
Abstract
Objectives
To relate major lifestyle habits with all-cause mortality in an almost extinct male middle-aged population.
Material and methods
A 40–59 aged male population of 1712 subjects was enrolled and examined in 1960 and then followed-up for 60 years. Baseline smoking habits, working physical activity and dietary habits, each subdivided into 3 classes, were related to 60-year mortality, by Kaplan–Meier survival curves, Cox proportional hazards model and to age at death during 60 years by multiple linear regression.
Results
Death rate in 60 years was of 99.7% with only 5 survivors and 2 lost to follow-up after 50 years. Two out of three classes of each behavior were significantly protective versus the third class in all the statistical approaches. Cox hazard ratios (and their 95% confidence limits) of never smokers versus smokers was 0.71 (0.63–0.79); that of vigorous physical activity versus sedentary activity was 0.75 (0.64–0.89); that of Mediterranean diet versus Not Mediterranean diet was 0.74 (0.66–0.84). The gain of age at death for never smokers versus smokers was 3.32 years (2.05–4.54); of vigorous physical activity versus sedentary activity was 3.53 years (1.68–5.37); that of Mediterranean diet versus Not Mediterranean diet was 3.67 years (2.32–5.02). Age at death was more than 10 years longer for men with the 3 best behaviors than for those with the 3 worst behaviors.
Conclusions
Some lifestyle habits are strongly related to lifetime mortality and longevity.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The role of some lifestyle behaviors, such as cigarette smoking, physical activity and eating habits, as determinants of all-cause mortality has been documented by many reports based on population studies frequently in combined way [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19]. The majority of these contributions covered relatively short follow-up periods, usually less than 25 years, while some population studies started in the mid of last century have reached very long observation periods towards the quasi-extinction of the original cohorts [4, 14, 18]. This allows to tackle systematically the problem by considering the outcome of a life-long experience in the search of behavioral determinants of longevity.
The Italian Rural Areas of the Seven Countries Study of Cardiovascular Diseases (IRA-SCS) enrolled in 1960, have reached 60 years of follow-up with complete data on life status and mortality and an overall death rate of 99.7%. The purpose of this analysis was to study the relationships of 3 lifestyle behaviors, that is cigarette smoking, physical activity and dietary habits, with all causes of death during the entire lifespan.
Material and methods
Population and measurements
The epidemiological material used for this analysis is made by the IRA-SCS that included 1712 middle-aged (40 to 59 years) men at entry examination in 1960, representing 98.5% of defined samples. More details can be found elsewhere [14, 18].
Three lifestyle behaviors were considered as follows: (A) Cigarette smoking was evaluated by a questionnaire and 3 classes of smoking habits were used for analysis: smokers, ex-smokers and never smokers; (B) Physical activity was derived from a questionnaire matched with the profession. Then, 3 levels of physical activity at work were defined, i.e. sedentary, moderate and vigorous. The mean energy expenditure of these 3 levels were estimated by a side study where ergonometric measurements were taken [20] and independently by the caloric intake measured on the diet [21]. Mean values of these estimates are given in Table 1; (C) Dietary habits were measured using the dietary history [21] and data were converted into 18 food groups. Factors analysis was carried out and factor 2 (out of the 3 explored) was chosen to produce factor score estimates for each subject. Details on the procedure are reported elsewhere [22]. Factor score, for each case was computed using the factor score coefficients, that is the estimate of an underlying factor formed from the linear combination of the observed variables. This means that a factor becomes a numerical characteristic of each individual and can be used as a variable in subsequent modelling. The dietary questionnaire was administered a few years after the entry examination, and therefore factor scores were regressed on age to reach the entry baseline value, while for 25% of subjects with missing data it was imputed by multivariate normal procedure using as reference 30 other personal characteristics [18]. No significant difference was found between the mean of the original values and that of the imputed values. Moreover, Cox models for the prediction of events with and without the imputed values of factor score 2 produced similar coefficients for the dietary indices. Factor score is a continuous variable that can be used as such or divided in sections to identify groups with different characteristics. We decided to divide it into 3 tertiles that were arbitrarily called: tertile 1 = Not Mediterranean diet; tertile 2 = Prudent diet; tertile 3 = Mediterranean diet. The term Prudent diet was assigned to the intermediate category after the end of the analysis when it was shown that it was beneficial versus the one called Not Mediterranean diet. In the original factor analysis the group called Mediterranean diet was characterized by different food consumption, compared to the Not Mediterranean, since it mainly had higher intakes of bread, cereals, potatoes, vegetable and fish and definitely lower intakes of fruit, meat, milk, sugar and alcohol. This was true to a lesser extent also comparing the Mediterranean diet group with the Prudent diet group.
