
Abstract
Background
Little is known about the relationship between metabolic syndrome (MetS) and disability in the oldest old.
Aims
To investigate the possible association between MetS and disability among community-dwelling older adults aged ≥ 90 years.
Methods
This was a secondary analysis of a cross-sectional study. MetS was defined by the International Diabetes Federation Criteria. Activities of daily living (ADL) and instrumental activities of daily living (IADL) disabilities were evaluated using the physical self-maintenance scale and the Lawton–Brody IADL scale, respectively.
Results
We included 725 participants (mean age: 93.8 ± 3.1 years). The prevalence of MetS was 13.0% in women and 9.8% in men, respectively. In women, ADL and IADL disabilities were more prevalent in the MetS group compared with the non-MetS group (ADL: 43.1 vs. 30.6%, p = 0.044; IADL: 73.8 vs. 59.8%, p = 0.030). After adjusting for relevant confounders, participants with MetS was associated with an increased risk of either ADL (odds ratio [OR] 1.81, 95% confidence interval [CI] 1.22–3.45) or IADL disability (OR 2.12, 95% CI 1.31–4.78) compared with those without MetS. In men, similar results were found with respect to the prevalence of ADL or IADL disability and the adjusted ORs, but the results were not statistically significant.
Conclusion
MetS is associated with an increased risk of either ADL or IADL disability in a study population of long-lived adults, especially in women.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Metabolic syndrome (MetS) is a cluster of cardiometabolic risk factors, including abdominal obesity, dyslipidemia, hypertension, and hyperglycemia [1]. Based on a study population of more than 8,000 participants, the prevalence of MetS across Europe was 24.3% in adults [2]. A recent study demonstrated that the prevalence of MetS increased from 25.3 to 34.2% among adults aged ≥ 18 years during 1988–2012 in the US [3]. The prevalence of MetS increases with advanced age [4]. According to the National Cholesterol Education Program (NCEP), the prevalence of MetS varied from 23 to 55% in older adults worldwide [4].
MetS has been shown to be independently associated with a high risk of many healthcare outcomes, such as cardiovascular diseases, diabetes, medical costs and mortality [5, 6]. However, the association of MetS with functional limitations or disability among older adults was controversial in previous studies [7,8,9]. For example, Liaw et al. reported that the components of MetS, particularly abdominal obesity and high triglyceride levels, were significantly associated with disability in community-dwelling older adults [7]. Another study also found that MetS was significantly related to functional dependence in both activities of daily living (ADL) and instrumental activities of daily living (IADL) among community-dwelling older adults [8]. However, Blaum et al. reported that MetS was associated with mobility limitation but not ADL or IADL disability among older Mexican Americans [9]. All these studies were conducted in relatively young older adults (mean age: 68.3–70.6 years).
Currently, there is limited evidence regarding the prevalence of MetS and its association with disability among the oldest old. We, therefore, conducted this study to investigate the possible association between MetS and disability among a population of older adults aged 90 years and older.
Methods
Study population
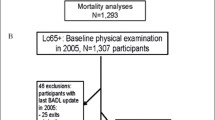
The study is a secondary analysis of a previously published cross-sectional study named “Project of Longevity and Aging in Dujiangyan” (PLAD) in April 2005 [10]. The study protocol was approved by the Research Ethics Committee of Sichuan University. We screened 1115 older adults (≥ 90 years) who living in Dujiangyan, China. Of whom, 870 individuals were evaluated through face-to-face interviews and anthropometric measurements by well-experienced staff. Their venous fasting blood samples were also collected. All participants (or their legal proxies) were asked to sign an informed consent.
