
Abstract
Despite overall gains in life expectancy at birth among Los Angeles County residents, significant disparities persist across population subgroups. The purpose of this study was to quantify the potential sex- and race/ethnicity-specific gains in life expectancy had we been able to fully or partially eliminate the leading causes of death in Los Angeles County. Complete annual life tables for local residents were generated by applying the same method used for the National Center of Health Statistics US life tables published in 1999. Based on 2010 Los Angeles County mortality records, sex- and race/ethnicity-specific potential gains in life expectancy were calculated using scenarios of 10, 20, 50, and 100 % elimination of 12 major causes of death. Coronary heart disease, the leading cause of death, was found to be most impactful on life expectancy. Its hypothetical full elimination would result in life expectancy gains ranging from 2.2 years among white females to 3.7 years among black males. Gains from complete elimination of lung cancer and stroke ranked second, with almost an additional year of life for each gender. However, marked disparities across racial/ethnic groups were noted from the elimination of several other causes of death, such as homicide, from which the gain among black males exceeded 13 times more than their white counterparts. By differentially targeting specific causes of death in disease prevention, not only can findings of this study aid in efficiently narrowing racial/ethnic disparities, they can also provide a quantitative means to identify and rank priorities in local health policymaking.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Life expectancy has been steadily increasing in the USA, but large racial and ethnic disparities remain [1]. This pattern is reflected in local jurisdictions as well. Los Angeles County, a major metropolitan jurisdiction, has one of the largest and most racially and ethnically diverse populations in the USA. With 88 incorporated cities and 53 unincorporated areas, Los Angeles County is home to over 10 million people, making it the most populous county in the nation [2, 3]. In 2013, the demographic composition of Los Angeles County consisted of approximately 48 % Latino, 28 % white, 15 % Asian/Native Hawaiian or other Pacific Islander (NHOPI), 9 % black, and 0.2 % American Indian or Alaska Native [3]. Overall life expectancy at birth for county residents has increased by an average of 0.29 years annually since 1991. More specifically, gains were observed among both genders, and all major racial/ethnic groups. However, these gains have not been equal across groups and substantial disparities in life expectancy have been reported [4].
To further examine these disparities, we looked at life expectancy trends by race/ethnicity from 2000 to 2010. We also generated sex- and race/ethnicity-specific life tables to quantify the potential gains in life expectancy resulting from partial to complete elimination of 12 major causes of death in Los Angeles County. The primary objective of the study was to illustrate a practical approach that can be applied to evaluate the impact that reductions in specific causes of death might have on (1) potential gains in life expectancy overall and (2) reducing racial/ethnic disparities in life expectancy. These findings could be used to inform policymakers on the potential value of interventions targeting specific causes of death.
Methods
Calculating Life Expectancy at Birth
To derive annual life expectancies at birth over the period of 2000 to 2010 among various subgroups of Los Angeles County residents, we first acquired via the Los Angeles County Vital Records Office the death statistical master files assembled by the California Department of Public Health [5]. Based on residence geocoding, county death records were extracted for subsequent generation of complete annual life tables. Registration completeness of death records was high, well capturing decedent's personal details and International Classification of Diseases 10th Revision (ICD-10) coded underlying cause of death. For the study period of 2000–2010, a total of 648,694 death records (99.9 %) were included in the overall life expectancy calculations. Among them, 647,899 records (99.9 %) contained usable race/ethnicity data for subgroup calculations. Mid-year resident population estimates were used as denominators for age-specific death rate derivations [6–8].
To convert age-specific death rates to probability of dying used for survivorship calculations in the life tables, we applied the methodology published by the National Center for Health Statistics [9]. Considering the substantial increase in survival at older ages in the USA over the last century, rising from about 6 % survival at age 85 years in 1900 to about 40 % in 2004, this method extends the open-ended age interval to age 100 years and over, and derives age-specific mortality rates for those over age 85 years using Medicare data for improved accuracy. In our study, the coefficients used for mortality rate adjustment were based on the most up-to-date insured Medicare data available at the time [10]. All computations were performed using SAS software version 9.3 for Windows.