Beyond the above behaviors we explored two variables of social and socio-economic type that could be indirectly involved into the problem. They were: (D) Marital status, derived from a questionnaire (married = 1; not married = 0); (E) High socio-economic status (SES yes = 1; no = 0) derived from a questionnaire and attributing a high level when the type of work was professional, business, public administrators, foreman and high rank clerks.
Systematic collection of mortality data was performed for 60 years and only 2 men were lost to follow-up at the time of the 50-year follow-up anniversary. All-cause mortality was used for this analysis.
Collection of data started before the era of the Helsinki Declaration, with consent implied by participation at the base-line examination while in subsequent surveys verbal or written consent was obtained for collection of follow-up data.
Statistical Analysis
Kaplan Meier survival curves were computed as a function of smoking habits, physical activity and diet and their classes.
Cox proportional hazards models were solved with all-cause of death as end-point and the 3 lifestyle behaviors as covariates, each divided into the 3 classes as described above, plus age.
A multiple linear regression model was solved using age at death (the age at the time of death or when the subject was last seen alive) as dependent variable (survival) and the 3 behaviors divided into the 3 classes as independent variables plus entry age. A matrix was built with the estimated age at death derived from the multiple linear regression model with all the possible combinations of the various lifestyle behaviors.
In side analyses, including the same procedures described above, we tested also the role of marital status and high SES.
A comparison was made of behavioral characteristics and for estimates derived from the multivariate models between centenarians and the others.
Results
Table 1 summarizes the behavioral habits of the study population, reflecting the situation of men living in rural communities in the mid of last century, with a relatively high prevalence of current smokers, high mean levels of physical activity bound to work, and varied dietary habits, still oriented in prevalence toward healthy habits.
In 60 years, 1707 men died out of the 1712 enrolled at entry (99.7%) with the almost extinction of the cohort, while 2 men were lost at year 50 of follow-up (as they moved to different locations repeatedly) when they were aged 91 and 96, respectively. Only 5 men were alive and all of them were aged 100 years or more.
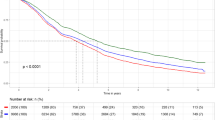
Kaplan–Meier survival curves for all-cause mortality as a function of the 3 behaviors and their classes are depicted in Figs. 1, 2 and 3. For each figure class 1 of a given behavior is the one carrying the worse outcome. In each of them there was a clear separation of the 3 components and the p of the log-rank chi squared was < 0.0001 for smoking and dietary habits and 0.0013 for physical activity. Comparing the log-rank Mantel–Haenszel probability in pairs of curves, a significant difference was found between never smokers and both ex-smokers and smokers; between sedentary and both moderate and vigorous physical activity; and between Mediterranean diet and both Prudent and Not Mediterranean diets.

Kaplan–Meier survival curves in 60 years as a function of 3 categories of smoking habits: smoke 1 = smokers; smoke 2 = ex-smokers; smoke 3 = never smokers

Kaplan–Meier survival curves in 60 years as a function of 3 categories of physical activity at work: phyac1 = sedentary; phyac2 = moderate; phyac3 = vigorous

Kaplan–Meier survival curves in 60 years as a function of 3 categories of dietary habits: diet1 = Not Mediterranean; diet2 = Prudent; diet3 = Mediterranean
In fact, the curves for smokers and ex-smokers were overlapping for the first 20 years of follow-up while later the curve for ex-smokers became closer to that of never smokers. In the case of physical activity, during the first 15 years the curves of vigorous was overlapping with that of moderate activity, but the latter clearly separated from the former during the next years. For dietary habits, the curves for Prudent and Not Mediterranean habits were overlapping for the first 10 years. Subsequently the curve of Prudent diet became closer to that of Mediterranean diet, eventually overlapping during the last 10 years.
In the Cox proportional hazards model for all-cause mortality as a function of age and the 3 behaviors (Table 2) reference class for each type was made by the one with the worst outcome so that hazard ratios (HR) were all smaller than 1. All HR were large and significant except that of moderate versus sedentary physical activity that had a p = 0.0836 for its multivariate coefficient. In general, never smokers, and men with vigorous physical activity and Mediterranean or Prudent diets were largely protected for all-cause mortality.
The individual risk of death estimated by the Cox model equation was very high with a range of 0.9828 to 0.9999, clearly due to the practical extinction of the cohort and this prevented the possibility to study the calibration of the system, that is to compute the number of cases in quantiles of estimated risk. On the other hand, the ROC curve had a value of 0.823.
