
Abstract
Introduction
Dual task (DT) training is becoming prominent in fall prevention. However, DT training should include task-managing strategies like task switching or task prioritization to be beneficial to improve gait performance under DT conditions. The aim of this pilot study was to evaluate the effect of a task managing training on gait stability.
Methods
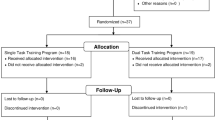
A DT training (12 sessions; 60 min each; 12 weeks) was compared to a non-training control group within a RCT (38 independent living participants; 72.7 ± 4.7 years). Single Task (ST) and DT walking (visual verbal Stroop task) were measured on a treadmill (FDM-T, 3.5 km/h, 100 HZ). Gait parameters like step length, step width, gait line, maximum forces and gait variability were compared.
Results
The training group improved their gait performance under ST and DT conditions as revealed by significant group × time interaction effects.
Discussion and conclusions
The training successfully improved gait performance and therefore might be a promising approach to prevent falls. Additional fall prevention studies should focus on motor–cognitive performance and reinforce outcomes of task managing strategies.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Walking means mobility and independence in old age. Therefore, fall prevention or mobility studies often focus on walking and gait stability. Gait stability describes dynamic motor–cognitive processes which are important for postural control during external perturbation [1]. From a biomechanical standpoint active rolling movements of the foot (from heel to toe) and ankle joint are necessary to maintain stability and to move forward simultaneously. Additionally, the center of mass has to be balanced over the base of support which also means that the pelvis needs to be stabilized from heel strike to midstance [1]. Thus, important characteristics of gait stability are the maximum ground reaction forces of the heel, mid- and forefoot, the gait line which describes the length of rolling movements and in addition, the step length and the step width. A review on kinematic measurements for gait stability in older adults observed variability of stride, swing and stance time as adequate parameters to discriminate fallers and non-fallers [2].
Since most activities of daily life require dual- or multi-task performance [3] and older adults’ suffer in those situations, many studies use a DT paradigm to investigate older adults gait stability [4–9]. Reduced DT performance is associated with an increased fall risk [3, 9–11]. Previous research observed higher gait variability and differences of step length in DT as compared to single task (ST) situations for older adults. Beauchet et al. [5] showed increased variability of step length and velocity as well as lower step length for older as compared to younger adults in DT situations. Springer et al. [7] reported that attention-demanding DT situations have a destabilizing effect with increased gait variability especially for older fallers. These reductions in DT performance can be described as DT costs (DTCs), indicating changes of walking kinematics which might be positive (e.g., reduced gait speed) or negative (e.g., reduced rolling movements with additional shift of plantar pressure) to maintain stability against perturbations. A review by Beurskens and Bock [12] revealed that age-related deficits in DT walking can mainly be observed during tasks which include visual control.
DTCs can also be observed as decrements in cognitive performance (e.g. increased reaction times). A review by Schäfer and Schumacher [13] reported that older adults show a tendency to prioritize the motor over the cognitive task. This occurs mainly in standing and walking tasks and might be a protecting factor against falling [13]. Particularly fallers in comparison to non-fallers showed reduced balance performance in DT situations, e.g. increased sway velocity, indicating that they have problems to shift attention to prioritize gait [7].
Considering these results, mobility training and fall prevention studies often aim to practice gait performance under DT conditions. Only few studies, however, explored the influence of a DT training intervention on gait stability in DT situations (for a review see [14]).
Motor (balance or strength) or cognitive training can improve DT performance in older adults [15, 16]. Training effects, however, are specific, in a way that pure motor training improves motor and pure cognitive training improves cognitive performance under DT conditions [17, 18], the DTCs are not necessarily diminished. The few existing DT trainings combining motor and cognitive tasks in DT settings are promising, but differ in their effects due to the specificity and design of the training [14].
