
Abstract
Aim
The aim of this systematic review was to understand the exergames that can be applied to the pre-frail and frail elderly people, to evaluate whether these games have a positive impact on physical outcomes in pre-frail and frail older adults, and to explore userʼs subjective feelings and compliance.
Methods
PubMed, EMBASE, CINAHL, Web of Science, and the Cochrane Library were searched until January 15, 2019. Only randomized controlled trials published in English for human beings were eligible. The review included studies which examined the effects of exergames on physical outcomes, feasibility and/or subjective feelings of pre-frail and frail older adults. Two researchers assessed the risk bias of all articles independently using the Cochrane collaboration’s tool for assessing risk of bias.
Results
Seven randomized controlled trials with 243 pre-frail and frail older adults met inclusion criteria and were included in this review. Results of the studies were heterogeneous. Physical outcomes (included muscle strength, balance ability, mobility function, gait and falls), subjective feeling outcomes, feasibility, attendance and some other functional outcomes were reported.
Conclusion
Exergames improved balance and mobility function of frail elderly, and it showed a tendency to increase muscle strength when combined with resistance training. As far as the limited evidence was concerned, exergames were feasible and generally accepted by participants.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Frailty is a complex geriatric syndrome resulting from the decline of multiple organ system function characterized by decreasing muscle strength, endurance and physiological function [1]. Senior people in a state of frailty is vulnerable to increase the risk of adverse events such as fall, hospitalization, disability, even dying, when subjected to disturbance of internal and external environment [2, 3], threatening the quality of life of the elderly. As a result, it becomes an important public health concerns and undoubtedly places an additional burden on public health expenditure and caregivers [4]. Therefore, it is urgent to find efficacious, feasible, and economic interventions to prevent or retard frailty to avoid or reduce the adverse events and maintain or improve quality of life of frail older adults [1, 5].
In the past few years, physical exercise, nutritional supplementation, cognitive training and comprehensive interventions in clinical trials in older persons have been repeatedly validated as effective interventions to alleviate frailty, especially physical exercise [2, 6,7,8,9,10]. Exercise has been recommended as an intervention to restore muscle strength and agility to pre-frail older persons, as well as decrease the risk for falling [11, 12]. Theou et al. systematically reviewed the effect of exercise interventions on frailty, the pooled evidence indicated that exercise had a positive impact on some physical determinants and on all functional outcomes [13]. Another systematic review was conducted to evaluate the effectiveness of multi-domain interventions in (pre)frail elderly on frailty, functional, and cognitive status, results showed that these interventions could enhance muscle strength and physical functioning, thereupon then improved frailty status [4]. But at the same time, the study also left question about how to improve the adherence rate. Poor adherence and insufficient exercise intensity could seriously dent the effectiveness of the interventions [14].
Exergame (also known as virtual reality training) is an emerging product used for video games that is also a form of exercise which relies on sensor technologies (cameras, body sensors, and hand held remotes) in such a way that users are required to ‘move’ to fully interact and best experience during the game [15, 16]. Exergame enables players to improve their motor and cognitive functions in the course of performing game tasks [17, 18]. Thus, it has several advantages compared to conventional or other exercises. First, exergame can train balance ability well, especially it has the advantage of providing step training which has been proved to be a powerful strategy to prevent a fall if persons lose their balance [19, 20]. Second, these games are interactive which can attract player’s interest, they also can give real-time immediate performance feedback to the players [19].Therefore, players can adjust their body at any time according to system feedback to control balance, which cannot be achieved by traditional training. Third, the simplicity of the games enables the elderly who are inconvenient to go out to have fun and exercise training at home without loss of medical monitoring which can reduce health system costs [21, 22]. Most importantly, the immersion of exergame makes people devote themselves to the game environment and increase the entertainment of training [23], which might increase adherence of rehabilitation training. In recent years, exergaming technologies have been used as an assessment and treatment tool in rehabilitation of Parkinson’s disease, stroke and other functional impairment diseases [24,25,26,27,28].
Exergame was an acceptable method for improving balance performance as well as functional mobility outcomes in healthy community dwellers [16]. A systematic review [29] was conducted to investigate the effect of Virtual Reality (VR) Training on balance and gait ability in patients with stroke, synthesized evidence showed that VR training was more effective for improving balance or gait ability in patients with stroke compared with balance or gait training without VR. A similar conclusion had been reached in another systematic review which assessed the effects of wii-based games on the balance function of independently functioning older adults [30]. However, there is no systematic review of the effect of exergame on the frail elderly, and it is not clear whether exergame is feasible and bring positive effect to frail elderly. Therefore, the purpose of this study is to:
-
1.
