
Abstract
The different branches of kynurenine pathways of tryptophan metabolism are the important mechanism to elucidate various neurological and immunological disorders. There is a substantial body of evidence indicating the involvement of kynurenine pathway (KP) in the pathophysiology of some neuropsychiatric and neurodegenerative perturbation. This pathway generates neuro-active compounds, those can interact with neurotransmitters receptors in the central nervous system (CNS). According to some recent studies, there are a strong relation between KP’s related enzymes such as indoleamine 2,3 dioxygenase (IDO) and tryptophan 2,3 dioxygenase (TDO) activation and neurological disease. In this review article, we focus on the level/ratios of different metabolites and precursors such as tryptophan (TRP), 5-hydroxytryptamine (5-HT), kynurenine (KYN), kynurenic acid (KYNA), and quinolinic acid (QUIN) in order to find the link with the KP-induced neuropathologies. Kynurenine metabolism is hypothesized to be one of the key mechanisms that link inflammation and depression. Some factors such as exercise (through PGC-1α), inflammation, stress, and some medication have the remarkable effects on KP. We highlight the role of different causes such as inflammation and stress, Tryptophan-kynurenine pathway with the whole biochemical and organ-specific biochemistry, and the neuropathomechanism of related pathologies. Here, we discuss the relations, the changes, and the mutual effects of KP with major depressive disorders, bipolar disorders, schizophrenia, Parkinson’s, and Alzheimer’s disease.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Tryptophan (TRP) is an essential amino acid and a mother molecule for 5-HT and the metabolites of KP such as kynurenine (KYN), 3-hydroxykynurenine (3-HK), KYNA, and QUIN. Kynurenine pathway (KP) is an important pathway of tryptophan metabolism that takes place in the kidneys, liver, and brain of various mammals such as human, rat, mice, rabbits, monkeys, and guinea pigs. Along this pathway, varied neuroactive and redox activities take place. A total of 95% Trp is metabolized within tissue-specific pathways by the rate-limiting enzymes tryptophan 2,3-dioxygenase (TDO1/2) and indolamine 2,3-dioxygenase (IDO1/2) [1] KP to produce NAD+, an important redox cofactor for energy metabolism [2]. IDO1 plays the key role by regulating L-tryptophan levels and T cell differentiation. In recent studies, several IDO1 inhibitors are currently being tested in clinical trials for cancer treatment as well as for the treatment of several other pathologies [3]. IDO1 genetic study shows its regulation by two pathways, i.e., interferon-gamma-dependent and interferon-gamma-independent pathways [4,5,6,7]. The increased neuroactive metabolite concentrations of KP in the central nervous system are associated to the pathophysiology of several inflammation-related neuropsychiatric and neurodegenerative diseases [8]. In response to inflammatory stimuli, the initial pathway is started with IDO1 which produces KYN from TRP. Subsequently, the KP has two different sub-pathways; the first sub-pathway is catalyzed by kynurenine 3-monooxygenase (KMO) which produces 3-HK and QUIN, and the second one is regulated by kynurenine aminotransferase (KAT) which is responsible for kynurenic acid (KYNA) production [9].
As it is highly important to describe KP regulatory mechanisms, therefore we focus on the properties of neuroactive metabolites, especially on the regulation of the KP enzymes in neuropsychiatric diseases. Whereas, interferon-gamma activity is increased with age, thus there is well-known associated relation between these findings and chronic health conditions such as diabetes, dementia, and sarcopenia [10]. Previous studies have demonstrated that associations between the imbalance of KP and depression are driven either by an increase in neurotoxic QUIN [11,12,13], or by a decrease in neuroprotective KYNA [14,15,16]. In recent studies, the individual metabolite QUIN shows to be driving the association between sleep disturbance and the reduction in KYNA/QUIN ratio observed in currently depressed subjects. The KYNA/QUIN might have contributed to the sleep disturbance in different degrees [17]. According to previous and recent studies, dysregulation of KP has been associated to neurodegenerative disorders such as Alzheimer’s, Huntington, and Parkinson’s diseases [18], and it is also confirmed that depression and inflammation exacerbate each other through KP [19]. Depression could increase systemic inflammation, which could activate the KP and lead to other neurobehavioral disturbances [20]. KYNA, QUIN, and xanthurenic acid are neuroactive compounds that interact with different types of glutamate receptors [21]. KYNA acts as a competitive antagonist at the glycine site of NMDA receptor, thereby exerts neuroprotective and anticonvulsant activity [22]. All the KP-related enzymes are involved in the above discussed cerebral disorders, but IDO is in the most predominant one [23]. An increase level of serum IL-6, IL-1β, and TNF-α were observed after 7 days bile duct ligation (BDL) in rats; progressive decline in memory, depressive disorders and anxiety, accompanied by IDO expression due to BDL, decrease in 5-HT and KYN, and increase in KYN and 3-HK levels was shown [23]. This phenomenon shows that KP is an important trajectory in mediating the effects of inflammatory cytokines in different regions of the brain [24]. In this case, TRP is more likely to be metabolized to KYN and subsequently to QUIN, an NMDA receptor agonist and excitotoxic agent [25], and in parallel, obviously a low cerebral 5-HT level will occur. Some studies have confirmed that IDO expression and relatively higher level of QUIN were found in animal model of depression, and the inflammation-induced depressive-like symptoms were prevented by IDO inhibitor, 1-methyl tryptophan treatment [26]. Protein and mRNA expression level of IDO1 was increased by inducing pro-inflammatory cytokines activation in cerebral cortex and hippocampus, while TDO enzyme activity was not modulated in any brain region by this mechanism [23]. Physiologically, the metabolism of kynurenine is compartmentalized within the brain regions of astrocyte and microglia, which depends on the location specificity of enzymes such as KAT and KMO [27]. To be more specific, it means that KYN is differently biotransformed by either astrocyte or microglia, in order to produce distinct neuroactive metabolites. The neurotoxic compound, 3-HK, and the downstream catabolites such as 3-hydroxyanthranilic acid (3-HAA) and QUIN are produced in microglia and other cells of monocytic origin, while the synthesis of neurotoxic compound KYNA is carried out in astrocytes, neurons, and oligodendrocytes [28].. Reactive oxygen species can also induce KP activation, which can be modulated in redox environment [29]. A recent study has shown that cellular and particularly the mitochondrial toxicity worsened by co-incubation of copper with 3-HK and 3-HAA [29]. These consequences are attributed to the effects of 3-HK and 3-HAA on respiratory control followed by ATP decline and cell death [30]. Alongside the above mechanism, these metabolites are able to form reactive compounds such as xanthommatin radical, p-quinone, and 4,6 dihydroxyquinolinequinone carboxylic acid, with mitochondrial and cellular toxicity [31]. GSH, an antioxidant which is abundant in astrocytes and necessary for SOD activity, could also be affected by oxidative kynurenines [32]. 3-HK could be deaminized in astrocyte by KAT to 3-hydroxykynurenin glucoside, which is able to form adduct to GSH and decrease active GSH level [29]. Besides, the QUIN toxicity to glutamatergic neurotransmission and excitotoxicity, oxidative stress induced by some KP metabolites triggers neurodegenerative diseases.
Major depressive disorders are partly attributed to TRP-5-HT-KYN metabolic machinery. Therefore, some recent studies focused on the correlation between KP and suicidality. Patients diagnosed with or in risk of suicidality have shown elevated level of central nervous system inflammation, as well as peripheral blood inflammation, dysregulation of KP, an imbalance of metabolites (increased QUINA and decreased KYNA serum level) [33], a predominant suggested mechanism to develop suicidality. The NMDA receptor antagonist, ketamine, has shown to produce anti-suicidal and anti-depressant effects via intravenous injection [34]. From this point of view, the role of KYNA, and QUIN brain level, would be taken into consideration in suicidality. Nevertheless, the biological mechanism underlying complete suicide or suicide attempt has not yet been known, but the disorders of hypothalamic-pituitary-adrenal axis and serotoninergic system can be involved [33]. Within inflammation-induced KP, the availability of TRP is decreased toward serotonin synthesis [35]. A total of 40% decrease in plasma TRP level and 40% increase of plasma KYN/TRP ratio was observed in suicide attempted patients diagnosed with major depressive disorder (MDD) compared with non-suicide attempted with MDD and healthy controls [36].
Some recent studies also show the interaction between endocannabinoid system and KP in relation to migraine, via glutamatergic system interference [37, 38]. It is clear that KP metabolites, particularly QUIN and KYNA have their effect through glutamatergic system. Besides AMPA, glutamate is an ionic neurotransmitter of NMDA receptor, and glutamate excitotoxicity is related to NMDA receptor hyperexcitability. A large body of evidences shows that increased glutamate level in synaptic space activates NMDA receptor and leads to large amount of Ca++ entry to the cell. Ca++ entry induces the activation of some proteolytic enzymes such as endonuclease, phospholipase, and protease, which are massively responsible for damaging cells and DNA structure and results into nerve cell death [39]. Hence, these mechanisms are strongly suggested to be involved in the pathophysiology of migraine [40]. QUIN is able to induce nerve cell death, lipid peroxidation, and inhibit the reuptake of glutamate resulting in increased synaptic glutamate level [41, 42]. Contrarily, KYNA and its related halogenated compounds are supposed to be the future drug candidates in migraine treatment. These compounds such as 7-chlorokynurenic acid and 5, 7-dichlorokynurenic acid can cross blood-brain barrier opposite to KYAN and both have increased affinity to glycine-binding site of NMDA receptor [43, 44]. These findings suggest that the decreased brain KYNA level shows that the glutamatergic system was overactive in chronic migraine.
