
Abstract
Background
The study analyzes the association between substance use among scheduled tribe men mostly known for their primitiveness, geographical isolation, insecurity, social, educational, and economic backwardness, and non-scheduled tribe men in India’s northeastern state and the eastern state of West Bengal.
Methods
The analysis of data representative across the country from the National Family and Health Survey's fifth wave (NFHS-5), which was conducted in 2019-2020, evaluated the prevalence of tobacco and alcohol use among 12,950 men between the ages of 15 and 54. Logistic regressions and bivariate analyses were performed to analyze the relationship between the socio-demographic determinants of substance use among ST and non-ST men.
Results
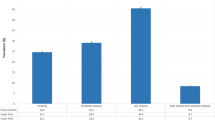
It has been found significant that 30.62% of non-ST males and 39.14% of ST males in the study’s sample consume any form of tobacco, whereas 49.23% of ST men and 29.56% of non-ST men consume alcohol. Men in the middle age groups, lower or uneducated, divorced, separated, or deserted, mainly from the urban residence; others, Buddhist, Hindu, and Christian religions belonging to the wealth quintiles of the poorest to richest; also, the unorganized workers consumed higher quantities of substances. Based on a correlation study between substance use and socioeconomic factors, middle-aged males who work in unorganized jobs, follow other religions, are from worse socioeconomic quintiles, are divorced, separated, deserted, or widowed are much more likely to consume substances.
Conclusion
This study concludes that both smoking and non-smoking tobacco substance, mostly alcohol, is more common among ST men compared to the non-STs in WB and NEI due to low sociodemographic status. The study also highlights the regional differences in substance use among both communities. However, there is a need to address substance misuse among the most vulnerable socioeconomic groups as it concerns their health and well-being.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The term “substance abuse” refers to the unsafe or abusive use of psychoactive substances, such as alcohol and illegal narcotics, that have negative health consequences and impose an immense financial strain on people, their families, and their communities. It is influenced by several variables, including sociodemographic ones, such as the population’s gender, age group, family dynamics, and social and economic status. (Substance Abuse | WHO, 2023). According to the WHO, more than 8 million deaths annually due to tobacco use remain among the most severe challenges to public health (Tobacco, 2023). On the other hand, as per WHO, alcohol abuse causes 3 million deaths globally each year. The consumption of alcohol increases the risk of psychological and behavioral conditions, non-communicable severe diseases such as liver cirrhosis, particular types of cancer, and cardiovascular disorders (WHO Factsheets, 2022).
The NFHS-V (2019–20) reports that 39% of Indian men between 15 and 49 smoke tobacco products. The most common form of tobacco use among men is chewing paan masala or gutkha (15%), followed by cigarette smoking (13%), khaini use (12%), and bidi smoking (7%) are the following most common methods. Twenty-two percent of men drink alcohol. Apart from that, it has been reported that the tribes drink alcohol more often (International Institute for Population Sciences and MoHFW, 2021). Mostly, the northeastern Indian states have the highest proportion of tobacco consumption among all Indian states and UTs, including Mizoram (73%), which has the highest rate of tobacco use of any of the States or UT, Manipur, and Meghalaya (58% apiece), Tripura (57%), and Assam (Singh et al., 2023). It is found that men who consume tobacco and alcohol considerably raise their risk of developing diabetes or heart disease. Numerous studies show an association between substance abuse and non-communicable diseases, showing that males from all socioeconomic groups, regardless of ethnicity, have a much higher risk of being diagnosed with diabetes or heart disease, also one of the significant risk factors of early mortality globally, and tuberculosis also the considerable health risk among the disadvantaged tribal population (Acharyya & Ghosh, 2022; Kumari & Salve, 2020; Fu et al., 2014; Rao et al., 2017).
These tribal people are distinguished by their unique culture, belief system, livelihood, organizational structure, dietary behaviors, traditions, and dialects, which differ from the cultures of the mainstream communities in which they dwell (Indigenous Peoples at the United Nations, n.d.). According to the 2011 Census of India, India consists of numerous scheduled tribe communities, accounting for approximately 5.8% of the population. West Bengal accounts for 5.08% of the total STs in India, with 40 ethnic groups (Scheduled Tribes of West Bengal, n.d.). There are 135 recognized tribes in India’s North Eastern States (Lhungdim et al., 2021) with an ST population percentage of 27.7% of the total STs in India (Ministry of Development of North Eastern Region, n.d.). It is found that compared to non-indigenous communities, the indigenous tribal communities take substance abuse more frequently (Sadath et al., 2021). Furthermore, increased alcohol intake was commonly shown to be one of the crucial factors that may have correlated to domestic violence against women, particularly in India’s northeastern region (Haobijam & Singh, 2021). Smoking is more common in India’s eastern and north-eastern regions, where there exists a significant difference in tobacco use between different states that reflects geographical, religious, cultural, and social factors regarding substance abuse, about scheduled tribes having the most prominent chances of substance use (Bhawna, 2013; Ruhil, 2019). Tikhute (2023) also found that the geographical clustering of smoking and alcohol consumption is moderate to high in the study region of the Eastern states of West Bengal and the North Eastern States of India. However, among all regions of the country, the Northeast has the highest rate of alcohol and tobacco consumption (Kalita, 2022). According to the NFHS-5, the consumption of illicit substances and a comparison between Eastern Indian state (West Bengal) and Northeastern India at the district and state-level prevalence of tobacco and alcohol use among men (15–54 years) was overviewed with an administrative boundary of India (Fig. 1) to demonstrate the State/UT-wise prevalence of tobacco and alcohol consumption across the country. This spatial approach shows that men in the Eastern and North Eastern states are highly prevalent in substance use compared to other States/ UTs in India.

