
Abstract
Background
The need for long-term care services increases with age. However, little is known about the predictors of long-term care (LTC) entry among the oldest old.
Aims
Aim of this study was to assess predictors of LTC entry in a sample of men and women aged 90 years and older.
Methods
This study was based on the Vitality 90 + Study, a population-based study of nonagenarians in the city of Tampere, Finland. Baseline information about health, functioning and living conditions were collected by mailed questionnaires. Information about LTC was drawn from care registers during the follow-up period extending up to 11 years. Cox regression models were used for the analyses, taking into account the competing risk of mortality.
Results
During the mean follow-up period of 2.3 years, 844 (43%) subjects entered first time into LTC. Female gender (HR 1.39, 95% CI 1.14–1.69), having at least two chronic conditions (HR 1.24, 95% CI 1.07–1.44), living alone (HR 1.37, 95% CI 1.15–1.63) and help received sometimes (HR 1.23, 95% CI 1.02–1.49) or daily (HR 1.68, 95% CI 1.38–2.04) were independent predictors of LTC entry.
Conclusion
Risk of entering into LTC was increased among women, subjects with at least two chronic conditions, those living alone and with higher level of received help. Since number of nonagenarians will increase and the need of care thereby, it is essential to understand predictors of LTC entry to offer appropriate care for the oldest old in future.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The number of the oldest old, those aged 90 years and over is increasing faster than ever before. In Finland, their number has doubled between the years 2000 and 2015, and is projected to double again by the year 2035 [1, 2]. Because this group is most likely to suffer from chronic conditions and functional limitations, the demand for the long-term care (LTC) will increase in future.
In Finland, round-the-clock LTC consists of inpatient care in health centre wards (primary care hospitals, which also provide short-term care), residential homes, and sheltered housing with 24 h assistance. Of these, health centres and residential homes are institutional settings, and sheltered housing provides primarily housing and closely related services, but also health and basic medical services. With the structural change in service organization, the residential homes and particularly LTC in health centre wards are increasingly replaced by sheltered housing and in practice all of these services respond mainly to similar care needs. The provision of these services is based on the principle of universal access, and is financed by general taxation, social security contributions and by client fees. The access to care is based on need and it is not dependent on ability to pay [3]. During the last decade, the use of round-the-clock LTC has increasingly concentrated in the oldest age groups and in the last years of life [4]. At the end of 2015, 0.4% of Finns aged over 75 years lived on a LTC ward and 1.7% in a residential home, whereas 7.1% lived in sheltered housing facilities [5].
To estimate future LTC needs, it is essential to identify the factors that predict LTC entry. Previously, several such risk factors have been identified. Older age [6,7,8,9,10,11], functional and cognitive impairments, low self-rated health and certain chronic conditions [6,7,8, 12,13,14,15] are commonly reported risk factors for entry into nursing home and other LTC facilities. Additionally, social factors, such as living arrangements and level of informal care have been shown to contribute to the risk of LTC admission [9, 10]. Previous studies, however, have often focused on relatively young old subjects (≥ 65 years), and less is known about the predictors of the LTC admission among the oldest old. In addition, since predictors of LTC are at least partially the same that predict mortality [16], it is essential to take death into account to accurately identify the risk factors of LTC [17]. The aim of this study was to identify the predictors of LTC entry in a population-based prospective study of men and women aged 90 years or older, treating death as a competing risk.
