
Abstract
Objective
Despite the increasing number of people with autism-spectrum disorder (ASD), intellectual disabilities (ID), and developmental disabilities (DDs), individuals with these conditions continue to have high levels of unmet physical and mental health needs. Robust training of health professionals can help bridge this gap. A systematic review was conducted to describe the features and educational outcomes of existing postgraduate medical education curricula to inform the development of future training to address the growing unmet care needs of people with intellectual and developmental disabilities (IDD) such as ASD and ID.
Methods
Four major databases were searched for peer-reviewed, English-language research focusing on post-graduate training in IDD education. Educational curricula and outcomes were summarized including Best Evidence in Medical Education (BEME) Quality of Evidence and Kirkpatrick training evaluation model.
Results
Sixteen studies were identified with a majority published after 2000 (69%). Pediatric departments were involved in 69%, Psychiatry 19%, Medicine-Pediatrics 19%, and Family Medicine 6.3%. Analysis of Kirkpatrick outcomes showed 31% were level 1 (satisfaction or comfort); 38% level 2 (change in objective knowledge or skills); 13% level 3 (change in behavior); and none at level 4. BEME analysis showed 19% of studies were grade 1 (no clear conclusions), 31% grade 2 (ambiguous results), and half (50%) grade 3 (conclusions can probably be based on findings), with none scoring four or higher.
Conclusions
There is a paucity of objectively evaluated research in the area. Studies reviewed show clear promise for specialized, interdisciplinary, competency-based education which may be foundational for future curriculum development.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
People with autism-spectrum disorder (ASD), intellectual disability (ID), and other developmental disabilities (DDs) represent a heterogenous group of diverse individuals that share unique challenges in their health. People with DDs encompass approximately 6.99–15.04% [1,2,3], ID 0.71–3% [1, 2, 4, 5], and those with ASD 0.47–2.76% [1, 2, 6,7,8,9,10,11,12] of the general population, all of which have been rising in prevalence in recent years [1, 2, 6, 8, 11]. These three groups are often described together as intellectual and developmental disabilities (IDD), and henceforth, the term IDD will be used to describe these three groups together [13]. Potential contributing reasons for this rise in prevalence include increased societal awareness, improvements in longevity, liberal changes in diagnostic classifications among other reasons [1, 3, 6, 8, 11]. These populations have been found to be at significantly inflated risk of increased contact [3, 14] with the healthcare system, medical-related financial burden [14, 15], and adverse functional and health outcomes [3, 14, 16, 17] including premature death [18, 19]. Several reports in the last couple of decades, including two Surgeon General reports and Future of Disability in America report, highlight the key challenges in people with intellectual and developmental disabilities such as poorly managed health outcomes, shorter lifespan, and less access to professional health care as compared to people without this condition [20]. Training of health care professionals can help meet health care needs of this population and reduce the wide societal disparities [20]. Unfortunately, the need for high-quality healthcare for this large group of people is largely unmet [21,22,23], and physicians’ confidence and perceived competence in providing this specialized care appears to be low [24,25,26,27,28].
To bridge this gap, we must look to how we are training our physicians to address the care needs of this patient population. Given the complexity of care and multimorbidity of IDD, care of this patient population does not fit neatly into the purview of one medical specialty. Rather, multiple medical specialties are well-placed to play critical roles in treating this population including family medicine, pediatrics, and psychiatry in the community, and increasingly in emergency departments [29], which is suggested to be preventable with increased specialized service availability [30, 31].
Surveys of family medicine residencies in the USA indicate that between 32 and 60% of programs provided any instruction and 24–84% provided the opportunity for any clinical experience with intellectual disability populations [32, 33]. Casson et al. (2019) described a program designed to increase the competency of family medicine residents in caring for adults with IDD. The program uses “health check” (clinical encounter) as a learning resource and proposes “field notes” as a template for formative feedback to residents [34]. Moreover, pediatric residents reported low self-assessed competence in treating patients with ASD [35], and despite an Accreditation Council for Graduate Medical Education (ACGME)–mandated USA-wide 1-month mandatory rotation in developmental/behavioral pediatrics in 1997, graduating residents continue to report feeling inadequately prepared to manage patients with IDD [36]. Interprofessional teams are an important aspect of healthcare teams working with people with IDD. Physicians, nurses, psychologists, behavior therapists, occupational therapists and social workers, among other professionals, work as a team in caring for people with developmental disabilities, especially those presenting with clinical complexities. The need for team-based education notwithstanding, gaps in training and interprofessional practice needs have been reported [37]. Moreover, little is known about IDD training opportunities for residents within an interprofessional framework.
In addition to pediatrics training, a Canadian survey [38] of IDD across psychiatry residency training programs found that just 31% of programs provided more than 6 h of teaching, less than half had mandatory rotations, and 56% offered elective rotations. In child and adolescent psychiatry fellowship programs, while the ACGME has made a policy change towards mandating clinical experience with IDD [39], survey data after this change indicated that learners received 7 h per year in instruction on IDD, and most commonly saw 1–5 of such cases per year in outpatient and inpatient settings [40]. Nearly half of programs surveyed endorsed a need for additional resources, including availability of specialized clinics or physicians to provide training in IDD [40]. This is in contrast to the psychiatric training of DDs in the UK, which has its own DD higher specialist training program [41]. While we can glean some limited cross-sectional data regarding training programs’ inclusion of IDD into their curricula, publications examining education intervention outcomes are lacking.
