
Abstract
Background
Hip fracture is the most clinically devastating and economically important complication of osteoporosis. Pain, suffering, loss of mobility and independence are some of the devastating consequences of hip fractures. The present study aimed to determine the main characteristics and outcomes of patients with osteoporotic hip fracture and treatment gaps at King Abdulaziz Medical City (KAMC), Riyadh, Saudi Arabia.
Methods
This is a single-center, retrospective cohort study analyzing charts of patients > 45 years who were admitted for hip fracture secondary to low-grade trauma from 2008 to 2012.
Results
A total of 264 patients (50.4% males and 49.6% females) were included. The most common fracture types were trochanter (49%) and femoral neck (46%). History of falls was documented in 115 (43.6%) patients. Bone mineral density (BMD) was assessed in only 41 (15.5%) patients. Majority underwent surgery (92%). Surgical complications occurred in 15 (5.7%) patients and medical complications in 21 (7.9%) patients. Vitamin D and calcium were the most common medications, but given only to 45 (17%) patients. Bone mineral density (BMD) assessment was significantly more frequent post-surgery than pre-surgery (p = 0.03). Very few patients received osteoporosis-specific therapy. F ollow-up revealed that 62 (23.5%) patients died 1 year after surgery.
Conclusion
These present findings warrant urgent reassessment of clinical care and treatments provided to patients with osteoporotic hip fractures to prevent recurrent fractures. The introduction of Fracture Liaison Service (FLS) in institutions caring for patients with hip fractures as internationally recommended will definitely change the current status of care.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Osteoporosis is a systemic disorder characterized by decreased bone mass with increased bone fragility resulting in great susceptibility to fractures [1]. It is well known that hip fracture is the most severe and important complication of osteoporosis with physical, psychological and economic impacts especially among aged people. More than 4% of hip fracture patients die during hospitalization [1] and up to one-third die within the first year after their index fracture [2]. Many hip fracture patients lose the ability to live independently and approximately 10% of those who are alive after the first post-fracture year are permanently bedridden [2]. The lifetime prevalence of hip fracture is 18% in women and 6% in men [3].
Estimates indicate that the annual number of osteoporotic hip fractures worldwide will increase from 1.66 million to 6.26 million by 2050 [4]. In Canada, it is expected to reach over 88,000 annually by the year 2041. Apart from the huge financial burden that is created (estimated at $1.3 billion annually in Canada in 1993), there is considerable societal burden [5]. Mortality within the first year after hip fracture ranges from 6 to 44% and was equal to breast cancer mortality in women and twice as high for men. One in four women and one in eight men over the age of 50 years has osteoporosis [3].
Thus, neither the National Osteoporosis Society (NOS) nor the National Osteoporosis Foundation (NOF) advised application of fracture risk assessment tool FRAX for treatment decisions in patients with fragility fracture as opposed to the International Osteoporosis Foundation [6, 7]. The NOF advocates drug treatment in such patients even without the need for bone mineral density (BMD) measurement, except in young postmenopausal women [6]. The UK National Osteoporosis Guideline Group (NOGG) recommended routine BMD measurement in patients aged between 60 and 80 years [8].
It should be emphasized that treatment decisions should not be hampered by the unavailability of dual-energy X-ray absorptiometry (DXA) machines for BMD measurement. A focus on BMD measurement prior to the initiation of anti-osteoporotic treatment in patients with a known history of fracture may result in missed opportunities for treatment. Thus, patients with hip fracture and satisfactory quality of life warrant treatment to prevent future fractures. Unfortunately, the proportion of post-hip fracture patients who are prescribed osteoporosis drugs remains low [4]. In a report from Belgium, just 6% of the previously untreated patients hospitalized for hip fractures were prescribed anti-osteoporotic therapy, with only 41% continuing treatment at 12 months. The median duration of treatment was 40 weeks [9]. Similarly, in a nationwide survey of 53,325 patients admitted with hip fracture to 318 hospitals in the US, only 6.6% were prescribed calcium and vitamin D, and only 7.3% started on anti-resorptive or bone-forming agents [10]. At a national level, it has been estimated that the prevalence of osteoporosis in either spine or femur in the Western region of Saudi Arabia was 44.5% in women and 33.2% in men [2]. A study conducted in the Eastern province of Saudi Arabia estimated that the annual cost of management for osteoporosis-related proximal femoral fractures was $12.78 million in that region alone [11]. It is expected that the number of elderly patients is bound to increase in Saudi Arabia owing to the considerable improvement in life expectancy, with an accompanying increase in all types of fractures. The above economic survey study, despite limitations, still raises serious concerns as to its impact on health care budget.