Portrays the consumption of substance such as tobacco and alcohol consumption among men (15–54 years) in all the states and union territories (UTs) of India, NFHS-5. State/UTs comparison of A tobacco and B alcohol consumption in men (15–54 years). Also, the State/Districts level comparison of C tobacco and D alcohol consumption in West Bengal and North Eastern States of India
In the North Eastern States of India and the Eastern State (West Bengal), no prior study has investigated substance consumption patterns and their correlations among scheduled tribes and non-scheduled tribe men. For this, the study has assessed the prevalence and extent of substance abuse in West Bengal and Northeast India. Furthermore, the study also enclosed the socioeconomic elements that influence ST and non-ST males’ substance usage in the age group of 15 to 54 years in WB and NEI. Through conducting this study, it has been possible to determine the demographic groups that needed interventions to reduce the use of illicit substances within the region and the actual and proportional burden of substance consumption.
Methods
Data Source
The study used information from the National Family Health Survey’s fifth round (NFHS-5). This NFHS-5 survey in India included data from 28 states and eight union territories, which was a cross-sectional, representative of the country survey that included men aged 15 to 54. For the study to provide district-level estimates, a two-stage sample design was used in each district’s urban and rural regions in India. In the NFHS-5, interviews were conducted with 636,699 households, 724,115 women, and 101,839 males from 30,198 primary sample units, which included both rural and urban census enumeration blocks scattered across 707 districts of India. The survey focused on the male population and had questions about demographic and socioeconomic traits (Fig. 2). Following the needs of the study, data from this large-scale, nationally representative survey were used to calculate the prevalence of substance misuse (including drinking, smoking, and use of smokeless tobacco) and its relationship to socioeconomic factors among men from ST and non-ST communities in India who were between the ages of 15 and 54. From a total sample of 101,839 men in India between the ages of 15 and 54 years, 12,950 men have been selected representing the eight North-Eastern states of Arunachal Pradesh, Assam, Manipur, Meghalaya, Mizoram, Nagaland, Sikkim, and Tripura, as well as the Eastern state of West Bengal.

Flowchart outlining the current research study’s data selection criteria
Socio-Economic and Demographic Variables
The following explanatory variables were taken into account in the study: the age of the male respondents in 4 categories (15 to 19 years, 20 to 34 years, 35 to 49 years, and 50 to 54 years), rural or urban residence, levels of educational attainment (no education, primary, secondary, and higher education), religious groups (Hinduism, Muslim, Christian, and others, including Neo-Buddhist Buddhism), wealth classification index (poorest, poorer, middle, richer, and richest), status of marriage (single, wedded, widowed, or other, including divorced, segregated, or deserted), and employment status (not employed, professional, technical, management, clerical, sales, or service-related; agricultural; skilled/unskilled manuals; or other). In addition, the categories of tobacco usage (no tobacco, smoking, non-smoking, smokes/other tobacco) and alcohol consumption (no alcohol, country’s tadi/madi/alcohol, beers, wines, hard liquor, and others) were considered while analyzing the data.
Outcome Factors
The two dependent variables used to examine alcohol and tobacco consumption were the substances that adults aged 15 to 54 abused most. Smoking and smokeless consumption of tobacco were divided into separate categories. Cigarettes and bidis are examples of tobacco used for smoking, while smokeless tobacco includes items like khaini, a pan that comes with tobacco, gutka pan masala, etc. There is consumption of wines, beer, hard liquor, tadi/madi/country alcohol, and other drinks that are alcoholic.
ST and Non-ST Community
The two groups of the population considered were scheduled tribe (ST) and non-scheduled tribe (non-ST) men. Non-ST men were classified as General (UR), Other Backward Castes (OBC), Scheduled Castes (SC), and others. The purpose of this study was to evaluate the relationship between men’s sociodemographic status and their use of illicit substances by ST and non-ST communities in the Eastern State of West Bengal and the North Eastern States of India for adult men aged 15 to 54 years.
