
Opinion statement
Behavioral economic and neuroeconomic understandings of addiction offer both established and empirically supported treatments as well as a foundation from which promising new treatment options are emerging. Addiction must be understood and treated as a state of pathological overvaluation of the reinforcement of drug use fueled by an imbalance of the competing neurobehavioral decision systems that govern decision making (CNDS theory). The CNDS theory presents two systems, the executive and impulsive, which are dysregulated in reinforcer pathology by greater relative control of the impulsive, hedonic system, and lesser relative control of the executive, regulatory system. This leads to a reinforcer pathology where drug use is maladaptively overvalued in comparison to other reinforcers, leading to a chronic and often relapsing state of addiction. Some treatments which directly alter economic variables associated with drug use have already been empirically supported, including contingency management (which increases the short-term price of drug use) and drug agonist therapies (which decrease the short-term value of drug use compared to other reinforcers). New, promising treatments which bring the fundamental CNDS dysregulation of addiction into balance include episodic future thinking, which increases the temporal window over which the opportunity costs of drug use are integrated by engaging executive control, and TMS therapies which directly increase activity, and therefore relative control, in the executive system. The maturing fields of behavioral economics and neuroeconomics provide conceptual understanding of the competing neurobehavioral decision systems theory (CNDS) and reinforcer pathology (i.e., high valuation of and excessive preference for drug reinforcers), allowing us to coherently categorize treatments into a theoretically comprehensive framework of addiction. In this chapter, we identify and clarify how existing and novel interventions can ameliorate reinforcer pathology in light of the CNDS and be leveraged to treat addiction.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Behavioral economics, the field resulting from the combining of economics with important aspects of psychology, began to be applied to addiction in 1990 [1]. Approximately a decade later, neuroeconomics [2], which incorporated neuroscience, economics, and aspects of decision science, developed and was later applied to addiction [3]. The congress of behavioral economics and neuroeconomics has contributed substantially to the field of addiction. Among those contributions include a new conceptual understanding of addiction [4, 3, 5] identifying neural substrates contributing to addictive behaviors [6], clarifying the relationship between measures of impulsivity and executive function [7], evolving the measurement of those dual systems, providing novel methods for the analysis of abuse liability of substances [8, 9], and expanding the range of phenomena to which it has been applied [10, 9].
A more recent contribution of behavioral economic and neuroeconomic approaches is an important relatively new conceptual understanding of addiction referred to as reinforcer pathology [11] [12•]. Reinforcer pathology refers to the combined effects of (1) high valuation for immediate drug reinforcers and (2) an excessive preference for immediate acquisition of a reinforcer in spite of negative long-term consequences. The combination of these two factors may be important contributors to the addictive process. Thus, treatments and interventions that can reduce either of these effects may be important for diminishing addictive behaviors and may contribute to our understanding of therapeutic efficacy.
As the behavioral economics and neuroeconomics of addiction have matured, these fields have begun to focus their attention on developing interventions that can alter and change either of these two processes of reinforcer pathology or the addictive behavior itself. Moreover, the conceptual understanding of behavioral economics and neuroeconomics has led to reinterpreting interventions and treatments into theoretically coherent categories that contribute to a comprehensive approach to addiction. The goal of this paper is to elucidate the conceptual approach of the behavioral economics and neuroeconomics of addictive behaviors by identifying and clarifying how existing and novel interventions can be integrated into a conceptually coherent perspective.
The competing neurobehavioral decision systems theory of reinforcer pathology
The competing neurobehavioral decision systems (CNDS) approach is a theory developed within neuroeconomics that specifies neural underpinnings of reinforcer pathology, as well as unique insights into the etiology and treatment of addiction [3] [7] [13•] [14]. The CNDS theory is a dual system approach that assumes that behavior is the product of two competing neural systems: (1) the reward-driven impulsive system, which comprises limbic and paralimbic brain regions (e.g., anterior cingulate cortex and nucleus accumbens), and (2) the evolutionarily newer executive system, which governs self-regulatory processes (e.g., planning and behavioral inhibition) and comprises prefrontal and parietal brain regions (e.g., dorsolateral prefrontal cortex; dlPFC). A variety of dual decision systems have been proposed to account for normative and non-normative decision-making (e.g., [15, 16]), although the CNDS theory is the only system focusing on addiction. In the CNDS theory, interactions between decision systems reflect a neuroeconomic understanding of the two components of reinforcer pathology, wherein addiction is the product of a hyperactive impulsive system and/or hypoactive executive system.
The interaction between impulsive and executive systems and their corresponding effects on behavioral control are represented in Fig. 1. The x- and y-axes depict the relative strength of each system, with interacting system strengths in this two-dimensional space ranging from dominant control by the impulsive system and high risk for reinforcer pathology (black) to dominant control by the executive system and low risk for reinforcer pathology (white). When systems are in balance (diagonal line), an individual may occasionally seek short-term, hedonic satisfaction associated with the impulsive system (e.g., overeating) but also engages in long-term, self-controlled pursuits (e.g., saving for retirement). In contrast, the behavior of individuals falling at the extreme ends of the color gradient is almost exclusively controlled by either short- or long-term sources of reinforcementFootnote 1 [17, 18].

Behavioral control in the competing neurobehavioral decision systems theory. Combined strengths of the impulsive and executive systems may fall at any coordinate in this two-dimensional space, with behavior controlled by relative contributions of each system (see color gradient). The diagonal line represents regulatory balance between impulsive and executive systems. In this illustration, interacting system strengths falling at coordinates a and b produce identical levels of impulsive behavior, with both producing more impulsive behavior than those at coordinate c.