Schizophrenia is also remarkably considered as one of the disorders with high risk of suicide [45]. Dopaminergic system hyperactivity is thought to be the predominate hypothesis. However KYNA induces both positive and negative symptoms, cognitive deficit and exacerbates psychotic symptoms in schizophrenic patients [46]. In different studies compared with the control group, significant increase of KYN level have been shown in patient diagnosed with schizophrenia [47].
Kynurenine Pathway of Tryptophan Metabolism
Tryptophan is one of the nine essential amino acids, which follows a complicated pathway of metabolism in animals. Tryptophan has a unique characteristics than other amino acids, such as being derivative of indol, circulates primarily 95% bound to albumin, and present in the blood at low concentration [19, 48]. Free tryptophan is metabolized in CNS, neurons, astrocytes, glial cells, and dendrites; and in periphery, by hepatocytes, immune cells, and skeletal muscles [49,50,51]. Inflammatory mediators such as interferon-gamma and some interleukins activate IDO, an enzyme that metabolizes tryptophan TRP to KYN; hence, the ratio of KYN/TRP reflects the level of IDO activity. IDO is also induced by some interleukins such as IL-1 and IL-6 [52], or by tumor necrosis factor (TNF) [24], while IL-4 reduce the activity of IDO [53]. KYN is metabolized into 3-HK by the enzyme KMO which is similarly upregulated under inflammatory conditions, leading to an increase QUIN level in the putative neurotoxic branch of the KP [14, 25]. TRP is also the main precursor for the synthesis of NAD+. Partially, TRP is broken down by different pathways, including KP in which the indol ring is cleaved by both TDO1/2, or by IDO1/2 [39]. TDO is generally expressed in the liver, while some recent studies show its expression in the CNS of rat and human [47, 54]. TDO’s activity is regulated by ROS, which reduce the ferric state (inactive form) to active form (ferrous state) of this enzyme [55, 56]. Both IDO1 and IDO2 have the same catalytic activity but differ in a sense that IDO1 has a significantly higher affinity toward TRP than IDO2 [57].
KP always remains responsible for 95% degradation of TRP, and the liver is a major site for TRP degradation [58]. In this pathway, the pyrrole site of TRP is opened by TDO in the liver or by IDO in other organs of the body such as the brain [49]; then, the product is hydrolyzed to KYN by N-formyl kynurenine formamidase [9]. KYN is further hydroxylated by kynurenine hydroxylase to 3-HK and subsequently hydrolyzed by kynureninase to 3-HAA [8, 9]. KYNA is produced when KYN is catalyzed by KAT [22]. KYN could also be converted to anthranilic acid by kynureninase. KYN and 3-HK is transaminated to KYNA and xanthurenic acid, respectively, within a minor reaction [59]. 3-HAA is converted to quinolinic acid by non-enzymatic cyclization of acroleyl aminofumarate [9]. Acroleyl aminofumarate may be converted to picolinic acid by a specific carboxylase, which is thought to be the second rate-limiting enzyme after TDO in rat liver [60]. Whereas, tryptophan is the precursor for KP and serotoninergic pathway, therefore a narrow association between these two pathways has been known (Fig. 1). The main route of elimination of KYN and its metabolites is renal excretion [61]. In addition, the kidneys are able to uptake KYN and 3-hydroxykynurenine (3-HK) from the blood, which are metabolized and excreted in the form of KYNA and xanthurenic (XA), respectively [62]. Thus, the impairment of the kidney function is likely to be associated with the retention of KYN and its metabolites. The above data suggests that exploration of KYN metabolism could help to explain the pathogenesis of certain diseases. KP metabolites could be found in the liver, plasma, brain, muscle, intestine, kidneys, and lungs [9]. In different pathologies, the level of KP metabolites and enzyme are affected in these tissues [63].

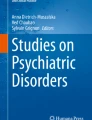
The kynurenine pathway of tryptophan metabolism. The predominant metabolite of the KP is L-kynurenine. The catabolism of L-tryptophan by IDO and TDO enzymes represents the rate-limiting step of L-kynurenine synthesis. IDO is induced by various inflammatory stimuli, while TDO is expressed in the liver in normal conditions. Kynurenine can be further metabolized to 3-HK, KYNA, or QUIN by different enzyme in various cerebral, hepatic, or extrahepatic regions. KAT (kynurenine amino transferase), QUIN (quinolinic acid), 3-HAA (3-hydroxy anthranilic acid), 3-HK (3-hydroxy kynurenine), NAD (nicotinamide adenine dinucleotide), KYNA (kynurenic acid), NAS (N, acetyl serotonin), 5-HIAA (5-hydroxy indoleacetic acid), IDO (indoleamine dioxygenase), TDO (tryptophan dioxygenase), KMO (kynurenin monoxygenase), TPH (tryptophan hydroxylase), MAO (monoamine oxidase), ASMT (acetyl-serotonin O-methyl transferase), AANAT (aralkylamine N-acetyltransferase)
Kynurenine
Kynurenine was first known as a precursor in the beginning of the twentieth century, in 1950. The main product of L-tryptophan kynurenine pathway degradation in peripheral tissues is L-kynurenine, which is further converted to a series of metabolites, such as 3-HK, and anthranilic (AA), KYNA, XA, and quinolinic (QA) acids [63]. As mentioned above, it is the intermediate metabolite which can convert to different neuroactive products. From this point of view, its study is significantly important in modern neurodegenerative and psychiatric disorders. KYN can easily pass through blood-brain barrier and similarly not physiologically very active; that’s why recent research works focus on its related active metabolites [19]. Nearly 60% of CNS KYN comes from peripherally produced KYN, which can be transported through blood-brain barrier [64]. KYNA and QUIN are not able to transport across the blood-brain barrier [14]. We found that KYN/TRP ratio was decreased by long-term endurance exercise in mice (Tutakhail et al., in preparation).
Quinolinic Acid
QUIN is an important heterocyclic catabolite of kynurenine pathway of tryptophan metabolism. Whereas, tryptophan is mostly converted to 5-hydroxytryptamine than N-formylkynurenine in serotonergic system of CNS; thus, the concentration of QUIN is lower in CNS than blood and systemic tissues [65]. During the brain inflammation, macrophage, microglia, and dendritic cells are the major source of QUIN production, while astrocytes did not show this ability due to the lack of KMO enzyme [66]. The higher concentration of QUIN in CNS is associated to many pathological conditions such as inflammation, depression, hyper-excitatory, and oxidative stress [67]. The increased activation of NMDA receptor produces excitotoxicity and lesion on CNS level catalyzed by nitric oxide synthase (NOS). ROS and other free radicals are produced in this reaction, perturb mitochondria and cellular death [68, 69]. Some recent studies show that QUIN induced neuronal cell death in intracerebral and neuronal cell culture, [70, 71]. As an agonist of NMDA receptor, QUIN increases glutamatergic transmission, decreases the reuptake of glutamate by astrocyte, and finally increases glutamate level in synaptic region, which potentiate excitotoxic effects in CNS [72]. QUIN maybe associated with many other neurodegenerative diseases such as Huntington disease [63], Alzheimer’s disease [73], and AIDS dementia complex [74].
Kynurenic Acid
KYNA is also an interesting metabolite produced by KP, by KAT in CNS and periphery [72]. It should be mentioned that KYNA cannot pass through blood-brain barrier [14]. KYNA is an endogenous catabolite, present in the brain in nanomolar concentration [75]. KYNA is antagonist of NMDA receptor and acts on glycine modulatory site at low concentration [76]. At higher concentration, it binds to glutamate site and also acts on α-amino-3-hydroxy-5-methyl-4-isoxazolepropionate (AMPA) receptor [77]. Recent studies have confirmed the neuroprotective role of KYNA by opposing the QUIN effects and reducing excitotoxicity [9]. KYNA similarly acts as α7-nicotinic acetyl cholinergic receptor (α7AchR) antagonist, which plays an important role in the pathogenesis of schizophrenia [14]. Therefore, a higher KYNA level was found in CSF of schizophrenic patients, around glutamatergic and dopaminergic site [78]. In some recent studies, G protein coupled receptor 35 (GPR35) and aryl hydrocarbon receptor (AhR), are the two receptors to which KYNA demonstrate agonistic effects. GPR35 is expressed in immune cells of gastrointestinal tissues and circulation monocytes. After activation of GPR35 by KYNA, promotion of monocyte extravasation, reduced inflammatory response to lipopolysaccharide, and regulated cytokine release were observed [39]. KYNA can ameliorate immune activation via AhR expression [51]. 4-chloro-kynunrenine a prodrug of KYNA, which can easily pass through BBB, has shown ketamine-like anti-depressant effects. Neurobehavioral changes, induced by 4-chloro-kynunrenine were compared with fluoxetine and ketamine, and the changes were significantly different with both of them [79]. In our research work, we have found that PGC-1α and KATs genes were significantly expressed and subsequently caused an increased KAT protein translation by the exercise-fluoxetine combination, in soleus and gastrocnemius muscle, respectively. The significantly increase level of PGC-1α and KATs gene, KAT protein and KYNA was confirmed in soleus muscle. Accordingly, such as some previous studies, we confirmed that the plasma levels of KP metabolites were remarkably changed by exercise and fluoxetine alone or in combination (Tutakhail et al., in preparation). We also found that the anxiolytic effects of exercise-fluoxetine combination were correlated to the KP metabolites level in the brain and muscles.
3-Hydroxykynurenine
3-HK is the neuroactive metabolite of KYN, catalyzed by kynureninase [29, 80]. The physiological role of this metabolite has not been known yet. The risk related to 3-HK can easily pass through BBB contrarily to other metabolites [3]. Many studies have shown that immune stimulation especially interferon-α increases the synthesis of 3-HK [67]. Contrary to QUIN and KYNA, its binding site and affinity with NMDA receptor have not been confirmed, and it is supposed that the neurotoxicity of 3-HK is associated to the ability of ROS and H2O2 production in CNS [19]. The intermediate metabolite of 3-HK, 3-HAA is capable of producing autoxidation as well as superoxide anion and ROS [80].
