic barriers to healthcare access among HLI subgroups in different settings is warranted. This will provide insight on ways to address contextually based geographic and other social determinants of healthcare access in order to appropriately inform and enhance interventions and policies aimed at reducing health inequities among HLI groups.
Geographic location has been shown to be an influential social determinant of health and healthcare access for certain underserved populations, such as HLIs. In utilizing GIS, this study was able to analyze and concisely depict large amounts of pertinent geographic and demographic data. Study findings provide significant implications and recommendations for future interdisciplinary and collaborative research in nursing, health services research, and GIS studies focused on establishing methods to examine the association between place and disparities in healthcare access and utilization. Future studies must focus on establishing systematic and continuous ways to assess geographic factors that serve as both barriers and facilitators to healthcare access for underserved, marginalized groups [38]. Furthermore, such research can be effectively utilized to inform interventions and policies aimed at promoting social and health equity.
References
Derose KP, Escarce JJ, Lurie N. Immigrants and health care: sources of vulnerability. Health Affairs. 1989;26(5):1258–68.
Gresenz CR, Rogowski J, Escarce JJ. Community demographics and access to health care among U.S. Hispanics. Health Serv Res. 2009;44(5):1542–62.
Abraido-Lanza AF, Cespedes A, Daya S, et al. Satisfaction with health care among Latinas. J Health Poor Underserved. 2011;22(2):491–505.
Alcalde, G. Cross cultural community conversations: beginning the dialogue to understand the strengths and unmet needs of the Hispanic/Latino community in Louisville Metro. 2005. Available at http://www.louisvilleky.gov/OFW/Publications/Reports.htm.
Capps R, Fortuny K, Zimmermann W, et al. A profile of the foreign-born in the Louisville Metropolitan area. Washington, D.C: The Urban Institute; 2006.
Coffman MJ, Shobe MA, Dmochowski J, et al. Health care access and utilization among Latino immigrants. Hispanic Health Care International. 2007;5(2):73–80.
Harari N, Davis M, Heisler M. Strangers in a strange land: health care experiences for recent Latino immigrants in Midwest communities. J Health Poor Underserved. 2008;19(4):1350–67.
Cristancho S, Garces DM, Peters KE, et al. Listening to rural Hispanic immigrants in the Midwest: a community-based participatory assessment of major barriers to health care access and use. Qual Health Res. 2008;18(5):633–46.
Berdahl TA, Kirby JB, Stone RAT. Access to health care for nonmetro and metro Latinos of Mexican origin in the United States. Medical Care. 2007;45(7):647–54.
Khan S, Velazquez V, O’Connor C, et al. Health care access, utilization, and needs in a predominantly Latino immigrant community in Providence, Rhode Island. Med Health: Rhode Island. 2011;94(10):284–7.
Fennelly K. (2006). Listening to the experts: provider recommendations on the health needs of immigrants and refugees. J Cult Div. 2006;13(4):190–200.
City-Data.com. Louisville, Kentucky poverty rate data—information about poor and low income residents. Illinois: Advameg, Inc.; 2013.
White C.. New survey shows Louisville’s growing Hispanic population lacks access to health care. Louisville, KY: Courier-Journal.com, 2011.
Agency for Healthcare Research and Quality. 2010 National Healthcare Disparities Report. Rockville, MD: U.S. Department of Health and Human Services; 2010.
Migration Policy Institute. Kentucky factsheet on the foreign born: demographic and social characteristics. Washington, D.C: Migration Policy Institute; 2007.
Office of Policy Planning and Evaluation. Louisville Metro Health Status Report. Louisville, KY: Louisville Metro Department of Public Health and Wellness, 2012.
U.S. Census Bureau. Language use. Washington, DC: U.S. Census Bureau; 2010.
Center for Health Equity. Louisville metro health equity report: the social determinants of health in Louisville metro neighborhoods. Louisville, KY: Louisville Metro Department of Public Health and Wellness; 2012.
Legislative Research Commission. Immigration in Kentucky. Frankfort, Kentucky: Legislative Research Commission, 2002.
Gatrell AC. Geographies of health: an introduction. Maiden (MA): Blackwell Publishers; 2002.
ESRI. ArcGIC desktop: release 10. Redlands, CA: Environmental Systems Research Institute; 2011.
Louisville and Jefferson County Information Consortium. Jefferson County geodatabase files. Louisville, KY: LOJIC; 2012.
Robinson AH, Morrison JL, Muehrke PC, et al. Elements of cartography. 6th ed. New York: Wiley; 1995.
Jenks GF. The data model concept in statistical mapping. International Yearbook Cartography. 1967;7:186–90.
Albert DP, Gesler WM, Wittie PS. Geographic information system. In: Albert DP, Gesler WM, Levergood B, editors. Spatial analysis, GIS, and remote sensing applications in the health sciences. Chelsea MI: Ann Arbor Press; 2000.
Dulin MF, Tapp H, Smith HA, et al. A trans-disciplinary approach to the evaluation of social determinants of health in a Hispanic population. BMP Public Health. 2012;12:769–79.
Phillips RL, Kinman EL, Schnitzer PG, et al. Using geographic information systems to understand health care access. Arch Fam Med. 2000;9(19):971–8.
U.S. Department of Health and Human Services. HHS poverty guidelines. Washington, DC: USDHHS; 2012. p. 2012.
Census Bureau US. State and county quick facts. Washington, DC: U.S. Census Bureau; 2013.
Friedrich JM. Systemic barriers for Latina women accessing healthcare services in Louisville, Kentucky: an assessment of social indicators in order to disclose social injustices. (Doctoral Dissertation). ProQuest Dissertations and Theses, 2009.
National Council of La Raza. Overcoming immigrant barriers to coverage: options for health care when major programs don’t cut it. Washington, D.C: National Council of La Raza, 2011.
Keating S, Carlson B, Jimenez S, et al. Psychometric testing of the immigrant barriers to health care scale: Hispanic version. Nursing and Health Sciences. 2009;11(3):235–43.
Kaiser Commission on Medicaid and the Uninsured. Improving access to adult primary care in Medicaid: exploring the potential role of nurse practitioners and physician assistants. Washington, D.C: The Henry J. Kaiser Family Foundation, 2011.
Stange K, Sampson D. Nurse practitioners and physician assistants in the United States: current patterns of distribution and recent trends. Princeton, NJ: Robert Wood Johnson Foundation; 2010.
Grumbach K, Hart GL, Mertz E, et al. Who is caring for the underserved? A comparison of primary care physicians and nonphysician clinicians in California and Washington. Annals of Family Medicine. 2003;1(2):97–104.
Hansen-Turton T, Line L, O’Connell M, et al. The nursing center model of health Care for the Underserved. Philadelphia, PA: National Nursing Centers Consortium; 2004.
Office of Technology Assessment. Nurse practitioners, physician assistants and certified nurse midwives: a policy analysis. Washington, D.C: U.S. Congress, 1986.
White K, Haas JS, Williams DR. Elucidating the role of place in health care disparities: the example of racial/ethnic residential segregation. Health Serv Res. 2012;46(3):1278–99.
Acknowledgments
Kentucky Nurses Association.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This study was funded by the Kentucky Nurses Foundation Research Grant program.
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Edward, J., Biddle, D.J. Using Geographic Information Systems (GIS) to Examine Barriers to Healthcare Access for Hispanic and Latino Immigrants in the U.S. South. J. Racial and Ethnic Health Disparities 4, 297–307 (2017). https://doi.org/10.1007/s40615-016-0229-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40615-016-0229-9