The multiple linear regression model with age at death as end-point and the same behaviors as covariates showed similar findings (Table 3). Again, the reference class for each behavior was chosen to be the one accompanied by the the worst outcome so that the multivariate coefficients were all positive. In this case the coefficient of each covariate indicates the number of years gained versus the reference of its behavioral group. Several years of life are gained being a never smoker, having a vigorous physical activity and following a Mediterranean diet. The intermediate class of each behavior was also significantly adding years of life except ex-smokers whose 95% confidence limits crossed zero.
The three lifestyle behaviors and their classes could be combined into 27 combinations and for each of them the estimated age at death was computed and reported in Table 4. There were large variations in the expected age at death ranging from 70.2 (for smokers, plus sedentarism, plus Not Mediterranean diet) to 80.7 years (for never smokers plus vigorous physical activity plus Mediterranean diet). The correspondent levels of age at death actually found were 69.6 years and 80.4 years, that fit well with those estimated by the model.
The above analyses were replicated including also marital status and high SES, that provided findings not so coherent across the three statistical procedures as found for the basic behaviors (details not tabulated). In particular, Kaplan–Meier curves for survival showed the beneficial role of being married (versus not married) with log-rank chi-squared p = 0.0265, while the curve for high SES versus not-high-SES had a p = 0.8207, although a protective role of high SES was clear during the first 20 years of follow-up. Cox model for mortality including marital status and high SES in addition of age and the three main behaviors provided not significant coefficients for these added variables. On the other hand, in the multiple linear regression model for prediction of age at death the role of being married and high SES was significant with coefficients around 2, that is adding about 2 years to age at death. The coefficients for the behavioral variables were not significantly different from those obtained in the previous model (without marital status and high SES). However, if all possible combinations of covariates were considered, the number of combinations in the matrix would increase from 27 to 108 and we thus omitted those.
Among the 1712 men enrolled in 1960, 10 reached the age of 100 years (6 per 1000) and some differences versus the others were found. In particular, the estimated Cox model probability of death had a mean of 0.9932 for the centenarians, versus 0.9974 for the others (p of difference = 0.0032), while age at death estimated from the multiple linear regression was 77.2 for the centenarians and 75.1 for the others (p = 0.0088). The frequency of beneficial behaviors was larger for the centenarians (7 out 10 with vigorous physical activity, 6 out of 10 never smokers; 9 out of 10 with Mediterranean or Prudent diets) but due to the small numbers the comparison with the others (not centenarians) was statistically significant only for smoking habits (p of chi squared = 0.0197).
Discussion
General comments
Findings from this investigation suggest that 3 common lifestyle behaviors play a role as determinants of all causes of death and age at death in a quasi-extinct male population sample. Some of those associations are confirmatory of what reported beforehand by this and other studies [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19]. The unique characteristic of this analysis is that it was run systematically in a population sample followed-up for 60 years and with a mortality rate of 99.7%. Moreover, it is impressive that single measurements taken at base-line in middle-aged men were strongly associated with mortality, age at death and longevity. The predictive power of the three behaviors was confirmed and proved to be rather similar using different statistical approaches, that is Kaplan–Meier curves for survival, Cox proportional hazards model for mortality prediction and multiple linear regression for age at death prediction.
The rank in prediction of outcome of the 3 levels in each of the 3 behaviors was similar in the various statistical approaches, with non-smoking, being physically active and following a Mediterranean diet showing the best outcome, while on the opposite being a smoker, a sedentary man and using a Not Mediterranean diet made the worst outcome. The intermediate classes of lifestyle habits (ex-smokers, moderate physical activity and Prudent diet) had an intermediate role versus the outcome.
The gains in additional years of life for the best versus the worst habit were around 10 years as shown in Table 4, while for the composite of the combined intermediate behaviors the gain was of almost 8 years.
Limits of the analysis
This analysis may have limits bound to the small numbers involved, partially compensated by the extremely long follow-up period of observation.
The definition of dietary habits was based on an established a-posteriori pattern that was not influenced by aprioristic decisions and was highly related (both as a continuous variable and when divided in subgroups) with all-cause deaths. On the other hand, we are aware that due to its mathematical characteristics it cannot be transferred to other populations but this was not the purpose of this analysis.
The classification of physical activity was based on rough data but indirectly validated by other techniques and was limited to working activity since those times and in that social environment leisure physical activity was absolutely marginal.