Given the dearth of literature on training programs for this patient population, we aimed to conduct a systematic review to describe the features of current IDD training programs and to assess their educational outcomes. The goal of this review is that the synthesis of the literature will help guide the way forward for residency programs to develop evidence-based curricula in IDD with which to train physicians capable of addressing the growing and yet unmet need of this population.
Methods
We employed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement, checklist, and supporting documents [42] as well as the Best Evidence Medical Education Guide (BEME) systematic review guide [43] to assist in conducting this review.
Search Strategy
The literature search was conducted on December 17, 2018, with the assistance of University of Toronto librarians in locating full-length copies of identified publications. Ovid search web software was employed to search the Medline, Embase, and PsycINFO databases using subject keyword ‘or’ combinations of ‘ASD’, ‘autis*’, ‘learning disab*’, ‘intellectual disab*’, ‘developmental disab*’, ‘mental retard*’, and ‘asperger*’ with ‘or’ combinations of ‘post-graduat*’, ‘residency’, and ‘internship’. The search was limited to English-language, peer-reviewed articles published from 1980 to current, with the start date as 1980 in concordance with the first formal recognition of the diagnosis of autism-spectrum illness with the publication of the DSM 3 in this year. Following the initial database search, identified articles’ references were perused for further applicable publications. The literature search was then updated to expand on dates from December 17, 2018, to August 20, 2020, utilizing the identical parameters.
Inclusion and Exclusion Criteria
Studies were included if they focused on an educational intervention for post-graduate medical trainees of any specialty intended to ameliorate knowledge, skills, competence, or attitudes regarding IDD evidenced by formally evaluated outcomes. Those studies which primarily focused on other participants such as psychology interns or nurses were not included in this review as the focus was on medical training. No sample size cut-off was employed, due to the anticipated relative paucity of work in this research area.
Excluded studies included those that described an intervention but did not formally evaluate it and those that evaluated trainees’ knowledge, skills, competencies, or attitudes but did not describe an IDD educational program associated with it.
Title and Abstract Review
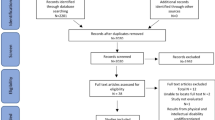
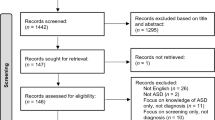
The initial database search identified 332 publications, in which, after removing duplicates, reviewing abstracts yielded 66 articles. Following imposition of the inclusion/exclusion criteria, and searching reference lists of included articles for additional relevant papers, 16 core papers [36, 44,45,46,47,48,49,50,51,52,53,54,55,56,57,58] were included in the final analysis of this review (Fig. 1) [59]. The updated search yielded a further 65 articles, which, following imposition of inclusion/exclusion criteria, did not yield any additional core papers.

PRISMA flow diagram
Full-Text Review, Data Extraction, Synthesis, and Analysis
Two authors (Z.A., A.T.) independently analyzed the core papers, and classified data from the 16 publications into a Microsoft Excel (Microsoft, Redmond, Washington) spreadsheet with particular focus on areas of interest which included the following: (i) author names; (ii) year of publication; (iii) country of origin; (iv) postgraduate training specialty; (v) learner level of participants in intervention; (vi) instructors; (vii) setting of instruction; (viii) timeline; (ix) pedagogical method; (x) focus of content; (xi) evaluation methodology; (xii) evaluation outcomes; (xiii) Kirkpatrick effectiveness of intervention score [60]; (xiv) BEME quality of evidence score [43]. Number and percentages for each category are summarized in Table 1.
We organized the instructor data into the following categories: (1) faculty members or staff physicians; (2) other specialized non-physician instructors; and/or (3) patients, parents, or caregivers. We classified the setting as one of the following: (a) specialized clinical setting; (b) non-specialized clinical setting and sub-stratified into (i) inpatient; (ii) outpatient; and (i) continuity-clinic based; (ii) non-clinical respectively. Curricula timelines were subtyped into (i) single-session; (ii) short-term less than 1 month; (iii) 1–3 months; and (iv) longitudinal of longer than 3 months. The pedagogical (instructional) methods are described in Table 1. Focus of content was transcribed as follows: (i) perspective/awareness; (ii) medical and clinical knowledge; (iii) other or unclear.
Evaluation methodology was organized as follows: (i) intervention evaluation (participant evaluation of the experience of the intervention); (ii) participant evaluation (participant of intervention assessing their benefit from the intervention); (iii) learning assessment (assessment of perspective/knowledge/skills gained during intervention); (iv) clinical change (monitoring of clinical practice after intervention). The evaluation outcomes were summarized uniquely for each paper, and Kirkpatrick [60] and BEME [43] classification was applied to each publication. Kirkpatrick classification is widely used in evaluation of training programs in medical education [61,62,63,64,65,66]. This model assesses the effectiveness of programs at various levels: trainee’s experience of the program is evaluated at the first level; changes in knowledge, skills, and attitude are assessed at the next level; transfer of knowledge to practice at a third level and at level 4, the overall impact of the program on broader organizational goals and objectives is evaluated. The model was adapted for this paper to (0) no change in learning or explored learner views on the quality of the learning experience itself; (1) alteration in learner perspective or comfort on the topic being learned; (2) amelioration of learning or skills; (3) changes in behavior or practice from the learning; and (4) difference in tractable results or outcomes due to the behavioral change. The BEME level of evidence grading [43] was employed to assess the strength of paper findings according to grades: (1) no clear conclusions can be deduced; (2) ambiguous results, although appearance of a trend; (3) conclusions can probably be based on the findings; (4) results are clear and highly likely to be true; (5) unequivocal results.