Statistical and Geospatial Techniques
To evaluate the use of alcohol and tobacco intake under the various socioeconomic and sociodemographic variables, descriptive and bivariate statistical analyses were performed, and a Chi2-test was used to find the differences in tobacco and alcohol use between two groups (ST and non-ST men). By statistical significance at a 95% confidence interval for the estimations, the factors used in the logistic regression analysis were carried out to determine the connection between substance use and sociodemographic characteristics. Using NFHS datasets, survey weights were calculated for all statistical analyses of the study outcomes. Statistical analyses were performed using Stata SE version 14.1 (Stata Corp LP). ArcGIS was the tool used for the geospatial mapping, which linked with the spatial database to prepare thematic maps and represent the spatial distribution of tobacco and alcohol use among ST and non-ST men in Eastern state (West Bengal) and North Eastern States of India.
Results
Frequency and Percentage Distribution of ST and Non-ST Male Respondents (15–54 years) by their Sociodemographic Characteristics
The descriptive analysis of the sociodemographic profile among the ST and non-ST male respondents aged 15–54 years is given in Table 1. Most ST respondents were 20–34 years (41.06%), and non-ST men were found highest in 20–34 years (40.38%). In place of residence, it is found that most STs (86.37%) came from rural areas compared to non-STs (69.05%). About 15.17% of the ST sample population had no education, which is higher than the non-ST (13.35%) sample population, while in primary and secondary level ST people found higher than non-ST, but in higher level of education ST (8.53%) found lower than the non-STs (13.32%). Mostly, the ST belonged to Hindu (59.47%) and Christian communities (35.93%), whereas, among non-STs, 75.30% were Hindus, 23.12% were Muslim, and the rest belonged to other religions. According to the wealth index, ST respondents were poorer than the non-STs, which shows that 74.1% of STs are poorer and poorest. In comparison, 59.59% of non-STs were in that category; similarly, in middle wealth, 14.34% of STs and 1.40% of non-STs, and in the rich category, only 11.07% of STs and 18.37% of non-ST represented the rich group in West Bengal and all states from N.E. states of India which were included in our study sample. Regarding marital status, most of the non-ST (67.59%) male respondents were married as ST (64.54%). When the survey was conducted, about 14.75% of ST and 13.22% of non-ST men were not working. Most agricultural occupants were found among STs (40.70%) and 24.92% among non-STs, and the rest of the sample populations were found in other occupations. It is evident from the study results that the majority of the community consumes smoking tobacco, followed by non-smoking and different tobacco. While analyzing the categories of alcohol consumption, it is found that tribal people consume mostly tadi/madi/country liquor (20.21%), followed by hard liquor (11.31%), beer (6.61%), wine (6.41%), and rest others, where in all these categories ST people found more than the non-STs. The third figure (Fig. 3) depicts the spatial distribution of consumption of tobacco and alcohol use among ST and non-ST men (15–54 years) in the North Eastern states and Eastern Indian state of West Bengal, as per NFHS-5.

Portrays the consumption of substance abuse such as tobacco and alcohol consumption among ST and non-ST men (15–54 years) in Eastern state of West Bengal and North Eastern States of India, NFHS-5. Where the district level A tobacco and B alcohol consumption among the ST men (15–54 years) comparison to the C tobacco and D alcohol consumption among the non-ST men (15–54 years) in the WB and NEI were presented side by side
The Chi-square test demonstrated (Table 2) that the associations between ethnic identities and substance use among men were statistically significant (P < 0.05). It was found that the prevalence of tobacco consumption among ST men (39.14%) was greater than that of non-ST men (30.62%), while the prevalence of alcohol consumption among ST women (49.22%) was also higher than that of non-ST men (29.55%). The relationship between these two variables was statistically significant (P < 0.05).
Influence of Sociodemographic Characteristics on the Alcohol and Tobacco Consumption Among ST and Non-ST Male Respondents (15–54 Years)
The occurrence of alcohol and tobacco consumption among males between the ages of 15 and 54 years by ST and non-ST communities by their sociodemographic characteristics bivariate analysis done in Table 3. Tobacco consumption was more common among ST males aged more than 20 years (more than 35%), and among non-ST, it is found that 20 to 34 years of age men (more than 35%). In terms of place of residence, urban residential men consume more tobacco than the rural in both communities. Surprisingly, individuals who were heavily susceptible to tobacco use belonged to STs (44.1%) and non-STs (32.8%) with higher education, and STs (53.1%) and non-STs (34.8%) those in the richest wealth quintile. Among STs, a higher percentage of men of Christians (50.7%), others (50.1%), and Hindus (31.7%) religions consume tobacco as compared to Muslim (9.7%) religious men. In contrast, among non-STs, it is 23.3% of Muslims to 39% of other religions. The results also show that the proportion of married ST men consume a high proportion of tobacco (42.1%). They are mainly engaged in other occupations (57.3%), but among non-STs, those in other categories, such as divorced/separated/deserted by their spouses, found 43.9% of tobacco consumers. They are mostly the non-agricultural occupants (more than 34%). Nearly one-third or more men in each of the selected states (West Bengal and N.E. states of India) consume tobacco, whereas, in all the States, ST men consume more tobacco than the non-STs except Sikkim and Tripura.