MetS criteria
We applied the International Diabetes Federation Criteria [11] to define MetS: abdominal obesity (defined as waist circumference [WC] ≥ 90 cm for Chinese men and ≥ 80 cm for Chinese women), combining with any two or more of the following four factors: (1) systolic blood pressure (SBP) ≥ 130 mmHg or diastolic blood pressure (DBP) ≥ 85 mmHg or receiving treatment of hypertension; (2) triglyceride (TG) ≥ 1.7 mmol/L or receiving lipid-lowering therapy; (3) high-density lipoprotein cholesterol (HDL-C) < 1.29 mmol/L in women or < 1.03 mmol/L in men or receiving treatment for this lipid abnormality; and (4) fasting blood glucose ≥ 5.6 mmol/L or receiving the treatment of type two diabetes.
Measurement of ADL and IADL disability
The ADL and IADL disability were evaluated with the physical self-maintenance scale (PSMS) and the Lawton–Brody IADL scale [12], respectively. The PSMS was a six-item scale, including eating, walking, grooming, dressing, toileting, and bathing. The Lawton–Brody IADL scale was an eight-item scale, including shopping, housekeeping, food preparation, laundry, transportation, self-management of medication, using the telephone, and handling finances. The options for each item was “cannot do by myself”, “need some help from other people”, “some difficulty but can do by myself”, “can do by myself”. In our study, impairment was defined as “cannot do by myself”, “need some help from other people”. The ADL disability was defined as having an impairment in any of the six items of the PSMS. The IADL disability was defined as having an impairment in any of the eight items of the Lawton–Brody IADL scale.
Other covariates
We included the following covariates in the analyses: age, gender, smoking status, alcohol drinking status, physical activities, cognitive impairment (evaluated with the Chinese version of Mini Mental Status Examination [MMSE]) [13], and depression (evaluated with the 23-item Geriatric Depression Scale—Chinese Edition [GDS-CD]) [14]. The following chronic diseases were also evaluated using a self-reported questionnaire: bone fracture, cardiovascular disease, respiratory disease, stroke, osteoarthritis, visual problems, and hearing problems.
Statistical analysis
All statistical analyses were performed in SPPS 20.0 (IBM Inc., Armonk, NY). Continuous and categorical data are presented as the mean ± standard deviation (SD) and number (percentage), respectively. Clinical characteristics were compared based on the MetS category. The differences between groups were tested by the Pearson chi-squared test and ANOVA for the categorical variables and the continuous variables, respectively. Two-tailed p value < 0.05 was considered to indicate statistically significant. We applied logistic regression models to estimate the adjusted odds ratios (OR) and 95% confidence intervals (CI) for disability by MetS and its components (abdominal obesity, high blood pressure, high TG, low HDL-C, and high FBG), separately. Model 1 was adjusted for age and gender. Model 2 included Model 1 + smoking status, alcohol drinking status, physical activities, hemoglobin, and the chronic diseases adjustment. Model 3 included Model 2 + cognitive impairment and depression adjustment. In addition, we stratified our data by gender, because previous studies found that the prevalence of either disability or MetS was significantly different between men and women [15, 16].
Results
We included 725 individuals (500 women and 225 men) in this study, 145 participants were excluded due to missing data on ADL/IADL (92 individuals) and/or MetS (82 individuals). There was no significant difference between the included and excluded populations with regard to age (mean age: 93.8 ± 3.1 years and 93.6 ± 3.5 years, respectively; p = 0.786) and gender (women: 69 and 62.1%, respectively; p = 0.105).
Characteristics of participants with or without MetS
The characteristics of the study population are presented in Table 1. The prevalence of MetS was 12, 13, and 9.8% in the whole study population, women, and men, respectively. The prevalence of ADL disability was 30.9, 32.2, and 28% in the whole study population, women and men; whereas the prevalence of IADL was 60.4, 61.6, and 57.8%, respectively.
Among the whole study population, individuals with MetS, compared with those without MetS, were more likely to have ADL disability (41.4 vs. 29.5%, p = 0.024) and IADL disability (71.3 vs. 58.9%, p = 0.027). Similarly, women with MetS, compared with women without MetS, were more likely to have ADL disability (43.1 vs. 30.6%, p = 0.044) and IADL disability (73.8 vs. 59.8%, p = 0.030). However, no significant difference was identified between men with MetS and men without MetS with regard to either ADL disability (36.4 vs. 27.1%, p = 0.358) or IADL disability (63.6 vs. 53.7%, p = 0.374). In addition, among both women and men, individuals with MetS were more prone to cardiovascular diseases than those without MetS.