Results
The results can be seen in coalesced form in Table 2.
Study Characteristics
Table 1 summarizes study characteristics for the 16 included publications. Twenty-five percent (4/16) were published in the 1980s [44, 46, 57, 58], 6% (1/16) in the 1990s [52], 38% (6/16) in the 2000s [36, 45, 50, 53,54,55], and 31% (5/16) in the 2010s [47,48,49, 51, 56]. All studies included were undertaken in North America, with 88% (14/16) conducted in the USA of America [36, 44,45,46, 48, 49, 51,52,53,54,55,56,57,58], and 13% (2/16) in Canada [47, 50]. Pediatric departments were involved in 75% (12/16) of the studies [36, 44,45,46, 48, 49, 51, 52, 56,57,58], Psychiatry 19% (3/16) [53,54,55], Medicine-Pediatrics 19% (3/16) [48, 49, 51], Family Medicine 6% (1/16) [50], Child and Adolescent Psychiatry 6% (1/16) [55], and Developmental and Behavioral Pediatrics 6% (1/16) [47]. Further in this paper, for simplicity, when pediatrics or psychiatry are mentioned they are in reference to pediatrics or psychiatry and subspecialty variants. The most commonly employed instructors were faculty members or staff physicians (63%; 10/16) [36, 44, 46, 47, 50, 51, 53,54,55,56], with other specialized non-physician instructors (25%; 4/16) [45, 47, 54, 58], and patients, parents, or caregivers (13%; 2/16) [48, 49] playing roles in two interventions each. In two studies [52, 57], it was not entirely clear on who provided the instruction.
With respect to learner level, the majority of the studies (88%; 14/16) [36, 44,45,46,47,48,49,50,51,52, 54,55,56, 58] offered their educational curricula to residents at multiple levels of training. PGY1s were included in 56% (9/16) of studies [36, 44,45,46, 50,51,52, 56, 58], PGY2s in 81% (13/16) [36, 44, 46, 48,49,50,51,52,53, 55,56,57,58], PGY3s in 75% (12/16) [36, 44,45,46, 48, 49, 51, 52, 54,55,56, 58], PGY4 residents just once [54] (6%; 1/16), and subspecialty residents/fellows in 13% (2/16) [47, 55]. Medical students were included in one study (6%; 1/16) [51], as well as clinical psychology interns (6%; 1/16) [47]. When separated by specialty, we see that Pediatrics interventions were quite evenly split between PGY1 (67%; 8/12) [36, 44,45,46, 51, 52, 56, 58], PGY2 (83.3%; 10/12) [36, 44, 46, 48, 49, 51, 52, 56,57,58], and PGY3 (67%; 8/12) [36, 44,45,46, 51, 52, 56, 58], with one study involving subspecialty Pediatric residents/fellows (8.3%;1/12) [47]. Psychiatry educational programs did not include any PGY1s, with PGY2s involved in 67% (2/3) of studies [53, 55], PGY3s included in the same number (67%; 2/3) [54, 55], one including PGY4s (33.3%; 1/3) [54], and one including subspecialty fellows (33.3% 1/3) [55]. Medicine-Pediatrics interventions focused on PGY3s (67%; 2/3), while one study did not clarify the component of Medicine-Pediatrics residents [51].
Curriculum Characteristics and Pedagogical Approach
More than half (56%; 9/16) of studies were based upon a specialized ASD/ID/DD training experience embedded with the clinical rotation [36, 44, 46, 48, 49, 53,54,55, 57]. Notably, all of the Psychiatry curricula (100%; 3/3) [53,54,55] were based in this model, with one inpatient-based (33%; 1/3) [53] and two outpatient-based (67%; 2/3) [54, 55], while half (58%; 6/12) of Pediatrics interventions were centered on specialized clinical experience [36, 44, 46, 48, 49, 57], of which one (17%; 1/6) was explicitly inpatient-based [57], with the other five being (83%; 5/6) outpatient-based or not clearly identifying [36, 44, 46, 48, 49]; however, one study although not directly evaluating a specialized IDD clinical rotation did mention that all resident participants also would have this rotation during their training [58].
Less than half (44%; 7/16) of studies were not based on specialized IDD clinical experiences [45, 47, 50,51,52, 56, 58]. These included half (50%; 6/12) of the pediatric interventions [45, 47, 51, 52, 56, 58], and the only family medicine program (100%; 1/1) [50]. Of these pediatric interventions, half (50%; 3/6) were based at ambulatory/longitudinal clinics [52, 56, 58], with the other half (50%; 3/5) without a clinical component [45, 47, 51] and the only family medicine program was non-clinical (100%; 1/1) [50].
The majority of the educational intervention timelines were 1–3 months in duration (59%; 9.5/16 [one study was 1–3 months for residents but longitudinal for fellows] [55]) [36, 44, 46, 48, 49, 53, 54, 57, 58]. Two interventions and a segment of another (16%; 2.5/16 [one study was longitudinal for fellows, but 1–3 months for residents] [55]) [45, 56] extended beyond 3 months, three were single-session interventions (19%; 3/16) [50,51,52], and a single intervention was multiple sessions occurring over less than 1 month (6%; 1/16) [47].