The present study aimed to determine the main characteristics and outcome of patients with osteoporotic hip fracture at King Abdulaziz Medical City (KAMC), Riyadh, Saudi Arabia as well as to estimate 1-year mortality rate of hip fractures in these patients. This will fill our current knowledge gap as to the care of our post hip fracture patients.
Materials and methods
This is a single-center, retrospective cohort study of randomly selected medical records of Saudi patients admitted with the diagnosis of hip fracture in a major tertiary care center (KAMC, Riyadh, Saudi Arabia). A random sampling technique was used to select participants and data were collected from patient charts and files into specifically designed questionnaire. The questionnaire included relevant data like: demographics, fracture type, severity of trauma, laboratory and radiological work up, medications, post-operative complications and mortality rates. All charts collected were reviewed by the primary author prior to inclusion. Comorbidities such as diabetes mellitus, heart diseases and other conditions were noted, if available in the charts. Inclusion criteria were: Saudi patients, men and women, admitted with osteoporotic hip fracture during the period of 2008–2012, diagnosed with hip fracture secondary to low-impact trauma and patients > 45 years old. Non-Saudis, patients with hip fracture secondary to major trauma, motor vehicle accidents (MVA), pathological hip fracture secondary to cancer, metastases or other metabolic bone diseases and hip fracture in patients with hematological disorders were excluded.
Statistical analysis
Data were entered using MS Excel. Data were verified, recoded and analyzed using IBM-SPSS version 21.0 software. Frequencies were presented in percentages (%). Continuous variables with normal distribution were presented as mean ± standard deviation while non-normal variables were presented as median (interquartile range). Chi square or Fisher’s exact test was used to compare the difference in distribution of frequencies among groups. For continuous variables; independent T test analysis was carried out to compare the means of normally distributed data, while Mann–Whitney U test was calculated to test the median differences of the data that don’t follow normal distribution. A p value < 0.05 was considered significant.
Results
A total of 264 patients’ records [133 (50.4%) males and 131 (49.6%) females] met the inclusion criteria and were included. About two-thirds of the studied cohort were above 70 years. The most common fracture type involved was the trochanter (49.3%), followed by the femur neck (46.2%). History of fall was obtained in 115 (44%) of patients. Majority (99%) of patients had low grade, mild, trauma that led to the fracture (not mentioned in tables).
Table 1 shows the percentages of available information from clinical data, investigations and treatment of the studied sample. Overall, there was poor documentation of many relevant variables. Only 92 (34.9%) out of 264 had information on the smoking status, of whom 11 (12%) were smokers. Likewise, only 32 (31.7%) out of the 101 documented cases had history of steroid use, with the remaining 163 (61.7% overall) cases unknown. 18 (21.4%) out of only 84 documented cases had family history of osteoporosis. 71 (36.6%) out of 194 documented cases underwent X-ray of the lumbar spine. Spinal compression fracture was seen in 15 (25.9%) out of 58 participants. Among the routine Laboratory investigations, less than one-fifth had specific bone related investigations [vitamin D (16.3%) and PTH (18.2%)] and less than half (45.8%) had TSH level done for them. Furthermore, bone mineral density (BMD) was assessed in only 41 (15.5%) of patients, of whom 24 (58.5%) were diagnosed with osteoporosis.