Preliminarily evaluate whether exergame has a positive impact on physical outcomes in the pre-frail and/or frail elderly.
-
2.
Explore userʼs subjective feeling and compliance.
Method
The review was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Search strategy
An electronic literature search was conducted in PubMed, EMBASE, CINAHL, Web of Science, and the Cochrane Library from inception of the database until January 15, 2019. The literature search was limited to articles published in English, and excluded animal experiments. We also manually retrieved the references, citations and other relevant articles of the authors from the first search to guarantee the comprehensiveness of retrieval. Selected search terms (free term and subject term if possible) were combined with Boolean conjunction (OR/AND) and applied on three steps. Details were shown in Table 1.
Eligibility criteria
Full-text articles published in a peer-reviewed journal were eligible. The inclusion criteria that the eligible studies had to meet are as follows:
Types of participants | The subjects were frail or/and pre-frail elderly people aged ≥ 65 years without neurological, orthopedic, cardiac conditions and/or other chronic diseases. Classification in terms of frail status should be according to an operationalized definition |
Types of interventions | Intervention was exergame which was defined as a term used for video games and was also a form of exercise that relied on technology that tracked body movement or reaction. The exergame device could be commercial off-the-shelf or self-designed program |
Types of outcomes | The study was required to report physical outcomes and/or subjective feelings of users as the primary or secondary outcome |
Types of study | Randomized controlled trails with pre-post testing were eligible with at least one control group that either did not receive any intervention and/or received a traditional intervention |
Study selection and data extraction
Identification of potentially relevant papers based on title and abstract was conducted by two reviewers independently. Afterwards, preliminary eligible articles were downloaded and to be read full text according to the inclusion criteria. If divergences arose during the screening process, they negotiated with each other, and if they were still unable to deal with, the third reviewer resolved the discrepancy and made the final decision. Data extraction was also done by two independent researchers following a unified form. The extracted information included author and year, country, study design, participants (included frailty status, gender and age), sample size, frailty diagnostic tool and details of interventions (included duration and frequency, interventions of experimental group and control group, outcome measures, results and exergame devices). The manner to deal with differences was the same as above.
Quality assessment
The methodological quality assessment of the included randomized controlled trials was accomplished by two researchers in accordance with the Cochrane collaborationʼs tool for assessing risk of bias which included six criteria: selection bias, performance bias, detection bias, attrition bias, reporting bias and other bias. The risk of each item was evaluated as low, high, and unclear.
Results
Study selection
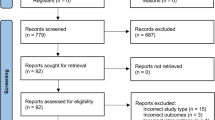
A total of 362 articles were included through electronic and manual retrieval through five biomedical databases. Among them 84 articles were deleted by eliminating duplication, and 278 articles were identified for the titles and abstracts screening. Then, 20 full-text articles were remained to be assessed according to the prespecified eligibility criteria. One study was close to our inclusion criteria, but was eventually excluded after repeated finalization due to the inaccurate inclusion criteria for the frailty [31]. Finally, 7 articles with 243 participants met the inclusion criteria to be qualitative synthesis [32,33,34,35,36,37,38]. The specific process is shown in Fig. 1.

Flow diagram of literature search
Study characteristics
The characteristics of the studies are shown in Table 2. Three studies were conducted in Europe [34, 37, 38], three in America [32, 33, 36] and one in Hong Kong, China [35]. All studies had a randomized controlled trial design published from 2010 to 2019. Studies included only frail [34, 35, 37, 38], only pre-frail [32, 36], or both pre-frail and frail phenotype [33]. One study involved only women [32]. The average age ranged from 69.5 to 85.47 [32, 34]. The studies ranged in sample size from 20 to 60 [32, 35]. Four studies used Fried phenotype to define frailty [32, 33, 36, 38], the remaining three studies used were Short Physical Performance Battery (SPPB) [34], Functional Ambulator Category (FAC) [35], and Dynamic Gait Index score (DGI) [37] separately.
Quality of studies
The risk of bias was assessed by the Cochrane collaboration’s tool for assessing risk of bias. The specific results are shown in Fig. 2. In terms of selection bias, one study failed to report the process of randomization [36], most studies on allocation concealment were not clear [32, 34,35,36]. Only one study clearly illustrated the blind method [33]. Blinding participants in the type of intervention was impossible, because they were always involved in the intervention. The outcome data of the studies were reported in all studies. In one study, it was difficult to determine whether there were other biases due to insufficient information about the process involved in the experiment [36].