Tryptophan Metabolism and Related Neuropathologies
Neuropsychiatric Disorders
Schizophrenia
Kynurenine pathway of tryptophan degradation produces various neuroactive metabolites [33]. The kynurenic acid hypothesis of schizophrenia is based on the kynurenic acid activity in CNS as NMDA and α7AchR receptors antagonist [14] This hypothesis, supported by different studies, shows elevated KYNA CNS level in schizophrenic patient [78, 81]. KYNA is a neuroprotective metabolite, but it is well confirmed that elevated brain KYNA concentration is contributed to alteration in glutamatergic, cholinergic, and dopaminergic signaling [76]. Some CSF and postmortem studies have confirmed the initial study reports about KYNA brain level elevation, both in drug-treated [82, 83], and drug-naïve schizophrenia patients [84]. KYN, the precursor of KYNA, has been also observed elevated both in CSF and cortical brain region of patients diagnosed with schizophrenia [11, 83]. 3-HK is seemed to be elevated in human dermal fibroblast in schizophrenia disease [85]. Similarly, another metabolite of KP, anthranilic acid, is also found to be increased in schizophrenia [86]. Interestingly, it has also been observed that the CNS KYNA level was higher in patient of schizophrenia with HIV infection, than in schizophrenia-diagnosed individuals without HIV infection [87]. It should be mentioned that plasma level of KYNA was observed both elevated [88] and decreased in schizophrenia [13, 14]. KYNA cannot cross the blood-brain barrier in normal condition [89]; therefore, the relation between plasma concentration and CSF, saliva, and other tissues could not be assessed comprehensively.
There are many factors which control KYNA brain level: (1) The brain level of some amino acids, such as glutamine, L-α aminoadipate and phenylalanine, which are competitive substrates for KAT 1 and 2 [90]; (2) KYN and probenecid as active pharmacological agents inhibit the efflux of KYNA out of the CNS; and (3) drugs inhibiting the neurotoxic branch of KP (blocking KMO and production of QUIN) [91,92,93].
According to some old and recent studies, indomethacin and diclofenac, inhibitor of COX-1, elevate brain level of KYNA [93, 94]. Whereas, the formation of KYNA is indirectly controlled by KMO activity; some recent studies have confirmed that the expression of KMO gene and KMO activity is reduced in the prefrontal cortex and ocular field of patients diagnosed with schizophrenia [82, 95]. There is a narrow relation between inflammation and KP, thus it is suggested that neuroinflammation or infection might be causal factor, underlying pathophysiology of schizophrenia [96, 97]. Some epidemiological studies have shown that offspring whose mothers were seropositive during pregnancy are more vulnerable for schizophrenia [98]. Enhanced activation of cytokines, recruitment of T cell, and neurodegeneration are the most known hallmarks of neuroinflammation. Whereas, interleukin plays inflammatory and non-inflammatory role, hereby IL-1β and IL-6 involvement in activation of KP is markedly considerable [15, 94, 96]. A postmortem study of patients diagnosed with schizophrenia has confirmed a higher level of mRNA of IDO and TDO expression, and TDO2 immunopositive astroglial cell in prefrontal cortex, than that of control subjects [99]. As TDO2 is located in astrocytes, thus the mentioned upregulation would lead to production of KYNA. Studies have shown that KYN administration in rodents, either in adolescence or during late pre-natal development stage, is associated with impaired neurobehavioral and social interaction, cognitive flexibility, and long-term potentiation [100,101,102].
Some behavioral investigations show that neonatal administration of L-kynurenine as well as infection was associated with increased responsiveness to d-amphetamine in the open field, disrupts prepulse inhibition (PPI), and reduces working memory [100, 101]. CSF level of KYNA has been confirmed to correlate with CSF 5-hydroxyindoleacetic acid (5-HIAA), but the reason for this correlation is unknown [102]. Low CSF 5-HIAA concentration, a clear sign of serotoninergic system deficit, can be contributed to mood disorders and suicidal behaviors [103].
Bipolar Disorders
Bipolar disorder (BD) is characterized by two episodes, manic and depressive [104]. The pathophysiology of bipolar disorder is less clear than other major psychiatric disorders [105]. There are three pathophysiologic hypotheses suggesting the mechanism of BD: (1) electrical signaling; (2) parasynaptic neurotransmitter-receptor signaling system; and (3) post-receptor neuro-chemical signaling [106]. Studies have been carried out to find the relation of BD with biogenic amino acids, but the result was inconsistent [107, 108]. Genetic studies on tryptophan hydroxylase and serotonin transporter gene have also shown controversial results [109, 110]. Recent studies have shown the involvement of NMDA receptor in manic relapse [111], and similarly the upregulation of KP was demonstrated in postmortem anterior cingulated cortex in patients diagnosed with BD [47]. The role of NMDA receptor involvement related to cytokine-serotonin system interaction through IDO is suggested to be responsible in the treatment resistance against major depressive disorders [112]. The ratio between kynurenic acid and kynurenine is lower in major depression, and this impaired neuroprotection is proposed to be involved in the pathophysiology of bipolar disorders, which is also NMDA receptor-dependent mood disorder [14].
Major Depressive Disorders
MDD is a major neurological problem around the world and will be the leading cause of years lost to disability in 2030 [113]. The role of KP in MDD is studied with its molecular and genetics level [49, 112]. It is strongly suggested that stressful life condition is associated with decreased brain-derived neurotropic factor (BDNF) and increased 3-HK level, and the myokine, so-called irisin (exercise hormone) and QUIN would be novel serum biomarkers of cognitive impairments [114]. In recent studies, exercise-induced BDNF alterations have been attributed to the irisin and KP. KP is a link between tringle of lifestyle factors, cognitive activity, and neuroplasticity [114]. Particularly, a decreased level of neuroprotective KP metabolite (KYNA) and increased level of neurotoxic KP metabolite (QUIN) were detected in several mood disorder types [115]. Whereas among mammals, females have greater expression of toll-like receptor (TLR), increased interferon-1 activity, elevated activity and number of macrophages, T cells, and B cells; therefore, they are more vulnerable to KP-induced major depressive disorders [116]. Studies have shown that lipopolysaccharides did not induce depression in rodents when the KP was blocked genetically or pharmacologically, even if the pro-inflammatory cytokines were remained elevated [115].
Major depressive disorder is a heterogeneous neurological problem characterized by low mood and anxiety, loss of interest, and pleasure in normally enjoyable life activities. Neurodegenerative and somatic symptoms and neurocognitive impairments are also the particular clinical symptoms. Whereas, the exact pathomechanism of MDD is still not been well known, but the most predominant nervous monoamine systems (5-HTergic, adrenergic and dopaminergic) are counted to be the most involved factors in MD. A huge body of evidences confirms that hypothalamo-pituitary-adrenal (HPA) axis hyperactivity is also associated to the pathogenesis of MDD. HPA system to the response of chronic stress increases the release of corticotropin and cortisol [117].
During the last two decades, the relationship between depression and some pathological conditions such as inflammatory and neurodegenerative disorders, diabetes, and cardiovascular disease have received progressively more attention in research [5, 49]. It is worth to mention that various diseases may contribute to direct or indirect pathophysiological effect on the brain [118]. Inflammation is a good example of the above-mentioned chronic somatic disease, which is strongly attributed to the neuropsychiatric deviations such as MDD [119]. Immune activation, the serotoninergic system, and KP are closely linked via few shared characteristics such as IDO1/2, HPA system and neurodegeneration [3, 112, 120]. A tight link is confirmed between the induction of IDO and neuropsychiatric symptoms, in patients suffering from immunopathologies [121]. In vitro, it was shown that IDO induction via T cell activation removed all the available tryptophan in culture medium within 48 h [122]. Due to immunobiochemical interaction between 5-HT biosynthesis and inflammation, a remarkable increased depressive-like behaviors were observed in patients with chronic inflammatory disorders [48, 122,123,124]. Some studies have shown that anti-depressants such as imipramine, venlafaxine, fluoxetine, and sertraline attenuate the expression of inflammatory biomarkers, responsible for the depressive symptoms and reduced TNF-γ/IL-10 ratio [125]. According to a recent study, serum IL-6 level represents a predictable biomarker for ketamine’s anti-depressive effects in patient with treatment-resistant depression [126]. These prove confirm the mutual effects between inflammation and depression.
The hippocampus and cortex are the most pivotal brain areas where the KP metabolites commence their toxic effects [23, 27]. Following inflammation, induced by peripheral lipopolysaccharides treatment, neuroactive metabolites level of KP was evaluated in the dorsal hippocampus, ventral hippocampus, central amygdala, and nucleus accumbens. KYN, 3-HK, QUIN, and XA levels were elevated in all aforementioned brain area, but in the dorsal hippocampus, the level was significantly higher for neurotoxic metabolites [27]. These changes were not seen in KMO−/− hydroxyanthranilic acid dioxygenase knockout (HAAO−/−) mice. While depressive-like neurobehavioral changes were re-expressed by 3-HK subcutaneous administration in dose-dependent manner. The IDO1 inhibitor, 1-MT (1-methyl tryptophan), in the same manner decrease KP neurotoxic branch metabolites in the hippocampus and cortex, and consequently decreased the depressive-like behaviors [23].