One component of reinforcer pathology as it relates to addiction is excessive valuation of drug reinforcement [19], which may be measured directly through the assessment of demand elasticity for drugs of abuse (i.e., sensitivity of drug consumption to increases in price; see [20]; [21•]). In this view, estimates of demand elasticity provide straightforward measures of value because they reflect the extent to which an individual will defend consumption of a given drug across increasing price. In recent years, several studies have documented robust associations between drug demand and either addiction severity (e.g., [22], [23] [24] [25]) or drug treatment failure [26]. From the perspective of the CNDS theory, excessive valuation of drug reinforcement is a product of relatively greater control of the impulsive over the executive decision systems.
The second component of reinforcer pathology is persistent drug use despite negative, long-term consequences [19]. Such disregard for the delayed outcomes associated with drug use suggests a rapid devaluation of future events. Thus, one measure of the relative activation of the impulsive and executive systems is delay discounting or the devaluation of reinforcement with increasing delay. Accumulating evidence demonstrates that high discounting rates are cross-sectionally and longitudinally associated with addiction (e.g., [27]; [28]; for review and meta-analysis, see [29, 30]). Such findings are consistent with the view that delay discounting plays an etiological role in addiction, as rapid devaluation of the delayed reinforcement associated with drug abstinence (e.g., long-term psychological and physical health) likely increases the reinforcing efficacy of immediate drug reinforcement. Consistent with the CNDS theory, high rates of delay discounting may be the product of relatively greater control of the impulsive over the executive decision system (e.g., see points A and B in Fig. 1). This possibility is further supported by reports in which rates of delay discounting are correlated with differential age- or species-dependent development of the impulsive and executive systems (e.g., [13•]; [31] [32]; [33]; [34]).
In the following sections, we provide overviews of interventions emerging from behavioral economic and neuroeconomic research on drug demand and delay discounting.
Drug demand
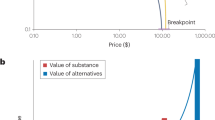
Reinforcer pathology is characterized, in part, by excessive valuation of select commodities. Excessive valuation of drugs is often measured by behavioral economic analyses of demand consisting of two interrelated concepts: (1) elasticity of demand, which is the sensitivity of consumption to price increases, and (2) intensity of demand, which is the level of consumption at near zero cost. Therapeutic opportunities targeting drug demand can shift consumption along an individual’s curve (i.e., increasing the price of the drug), shift the entire demand curve to a lower level (i.e., reducing the valuation of the drug across all prices), and/or shift the elasticity of the demand curve (i.e., increasing sensitivity to price) [35] [36].
Single commodity demand
When considering elasticity, the primary predictor of consumption is unit price or the cost-benefit ratio of the commodity cost to the magnitude of benefit of the reward. Unit price stipulates that the same consumption should be achieved at the same unit price regardless of the price’s constituents; that is, consumption is the same whether the unit price of 10 is achieved by 10 responses for 1 unit of drug or 100 responses for 10 units of drug [1, 37]. Thus, consumption of a substance can be decreased by increasing the unit price to obtain it (e.g., [38, 39, 39]).
Contingency management
Contingency management increases the price of substance use by adding an immediate incentive for abstinence that will be forfeited by drug consumption. This treatment delivers incentives such as money, vouchers, or prizes contingent on drug abstinence and is effective in stimulant, opioid, marijuana, and tobacco use (see [40] for meta-analysis). Contingency management has been used to encourage other healthy behaviors such as weight loss and medication adherence. This treatment uses a specialized form of price referred to as opportunity cost [41]. For example, if an individual has the choice between using an illicit drug now or receiving $3 at their next appointment and chooses to use the illicit drug, the opportunity cost of using the drug is $3. These incentives are then offered over repeated appointments and can encourage a reduction in consumption that allows for contact with alternative prosocial, therapeutic reinforcers that may later decrease overall drug valuation. In this way, contingency management decreases consumption by increasing the unit price of drug use, decreasing the relative control of the impulsive decision system.Footnote 2
Cost-focused motivational interventions
Another way to increase the opportunity cost of substance consumption is cost-focused motivational intervention. These interventions combine behavioral economic enhancements and traditional treatments to alter drug consumption by increasing awareness and salience of delayed consequences of substance use [42]. These cost-focused motivational interventions emphasize the opportunity costs associated with substance use, such as lost productivity and health (e.g., [43]). However, unlike contingency management, these interventions do not directly increase cost; rather, they increase salience of natural consequences. These treatments have been tested in problematic alcohol and marijuana use in early adulthood and have been shown to reduce drug use, though not uniformly, while increasing the relative value of prosocial reinforcers [44, 45]. As such, cost-focused motivational interventions shift the relative control of the competing decision systems in favor of the executive.
Transcranial magnetic stimulation
A neuroeconomic intervention may effectively reduce the overall demand curve by reducing the reward valuation across prices. For example, decreased cigarette consumption [46] [47] and cocaine use [48] following repeated administration of a non-invasive neurotherapeutic brain stimulation technique, transcranial magnetic stimulation (TMS), suggests decreased reward valuation. This decrease in consumption following administration of repetitive TMS (rTMS) to the dlPFC is consistent with increasing the relative control of the executive decision system of the CNDS. What remains to be determined is whether this intervention functions as a shift in the demand curve or, rather, increases unit price indirectly (see below for a discussion of the effects of TMS on delay discounting, the second reinforcer pathology subtype).
Cross-price drug demand
Real-life choices often require us to choose between more than one commodity at the same time. The economic relationship between multiple commodities at varying prices is called cross-price demand elasticity. If the price of one commodity is increased and consumption of a second increases, the second commodity is a substitute; if consumption of the second decreases, it is a complement; and if it stays the same, it is an independent. Importantly, substitutes, complements, and independents exist on a continuum where substitutes and complements make up the two extremes and independents fall in the middle [49]. For example, both denicotinized cigarettes and gum function as substitutes as the price of cigarettes increases [50]; however, money functions as an independent [51]. Experimental studies of human behavior demonstrate how consumption of different commodities, such as addictive substances, is altered when price changes. Thus, cross-price demand interactions inform how purchase patterns will change in response to price manipulations.