Accordingly, in the case of alcohol, the high prevalence of consumption was found among ST men, in the age group of 35–49 years (65%), whereas among non-ST, it was recorded highest (34%) in the age group of 35–49 years. In terms of men’s residence, it is evident from the results that rural STs consume more alcohol (49.7%), while among non-STs, urban residents consume more alcohol. Generally, the fact that alcohol drinking was frequently a habit among men belonged to STs (65.0%) and non-STs (35.2%) with primary education, and STs (51.4%) poorer and non-STs (34.8%), those in the poorest wealth quintile. Furthermore, compared to other social categories, socioeconomically disadvantaged communities had a higher rate of alcohol consumption. From the religious perspective, among STs, a higher proportion of Hindus (57.3%), others (48.3%), and Christians (36.5%) take alcohol more frequently than Muslims (10.8%). In contrast, among non-STs, it is found that 4.9% of Muslims to 57.7% of other religions. It was found that those who were married and other categories such as divorced/separated/deserted by their spouses were more alcohol consumers than the never-married men. In most skilled/unskilled manuals, occupants are the most alcohol consumers (more than 60% among STs and 35% among non-STs). Even though alcohol is illegal in some Indian states, it is evident that alcohol consumption is very prone among the ST communities as of non-STs (except Meghalaya state) in West Bengal and the North Eastern States of India.
The Correlation Between Sociodemographic Characteristics and Substance Use Among Men of ST and Non-ST Groups
According to logistics regression analysis findings, tobacco and alcohol use are substantially correlated with the demographic and socioeconomic backgrounds of ST and non-ST men. The adjusted odds ratios (ORs) for the outcome variables are shown in Table 4, along with a confidence interval of 95% (CI). Middle-aged ST men who are younger exhibit a positive connection with using tobacco products. For instance, men between the ages of 20 and 34 are substantially more likely than men between 50 and 54 (OR: 2.11; 95% CI: 1.65–2.68) to have consumed tobacco. However, it is determined to be significant that non-ST men between the ages of 20 and 34 are more inclined to consume tobacco than non-ST men beyond the age of 35 years. Urban male adults were considerably more likely to use tobacco products (ST men OR: 1.12; 95% CI: 0.92–1.22; non-ST men OR: 0.97; 95% CI: 0.84–1.11) than those who were not. However, men with greater levels of education had a lower likelihood of using tobacco products than men without higher education (ST men OR: 0.92; 95% CI: 0.74–1.11 and non-ST men OR: 0.73; 95% CI: 0.57–0.93). The results found no statistically significant connection between religion and smoking or religion and smokeless tobacco, even though the probability of tobacco intake is lowest among males of other religions ST (OR: 1.28; 95% CI: 1.05–1.56). Compared to Christians and members of other religions, non-ST Muslim men have the lowest odds of smoking (OR: 0.53; 95% CI: 0.44–0.62). Also, the study revealed that ST males from the middle and richer (OR: 0.86; 95% CI: 0.75–0.99 and OR: 0.66; 0.55–0.79, respectively) wealth quintiles have considerably lower tobacco consumption rates than other men in the poorer and richest categories. The least wealthy quintiles among non-STs are shown to be the lowest (OR: 0.87; 95% CI: 0.63–1.16). The likelihood of smoking is significantly higher within ST men than non-ST men for both skilled and non-skilled manual occupations (ST men OR: 2.36; 95% CI: 1.96–2.83 and non-ST men OR: 2.47; 95% CI: 1.99–3.08) but not significantly higher for divorced, separated, and deserted men (ST men OR: 1.29; 95% CI: 0.91–1.83 and non-ST men OR: 1.48; 95% CI: 0.92–2.38).