Classification of Race/Ethnicity
To examine disparities in life expectancy across population subgroups, both sex- and race/ethnicity-specific life expectancy calculations were performed. The following four mutually exclusive race/ethnicity classifications were included in the analysis: white, black, and Asian/NHOPI (all of non‐Hispanic descent) as well as Latino/Hispanic. American Indians or Alaska Natives (including Eskimos and Aleuts) were also initially examined, but this relatively small group was subsequently excluded because most of its age-specific death counts were found to be too small to provide stable results. This left a total of eight sex- and race/ethnicity-specific population subgroups in the analysis.
Leading Causes of Death
Twelve major underlying causes of death were selected in the analysis, including the top 10 leading causes of death in Los Angeles County in 2010, as well as human immunodeficiency virus (HIV) infection, a leading cause of premature death among young black males; and homicide, a leading cause of death among both Latinos and blacks [11] (Table 1).
Calculating Potential Gains in Life Expectancy at Birth
The impact from each cause of death was quantified by measuring the hypothetical gain in life expectancy at birth if the deaths from a cause were reduced by 10, 20, 50, and 100 %. In our analysis, we used 2010 death records, the latest data available, to produce new life tables for Los Angeles County that would result from these incremental decreases in mortality (Table 2). The reduction in cause-specific number of deaths was assumed to be proportionally distributed across all ages within each population subgroup. For instance, 10 % homicide deaths were reduced for every age from 0 to over 100 years among all white males. Potential gains were then determined by comparing the projected life expectancy values to the original values for each sex- and race/ethnicity-specific group. To illustrate relative gains, inter-racial/ethnic comparisons were made using intra-cause rankings and by calculating ratios of life expectancy gains using the white population as the reference group.
Results
Trends in Life Expectancy at Birth
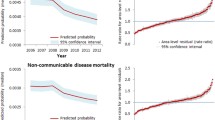
From 2000 to 2010, both male and female Los Angeles County residents enjoyed steady improvements in life expectancy at birth. In 2010, life expectancy at birth was 78.9 years for males and 84.0 years for females, representing an increase of 2.9 and 2.7 years, respectively, since 2000. A positive trend was observed among all sex- and racial/ethnic-specific subgroups, with the largest gain (3.9 years) observed among black males, and the smallest (1.7 years) among Latinas (Fig. 1). Males in each racial/ethnic group had greater gains in life expectancy than females. In 2010, Asian/NHOPI females had the longest life expectancy at birth (87.6 years), while black males had the shortest (72.0 years), a 15.6-year difference.

Life expectancy at birth (in years) by race/ethnicity and sex, Los Angeles County 2000–2010
The relative rankings of life expectancy among the four major racial/ethnic groups persisted throughout the time period for both males and females. Asians/NHOPI had the highest life expectancy, followed closely by Latinos (−3.2 years for males, −2.0 years for females), and whites (−5.0 years for males, −4.5 years for females). Life expectancy among blacks was much lower compared to all other groups (−11.5 years for males, −8.6 years in females). Furthermore, babies born in Los Angeles County in 2010 were expected to live to 81.5 years, almost 3 years longer than the US average [1].
Potential Gains in Life Expectancies from Reduction of Specific Causes
Coronary heart disease (CHD) was the leading cause of death among all racial/ethnic groups in 2010, accounting for 22 % of all deaths in the Los Angeles County [11]. Deaths from CHD occurred mostly among older individuals (10,189 or 81 % of CHD deaths were individuals aged 65 years and older), and therefore would theoretically contribute relatively little to life expectancy at birth. However, the potential gains among both male and female residents from the complete elimination of CHD was greater than for all other causes due to the sheer number of cases. This resulted in life expectancy gains of 2.89 and 2.38 years for males and females, respectively (see Appendix: Tables 3 and 4). The potential life expectancy gains pertaining to elimination of other causes studied were generally small in absolute terms, ranging from 0.02 years for HIV among females to 0.72 years for lung cancer among males (Fig. 2). Overall trends in potential gains roughly paralleled the mortality trends except for homicide among males, and Alzheimer’s disease and breast cancer among females.

