
Abstract
Background
To improve physical function, physical activity (PA) guidelines for older adults recommend completing PA in bouts of 10 min or more. Spontaneous PA (< 10 min) can also benefit older adults. However, a paucity of research exists examining if shorter bouts of PA are associated with greater physical function.
Aim
To determine the association between various patterns of PA and the likelihood of greater physical function in older adults.
Methods
Older adults from the 2003–2004 and 2005–2006 cycles of the National Health and Nutrition Examination Survey were included for analysis. PA lasting 1, 5, 10, 30, and 60 min was quantified using accelerometers. Physical function was assessed using a Likert scale reflecting the self-reported capability to complete 11 tasks. A single function score was then computed using factor analysis. Logistic regression analyses calculated the association between PA bout length and the likelihood of above average function.
Results
PA performed in 1-min (odds ratio [OR] 1.02; 95% confidence interval [CI] 1.01–1.03), 5-min (OR 1.02; CI 1.01–1.03), or 10-min bouts (OR 1.02; CI 1.01–1.03) was associated with greater physical function following adjustment for confounders. When scaled to represent an accumulation of 10 min of MVPA, likelihoods increased for both 1-min ([OR] 1.25; 95% [CI] 1.11–1.39) and 5-min (OR 1.22; 95% CI 1.08–1.37) bouts.
Discussion/conclusions
Our findings suggest bouts of PA lasting 10 min or shorter in duration are associated with greater physical function in older adults.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Reduced physical function correlates with detrimental long-term health outcomes, and may progress into a loss of independence as one ages [1,2,3]. The costs associated with caring for older adults with reduced physical function, or who have lost independence, are tremendously high [4]. As such, strategies targeted at maintaining physical function in older adults are necessary.
Engaging in regular physical activity preserves, and can potentially improve, physical function in older adults [1,2,3, 5]. To obtain health benefits and improve function, the World Health Organization currently recommends older adults should partake in at least 150 min of moderate to vigorous physical activity (MVPA) per week, in bouts of 10 min or more [6]. However, the vast majority of older adults do not meet these recommendations [8,9,10]. The United States of America recently updated their physical activity guidelines, and no longer require the accumulation of MVPA in bouts of 10 min or more [11]. This represents a significant transition from previous (older) guidelines, as this update seemingly recognizes the potential benefits associated with various patterns of physical activity, including the accumulation of spontaneous bouts (< 10 min in duration) of MVPA. Specifically pertaining to older adults, the accumulation of spontaneous bouts of MVPA has been associated with reduced levels of frailty [12] and lower all-cause mortality risk [13], suggesting the overall volume of MVPA may matter more than the pattern of accumulation. Based on these findings, accumulating spontaneous bouts of MVPA may be a sufficient method for maintaining physical function as one ages. However, the association between spontaneous MVPA and the physical function of older adults is currently unknown.
Reduced physical function in older adults may be further catalysed by extraneous sedentary behaviour [5], a troubling sentiment considering older adults are the most sedentary cohort of the population [14]. Regularly breaking up bouts of sedentary behaviour may represent a viable method for mitigating the detrimental impact of sedentary behaviour on physical function [15]. However, research investigating the relationship between sedentary behaviour and physical function in older adults is limited and requires further investigation [16].
Identifying how various patterns of MVPA and sedentary behaviour influence physical function in older adults could provide further support for the benefits associated with accumulating spontaneous MVPA. Accordingly, the purpose of this study was to determine the association between various patterns of MVPA and sedentary behaviour with physical function in older adults. It was hypothesized that MVPA accumulated in bouts shorter than 10 min would be associated with higher physical function in older adults. Similarly, it was hypothesized that longer bouts of sedentary behaviour would be associated with lower physical function in older adults.
Methods
Participants
This cross-sectional analysis used data from the 2003–2004 and 2005–2006 cycles of the National Health and Nutrition Examination Survey (NHANES). These cycles were selected as they include accelerometer data and self-reported physical function assessments. NHANES is a nation-wide survey conducted throughout the United States of America, providing a sample representative of the American population aged up to 85 years. Analyses were restricted to participants age 65 and older, who completed the steps necessary to compute the primary outcome measure (physical function) and the primary exposure variables (physical activity and sedentary), as well as those who provided interpretable responses to the 11 selected indicators of physical function (see section titled “Physical function assessment”). All participants in NHANES provide informed consent, as approved by the Institutional Review Board of the Centers for Disease Control and Prevention.