Age is substantially correlated with ST and non-ST men’s consumption of alcohol, according to an analysis of the relationship between sociodemographic variables and male alcohol consumption behavior (Table 5). Both ST (OR: 3.79; 95% CI: 3.12–4.61) and non-ST men (OR: 2.64; 95% CI: 2.04–3.44) aged 20 to 34 years found significant and higher alcohol consumption. Male individuals who lived in rural regions had significantly greater odds among ST (OR: 1.19; 95% CI: 1.03–1.38) compared to those who lived in urban areas, and non-significantly different odds of non-ST (OR: 1.00; 95% CI: 0.86–1.16). ST males with only a primary education status had more propensity to drink alcohol (OR: 1.10; 95% CI: 0.92–1.32). However, compared with ST men, non-ST men with any form of education had lower probabilities of consumption than the rest, which may indicate a negative relationship between education and the consumption of alcohol. Similarly, men from other religious groups are more prone to consume substances like alcohol (OR: 1.02; 95% CI: 0.84–1.25), and non-ST men from Christian (OR: 1.40; 95% CI: 1.02–1.94) and other religious groups are significantly more likely to consumes alcohol (OR: 1.40; 95% CI: 1.05–1.85) than men compared to Hindu and Muslim religions. Men in the lowest wealth quintile have the highest odds of STs (OR: 1.02; 95% CI: 0.90–1.15), but non-STs have lower odds of alcohol use across all wealth quantiles. The males in both communities (ST and non-ST) who are divorced, distinguished from their spouses, or have been abandoned by them (ST males OR: 2.28; 95% CI: 1.61–3.22 and for non-ST men OR: 2.64; 1.60–4.35) are noticeably more likely to engage in alcohol use compared with men who are married, younger, or single. Furthermore, males working in manual labor, both trained and untrained (ST men OR: 2.80; 95% CI: 2.31–3.40 and for non-ST men OR: 3.62; 2.82–4.64), are much more likely to drink alcohol than men in other occupations, which is significant for both the ST and non-ST men’s.
After studying the sociodemographic factors, it was determined that Mizoram had the highest odds of ST men using tobacco products, followed by Meghalaya, Manipur, Nagaland, and Arunachal Pradesh. Mizoram also had the highest odds of non-ST men using tobacco products and was significantly higher than Manipur and Arunachal Pradesh. Comparably, Assam, Arunachal Pradesh, and Manipur had the highest probability of ST males drinking alcohol. In contrast, Manipur, Arunachal Pradesh, and Mizoram had the highest chances of non-ST men drinking alcohol.
Discussion
Globally, there are disparities in substance use and well-being status between tribal and non-indigenous communities, where scheduled tribes in India are also exposed to more possibilities of using tobacco products and drinking alcohol when compared to national averages (Debbarma, 2019). From this perspective, the current article attempts to determine and measure the role that sociodemographic determinants factors on the level of prevalence of illicit substance use in the form of tobacco and alcohol among males from scheduled tribes and non-scheduled tribes groups in India’s Eastern states like West Bengal and the other 8 North Eastern states. It is vital to understand the severity and discrepancy of substance abuse behaviors among different socioeconomic groups in the NEI states, which differ from that in the rest of the country due to history, culture, and ethnic diversification, as well as diverse geographical landscape (Saikia & Debbarma, 2020).
The findings of our study showed that alcohol consumption among men in the North Eastern States of India and the eastern states like West Bengal was 49.23% among ST and 29.56% among non-ST, while smoke exposure was 39.14% among ST and 30.62% among non-ST, aged 15 to 54. It was found that substance usage was more common among ST and non-ST men, those who are above 20 years old, and those who are lower and not educated, which is possibly a result of lower consciousness and understanding of tobacco’ adverse effects and related difficulties (Pradhan et al., 2019). In terms of place of residence, urban residential men consume more substances than the rural in both communities. Among ST and non-ST men of other religions such as Buddhist, Hindu, and Christian belonging to the poorer to richest ST and middle to richest wealth quintile among non-ST men, also those who are married and others like divorced, separated, deserted, or widowed, men from the clerical/sales/services, skilled/unskilled manuals, and other workers consume more substance in the both communities. This was also found in the study by Anand and Roy (2022) that middle age ranges, low levels of education, and employment in the unorganized sector were the most crucial risk factors associated with the typical consumption of such substances among men.
The results are emphasized by logistics regression analysis, which demonstrates that ST men in the middle age group (35–39 years old) and non-ST men in the 20–29 years old consume more tobacco and that men working in manual labor, both trained and untrained, in both the ST and non-ST groups are significantly more likely to smoke. While it was determined that ST men in the age range of 30–34 years and non-ST men in the age range of 25–29 years consumed more alcohol, those in other religious categories among non-ST, poor wealth quantiles in both communities, as well as those in other categories, such as divorced, segregated, deserted, or widowed men who are working in trained and untrained manual labor in both communities, were also found to be significantly more likely to use alcohol substances than their opponents in the respective categories. The analysis presented in the article verifies prior studies of research that focused on the sociodemographic factors that influence the consumption of substances (Neufeld et al., 2005; Subramanian et al., 2006).