The vast majority of studies included a theoretical pedagogical framework (88%; 14/16) [44,45,46, 48,49,50,51,52, 54,55,56,57,58], most commonly didactic or seminar (86%; 12/14) [44,45,46, 48,49,50, 52, 54,55,56,57,58], and less often reading lists (57%%; 8/14) [44, 46, 51,52,53,54, 57, 58]. Experiential pedagogical principles of learning were frequently employed (75%; 11/16) [36, 44, 46,47,48,49, 53,54,55,56,57], most commonly clinical practice (91%; 10/11) [36, 44, 46, 48, 49, 53,54,55,56,57], although there was one simulation-based program (9%; 1/11) [47]. Immersive experiences were employed by nearly half of studies (44%; 7/16) [44, 46, 48, 49, 54, 57, 58], while a smaller number of studies included interactive (31%; 5/16) [44, 46, 47, 50, 51] approaches.
Of the educational interventions based at specialized IDD clinical rotation, most were supplemented by theoretical pedagogy (89%; 8/9) [44, 46, 48, 49, 53,54,55, 57] followed by immersive methodology (67%; 6/9) [44, 46, 48, 49, 54, 57]. Studies where learning was based at continuity clinics were always supplemented with theoretical teaching cases (100%; 3/3) [52, 56, 58], in one case additionally with immersive methods (33%; 1/3) [58], and in one case with an unclassifiable tool of clinical reminders in charts [52]. In terms of the non-clinical interventions, we see that most incorporated theoretical (75%; 3/4) [45, 50, 51] and interactive components (75%; 3/4) [47, 50, 51], and just one emphasized experiential learning in the form of simulation (25%; 1/4) [47].
The experiential learning ranged from classical rotation-based service-oriented experiences, a telepsychiatry clinic, observation of physicians’ work, to simulation-based models. Theoretical teaching included didactic lecture and seminar series, annotated notes provided to learners, and assigned readings. Interactive learning included discussions with and without facilitators, case-based modules, and journal rounds discussions. Immersive learning ranged from home visits, school visits, to placements with specialized allied-health staff in multi-disciplinary IDD support facilities.
The vast majority of studies (81%; 13/16) [44,45,46,47, 50,51,52,53,54,55,56,57,58] explicitly focused their interventions on medical and clinical knowledge, while 38% (6/16) [44,45,46, 48, 49, 58] mentioned an intent on broadening learners’ perspectives and awareness of the conditions and their contexts, two of which only focused on this aspect (13%; 2/16) [48, 49]. One study did not have a clear content description [36].
Educational Outcomes
Studies used a range of measures to assess educational outcomes. In just over half of the educational interventions, direct assessments of knowledge (56%; 9/16) [44,45,46, 50,51,52, 55,56,57] or learner’s evaluations of their own learning (56%; 9/16) [36, 44, 46, 48, 51, 53, 54, 56, 58] were employed. In fewer studies, learner and instructor evaluations of the intervention itself (18.8%; 3/16) [49, 51, 53, 54] were looked at, two studies looked at clinical changes associated with the intervention (13%; 2/16) [45, 52], and one study looked at qualitative observed behavioral change [47].
A variety of outcomes were found upon application of the Kirkpatrick model for evaluating education program outcomes. Nineteen percent (3/16) [36, 49, 52] were graded level 0 due to lack of change demonstrated or only assessment of satisfaction levels, 31% (5/16) [48, 53, 54, 56, 58] were level 1 indicating an alteration in perspective or comfort following the intervention, 38% (6/16) [44, 46, 50, 51, 55, 57] were level 2 demonstrating alteration in objective knowledge or skills, and 13% (2/16) [45, 47] were assessed as level 3 showing an alteration in behavior as a result of the intervention. No studies were scored a level 4 showing a clear systems or outcome benefit.
Applying the BEME evidence-based scoring system to our collection of publications, the mean and median scores are 2.31 and 2.5 respectively. We found three studies (19%; 3/16) [52, 56, 58] were BEME grade 1—no clear conclusions can be deduced; five studies (31%; 5/16) [45, 47, 48, 53, 54] were BEME grade 2—ambiguous results, although appearance of a trend; and half of the studies (50%; 8/16) [36, 44, 46, 49,50,51, 55, 57] were scored a 3—conclusions can probably be based on the findings. Of the studies graded 2 and above, we see that only one was significant in its negative findings for benefits of educational interventions. No studies were deemed appropriate for BEME gradings of 4 or 5, due to generally small samples, somewhat low attendance of intervention learning opportunities, large reliance on questionnaires with relatively low participation, and challenging ways of evaluating.
Discussion
In conducting this systematic review, we aimed to summarize the literature for the current state of evidence for post-graduate medical training in the growing population of IDD. This analysis illuminates several noteworthy points of discussion. We found that just half of publications (8/16; 50%) [44,45,46,47, 50, 51, 55, 57] achieved a Kirkpatrick [60] level 2 or higher, with just 38% (6/16) achieving level 2 outcomes [44, 46, 50, 51, 55, 57] which corresponds to objective knowledge or skills benefit and just two studies (2/16; 13%) [45, 47] achieving a level 3 outcome, specifically a change in behavior or practice as a result of the teaching. The low number of educational interventions showing improvement in learner outcomes beyond level 2 is further buttressed by our finding that only just over half of the educational interventions directly assessed learner knowledge or skills before and after the intervention (56%; 9/16) [44,45,46, 50,51,52, 55,56,57] and two recent studies [48, 49] were limited to changing perspectives, attitudes, and values. Given the limited advancement of learner outcomes related to DD educational programs in the literature in recent years, we are left to consider that curriculum development for this population is in its infancy. This is consistent with previous survey-based research indicating a diversity of, and lack of, consistent application of curricula for treating patients with IDD in multiple postgraduate medical education specialties [32, 33, 35, 36, 38], and in medical students [67]. There is a great societal need for training in DD but limited consistency in the types of curricula and outcomes.