Furthermore, DT training studies have been conducted to improve motor–cognitive DT performance while walking. A review by Wollesen and Voelcker-Rehage [14] summarized that DT walking performance was improved by only 4 of the identified 11 DT interventions [18, 19, 21, 22]. The studies reported improved cadence, gait variability and walking speed [19–22]. None of them focussed on kinematic variables or reported specific changes like active rolling movements of the feet which are important for gait stability. Moreover, cognitive DT training studies revealed transfer effects when the training fulfills specific criteria, that is a variable or randomized task switching training (switch of attention from one task to another [18, 23, 24]) or task prioritization training (focus on one of the tasks; [20, 24, 25]). In this context, a driving intervention and a balance training both with a variable task prioritization training, revealed positive transfer effects to new DT situations [25]. This leads to the assumption that variable cognitive–motor task prioritization training may also be successful to promote transfer [20] and results indicate that the continuous switch of attentional focus is one key factor to gain effects on DT performance. DT training with variable task priorities on the motor and cognitive tasks seems to be more effective than self-selected or fixed task priority training [18, 19].
Thus, it seems reasonable that mobility or fall prevention training should include variable task prioritization and task switching elements to assure transfer effects [14]. Moreover, the training protocols should include rising difficulties, a certain duration and level of task specificity to gain task-related adaptations and to improve cognitive and motor performance optimally [14]. Further, participants should acquire strategies how to switch between tasks and to prioritize the motor task when there is an unstable balance situation to avoid falling (task managing strategies). Integration and examination of all of these elements in DT training has not been done so far.
Accordingly, we developed and conducted a DT balance training which includes tasks to develop task managing strategies to master daily activities. The objective of this feasibility study was to evaluate the effect of a task managing training on gait stability under ST and DT conditions within a randomized controlled trail. We assumed that the training improves motor DT performance while walking in the relevant gait variables like step width, gait line, maximum forces of the heel, middle- and forefoot as well as for gait variability in step width and step length.
Methods/design
Participants
A priori sample size calculation (G*power 3.1., ANOVA: Repeated measures between factors; f = 0.5; alpha err prob 0.05; power 0.95, number of measurements = 2) calculated a total number of 42 participants.
38 participants (mean age = 72.7 ± 4.7 year) joined in the study. They were recruited using advertisements in common newspapers. The inclusion criteria were: independent living; age 70–85 years and mobility to join the group trainings.
Exclusion criteria were: acute or chronical diseases with a documented influence on balance control (e.g. Parkinson’s disease; diabetes); use of gait assistance (e.g. walking frames, rolling walkers). To avoid confounding factors of additional exercises, participants who participated in other exercises were excluded. Further participants with a score less than 10 points in the short physical performance battery (SPPB) were excluded [26] to avoid instability on the main outcomes due to motoric restricted participants Table 1.
The randomization process was conducted by a senior researcher not involved in the study. A web-based program (http://www.randomizer.org) was used. Randomization was stratified for sex and age. No significant group differences for the demographic and health-related data were found. The SPPB score for the intervention group was 11.2 ± 0.94 and for the control group 11.2 ± 0.95 at pre-test [F(2,36) = 0.47, p = .5, η 2p = 0.013].
Design
In this non-clinical group-based intervention, the training group received 12 sessions of group exercises during 12 weeks (once a week; 1 h each). This design was chosen in relation to refunding practice of the German health insurances. In Germany, prevention courses offered and compensated by the health insurance companies run for a maximum of 12 sessions, one session per week with a duration of 60–90 min for each session. Moreover, certain quality criteria defined for prevention programs have to be fulfilled such as quality of the exercise training, standardization of the program and qualification of the trainer [27]. Next to the DT training no other co-interventions like additional exercises or cognitive training were reported. Measurements for all groups were executed at baseline (pre-test, t1) and after 12 weeks (post-test, t2). Compliance was controlled by attendance lists. All participants took part in at least 10 out of 12 sessions (no drop outs).
Ethical considerations
The study was proofed by the ethics committee of the Hamburg Chamber of Physicians (registration number PV4376). All participants were informed about the study goals, and signed informed consent according to the Declaration of Helsinki.
Description of the intervention
The standardized group-based DT training included two phases with raising difficulties. The instructors were especially qualified and certified for the program.