The results of this study ensure the findings from earlier research that addressed the socioeconomic factors that influence substance use in Eastern states like West Bengal and the North Eastern States of India (Balasubramani et al., 2021). Similar findings were made in the last round of the NFHS survey, which showed that men from NEI states had much higher substance use rates than men from other Indian states and UTs, where the use of alcohol is most prevalent, followed by smoking and tobacco products that are smokeless (Saikia & Debbarma, 2020). Additionally, the district-wise distributions and, subsequently, hot spot analysis of the study by Balasubramani et al. (2021) demonstrate that the NE area constitutes the first hot spot regarding alcohol consumption. The access to comparatively inexpensive tobacco and alcohol in the region that is smuggled through the neighborhood countries of Bangladesh and Myanmar through their insecure international borders might be a significant factor in the prevalence of using substances in the Eastern and NE regions of India (Singh, 2007). The tribal population frequently consumes both tobacco and alcohol. And this phenomenon might have been carried on by their traditional beliefs and the societal acceptance of alcohol. They usually drink alcohol, primarily locally sourced rice brew, drunk by their community members and prepared in their homes. Apart from alcohol, tobacco is the most widely available and inexpensive substance, often shared among close companions and other people, and is used as a stimulant through smoking or chewing (Chaturvedi et al., 2003, 2016).
Suggestive Measures
According to the study’s findings, the following suggestions are made:
-
(a)
The sociodemographic factors that directly and indirectly contribute to wilful substance abuse must be addressed.
-
(b)
Interventions that need to focus on community-based strategies to reduce substance usage.
-
(c)
Parents should not be hesitant to speak freely with their children by encouraging them to grasp the laws and expectations by imparting clear messages regarding substance misuse.
-
(d)
The government, in particular, the legislators who authorize these consumptions, should recognize that it is necessary to decrease these substance users by providing addiction treatment/counseling facilities and imposing considerable taxes on substance-related things.
-
(e)
Adopting straight measures to strengthen society’s cognition through various awareness operations, which must incorporate the development of educational curricula and initiatives to combat substance consumption irrespective of different religions and communities.
-
(f)
There is a need for stronger awareness of the potential health dangers associated with substance use among various disadvantaged communities and the harmful practices’ detrimental consequences on their well-being and quality of life.
-
(g)
The priority should be placed on the specific regions with higher substance usage rates by the government’s national plan and nonprofit organizations operating under specialized administration and persuasive interventions.
Strengths and Limitations of the Study
The strength of this study is that it is a comparative study that examines the prevalence of substance use among ST and non-ST populations in the Eastern state of West Bengal and eight North Eastern Indian states. This is the study’s significant aspect. The study’s main limitation is that the data are cross-sectional. Furthermore, it was limited to a geographical area at the district and state levels, and in this study, only some of the socioeconomic and demographic criteria were considered.
Conclusion
This study examined the prevalence, nature, and socio-demographic determinants of alcohol and tobacco consumption among men (15–54 years old), ST, and non-ST in the Eastern state (West Bengal) and the North Eastern States of India. The sociodemographic factors of ST and non-ST people, such as their age group, place of residence, education, religion, marital status, level of wealth, occupation, and degree of spatial deprivation, are important social predictors of substance use. According to the national consumption rates in India, substance use is more common among ST men in West Bengal and NEI. Addressing the most vulnerable socioeconomic groups is a prerequisite; substance misuse is a large issue in these regions and is one of the leading causes of multimorbidity and health concerns. However, it requires to be implemented a program that will be appropriately maintained at the community level in the specific geographical region to reduce substance misuse. The consumption of both alcohol and tobacco products needs to be discouraged by health consciousness; instruction, advertising messages, and other measures will be required. Significant taxes will also be imposed on substance items to reduce substance misuse among vulnerable people in Eastern states like West Bengal and the North Eastern States of India.
Notes
Terminologies regarding various forms of substance usage are as follows: Khaini is made with roasted tobacco flakes and slaked lime, whereas Gutka is a prepared smokeless tobacco product (MSTP), a blend of areca nut, tobacco, and certain condiments sold in colorful pouches in various flavors, while Pan masala is a betel quid concoction that may or may not consist of tobacco, areca nut, and other additives, and Bidi is a low-cost smoking stick created by rolling a dried, rectangle piece of temburni leaf (Diospyros melanaxylon) with 0.15–0.25 g of dried in the sunlight, flaked tobacco into a conical form and securing the roll with a thread (Gaidhane et al., 2011)
Availability of Data and Material
The datasets and materials used are accessible on the DHS website at https://dhsprogram.com/data/.
Abbreviations
- NEI:
-
North Eastern States of India
- ST:
-
Scheduled Tribe
- NFHS:
-
National Family Health Survey
- WB:
-
West Bengal
References
Acharyya, A., & Ghosh, K. (2022). NCD risk factors in different administrative divisions of West Bengal: An insight analysis from National Family Health Survey-5 Report. Journal of the Indian Medical Association, 120(5), 26–32.