Majority of patients underwent surgery (n = 243, 92%). Surgical complications were noted in 15 (5.7%) of patients and medical complications in 21 (7.9%) of patients. Vitamin D and calcium were the most common specific medications given during hospitalization and/or upon discharge (17%) (Table 1).
Table 2 shows the BMD assessment and results pre- and post-surgery of participants. Only a small number of patients had BMD testing in the pre-surgery period (n = 15, 5.7%), but doubled to 11.4% (n = 30) post-surgery, which is still quite unsatisfactory. Out of the 15 patients with pre-surgery BMD, 8 (53.3%) had osteoporosis, 2 (13.3%) had osteopenia and 5 (33.3%) were normal. Consequently, post-surgery BMD findings indicated that 17 (56.7%) out of 30 had osteoporosis, 10 (33.3%) had osteopenia and only 3 (10%) were normal.
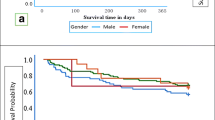
Table 3 illustrates the investigations and treatment received by patients post-surgery in males and females. Males had significantly higher mean 25(OH) vitamin D than females (41.4 nmol/l versus 28.1 nmol/l; p = 0.049). Serum urea was also significantly higher in males than females (p = 0.003) while serum phosphate was significantly higher in females than males (p = 0.03). Likewise, the prevalence of osteoporosis according to BMD testing was significantly higher among females (15.3%) compared with males (3%) (p = 0.001). The rest of the comparisons were not significant (Fig. 1).

Number of patients diagnosed with osteoporosis pre- and post-surgery
Post-operative 1-year follow-up was assessed in Table 4. Majority of charts were lacking documentation of functional ability in the post-operative follow up. Among documented charts, 20% of patients had good mobility with 10% able to walk independent and only 6% reported limitations of movement. With regards to mortality, the total reported deaths were 62 (23.5%) patients after surgery whereas 29 of them (11.1%) died within 1 year after surgery. The trends in total and 1-year case fatality for fractured neck of femur after hospital admission (2009–2015) is shown in Fig. 2. The trends of 1-year deaths decreased till the fifth year while total deaths decreased till the second year and then showed marked increase.

Total number of deaths and those who died within 1 year of surgery between 2009 and 2015
Discussion
Hip fracture is the most devastating complication afflicting patients with osteoporosis worldwide and it represents a significant health and economic burden [1]. It also ranks high among the causes of disability and mortality [4]. The current study was carried out to determine the main characteristics and outcome of patients with osteoporotic hip fracture at a complex medical center in Riyadh, Saudi Arabia.
Unexpectedly, out of 264 patients, 50.4% were males with two-thirds of the studied cohort aged ≥ 70 years. The high proportion of males with hip fracture is surprising and contradicts other population-based studies [12, 13]. Nevertheless, the figures in the present study are consistent with another local study done in 2017 [14]. The most common fracture types involved was the trochanter (49.3%), followed by the femur neck fracture (46.2%). History of fall was present in 44% (n = 115) of patients. Only 4% of patients were smokers (n = 11). Likewise, only 12% of patients had a history of steroid use (n = 32). This was in agreement with a study of hip fracture correlates in elderly which found that current smoker represent 6% of cases and using steroid was found in 9% of patients [15]. Moreover, about one-quarter of the patients had x-ray of lumber spine (n = 71). More than three-quarters underwent basic laboratory investigations (calcium, phosphate, albumin, urea and creatinine). However, less than one-fifth had bone health specific investigations (vitamin D and PTH) and less than half had TSH investigations. BMD was assessed preoperatively in only 15% of patients with approximately 9% of patients diagnosed with osteoporosis before their hip fracture (n = 24). This indicates that osteoporosis was not suspected in the majority of patients before their index fracture. Lack of primary practitioners’ access to specific laboratory tests and BMD could be one reason. This was the finding in KAP study of osteoporosis among PHC physicians in Riyadh, KSA which found that only 13% of the respondents declared that they had access to perform BMD and only one-fifth can ask for relevant biochemical testing for their clients [16]. A study in France on the management of osteoporosis after major fracture in postmenopausal females came up with similar findings [17].