While not elaborated on in Boreman et al.’s surveying study [36], we did see that all interventions based upon specialized rotations that described their curricula thoroughly were supplemented with another non-experiential form of instruction. These included theoretical pedagogy (89%; 8/9) [44, 46, 48, 49, 53,54,55, 57], immersive methodology (67%; 6/9) [44, 46, 48, 49, 54, 57], and interactive structured teaching (22%; 2/9) [44, 46]. Several studies in the review which used multimodal approaches in training were more likely to achieve higher level outcomes in Kirkpatrick scores [44, 46, 47, 50, 51, 57]. While there is promise that programs used multi-modal approaches to training, which have been linked to improved effectiveness of educational programs [68], the lack of evidence of provider and patient improvement in outcomes observed in our review calls for alignment of instructional methods with intended goals.
This review reveals a subtle underlying trend towards interdisciplinary learning, and a relative absence of focus on competency-based teaching. A considerable group of studies (31%; 5/16) [47,48,49, 51, 55] educated multiple specialties and subspecialties of physicians together, and a broader group of healthcare professionals including non-physician trainees such as clinical psychology interns as well (13%; 2/16) [47, 51]. While interprofessional education (IPE) has been found to be valuable by interdisciplinary learners working with this population [69], it is thought to be optimally valuable when combined with defined competencies based on the learner characteristics such as milestones and entrustable professional activities (EPAs) [70]. This emphasizes the importance of further development in identifying competencies and learning opportunities specific to healthcare practice with the growing population of people with IDD. The establishment of specific competencies relevant to each learner’s role in supporting and treating those with IDD would provide an avenue towards unifying this area of medicine’s natural interdisciplinary nature with objectively measurable effective training practices. In fact, the Association of University Centres on Disabilities (AUCD)’s Leadership Education in Neurodevelopmental and Related Disorders (LEND) [71], an organization which provides graduate training to an interdisciplinary learner base, has been aiming towards developing such core competencies [72] for its learners in recent years, which may be a model for other training programs. Additionally, interprofessional care competencies can be integrated in the IDD curricula to equip residents with the skills to work collaboratively [73]. Advancing from competencies, robust assessment of educational interventions aimed at behavioral change and clinical outcomes is desirable [74]. Alignment of curricula to its various components such as instructional methods, assessment, faculty development, and a greater purpose of serving student and societal needs has been highlighted. This is of greater significance for underserved population such as people with IDD. Future research should continue to focus on inter-disciplinary training and curricula, with more consistent assessment methods and a greater alignment with competency-based medical education.
High level education outcomes such as behavioral changes were not observed consistently in the studies reviewed. One of the possible reasons can be due to the preponderance of variation in educational delivery in this field. Secondly, there is a lack of consistent use of competencies for DD training in published curricula despite their availability. Thirdly, it may be related to unclear education outcome measures and inconsistent use of longitudinal multi-modal approaches to pedagogy. Substantial efforts to develop effective curricula standards have been made in this field which is an encouraging trend. Examples of this include the development of a specialized adult psychiatric senior residency training in learning disabilities in the UK [41], and a nationally mandated developmental/behavioral pediatrics rotation in US pediatrics residencies [75].
The findings of the study are limited by the narrowed focus on literature published in English. Additionally, the exclusion of studies which did not have a well-defined educational program or formal evaluation limited the study of educational programs in developmental disabilities in its full entirety. Moreover, as this study reviewed only published educational literature, it is likely that training curricula already in place which have not published educational effectiveness data were not captured in this review. Specifically, just one study was found in Child and Adolescent Psychiatry [55] and Developmental and Behavioral Pediatrics [47], which may be indicative of paradoxically low publications due to existing integration of IDD in the overall curricula. While this may be the case, as medical education moves further ahead towards competency-based medical education (CBME), there is greater need for further academic scholarship in this area, to ensure the effectiveness of the training in place, and to support scientific collaboration in developing tomorrow’s educational models especially for programs currently developing curricula for treating the growing population of those with ASD/ID/DD.
In conclusion, this review of evaluated postgraduate medical education in IDD across all specialty programs provides a glimpse into the published community, and highlighted two overarching trends. Firstly, literature in this field is in its early days which is reflected by a diversity of curricula characteristics, a significant proportion employing more subjective evaluation methods, and a greater focus on learner satisfaction, attitudes, and values, as opposed to changes in learner behavior and patient outcomes. Secondly, our review did identify a trend towards a specialized IDD rotation which can then be supplemented with further instruction involving more experiential, theoretical, interactive, and immersive learning. Despite this trend, the effectiveness of this holistic educational model using multiple instructional methods remains unclear and represents an opportunity for future study. Future studies are needed comparing different duration and instructional methods, such as online blended formats, simulation, and patient/family co-taught sessions.