Materials and methods
Participants and study design
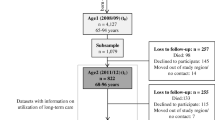
This study was based on the Vitality 90 + Study, a prospective multi-disciplinary population-based study of subjects aged 90 years or older living in the city of Tampere, Finland [18, 19]. Tampere is the third-largest city in Finland, with over 200,000 inhabitants [20]. The proportion of older adults in Tampere is very close to that for the whole country. A questionnaire was mailed to all subjects of this age group who, according to the Tampere City Population Register, resided in community or in institution in 2001, 2003, 2007 or 2010 (n = 4994). The total number of completed and returned questionnaires was 4074, response rate being 82% (79% in 2001, 86% in 2003, 82% in 2007, and 80% in 2010). The study population of the present study included those subjects who answered to the questionnaire and were not in the LTC at baseline. If a subject had answered to the questionnaire in more than one of these years, only the first entry was taken into account in the analyses. Table 1 shows the participants of the Vitality 90 + survey, participation rate, and the size of the final study population, according to the study year. The final study population consisted of 1954 subjects (465 men and 1489 women). Subjects were allowed to ask for help from a family member, a caregiver or a friend in case they were unable to fill in the questionnaire themselves. If a subject was unable to select an answer a family member, a caregiver or a friend was allowed to participate as a proxy. The proxy rate in this study population was 4.0%.
The baseline data of the Vitality 90 + were linked with the follow-up information on LTC use and dates of death. The information about LTC use was drawn from the Care Registers for Health and Social Welfare provided by the National Institute for Health and Welfare. The dates of death were drawn from the Causes of Death register. These registers have been shown to be reliable and accurate source of information with a nationwide coverage [21]. The data linkage was performed by Statistics Finland using the unique personal identification code (PIC) assigned to all persons residing in Finland. Permissions to access the registers were granted by the registers’ administrators. The study protocol was approved by the ethics committee of the Pirkanmaa Hospital District and the Ethics Committee of the Tampere Health Center. All participants or their legal representatives gave their written informed consent.
Long-term care
Participants were categorised as LTC users if (1) they spent 90 days or more in a residential home, in a service home with 24 h assistance, or in the inpatient ward of a health centre or hospital, or if (2) they had a confirmed LTC decision from the municipal service providers. The 90 days could be spent at the same facility or successively at several facilities without returning home for more than one night [22]. The follow-up period started at the index date of each study year and continued until the date of the first entry into LTC, until the date of death or until the end of 2012, whichever came first.
Predictors
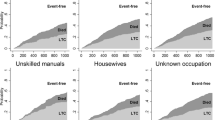
The questionnaire elicited information about mobility, self-rated health, chronic conditions, living arrangements, received help and main lifetime occupation. Mobility was assessed by questions asking whether a subject was able to move about indoors, walk 400 m, and use stairs. The alternative answers to these questions were: yes, without difficulty; yes, with difficulty; only with help, and unable. The first two answer alternatives were regarded to indicate independence and the last two alternatives dependence. To distinguish subjects who were and were not able to perform these tasks, the answers to these three questions were further combined into two categories; (1) independent in all and (2) dependent at least in one of the functions. Self-rated health was assessed by the question: “How would you evaluate your present health?” with five answer alternatives; very good, fairly good, average, fairly poor, and poor. To have sufficient number of respondents in each category, the answer alternatives were further categorized as good SRH (very good and fairly good), average, and poor SRH (fairly poor and poor) [23, 24]. For self-rated health, only the individual’s own answers were taken into account and in the analyses, proxy answers were classified as a proxy category. Subjects were asked whether they had been diagnosed for heart disease, diabetes, dementia, depression, hip fracture, stroke or osteoarthritis. Total number of chronic conditions was calculated, and categories of 0–1 diseases and at least two diseases were formed [24]. This categorization was done because we wanted to assess the contribution of morbidity in general rather than that of any individual diagnosis to the risk of LTC entry. However, since the number of those without any disease was low (n = 140) we combined those with 0 or 1 disease in one category. Subjects were also asked whether they lived alone or with their spouse, children, grandchildren or others. The answers were classified into two categories: living alone and living with other(s). Answers to the question “Does someone help you at home, for example, in dressing, washing or cooking?” elicited information about the level of received help, either informal (e.g., from family member) or formal (paid services) help. The answers were: yes, almost every day; yes, sometimes; I don’t get help even though I would need, and I don’t need help. The information about main lifetime occupation was classified into categories of non-manual worker, manual worker, housewife and unknown [25].