Almost all patients underwent surgery (n = 243, 92%). Surgical complications were noted in 15 (5.7%) patients and medical complications in 21 (7.9%) patients. This was in accordance with a study in China investigating the incidence of medical complications of osteoporotic hip fracture in 2018. The study found that surgical complications were reported in 4% and medical complications in 6–12% [18]. Vitamin D and calcium were the most common medications given (17%) postoperatively and this was comparable to similar studies done in France and Italy [17, 19]. The provision of anti-osteoporosis treatment, including vitamin D and calcium, has been observed to significantly increase following BMD assessment [20]. Although this association was not assessed in the present study, it was nevertheless observed that the rate of BMD testing has significantly doubled postoperatively compared to the preoperative period. This could be explained by the consideration of the presence of osteoporosis because of the low energy nature of the fracture. Follow up by endocrinologists or internists in the 1st postoperative year is another possibility as well, aside from the availability of national guidelines for osteoporosis and post fracture care [21].
Additionally, a study of 221 osteoporotic hip fracture patients with a median follow up of 27.5 months showed 36% reduction in deaths among females and 43% reduction in males who used calcium with vitamin D supplementation. Survival of females who concomitantly used anti-osteoporotic drugs was even greater with 43% reduction in deaths over the entire follow-up period. Excess mortality was highest in females and males who used neither anti-osteoporotic drugs nor prescribed calcium and vitamin D [22]. The same study found that only 8% used specific osteoporosis treatment and 8% used calcium and vitamin D supplementation before their index fracture. During the follow up period, 39% used osteoporosis treatment and 53% used calcium and vitamin D supplementation compared to 25% and 44% at the end of follow up, respectively. Increasing availability of drug treatments over the past 20 years has revolutionized management of patients with osteoporosis. Data with vitamin D treatment suggest that it may reduce risk of fracture by up to 25% [22].
Male patients had significantly higher mean values of calcium and vitamin D (2.4 mmol/l and 41.4 nmol/l) than females (2.2 mmol/l and 28.1 nmol/l). Subclinical vitamin D deficiency is quite common in Saudi Arabia over-all and women in particular due to traditional clothing and deliberate avoidance of sunlight [23], and there is a major need for the diagnosis and treatment of persons with suboptimal vitamin D especially in females. Correlation of vitamin D deficiency to low BMD in Saudi population has been documented [24]. Majority of patients in our study did not receive specific therapy for osteoporosis after admission with hip fracture. This is of great concern since these patients are liable to more subsequent fractures with associated major potential complications in addition to family, societal and financial burdens. This represents a great gap in patient care. The total reported deaths in our study was 62 (23.5%), 29 (11.1%) of whom died within a year post-surgery. This was in agreement with a recent local study done in 2017, with 26.9% overall mortality rate [14]. A study in the US on 1538 patients observed that the mortality rate three months postoperatively was 9.6% [25]. Another US study found that mortality rate at the first month, sixth months and 1 year were 3.2%, 6.5% and 9.7% respectively [26]. In Norway, the mortality rate 1-year post-surgery was 21% for males and 32.5% for females [27]. Likewise, a study in Hong Kong found that mortality rates at 1 month, 6 months and 1 year were 3%, 11% and 17%, respectively while it was 47% at 5 years [28]. Thus, our mortality findings are in close agreement with those from other parts of the world.
However, while our 1-year deaths showed downward trends till the fifth year, the total death rate showed downward trends till the second year and then showed upward trends. This concur with a Swedish study on fracture related mortality between the years 1998–2014 [29]. This finding in our current study goes along with publications which looked at trends and geographical variations of hip fracture mortality over the past 40 years (1959–1998) which support our findings [30]. A recent study which utilized the Danish National Patient Registry involving ≥ 125,000 patients with hip fracture from 1999 to 2012 was also in agreement with our findings [31].