BDNF is necessary for normal brain activity [125, 127]. Studies show that BDNF−/+ mice are more vulnerable to low level stress than wild-type mice [127]. In some recent researches, the relations between stress, inflammation, KP induction in hippocampus and forebrain as well as the role of BDNF in modulation this pathway was studied. It was also confirmed that the anti-inflammatory cytokine, IL-10, was not expressed in heterozygous BDNF−/+ mice. IL-10, which negatively modulates microglia activation, was significantly increased in the hippocampus and forebrain of wild-type mice [128]. KYNA was increased in wild-type mice due to astrocytes activation, while 3-HK was increase in BDNF−/+ mice due to microglia activation, after unpredictable mild stress [128]. This study shows that stress-sensitive BDNF−/+ mice are more vulnerable to mild stress application, which induce the neurotoxic branch of KP by producing neurotoxic metabolites such as 3-HK and subsequently QUIN. The real molecular mechanism between BDNF deficiency and depressive-like behavior remains unclear, and further studies are suggested in this regard. Depressive-like behaviors were raised by lipopolysaccharide-induced inflammation, via BDNF-TrkB pathway alteration in the prefrontal cortex, hippocampus, and nucleus accumbens [125]. These effects were confirmed by BDNF receptor TrkB (tropomycin receptor kinase B), agonist and antagonist. BDNF expression is decreased in PFC and, CA3 and dentate gyrus area of the hippocampus and decrease in nucleus accumbens [129] of patients with depressive symptoms [125]. Stressful life events were confirmed to be associated with reduced BDNF and increased 3-HK serum level [114]. Some experiments show the involvement of BDNF in positive effects of physical exercise, which have been linked to the induction of physical exercise–activated myokine irisin (exercise hormone) and KP [114, 130]. Irisin is cleaved from the transmembrane receptor fibronectin type III domain-containing 5 (FNDC5) in skeletal muscle and secreted into the periphery as a myokine from where it acts on adipocytes. FNDC5 which is expressed by physical exercise resulted in elevated irisin and BDNF and subsequent stimulated hippocampal neurogenesis in vitro [131].
Neurodegenerative Diseases
Multiple Sclerosis
Multiple sclerosis (MS) is one of the most known neurodegenerative disorder, attributed to impaired KP metabolism and altered KP intermediates presence in CNS [132]. It is thought that MS progression is due to the activation of pro-inflammatory cytokines IFN-gamma and TNF-alpha, thereby related to IDO1 expression [133]. KAT activity as a compensatory mechanism was elevated in plasma of MS patients.
Some recent studies have strongly suggested the role of KP in prevalence of Huntington disease (HD) [118, 134]. The clear evidence of involvement of neurotoxic/neuroinflammatory branch of KP and HD was found in animal studies and in HD patients [135]. The level of neuroprotective KP’s metabolite, KYNA, was decreased in the brain cortex, striatum, and CSF, whereas QUIN, 3-HK, and other neurotoxic metabolites levels were elevated in MS [135] . In mice model of HD, the inhibition of KMO has shown a decrease in neurodegeneration and a significant amelioration of the MS pathology [136]. Depressive symptoms caused by IFN-α, which activates IDO1, enhances KP and decreases serotonin availability. This phenomenon was confirmed in patients undergoing IFN treatment for hepatitis C or cancer [123]. Beside serotonin degradation by MAO to 5-hydroxyindolacetic acid, IDO1 also catabolize serotonin into formyl-5-hydroxykynuramine [123]. As the serotonergic system alteration have been directly related to MS [137], therefore this co-metabolism of serotonin will further exacerbates the depressive state due to the serotonin deficiency which subsequently affects the neurotransmission of dopamine, norepinephrine, and melatonin. IDO also degrades melatonin, the circadian rhythm regulator, into N-acetyl-N-formyl-5-methoxykunuramine within KP and mediate seizure activity in MS [138]. As the melatonin precursor, serotonin level is already decreased in inflammatory state and melatonin production is disrupted. These two additive mechanisms worsen the MS pathology [139].
Parkinson’s Disease
Parkinson’s disease (PD) is a long-term neurodegenerative worldwide CNS disease that mainly effects the motor neurons and induced by multiple pathogenic factors which are not yet fully elucidated [140]. PD effects 1% of world’s population aged over 60 [141]. It is characterized by tremor, bradykinesia, limb rigidity, and freezing of gait due to progressive degeneration of dopaminergic system neurons [142]. KP is one of the inducible causes of PD [140, 143]. Lower plasma level of TRP, KYN, KYNA, and KYNA/KYN, and higher level of QUIN/KYNA ratio were confirmed in a cohort study of 118 PD patients compared with normal controls [144]. Kynurenine pathway’s abnormality and production of neuroactive toxic metabolites have been closely linked to PD [143]. The NMDA receptor activation, excitotoxicity and lesion to the brain, lipid peroxidation in iron dependent manner, ROS production [145], and similarly the increase in brain nitric oxide synthase level are the most cited mechanisms attributed to QUIN-induced PD [144]. QUIN level in the striatum and cortex was elevated, whereas the KYNA level in striatum and CSF was significantly reduced in patients diagnosed with PD [145]. Some recent works demonstrated a significant change in the KP plasma metabolites in PD patients with levodopa induced dyskinesia (LID) compared with non-LID [146]. The increased 3-HK/KYN and decreased 3-HAA/3HK and XA/3-HK plasma levels are directly related to the elevated KMO activity [144]. As the absolute plasma level of TRP and KYN was not significantly different between PD and non-PD patients, it supports that the KP was shifted toward increased level 3-HK by KMO activity and decreased KYNA and anthranilic acid [146]. The enhanced 3-HK/KYN plasma level and its special tendency toward CSF suggest that this specific change in KP have being carried out in synaptic zone of basal ganglia, where it activates glutamatergic neurotransmission [147]. The main factor in this change is higher activity of NMDR, potentiated by endogenous glycine and pre-synaptic nicotinic acetyl-choline receptors in glutamatergic terminal, following low KYNA level [148]. Increased level of 3-HK or QUIN potentiates oxidative stress, however decreased level of KYNA increases excitotoxicity which may contribute to the striatal spine loss and development of PD [149]. LID in PD was removed in MTPT model monkeys by enhancing brain KYNA level using systemic treatment with KMO inhibitor [150]. Many recent researches have shown increased KYN/TRP ratio in plasma and increased 3-HK/KYNA ratio in postmortem CSF of patients diagnosed with PD [151]. Elevated level of 3-HK and lower level of KYNA was found in the frontal cortex, putamen, and substantia nigra of PD patients [143]. Factors such as advanced PD, oxidative stress, and Sever’s inflammation may contribute to the neurotoxic branch of KYN metabolism [152]. TRP-KYN pathway metabolism is also influenced by gut microbiota which induces significant neurological consequences [153].
Alzheimer’s Disease
As discussed above, KP is a complicated pathway with various metabolites, representing different effects in the CNS. According to some previous studies, these metabolites are proposed to be remarkable Alzheimer’s disease–inducing agents [154]. A positive correlation was found between cognitive function test and KYNA plasma level, and an inversed correlation was found between the mentioned test and QUIN level in CNS [155]. There are many mechanisms to be attributed for KP-induced AD [156]. Overstimulation of NMDA receptor by QUIN following by neurons death during excitotoxicity [77], neuronal dysfunction [157, 158], ROS production, lipid peroxidation, and production of TNF-α, IFN-γ, and IL-1β by astrocyte induction [73, 158] are the most suggested mechanisms. Immune system modification, IDO induction, and QUIN have been found to have considerable result in AD research [155]. Contrarily to the QUIN, the serum level of KYNA was found decreased in AD patients [159]. The relation between beta amyloid protein (Aβ1-42) level and KP was studied, and potential positive correlation was found. Human IDO mRNA was expressed by Aβ1-42 in macrophage and microglia of patients diagnosed with AD [160]. QUIN and Aβ1-42 synergistically induce cytokine production such as TNF-α, IFN-γ, and IL-1β [158]. Continued circulatory TNF-α and IFN-γ re-stimulate Aβ1-42 and IDO production [161]. This is responsible for senile plaque production inflammatory process as a countable factor in AD pathology. In a recent research, the KP metabolites such as 3-HK and 3-HAA have been found to increase Cu++-induced neurotoxicity in rat astrocyte culture [29]. Chemically, both Cu++ and the KP metabolites are capable for neurodegeneration in AD. A remarkable number of studies suggest that 3-HK, which is found in nanomolar level in the brain during normal conditions and increases 3 times during neurodegenerative disorder, is able: (1) to induce cell death through apoptosis, both in brain regions and/or cell culture [162]; (2) to induce DNA fragmentation and chromatin condensation [162]; (3) to generate oxidative stress and protein aggregation [163]. 3-HAA is also confirmed to damage protein due to its interaction to metals in neuronal culture [163] and produces hydroxyl radical through Fenton’s reaction [157]. 3-HAA is able to produce uncoupling effects during oxidative phosphorylation, and consequently decreased oxygen consumption-activating astrocyte and leads to neuronal death [157]. Thus, we conclude that 3-HK, 3-HAA, and QUIN may be the most toxic metabolites of KP involved in AD. Furthermore, QUIN is found with hyperphosphorylated tau (tubulin-associated unit) protein (pathological protein of AD) and induces its phosphorylation in cortical neurons in patients diagnosed with AD-type dementia [164].
Conclusion
Metabolic pathways of different biological system are the most important targets in the study of disease diagnosis, diversified metabolism, drug development and design, and the interaction between body systems in various pathologies. Changes or disruption in the balance of indigenous metabolites can lead to the induction of varied consequences and may be sometimes dangerous to human or animal health. In recent studies, kynurenine pathway is confirmed to be induce by pro-inflammatory cytokines, oxidative stress, cancer, environmental factors and lead to different pathologies such as psychotic disorders, neurodegenerative disorders, and behavioral impairments. In summary, we conclude that the imbalance in KP or divert metabolism might be attributed to behavioral impairment, major depressive disorders, schizophrenia, Alzheimer’s disease, and Parkinson’s disease. Meanwhile, the related enzyme and catabolite production are strongly suggested to be studied more in order to elucidate the concrete involvement and highlight the mechanisms which have not yet been known.