Quality of included studies
Outcomes
Interventions against frailty
Interventions implemented in the studies were in high heterogeneity as shown in Table 2. The duration of the intervention varied between 2 weeks to 15 weeks [33, 36]. The frequency of the training sessions was two sessions per week [33, 37] and three sessions per week [32, 34,35,36]. Each session lasts from 20 to 90 min. All trainings were collective and supervised, three studies reported the setting [33,34,35], the rest was not mentioned. Six studies consisted of two groups [32,33,34,35, 37, 38], and the other was divided into three groups [36]. The X-box 360 [32], Nintendo Wii [33, 35, 36], Fovea Interactive® [38], the system manufactured by Personics, Denmark [37] and a self-developed equipment named FRED game [34] were used to conducted interventions.
Physical outcomes
Muscle strength
Exergames were usually combined with (progressive) resistance muscle strength training to enhance muscle strength. Two studies in the review reported muscle strength outcomes using different measurements. In the study of Santos [32], muscle strength was one of the primary outcomes which was measured by the peak torque, average power and total work around the ankle and knee joints at both 60°/s and 180°/s. The results showed that both moderate exercise intensity group (MG) and vigorous exercise intensity group (VG) improved most indicators of muscle strength from pre- to post-training, and MG presented greater average power than VG for knee extensor (20%) and flexor muscles (23%) (p < 0.039). There was main time effect of peak torque at 180°/s for knee ex tensor, flexor and plantiflexor muscles as well as average power and work on the knee flexor muscles (p < 0.046). In another study by Hagedorn and Holm [37], knee extension and ankle dorsiflexion were assessed to evaluate changes in muscle strength. After 12-week exercise, the muscle forces of both two groups were significantly improved after the exercise than before, especially the knee extension of the exergame group (p < 0.001).
Balance and mobility functions
After exergame balance training, the frail elderly improved balance, and mobility functions. Sit to Stand (STS), Time Up and Go test (TUG), Mini-Balance Evaluation Systems Test (Mini-BESTest), and Berg Balance Scale (BBS) were commonly used to test balanced capacity. Walking test was measured to evaluate gait speed. In the study of Santos [32], after 12 weeks training, only TUG performance significantly improved (p < 0.001) in MG, among the outcomes of TUG, STS and 10 m Walk test. In addition, there was main time effect for the speed during the 10 m-Walk test (p < 0.003) after two-way mixed model ANOVA. But in study of Hagedorn and Holm [37], the TUG test showed no training increased improvement in two groups, and the STS outcome was improved in the traditional balance training group (TB), while the exergame group showed significant improvement in 6-min walk test from 298 to 333 m (p < 0.05). There was no significant improvement in other balance and gait test results, such as one-legged balance, BBS, tandem test, and Dynamic Gait Index score between the two groups. Only one item (eyes closed, foam mat) of modified clinical test of sensory interaction and balance (MCTSIB) showed significant improvement in TB (p < 0.05). Another study [33] used balance function and gait as secondary outcomes. Significant improvement was seen on the Mini-BESTest and FGA in the EG compared with the CG (p < 0.05). Short Physical Performance Battery (SPPB) is a comprehensive measurement of physical function by measuring strength, dynamic balance and mobility function. In Mugueta-Aguinaga’s study [34], after nine physical activity sessions using the FRED game for 3 weeks, it was noted that the results from the study group increased whereas those from the control group decreased in SPPB scores. Another comprehensive measurement tool named Senior Fitness Test (SFT) including chair stands, time up and go, arm curls, sit and reach, steps, back scratch, and 6-min walk was used in Daniel’s study [36], and there was improvement on several of the measures of SFT containing chair stands, arm curls, steps, 6-min walk, sit and reach, and the time up and go. One study was conducted by Kubicki [38] to explore the effects of a two-dimensional virtual reality game program on the rapid arm movement and posture control of the frail older adults by assessing the hand kinematics and centre-of-pressure (CoP) displacement parameters of pre- and post-training. After training, hand movement time in the experimental group was significantly shorter than that before the training (before 1.95 ± 0.68 s, after 1.34 ± 0.47 s). The CoP mean velocity in the experimental group was significantly higher than that before the training (before 0.024 ± 0.01 m s−1, after 0.031 ± 0.022 m s−1).