The authors acknowledge several limitations. As is true with retrospective designs, the reliability and accuracy of information derived from chart reviews are difficult to verify. Information on the time course of treatments among those who received pharmacological management were missing and only highlights the poor documentation that needs to be addressed even among major hospitals in KSA. While the findings cannot be generalized, it can still serve as a reference that can be used for comparison to other local and international health institutions. Several factors such as the effect of sex of participants were also not analyzed in the present study.
Conclusion
There is a great gap in fracture care even in one of the best tertiary care centers in Saudi Arabia. Proper post hip fracture assessment and care are lacking, essential laboratory and BMD tests are rarely documented or requested for patients admitted with hip fracture secondary to low-grade trauma at KAMC. Minority of patients received proper osteoporosis treatment after hip fracture. Mortality rate among these patients is quite high but coincide with international figures. Findings warrant reassessment of standards of care provided to these patients. Utilization of clinical pathways or post fracture road map will help to fill the current gap in care. The introduction of Fracture Liaison Service (FLS) in institutions which care for patients with fragility fractures as internationally recommended will definitely change the current status of care. Further studies comparing outcomes of patients who did not undergo surgery are worth investigating.
References
American Academy of Orthopedic Surgeons (AAOS) (1999) Hip fracture in seniors: A call for health system reform. Position Statement 1144. Rosemont, IL
Ardawi M, Maimany A, Bahksh T et al (2005) Bone mineral density of the spine and femur in healthy Saudis. Osteoporosis Int 16:43–55
Gillespie W (2001) Extracts from “clinical evidence”: hip fracture. BMJ 322:986–1075
Sambrook P, Cooper C (2006) Osteoporosis. Lancet 367:2010–2018
Juby A, Geus-Wenceslau C (2002) Evaluation of osteoporosis treatment in seniors after hip fracture. Osteoporos Int 13:205–210
Kanis JA, Cooper C, Rizzoli R et al (2019) Executive summary of European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Aging Clin Exp Res 31:15–17
Kanis JA, Cooper C, Rizzoli R et al (2019) European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int 1:3–44
Compston J, Cooper A, Cooper C, National Osteoporosis Guideline Group (NOGG) et al (2009) Guidelines for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK. Maturitas 62:105–8
Rabenda V, Vanoverloop J, Fabri V et al (2008) Low incidence of anti-osteoporosis treatment after hip fracture. Bone Jt Surg Am 90:2142–2148
Jennings L, Auerbach A, Maselli J et al (2010) Missed opportunities for osteoporosis treatment in patients hospitalized for hip fracture. J Am Geriatr Soc 58:650–657
Bubshait D, Sadat-Ali M (2007) Economic implications of osteoporosis-related femoral fractures in Saudi Arabian society. Calcif Tissue Int 81:455–458
Wei J, Zeng L, Li S et al (2019) Relationship between comorbidities and treatment decision-making in elderly hip fracture patients. Aging Clin Exp Res. https://doi.org/10.1007/s40520-019-01134-5
Abtahi S, Driessen JHM, Vestergaard P et al (2019) Secular trends in major osteoporotic fractures among 50+ adults in Denmark between 1995 and 2010. Osteoporos Int. https://doi.org/10.1007/s00198-019-05109-0
Sadat-Ali M, Alfaraidy M, AlHawas A et al (2017) Morbidity and mortality after fragility hip fracture in a Saudi Arabian population: report from a single center. J Int Med Res 45:1175–1180
Cauley J (2006) Osteoporosis in men: prevalence and investigation. Clin Cornerstone 8:S20–S25