Potential gains in life expectancy at birth (in years) by sex from 100 % disease elimination, Los Angeles County 2010
Blacks showed the largest potential gains for most conditions relative to the other groups (Table 2). This was particularly evident for homicide, from which black males and females would receive 13.3 and 6.3 times greater gains, respectively, than their white counterparts (Fig. 3a, b). With the elimination HIV deaths, black females would have 5.6 times greater potential gains in life expectancy compared to white females. In contrast, there were only a few causes where whites or Asians/NHOPI had the largest potential gains. With the elimination of emphysema/COPD and Alzheimer’s disease, both white males and females would experience greater potential gains compared to other racial/ethnic groups. For Asian/NHOPI males, eradicating stroke and pneumonia/influenza deaths would produce potential gains 2.4 and 1.8 times that of white males, respectively. Latinos showed the greatest potential gains from the removal of liver disease and diabetes. For liver disease elimination specifically, Latino males would have more than double the potential gain of life expectancy compared to white males.

a Male potential gains in life expectancy at birth (in years) by race/ethnicity from 100 % disease elimination, Los Angeles County 2010. b Female potential gains in life expectancy at birth (in years) by race/ethnicity from 100 % disease elimination, Los Angeles County 2010
Discussion
Mortality rates and life expectancy are two commonly used indicators for a population’s health status. They reflect the impact of major illnesses and injuries, and their underlying causes—including social, economic, and environmental conditions. A thorough understanding of mortality patterns in a population is essential for formulating sound health policy, and decreases in cause-specific mortality rates are frequently used for setting population health goals. However, mortality rates can be misleading if the underlying demographic structure of the population is not well understood. Using standardized mortality rates can only partially correct the problem, since the selection of a standard population itself significantly affects the results. On the other hand, life expectancy at birth can be regarded as a composite index summarizing the mortality pattern that prevails across all age groups. Although the relationship between life expectancy and mortality is mathematically complex, the relationship is in essence reciprocal. Quantifying cause-specific impacts on life expectancy may therefore be a useful alternative for conveying analogous information to policymakers in a more easily interpretable form.
Our results highlight the disparities in life expectancy between males and females, and among different racial/ethnic groups. At its worst, there is an unconscionable 16-year gap in life expectancy between black males and Asian/NHOPI females. This study demonstrates the usefulness of life table analysis in identifying major causes of death which contribute to these disparities, through examining potential gains in life expectancy at birth from the reduction or elimination of specific causes of death. Quantifying potential gains is effective for illustrating cause-specific impacts on overall life expectancy, as well as their differential impacts on racial/ethnic disparities.
Our results show that reducing CHD deaths has the greatest potential for increasing life expectancy across all four racial/ethnic groups. The elimination of CHD would result in an additional 2.9 years of life for males and 2.4 years for females. Results for homicide and HIV reduction, however, highlight the opportunities that exist for reducing racial/ethnic disparities in life expectancy. Although these causes of death appear to have less of an impact on overall life expectancy when examining absolute gains, the differences in relative gains among the racial groups are very pronounced. Blacks showed the largest potential gains for many causes and particularly striking relative gains for homicide and HIV, which is consistent with previous studies [12–14].
Coronary Heart Disease
CHD continues to be the leading cause of death, and as expected, its elimination yields the greatest gains in life expectancy for all races. The racial disparities are less striking when studying CHD in relation to other causes of death, but its reduction and elimination still yields the greatest gains for blacks relative to other races/ethnicities. Factors that may explain blacks’ increased CHD mortality include their high prevalence of risk factors such as hypertension, obesity, and physical inactivity [12]. Related to these factors are important social issues, such as differential access to care and socioeconomic status (SES)—which affect one’s health status, ability to obtain health services, and likelihood of participating in health-promoting practices [12, 15].
Homicide
In our study, the most striking disparities in potential gains in life expectancy were observed for homicide. If homicide was completely eliminated, black males would gain 13 times more and Latino males almost four times more in life expectancy, in comparison to their white counterparts. Although homicide was the 17th leading cause of death in the overall county population, it is the second leading cause of premature death, or death before 75 years of age. More specifically, among black and Latino males, it is the leading cause of premature death [11]. Racial disparities in life expectancy related to homicide deaths in Los Angeles County have been previously reported [14, 16]. There are a multitude of factors that contribute to high homicide rates, including neighborhood poverty, availability of firearms, and other social environmental factors—such as high unemployment, presence of gang activity, limited access to quality education, family disruption, and low levels of social cohesion [16–19].