Falls
Four studies of the review reported falls-related results. The Fall Efficacy Scale-International (FES-I) and Activities-Specific Balance Confidence Scale (ABC) were usually used to assess the degree of fear of falling. There was no significant effect on FES-I in study of Gomes [33]. In the pilot study after 12 weeks balance training [37], the scores of the FES-I in both groups decreased, but there was no statistical significance. Similarly, another study [36] also showed that there was no significant difference between the changes of ABC before and after Wii Fit balance training (p = 0.3). One study [35] compared Wii Fit training and conventional balance training with Physical Profile Assessment (PPA) and the fall incidence as the primary outcomes. The results showed that Physical Profile Assessment (PPA) scores improved and fall incidence decreased significantly in both groups after the intervention, but the subjects in the Wii Fit training group showed significantly greater improvement in both outcome measures (p < 0.01).
Subjective feeling outcomes
Two studies conducted questionnaires on experience feelings of users. One study [33] applied a game satisfaction questionnaire that consists of 17 questions divided into five domains (perception of the games, motivation, protocol, safety, the perception of the training). 100% participants thought the Nintendo Wii Fit Plus™ games were very good and safety, and 83% answered that games were very motivated. Talking about the arrangement of the game, 74.7% participants said that the number of attempts was suitable, but the intervention time could have more sessions (58.1%). Majority of participants understood and enjoyed the tasks of the games, and were willing to continue practicing as a form of exercise and recommend it to others. In another study [32], they used Feeling Scale to assess the average of affective responses of subjects when playing exergames. This scale was composed of life enhancement, physical performance, tasks, pleasure and health prevention subscales, when examining the perceived benefit at post-training period for the groups exercising at moderate and vigorous intensities, positive affect and pleasure were reported only when subjects in moderate exercise intensity group (p = 0.028).
Feasibility and attendance
Feasibility was assessed through participants’ performance in the games, measured by the score participants achieved. Two studies reported game scores. In one study in which participants played 10 Nintendo Wii Fit Plus games, participants improved their scores in all 10 games (p < 0.05), and presented few adverse events during the practice [33]. In study using self-developed games FRED [34], the minimum increase was from 6 to 7, and 60% of subjects from the study group obtained a score of ≥ 10 points at the end of the study. The minimum increase was from 6 to 7. The degree of compliance with and adherence to the game were confirmed by 100% attendance of the sessions. In another study, twenty-three participants were recruited but only 21 completed, because two participants dropped from the control group due to personal crises unrelated to the study [36].
Discussion
It was obvious that there was notable incongruousness in the outcome measures used within the included studies, so that it was not possible to conduct a meta-analysis, but to sum up the existing evidence in the form of a total. This review summarized the effects of several different forms of exergames on the functional outcomes in the pre-frail and/or frail elderly, and explored the feasibility, acceptance and participants’ compliance of exergaming training. We found that exergames played an active role in improving the balance and functional mobility outcomes of frail older adults comparing with traditional physical activity training or with daily activities. Additionally, there was a tendency to increase muscle strength by combining exergames with resistance training. Although only seven original articles were included, this study had certain predictability and prospects for future research.
The most discussed indicators were balance and mobility function, which was consistent with the original intention of game design [16]. A total of five studies [32,33,34, 36, 37] involved 137 participants with balance and mobility function as outcome measures were included in our review. In summary, all evidence from the results came together to show a positive effect. Previous studies had explored and reviewed the effects of similar interventions on balance and mobility function in healthy older or patients with other functional impairments [16, 39, 40], mainly concentrated in the past 5 years. The studies included in these reviews were not exactly the same in terms of interventions (e.g., virtual reality interventions include Nintendo Wii™ games, or some other exergames), control interventions (no treatment, standard training, or other alternative exercise-based training), subjects (from young to old in a state of health or balance function damaged) and duration (from 2 weeks to 20 weeks) and frequency of exercises (from 1 session per week to 5 sessions per week), the length of each session varied from 10 to 60 min. Moreover, the results of these studies were inconsistent. One systematic review [39] evaluated the effect of Nintendo Wii™ exergames on older adults with chronic disease. The conclusion was that the Wii exergames were safe and feasible to encourage older adults with chronic disease to take part in exercise with the potential to improve physical function, cognition, and psychosocial outcomes. Similar results were found by Vicky Booth et al. [40] when valuated whether virtual reality interventions were effective at improving balance in adults with impaired balance. But no significant difference was found from the pooled results. This may be because the study included a wide range of subjects including patients aged 16 years and older with impaired balance function, different groups of people may have different responses to exergames, which may offset some of the effects when pooling the results, while subjects of this review were relatively consistent, and the results of our study could not be merged, but could only draw a relatively exergame-favored conclusion on the whole. Another meta-analytical review [16] examined the effects of virtual reality training (VRT) on fall-risk relevant balance performance and functional mobility in healthy seniors compared to alternative balance training programs (VT) and inactive control condition (CON). They found that VRT could be employed to improve balance performance and functional mobility in healthy community dwellers. On the contrary, meta-analyses revealed that the VRT was slightly less effective than VT. Sensitivity analysis indicated that the overall effect was attributed to the lower quality of several articles. However, it was well accepted, perhaps it could be used as a supplementary method of training for the elderly owing to its attraction.