Chemical machinery of KP takes place in the brain, hepatic and extrahepatic level of the body. Therefore, the correlation, the interactions, the pathomechanism, the role of microbiota, and finally the treatment through KP are worthy for more attention in the treatment of the abovementioned pathologies. For screening and diagnostic purposes, it would be beneficial to measure the KP metabolites in order to achieve the suitable treatment goals (Tables 1 and 2 ).
Abbreviations
- KP:
-
Kynurenine pathway
- KYN:
-
Kynurenine
- KYNA:
-
Kynurenic acid
- TRP:
-
Tryptophan
- 3-HK:
-
3-Hydroxykynurenine
- AA:
-
Anthranilic acid
- XA:
-
Xanthurenic acid
- TDO:
-
Tryptophan 2, 3 dioxygenase
- IDO:
-
Indoleamine 2, 3 dioxygenase
- KAT:
-
Kynurenine aminotransferase
- KMO:
-
Kynurenine monoxygenase
- NAD:
-
Nicotinamide adenine dinucleotide
- BDL:
-
Bile duct ligation
- NMDA:
-
N-methyl D-aspartate
- GSH:
-
Glutathione
- TPH:
-
Tryptophan hydroxylase
- 5-HIAA:
-
5-hydroxyindoleacetic acid
- BD:
-
Bipolar disorders
- HD:
-
Huntington disease
- AD:
-
Alzheimer’s disease
- PD:
-
Parkinson’s disease
- MDD:
-
Major depressive disorders
- TLR:
-
Toll-like receptors
- MT:
-
1-Methyl tryptophan
- BDNF:
-
Brain-derived neurotrophic factor
- TrkB:
-
Tropomycin receptor kinase B
- PFC:
-
Prefrontal cortex
- CA3:
-
Cornu ammonis of hippocampus
- MS:
-
Multiple sclerosis
- FNDC5:
-
Fibronectin type III domain containing 5
- CSF:
-
Cerebrospinal fluid
- PPI:
-
Prepulse Inhibition
- MPTP:
-
1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine
- PIC:
-
Picolinic acid
References
Austin CJD, Rendina LM. Targeting key dioxygenases in tryptophan-kynurenine metabolism for immunomodulation and cancer chemotherapy. Drug Discov Today. 2015;20:609–17.
Opitz CA, Heiland I. Dynamics of NAD-metabolism: everything but constant. Biochem Soc Trans. 2015;43:1127–32.
Moyer BJ, Rojas IY, Murray IA, Lee S, Hazlett HF, Perdew GH, et al. Indoleamine 2,3-dioxygenase 1 (IDO1) inhibitors activate the aryl hydrocarbon receptor. Toxicol Appl Pharmacol. 2017;323:74–80.
Brandacher G, Hoeller E, Fuchs D, Weiss HG. Chronic immune activation underlies morbid obesity: is IDO a key player? Curr Drug Metab. 2007;8:289–95.
Sarkar SA, Wong R, Hackl SI, Moua O, Gill RG, Wiseman A, et al. Induction of indoleamine 2,3-dioxygenase by interferon-gamma in human islets. Diabetes. 2007;56:72–9.
Chen W. IDO: more than an enzyme. Nat Immunol. 2011;12:809–11.
Bessede A, Gargaro M, Pallotta MT, Matino D, Servillo G, Brunacci C, et al. Aryl hydrocarbon receptor control of a disease tolerance defence pathway. Nature. 2014;511:184–90.
Fujigaki H, Yamamoto Y, Saito K. L-tryptophan-kynurenine pathway enzymes are therapeutic target for neuropsychiatric diseases: focus on cell type differences. Neuropharmacology. 2017;112:264–74.
Badawy AA-B. Tryptophan availability for kynurenine pathway metabolism across the life span: control mechanisms and focus on aging, exercise, diet and nutritional supplements. Neuropharmacology. 2017;112:248–63.
Oxenkrug G. Interferon-gamma - inducible inflammation: contribution to aging and aging-associated psychiatric disorders. Aging Dis. 2011;2:474–86.
Raison CL, Dantzer R, Kelley KW, Lawson MA, Woolwine BJ, Vogt G, et al. CSF concentrations of brain tryptophan and kynurenines during immune stimulation with IFN-alpha: relationship to CNS immune responses and depression. Mol Psychiatry. 2010;15:393–403.
Baranyi A, Meinitzer A, Breitenecker RJ, Amouzadeh-Ghadikolai O, Stauber R, Rothenhäusler H-B. Quinolinic acid responses during interferon-α-induced depressive symptomatology in patients with chronic hepatitis C infection - a novel aspect for depression and inflammatory hypothesis. PLoS One. 2015;10:e0137022.
Steiner J, Walter M, Gos T, Guillemin GJ, Bernstein H-G, Sarnyai Z, et al. Severe depression is associated with increased microglial quinolinic acid in subregions of the anterior cingulate gyrus: evidence for an immune-modulated glutamatergic neurotransmission? J Neuroinflammation. 2011;8:94.
Myint A-M, Kim YK, Verkerk R, Scharpé S, Steinbusch H, Leonard B. Kynurenine pathway in major depression: evidence of impaired neuroprotection. J Affect Disord. 2007;98:143–51.
Schwieler L, Samuelsson M, Frye MA, Bhat M, Schuppe-Koistinen I, Jungholm O, et al. Electroconvulsive therapy suppresses the neurotoxic branch of the kynurenine pathway in treatment-resistant depressed patients. J Neuroinflammation. 2016;13:51.
Bay-Richter C, Linderholm KR, Lim CK, Samuelsson M, Träskman-Bendz L, Guillemin GJ, et al. A role for inflammatory metabolites as modulators of the glutamate N-methyl-D-aspartate receptor in depression and suicidality. Brain Behav Immun. 2015;43:110–7.
Cho HJ, Savitz J, Dantzer R, Teague TK, Drevets WC, Irwin MR. Sleep disturbance and kynurenine metabolism in depression. J Psychosom Res. 2017;99:1–7.
Schwarcz R, Bruno JP, Muchowski PJ, Wu H-Q. Kynurenines in the mammalian brain: when physiology meets pathology. Nat Rev Neurosci. 2012;13:465–77.
Refaey ME, McGee-Lawrence ME, Fulzele S, Kennedy EJ, Bollag WB, Elsalanty M, et al. Kynurenine, a tryptophan metabolite that accumulates with age, induces bone loss. J Bone Miner Res Off J Am Soc Bone Miner Res. 2017;32:2182–93.
Matthews KA, Schott LL, Bromberger JT, Cyranowski JM, Everson-Rose SA, Sowers M. Are there bi-directional associations between depressive symptoms and C-reactive protein in mid-life women? Brain Behav Immun. 2010;24:96–101.
Prescott C, Weeks AM, Staley KJ, Partin KM. Kynurenic acid has a dual action on AMPA receptor responses. Neurosci Lett. 2006;402:108–12.
Moroni F, Cozzi A, Sili M, Mannaioni G. Kynurenic acid: a metabolite with multiple actions and multiple targets in brain and periphery. J Neural Transm Vienna Austria 1996. 2012;119:133–9.
Jiang X, Xu L, Tang L, Liu F, Chen Z, Zhang J, et al. Role of the indoleamine-2,3-dioxygenase/kynurenine pathway of tryptophan metabolism in behavioral alterations in a hepatic encephalopathy rat model. J Neuroinflammation. 2018;15:3.
O’Connor JC, André C, Wang Y, Lawson MA, Szegedi SS, Lestage J, et al. Interferon-gamma and tumor necrosis factor-alpha mediate the upregulation of indoleamine 2,3-dioxygenase and the induction of depressive-like behavior in mice in response to bacillus Calmette-Guerin. J Neurosci. 2009;29:4200–9.
Walker AK, Budac DP, Bisulco S, Lee AW, Smith RA, Beenders B, et al. NMDA receptor blockade by ketamine abrogates lipopolysaccharide-induced depressive-like behavior in C57BL/6J mice. Neuropsychopharmacology. 2013;38:1609–16.
Heisler JM, O’Connor JC. Indoleamine 2,3-dioxygenase-dependent neurotoxic kynurenine metabolism mediates inflammation-induced deficit in recognition memory. Brain Behav Immun. 2015;50:115–24.
Parrott JM, O’Connor JC. Kynurenine 3-monooxygenase: an influential mediator of neuropathology. Front Psychiatry. 2015;6:116.
Wejksza K, Rzeski W, Okuno E, Kandefer-Szerszen M, Albrecht J, Turski WA. Demonstration of kynurenine aminotransferases I and II and characterization of kynurenic acid synthesis in oligodendrocyte cell line (OLN-93). Neurochem Res. 2005;30:963–8.
Ramírez-Ortega D, Ramiro-Salazar A, González-Esquivel D, Ríos C, Pineda B, Pérez de la Cruz V. 3-Hydroxykynurenine and 3-hydroxyanthranilic acid enhance the toxicity induced by copper in rat astrocyte culture. Oxidative Med Cell Longev. 2017;2017:2371895.
Baran H, Staniek K, Bertignol-Spörr M, Attam M, Kronsteiner C, Kepplinger B. Effects of various kynurenine metabolites on respiratory parameters of rat brain, liver and heart mitochondria. Int J Tryptophan Res. 2016;9:17–29.
Vazquez S, Garner B, Sheil MM, Truscott RJ. Characterisation of the major autoxidation products of 3-hydroxykynurenine under physiological conditions. Free Radic Res. 2000;32:11–23.
Hirrlinger J, Dringen R. The cytosolic redox state of astrocytes: maintenance, regulation and functional implications for metabolite trafficking. Brain Res Rev. 2010;63:177–88.