The paucity of studies calls for more research in this area, especially with the increased prevalence of IDD and the growing societal care needs of this patient population. By blending the positive aspects of the educational diversity identified in this review, with the drive towards developing a more standardized and effective curriculum, education leaders and curriculum experts have the opportunity to utilize the breadth of learner levels, instructor types, settings, timelines, and pedagogical methods identified in this review towards creating an interdisciplinary, competency-based curriculum that makes a quantifiable difference for the growing population of patients living with IDD and their families.
References
Zablotsky B, Black LI, Blumberg SJ. Estimated prevalence of children with diagnosed developmental disabilities in the United States, 2014-2016. NCHS Data Brief. 2017(291):1–8.
Boyle CA, Boulet S, Schieve LA, Cohen RA, Blumberg SJ, Yeargin-Allsopp M, et al. Trends in the prevalence of developmental disabilities in US children, 1997-2008. Pediatrics. 2011;127(6):1034–42.
Boulet SL, Boyle CA, Schieve LA. Health care use and health and functional impact of developmental disabilities among US children, 1997-2005. Pediatr Adolesc Med. 2009;163(1):19–26.
Maulik PK, Mascarenhas MN, Mathers CD, Dua T, Saxena S. Prevalence of intellectual disability: a meta-analysis of population-based studies. Res Dev Disabil. 2011;32(2):419–36.
Yeargin-Allsopp M, Murphy CC, Oakley GP, Sikes RK. A multiple-source method for studying the prevalence of developmental disabilities in children: the Metropolitan Atlanta Developmental Disabilities Study. Pediatrics. 1992;89(4 Pt 1):624–30.
Elsabbagh M, Divan G, Koh YJ, Kim YS, Kauchali S, Marcin C, et al. Global prevalence of autism and other pervasive developmental disorders. Autism Res. 2012;5(3):160–79.
Mattila ML, Kielinen M, Linna SL, Jussila K, Ebeling H, Bloigu R, et al. Autism spectrum disorders according to DSM-IV-TR and comparison with DSM-5 draft criteria: an epidemiological study. J Am Acad Child Adolesc Psychiatry. 2011;50(6):583–92 e11.
Kim YS, Leventhal BL, Koh YJ, Fombonne E, Laska E, Lim EC, et al. Prevalence of autism spectrum disorders in a total population sample. Am J Psychiatry. 2011;168(9):904–12.
Baron-Cohen S, Scott FJ, Allison C, Williams J, Bolton P, Matthews FE, et al. Prevalence of autism-spectrum conditions: UK school-based population study. Br J Psychiatry. 2009;194(6):500–9.
Idring S, Rai D, Dal H, Dalman C, Sturm H, Zander E, et al. Autism spectrum disorders in the Stockholm Youth Cohort: design, prevalence and validity. PLoS One. 2012;7(7):e41280.
Blumberg SJ, Bramlett MD, Kogan MD, Schieve LA, Jones JR, Lu MC. Changes in prevalence of parent-reported autism spectrum disorder in school-aged U.S. children: 2007 to 2011–2012. Natl Health Stat Rep. 2013;(65):1–11.
Saemundsen E, Magnusson P, Georgsdottir I, Egilsson E, Rafnsson V. Prevalence of autism spectrum disorders in an Icelandic birth cohort. BMJ Open. 2013;3(6).
Wehmeyer MLBI, Percy M, Shogren KA, Fung WLA. A comprehensive guide to intellectual and developmental disabilities. 2nd ed. Baltimore: Brookes Publishing; 2017.
Liptak GS, Stuart T, Auinger P. Health care utilization and expenditures for children with autism: data from U.S. national samples. J Autism Dev Disord. 2006;36(7):871–9.
Mandell DS, Cao J, Ittenbach R, Pinto-Martin J. Medicaid expenditures for children with autistic spectrum disorders: 1994 to 1999. J Autism Dev Disord. 2006;36(4):475–85.
Msall ME, Avery RC, Tremont MR, Lima JC, Rogers ML, Hogan DP. Functional disability and school activity limitations in 41,300 school-age children: relationship to medical impairments. Pediatrics. 2003;111(3):548–53.
Beange H, McElduff A, Baker W. Medical disorders of adults with mental retardation: a population study. Am J Ment Retard. 1995;99(6):595–604.
Tyrer F, McGrother C. Cause-specific mortality and death certificate reporting in adults with moderate to profound intellectual disability. J Intellect Disabil Res. 2009;53(11):898–904.
Heslop P, Blair PS, Fleming P, Hoghton M, Marriott A, Russ L. The confidential inquiry into premature deaths of people with intellectual disabilities in the UK: a population-based study. Lancet. 2014;383(9920):889–95.
Anderson LL, Humphries K, McDermott S, Marks B, Sisirak J, Larson S. The state of the science of health and wellness for adults with intellectual and developmental disabilities. Intellect Dev Disabil. 2013;51(5):385–98.
Lennox N, Bain C, Rey-Conde T, Purdie D, Bush R, Pandeya N. Effects of a comprehensive health assessment programme for Australian adults with intellectual disability: a cluster randomized trial. Int J Epidemiol. 2007;36(1):139–46.
Iacono T, Davis R. The experiences of people with developmental disability in Emergency Departments and hospital wards. Res Dev Disabil. 2003;24(4):247–64.
Sutherland G, Couch MA, Iacono T. Health issues for adults with developmental disability. Res Dev Disabil. 2002;23(6):422–45.