According to the recommendation from the American College of Sports Medicine and the American Heart Association [41], the elderly should participate in intensive muscle training at least twice a week to maintain their health and independence. So, in addition to the balance function frequently studied, the maintenance of muscle strength is particularly important for the elderly, especially the frailty elderly. Two studies involved progressive resistance muscle strength training [32, 37]. After exergaming training, both studies found that muscle strength of the subjects in experimental groups increased significantly compared to pre-treatment. Four studies measured gait speed as primary or secondary outcome [32, 34, 36, 37], and two of them showed that exergames had positive effects on gait of the frail elderly [36, 37]. One study improved the SPPB scores which included gait speed test, balance test and chair stand test, but it was unclear whether the gait speed had improved among the three tests [34]. Furthermore, the commonly used definition of frailty is the criterion of Fried, which consists of weight loss, weakness, exhaustion, slow gait, and low physical [3, 42]. Among the five diagnostic indicators of frailty, the effectiveness of exergames in other items besides muscle strength (weakness) and gait remains to be tested.
Frail constitution is the main factor for disability, especially easily caused by falls. Prevention of falls in the elderly can reduce the occurrence of adverse consequences, such as disability and long-term bedridden. Conventional strength, endurance and balance training have been shown to be efficacious in reducing the incidence of falls in the frail elderly [43]. Four articles included in this study investigated the effects of exergames on the occurrence of falls and fear of falling [33, 35,36,37], one obtained significant positive results in fall occurrence [35], and one mentioned a reduction in falls, but no specific data were available [37]. The remaining two articles [33, 36] only investigated the participants’ psychology and degree of fear of falling, and did not report the incidence of falling. Moreover, the probability of falling during a short training period was not very high, thus may not get satisfactory results. The effect of exergames on falls of the frail elderly remains to be further examined.
It was mentioned in Lenore Dedeyne’s review [4] that for the frail elderly, the optimal exercise frequency was at least three times a week with 30–45 min each session, lasting at least 5 months. However, in the including studies of this review, the duration varied from 2 weeks to 15 weeks, all less than 5 months, but the frequency of exercise and the length of each session were more appropriate. Only one study conducted a follow-up study on the physical outcome, and the significant effect on balance function had been maintained at 30 days after stopping the intervention, but the persistent effect of other studies was not clear.
Exergame had been shown feasible and safe in healthy older adults, and other patients with chronic disease [39, 44], which was in agreement with the results of our study. We also found that exergames were acceptable and feasible in improving the functional outcomes of the frail elderly. But before definitive conclusions can be drawn, more research is needed to prove its efficacy and safety [45].
At the same time, we found that with the development of the severe aging situation, experts in this field paid much more attention to the management of frailty. Protocols of exergaming interventions for the frail elderly were gradually emerging in recent years, besides the including studies of our review. Vojciechowski et al. [46] drafted a protocol that verified the effect of exergames on musculoskeletal function, nutritional status, and risk of falls in pre-frail older women compared with no training, routine physical training and exergames with isoenergetic supplementation. The primary outcomes would be muscle strength and architecture,body composition, functional mobility and risk of falls. Another protocol published on the U.S. National Library of Medicine in 2015 aimed to investigate the effectiveness of exergames associated with conventional physiotherapy in physical functioning in frail elderly compared to conventional physiotherapy with the SPPB, walking speed test, and Four Step Square Test as primary outcome measures. The study would last 12 weeks. The results of the above studies will give us a better understanding of the effect of exergames in the frailty elderly based on the known evidence in now, and provide guidance for the prevention, management and treatment of frailty.