Phase (1): training of daily actions with a huge fall risk (weeks 1–6)
Phase (1) focused on daily situations which are associated with an increased fall risk like challenging walking exercises (e.g. brisk walking, starting, stopping, avoiding obstacles, sidesteps, turns). Moreover, the participants had to pay attention to tripping hazards, speed rating, etc. (including visual and proprioceptive tasks), had to execute tasks with reduced area of support, in order to compensate balance disturbances or motor and cognitive DT with visual stimulus. In these exercises they had to manage the tasks with different focus of attention, i.e., prioritization of the motor task, the cognitive task or both tasks at the same time (task managing). All exercises were accompanied with additional standardized explanations by the instructors as verbal feedback for the whole group to improve task managing. Examples of different body positions and motor actions and their influence on the shift of the center of mass were given and the different strategies to maintain, e.g., balance were practiced. It was exemplified why the conducted tasks are important for fall prevention and which mechanisms of movement organization (how to maintain balance while starting/stopping; one leg balance with ankle, hip or knee strategy) and postural control (influence of vision on balance) were trained. Moreover, examples were given to reflect the importance of these mechanisms for balance control in daily situations.
Phase (2): training of task prioritization, task switching and transfer (week 7–12)
In phase (2) the tasks became more complex and all tasks from the first phase were trained under DT conditions combined with precision tasks, time pressure, task prioritization and task switching. Daily situations were imitated and task managing strategies, as described above, under DT balance situations were built up.
Control group
The control group did not receive any exercises for 12 weeks and participated in exercises after the intervention groups had finished their training.
Test instruments and measurements
The measurements included a 30-s walking test at constant speed on a treadmill (FDM-T, 3.5 km/h—following Peel et al. [28] who revealed 3.48 km/h as the medium gait speed for unhealthy persons and 5.34 km/h as maximum gait speed for healthy older adults) [28] the 3.5 km/h was chosen as a comfortable, manageable gait speed for all participants under ST and DT conditions). Participants practiced treadmill walking before the test session to become familiar with the task until they felt comfortable. In the DT condition, a visual–verbal Stroop test with 16 events of incongruent color words, e.g., the word “blue” presented in a different color, e.g., in yellow letters was added. Stimuli were projected onto a white wall 2 m in front of the participants. Participants had to name the color of the font letters word and to inhibit reading the word. For this pilot study the quality of gait performance under DT conditions represents the ability of task managing while walking.
Gait parameters as step length, step width, and gait line as well as the vertical maximum impact (maximum forces of heel, midfoot and forefoot) were measured as main outcome parameters. Force data were collected for both feet 100 Hz. The variability of gait parameters was analyzed with standard deviation (SD) and coefficient of variation (SD/mean value [29]). Motor DTCs were calculated with ST-DT/ST*100 (following [30]).
Analysis
The data were analyzed with SPSS © 16.0. using repeated measures ANOVAs with Group (control group, DT training) as between subject factor and measurement point (pre, post) as within subject factor. Outcome variables were the gait parameters (gait kinematics, maximum forces, gait variability) under ST and DT conditions and DTC). Effect sizes are given as partial eta squares (η 2p ). The level of significance was set to p < 0.05.
Results
Walking variables under ST conditions
Gait kinematics
With regard to the gait kinematics under ST task conditions there was no significant change of step length from pre- to post-test, no significant group effect and no significant group × time interaction. Step width decreased from pre- to post-test [F(1,36) = 15,1, p = .00; η 2p = 0.295] in both groups (intervention group, −2 cm; control group −1.89 cm; cf. Table 2). We found, however, no group effect and no group × time interaction. The gait line increased significantly for both feet after 12 weeks of training [left foot: F(1,36) = 4.64, p = .038, η 2p = 0.114; right foot: F(1,36) = 6.09, p = .019, η 2p = 0.145]. This increase was more pronounced in the intervention group for the left (+15.95 mm) and the right foot (+17.68 mm), whereas it was less in the control group (+5.45 mm left; +8 mm right foot). These differences resulted in a significant group × time interaction for both feet [left: F(2,36) = 9.05, p = .005, η 2p = 0.206; right: F(2,36) = 10.65, p = .002; η 2p = 0.233] and significant between subject effects [left: F(1,36) = 11.67, p = .002, η 2p = 0.245; right: F(1,36) = 14.93, p = .000; η 2p = 0.293] (cf. Table 2 for descriptives).