Statistical methods
Comparisons between the subjects who entered into LTC, who were community-dwelling at the end of follow-up and who died during the follow-up period without prior entry into LTC were performed using Kruskal–Wallis test and paired samples t test for continuous variables, and Chi-square test for categorical variables. Associations between potential predictors and entry into LTC during the follow-up was estimated by adjusted hazard ratios (HR) with 95% confidence intervals (CI) using Cox proportional hazard models. Three different models were performed: (1) each potential predictor separately adjusted for age and gender, (2) a multivariate model including all variables, and (3) a multivariate competing risk regression model [26] to estimate subhazard ratios (SHR), treating death without entry into LTC as a competing event. The model 3 was performed to distinguish the risk factors of dying from those of LTC entry. To investigate the subhazard proportionality assumption, interaction between potential predictors and log of time was tested in the competing risk model. All analyses were performed using the SAS software (version 9.4; SAS Institute Inc., Cary, NC, USA) and Stata (StataCorp. 2013. Stata Statistical Software: Release 13. College Station, TX: StataCorp LP).
Results
During the mean follow-up of 2.3 years (range 4 days–11.0 years), 844 (43% of the total study populations) subjects entered first time into LTC at the mean age of 93.6 years. Of those 1110 subjects who did not enter into LTC, 443 (40%) were community-dwelling at the end of follow-up, and 667 (60%) had died without entering into LTC during the follow-up. Table 2 presents the baseline characteristics of these groups.
The proportion of women was highest among those who entered into LTC during the follow-up (81%) and lowest among those who died without entering into LTC (69%), while the proportion of men was highest among those who died (31%) and lowest among those who entered into LTC (19%). Compared to those who remained community-dwelling, subjects who entered into LTC were older, were more likely to be dependent in mobility, to have poor self-rated health, at least two chronic conditions, and higher level of received help. In addition, they belonged more likely to manual worker group by main lifetime occupation. On the other hand, compared to those who died during the follow-up, subjects who entered into LTC differed only with respect to gender, number of chronic conditions and living arrangements.
Table 3 presents the associations between the studied predictors and the first entry into LTC during the follow-up. Higher age and female gender, adjusted for each other, significantly predicted entry into LTC. Dependency in mobility functions, poor self-rated health, higher number of reported chronic conditions, and higher level of received help were significantly associated with higher probability of entering into LTC in age- and gender-adjusted models. When all potential predictors were simultaneously added to the model, age and gender did not quite reach statistical significance. Otherwise the same variables as in the age- and gender-adjusted models, and also, living alone, were independent and significant predictors of LTC entry. In the model taking into account the competing risk of death, female gender, higher number of chronic conditions, living alone and higher level of received help remained significant and independent predictors of LTC entry.
Discussion
According to the results of the present study female gender, higher number of chronic conditions, living alone, and higher level of received help were significant and independent predictors of LTC entry, when the competing risk of death was taken into account. These findings are in accordance with previous studies on younger old subjects showing that female gender is associated with an excess risk for institutionalization even after adjusting for potentially contributing factors, such as age and living arrangements [10, 16]. Additionally, in line with previous population-based studies [27] higher number of chronic conditions was associated with an increased risk of LTC entry. Especially dementia or cognitive impairment [6,7,8, 12, 14, 28], depression [28], stroke, diabetes [28,29,30], and hip fracture [15, 28] have been shown to be predictive factors for institutionalization. In our study, individual diseases significantly associated with increased risk were dementia, depression and hip fracture (data not shown). These diseases potentially lead to severe cognitive and/or functional limitations, and thereby increase the need of LTC [7, 31].