General characteristics
In line with NHANES protocols, trained personnel conducted at home interviews to gather demographic, socioeconomic, education, and health information from all participants. As part of this process, participants were asked if they had ever been informed by a doctor that they had asthma, arthritis, heart failure, coronary heart disease, angina, myocardial infarction, stroke, emphysema, chronic bronchitis, any liver condition, or cancer. The total number of ‘yes’ responses were summed to compute the number of chronic conditions each participant lived with. Medical personnel conducted the physical examination component in mobile examination centres, during which anthropometric data, including participant height, weight, and waist circumference, were collected and body mass index (BMI) was calculated.
Physical function assessment
Physical function was evaluated based on the aggregation of 11 variables from the physical functioning questionnaire included in NHANES. Participants self-rated their capability to complete the following tasks: walk a quarter mile, walk up ten steps, stoop/crouch/kneel, lift or carry objects, complete household chores, walk between rooms on the same floor, stand up from an armless chair, get in and out of bed, stand for a long period of time, sit for a long period of time, and push or pull large objects. Participants reported their perceived difficulty in completing these tasks as ‘no difficulty’, ‘some difficulty’, ‘much difficulty’, ‘unable to do’, ‘do not do this activity’, ‘refused’, or ‘do not know’. For the purpose of this analysis, the responses were then amalgamated and converted to a scale of 1–4, based on the response indicating that they ‘can accomplish’ (1), ‘have some difficulty’ (2), ‘have much difficulty’ (3), or ‘cannot do’ (4) each task. Participants who indicated they did not complete the activity, refused to answer, or did not know were excluded from the analysis.
Patterns of physical activity and sedentary behaviour
Minute-by-minute MVPA and sedentary behaviour were measured with an ActiGraph AM-7164 uniaxial accelerometer. Participants were instructed to wear the device on their hip during all waking hours for seven consecutive days, removing it only during bathing and swimming activities. In order to be included in this analysis, participants must have worn the accelerometer for at least 10 h on 4 days. Non-wear time was identified as 60 consecutive minutes (or longer) of zero-intensity counts. Wear time was then calculated by subtracting non-wear time from the total 24-h period of a day. MVPA was defined as 2020 counts per minute or higher, whereas sedentary behaviour was defined as any time spent with counts per minute below 100 counts per minute [17]. Each minute spent within one of these categories was summed as total MVPA or sedentary behaviour. There was no permissible minutes for spontaneous MVPA to drop below the MVPA threshold. Patterns of MVPA and sedentary behaviour were broken into continuous bouts of 1 min, 5 min, 10 min, 30 min, and 60 min in duration, inclusively.
Statistical analysis
Descriptive statistics were calculated as mean ± standard deviation and frequencies (percent) for continuous and categorical variables, respectively. The number of participants who completed each of the MVPA and sedentary bout durations was determined. Longer bout durations were inclusive of shorter bouts, meaning an individual who completed a 10-min bout of MVPA was also counted as completing a 1-min, and 5-min bout. The amount of time spent in each bout was standardized to represent minutes per day throughout a 7-day week, averaged across the entirety of the sample.
An exploratory factor analysis was conducted to compute an individualized factor score based on each participant’s responses to the 11 categorical physical function questions using Mplus version 8.1. Orthogonal rotation was used with a weighted least squares mean and variance-adjusted estimation algorithm. This was done to account for differences in participants’ perception of difficulty, as well as the potential association between the variables selected to represent physical function. Three factor scores were extracted based on a high probability (0.977) of the root mean square error of approximation being less than 0.05, a comparative fit index score above 0.95, and a standardized root mean square residual below 0.05. Once these factors were determined, a polychoric correlation matrix was used to determine the captured variable changes. Afterward, the data were interrupted by evaluating the loading of the physical function variables on each factor based on a salience criterion of 0.4 to ensure no cross-loading was present. Based on this analysis, three factors were determined. The three factors were then summed to create a single factor score for each participant. Data distribution were observed as a whole as well as by age (5-year categories) and sex categories. The factor score was not distributed linearly, but rather as two groupings. Thus, participants were categorized as scoring either above or below the median function score of their respective sex (male/female) and age (65–69, 70–74, 75–79, 80 +) grouping.