Community reinforcement approach
Experimental evaluation of cross-price demand has set the stage for therapeutic interventions that are based on a tradeoff between substance use and alternative forms of reinforcement. The community reinforcement approach, a treatment where prosocial activities are encouraged, while substance use is discouraged, leverages cross-commodity substitution to combat substance use disorders. Given that excessive valuation of substances result, in part, from the paucity of alternatively available reinforcers by facilitating employment, community, recreation, and family opportunities, new behaviors can compete with substance use as viable reinforcers. The treatment forces a tradeoff between interdependent choices of substance use and prosocial reinforcers. For example, a patient can choose between incompatible behaviors such as drinking at the bar or spending time playing in a community sports league. In this way, the community reinforcement approach decreases relative impulsive decision system control by discouraging drug use while simultaneously increasing relative executive decision system control by nurturing prosocial behaviors. The community reinforcement approach, alone and in conjunction with contingency management, outperforms comparator treatments including 12-step and standard outpatient treatment [52] [53] [54] [55].
Drug agonist therapies
In addition to behavioral interventions, pharmacological interventions seek to provide a substitute for drugs of abuse. Though no FDA-approved medications for the treatment of stimulant dependence exist [56], approved medications for the treatment of opioid, nicotine, and alcohol dependence are available and function as substitutes by decreasing drug demand through both positive and negative reinforcement [12•]. For example, opioid replacement therapies, including methadone [57] and buprenorphine [58], provide alternative, possibly less addictive, and better - controlled alternatives to treat dependence. Though no current research directly investigates the effects of pharmacotherapy on reinforcer demand, the mechanism by which agonist replacement therapies function suggests that demand may be decreased [12•]. That is, these medications may function mechanistically by decreasing relative control of the impulsive decision system to decrease drug demand. When used in conjunction with behavioral interventions, such as contingency management or the community reinforcement approach, drug agonist therapies may be highly efficacious and offer the benefit of providing alternative reinforcers for both the external and internal reinforcing properties of substances [59].
Drug demand summary
In summary, behavioral economic laboratory studies have elucidated the relationship between addictive substances and the excessive demand subtype of reinforcer pathology. Experimental research on demand processes supports interventions including contingency management, cost-focused motivational interventions, TMS, the community reinforcement approach, and agonist replacement therapies. The reinforcer pathology perspective has contributed to the development of some of the therapies reviewed above and in other cases provides a theoretical understanding in order to develop new and employ existing treatments.
Delay discounting
Delay discounting can be used to measure the extent to which an individual has an excessive preference for immediate acquisition of a reinforcer. High rates of discounting measured by choice of smaller, immediate rewards over larger, delayed rewards is associated with substance use, overeating, and excessive gambling (see [19] for review). Excessive preference for immediate rewards may be described as a trans-disease process [60•], wherein hyperactivation of the impulsive system and/or hypoactivation of the executive system act in concert to produce these maladaptive behaviors [3]. While some interventions seek to decrease the relative control of the impulsive decision system, we hypothesize that amplification of the executive decision system will enhance self-control in order to decrease substance use. Here, we suggest potential behavioral therapeutic and neurotherapeutic interventions for increasing relative executive control.
Behavioral treatments
Working memory training
Significant functional overlap occurs in the left dlPFC, a brain region associated with executive function, during both delay discounting and working memory tasks [61] supporting the notion that executive control and self-regulation interact [7]. For example, increases in working memory load significantly increase discounting [62]. Importantly, working memory impairments are present in pathologies, such as substance use [63] [64] [65] [66] [67] [68] [69]. Moreover, individuals who use substances perform worse than matched controls on both gambling and working memory tasks [70]. From the CNDS perspective, improvement in working memory will strengthen executive function and relative control [3]; [65].
Indeed, working memory training has been demonstrated to successfully improve self-regulation in some cases. For example, working memory training reduced delay discounting in stimulant-dependent participants [71] and decreased alcohol intake in alcohol-dependent individuals [72]. While these results support the use of working memory training as an effective adjunct therapy for addiction [73], some evidence suggests that working memory training was ineffective in improving self-regulation among heroin-dependent individuals (see [74]) Thus, further investigation into the mechanism of the therapeutic efficacy of working memory training in addiction is required.
The CNDS theory proposes a mechanism that involves increasing the relative control of the executive decision system to buffer hyperactive impulsive decision-making. Functional activation has been demonstrated consistently with the CNDS theory following working memory training. For example, the left dlPFC activates proportionally with the difficulty of a working memory task in cigarette smokers. Importantly, functional magnetic resonance imaging (fMRI) studies have demonstrated increases in prefrontal and parietal region activation [75] and plasticity in frontal cortex [76] in individuals following working memory training. In sum, several studies suggest working memory activates regions associated with the executive decision system and working memory training increases its relative control.
Episodic future thinking
Episodic future thinking is the second behavioral intervention that may improve valuation of temporally distant reinforcers. By vividly describing and imagining specific, plausible, and positive future events for specific time points, individuals can significantly widen their temporal window and enhance the salience of delayed rewards. Episodic future thinking reduced delay discounting and ad libitum food intake in healthy participants [77, 78, 79] and in obese adults and adolescents [80, [10, 81, 82]. Importantly, episodic future thinking also decreases delay discounting in alcohol-dependent participants [83] which suggests that preexperiencing a positive future event can help bring the future closer in time for drug-dependent individuals, thus supporting a potential therapeutic intervention for improving the relative control of the executive decision system.