Association of MetS and its components with ADL disability
The results of the logistic regression models regarding the association of MetS with ADL and IADL disability are presented in Table 2. After adjusting for potential confounders, MetS was significantly associated with an increased risk of ADL disability in the whole study population (fully adjusted OR, 1.65; 95% CI 1.10–3.21) and in women (fully adjusted OR, 1.81; 95% CI 1.22–3.45). In men, there was a trend that MetS was associated with ADL disability, but the result was not statistically significant (fully adjusted OR, 1.92; 95% CI 0.98–3.11).
When considering the components of MetS, only abdominal obesity was significantly related to an increased risk of ADL disability in the whole study population (fully adjusted OR 1.28; 95% CI 1.08–3.41). This relationship was significant in women (fully adjusted OR 1.41; 95% CI 1.25–4.11) but not in men (fully adjusted OR 1.25; 95% CI 0.88–4.14).
Association of MetS and its components with IADL disability
Similarly, MetS was significantly associated with an increased risk of IADL disability in the whole study population (fully adjusted OR 2.09; 95% CI 1.17–4.32) and in women (fully adjusted OR 2.12; 95% CI 1.31–4.78), but the result was not statistically significant in men (fully adjusted OR 2.20; 95% CI 0.87–4.01) (Table 2).
In the components of MetS, only abdominal obesity was significantly related to an increased risk of IADL disability in the whole study population (fully adjusted OR 1.75; 95% CI 1.21–3.73) and in women (fully adjusted OR 1.77; 95% CI 1.19–3.77). However, this relationship was not significant in men (fully adjusted OR 1.60; 95% CI 0.92–4.55).
Other significant covariables associated with disability
Not surprisingly, age was significantly associated with both ADL (fully adjusted OR 1.15; 95% CI 1.05–1.50) and IADL disabilities (fully adjusted OR 1.31; 95% CI 1.09–1.71). In addition, bone fracture was significantly associated with ADL (fully adjusted OR 1.33; 95% CI 1.08–3.55) and IADL disabilities (fully adjusted OR 1.82; 95% CI 1.29–2.56). The sub-group analysis also demonstrated that age and bone fracture were significantly associated with ADL and IADL disabilities in both men and women (Table 2).
Discussion
In our study population, MetS was not common (12%), but it was still independently associated with a higher risk of both ADL and IADL disabilities, especially in women. In both genders, individuals with MetS were more prone to cardiovascular diseases compared with those without MetS.
To the best of our knowledge, this study is the first to provide the evidence of the association between MetS and ADL/IADL disability among a population of nonagenarians and centenarians. Our findings were in line with some previous cross-sectional and prospective studies conducted in young older adults [7, 8]. However, some other studies did not identify the association between MetS and disability among various populations. For example, a cross-sectional study reported that MetS is prevalent in older adults with the risk of disability, but it was not independently associated with walking speed, lower extremity function, or self-reported ADL/IADL disability [17]. Another prospective study indicated that MetS was associated with an increased risk of new-onset IADL disability but not ADL disability [18]. Moreover, a prospective study even found that MetS was a protective factor of ADL disability among older adults aged 70 to 89 years [19]. Because of the significant difference across studies with respect to the study population, the definition of disability and MetS, and the adjusted confounders, it was hard to compare the results of these studies. Based on current evidence, we cannot draw any robust conclusion regarding the relationship between MetS and disability.
The prevalence of MetS among our study population was lower than that among younger elderly people in previous studies. One possible reason for this low prevalence might be due to survival bias: individuals with MetS were less likely to survive into their 90-year age. Additionally, the prevalence of MetS depends on the definition of MetS [20]. In our study, we used the International Diabetes Federation Criteria [11] to define MetS, however, it remained unclear whether this definition and the relevant cut-off points were appropriate for diagnosing MetS in the oldest old.