Maximum forces
The mean maximum forces decreased significantly from pre- to post-test in both groups (left, intervention group −36.79 N; control, −17.68 N, F(1,36) = 11.27, p = .002; η 2p = 0.239; right, intervention group −40.05 N; control, −19.11 F(1,36) = 13.57, p = .001; η 2p = 0.274). Group effects were not significant and the group × time interaction was only significant for maximum forces of the right foot (F(2, 36) = 4.37; p = .044; η 2p = 0.111). Comparing the maximum forces of the heel, mid- and forefoot, there was no group effect and but a significant pre-post effect for the heel forces (left: +18.16 N intervention group; +30.61 N control group, F(1,36) = 6.63, p = .014, η 2p = 0.156; right: +34.42 N intervention group; +17.61 N control group, F(1,36) = 4.824, p = .035, η 2p = 0.118). The group × time interaction for the maximum heel forces of the right foot indicate that the forces of the intervention group increased to a higher extend from pre- to post-test then of the control group [F(2,36) = 5.354; p = .027, η 2p = 0.129; cf. Table 2]. Additionally, there was a significant group effect for the midfoot [left: F(1,36) = 4.52, p = .033, η 2p = 0.120; right: F(1,36) = 6.08, p = .013, η 2p = 0.155].
Gait variability
Significant pre- to post-test differences in step length were found [F(1,36) = 3.73, p = .000; η 2p = 0.912], but no significant group effect. The SD of step length under ST condition decreased significantly in both groups for the right foot (left: intervention group −0.47; control group −0.51; right −0.28 intervention group; −0.40 control group). There was no interaction effect. The coefficients of variation showed the same results (left: intervention group −1.37; control group −1.02; right −0.89 intervention group; −0.82. control group; F(1,36) = 6.36 p = .016; η 2p = 0.150). There were no group and no group × time interaction effects and no effects for differences in step width.
Walking variables under DT conditions
Gait kinematics
Step width declined from pre- to post-test [intervention group −1.32; control group −0.77 F(1,36) = 9.559, p = .004, η 2p = 0.210], intervention and control group differed not significantly. However, the group × time interaction was significant [F(2,36) = 16.538, p = .00, η 2p = 0.321]. There were no significant effects for step length (cf. Table 3).
Moreover, the gait line increased after the training (left, intervention group +2.5 mm; control group +0.61 mm; right, intervention group +5.58 mm; control group, +0.61 mm) with significant group differences for both feet [left: F(1,36) = 10.6, p = .00; η 2p = 0.226; right: F(1,36) = 12.71, p = .001; η 2p = 0.261] and a significant group × time interaction for the right foot [F(2,36) = 6.867, p = .013, η 2p = 0.164].
Maximum forces
There was a main pre–post effect for the maximum forces which decreased for both feet (left: intervention group −39.58; control −6.52; F(1,36) = 6.984, p = .012; η 2p = 0.162; right: intervention group −41.68; control −4.53; F(1,36) = 6.026, p = .019; η 2p = 0.143) and no group effects. The group × time interaction was only significant for maximum forces of the left foot [F(2, 36) = 5.581; p = .024; η 2p = 0.131]. In addition, there was a significant group × time interactions for maximum forefoot forces of the left foot; in the intervention group the maximum forces (−13.79 N) decreased to a higher amount than in the control group [−12 N; F(2,36) = 8.48, p = .005; η 2p = 0.197]. No other developments of the maximum forces were observed.
Gait variability
The analysis of the gait variability under DT conditions revealed a decline from pre- to post-test for the SD of the step length for both feet [left: intervention group −0.67; control: −0.56; F(1,36) = 12.41 p = .001; η 2p = 0.001; right: intervention group −0.74; control −0.15 F(1,36) = 6.44; p = .016; η 2p = 0.125]. Group effect and group × time interaction were not significant. The variability of the step width (CoV) increased in the intervention group (+0.15) and decreased in the control group (−0.3) with no significant effects. The CoV of the step length decreased as well (left: intervention group −1.74; control −1.20; right: intervention group −1.89; control: −0.19) significant from pre- to post-test [left: F(1,36) = 10.386; p = .023; η 2p = 0.224; right: F(1,36) = 5.61; p = .023; η 2p = 0.135]. Group effects and the group × time interaction were not significant.