Logistic regression analyses were conducted to examine the association between the various bouts of MVPA and sedentary behaviour, and the likelihood of scoring above the median function score. Analysis was adjusted for BMI, ethnicity, household income, and total number of chronic diseases. Analyses determining the association between sedentary time and physical function were then adjusted for total MVPA time, and analyses determining the association between MVPA and physical function were adjusted for total sedentary time. All the logistic regressions were performed with men and women combined since no interaction terms was found to be significant between sex and MVPA (p values ranging from 0.72 to 0.92) or sex and sedentary bouts (p values ranging from 0.69 to 0.86).
Descriptive data were calculated using SPSS version 25. Regression analyses were conducted using SAS version 9.4, adjusting for strata and sample weight.
Results
Participants
An initial sample of 20,410 participants was available for use from the 2003–2004 and 2005–2006 NHANES databases. The final sample was reduced to 1274 once those who did not complete the NHANES physical functioning questionnaire adequately, did not have the appropriate accelerometer data, or were younger than age 65 were removed from analysis. A flowchart outlining the filtering of participants is available in Fig. 1.

Participant flowchart
Descriptive data
Descriptive statistics for the sample population are shown in Table 1. The average age of the included sample was 74 years, and categorized as overweight based on the calculated BMI. Participants reported being diagnosed with an average of one chronic condition. The majority of the sample identified as non-Hispanic White, with a high-school (or lower) education.
Physical activity and sedentary behaviour patterns
The number of participants who engaged in each of the various MVPA and sedentary bouts, and the average time spent in those bouts per day, are shown in Table 2. The prevalence of, and time spent engaging in, MVPA bouts dropped substantially as the bout length increased. Only 30.1% of the sample performed at least one bout of MVPA lasting the previously recommended 10 min or more, whereas 93.8% of participants engaged in a 1-min bout, averaging an accumulation of 10.4 min of MVPA per day in bouts of 1 min or more. Likewise, 62.1% of participants engaged in a 5-min bout, averaging an accumulation of 7.4 min of MVPA per day in bouts of 5 min or more. Every participant had at least one bout of 1 min, 5 min, 10 min, and 30 min of consecutive sedentary time, and nearly every participant (97.4%) had at least one bout of 60 min of consecutive sedentary time.
Association between MVPA bouts and physical function
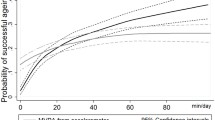
Results of the adjusted and weighed logistic regression for the association between various patterns of MVPA and an above average physical function score can be viewed in Table 3. The regression analysis found 1-min, 5-min, and 10-min bout lengths were all associated with having higher physical function (p < 0.05). However, the 30-min (p = 0.899) and 60-min bouts (p = 0.437) of MVPA were not. When scaled to represent every 10-min totality of MVPA, likelihoods increased for both the 1-min (odds ratio [OR] 1.25; 95% confidence interval [CI] 1.11–1.39) and 5-min (OR 1.22; 95% CI 1.08–1.37) bouts (p < 0.05).
Association between sedentary bouts and physical function
When weighed and adjusted for age, sex, BMI, ethnicity, household income, and total number of chronic conditions, the logistic regression analysis found each of the sedentary bout lengths were associated with a small, yet significant decrease in participant likelihood of having an above average function score (p < 0.05). Moreover, when scaled for every 30-min totality of 1-min (OR 0.96; 95% CI 0.93–0.99), 5-min (OR 0.96; 95% CI 0.93–0.99), or 10-min (OR 0.96; 95% CI 0.93–0.99) bouts, accumulated sedentary time was also found to decrease the likelihood of a participant having above average physical function (p < 0.05). Similar findings resulted when the 30-min bouts (OR 0.84; 95% CI 0.75–0.95) and 60-min bouts (OR 0.78; 95% CI 0.65–0.93) were scaled to represent every 120 min totaled throughout the day (p < 0.05). However, once the regression model was further adjusted to account for total MVPA time the associations were no longer significant. These results can be viewed in Table 4a and b.
Discussion
The purpose of this cross-sectional analysis was to determine the association between various patterns of MVPA and sedentary behaviour with the physical function of older adults. For the first time we have shown MVPA in bouts shorter than 10 min in duration are associated with physical function in older adults. Specifically, both 1- and 5-min bouts of MVPA were associated with a 2% increase in the likelihood of having above average physical function. Conversely, sedentary behaviour patterns are not associated with physical function, once adjusted for total MVPA. These findings support previous literature highlighting the potential health benefits associated with various bouts of MVPA; while also challenging previously reported negative associations between sedentary behaviour and physical function.