In addition to individual’s health, social and environmental factors may be important contributing factors for LTC needs. Our results, as those of several previous studies [9, 10, 27, 32,33,34], showed that living alone was significantly associated with an increased probability of entering into LTC, even independently of baseline health status. This finding obviously indicates the importance of available social contacts, emotional support and informal help in delaying or preventing institutionalization [7, 35]. A spouse or other household member may help to maintain positive health behaviors, provide help in everyday tasks, and give assistance in obtaining formal community-based services, which help to maintain functional capacity and independency longer.
Receiving help from family members or relatives may thus be regarded as a preventive factor for LTC entry. On the other hand, an increased use of formal home care may reflect an increased need of help [7]. According to the results of the present study, those receiving help more often were more likely to enter into LTC. It may be that at certain point even a high amount of received help does not meet the needs, and is thereby associated with an increased probability of entering into LTC. It should be noted, however, that in addition to personal needs the probability of entering into LTC is affected by current care policies and availability of the resources [8].
Many previous population-based studies have found functional impairment, assessed by ADL or IADL functions or mobility, to be among the most important predictors of institutionalization among subjects 65 years or over [6,7,8, 12, 14]. Similarly in our study, dependency in mobility functions was a significant predictor of LTC entry when other potential predictors were included in the model. However, this association was no longer significant when risk of dying was taken into account. Additionally, poor self-rated health, although significant in the fully adjusted model, showed no longer statistically significant association with LTC entry when the risk of dying was taken into account. Both functional impairment and self-rated health have previously been shown to predict both nursing home placement [7, 16] and mortality [16, 24, 36]. Results of our analyses suggested that the associations of mobility limitations and self-rated health were stronger with mortality than with LTC entry among subjects aged 90 years or older.
Several earlier studies imply that age is an important predictor of institutionalization [6, 7, 9,10,11]. This was true also in our study, even if all participants were 90 years old or older. The contribution of age is likely mediated through functioning and chronic conditions, and in multivariate model it was no longer significant. Additionally, as age is a strong predictor of mortality, it was not an independent predictor of LTC when mortality was taken into account as competing risk.
This study adds important knowledge about predictors of LTC entry among subjects aged 90 years and older. The strengths of this study were that an entire age cohort of the study area was available, the follow-up time was exceptionally long for this age group (up to 11 years), and the response rate was high. Moreover, the linked data of the Finnish Care Registers for the information about LTC entry were available. Additionally, we were able to account for the selection effects due to mortality, which has been shown to be essential in accurate identification of predictors of LTC entry [16]. The main limitation of this study was that the information of potential predictors was based on self-reports. However, previous comparisons between self-reports of these data and corresponding hospital record data have shown sufficient reliability [37]. Additionally, the proxy responses for functioning and disease have been shown to be sufficiently reliable to be used in the analyses [38].
In conclusion, our findings in the population aged 90 years and older show that female gender, chronic conditions, living arrangements, and level of received help predicted LTC entry. As survival until the age of 90 years and the life expectancy at the age of 90 years are increasing, the number and proportion of nonagenarians will grow [2]. At the same time, no clear decrease in prevalence of disabling conditions such as dementia have been observed among the oldest old [19]. Additionally, the proportion of old people living alone has increased during the recent decades [39]. This will inevitably increase the need of care. Too be able to offer timely and appropriate care for the oldest old in future, it is essential to recognize these demographic changes, their impact on long-term care needs and demonstrated predictors of LTC entry.