Paramount for improved relative executive control following episodic future thinking is increased activation of the prefrontal brain regions. During the generation of future events and during a delay discounting task, episodic future thought activates frontal poles (i.e., executive decision system areas; [84] [85] and episodic future thought reduces delay discounting via activation of the medial rostral prefrontal cortex (mrPFC), another prefrontal region within the executive decision system [86]. Thus, increased relative control in the executive decision system can be manipulated by episodic future thinking while also decreasing delay discounting (i.e., excessive immediate preference).
Neurotherapeutic treatments
Transcranial magnetic stimulation
Change in delay discounting has also been investigated with non-behavioral interventions, including TMS. Activating the executive decision system through high-frequency rTMS to the medial prefrontal cortex [87] and a specific type of rTMS, continuous theta burst stimulation, targeting the dlPFC [88], both decreased delay discounting in healthy participants. High frequency stimulation to the left dlPFC also decreased rate of delay discounting for monetary gains in both smokers and non-smokers [89]. Conversely, low-frequency rTMS to the left lateral prefrontal cortex, which inhibits the executive system, increased delay discounting rate [90]. Together, these results suggest that targeting the dlPFC directly manipulates relative control of the executive decision system. Moreover, TMS administration may be the most focused intervention to change the relative control between the executive and impulsive decision systems [91] given the ability to directly manipulate the neurocorrelates of at least one decision system of the CNDS (see above for a discussion of the effects of TMS on drug demand, the first reinforcer pathology subtype).
Nootropic therapies
Excessive preference for the immediate choice can also be altered by pharmacotherapies, most often investigated with stimulant medications, in both preclinical and clinical populations [91] [92] [93]. In clinical populations, modafinil administration decreased delay discounting in alcohol-dependent individuals, while preference did not change in healthy participants [94]. Decreased activation in the vmPFC and simultaneous increased activation in the frontal and parietal cortices following stimulant administration suggests that regulatory balance of the CNDS accompanies decreases in delay discounting [94]. The effects of medications on delay discounting may be a result of increased executive control; however, further neuroimaging research is required to determine the functional neurocorrelates of nootropics as CNDS-targeted interventions.
Rate dependence and the CNDS
Discrepant results between studies investigating the same intervention are often attributed to variance intrinsic to the individual when, in fact, an orderly, lawful relationship with baseline rate of behavior may exist [95] [96]. This relationship is referred to as rate dependence and is a well-known behavioral phenomenon, often demonstrated as an inverse association when responding at low rate increases and responding at high rate decreases after drug administration [97]. Recent investigations have found that rate dependence is a robust and overlooked phenomenon that occurs in approximately 50 % of studies, including those with non-pharmacological interventions [60•, 92].
The first explicit description of a rate-dependent brain activation effect using fMRI used rTMS as an intervention technique. In alcohol-dependent treatment-seeking individuals, 15 sessions of rTMS over a 4-week program changed anterior cingulate cortex (ACC) activation dependent upon baseline ACC activation [98]. This baseline activation level was also predictive of relapse such that individuals with high baseline ACC activation were less likely to relapse than those with low baseline ACC activation. This evidence suggests that identifying individuals that may benefit the most from a particular treatment is dependent on their individual baseline level of activation or excitability. Thus, rate dependence may be an observation of approximating regulatory balance between the two decision systems of the CNDS, wherein increases in low baseline levels of activation of the executive decision system may occur following some intervention producing greater regulatory balance. Conversely, individuals with high baseline levels of executive decision system activation may not change following the same intervention.
Delay discounting summary
In sum, behavioral and neurotherapeutic interventions reduce excessive preference for the immediate choice and demonstrate brain activation consistent with the CNDS theory, in a variety of populations. That is, implementation of these interventions activates and enhances function in brain regions associated with greater relative control of the executive decision system. Future exploration of the association between the treatment efficacy of interventions that change delay discounting and clinical outcomes (e.g., decreased drug use) are necessary to apply these treatments more widely in the clinic. Moreover, rate dependence analyses can identify individuals who may most benefit from particular treatments based on their baseline level of CNDS regulation.
Conclusion
We are currently at the forefront of a new conceptual approach to the science of addiction and its treatment. The application and utility of behavioral economic and neuroeconomics to the problems of drug dependence have become increasingly evolved and the scope of this work is broadening. One important arbiter of the success of this approach will be the extent to which it is able to alter drug use and the concomitant behaviors associated with addiction. In this chapter, we have clarified and outlined the important conceptual components of this new system. That is, we have elucidated the CNDS and reinforcer pathology conceptions and how they are related to each other. More importantly, they provide a theoretical basis for treatment development and a conceptual frame by which to evaluate existing interventions.
Just as some of these behavioral economic processes may be operative in multiple disorders beyond addiction, it may be that some of these treatments discussed above, although diverse in procedure and detail, may also have what we would call trans-disease therapeutic properties. Exploring the treatments that we reviewed here in the context of the CNDS and reinforcer pathology conceptions provides a way to examine the extant knowledge and to highlight future areas of potential investigation. Table 1 depicts the types of interventions discussed here and how they may target components of the CNDS, separated by reinforcer pathology subtype. Consistent with the long-term view of addiction as being primarily an issue of the impulsive decision system, we see that the majority of established treatments fall into the high valuation/impulsive decision system quadrant of Table 1. While, the novel and less well established treatments appear in the excessive immediate preference/executive decision system quadrant. Surprisingly, there are no therapies, as we have categorized them, in the excessive immediate preference/impulsive system quadrant. This absence may suggest an important avenue for future therapeutic development. Conversely, the absence of any intervention in this quadrant may reflect the paucity of opportunity there.