Gender differences in the prevalence of MetS were widely reported in previous studies. Our study found a higher prevalence of MetS in women compared with men. This finding was in accordance with some previous studies. For example, a systematic review of nine studies reported that the prevalence of MetS ranged from 29.6 to 36.2% in men and from 36.1 to 45.9% in women in Gulf Cooperation Council Countries [21]. However, some other studies reported opposite results. For example, a previous study found that the prevalence of MetS was 26.4% in men and 15.7% in women in Australia [22].
When focusing on the components of MetS, our study found that only abdominal obesity was independently associated with ADL and IADL disabilities, whereas the other four components (high blood pressure, high TG, Low HDL-C, and High FBG) were not. This finding was similar to a recent study [7]. In that study, among the five components of MetS, only abdominal obesity and high TG levels were independently associated with functional disability in older adults [7]. These findings imply that although the impairment of a certain component of MetS may not be associated with disability independently, the “cumulative” impairments of these components may contribute to disability.
One possible mechanism underlying the association between MetS and disability might be chronic low-grade systemic inflammation, which has been shown to connect aging and MetS [23]. A prospective cohort study demonstrated that older women with high interleukin (IL)-6 serum levels are at an increased risk of disability compared with those with lower levels [24]. Another prospective study included 880 older adults aged 70 to 79 years and reported that the serum IL-6 level predicted the onset of disability during 7-year follow-up [25]. These findings indicated that chronic systemic inflammation might play a role in functional disability as well.
MetS may contribute to disability not only via chronic low-grade inflammation but also via artery aging. For example, Scuteri et al. reported that MetS was associated with increased arterial thickness and stiffness [26], the latter has been associated with walking disability in older adults with peripheral artery disease [27] and cognitive decline [28].
Our study has some limitations. First, we failed to adjust for some important confounders, such as frailty and sarcopenia. Because these factors were not evaluated in the PLAD study. A prospective study showed that frailty and its components (including slowness, weakness and weight loss) has a significant impact on the incidence of disability [29]. Previous studies demonstrated that sarcopenia was associated with a higher risk of both disability [30] and MetS [31, 32] in older adults. Therefore, future studies addressing the relationship between disability and MetS should consider adjusting for sarcopenia and frailty. Second, because of the cross-sectional design, we could not make a causal inference about the association between MetS and ADL or IADL disability. Third, we did not adjust for medications and polypharmacy (the concomitant use of ≥ 5 medications) in our study. Previous studies indicated that some medications (e.g., benzodiazepine or anticholinergic drugs) [33] and polypharmacy [34] was associated with functional decline in older adults. Last, because our study is a secondary analysis of the PLAD study, survival bias and reporting bias might exist.
In conclusion, both ADL and IADL disabilities were prevalent among a population of Chinese older adults aged 90 years or older. MetS was not common, but individuals with MetS, compared those without MetS, were more likely to report ADL or IADL disability. This trend was significant in women. These findings need to be validated in future prospectively studies.