References
Statistics Finland (2017) Population according to age and gender 1970–2016. http://pxnet2.stat.fi/PXWeb/pxweb/en/StatFin/StatFin__vrm__vaerak/?tablelist=true. Accessed 2017
Statistics Finland (2017) Population projection 2015 according to age and sex 2015–2065. http://pxnet2.stat.fi/PXWeb/pxweb/en/StatFin/StatFin__vrm/?rxid=3446fcc3-2523-4a81-9843-57e5cd9139dd. Accessed 2017
STAKES (2007) Care and services for older people 2005. National Research and Development Centre for Welfare and Health, Helsinki
Forma L, Aaltonen M, Pulkki J et al (2017) Long-term care is increasingly concentrated in the last years of life: a change from 2000 to 2011. Eur J Public Health 27:665–669
Sotkanet (2017) Statistics and Indicator Bank; National Institute for Health and Welfare 2005–2017. https://www.sotkanet.fi/sotkanet/en/index. Accessed 2017
Gnjidic D, Stanaway FF, Cumming R et al (2012) Mild cognitive impairment predicts institutionalization among older men: a population-based cohort study. PLoS One 7:e46061
Luppa M, Luck T, Weyerer S et al (2010) Prediction of institutionalization in the elderly. A systematic review. Age Ageing 39:31–38
Bharucha AJ, Pandav R, Shen C et al (2004) Predictors of nursing facility admission: a 12-year epidemiological study in the United States. J Am Geriatr Soc 52:434–439
Martikainen P, Moustgaard H, Murphy M et al (2009) Gender, living arrangements, and social circumstances as determinants of entry into and exit from long-term institutional care at older ages: a 6-year follow-up study of older Finns. Gerontologist 49:34–45
Grundy E, Jitlal M (2007) Socio-demographic variations in moves to institutional care 1991–2001: a record linkage study from england and wales. Age Ageing 36:424–430
Woo J, Ho SC, Yu AL et al (2000) An estimate of long-term care needs and identification of risk factors for institutionalization among Hong Kong Chinese aged 70 years and over. J Gerontol A Biol Sci Med Sci 55:M64–M69
von Bonsdorff M, Rantanen T, Laukkanen P et al (2006) Mobility limitations and cognitive deficits as predictors of institutionalization among community-dwelling older people. Gerontology 52:359–365
Nuotio M, Tammela TL, Luukkaala T et al (2003) Predictors of institutionalization in an older population during a 13-year period: the effect of urge incontinence. J Gerontol A Biol Sci Med Sci 58:756–762
Gaugler JE, Duval S, Anderson KA et al (2007) Predicting nursing home admission in the U.S: a meta-analysis. BMC Geriatr 7:13
Aguero-Torres H, von Strauss E, Viitanen M et al (2001) Institutionalization in the elderly: the role of chronic diseases and dementia. Cross-sectional and longitudinal data from a population-based study. J Clin Epidemiol 54:795–801
Castora-Binkley M, Meng H, Hyer K (2014) Predictors of long-term nursing home placement under competing risk: evidence from the health and retirement study. J Am Geriatr Soc 62:913–918
Murphy TE, Han L, Allore HG et al (2011) Treatment of death in the analysis of longitudinal studies of gerontological outcomes. J Gerontol A Biol Sci Med Sci 66:109–114
Jylhä M, Hervonen A (1999) Functional status and need of help among people aged 90 or over: a mailed survey with a total home-dwelling population. Scand J Public Health 27:106–111
Jylhä M, Enroth L, Luukkaala T (2013) Trends of functioning and health in nonagenarians: the vitality 90+ study. In: Robine J, Jagger C, Crimmins E (eds) Annual review of gerontology and geriatrics. Springer Publishing Company, pp 313–332
Statistics Finland (2017) Population structure 2016. http://www.stat.fi/tup/suoluk/suoluk_vaesto_en.html. Accessed 2017
Sund R (2012) Quality of the Finnish hospital discharge register: a systematic review. Scand J Public Health 40:505–515
Martikainen P, Moustgaard H, Einio E et al (2014) Life expectancy in long-term institutional care by marital status: multistate life table estimates for older Finnish men and women. J Gerontol B Psychol Sci Soc Sci 69:303–310
Vuorisalmi M, Pietilä I, Pohjolainen P et al (2008) Comparison of self-rated health in older people of St. Petersburg, Russia, and Tampere, Finland: how sensitive is SRH to cross-cultural factors? Eur J Ageing 5:327