Dual task costs
Overall, DTCs significantly decreased for gait line [left: intervention group −16.61; control −0.29 F(1,36) = 4.44; p = .042; η 2p = 0.110; right: intervention group −14.71; control −1.28 F(1,36) = 5.14; p = .029; η 2p = 0.125]. Group effects failed to be significant and the group × time interaction for the left foot was significant [left: F(2, 36) = 4.14; p = .049; η 2p = 0.103; right: F(2, 36) = 3.67; p = .063; η 2p = 0.092] indicating a higher decline in DTCs for the interventions as compared to the control group.
Discussion
The aim of this randomized controlled study was to examine the feasibility and the effects of a DT intervention with task managing strategies on ST and DT motor performance while walking. The overall aim of the intervention was the reduction of fall risks in older adults by investigating changes in gait stability and gait variability, two parameters known to be indicators of fall risks. Therefore common kinematic walking variables (e.g. step width, step length) and kinetic gait variables like maximum forces under ST and DT conditions were analyzed. These factors describe an active use of the ankle joint and roll movements, which is an important factor to compensate gait disturbances and maintain postural control [1].
The results showed a significantly increased gait line in the intervention group after 12 weeks of training accompanied with a shift of the maximum forces from midfoot to the heel under ST conditions. This might lead to the conclusion that there is an improvement of the foot roll movements leading to a more balanced, less accident-sensitive gait pattern with an accentuated heel strike as described by Perry [1]. We cannot prove this within our study, however, there are different possible explanations for this result. First, according to previous study results of Long and colleagues [31] with comparable training movements (e.g. heel raises, single leg stand) one might conclude that the intervention improved the range of motion of the ankle joint and the involved muscle activation and coordination leading to a more controlled foot posture and roll-over movements [31]. Second, the intervention based on different strategies to manage balance control including tasks which need an expansion of the limits of stability. Task performance required to compensate large amplitudes of motions of the hip, knee and ankle joints. Therefore increased range of motion of the ankle joint is necessary. This might explain the observed group differences of the gait line and the maximum forces under ST condition. Future studies should verify this hypothesis by the use of mobility tests like, for example, the Star execution balance test [32] as control variable. Under DT conditions the same tendency could be observed (reduced DTCs for the gait line in the intervention group). Following the reduced resources allocation model by Kahnemann [33], one might argue that under DT conditions a higher amount of attention is needed to manage both tasks similarly. This results in DTCs for one of the tasks. Nevertheless, motor performance under DT conditions improved in the intervention group to a higher amount than in the control group, pointing to a better resource allocation under DT conditions. This hypothesis should be proven in future studies by examining the DTCss for cognitive performance in order to get more insights into the intervention effects, e.g., whether the intervention frees up also cognitive resources.
Except for the variability of the step width, the intervention group gained reduced gait variability under DT conditions. According to Springer et al. [7] a high variability has a destabilizing effect. Thus, the reduced variability indicates a more stable gait pattern even under the more conflicting DT conditions.
Controversially to previous results [2] our study did not reveal improvements in step length under ST or DT conditions. We used a fixed gait speed, which might have influenced the range of adaptations within this gait parameter because gait speed determines the step length. However, a review by Bock and Beurskens [34] revealed that walking on a treadmill in comparison to normal walking did not influence older adults DT walking performance. Additionally, gait analysis with respect to age, gender, and speed showed that most values of plantar pressure were determined by gait velocity and body mass [35]. Moreover, older participants increase stride length and frequency to manage the same gait velocity of younger participants [35]. These changes are accompanied with an increased maximum of the plantar pressure. Future studies on plantar pressure should use a relative gait velocity, i.e. as a percentage of the individual preferred speed [36] and analyze gait velocity in relation to individuals’ body mass to control for confounding factors on the internal validity. Also, the differences between preferred and fixed gait speed have to be controlled for to assign the DT effects.
After all, the intervention group showed significant improvements of relevant gait patterns under DT conditions. Due to the fact that walking with visual–verbal Stroop task was not part of the training intervention one might conclude that these improvements are a result of the exercise program. Nevertheless the duration of the intervention has to be enlarged to control whether the differences between the intervention and control group might increase. Another reason for the increased performance of the intervention group might be that the intervention improved DT managing strategies. Future studies should use additional tests to verify that the intervention can build up or change DT managing strategies.