Human Immunodeficiency Virus
The disproportionate HIV mortality in blacks is another major contributor to life expectancy disparities. HIV is an infectious disease that has transformed into a largely chronic illness with the advent of highly active antiretroviral therapy (HAART) [13]. Due to the high effectiveness of HAART, HIV mortality has declined significantly in the overall population [20]. However, there are racial differences in these declines, which are likely related to delayed diagnosis, and differential access and adherence to HAART treatment [21, 22]. Studies have shown that blacks were less likely to receive HAART and had lower rates of antiretroviral medication use in comparison to other races, potentially increasing the risk of HIV mortality among this population [22].
Policy Implications
Despite recent improvements in life expectancy, our analysis highlights the striking disparities that persist across racial/ethnic groups. Understanding the factors that contribute most to life expectancy and the root causes of disparities can help communities, policymakers, and public health officials identify effective strategies and targets for interventions to reduce these disparities and to promote longevity for all groups.
One strategy would be to focus resources on preventing all deaths from CHD, which would result in the largest potential gains overall. Despite the high prevalence of CHD across all major racial groups, blacks still stand to gain the most life-years with its reduction. To achieve greater reductions in life expectancy disparities, however, a more effective strategy might be to focus on the diseases and injuries that have the greatest influence on these disparities, such as homicide and HIV. In addition to disproportionately impacting blacks, both causes of death tend to impact younger, working age populations, and have significant implications for long-term economic costs and productivity [23]. There are a broad range of strategies that can be applied, and multisectorial approaches are needed. Strategies to reduce homicides may include decreasing the availability of firearms, increased community policing, providing economic opportunities, increasing high school graduation rates, increasing social cohesion, and creating safe physical environments that foster community interaction [24–26]. Efforts to reduce HIV mortality could include implementing community-level interventions to build individual skills to reduce HIV risk behavior, changing sexual norms, and increasing condom use among high-risk populations, and improving access to HIV testing and treatment [27].
In either case, it is clear that any significant progress in improving life expectancy and reducing disparities will require multisectorial approaches that address the underlying environmental and sociocultural causes that contribute to disproportionately high mortality—including lack of educational opportunities, poverty, racism, poor access to health care, and living in communities with unsafe neighborhoods and higher levels of social disorder [15].
Limitations
As our analysis was solely dependent upon single, underlying causes of death, it implicitly assumed that there were no interdependencies among different causes of deaths. However, in reality, this is often not the case since a given disease may render individuals more susceptible or resistant to some other diseases. Certain diseases, such as diabetes mellitus and CHD, tend to frequently co-occur. These interdependencies are complex and have yet to be accurately quantified. We felt that our assumption of independence was suitable for the purposes of the study. Similarly, we made no attempt to take the mortality with competing risks approach, which might otherwise cause even more incongruity as we had assumed the increases in death rates from competing causes were negligible, and could otherwise further distort the potential gains from our calculation. In utilizing our findings, it would therefore be judicious to focus on relative rankings than absolute values of the gains derived. Further, since many deaths could be attributed to multiple causes, it has always been difficult to assign a single specific cause to each death especially amid diseases known to have common risk factors [28]. Although at the national level, a standardized algorithm is applied in deciding on the underlying cause of death to minimize potential biases, death certificates are still unduly susceptible to misclassification. Hence, there exists a high likelihood of underestimation of those chronic ailments that frequently lead to diseases of high fatality, such as diabetes mellitus or hypertension. [13]. This would be of less concern in dealing with diseases that are pathologically distinct [28].
As compared to other leading causes of death, the life expectancy gains associated with chronic ailments that generally occur later in life, such as CHD and cancers, might have also been underestimated in our calculation. This is due to their disproportionately higher prevalence among the older populations, pushing the number of deaths falsely low as many of the elderly would probably die of other acute causes. Further, limited exclusively to life expectancy, our study fell short of making any quantitative assessment of overall disease burden or years of quality of life lived. Analyses from those perspectives may shed more light on the true burden of disease, specifically across diverse racial/ethnic groups, and suggest different targets for intervention.