MVPA bouts and physical function
While the influence shorter bouts of MVPA have on physical function is seemingly small, the additive impact of such activity is noteworthy, as scaling 1-min and 5-min bouts of MVPA to represent an accumulation of 10 min increased the likelihood of having above average physical function to 23–26%. These data suggest every minute spent participating in MVPA, when accumulated throughout the day, contributes to having an above average physical function score. This aligns with conclusions drawn following a longitudinal cohort study conducted by Jefferis et al. [13], who stated the total volume of physical activity was of greater importance than the pattern of accumulation to reduce mortality amongst community-dwelling older men.
Physical activity guidelines around the world emphasize the importance of older adults completing 150 min of MVPA to achieve functional benefits [6, 7, 11, 18]. Despite knowledge of the health benefits associated with MVPA, older adults are among the most inactive segment of the population; often citing pain, poor health, and shortness of breath—particularly when standing or engaging in physical activity for prolonged periods—as reasons for being inactive [19,20,21]. As anticipated, our results found a significant reduction in participation in MVPA bouts lasting 10 min or longer, when compared to 1- and 5-min bout lengths. It is likely the reduced participation was, in part, due to these aforementioned limitations. Likewise, the relatively high engagement in 1- and 5-min bouts of MVPA suggests an increased tolerance for shorter bouts of MVPA. Such an occurrence is encouraging, as bouts of MVPA shorter than the recommended 10-min duration were found to be associated with above average physical function. This is in line with mounting evidence providing similar support for spontaneous MVPA, as benefits including reduced rates frailty, mortality, metabolic syndrome, and various risk factors related to cardiovascular disease have been conferred without 10 min of continuous MVPA [12, 13, 22, 23]. As such, the results found here are in support of the recent update to the American Physical Activity Guidelines which encourage MVPA, regardless of duration [11]. Doing so may provide older adults with an alternative option they perceive as feasible, while also providing the desired health benefits. Future research should attempt to identify how previously identified determinants of physical activity, such as increased self-efficacy [24, 25] or local physical environments [26, 27], interact with shorter bouts of MVPA to increase overall activity levels.
Sedentary bouts and physical function
Numerous research has indicated an association between sedentary behaviour and lower physical function in older adults [5, 28]. While a recent systematic review conducted by Copeland et al. [17] discusses many such results, the authors bring forward a number of articles contradicting such a relationship. Of particular interest, two studies adjusting for MVPA found doing so accounted for the potential relationship between sedentary behaviour and physical function, resulting in the relationship no longer achieving significance [29, 30]. Similar results were found here, as adjustment for total MVPA accounted for the observed relationship between the various bouts of sedentary behaviour and the observed association with physical function.
Regardless of the controversial relationship between sedentary behaviour and physical function, a meta-analysis conducted by Shrestha et al. [31] highlights the lack of randomized control trials attempting to evaluate the effectiveness of lifestyle interventions aiming to reduce sedentary time in older adults. The authors’ analysis of adults aged 18–60 identified short- and medium-term reductions in sedentary time as a result of a variety of lifestyle interventions, averaging a reduction of approximately 30 min per day. Our results indicate that such a change, should their findings translate to the older adult population, may not be sufficient to benefit physical function. Nonetheless, further research is necessary to identify both the potential benefits and the effectiveness that interventions aimed at reducing sedentary time in older adults may have.
Strengths and limitations
The study described above is strengthened through the utility of NHANES, as the database provides a large, nationally representative, appropriately weighted sample, thus increasing external validity. The objective measurement of MVPA and sedentary behaviour via accelerometry provided an accurate indication of participant movement, thus reducing recall error and social desirability bias. Finally, the scope of the NHANES database allowed for the adjustment for major confounding factors. Despite these strengths, limitations exist which require consideration as well. First, while the analysis was weighed to account for the complexity in the design it remains possible that the final sample was no longer absolutely representative of older adults in the United States. Of note, the percentage of university attendees who also completed graduate school is high, and the influence of such an occurrence is unknown. The discussed results are also cross-sectional in nature. As such, the potential causality of the described relationships remains unknown. The NHANES outcomes used to describe physical function were self-reported, thus introducing potential bias to the outcomes. Objective measurement of physical function would provide higher confidence, and aid in reducing potential biases. The relatively short duration of the sedentary bouts may have impacted the results. It remains possible that longer durations of sedentary behaviour could have a negative association with physical function. Finally, the number of participants who completed bouts of MVPA lasting 30 min or longer was limited. This likely influenced the results in interpreting the relationship between longer-duration bouts of MVPA and physical function.