Anand, A., & Roy, N. (2022, April 13). Prevalence and determinants of co-use of alcohol and tobacco among men in working age group (18–59 years) in India. Epidemiology, Biostatistics, and Public Health, 13(1). https://doi.org/10.2427/11642
Balasubramani, K., Paulson, W., Chellappan, S., Ramachandran, R., Behera, S. K., & Balabaskaran Nina, P. (2021, August 27). Epidemiology, hot spots, and sociodemographic risk factors of alcohol consumption in Indian men and women: Analysis of national family health survey-4 (2015–16), a nationally representative cross-sectional study. Frontiers in Public Health, 9. https://doi.org/10.3389/fpubh.2021.617311
Bhawna, G. (2013, May 30). Burden of smoked and smokeless tobacco consumption in India - Results from the global adult tobacco survey india (GATS-India)- 2009–2010. Asian Pacific Journal of Cancer Prevention, 14(5), 3323–3329. https://doi.org/10.7314/apjcp.2013.14.5.3323
Chaturvedi, H. K., Bajpai, R. C., & Pandey, A. (2016). Predictors of substance use in the tribal population of northeast India: Retrospective analysis of a cross-sectional survey. Journal of Addiction Research & Therapy, 7(5). https://doi.org/10.4172/2155-6105.1000295
Chaturvedi, H. K., Phukan, R. K., & Mahanta, J. (2003, January 1). The association of selected sociodemographic factors and differences in patterns of substance use: A pilot study in selected areas of northeast India. Substance Use & Misuse, 38(9), 1305–1322. https://doi.org/10.1081/ja-120018488
Debbarma. (2019, June). Behavioural health risks associated with substance use: Tobacco and alcohol consumption among ethnic population in Tripura. Journal of North East India Studies, 9(1), 64–82. Retrieved August 7, 2023, from https://www.jneis.com/9-1-4/
Fu, S. H., Jha, P., Gupta, P. C., Kumar, R., Dikshit, R., & Sinha, D. (2014, July 15). Geospatial analysis on the distributions of tobacco smoking and alcohol drinking in India. PLoS ONE, 9(7), e102416. https://doi.org/10.1371/journal.pone.0102416
Gaidhane, A., Nazli, K., Zahiruddin, Q., Bawankule, S., & Zodpey, S. (2011). Prevalence and pattern of tobacco use among tribal adolescents: Are tobacco prevention messages reaching the tribal people in India? Annals of Tropical Medicine and Public Health, 4(2), 74. https://doi.org/10.4103/1755-6783.85756
Haobijam, S., & Singh, K. A. (2021, March 27). Socioeconomic determinants of domestic violence in northeast India: Evidence from the National Family Health Survey (NFHS-4). Journal of Interpersonal Violence, 37(15–16), NP13162–NP13181. https://doi.org/10.1177/08862605211005133
Indigenous Peoples at the United Nations | United Nations for Indigenous Peoples. (n.d.). Retrieved October 19, 2023, from https://www.un.org/development/desa/indigenouspeoples/about-us.html
International Institute for Population Sciences and MoHFW. (2021). National Family Health Survey (NFHS-5). Retrieved August 5, 2023, from http://rchiips.org/nfhs/factsheet_NFHS-5.shtml
Kalita, K. (2022, June 9). Northeast has highest prevalence of alcohol and tobacco consumption in India: Survey. The Times of India. Retrieved August 5, 2023, from https://timesofindia.indiatimes.com/city/guwahati/ne-has-highest-prevalence-of-alcohol-and-tobacco-consumption-in-country-survey/articleshow/92092054.cms
Kumari, N., & Salve, P. S. (2020, May 18). Substance use and non-communicable diseases in India: Evidence from national family health survey-4. Journal of Substance Use, 26(1), 30–35. https://doi.org/10.1080/14659891.2020.1766126
Lhungdim, Sahoo, & Ladusingh. (2021, July). Population growth, ethnic diversity, socio-economic status, and healthcare utilization in North East India: With special reference to the recognized tribes (IIPS working paper series no. 21). International institute for population sciences. Retrieved October 19, 2023, from https://www.iipsindia.ac.in/sites/default/files/IIPS_Working_Paper_Series_No_21_0.pdf
Ministry of Development of North Eastern Region, North East India. (n.d.). Retrieved October 19, 2023, from https://mdoner.gov.in/
Neufeld, K., Peters, D., Rani, M., Bonu, S., & Brooner, R. (2005, March). Regular use of alcohol and tobacco in India and its association with age, gender, and poverty. Drug and Alcohol Dependence, 77(3), 283–291. https://doi.org/10.1016/j.drugalcdep.2004.08.022
Pradhan, M. R., Patel, S. K., & Prusty, R. K. (2019, October 1). Pattern and predictors of tobacco use in India: Evidence from national family health survey (2015–2016). Journal of Health Management, 21(4), 510–524. https://doi.org/10.1177/0972063419868566