Conclusion
Understanding the mortality patterns in a population, including historical trends, underlying determinants, contributing factors and disparities, is essential to formulating sound health policy. While eliminating coronary heart disease could result in the greatest potential gains in life expectancy for all races, we found striking disparities for homicide and HIV, especially among blacks. In spite of the known limitations, these results provide a useful means for identifying and ranking priorities in public health policy formation.
As occurred in the rest of the nation, residents of Los Angeles County enjoyed a steady rise in longevity over the last few decades. However, substantial dipartites in general health among racial and ethnic subgroups of the population remained. Through applying multiple hypothetical mortality eliminations to local vital records, this study quantifies the differential impacts of major causes of death on life expectancy. While biological and risk behavior differences are likely playing important roles, underlying factors pertinent to both physical and social environments have long been recognized as influential components.
Social determinants, such as income, educational attainment, and access to primary care etc. are tightly correlated with population health [29, 30]. However, the insufficiency of reporting on death certificates prohibited stratified analyses with tolerable levels of statistical confidence. It would be therefore worth replicating the study using data aggregated from a longer period of time or larger jurisdictions to strengthen the validity of the method in future work.
The quantitative approach presented in this article may prove valuable in delineating further population health evaluation in terms of life expectancy, a health indicator gaining popularity in recent years partly due to its intuitiveness. Focused public health efforts directed at decreasing mortality from specific causes of death are needed, as well as policy and system changes that would foster communities and environments in which people of all backgrounds can benefit. Mitigating both individual and environmental risk factors associated with preventable causes of death should be the priority for policymakers, communities, and public health officials if they hope to effectively eliminate life expectancy disparities, and prolong overall longevity.
References
Murphy SL, Xu JQ, Kochanek KD. Deaths: final data for 2010. Natl Vital Stat Rep. 2013;61(4).
US Census Bureau. Cartographic boundary files - places (Incorporated Places and Census Designated Places). 2011. http://www.census.gov/geo/maps-data/data/cbf/cbf_place.html. Accessed 16 Apr 2015.
Hedderson Demographic Services. July 1, 2013 population estimates [dataset]. Los Angeles: Los Angeles County Internal Services Department; 2014.
Los Angeles County Department of Public Health, Office of Health Assessment and Epidemiology. Life expectancy in Los Angeles County: how long do we live and why? A cities and communities report. Los Angeles: Los Angeles County Department of Public Health; 2010.
State of California, Department of Public Health. 2000–2010 Death statistical master files for Los Angeles County residents [dataset]. Los Angeles: Los Angeles County Department of Public Health; 2012.
Walter R. McDonald & Associates. Inc. July 1, 2000 population estimates [dataset]. Los Angeles: Los Angeles County Internal Services Department; 2007.
Hedderson Demographic Services. July 1, 2010 population estimates [dataset]. Los Angeles: Los Angeles County Internal Services Department; 2012.
Los Angeles County Department of Public Health, Office of Health Assessment and Epidemiology. July 1, 2001–2009 smoothed population estimates [dataset]. Los Angeles: Los Angeles County Department of Public Health; 2013.
Anderson RN. A method for constructing complete annual U.S. life tables. Vital Health Stat. 1999;2(129).
Arias E. United States life tables, 2004. Natl Vital Stat Rep. 2007;56(9).
Los Angeles County Department of Public Health, Office of Health Assessment and Epidemiology. Mortality in Los Angeles County 2010: leading causes of death and premature death with trends for 2001–2010. Los Angeles: Los Angeles County Department of Public Health; 2013.
Palaniappan L, Wang Y, Fortmann SP. Coronary heart disease mortality for six ethnic groups in California, 1990–2000. Ann Epidemiol. 2004;14(7):499–506.
Harper S, Lynch J, Burris S, Davey SG. Trends in the black-white life expectancy gap in the United States, 1983–2003. JAMA. 2007;297(11):1224–32.