Exergames are increasingly being used to compare with other interventions exploring their effects on some functional outcomes, especially balance function of the elderly. It is worth considering that, although the results of the randomized controlled trials showed the comparable or slightly better effects of exergame than other interventions, we lack evidence on its potential of improving the functional status of the elderly, as well as the motion characteristics induced by exergame, which makes it difficult to explain the results of intervent studies and to draw conclusions about the effectiveness of exergame on exercising and improving specific functions. Moreover, few of these games are designed specifically for the elderly, and fewer are designed specially for the rehabilitation training of the elderly. Therefore, it may not be negligible to explore how to design a game specially designed for the rehabilitation of the elderly and to explore the specific effects of exergames on them. As a result, it may not be enough to compare the effects of exergames only in randomized controlled trials for developers, as far as this goal is concerned. To inform exergame design for movement quality, Skjaeret et al. conducted an observational study to explore game elements (physical space, graphics and sound, game mechanism, etc.) and the movement characteristics (weight shift, step length, etc.) of the elderly when playing stepping exergame [47]. Results showed that different game elements might help stimulate specific motion characteristics, which was conducive to design for movement quality in exergames.
This review has the following limitations. First, only seven studies met the criteria and were included in this review. The limited number of articles limited the strength of the evidence, which made it difficult to draw definite conclusions and lead to a poor interpretation of the findings. Second, inclusive researches were heterogeneous in exergaming interventions (different in game settings, frequency and duration). As a result, the optimal intervention design to achieve the most obvious intervention effect was not yet clear. Third, there were some limitations in the outcomes of this systematic review. Although studies used the same indicators as their outcomes, the measurement tools were different, which made it impossible to amalgamate the result data for meta-analysis.
The limited systematic review preliminarily verified the potential impact of exergames on the frail elderly. Further studies should pay more attention on the following points. First, it is better to combine exergames with resistance training, especially progressive resistance muscle strength training, to enhance the balance and mobility function of the frailty elderly as well as improve muscle strength at the same time. Second is in the premise of ensuring the safety of the participants, to explore the optimum design scheme (duration, frequency, intensity, game type etc.) through which one can get the strongest intervention effect. Third, there is insufficient evidence about the effects of exergames on the fear of falling, cognitive function and mood-related outcomes of the frail elderly in this review, future studies could appropriately conduct the measurement of these indicators. Fourth, since frailty is caused by the decline in the function of the multiple organs, the health status of frail elderly is slightly worse in other areas, such as nutriture, than that of the healthy elderly or those with impaired balance function, interventions should therefore be multidisciplinary [4]. Future researches could try to combine exergames with interventions in other domain (e.g., nutrient supply) to explore whether it will get better effects. The last but not the least, more observational studies are needed to explore the relationship between different game elements and movement characteristics to design appropriate rehabilitation exergames for the elderly.
Conclusion
Exergames can be combined with progressive resistance muscle strength training to increase muscle strength for frail adults. In addition, participants can improve their balance and mobility function by participating in complex and dynamic human–computer interactive game tasks. In terms of game performance, exergames are feasible, and given the interaction and interest of the virtual game, it is universally recognized and acceptable for frail elderly. But effects of exergames on fear of falling, cognitive function, mood-related outcomes and other physical, psychological and social outcomes of frail elderly are not clear because of the limited studies. So far, there is limited evidence on the role of exergames in the treatment of frail elderly people. Therefore, more studies with more rigorous design are needed to enrich the data and evidence in this field, and the effectiveness on the unclear outcomes are waiting for further exploration.