Bryleva EY, Brundin L. Kynurenine pathway metabolites and suicidality. Neuropharmacology. 2017;112:324–30.
Fond G, Loundou A, Rabu C, Macgregor A, Lançon C, Brittner M, et al. Ketamine administration in depressive disorders: a systematic review and meta-analysis. Psychopharmacology. 2014;231:3663–76.
Maes M, Leonard BE, Myint AM, Kubera M, Verkerk R. The new “5-HT” hypothesis of depression: cell-mediated immune activation induces indoleamine 2,3-dioxygenase, which leads to lower plasma tryptophan and an increased synthesis of detrimental tryptophan catabolites (TRYCATs), both of which contribute to the onset of depression. Prog Neuro-Psychopharmacol Biol Psychiatry. 2011;35:702–21.
Bradley KAL, Case JAC, Khan O, Ricart T, Hanna A, Alonso CM, et al. The role of the kynurenine pathway in suicidality in adolescent major depressive disorder. Psychiatry Res. 2015;227:206–12.
Vikelis M, Mitsikostas DD. The role of glutamate and its receptors in migraine. CNS Neurol Disord Drug Targets. 2007;6:251–7.
Vécsei L, Majláth Z, Balog A, Tajti J. Drug targets of migraine and neuropathy: treatment of hyperexcitability. CNS Neurol Disord Drug Targets. 2015;14:664–76.
Sas K, Szabó E, Vécsei L. Mitochondria, oxidative stress and the kynurenine system, with a focus on ageing and neuroprotection. Molecules Basel Switz. 2018;23.
Gasparini CF, Griffiths LR. The biology of the glutamatergic system and potential role in migraine. Int J Biomed Sci. 2013;9:1–8.
Behan WM, McDonald M, Darlington LG, Stone TW. Oxidative stress as a mechanism for quinolinic acid-induced hippocampal damage: protection by melatonin and deprenyl. Br J Pharmacol. 1999;128:1754–60.
Tavares RG, Tasca CI, Santos CE, Wajner M, Souza DO, Dutra-Filho CS. Quinolinic acid inhibits glutamate uptake into synaptic vesicles from rat brain. Neuroreport. 2000;11:249–53.
Kemp JA, Foster AC, Leeson PD, Priestley T, Tridgett R, Iversen LL, et al. 7-Chlorokynurenic acid is a selective antagonist at the glycine modulatory site of the N-methyl-D-aspartate receptor complex. Proc Natl Acad Sci U S A. 1988;85:6547–50.
Sas K, Robotka H, Rózsa E, Agoston M, Szénási G, Gigler G, et al. Kynurenine diminishes the ischemia-induced histological and electrophysiological deficits in the rat hippocampus. Neurobiol Dis. 2008;32:302–8.
Pompili M, Orsolini L, Lamis DA, Goldsmith DR, Nardella A, Falcone G, et al. Suicide prevention in schizophrenia: do long-acting injectable antipsychotics (LAIs) have a role? CNS Neurol Disord Drug Targets. 2017;16:454–62.
Jentsch JD, Roth RH. The neuropsychopharmacology of phencyclidine: from NMDA receptor hypofunction to the dopamine hypothesis of schizophrenia. Neuropsychopharmacology. 1999;20:201–25.
Miller CL, Llenos IC, Dulay JR, Weis S. Upregulation of the initiating step of the kynurenine pathway in postmortem anterior cingulate cortex from individuals with schizophrenia and bipolar disorder. Brain Res. 2006;1073–1074:25–37.
Stewart JC, Rand KL, Muldoon MF, Kamarck TW. A prospective evaluation of the directionality of the depression-inflammation relationship. Brain Behav Immun. 2009;23:936–44.
Zepf FD, Stewart RM, Guillemin G, Ruas JL. Inflammation, immunology, stress and depression: a role for kynurenine metabolism in physical exercise and skeletal muscle. Acta Neuropsychiatr. 2016;28:244–5.
Agudelo LZ, Femenía T, Orhan F, Porsmyr-Palmertz M, Goiny M, Martinez-Redondo V, et al. Skeletal muscle PGC-1α1 modulates kynurenine metabolism and mediates resilience to stress-induced depression. Cell. 2014;159:33–45.
Cervenka I, Agudelo LZ, Ruas JL. Kynurenines: Tryptophan’s metabolites in exercise, inflammation, and mental health. Science. 2017;357.
Wirleitner B, Neurauter G, Schröcksnadel K, Frick B, Fuchs D. Interferon-gamma-induced conversion of tryptophan: immunologic and neuropsychiatric aspects. Curr Med Chem. 2003;10:1581–91.
Musso T, Gusella GL, Brooks A, Longo DL, Varesio L. Interleukin-4 inhibits indoleamine 2,3-dioxygenase expression in human monocytes. Blood. 1994;83:1408–11.
Kanai M, Nakamura T, Funakoshi H. Identification and characterization of novel variants of the tryptophan 2,3-dioxygenase gene: differential regulation in the mouse nervous system during development. Neurosci Res. 2009;64:111–7.
Li J, Wang Y, Zhou R, Zhang H, Yang L, Wang B, et al. Association between tryptophan hydroxylase gene polymorphisms and attention deficit hyperactivity disorder in Chinese Han population. Am J Med Genet Part B Neuropsychiatr Genet. 2006;141B:126–9.
Li JS, Han Q, Fang J, Rizzi M, James AA, Li J. Biochemical mechanisms leading to tryptophan 2,3-dioxygenase activation. Arch Insect Biochem Physiol. 2007;64:74–87.
Metz R, Smith C, DuHadaway JB, Chandler P, Baban B, Merlo LMF, et al. IDO2 is critical for IDO1-mediated T-cell regulation and exerts a non-redundant function in inflammation. Int Immunol. 2014;26:357–67.
Saito K, Crowley JS, Markey SP, Heyes MP. A mechanism for increased quinolinic acid formation following acute systemic immune stimulation. J Biol Chem. 1993;268:15496–503.
Bender DA. Biochemistry of tryptophan in health and disease. Mol Asp Med. 1983;6:101–97.
Salter M, Knowles RG, Pogson CI. Quantification of the importance of individual steps in the control of aromatic amino acid metabolism. Biochem J. 1986;234:635–47.
Holmes EW. Determination of serum kynurenine and hepatic tryptophan dioxygenase activity by high-performance liquid chromatography. Anal Biochem. 1988;172:518–25.
Takeuchi F, Tsubouchi R, Izuta S, Shibata Y. Kynurenine metabolism and xanthurenic acid formation in vitamin B6-deficient rat after tryptophan injection. J Nutr Sci Vitaminol (Tokyo). 1989;35:111–22.
Pawlak D, Tankiewicz A, Matys T, Buczko W. Peripheral distribution of kynurenine metabolites and activity of kynurenine pathway enzymes in renal failure. J Physiol Pharmacol. 2003;54:175–89.
Gál EM, Sherman AD. L-kynurenine: its synthesis and possible regulatory function in brain. Neurochem Res. 1980;5:223–39.
Heyes MP, Chen CY, Major EO, Saito K. Different kynurenine pathway enzymes limit quinolinic acid formation by various human cell types. Biochem J. 1997;326(Pt 2):351–6.
Heyes MP, Achim CL, Wiley CA, Major EO, Saito K, Markey SP. Human microglia convert l-tryptophan into the neurotoxin quinolinic acid. Biochem J. 1996;320(Pt 2):595–7.
Schwarcz R, Pellicciari R. Manipulation of brain kynurenines: glial targets, neuronal effects, and clinical opportunities. J Pharmacol Exp Ther. 2002;303:1–10.
Bordelon YM, Chesselet MF, Nelson D, Welsh F, Erecińska M. Energetic dysfunction in quinolinic acid-lesioned rat striatum. J Neurochem. 1997;69:1629–39.
Santamaría A, Galván-Arzate S, Lisý V, Ali SF, Duhart HM, Osorio-Rico L, et al. Quinolinic acid induces oxidative stress in rat brain synaptosomes. Neuroreport. 2001;12:871–4.
Schwarcz R, Whetsell WO, Mangano RM. Quinolinic acid: an endogenous metabolite that produces axon-sparing lesions in rat brain. Science. 1983;219:316–8.
Kim JP, Choi DW. Quinolinate neurotoxicity in cortical cell culture. Neuroscience. 1987;23:423–32.
Laugeray A, Launay J-M, Callebert J, Surget A, Belzung C, Barone PR. Peripheral and cerebral metabolic abnormalities of the tryptophan-kynurenine pathway in a murine model of major depression. Behav Brain Res. 2010;210:84–91.
Guillemin GJ, Brew BJ, Noonan CE, Takikawa O, Cullen KM. Indoleamine 2,3 dioxygenase and quinolinic acid immunoreactivity in Alzheimer’s disease hippocampus. Neuropathol Appl Neurobiol. 2005;31:395–404.
Guillemin GJ, Kerr SJ, Brew BJ. Involvement of quinolinic acid in AIDS dementia complex. Neurotox Res. 2005;7:103–23.
Moroni F, Russi P, Lombardi G, Beni M, Carlà V. Presence of kynurenic acid in the mammalian brain. J Neurochem. 1988;51:177–80.
Stone TW. Neuropharmacology of quinolinic and kynurenic acids. Pharmacol Rev. 1993;45:309–79.
Stone TW, Addae JI. The pharmacological manipulation of glutamate receptors and neuroprotection. Eur J Pharmacol. 2002;447:285–96.
Erhardt S, Blennow K, Nordin C, Skogh E, Lindström LH, Engberg G. Kynurenic acid levels are elevated in the cerebrospinal fluid of patients with schizophrenia. Neurosci Lett. 2001;313:96–8.