Conclusion
In conclusion, various patterns of MVPA are associated with an increased likelihood of above average physical function for one’s respective sex and age, in independent older adults. It may be beneficial for future physical activity guidelines to encourage various patterns of MVPA, as opposed to the current strategy of requiring bouts of 10 min or more. Conversely, bouts of sedentary behaviour of up to 60 min in duration are not associated with physical function, once adjusted for total MVPA. In other words, this study suggests that various patterns of physical activity have a more meaningful relationship with physical function than sedentary behaviour for independent older adults living.
References
Martinez-Gomez D, Bandinelli S, Del-Panta V et al (2017) Three-year changes in physical activity and decline in physical performance over 9 years of follow-up in older adults: The Invecchiare in Chianti Study. J Am Geriatr Soc 65:1176–1182. https://doi.org/10.1111/jgs.14788
Visser M, Simonsick EM, Colbert LH et al (2005) Type and intensity of activity and risk of mobility limitation: the mediating role of muscle parameters. J Am Geriatr Soc 53:762–770. https://doi.org/10.1111/j.1532-5415.2005.53257.x
Miller ME, Rejeski WJ, Reboussin BA et al (2015) Physical activity, functional limitations, and disability in older adults. J Am Geriatr Soc 48:1264–1272. https://doi.org/10.1111/j.1532-5415.2000.tb02600.x
Guralnik JM, Alecxih L, Branch LG et al (2002) Medical and long-term care costs when older persons become more dependent. Am J Public Health 92:1244–1245
Santos DA, Silva AM, Baptista F et al (2012) Sedentary behavior and physical activity are independently related to functional fitness in older adults. Exp Gerontol 47:908–912. https://doi.org/10.1016/j.exger.2012.07.011
World Health Organization (2010) Global recommendations on physical activity for health. WHO Press
Tremblay MS, Warburton DER, Janssen I et al (2011) New canadian physical activity guidelines. Appl Physiol Nutr Metab 36:36–46. https://doi.org/10.1139/H11-009
Colley RC, Garriguet D, Janssen I et al (2011) Physical activity of Canadian adults: accelerometer results from the 2007 to 2009 Canadian Health Measures Survey. Health Rep 22:7–14
Watson KB (2016) Physical inactivity among adults aged 50 years and older—United States, 2014. MMWR. https://doi.org/10.15585/mmwr.mm6536a3
Chau J, Chey T, Burks-Young S et al (2017) Trends in prevalence of leisure time physical activity and inactivity: results from Australian National Health Surveys 1989–2011. Aust N Z J Public Health 41:617–624. https://doi.org/10.1111/1753-6405.12699
Piercy KL, Troiano RP, Ballard RM et al (2018) The physical activity guidelines for Americans. JAMA 320:2020–2028. https://doi.org/10.1001/jama.2018.14854
Kehler DS, Clara I, Hiebert B et al (2018) The association between bouts of moderate to vigorous physical activity and patterns of sedentary behavior with frailty. Exp Gerontol 104:28–34. https://doi.org/10.1016/j.exger.2018.01.014
Jefferis BJ, Parsons TJ, Sartini C et al (2018) Objectively measured physical activity, sedentary behaviour and all-cause mortality in older men: does volume of activity matter more than pattern of accumulation. Br J Sports Med. https://doi.org/10.1136/bjsports-2017-098733
Matthews CE, Chen KY, Freedson PS et al (2008) Amount of time spent in sedentary behaviors in the United States, 2003–2004. Am J Epidemiol 167:875–881. https://doi.org/10.1093/aje/kwm390
Sardinha LB, Santos DA, Silva AM et al (2015) Breaking-up sedentary time is associated with physical function in older adults. J Gerontol Ser A 70:119–124. https://doi.org/10.1093/gerona/glu193
Copeland JL, Ashe MC, Biddle SJ et al (2017) Sedentary time in older adults: a critical review of measurement, associations with health, and interventions. Br J Sports Med 51:1539. https://doi.org/10.1136/bjsports-2016-097210
Troiano RP, Berrigan D, Dodd KW et al (2008) Physical activity in the united states measured by accelerometer. Med Sci Sports Exerc 40:181. https://doi.org/10.1249/mss.0b013e31815a51b3