References
Walston J, Hadley EC, Ferrucci L et al (2006) Research agenda for frailty in older adults: toward a better understanding of physiology and etiology: summary from the American Geriatrics Society/National Institute on Aging Research Conference on Frailty in Older Adults. J Am Geriatr Soc 54:991–1001
Ng TP, Feng L, Nyunt MS et al (2015) Nutritional, physical, cognitive, and combination interventions and frailty reversal among older adults: a randomized controlled trial. Am J Med 128:1225–1236.e1
Fried LP, Tangen CM, Walston J et al (2001) Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci 56:M146–M156
Dedeyne L, Deschodt M, Verschueren S et al (2017) Effects of multi-domain interventions in (pre)frail elderly on frailty, functional, and cognitive status: a systematic review. Clin Interv Aging 12:873–896
Rizzoli R, Reginster JY, Arnal JF et al (2013) Quality of life in sarcopenia and frailty. Calcif Tissue Int 93:101–120
Cesari M, Vellas B, Hsu FC et al (2015) A physical activity intervention to treat the frailty syndrome in older persons-results from the LIFE-P study. J Gerontol A Biol Sci Med Sci 70:216–222
Chan DC, Tsou HH, Yang RS et al (2012) A pilot randomized controlled trial to improve geriatric frailty. BMC Geriatr 12:58
Wolf SL, O’Grady M, Easley KA et al (2006) The influence of intense Tai Chi training on physical performance and hemodynamic outcomes in transitionally frail, older adults. J Gerontol A Biol Sci Med Sci 61:184–189
Rosendahl E, Lindelof N, Littbrand H et al (2006) High-intensity functional exercise program and proteinenriched energy supplement for older persons dependent in activities of daily living: a randomised controlled trial. Aus J Physiother 52:105–113
de Jong N, Chin APMJ, de Graaf C et al (2000) Effect of dietary supplements and physical exercise on sensory perception, appetite, dietary intake and body weight in frail elderly subjects. Br J Nutr 83:605–613
Elley CR, Robertson MC, Garrett S et al (2008) Effectiveness of a falls-and-fracture nurse coordinator to reduce falls: a randomized, controlled trial of at-risk older adults. J Am Geriatr Soc 56:1383–1389
Faber MJ, Bosscher RJ, Chin APMJ et al (2006) Effects of exercise programs on falls and mobility in frail and pre-frail older adults: A multicenter randomized controlled trial. Arch Phys Med Rehabil 87:885–896
Theou O, Stathokostas L, Roland KP et al (2011) The effectiveness of exercise interventions for the management of frailty: a systematic review. J Aging Res 2011:569194
Sohng KY, Moon JS, Song HH et al (2003) Fall prevention exercise program for fall risk factor reduction of the community-dwelling elderly in Korea. Yonsei Med J 44:883–891
Benzing V, Schmidt M (2018) Exergaming for children and adolescents: strengths, weaknesses, opportunities and threats. J Clin Med 7:422
Donath L, Rossler R, Faude O (2016) Effects of virtual reality training (exergaming) compared to alternative exercise training and passive control on standing balance and functional mobility in healthy community-dwelling seniors: a meta-analytical review. Sports Med 46:1293–1309
van Diest M, Lamoth CJ, Stegenga J et al (2013) Exergaming for balance training of elderly: state of the art and future developments. J Neuroeng Rehabil 10:101
Skjaeret N, Nawaz A, Morat T et al (2016) Exercise and rehabilitation delivered through exergames in older adults: an integrative review of technologies, safety and efficacy. Int J Med Inform 85:1–16
Okubo Y, Schoene D, Lord SR (2017) Step training improves reaction time, gait and balance and reduces falls in older people: a systematic review and meta-analysis. Br J Sports Med 51:586–593
Skjaeret-Maroni N, Vonstad EK, Ihlen EA et al (2016) Exergaming in older adults: movement characteristics while playing stepping games. Front Psychol 7:964
Eckert M, Gomez-Martinho I, Meneses J et al (2017) New approaches to exciting exergame-experiences for people with motor function impairments. Sensors (Basel) 17:354
Choi SD, Guo L, Kang D et al (2017) Exergame technology and interactive interventions for elderly fall prevention: a systematic literature review. Appl Ergon 65:570–581
Jin SA (2009) Avatars mirroring the actual self versus projecting the ideal self: the effects of self-priming on interactivity and immersion in an exergame, Wii Fit. Cyberpsychol Behav 12:761–765
Ribas CG, Alves da Silva L, Correa MR et al (2017) Effectiveness of exergaming in improving functional balance, fatigue and quality of life in Parkinson’s disease: a pilot randomized controlled trial. Parkinsonism Relat Disord 38:13–18
Hung JW, Chou CX, Chang HF et al (2017) Cognitive effects of weight-shifting controlled exergames in patients with chronic stroke: a pilot randomized comparison trial. Eur J Phys Rehabil Med 53:694–702
Shih MC, Wang RY, Cheng SJ et al (2016) Effects of a balance-based exergaming intervention using the Kinect sensor on posture stability in individuals with Parkinson’s disease: a single-blinded randomized controlled trial. J Neuroeng Rehabil 13:78