Redelings M, Lieb L, Sorvillo F. Years off your life? The effects of homicide on life expectancy by neighborhood and race/ethnicity in Los Angeles County. J Urban Health. 2010;87(4):670–6.
Williams DR, Jackson PB. Social sources of racial disparities in health. Health Aff (Millwood). 2005;24(2):325–34.
From the Centers for Disease Control and Prevention. Influence of homicide on racial disparity in life expectancy–United States, 1998. JAMA. 2001;286(22):2805–6.
Wilkinson RG, Kawachi I, Kennedy BP. Mortality, the social environment, crime and violence. Soc Health Illness. 1998;20(5):578–97.
Kawachi I, Kennedy BP, Lochner K, Prothrow-Stith D. Social capital, income inequality, and mortality. Am J Public Health. 1997;87(9):1491–8.
Robinson PL, Boscardin WJ, George SM, Teklehaimanot S, Heslin KC, Bluthenthal RN. The effect of urban street gang densities on small area homicide incidence in a large metropolitan county, 1994–2002. J Urban Health. 2009;86(4):511–23.
Gebo KA, Fleishman JA, Conviser R, et al. Racial and gender disparities in receipt of highly active antiretroviral therapy persist in a multistate sample of HIV patients in 2001. J Acquir Immune Defic Syndr. 2005;38(1):96–103.
Lai D, Tsai SP, Hardy RJ. Impact of HIV/AIDS on life expectancy in the United States. AIDS. 1997;11(2):203–7.
Lai DJ, Tarwater PM, Hardy RJ. Measuring the impact of HIV/AIDS, heart disease and malignant neoplasms on life expectancy in the USA from 1987 to 2000. Public Health. 2006;120(6):486–92.
Tsai SP, Lee ES, Hardy RJ. The effect of a reduction in leading causes of death: potential gains in life expectancy. Am J Public Health. 1978;68(10):966–71.
Cohen L, Swift S. A public health approach to the violence epidemic in the United States. Environ Urban. 1993;5(2):50–66.
Resnick MD, Ireland M, Borowsky I. Youth violence perpetration: what protects? What predicts? Findings from the national longitudinal study of adolescent health. J Adolesc Health. 2004;35(5):424.e1–10.
Office of the Surgeon General, National Center for Injury Prevention and Control, National Institute of Mental Health, and Center for Mental Health Services. Youth violence: a report of the Surgeon General. Rockville, MD: Office of Surgeon General; 2001.
Sutton MY, Jones RL, Wolitski RJ, Cleveland JC, Dean HD, Fenton KA. A review of the centers for disease control and prevention’s response to the HIV/AIDS crisis among blacks in the United States, 1981–2009. Am J Public Health. 2009;99 Suppl 2:S351–9.
Wong MD, Shapiro MF, Boscardin WJ, Ettner SL. Contribution of major diseases to disparities in mortality. N Engl J Med. 2002;347(20):1585–92.
Frieden TR. A framework for public health action: the health impact pyramid. Am J Public Health. 2010;100(4):590–5.
Galea S, Tracy M, Hoggatt KJ, Dimaggio C, Karpati A. Estimated deaths attributable to social factors in the United States. Am J Public Health. 2011;101(8):1456–65.
Acknowledgments
This work was partially supported by the National Institute of Environmental Health Sciences under Grant T32ES013678. We thank Ricardo Basurto-Davila, PhD, MS, and Douglas Frye, MD, MPH for commenting on our final study report.
Compliance with Ethical Standards
ᅟ
Ethical Approval
This study involved secondary data analysis of publically available data and is exempted research. This article does not contain any studies with animals performed by any of the authors.
Conflict of Interest
Alex Ho, Heena Hameed, Alice W. Lee, and Margaret Shih declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Rights and permissions
About this article

Cite this article
Ho, A., Hameed, H., Lee, A.W. et al. Potential Gains in Life Expectancy from Reductions in Leading Causes of Death, Los Angeles County: a Quantitative Approach to Identify Candidate Diseases for Prevention and Burden Disparities Elimination. J. Racial and Ethnic Health Disparities 3, 431–443 (2016). https://doi.org/10.1007/s40615-015-0156-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40615-015-0156-1