The treatment of addiction has improved over time, but arguably, we have reached some of the limits of our existing conceptions and treatment approaches. At such moments, it is useful to consider whether new conceptual approaches permit us to view our subject matter in a new light. Whether this new conception will adequately provide new therapeutic approaches that will significantly improve our ability to treat addiction remains to be seen. However, given the strength of the basic laboratory findings, the important translational advancements, and the new treatment options that are being developed, we are optimistic that this approach may hold substantial benefit for the treatment of those afflicted with the challenges of addiction.
Notes
We note that dominant control by the executive system may produce pathologies other than addiction, such as those characterized by excessive concern over future events (e.g., anorexia nervosa and obsessive-compulsive disorder). However, our focus in this chapter is on dominant control by the impulsive system and the resulting risk for addiction.
For further discussion of contingency management in the other subtype of reinforcer pathology and the executive decision system of the CNDS, see [13].
References and Recommended Reading
Papers of particular interest, published recently, have been highlighted as: • Of importance
Bickel WK, Degrandpre RJ, Higgins ST, Hughes JR. Behavioral economics of drug self-administration. I. Functional equivalence of response requirement and drug dose. Life Sci. 1990;47:1501–10.
Glimcher P. Decisions, uncertainty, and the brain: the science of neuroeconomics. Cambridge, Mass: MIT Press; 2003. 395 p.
Bickel WK, Miller ML. Yi R, Kowal BP, Lindquist DM, Pitcock Ja. Behavioral and neuroeconomics of drug addiction: Competing neural systems and temporal discounting processes. Drug Alcohol Depend. 2007;90:85–91.
Bechara A. Decision making, impulse control and loss of willpower to resist drugs: a neurocognitive perspective. Nat Neurosci. 2005;8:1458–63.
Bickel WK, Mueller ET, Jarmolowicz DP. What is Addiction? In: McCrady B, Epstein E, editors. Addictions: a comprehensive guidebook. 2nd ed. New York: Oxford University Press; 2013.
Bjork JM, Smith AR, Hommer DW. Striatal sensitivity to reward deliveries and omissions in substance dependent patients. Neuroimage. 2008;42(4):1609–21.
Bickel WK, Jarmolowicz DP, Mueller ET, Gatchalian KM, McClure SM. Are executive function and impulsivity antipodes? A conceptual reconstruction with special reference to addiction. Psychopharmacology. 2012;221:361–87.
Quisenberry AJ, Koffarnus MN, Hatz LE, Epstein LH, Bickel WK. The experimental tobacco marketplace i: substitutability as a function of the price of conventional cigarettes. Nicotine Tob Res. 2015.
Mackillop J, Few LR, Murphy JG, Wier LM, Acker J, Murphy C, et al. High-resolution behavioral economic analysis of cigarette demand to inform tax policy. Addiction. 2012;107(12):2191–200.
Bickel WK, Moody L, Quisenberry AJ, Ramey CT, Sheffer CE. The competing neurobehavioral decision systems model of SES-related health and behavioral disparities. Preventative Medicine. 2013;18:1199–216.
Bickel W, Jarmolowicz D, MacKillop J. The behavioral economics of reinforcement pathologies: novel approaches to addictive disorders. APA Addiction Syndrome Handbook. 22012. p. 333–63.
Bickel WK, Johnson MW, Koffarnus MN, Mackillop J, Murphy JG. The behavioral economics of substance use disorders: reinforcement pathologies and their repair. Annu Rev Clin Psychol. 2014;10:641–77. This article links the overvaluation of drug reinforcement with the preference for the immediate choice to describe reinforcer pathology. It contains descriptions of the etiology of reinforcer pathology and approaches and procedures that can improve them.
Bickel WK, Snider SE, Quisenberry AJ, Stein JS, Hanlon CA. Competing neurobehavioral decision systems theory of cocaine addiction: From mechanisms to therapeutic opportunities. Progress in Brain Research. 2015:1–25. This chapter provides an overview of the CNDS theory of addiction through the chronically relapsing condition of cocaine dependence. It offers a unified understanding of impulsivity, developmental time course, comorbidities, and neuro-phenotype of cocaine dependence.
Sofis MJ, Jarmolowicz DP, Martin LE. Competing neurobehavioral decision systems and the neuroeconomics of craving in opioid addiction. Neuroscience & Neuroeconomicss. 2014;3:87–99.
Kahneman D. Thinking, fast and slow. New York: Farrar, Straus, and Giroux; 2011. 512 p.
Metcalfe J, Mischel W. A hot/cool system analysis of delay of gratification: dynamics of willpower. Psychol Rev. 1999;106(1):3–19.
Pinto A, Steinglass JE, Greene AL, Weber EU, Simpson HB. Capacity to delay reward differentiates obsessive-compulsive disorder and obsessive-compulsive personality disorder. Biol Psychiatry. 2014;75(8):653–9.
Steinglass JE, Figner B, Berkowitz S, Simpson HB, Weber EU, Walsh BT. Increased capacity to delay reward in anorexia nervosa. J Int Neuropsychol Soc. 2012;18(4):773–80.
Bickel WK, Jarmolowicz DP, Mueller ET, Gatchalian KM. The behavioral economics and neuroeconomics of reinforcer pathologies: implications for etiology and treatment of addiction. Curr Psychiatry Rep. 2011;13(5):406–15.
Hursh SR, Silberberg A. Economic demand and essential value. Psychol Rev. 2008;115:186–98.
Hursh SR, Roma PG. Behavioral economics and empirical public policy. J Exp Anal Behav. 2013;99:98–124. This chapter summarizes insights from behavioral economics relevant to basic research, preclinical behavioral pharmacology, and clinical drug abuse. It describes demand curve analysis to allow for cross-commodity comparisons of reinforcer valuation and defines common interactions between commodities.