Limitations of the study
One limitation is that also the control group improved gait patterns, probably because they get used to walking on the treadmill. In future studies these learning effects might be controlled for by an extended practice phase and the choice of one’s preferred walking speed. However, as indicated by the significant group × measurement point interactions, improvements in the experimental group exceed those of the control group, at least for gait line and variability under DT conditions illustrating the positive benefits of the intervention. Another limitation is that DTCs for the Stroop test are missing. Moreover, a ST training group and a DT training group without task managing training should be included to specify the DT and task managing training effects.
Conclusions
The feasibility study showed some important results for future DT training interventions including task managing strategies. It has been shown that the active rolling movements of the feet increased under ST and DT conditions and the gait variability decreased. Therefore, we conclude a raise of gait stability which is important for mobility and prevention of falls in older adults. The duration and evaluation of the program should be enlarged, e.g., to show effects on motor and cognitive DTCs as well as on task managing strategies.
References
Perry J (2003) Ganganalyse: Norm und Pathologie des Gehens. Urban & Fischer, München
Hamacher D, Singh NB, Van Dieen JH, Heller MO, Taylor WR (2011) Kinematic measures for assessing gait stability in elderly individuals: a systematic review. J R Soc Interface 8(65):1682–1698
Faulkner KA, Redfern MS, Cauley JA, Landsittel DP, Studenski SA, Rosano C et al (2007) Multitasking: association between poorer Performance and a history of recurrent falls. JAGS 55:570–576
Beauchet O, Kressig RW, Najafi B, Aminian K, Dubost V, Mourey F (2003) Age-related decline of gait control under dual-task condition. J Am Geriatr Soc 51:1187–1188
Beauchet O, Dubost V, Aminian K, Gonthier R, Kressig RW (2005) Dual-Task-related gait changes in the elderly: does the type of cognitive task matter? J Mot Behav 37:259–264
Hollmann JH, Kovash FM, Kubik JJ, Linbo RA (2006) Age-related differences in spatiotemporal markers of gait stability during dual task walking. Gait Posture 26:113–119
Springer S, Giladi N, Peretz C, Yogev G, Simon ES, Hausdorff JM (2006) Dual-tasking effects on gait variability: the role of aging, falls and executive function. Mov Disord 21(7):950–957
Yogev-Seligmann G, Rotem-Galili Y, Mirelmann A, Dickstein R, Giladi N, Hausdorff JM (2010) How does explicit prioritization alter walking during dual-task performance? Effects of age and sex on gait speed and variability. Phys Ther 90(2):177–186
Al-Yahya E, Dawes H, Smith L, Dennis A, Howells K, Cockburn J (2010) Cognitive motor interference while walking: a systematic review and meta-analysis. Neurosci Biobehav Rev 35:715–728
Siu K-C, Lugade V, Chou L-S, van Donkelaar P, Woollacott MH (2008) Dual-task interference during obstacle clearance in healthy and balance-impaired older adults. Aging Clin Exp Res 20(4):349–354
Woollacott M, Shumway-Cook A (2002) Attention and the control of posture and gait: a review of an emerging area of research. Gait Posture 16:1–14
Beurskens R, Bock O (2012) Age-related deficits of dual-task walking: a review. Neural Plasticity. doi:10.1155/2012/131608
Schäfer S, Schumacher V (2011) The interplay between cognitive and motor functioning in healthy older adults: findings from dual-task studies and suggestions for intervention. Gerontology 57:239–246
Wollesen B, Voelcker-Rehage C (2014) Training effects on motor–cognitive dual-task performance in older adults. Eur Rev Aging Phys Act 11(1):5–24
Doumas M, Smoklers C, Krampe RT (2008) Task prioritization in aging: effects of sensory information on concurrent posture and memory performance. Exp Brain Res 187:275–281
Voelcker-Rehage C, Alberts JL (2007) Effect of motor practice on dual-task performance in older adults. J Gerontol Psychol Sci Soc Sci 62(3):141–148