Measurements of lifestyle habits were taken at baseline and the analysis was focused on their relationship extended to the whole observation period. Systematic measurements taken during subsequent examinations were not available or incomplete and therefore time trends cannot be used for this analysis. By sure, there has been a decline in the proportion of current smokers, and a decline of physical activity bound to advancing age. Some partial surveys showed also that some of the characteristics of the Mediterranean diet were partially lost during the follow-up. However, the multivariable coefficients of the Cox model for the behavioral characteristics estimated for the first 25 years of follow-up were not statistically different from those estimated for 50 years [18], nor those of 60-year versus those of 30-year follow-up in the present analysis thus suggesting a relative stability in the relationships between lifestyle habits and outcome.
The exploration of the role of marital status and high SES was substantially inconclusive because these characteristics are not clearly behavioral habits and because of the inconsistency in the outcome across the different statistical approaches. However, referring to the matrix of Table 4, we can say that the presence of those characteristics might increase the age at death of 2 years each.
Clearly these findings cannot be directly and fully transferred to present days, due to different levels of risk factors and behaviors, the present possibilities of prevention and treatment and the decline of mortality (mainly cardiovascular) occurred during the last years of the past century. However, to study a life-time experience we must rely on the past in order to learn hints for the future. The search is directed to find general rules connecting behaviors with health and disease and apparently our conclusions are in line with past and recent findings based on shorter follow-up observations.
Literature contribution
The literature is rich of reports documenting the separate role of the 3 behavioral habits on health, and this is particularly true, during the last few years, for eating habits with the identification of subgroups of populations, almost in every country, that follow dietary habits resembling the so-called Mediterranean diet and was associated with reduction of all-cause of death and specific morbid conditions. Reports dealing with the 3 behaviors considered together are less frequent, but still numerous [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16]. There are impressive aspects in these findings since the contributions come from largely different countries and cultures. Since these findings are rather similar across the various studies and none contradicts the others, it seems that some universal rules apply everywhere when smoking habits, physical activity and dietary habits are concerned in relation with health and disease and expectancy of life.
There are other ways to study long-term survival and longevity, for example to measure the characteristics of the centenarians that has risen much interest in the last decades as exemplified by Zyczkowska et al. [23] and particularly by a Japanese book on the issue [24]. However, this information, still of great interest, says very little on the possible behavioral causes of longevity. Some investigators, on the other hand believe, on the basis of similar analyses, that a low profile of cardiovascular risk factors is a pre-requisite for longevity and the same is found at the age of 100 years or more [25]. Finally, the search of the gene of longevity is the other extreme approach [26] and it should be combined with the exploration of gene-behavior interactions. Further predictive studies on centenarians versus those who did not live long but were followed-up longitudinally and the exploration of concomitant biological covariates and/or their changes will certainly help unveiling the secrets of an healthy and long life.
Conclusions
It is concluded that in view of the prominence of some behavioral risk factors, behavioral and social science research on interventions for these risks should be strengthened which may be facilitated by the fact that many prevention and primary care policy options are available now to act on key risks. Acting effectively on smoking habits, physical activity and dietary habits as shown in the present investigation should be a good starting point for cardiovascular and overall disease-burden prevention and life prolongation. Whether these behavioral lifestyle characteristics are associated with biological, potentially modifiable covariates, is the needed topic of important future investigations.
References
Davis MA, Neuhaus JM, Moritz DJ, Lein D, Barclay JD, Murphy SP (1994) Health behaviors and survival among middle-aged and older men and women in the NHANES I Epidemiologic Follow-up Study. Prev Med 23:369–376
Ruigómez A, Alonso J, Antó JM (1995) Relationship of health behaviors to five-year mortality in an elderly cohort. Age Ageing 24:113–119
Knoops KTB, de Groot LCPGM, Kromhout D, Perrin AE, Moreiras-Varela O, Menotti A et al (2004) Mediterranean diet, lifestyle factors, and 10-year mortality in elderly European men and women: the HALE project. JAMA 292:1433–1439