Few LR, Acker J, Murphy C, Mackillop J. Temporal stability of a cigarette purchase task. Nicotine Tob Res. 2012;14:761–5.
Murphy JG, MacKillop J, Skidmore JR, Pederson AA. Reliability and validity of a demand curve measure of alcohol reinforcement. Exp Clin Psychopharmacol. 2009;17:396–404.
Murphy JG, Mackillop J, Tidey JW, Brazil LA, Colby SM. Validity of a demand curve measure of nicotine reinforcement with adolescent smokers. Drug Alcohol Depend. 2011;113(2–3):207–14.
Yurasek AM, Murphy JG, Clawson AH, Dennhardt AA, Mackillop J. Smokers report greater demand for alcohol on a behavioral economic purchase task. J Stud Alcohol Drugs. 2013;74:626–34.
Mackillop J, Murphy JG. A behavioral economic measure of demand for alcohol predicts brief intervention outcomes. Drug Alcohol Depend. 2007;89(2–3):227–33.
Madden GJ, Petry NM, Badger GJ, Bickel WK. Impulsive and self-control choices in opioid-dependent patients and non-drug-using control participants: drug and monetary rewards. Exp Clin Psychopharmacol. 1997;5:256–62.
Audrain-Mcgovern J, Rodriguez D, Epstein LH, Cuevas J, Rodgers K, Wileyto EP. Does delay discounting play an etiological role in smoking or is it a consequence of smoking? Drug Alcohol Depend. 2009;103:99–106.
Bickel WK, Koffarnus MN, Moody L, Wilson AG. The behavioral- and neuro-economic process of temporal discounting: a candidate behavioral marker of addiction. Neuropharmacology. 2014;76:518–27.
Mackillop J, Amlung MT, Few LR, Ray L, Sweet LH, Munafò MR. Delayed reward discounting and addictive behavior: a meta-analysis. Psychopharmacology. 2011;216:305–21.
Green L, Fry AF, Myerson D o d r. A Life-Span Comparison. Psychol Sci. 1994;5:33–6.
Green L, Myerson J, Lichtman D, Rosen S, Fry A. Temporal discounting in choice between delayed rewards: the role of age and income. Psychol Aging. 1996;11:79–84.
Pinkston JW, Lamb RJ. Delay discounting in C57BL/6J and DBA/2J mice: adolescent-limited and life-persistent patterns of impulsivity. Behav Neurosci. 2011;125(2):194–201.
Tobin H, Logue AW. Self-control across species (Columba livia, Homo sapiens, and Rattus norvgicus. J Cogn Psychother. 1994;108(2):126–33.
Hursh SR. Behavioral economics of drug self-administration and drug abuse policy. J Exp Anal Behav. 1991;56(2):377–93.
Hursh SR. Behavioral economics and the analysis of consumption and choice. In: Mcsweeney FK, Murphy ES, editors. The Wiley Blackwell handbook of operant and classical conditioning. Hoboken: Wiley; 2014. p. 275–305. This chapter describes complements, substitutes, and independents as well as providing a novel equation to quantify cross-price elasticity. This offers insights not just into the elasticity of a commodity’s own price but direct report on the effect of a second commodity’s price on consumption of the first commodity.
Degrandpre RJ, Bickel WK, Hughes JR, Layng MP, Badger GJ. Unit price as a useful metric in analyzing effects of reinforcer magnitude. J Exp Anal Behav. 1993;60(3):641–66.
Greenwald MK, Hursh SR. Behavioral economic analysis of opioid consumption in heroin-dependent individuals: effects of unit price and pre-session drug supply. Drug Alcohol Depend. 2006;85(1):35–48.
Bickel WK et al. Modeling the effects of combined behavioral and pharmacological treatment on cigarette smoking: behavioral-economics analyses. Exp Clin Psychopharmacol. 1997;5(4):334–43.
Prendergast M, Podus D, Finney J, Greenwell L, Roll J. Contingency management for treatment of substance use disorders: a meta-analysis. Addiction. 2006;101(11):1546–60.
Higgins ST, Petry NM. Contingency management: incentives for sobriety. Alcohol Res Health. 1999;23(2):122–7.
Murphy JG, Correia CJ, Barnett NP. Behavioral economic approaches to reduce college student drinking. Addict Behav. 2007;32(11):2573–85.
Walters ST, Neighbors C. Feedback interventions for college alcohol misuse: what, why and for whom? Addict Behav. 2005;30(6):1168–82.
Dennhardt AA, Murphy JG. Prevention and treatment of college student drug use: a review of the literature. Addict Behav. 2013;38(10):2607–18.
Dennhardt AA, Yurasek AM, Murphy JG. Change in delay discounting and substance reward value following a brief alcohol and drug use intervention. J Exp Anal Behav. 2015;103:125–40.
Eichhammer P, Johann M, Kharraz A, Binder H, Pittrow D, Wodarz N, et al. High frequency repetitive transcranial magnetic stimulation decreases cigarette smoking. J Clin Psychiatry. 2003;64(8):951–3.
Amiaz R, Levy D, Vainiger D, Grunhaus L, Zangen A. Repeated high-frequency transcranial magnetic stimulation over the dorsolateral prefrontal cortex reduces cigarette craving and consumption. Addiction (Abingdon, England). 2009;104:653–60.
Terraneo A, Leggio L, Ermani M, Bonci A. Transcranial magnetic stimulation of dorsolateral prefrontal cortex reduces cocaine use: a pilot study. Eur Neuropsychopharmacol. 2015;1–8.