References
Penninx BW, Nicklas BJ, Newman AB, Harris TB, Goodpaster BH, Satterfield S et al (2009) Metabolic syndrome and physical decline in older persons: results from the Health, Aging And Body Composition Study. J Gerontol Series A Biol Sci Med Sci 64:96–102
Scuteri A, Laurent S, Cucca F, Cockcroft J, Cunha PG, Manas LR et al (2015) Metabolic syndrome across Europe: different clusters of risk factors. Eur J Prev Cardiol 22:486–491
Moore JX, Chaudhary N, Akinyemiju T (2017) Metabolic syndrome prevalence by race/ethnicity and sex in the United States, National Health and Nutrition Examination Survey, 1988–2012. Prev Chronic Dis 14:E24. https://doi.org/10.5888/pcd14.160287
Denys K, Cankurtaran M, Janssens W, Petrovic M (2009) Metabolic syndrome in the elderly: an overview of the evidence. Acta Clin Belg 64:23–34
Boudreau DM, Malone DC, Raebel MA, Fishman PA, Nichols GA, Feldstein AC et al (2009) Health care utilization and costs by metabolic syndrome risk factors. Metab Syndr Relat Disord 7:305–314
Malik S, Wong ND, Franklin SS, Kamath TV, L’Italien GJ, Pio JR et al (2004) Impact of the metabolic syndrome on mortality from coronary heart disease, cardiovascular disease, and all causes in United States adults. Circulation 110:1245–1250
Liaw FY, Kao TW, Wu LW, Wang CC, Yang HF, Peng TC et al (2016) Components of metabolic syndrome and the risk of disability among the elderly population. Sci Rep 6:22750
Roriz-Cruz M, Rosset I, Wada T, Sakagami T, Ishine M, Roriz-Filho JS et al (2007) Stroke-independent association between metabolic syndrome and functional dependence, depression, and low quality of life in elderly community-dwelling Brazilian people. J Am Geriatr Soc 55:374–382
Blaum CS, West NA, Haan MN (2007) Is the metabolic syndrome, with or without diabetes, associated with progressive disability in older Mexican Americans? J Gerontol Series A Biol Sci Med Sci 62:766–773
Yang M, Hao Q, Luo L, Ding X, Wu H, Zhang Y et al (2014) Body mass index and disability in chinese nonagenarians and centenarians. J Am Med Dir Assoc 15:303 e1–e6
Lu YH, Lu JM, Wang SY, Li CL, Liu LS, Zheng RP et al (2006) Comparison of the diagnostic criteria of metabolic syndrome by International Diabetes Federation and that by Chinese Medical Association Diabetes Branch. Zhonghua yi xue za zhi 86:386–389
Lawton MP, Brody EM (1969) Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist 9:179–186
Katzman R, Zhang MY, Ouang Ya Q, Wang ZY, Liu WT, Yu E et al (1988) A Chinese version of the Mini-Mental State Examination; impact of illiteracy in a Shanghai dementia survey. J Clin Epidemiol 41:971–978
Chan AC (1996) Clinical validation of the Geriatric Depression Scale (GDS): Chinese version. J Aging Health 8:238–253
Beigh SH, Jain S (2012) Prevalence of metabolic syndrome and gender differences. Bioinformation 8:613–616
Murtagh KN, Hubert HB (2004) Gender differences in physical disability among an elderly cohort. Am J Public Health 94:1406–1411
Botoseneanu A, Ambrosius WT, Beavers DP, de Rekeneire N, Anton S, Church T et al (2015) Prevalence of metabolic syndrome and its association with physical capacity, disability, and self-rated health in Lifestyle Interventions and Independence for Elders Study participants. J Am Geriatr Soc 63:222–232
Carriere I, Peres K, Ancelin ML, Gourlet V, Berr C, Barberger-Gateau P et al (2014) Metabolic syndrome and disability: findings from the prospective three-city study. J Gerontol A Biol Sci Med Sci 69:79–86
Laudisio A, Bandinelli S, Gemma A, Ferrucci L, Incalzi RA (2014) Metabolic syndrome and functional ability in older age: the InCHIANTI study. Clin Nutr 33:626–633
Ghosh A (2011) The metabolic syndrome: a definition dilemma. Cardiovasc J Afr 22:295–296
Mabry RM, Reeves MM, Eakin EG, Owen N (2010) Gender differences in prevalence of the metabolic syndrome in Gulf Cooperation Council Countries: a systematic review. Diabet Med 27:593–597