Zanos P, Piantadosi SC, Wu H-Q, Pribut HJ, Dell MJ, Can A, et al. The prodrug 4-chlorokynurenine causes ketamine-like antidepressant effects, but not side effects, by NMDA/glycineB-site inhibition. J Pharmacol Exp Ther. 2015;355:76–85.
Goldstein LE, Leopold MC, Huang X, Atwood CS, Saunders AJ, Hartshorn M, et al. 3-Hydroxykynurenine and 3-hydroxyanthranilic acid generate hydrogen peroxide and promote alpha-crystallin cross-linking by metal ion reduction. Biochemistry. 2000;39:7266–75.
Schwarcz R, Rassoulpour A, Wu HQ, Medoff D, Tamminga CA, Roberts RC. Increased cortical kynurenate content in schizophrenia. Biol Psychiatry. 2001;50:521–30.
Sathyasaikumar KV, Stachowski EK, Wonodi I, Roberts RC, Rassoulpour A, McMahon RP, et al. Impaired kynurenine pathway metabolism in the prefrontal cortex of individuals with schizophrenia. Schizophr Bull. 2011;37:1147–56.
Linderholm KR, Skogh E, Olsson SK, Dahl M-L, Holtze M, Engberg G, et al. Increased levels of kynurenine and kynurenic acid in the CSF of patients with schizophrenia. Schizophr Bull. 2012;38:426–32.
Nilsson LK, Linderholm KR, Engberg G, Paulson L, Blennow K, Lindström LH, et al. Elevated levels of kynurenic acid in the cerebrospinal fluid of male patients with schizophrenia. Schizophr Res. 2005;80:315–22.
Johansson A-S, Owe-Larsson B, Asp L, Kocki T, Adler M, Hetta J, et al. Activation of kynurenine pathway in ex vivo fibroblasts from patients with bipolar disorder or schizophrenia: cytokine challenge increases production of 3-hydroxykynurenine. J Psychiatr Res. 2013;47:1815–23.
Oxenkrug G, van der Hart M, Roeser J, Summergrad P. Anthranilic acid: a potential biomarker and treatment target for schizophrenia. Ann Psychiatry Ment Health. 2016;4.
Atlas A, Gisslén M, Nordin C, Lindström L, Schwieler L. Acute psychotic symptoms in HIV-1 infected patients are associated with increased levels of kynurenic acid in cerebrospinal fluid. Brain Behav Immun. 2007;21:86–91.
Ravikumar A, Deepadevi KV, Arun P, Manojkumar V, Kurup PA. Tryptophan and tyrosine catabolic pattern in neuropsychiatric disorders. Neurol India. 2000;48:231–8.
Fukui S, Schwarcz R, Rapoport SI, Takada Y, Smith QR. Blood-brain barrier transport of kynurenines: implications for brain synthesis and metabolism. J Neurochem. 1991;56:2007–17.
Chang YF, Cauley RK, Chang JD, Rao VV. L-alpha-aminoadipate inhibits kynurenate synthesis in rat brain hippocampus and tissue culture. Neurochem Res. 1997;22:825–9.
Speciale C, Wu HQ, Cini M, Marconi M, Varasi M, Schwarcz R. (R,S)-3,4-dichlorobenzoylalanine (FCE 28833A) causes a large and persistent increase in brain kynurenic acid levels in rats. Eur J Pharmacol. 1996;315:263–7.
Röver S, Cesura AM, Huguenin P, Kettler R, Szente A. Synthesis and biochemical evaluation of N-(4-phenylthiazol-2-yl)benzenesulfonamides as high-affinity inhibitors of kynurenine 3-hydroxylase. J Med Chem. 1997;40:4378–85.
Clunie M, Crone L-A, Klassen L, Yip R. Psychiatric side effects of indomethacin in parturients. Can J Anaesth. 2003;50:586–8.
Schwieler L, Erhardt S, Nilsson L, Linderholm K, Engberg G. Effects of COX-1 and COX-2 inhibitors on the firing of rat midbrain dopaminergic neurons--possible involvement of endogenous kynurenic acid. Synapse. 2006;59:290–8.
Wonodi I, Stine OC, Sathyasaikumar KV, Roberts RC, Mitchell BD, Hong LE, et al. Downregulated kynurenine 3-monooxygenase gene expression and enzyme activity in schizophrenia and genetic association with schizophrenia endophenotypes. Arch Gen Psychiatry. 2011;68:665–74.
Sellgren CM, Kegel ME, Bergen SE, Ekman CJ, Olsson S, Larsson M, et al. A genome-wide association study of kynurenic acid in cerebrospinal fluid: implications for psychosis and cognitive impairment in bipolar disorder. Mol Psychiatry. 2016;21:1342–50.
Karlsson H. Viruses and schizophrenia, connection or coincidence? Neuroreport. 2003;14:535–42.
Canetta SE, Brown AS. Prenatal infection, maternal immune activation, and risk for schizophrenia. Transl Neurosci. 2012;3:320–7.
Miller CL, Llenos IC, Dulay JR, Barillo MM, Yolken RH, Weis S. Expression of the kynurenine pathway enzyme tryptophan 2,3-dioxygenase is increased in the frontal cortex of individuals with schizophrenia. Neurobiol Dis. 2004;15:618–29.
Asp L, Beraki S, Kristensson K, Ogren SO, Karlsson H. Neonatal infection with neurotropic influenza a virus affects working memory and expression of type III Nrg1 in adult mice. Brain Behav Immun. 2009;23:733–41.
Liu X-C, Holtze M, Powell SB, Terrando N, Larsson MK, Persson A, et al. Behavioral disturbances in adult mice following neonatal virus infection or kynurenine treatment--role of brain kynurenic acid. Brain Behav Immun. 2014;36:80–9.
Carlborg A, Winnerbäck K, Jönsson EG, Jokinen J, Nordström P. Suicide in schizophrenia. Expert Rev Neurother. 2010;10:1153–64.
Asberg M. Neurotransmitters and suicidal behavior. The evidence from cerebrospinal fluid studies. Ann N Y Acad Sci. 1997;836:158–81.
Barrett TB, Hauger RL, Kennedy JL, Sadovnick AD, Remick RA, Keck PE, et al. Evidence that a single nucleotide polymorphism in the promoter of the G protein receptor kinase 3 gene is associated with bipolar disorder. Mol Psychiatry. 2003;8:546–57.
Barrett TB, Emberton JE, Nievergelt CM, Liang SG, Hauger RL, Eskin E, et al. Further evidence for association of GRK3 to bipolar disorder suggests a second disease mutation. Psychiatr Genet. 2007;17:315–22.
Askland K, Parsons M. Toward a biaxial model of “bipolar” affective disorders: spectrum phenotypes as the products of neuroelectrical and neurochemical alterations. J Affect Disord. 2006;94:15–33.
Anguelova M, Benkelfat C, Turecki G. A systematic review of association studies investigating genes coding for serotonin receptors and the serotonin transporter: I. Affective disorders. Mol Psychiatry. 2003;8:574–91.
Mahmood T, Silverstone T. Serotonin and bipolar disorder. J Affect Disord. 2001;66:1–11.
Serretti A, Lilli R, Lorenzi C, Lattuada E, Cusin C, Smeraldi E. Serotonin transporter gene (5-HTTLPR) and major psychoses. Mol Psychiatry. 2002;7:95–9.
Bellivier F, Henry C, Szöke A, Schürhoff F, Nosten-Bertrand M, Feingold J, et al. Serotonin transporter gene polymorphisms in patients with unipolar or bipolar depression. Neurosci Lett. 1998;255:143–6.
Hoekstra R, Fekkes D, Loonen AJM, Pepplinkhuizen L, Tuinier S, Verhoeven WMA. Bipolar mania and plasma amino acids: increased levels of glycine. Eur Neuropsychopharmacol. 2006;16:71–7.
Myint AM, Kim YK. Cytokine-serotonin interaction through IDO: a neurodegeneration hypothesis of depression. Med Hypotheses. 2003;61:519–25.
Sheehan DV, Nakagome K, Asami Y, Pappadopulos EA, Boucher M. Restoring function in major depressive disorder: a systematic review. J Affect Disord. 2017;215:299–313.
Küster OC, Laptinskaya D, Fissler P, Schnack C, Zügel M, Nold V, et al. Novel blood-based biomarkers of cognition, stress, and physical or cognitive training in older adults at risk of dementia: preliminary evidence for a role of BDNF, irisin, and the kynurenine pathway. J Alzheimers Dis. 2017;59:1097–111.
Meier TB, Drevets WC, Teague TK, Wurfel BE, Mueller SC, Bodurka J, et al. Kynurenic acid is reduced in females and oral contraceptive users: implications for depression. Brain Behav Immun. 2018;67:59–64.
Klein SL, Flanagan KL. Sex differences in immune responses. Nat Rev Immunol. 2016;16:626–38.
Holsboer F. How can we realize the promise of personalized antidepressant medicines? Nat Rev Neurosci. 2008;9:638–46.
Pearson SJ, Reynolds GP. Increased brain concentrations of a neurotoxin, 3-hydroxykynurenine, in Huntington’s disease. Neurosci Lett. 1992;144:199–201.
Haroon et al., 2012 - PubMed - NCBI [Internet]. [cited 2018 Aug 14]. Available from: https://www-ncbi-nlm-nih-gov.gate2.inist.fr/pubmed/?term=Haroon+et+al.%2C+2012
Maddison DC, Giorgini F. The kynurenine pathway and neurodegenerative disease. Semin Cell Dev Biol. 2015;40:134–41.
Myint AM, Schwarz MJ, Verkerk R, Mueller HH, Zach J, Scharpé S, et al. Reversal of imbalance between kynurenic acid and 3-hydroxykynurenine by antipsychotics in medication-naïve and medication-free schizophrenic patients. Brain Behav Immun. 2011;25:1576–81.