Bickel WK, Degrandpre RJ, Higgins ST. The behavioral economics of concurrent drug reinforcers: a review and reanalysis of drug self-administration research. Psychopharmacology. 1995;118(3):250–9.
Johnson MW, Bickel WK, Kirshenbaum AP. Substitutes for tobacco smoking: a behavioral economic analysis of nicotine gum, denicotinized cigarettes, and nicotine-containing cigarettes. Drug Alcohol Depend. 2004;74:253–64.
Johnson MW, Bickel WK. The behavioral economics of cigarette smoking: the concurrent presence of a substitute and an independent reinforcer. Behav Pharmacol. 2003;14(2):137–44.
Budney AJ, Bickel WK, Hughes JR. A behavioral approach to achieving initial cocaine abstinence. Am J Psychiatr. 1991;148:1218–24.
Secades-Villa R, Garcia-Rodriguez O, Higgins ST, Fernandez-Hermida JR, Carballo JL. Community reinforcement approach plus vouchers for cocaine dependence in a community setting in Spain: six-month outcomes. J Subst Abuse Treat. 2008;34(2):202–7.
Higgins ST, Sigmon SC, Wong CJ, Badger GJ, Donham R, et al. Community reinforcement therapy for cocaine-dependent outpatients. Arch Gen Psychiatry. 2003;60(10):1043–52.
Hunt GM, Azrin NH. A community-reinforcement approach to alcoholism. Behav Res Ther. 1973;11:91–104.
Sofuoglu M. Cognitive enhancement as a pharmacotherapy target for stimulant addiction. Addiction. 2010;105(1):38–48.
Mattick R, Breen C, Kimber J, Davoli M. Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence. Cochrane Database System Reviews. 2009;1(3).
Bickel WK, Stitzer M, Bigelow GE, Liebson IA, Jasinski DR, Johnson RE. A clinical trial of buprenorphine: comparison with methadone in the detoxification of heroin addicts. Clin Pharmacol Ther. 1988;43(1):72–8.
Campbell A, Nunes E, Matthews A, Stitzer M, Miele G, Polsky D, et al. Internet-delivered treatment for substance abuse: a multisite randomized controlled trial. Am J Psychiatr. 2014;171:683–90.
Bickel WK, Quisenberry AJ, Moody L, Wilson AG. Therapeutic opportunities for self-control repair in addiction and related disorders: change and the limits of change in trans-disease processes. Clin Psychol Sci. 2014;3:140–53. This review describes the CNDS as a dual model of self control failure and specifically highlights altered delay discounting as a hallmark of multiple diseases in which the balance between these two systems is altered.
Wesley MJ, Bickel WK. Remember the future II: meta-analyses and functional overlap of working memory and delay discounting. Biol Psychiatry. 2014;75(6):435–48.
Hinson JM, Jameson TL, Whitney P. Impulsive decision making and working memory. J Exp Psychol Learn Mem Cogn. 2003;29(2):298–306.
Griffiths A, Hill R, Morgan C, Rendell PG, Karimi K, Wanagaratne S, et al. Prospective memory and future event simulation in individuals with alcohol dependence. Addiction. 2012;107(10):1809–16.
Hester R, Garavan H. Executive dysfunction in cocaine addiction: evidence for discordant frontal, cingulate, and cerebellar activity. J Neurosci. 2004;24(49):11017–22.
Hofmann W, Schmeichel BJ, Baddeley AD. Executive functions and self-regulation. Trends Cogn Sci. 2012;16(3):174–80.
Mendrek A, Monterosso J, Simon SL, Jarvik M, Brody A, Olmstead R, et al. Working memory in cigarette smokers: comparison to non-smokers and effects of abstinence. Addict Behav. 2006;31(5):833–44.
Xu J, Mendrek A, Cohen MS, Monterosso J, Rodriguez P, Simon SL, et al. Brain activity in cigarette smokers performing a working memory task: effect of smoking abstinence. Biol Psychiatry. 2005;58(2):143–50.
Jacobsen LK, Mencl WE, Constable RT, Westerveld M, Pugh KR. Impact of smoking abstinence on working memory neurocircuitry in adolescent daily tobacco smokers. Psychopharmacology (Berl). 2007;193(4):557–66.
Patterson F, Jepson C, Loughead J, Perkins K, Strasser AA, Siegel S, et al. Working memory deficits predict short-term smoking resumption following brief abstinence. Drug Alcohol Depend. 2010;106(1):61–4.
Bechara A, Martin EM. Impaired decision making related to working memory deficits in individuals with substance addictions. Neuropsychology. 2004;18(1):152–62.
Bickel WK, Yi R, Landes RD, Hill PF, Baxter C. Remember the future: working memory training decreases delay discounting among stimulant addicts. Biol Psychiatry. 2011;69(3):260–5.
Houben K, Wiers RW, Jansen A. Getting a grip on drinking behavior: training working memory to reduce alcohol abuse. Psychol Sci. 2011;22(7):968–75.
Bickel WK, Moody L, Quisenberry AJ. Computerized working-memory training as a candidate adjunctive treatment for addiction. Alcohol Res. 2014;36(1):123–6.
Rass O, Schacht RL, Buckheit K, Johnson MW, Strain EC, Mintzer MZ. A randomized controlled trial of the effects of working memory training in methadone maintenance patients. Drug Alcohol Depend. 2015;156:38–46.
Olesen PJ, Westerberg H, Klingberg T. Increased prefrontal and parietal activity after training of working memory. Nat Neurosci. 2004;7(1):75–9.
Klingberg T. Training and plasticity of working memory. Trends Cogn Sci. 2010;14(7):317–24.
Lin H, Epstein LH. Living in the moment: effects of time perspective and emotional valence of episodic thinking on delay discounting. Behav Neurosci. 2014;128(1):12–9.