Rao, V., Bhat, J., Yadav, R., Muniyandi, M., Bhondeley, M., & Wares, D. (2017, January). Smoking and alcohol consumption: Risk factors for pulmonary tuberculosis among the tribal community in central India. Indian Journal of Tuberculosis, 64(1), 40–43. https://doi.org/10.1016/j.ijtb.2016.11.009
Ruhil, R. (2019, April). Sociodemographic determinants of tobacco use in India: Risks of risk factor—An analysis of global adult tobacco survey india 2016–2017. SAGE Open, 9(2), 215824401984244. https://doi.org/10.1177/2158244019842447
Sadath, A., Jose, K., Jiji, K., Mercy, V., Ragesh, G., & Arensman, E. (2021, January 25). Prevalence and determinants of substance use among indigenous tribes in South India: Findings from a tribal household survey. Journal of Racial and Ethnic Health Disparities, 9(1), 356–366. https://doi.org/10.1007/s40615-021-00964-2
Saikia, N., & Debbarma, B. (2020, March). The socioeconomic correlates of substance use among male adults in Northeast India. Clinical Epidemiology and Global Health, 8(1), 149–157. https://doi.org/10.1016/j.cegh.2019.06.004
Singh, T. B. (2007, December). India’s border trade with its neighbouring countries with special reference to Myanmar. Margin, 1(4), 359–382. https://doi.org/10.1177/097380100700100402
Singh, S. K., Kumar, S., & Kashyap, G. C. (2023). March 22). Tobacco use and cessation among a nationally representative sample of men in India, 2019–2021. Journal of Smoking Cessation, 2023, 1–15. https://doi.org/10.1155/2023/4292647
Subramanian, S. V., Smith, G. D., & Subramanyam, M. (2006, October 24). Indigenous health and socioeconomic status in India. PLoS Medicine, 3(10), e421. https://doi.org/10.1371/journal.pmed.0030421
Substance Abuse | WHO. (2023, August 3). WHO | Regional office for Africa.
Tikhute, V. (2023, October 17). Geospatial patterns of alcohol and tobacco use in India: A cluster analysis of NFHS 4. https://doi.org/10.33774/coe-2023-0wf8j
Tobacco, N. (2023, July 31). WHO report on the global tobacco epidemic, 2023: Protect people from tobacco smoke. Retrieved August 2, 2023, from https://www.who.int/publications/i/item/9789240077164
West Bengal Tribal Development Department. (n.d.). Scheduled tribes of West Bengal. Retrieved October 19, 2023, from https://adibasikalyan.gov.in/scheduled-tribes-of-west-bengal
WHO Factsheets. (2022, May 9). Alcohol. Retrieved August 3, 2023, from https://www.who.int/news-room/fact-sheets/detail/alcohol
Acknowledgements
The DHS program of the International Institute for Population Sciences (IIPS) India has been acknowledged by the authors for collecting data on alcohol and tobacco usage among men. The Indian Council of Social Science Research (ICSSR) for providing funding and the University of North Bengal’s Department of Geography and Applied Geography are also acknowledged by the authors for giving research settings, respectively.
Funding
This research work has been carried out with financial support from the Indian Council of Social Science Research (ICSSR) Funded Research Project (Major) entitled “Understanding Quality of Life (QoL) of the Tribes in the Hilly Region of Darjeeling and Kalimpong District, West Bengal: A Future Road Maps for the Sustainable Development” (F.No.Gen.-32/2021-22/ICSSR/RP, Dated: 22-03-2022), and the Scholar, namely “Dr. Indrajit Roy Chowdhury, Assistant Professor, Department of Geography & Applied Geography, University of North Bengal, West Bengal, India,” is the awardee of ICSSR Major Research Project.
Author information
Authors and Affiliations
Contributions
Manabindra Barman1: visualization, validation, conceptualization, data curation, formal analysis, methodology, software, created tables, figures, writing-original draft, writing-reviewing, editing. Dr. Indrajit Roy Chowdhury2: supervision, reviewing, funding acquisition, project administration.
Corresponding author
Ethics declarations
Ethical Approval
The study used a secondary dataset from the Demographic Health Survey of India’s National Family Health Survey (NFHS), which contains no information that may be used to identify the survey participants personally. NFHS used the usual questionnaire to get consent before and throughout the investigation. The datasets are available on the DHS site; however, access is only permitted after registering and submitting the required research interest.
Consent for Publication
Not applicable.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Barman, M., Chowdhury, I.R. Substance Uses and Associated Sociodemographic Factors Among Male Tribes and Non-Tribal Communities of Eastern and North Eastern States in India: An Evidence-Based Study from the National Family Health Survey-5. Glob Soc Welf 11, 257–270 (2024). https://doi.org/10.1007/s40609-023-00328-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40609-023-00328-0