Bherer L, Kramer AF, Peterson MS, Colcombe S, Erickson K, Becic E (2008) Transfer effects in task-set cost and dual-task cost after dual-task training in older and younger adults: further evidence for cognitive plasticity in attentional control in late adulthood. Exp Aging Res 34(3):188–219
Silsupadol P, Lugade V, Shumway-Cook A, van Donkelaar P, Chou LS, Mayr U, Woollacott MH (2009) Training-related changes in dual-task walking performance of elderly persons with balance impairment: a double-blind, randomized controlled trial. Gait Posture 29(4):634–639
Silsupadol P, Shumway-Cook A, Lugade V, van Donkelaar P, Chou LS, Mayr U et al (2009) Effects of single-task versus dual-task training on balance performance in older adults: a double-blind, randomized controlled trial. Arch Phys Med Rehabil 90:381–387
You JH et al (2009) Effects of dual-task cognitive-gait intervention on memory and gait dynamics in older adults with a history of falls: a preliminary investigation. NeuroRehabilitation 24:193–198
Toulotte C, Thevenon A, Fabre C (2006) Effects of training and detraining on the static and dynamic balance in elderly fallers and non-fallers: a pilot study. Disabil Rehabil 28:125–133
Trombetti A, Hars M, Herrmann FR, Kressig RW, Ferrari S, Rizzoli R (2011) Effect of music-based multitask training on gait, balance, and fall risk in elderly people: a randomized controlled trial. Arch Intern Med 171(6):525–533
Li KZ, Roudaia E, Lussier M, Bherer L, Leroux A, Kinley PA (2010) Benefits of cognitive dual-task training on balance performance in healthy older adults. J Gerontol A Biol Sci Med Sci 65(12):1344–1352
Jaeggi SM, Buschkuehl M, Jonides J, Perrig WJ (2008) Improving fluid intelligence with training on working memory. Proc Natl Acad Sci 105(19):6829–6833
Cassavaugh ND, Kramer AF (2009) Transfer of computer-based training to simulated driving in older adults. Applied Ergonomics 4:943–952
Guralnik JM, Simonsick EM, Ferrucci L, Glynn RJ, Berkman LF, Blazer DG et al (1994) A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol 49:M85–M94
GKV-Spitzenverband (2010) Leitfaden Prävention. Handlungsfelder und Kriterien des GKV-Spitzenverbandes zur Umsetzung von §§20 und 20a SGB V. GKV-Spitzenverband, Berlin
Peel NM, Kuys SS, Klein K (2012) Gait speed as a measure in geriatric assessment in clinical settings: a systematic review. J Gerontol A Biol Sci Med Sci 68(1):39–46
Faude O, Donath L, Roth R, Fricker L, Zahner L (2012) Reliability of gait parameters during treadmill walking in community-dwelling healthy seniors. Gait Posture 236(3):444–448
Doumas M, Rapp MA, Krampe RT (2009) Working memory and postural control: adult age differences in potential for improvement, task priority, and dual tasking. J Gerontol Series B Psychol Sci Soc Sci 64(2):193–201. doi:10.1093/geronb/gbp009
Long L, Jackson K, Laubach L (2013) A home-based exercise program for the foot and ankle to improve balance, muscle performance and flexibility in community dwelling older adults: a pilot study. Int J Phys Med Rehabil 1:120. doi:10.4172/2329-9096.1000120
Kinzey SJ, Armstrong CW (1998) The reliability of the star-excursion test in assessing dynamic balance. J Orthop Sports Phys Ther 27:356–360
Kahnemann D (1973) Attention and effort. Prentice Hall, Englewood Cliffs
Bock O, Beurskens R (2011) Age-related deficits of dual-task walking: the role of foot vision. Gait Posture 33:190–194
Wollesen B, Mattes K (2013). The influence of gait velocity, gender and age on plantar pressure of seniors under DT conditions. In: Balagué N, Torrents C, Vilanova A, Cadefau J, Tarragó R, Tsolakidis E (eds) 18th Congress ECSS, Barcelona, Spain. Book of Abstracts, 423. ISBN 978-84-695-7786-8
Chung MJ, Wang MJ (2012) Gender and walking speed effects of plantar pressure distribution for adults aged 20–60 years. Ergonomics 55(29):194–200
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Wollesen, B., Voelcker-Rehage, C., Willer, J. et al. Feasibility study of dual-task-managing training to improve gait performance of older adults. Aging Clin Exp Res 27, 447–455 (2015). https://doi.org/10.1007/s40520-014-0301-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-014-0301-4