Peters J, Buchel C. Episodic future thinking reduces reward delay discounting through an enhancement of prefrontal-mediotemporal interactions. Neuron. 2010;66(1):138–48.
Dassen FC, Jansen A, Nederkoorn C, Houben K. Focus on the future: episodic future thinking reduces discount rate and snacking. Appetite. 2016;96:327–32.
Daniel TO, Stanton CM, Epstein LH. The future is now: reducing impulsivity and energy intake using episodic future thinking. Psychol Sci. 2013;24(11):2339–42.
Schacter DL, Benoit RG, De Brigard F, Szpunar KK. Episodic future thinking and episodic counterfactual thinking: intersections between memory and decisions. Neurobiol Learn Mem. 2015;117:14–21.
O’Neill J, Daniel TO, Epstein LH. Episodic future thinking reduces eating in a food court. Eat Behav. 2016;20:9–13.
Snider SE, LaConte SM, Bickel WK. Episodic future thinking: expansion of the temporal window in alcohol dependents. Alcoholism: clinical and experimental research. 2016;1–9. doi: 10.1111/acer.13112.
Bertossi E, Aleo F, Braghittoni D, Ciaramelli E. Stuck in the here and now: construction of fictitious and future experiences following ventromedial prefrontal damage. Neuropsychologia. 2015;81:107–16.
Okuda J, Fujii T, Ohtake H, Tsukiura T, Tanji K, Suzuki K, et al. Thinking of the future and past: the roles of the frontal pole and the medial temporal lobes. NeuroImage. 2003;19(4):1369–80.
Benoit RG, Gilbert SJ, Burgess PW. A neural mechanism mediating the impact of episodic prospection on farsighted decisions. J Neurosci. 2011;31(18):6771–9.
Cho SS, Koshimori Y, Aminian K, Obeso I, Rusjan P, Lang AE, et al. Investing in the future: stimulation of the medial prefrontal cortex reduces discounting of delayed rewards. Neuropsychopharmacology. 2014;40:1–8.
Cho SS, Ko JH, Pellecchia G, Van Eimeren T, Cilia R, Strafella AP. Continuous theta burst stimulation of right dorsolateral prefrontal cortex induces changes in impulsivity level. Brain stimulation. 2010;3:170–6.
Sheffer CE, Mennemeier M, Landes RD, Bickel WK, Brackman S, Dornhoffer J, et al. Neuromodulation of delay discounting, the reflection effect, and cigarette consumption. J Subst Abus Treat. 2013;45:206–14.
Figner B, Knoch D, Johnson EJ, Krosch AR, Lisanby SH, Fehr E, et al. Lateral prefrontal cortex and self-control in intertemporal choice. Nat Neurosci. 2010;13(5):538–9.
Koffarnus MN, Jarmolowicz DP, Mueller ET, Bickel WK. Changing delay discounting in the light of the competing neurobehavioral decision systems theory: a review. J Exp Anal Behav. 2013;99:32–57.
Bickel WK, Quisenberry AJ, Snider SE. Does impulsivity change rate dependently following stimulant administration? Psychopharmacology: A translational selective review and re-analysis; 2015.
Gray J, Mackillop J. Impulsive delayed reward discounting as a genetically- influenced target for drug abuse prevention: a critical evaluation. Front Psychol. 2015;6:1–13.
Schmaal L, Goudriaan AE, Joos L, Dom G, Pattij T, van den Brink W, et al. Neural substrates of impulsive decision making modulated by modafinil in alcohol-dependent patients. Psychol Med. 2014;44(13):2787–98.
Quisenberry AJ, Snider SE, Bickel WK. The return of rate dependence: a commentary. Behavioral Analysis: Research and Practice. 2016 (in press).
Snider SE, Quisenberry AJ, Bickel WK. Order in the absence of an effect: rate dependent relationships revealed. Behavioural Processes. 2016;127:18–24.
Wenger GR, Dews PB. The effects of phencyclidine, ketamine, d-amphetamine and pentobarbital on schedule-controlled behavior in the mouse. J Pharmacol Exp Ther. 1976;616–24.
Herremans SC, De Raedt R, Van Schuerbeek P, Marinazzo D, Matthys F, De Mey J, et al. Accelerated HF-rTMS protocol has a rate-dependent effect on dACC activation in alcohol-dependent patients: an open-label feasibility study. Alcohol Clin Exp Res. 2016;40:196–205.
Acknowledgments
The following grants contributed to the support of the authors during the development of this work: NIH grants R01AA021529, R01DA034755, U19CA157345, UH2DK109543, and F31AA024368-01.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Warren K. Bickel declares that he has no conflict of interest.
Alexandra M. Mellis declares that she has no conflict of interest.
Sarah E. Snider declares that she has no conflict of interest.
Lara Moody declares that she has no conflict of interest.
Jeffrey S. Stein declares that he has no conflict of interest.
Amanda J. Quisenberry declares that she has no conflict of interest.
Human and animal rights and informed consent
This article contains citations to studies with human subjects performed by authors Warren K. Bickel, Sarah E. Snider, Jeffery S. Stein, and Amanda J. Quisenberry. All studies performed by authors with human subjects were approved by the institutional review boards where the research was completed. This article does not contain any studies with animal subjects performed by its authors.
Additional information
This article is part of the Topical Collection on Substance Use Disorders
Rights and permissions
About this article

Cite this article
Bickel, W.K., Mellis, A.M., Snider, S.E. et al. Novel Therapeutics for Addiction: Behavioral Economic and Neuroeconomic Approaches. Curr Treat Options Psych 3, 277–292 (2016). https://doi.org/10.1007/s40501-016-0088-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40501-016-0088-3