Hung JW, Chou CX, Hsieh YW et al (2014) Randomized comparison trial of balance training by using exergaming and conventional weight-shift therapy in patients with chronic stroke. Arch Phys Med Rehabil 95:1629–1637
Taylor L, Kerse N, Klenk J et al (2018) Exergames to improve the mobility of long-term care residents: a cluster randomized controlled trial. Games Health J 7:37–42
de Rooij IJ, van de Port IG, Meijer JG (2016) Effect of virtual reality training on balance and gait ability in patients with stroke: systematic review and meta-analysis. Phys Ther 96:1905–1918
Laufer Y, Dar G, Kodesh E (2014) Does a Wii-based exercise program enhance balance control of independently functioning older adults? A systematic review. Clin Interv Aging 9:1803–1813
Szturm T, Betker AL, Moussavi Z et al (2011) Effects of an interactive computer game exercise regimen on balance impairment in frail community-dwelling older adults: a randomized controlled trial. Phys Ther 91:1449–1462
Santos GOR, Wolf R, Silva MM et al (2019) Does exercise intensity increment in exergame promote changes in strength, functional capacity and perceptual parameters in pre-frail older women? A randomized controlled trial. Exp Gerontol 116:25–30
Vieira Gomes GC, Simoes MdS, Lin SM et al (2018) Feasibility, safety, acceptability, and functional outcomes of playing Nintendo Wii Fit Plus (TM) for frail older adults: a randomized feasibility clinical trial. Maturitas 118:20–28
Mugueta-Aguinaga I, Garcia-Zapirain B (2017) FRED: exergame to prevent dependence and functional deterioration associated with ageing. A pilot three-week randomized controlled clinical trial. Int J Environ Res Public Health 14:1439
Fu AS, Gao KL, Tung AK et al (2015) Effectiveness of exergaming training in reducing risk and incidence of falls in frail older adults with a history of falls. Arch Phys Med Rehabil 96:2096–2102
Daniel K (2012) Wii-hab for pre-frail older adults. Rehabil Nurs 37:195–201
Hagedorn DK, Holm E (2010) Effects of traditional physical training and visual computer feedback training in frail elderly patients. A randomized intervention study. Eur J Phys Rehabil Med 46:159–168
Kubicki A, Bonnetblanc F, Petrement G et al (2014) Motor-prediction improvements after virtual rehabilitation in geriatrics: frail patients reveal different learning curves for movement and postural control. Neurophysiol Clin 44:109–118
Chao YY, Scherer YK, Montgomery CA (2015) Effects of using Nintendo Wii exergames in older adults: a review of the literature. J Aging Health 27:379–402
Booth V, Masud T, Connell L et al (2014) The effectiveness of virtual reality interventions in improving balance in adults with impaired balance compared with standard or no treatment: a systematic review and meta-analysis. Clin Rehabil 28:419–431
Nelson ME, Rejeski WJ, Blair SN et al (2007) Physical activity and public health in older adults: recommendation from the American College of Sports Medicine and the American Heart Association. Med Sci Sports Exerc 39:1435–1445
Sternberg SA, Wershof Schwartz A, Karunananthan S et al (2011) The identification of frailty: a systematic literature review. J Am Geriatr Soc 59:2129–2138
Cadore EL, Rodriguez-Manas L, Sinclair A et al (2013) Effects of different exercise interventions on risk of falls, gait ability, and balance in physically frail older adults: a systematic review. Rejuvenation Res 16:105–114
Barry G, Galna B, Rochester L (2014) The role of exergaming in Parkinson’s disease rehabilitation: a systematic review of the evidence. J Neuroeng Rehabil 11:33
Mat Rosly M, Mat Rosly H, Davis Oam GM et al (2017) Exergaming for individuals with neurological disability: a systematic review. Disabil Rehabil 39:727–735
Vojciechowski AS, Biesek S, Melo Filho J et al (2018) Effects of physical training with the Nintendo Wii Fit Plus. Maturitas 111:53–60
Skjaeret N, Nawaz A, Ystmark K et al (2015) Designing for movement quality in exergames: lessons learned from observing senior citizens playing stepping games. Gerontology 61:186–194
Funding
Funding received from the 13th Five-Year Plan science and technology research project of the Education Department of Jilin Province (JJKH20190006KJ) and the industrial technology research and development project of the Development and Reform Commission of Jilin Province (2019C047-4).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest.
Statement of human and animals rights
This review reports no participant data or original research findings that require ethics approval.
Informed consent
For this type of study, formal consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Zheng, L., Li, G., Wang, X. et al. Effect of exergames on physical outcomes in frail elderly: a systematic review. Aging Clin Exp Res 32, 2187–2200 (2020). https://doi.org/10.1007/s40520-019-01344-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-019-01344-x