Adams RJ, Appleton S, Wilson DH, Taylor AW, Dal Grande E, Chittleborough C et al (2005) Population comparison of two clinical approaches to the metabolic syndrome: implications of the new International Diabetes Federation consensus definition. Diabetes Care 28:2777–2779
Guarner V, Rubio-Ruiz ME (2015) Low-grade systemic inflammation connects aging, metabolic syndrome and cardiovascular disease. Interdiscip Top Gerontol 40:99–106
Ferrucci L, Penninx BWJH., Volpato S, Harris TB, Bandeen-Roche K, Balfour J et al (2002) Change in muscle strength explains accelerated decline of physical function in older women with high interleukin-6 serum levels. J Am Geriatr Soc 50:1947–1954
Taaffe DR, Harris TB, Ferrucci L, Rowe J, Seeman TE (2000) Cross-sectional and prospective relationships of interleukin-6 and C-reactive protein with physical performance in elderly persons: MacArthur Studies of Successful Aging. J Gerontol Series A Biol Sci Med Sci 55:M709–M715
Scuteri A, Orru M, Morrell C, Piras MG, Taub D, Schlessinger D et al (2011) Independent and additive effects of cytokine patterns and the metabolic syndrome on arterial aging in the SardiNIA Study. Atherosclerosis 215:459–464
Grenon SM, Chong K, Alley H, Nosova E, Gasper W, Hiramoto J et al (2014) Walking disability in patients with peripheral artery disease is associated with arterial endothelial function. J Vasc Surg 59:1025–1034
Scuteri A, Wang H (2014) Pulse wave velocity as a marker of cognitive impairment in the elderly. J Alzheimers Dis 42(Suppl 4):S401–S410
Makizako H, Shimada H, Doi T, Tsutsumimoto K, Suzuki T (2015) Impact of physical frailty on disability in community-dwelling older adults: a prospective cohort study. BMJ Open 5:e008462
Cesari M, Rolland Y, Abellan Van Kan G, Bandinelli S, Vellas B, Ferrucci L (2015) Sarcopenia-related parameters and incident disability in older persons: results from the “invecchiare in Chianti” study. J Gerontol Series A Biol Sci Med Sci 70:457–463
Lee J, Hong YP, Shin HJ, Lee W (2016) Associations of sarcopenia and sarcopenic obesity with metabolic syndrome considering both muscle mass and muscle strength. J Prev Med Public Health 49:35–44
Ishii S, Tanaka T, Akishita M, Ouchi Y, Tuji T, Iijima K et al (2014) Metabolic syndrome, sarcopenia and role of sex and age: cross-sectional analysis of Kashiwa cohort study. PLoS One 9:e112718
Peron EP, Gray SL, Hanlon JT (2011) Medication use and functional status decline in older adults: a narrative review. Am J Geriatr Pharmacother 9:378–391. https://doi.org/10.1016/j.amjopharm.2011.10.002
Maher RL, Hanlon J, Hajjar ER (2014) Clinical consequences of polypharmacy in elderly. Expert opinion on drug safety 13:57–65
Acknowledgements
The authors are grateful to the staff of the Department of Geriatrics, Dujiangyan Hospital; and all participants (as well as their legal proxies) for their great contributions.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None of the authors has any conflict of interest related to this work.
Human and animal rights
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any study with animals performed by any of the authors.
Informed consent
Informed consent was obtained from all the participants in this study or their legal proxies.
Funding
The PLAD study was supported by Discipline Construction Foundation of Sichuan University, grants from the project of Science and Technology Bureau of Sichuan, Province (2006Z09-006-4), and Construction Fund for Subjects of West China, Hospital of Sichuan University (XK05001). Additional funding for this secondary analysis came from the Sichuan Provincial Science and Technology Department (2016JY0058). The sponsors had no role in the design, methods, data collection, analysis, and preparation of this work.
Rights and permissions
About this article

Cite this article
Yang, M., Xu, H., Yang, L. et al. Metabolic syndrome and disability in Chinese nonagenarians and centenarians. Aging Clin Exp Res 30, 943–949 (2018). https://doi.org/10.1007/s40520-017-0877-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-017-0877-6