Tiainen K, Luukkaala T, Hervonen A et al (2013) Predictors of mortality in men and women aged 90 and older: a nine-year follow-up study in the vitality 90 + study. Age Ageing 42:468–475
Statistics Finland (1976) Occupational and industrial classification. Statistics Finland, Helsinki
Fine JP, Gray RJ (1999) A proportional hazards model for the subdistribution of a competing risk. J Am Stat Assoc 94:496–509
Miller EA, Weissert WG (2000) Predicting elderly people’s risk for nursing home placement, hospitalization, functional impairment, and mortality: a synthesis. Med Care Res Rev 57:259–297
Nihtilä EK, Martikainen PT, Koskinen SV et al (2008) Chronic conditions and the risk of long-term institutionalization among older people. Eur J Public Health 18:77–84
Banaszak-Holl J, Fendrick AM, Foster NL et al (2004) Predicting nursing home admission: estimates from a 7-year follow-up of a nationally representative sample of older Americans. Alzheimer Dis Assoc Disord 18:83–89
Valiyeva E, Russell LB, Miller JE et al (2006) Lifestyle-related risk factors and risk of future nursing home admission. Arch Intern Med 166:985–990
Stuck AE, Walthert JM, Nikolaus T et al (1999) Risk factors for functional status decline in community-living elderly people: a systematic literature review. Soc Sci Med 48:445–469
Nihtilä E, Martikainen P (2008) Why older people living with a spouse are less likely to be institutionalized: the role of socioeconomic factors and health characteristics. Scand J Public Health 36:35–43
Grundy E, Glaser K (1997) Trends in, and transitions to, institutional residence among older people in England and Wales, 1971–91. J Epidemiol Community Health 51:531–540
Breeze E, Sloggett A, Fletcher A (1999) Socioeconomic and demographic predictors of mortality and institutional residence among middle aged and older people: results from the longitudinal study. J Epidemiol Community Health 53:765–774
Russell DW, Cutrona CE, de la Mora A et al (1997) Loneliness and nursing home admission among rural older adults. Psychol Aging 12:574–589
Jylhä M (2009) What is self-rated health and why does it predict mortality? Towards a unified conceptual model. Soc Sci Med 69:307–316
Goebeler S, Jylhä M, Hervonen A (2007) Self-reported medical history and self-rated health at age 90. Agreement with medical records. Aging Clin Exp Res 19:213–219
Vuorisalmi M, Sarkeala T, Hervonen A et al (2012) Among nonagenarians, congruence between self-rated and proxy-rated health was low but both predicted mortality. J Clin Epidemiol 65:553–559
Official Statistics of Finland (OSF) (2016) Families [e-publication]. Annual review 2011, 7. Middle-aged men live alone more often than women. http://www.stat.fi/til/perh/2011/02/perh_2011_02_2012–11-09_kat_007_en.html. Accessed 2016
Author information
Authors and Affiliations
Contributions
MK and MJ developed the study design and supervised this study. MK and JR performed statistical analyses. MK wrote the first draft. All authors contributed to analysis and interpretation of data, and drafting or critical revision of the manuscript.
Corresponding author
Ethics declarations
Funding
This study was supported by Grants from the Academy of Finland (Project 250602) and from the Competitive Research Funding by the Pirkanmaa University Hospital to MJ.
Conflict of interest
The authors declare that they have no conflict of interest.
Statement of human and animal rights
The study protocol was approved by the ethics committee of the Pirkanmaa Hospital District and the Ethics Committee of the Tampere Health Center.
Informed consent
All participants or their legal representatives gave their written informed consent.
Rights and permissions
About this article

Cite this article
Kauppi, M., Raitanen, J., Stenholm, S. et al. Predictors of long-term care among nonagenarians: the Vitality 90 + Study with linked data of the care registers. Aging Clin Exp Res 30, 913–919 (2018). https://doi.org/10.1007/s40520-017-0869-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-017-0869-6