Doll R, Peto R, Boreham J, Sutherland I (2004) Mortality in relation to smoking: 50 years’ observations on male British doctors. Br Med J 328:1519–1531
van Dam RM, Li T, Spiegelman D, Franco OH, Hu FB (2008) Combined impact of lifestyle factors on mortality: prospective cohort study in US women. Br Med J 337:a1440
Kvaavik E, Batty GD, Ursin G, Huxley R, Gale CR (2010) Influence of individual and combined health behaviors on total and cause-specific mortality in men and women: the United Kingdom health and lifestyle survey. Arch Intern Med 170:711–718
Nechuta SJ, Shu XO, Li HL, Yang G, Xiang YB, Cai H et al (2010) Combined impact of lifestyle-related factors on total and cause-specific mortality among Chinese women: prospective cohort study. PLoS Med 7:e1000339
Loef M, Walach H (2012) The combined effects of healthy lifestyle behaviors on all cause mortality: a systematic review and meta-analysis. Prev Med 55:163–170
Yun JE, Won S, Kimm H, Jee SH (2012) Effects of a combined lifestyle score on 10-year mortality in Korean men and women: a prospective cohort study. BMC Public Health 20:673
Carlsson AC, Wändell PE, Gigante B, Leander K, Hellenius ML, de Faire U (2013) Seven modifiable lifestyle factors predict reduced risk for ischemic cardiovascular disease and all-cause mortality regardless of body mass index: a cohort study. Int J Cardiol 168:946–952
Behrens G, Fischer B, Kohler S, Park Y, Hollenbeck AR, Leitzmann MF (2013) Healthy lifestyle behaviors and decreased risk of mortality in a large prospective study of U.S. women and men. Eur J Epidemiol 28:361–372
Menotti A, Puddu PE, Lanti M, Maiani G, Catasta G, Fidanza AA (2014) Lifestyle habits and mortality from all and specific causes of death: 40-year follow-up in the Italian rural areas of the Seven Countries Study. J Nutr Health Aging 18:314–321
Reedy J, Krebs-Smith SM, Miller PE, Liese AD, Kahle LL, Park Y et al (2014) Higher diet quality is associated with decreased risk of all-cause, cardiovascular disease, and cancer mortality among older adults. J Nutr 144:881–889
Li K, Hüsing A (2014) Kaaks R (2014) Lifestyle risk factors and residual life expectancy at age 40: a German cohort study. BMC Med 12:59
Prinelli F, Yannakoulia M, Anastasiou CA, Adorni F, Di Santo SG, Musicco M et al (2015) Mediterranean diet and other lifestyle factors in relation to 20-year all-cause mortality: a cohort study in an Italian population. Br J Nutr 113:1001–1011
May AM, Struijk EA, Fransen HP, Onland-Moret NC, de Wit GA, Boer JM et al (2015) The association between single health behaviors and incidence of and premature mortality. BMC Med 13:39
Menotti A, Puddu PE, Maiani G, Catasta G (2016) Cardiovascular and other causes of death as a function of lifestyle in a quasi extinct middle-aged male population. A 50-year follow-up study. Int J Cardiol 201:173–178
Urtamo A, Jyväkorpi SK, Kautiainen H, Pitkälä KH, Strandberg TE (2020) Major cardiovascular disease (CVD) risk factors in midlife and extreme longevity. Aging Clin Exp Res 32:299–304
Menotti A, Puddu V (1979) Ten-year mortality from coronary heart disease among 172,000 men classified by occupational physical activity. Scand J Work Environ Health 5:100–108
Alberti Fidanza A, Seccareccia F, Torsello S, Fidanza F (1988) Diet of two rural population groups of middle-aged men in Italy. Int J Vit Nutr Res 58:442–451
Menotti A, Puddu PE (2018) Comparison of four dietary scores as determinants of coronary heart disease mortality. Sci Rep 8:15001
Zyczkowska J, Klich-Raczka A, Wizner B, Mossakowska M, Wieczorowska-Tobis K, Grodzicki T (2006) The prevalence of cardiovascular risk factors among centenarians is low risk factors in centenarians. Eur J Cardiovasc Prev Rehabil 13:993–995
Tauchi H, Sato T, Watanabe T (eds) (1999) Medical research for the final stages of human aging: Japanese centenarians. Editorial and Publishing Office of Japanese Centernatians. Aichi Medical University, Aichi, Japan, pp 1–200
Galioto A, Dominguez LJ, Pineo A, Ferlisi A, Putignano E, Belvedere M et al (2008) Cardiovascular risk factors in centenarians. Exp Gerontol 43:106–113
Lescai F, Marchegiani F, Franceschi C (2009) PON1 is a longevity gene: results of a meta-analysis. Ageing Res Rev 8:277–284
Funding
The present investigation received no funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None of the authors report any conflict of interests in relation to this MS and related analyses.
Ethical approval
The initial field examination was held only a few months after the Helsinki Declaration and acceptance from the subjects was implied in participation. All methods were carried out in accordance with relevant guidelines and regulations at the time of the study start, although institutional or licensing committees were not still present in the Country and accordingly were not consulted.
Informed consent
Informed consent was obtained from all subjects during subsequent examinations.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Menotti, A., Puddu, P.E. & Catasta, G. Lifestyle as determinant of all-cause mortality and age at death. A middle-aged male population followed-up 60 years until the survivors were aged 100 years. Aging Clin Exp Res 33, 3091–3098 (2021). https://doi.org/10.1007/s40520-021-01849-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-021-01849-4