Saeedi M, Al-Amri F, Mohamed A, Ibrahim A (2014) Knowledge, attitude and practice towards osteoporosis among primary health care physicians in Riyadh, Saudi Arabia. Sci J Public Health 2:624–630
Nutz A, Bastide S, Flaisler F et al (2018) AB0986 Management of osteoporosis after major fracture in a cohort of women aged over 50 in a real life setting. Ann Rheum Dis 77:1615
Liu R, Chao A, Wang K et al (2018) Incidence and risk factors of medical complications and direct medical costs after osteoporotic fracture among patients in China. Arch Osteoporos 13:12
Gonnelli S, Caffarelli C, Iolascon G et al (2017) Prescription of anti-osteoporosis medications after hospitalization for hip fracture: a multi-centre Italian survey. Aging Clin Exp Res 29:1031–1037
Wang P, Li Y, Zhuang H et al (2018) Influence of bone densitometry on the anti-osteoporosis treatment after fragility hip fracture. Aging Clin Exp Res. https://doi.org/10.1007/s40520-018-1094-7
Al-Saleh Y, Sulimani R, Sabico S et al (2015) 2015 Guidelines for osteoporosis in Saudi Arabia: recommendations from the Saudi Osteoporosis Society. Ann Saudi Med 35:1–12
Nurmi-Luthje I, Luthje P, Kaukonen J (2009) Post-fracture prescribed calcium and vitamin D supplements alone or, in females, with concomitant anti-osteoporotic drugs is associated with lower mortality in elderly hip fracture patients: a prospective analysis. Drug Aging 26:409–421
Alsuwadia AO, Farag YM, Al Sayyari AA et al (2013) Prevalence of vitamin D deficiency in Saudi adults. Saudi Med J 34:814–818
Sadat-Ali M, Al Elq AH, Al-Turki HA et al (2011) Influence of vitamin D levels on bone mineral density and osteoporosis. Ann Saudi Med 31:602–608
Frisch N, Wessell N, Charters M et al (2018) Hip fracture mortality: differences between intertrochanteric and femoral neck fractures. J Surg Orthop Adv 27:64–71
Boylan M, Riesgo A, Paulino C et al (2018) Mortality following periprosthetic proximal femoral fractures versus native hip fractures. J Bone Jt Surg Am 100:578–585
Riska B, Forsén L, Omsland T et al (2018) Does the association of comorbidity with 1-Year mortality after hip fracture differ according to gender? The Norwegian Epidemiologic Osteoporosis Studies (NOREPOS). J Am Geriatr Soc 66:553–558
Yee D, Fang C, Lau T et al (2017) Seasonal variation in hip fracture mortality. Geriatr Orthop Surg Rehabil 8:49–53
Kiadaliri A, Rosengren B, Englund M (2018) Fracture-related mortality in Southern Sweden: a multiple cause of death analysis, 1998–2014. Injury 49:236–242
Haleem S, Lutchman L, Mayahi R et al (2008) Mortality following hip fracture: trends and geographical variations over the last 40 years. Injury 39:1157–1163
Jantzen C, Madsen C, Lauritzen J et al (2018) Temporal trends in hip fracture incidence, mortality, and morbidity in Denmark from 1999 to 2012. Acta Orthop 89:170–176
Acknowledgements
The authors are thankful for the Researchers Supporting Group (RSP-2019/21) in King Saud University, Riyadh, Saudi Arabia for their assistance.
Funding
The study received no funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethical approval
The study was approved by the Institutional Review Board of King Abdullah International Medical Research Center (KAIMRC), Riyadh, Saudi Arabia (IRB Ref # SP14/055).
Statement of human and animal rights
The authors confirm that procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation.
Informed consent
Not applicable in the present study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Al Saleh, Y., El Seid, M.E., Ruhaiyem, M.E. et al. Characteristics and outcomes of osteoporotic hip fractures: treatment gaps in a tertiary care center in Riyadh, Saudi Arabia. Aging Clin Exp Res 32, 1689–1695 (2020). https://doi.org/10.1007/s40520-019-01377-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-019-01377-2