Department of health, physical activity, health improvement and protection (2011) Start active, stay active: a report on physical activity from the four home countries’Chief Medical Officers. Crown, London
Chastin SFM, Buck C, Freiberger E et al (2015) Systematic literature review of determinants of sedentary behaviour in older adults: a DEDIPAC study. Int J Behav Nutr Phys Act 12:127. https://doi.org/10.1186/s12966-015-0292-3
Crombie IK, Irvine L, Williams B et al (2004) Why older people do not participate in leisure time physical activity: a survey of activity levels, beliefs and deterrents. Age Ageing 33:287–292. https://doi.org/10.1093/ageing/afh089
Mathews AE, Laditka SB, Laditka JN et al (2010) Older adults’ perceived physical activity enablers and barriers: a multicultural perspective. J Aging Phys Act 18:119–140. https://doi.org/10.1123/japa.18.2.119
Loprinzi PD, Cardinal BJ (2013) Association between biologic outcomes and objectively measured physical activity accumulated in ≥ 10-minute bouts and < 10-minute bouts. Am J Health Promot 27:143–151. https://doi.org/10.4278/ajhp.110916-QUAN-348
Glazer NL, Lyass A, Esliger DW et al (2013) Sustained and shorter bouts of physical activity are related to cardiovascular health. Med Sci Sports Exerc 45:109–115. https://doi.org/10.1249/MSS.0b013e31826beae5
Burton LC, Shapiro S, German PS (1999) Determinants of physical activity initiation and maintenance among community-dwelling older persons. Prev Med 29:422–430. https://doi.org/10.1006/pmed.1999.0561
Kosteli M-C, Williams SE, Cumming J (2016) Investigating the psychosocial determinants of physical activity in older adults: a qualitative approach. Psychol Health 31:730–749. https://doi.org/10.1080/08870446.2016.1143943
Michael YL, Perdue LA, Orwoll ES et al (2010) Physical activity resources and changes in walking in a cohort of older men. Am J Public Health 100:654–660. https://doi.org/10.2105/AJPH.2009.172031
Li F, Fisher J, Brownson RC (2005) A multilevel analysis of change in neighborhood walking activity in older adults. J Aging Phys Act 13:145–159
Gennuso KP, Thraen-Borowski KM, Gangnon RE et al (2016) Patterns of sedentary behavior and physical function in older adults. Aging Clin Exp Res 28:943–950. https://doi.org/10.1007/s40520-015-0386-4
Cooper AJM, Simmons RK, Kuh D et al (2015) Physical activity, sedentary time and physical capability in early old age: British birth cohort study. PLoS One. https://doi.org/10.1371/journal.pone.0126465
Ortlieb S, Dias A, Gorzelniak L et al (2014) Exploring patterns of accelerometry-assessed physical activity in elderly people. Int J Behav Nutr Phys Act 11:28. https://doi.org/10.1186/1479-5868-11-28
Shrestha N, Grgic J, Wiesner G et al (2018) Effectiveness of interventions for reducing non-occupational sedentary behaviour in adults and older adults: a systematic review and meta-analysis. Br J Sports Med. https://doi.org/10.1136/bjsports-2017-098270
Funding
The authors have no funding to report.
Author information
Authors and Affiliations
Contributions
Hrubeniuk T.J.: statistical analysis and interpretation of data, study concept, wrote manuscript. Sénéchal M.: analysis and interpretation of data, preparation of manuscript. Mayo A.: statistical analysis and interpretation of data, review of manuscript. Bouchard D.R.: study concept and design, analysis and interpretation of data, preparation of manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval and compliance
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The NHANES data collection was ethically approved by the Institutional Review Board of the Centers for Disease Control and Prevention.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hrubeniuk, T.J., Sénéchal, M., Mayo, A. et al. Association between physical function and various patterns of physical activity in older adults: a cross-sectional analysis. Aging Clin Exp Res 32, 1017–1024 (2020). https://doi.org/10.1007/s40520-019-01288-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-019-01288-2