Lennox NG, Diggens JN, Ugoni AM. The general practice care of people with intellectual disability: barriers and solutions. J Intellect Disabil Res. 1997;41(Pt 5):380–90.
Bond L, Kerr M, Dunstan F, Thapar A. Attitudes of general practitioners towards health care for people with intellectual disability and the factors underlying these attitudes. J Intellect Disabil Res. 1997;41(Pt 5):391–400.
Dosreis S, Weiner CL, Johnson L, Newschaffer CJ. Autism spectrum disorder screening and management practices among general pediatric providers. J Dev Behav Pediatr. 2006;27(2 Suppl):S88–94.
Golnik A, Ireland M, Borowsky IW. Medical homes for children with autism: a physician survey. Pediatrics. 2009;123(3):966–71.
Golnik AE, Ireland M. Complementary alternative medicine for children with autism: a physician survey. J Autism Dev Disord. 2009;39(7):996–1005.
Vohra R, Madhavan S, Sambamoorthi U. Emergency department use among adults with autism spectrum disorders (ASD). J Autism Dev Disord. 2016;46(4):1441–54.
Lunsky Y, Balogh R, Cairney J. Predictors of emergency department visits by persons with intellectual disability experiencing a psychiatric crisis. Psychiatr Serv. 2012;63(3):287–90.
Lunsky Y, Paquette-Smith M, Weiss JA, Lee J. Predictors of emergency service use in adolescents and adults with autism spectrum disorder living with family. Emerg Med J. 2015;32(10):787–92.
Goodenough GK, Hole-Goodenough J. Training for primary care of mentally handicapped patients in US family practice residencies. J Am Board Fam Pract. 1997;10(5):333–6.
Tyler CV Jr, Snyder CW, Zyzanski SJ. Caring for adults with mental retardation: survey of family practice residency program directors. Ment Retard. 1999;37(5):347–52.
Casson I, Abells D, Boyd K, Bradley E, Gemmill M, Grier E, et al. Teaching family medicine residents about care of adults with intellectual and developmental disabilities. Can Fam Physician. 2019;65(Suppl 1):S35–40.
Broder-Fingert S, Ferrone CF, Giauque A, Connors SL. Residents’ knowledge and comfort with caring for children with autism spectrum disorder. Clin Pediatr (Phila). 2014;53(14):1390–2.
Boreman CD, Thomasgard MC, Fernandez SA, Coury DL. Resident training in developmental/behavioral pediatrics: where do we stand? Clin Pediatr (Phila). 2007;46(2):135–45.
Schmitt M, Blue A, Aschenbrener CA, Viggiano TR. Core competencies for interprofessional collaborative practice: reforming health care by transforming health professionals’ education. Acad Med. 2011;86(11):1351.
Lunsky Y, Bradley E. Developmental disability training in Canadian psychiatry residency programs. Can J Psychiatr. 2001;46(2):138–43.
Accreditation Council for Graduate Medical Education. ACGME Program Requirements for Graduate Medical Education in Child and Adolescent Psychiatry. 2020. https://www.acgme.org/Portals/0/PFAssets/ProgramRequirements/405_ChildAdolescentPsychiatry_2020.pdf?ver=2020-06-19-130331-607. Last accessed August 31st, 2020.
Marrus N, Veenstra-Vanderweele J, Hellings JA, Stigler KA, Szymanski L, King BH, et al. Training of child and adolescent psychiatry fellows in autism and intellectual disability. Autism. 2014;18(4):471–5.
Royal College of Psychiatrists. A competency based curriculum for specialist training in psychiatry: specialists in the psychiatry of learning disability. 2010 (Revised May 2017) [cited 2019 January 11th]; Available from: https://www.gmc-uk.org/-/media/documents/psychiatry-of-learning-disability-curriculum-august-2017-admin-change_pdf-71642082.pdf.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1–34.
Hammick M, Dornan T, Steinert Y. Conducting a best evidence systematic review. Part 1: From idea to data coding. BEME Guide No. 13. Med Teach. 2010;32(1):3–15.
Bennett FC, Guralnick MJ, Richardson HB Jr, Heiser KE. Teaching developmental pediatrics to pediatric residents: effectiveness of a structured curriculum. Pediatrics. 1984;74(4):514–22.
Bauer SC, Smith PJ, Chien AT, Berry AD, Msall ME. Educating pediatric residents about developmental and social-emotional health. Infants Young Child. 2009;22(4):309–20.
Guralnick MJ, Bennett FC, Heiser KE, Richardson HB Jr, Shibley RE Jr. Training residents in developmental pediatrics: results from a national replication. J Dev Behav Pediatr. 1987;8(5):260–5.
Kawamura A, Mylopoulos M, Orsino A, Jimenez E, McNaughton N. Promoting the development of adaptive expertise: exploring a simulation model for sharing a diagnosis of autism with parents. Acad Med. 2016;91(11):1576–81.
Keisling BL, Bishop EA, Kube DA, Roth JM, Palmer FB. Long-term pediatrician outcomes of a parent led curriculum in developmental disabilities. Res Dev Disabil. 2017;60:16–23.
Kube DA, Bishop EA, Roth JM, Palmer FB. Evaluation of a parent led curriculum in developmental disabilities for pediatric and medicine/pediatric residents. Matern Child Health J. 2013;17(7):1304–8.
Kennedy T, Regehr G, Rosenfield J, Roberts SW, Lingard L. Exploring the gap between knowledge and behavior: a qualitative study of clinician action following an educational intervention. Acad Med. 2004;79(5):386–93.
Major NE, Peacock G, Ruben W, Thomas J, Weitzman CC. Autism training in pediatric residency: evaluation of a case-based curriculum. J Autism Dev Disord. 2013;43(5):1171–7.
Nalven LM, Hofkosh D, Feldman H, Kelleher K. Teaching pediatric residents about early intervention and special education. J Dev Behav Pediatr. 1997;18(6):371–6.
Reinblatt SP, Rifkin A, Castellanos FX, Coffey BJ. General psychiatry residents’ perceptions of specialized training in the field of mental retardation. Psychiatr Serv. 2004;55(3):312–4.
Ruedrich S, Dunn J, Schwartz S, Nordgren L. Psychiatric resident education in intellectual disabilities: one program's ten years of experience. Acad Psychiatry. 2007;31(6):430–4.
Szeftel R, Hakak R, Meyer S, Naqvi S, Sulman-Smith H, Delrahim K, et al. Training psychiatric residents and fellows in a telepsychiatry clinic: a supervision model. Acad Psychiatry. 2008;32(5):393–9.
Thompson LA, Tuli SY, Saliba H, DiPietro M, Nackashi JA. Improving developmental screening in pediatric resident education. Clin Pediatr (Phila). 2010;49(8):737–42.
Wolraich ML. Pediatric practitioners’ knowledge of developmental disabilities. J Dev Behav Pediatr. 1980;1(4):147–51.
Wysocki T, Gururaj VJ, Rogers MA, Galey G. Training pediatric residents in early intervention with handicapped children. J Med Educ. 1987;62(1):47–52.
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol. 2009;62(10):1006–12.
Kirkpatrick DL, Kirkpatrick JD. Evaluating training programs : the four levels. 3rd ed. San Francisco, CA: Berrett-Koehler; 2006.
Sultan N, Torti J, Haddara W, Inayat A, Inayat H, Lingard L. Leadership development in postgraduate medical education: a systematic review of the literature. Acad Med. 2019;94(3):440–9.
Webb AM, Tsipis NE, McClellan TR, McNeil MJ, Xu M, Doty JP, et al. A first step toward understanding best practices in leadership training in undergraduate medical education: a systematic review. Acad Med. 2014;89(11):1563–70.
Chung HO, Oczkowski SJ, Hanvey L, Mbuagbaw L, You JJ. Educational interventions to train healthcare professionals in end-of-life communication: a systematic review and meta-analysis. BMC Med Educ. 2016;16:131.
Boje RB, Ludvigsen MS. Educational interventions that address handover skills of healthcare professionals: a scoping review protocol. JBI Database System Rev Implement Rep. 2017;15(12):2842–7.
Pincavage AT, Donnelly MJ, Young JQ, Arora VM. Year-end resident clinic handoffs: narrative review and recommendations for improvement. Jt Comm J Qual Patient Saf. 2017;43(2):71–9.
Wong BM, Etchells EE, Kuper A, Levinson W, Shojania KG. Teaching quality improvement and patient safety to trainees: a systematic review. Acad Med. 2010;85(9):1425–39.
Trollor JN, Ruffell B, Tracy J, Torr JJ, Durvasula S, Iacono T, et al. Intellectual disability health content within medical curriculum: an audit of what our future doctors are taught. BMC Med Educ. 2016;16:105.
Cervero RM, Gaines JK. The impact of CME on physician performance and patient health outcomes: an updated synthesis of systematic reviews. J Contin Educ Heal Prof. 2015;35(2):131–8.
Anderson ES, Smith R, Thorpe LN. Learning from lives together: medical and social work students' experiences of learning from people with disabilities in the community. Health Soc Care Commun. 2010;18(3):229–40.
Wagner SJ, Reeves S. Milestones and entrustable professional activities: the key to practically translating competencies for interprofessional education? J Interprof Care. 2015;29(5):507–8.
Association of University Centers on Disabilities. Association of University Centers on Disabilities. [August 31st 2020]; Available from: https://www.aucd.org/template/page.cfm?id=473.
Leff SS, Baum KT, Bevans KB, Blum NJ. Development, validation, and utility of an instrument to assess core competencies in the Leadership Education in Neurodevelopmental and Related Disabilities (LEND) program. Matern Child Health J. 2015;19(2):314–23.
Leggat SG. Effective healthcare teams require effective team members: defining teamwork competencies. BMC Health Serv Res. 2007;7:17.
Kulasegaram K, Mylopoulos M, Tonin P, Bernstein S, Bryden P, Law M, et al. The alignment imperative in curriculum renewal. Med Teach. 2018;40(5):443–8.
Accreditation Council for Graduate Medical Education. ACGME Program Requirements for Graduate Medical Education in Pediatrics. 2013. http://www.acgme.org/Portals/0/PDFs/archive/320_pediatrics_PRs_RC.pdf. Last accessed August 31st, 2020.
Acknowledgments
We would like to acknowledge the community at the Centre for Addictions and Mental Health, and University of Toronto for advancing medical research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
On behalf of all authors, the corresponding author declares that there is no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Adirim, Z., Sockalingam, S. & Thakur, A. Post-graduate Medical Training in Intellectual and Developmental Disabilities: a Systematic Review. Acad Psychiatry 45, 371–381 (2021). https://doi.org/10.1007/s40596-020-01378-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40596-020-01378-8