Sperner-Unterweger B, Kohl C, Fuchs D. Immune changes and neurotransmitters: possible interactions in depression? Prog Neuro-Psychopharmacol Biol Psychiatry. 2014;48:268–76.
Jeon SW, Kim Y-K. Inflammation-induced depression: its pathophysiology and therapeutic implications. J Neuroimmunol. 2017;313:92–8.
Hashimoto K. Inflammatory biomarkers as differential predictors of antidepressant response. Int J Mol Sci. 2015;16:7796–801.
Zhang J-C, Yao W, Hashimoto K. Brain-derived neurotrophic factor (BDNF)-TrkB signaling in inflammation-related depression and potential therapeutic targets. Curr Neuropharmacol. 2016;14:721–31.
Yang J-J, Wang N, Yang C, Shi J-Y, Yu H-Y, Hashimoto K. Serum interleukin-6 is a predictive biomarker for ketamine’s antidepressant effect in treatment-resistant patients with major depression. Biol Psychiatry. 2015;77:e19–20.
Burke TF, Advani T, Adachi M, Monteggia LM, Hensler JG. Sensitivity of hippocampal 5-HT1A receptors to mild stress in BDNF-deficient mice. Int J Neuropsychopharmacol. 2013;16:631–45.
Dugan AM, Parrott JM, Redus L, Hensler JG, O’Connor JC. Low-level stress induces production of neuroprotective factors in wild-type but not BDNF+/− mice: interleukin-10 and kynurenic acid. Int J Neuropsychopharmacol. 2015;19:pyv089.
Berton O, McClung CA, Dileone RJ, Krishnan V, Renthal W, Russo SJ, et al. Essential role of BDNF in the mesolimbic dopamine pathway in social defeat stress. Science. 2006;311:864–8.
Jin Y, Sumsuzzman DM, Choi J, Kang H, Lee S-R, Hong Y. Molecular and functional interaction of the myokine irisin with physical exercise and Alzheimer’s disease. Molecules Basel Switz. 2018;23.
Wrann CD, White JP, Salogiannnis J, Laznik-Bogoslavski D, Wu J, Ma D, et al. Exercise induces hippocampal BDNF through a PGC-1α/FNDC5 pathway. Cell Metab. 2013;18:649–59.
Mancuso R, Hernis A, Agostini S, Rovaris M, Caputo D, Fuchs D, et al. Indoleamine 2,3 dioxygenase (IDO) expression and activity in relapsing-remitting multiple sclerosis. PLoS One. 2015;10:e0130715.
Lovelace MD, Varney B, Sundaram G, Lennon MJ, Lim CK, Jacobs K, et al. Recent evidence for an expanded role of the kynurenine pathway of tryptophan metabolism in neurological diseases. Neuropharmacology. 2017;112:373–88.
Manoharan S, Guillemin GJ, Abiramasundari RS, Essa MM, Akbar M, Akbar MD. The role of reactive oxygen species in the pathogenesis of Alzheimer’s disease, Parkinson’s disease, and Huntington’s disease: a mini review. Oxidative Med Cell Longev. 2016;2016:8590578.
Vécsei L, Szalárdy L, Fülöp F, Toldi J. Kynurenines in the CNS: recent advances and new questions. Nat Rev Drug Discov. 2013;12:64–82.
Zwilling D, Huang S-Y, Sathyasaikumar KV, Notarangelo FM, Guidetti P, Wu H-Q, et al. Kynurenine 3-monooxygenase inhibition in blood ameliorates neurodegeneration. Cell. 2011;145:863–74.
Malinova TS, Dijkstra CD, de Vries HE. Serotonin: a mediator of the gut-brain axis in multiple sclerosis. Mult Scler. 2018;24:1144–50.
Anderson G, Rodriguez M. Multiple sclerosis, seizures, and antiepileptics: role of IL-18, IDO, and melatonin. Eur J Neurol. 2011;18:680–5.
Rozov SV, Filatova EV, Orlov AA, Volkova AV, Zhloba ARA, Blashko EL, et al. N1-acetyl-N2-formyl-5-methoxykynuramine is a product of melatonin oxidation in rats. J Pineal Res. 2003;35:245–50.
Sveinbjornsdottir S. The clinical symptoms of Parkinson’s disease. J Neurochem. 2016;139(Suppl 1):318–24.
de Lau LML, Breteler MMB. Epidemiology of Parkinson’s disease. Lancet Neurol. 2006;5:525–35.
Lang AE, Lozano AM. Parkinson’s disease. First of two parts. N Engl J Med. 1998;339:1044–53.
Ogawa T, Matson WR, Beal MF, Myers RH, Bird ED, Milbury P, et al. Kynurenine pathway abnormalities in Parkinson’s disease. Neurology. 1992;42:1702–6.
Chang K-H, Cheng M-L, Tang H-Y, Huang C-Y, Wu Y-R, Chen C-M. Alternations of metabolic profile and kynurenine metabolism in the plasma of Parkinson’s disease. Mol Neurobiol. 2018:1–10.
Jauch D, Urbańska EM, Guidetti P, Bird ED, Vonsattel JP, Whetsell WO, et al. Dysfunction of brain kynurenic acid metabolism in Huntington’s disease: focus on kynurenine aminotransferases. J Neurol Sci. 1995;130:39–47.
Havelund JF, Andersen AD, Binzer M, Blaabjerg M, Heegaard NHH, Stenager E, et al. Changes in kynurenine pathway metabolism in Parkinson patients with L-DOPA-induced dyskinesia. J Neurochem. 2017;142:756–66.
Schwarcz R. Kynurenines and glutamate: multiple links and therapeutic implications. Adv Pharmacol. 2016;76:13–37.
Schwarz MJ, Guillemin GJ, Teipel SJ, Buerger K, Hampel H. Increased 3-hydroxykynurenine serum concentrations differentiate Alzheimer’s disease patients from controls. Eur Arch Psychiatry Clin Neurosci. 2013;263:345–52.
Amori L, Wu H-Q, Marinozzi M, Pellicciari R, Guidetti P, Schwarcz R. Specific inhibition of kynurenate synthesis enhances extracellular dopamine levels in the rodent striatum. Neuroscience. 2009;159:196–203.
Grégoire L, Rassoulpour A, Guidetti P, Samadi P, Bédard PJ, Izzo E, et al. Prolonged kynurenine 3-hydroxylase inhibition reduces development of levodopa-induced dyskinesias in parkinsonian monkeys. Behav Brain Res. 2008;186:161–7.
Lewitt PA, Li J, Lu M, Beach TG, Adler CH, Guo L, et al. 3-hydroxykynurenine and other Parkinson’s disease biomarkers discovered by metabolomic analysis. Mov Disord. 2013;28:1653–60.
Lim CK, Fernández-Gomez FJ, Braidy N, Estrada C, Costa C, Costa S, et al. Involvement of the kynurenine pathway in the pathogenesis of Parkinson’s disease. Prog Neurobiol. 2017;155:76–95.
Kennedy PJ, Cryan JF, Dinan TG, Clarke G. Kynurenine pathway metabolism and the microbiota-gut-brain axis. Neuropharmacology. 2017;112:399–412.
Pláteník J, Stopka P, Vejrazka M, Stípek S. Quinolinic acid-iron(ii) complexes: slow autoxidation, but enhanced hydroxyl radical production in the Fenton reaction. Free Radic Res. 2001;34:445–59.
Gulaj E, Pawlak K, Bien B, Pawlak D. Kynurenine and its metabolites in Alzheimer’s disease patients. Adv Med Sci. 2010;55:204–11.
Ardura-Fabregat A, Boddeke EWGM, Boza-Serrano A, Brioschi S, Castro-Gomez S, Ceyzériat K, et al. Targeting neuroinflammation to treat Alzheimer’s disease. CNS Drugs. 2017;31:1057–82.
Braidy N, Grant R, Adams S, Brew BJ, Guillemin GJ. Mechanism for quinolinic acid cytotoxicity in human astrocytes and neurons. Neurotox Res. 2009;16:77–86.
Ting KK, Brew BJ, Guillemin GJ. Effect of quinolinic acid on human astrocytes morphology and functions: implications in Alzheimer’s disease. J Neuroinflammation. 2009;6:36.
Hartai Z, Juhász A, Rimanóczy A, Janáky T, Donkó T, Dux L, et al. Decreased serum and red blood cell kynurenic acid levels in Alzheimer’s disease. Neurochem Int. 2007;50:308–13.
Guillemin GJ, Smythe GA, Veas LA, Takikawa O, Brew BJ. A beta 1-42 induces production of quinolinic acid by human macrophages and microglia. Neuroreport. 2003;14:2311–5.
Walker DG, Link J, Lue L-F, Dalsing-Hernandez JE, Boyes BE. Gene expression changes by amyloid beta peptide-stimulated human postmortem brain microglia identify activation of multiple inflammatory processes. J Leukoc Biol. 2006;79:596–610.
Okuda S, Nishiyama N, Saito H, Katsuki H. 3-Hydroxykynurenine, an endogenous oxidative stress generator, causes neuronal cell death with apoptotic features and region selectivity. J Neurochem. 1998;70:299–307.
Vazquez S, Aquilina JA, Jamie JF, Sheil MM, Truscott RJW. Novel protein modification by kynurenine in human lenses. J Biol Chem. 2002;277:4867–73.
Rahman A, Ting K, Cullen KM, Braidy N, Brew BJ, Guillemin GJ. The excitotoxin quinolinic acid induces tau phosphorylation in human neurons. PLoS One. 2009;4:e6344.
Forrest CM, McNair K, Pisar M, Khalil OS, Darlington LG, Stone TW. Altered hippocampal plasticity by prenatal kynurenine administration, kynurenine-3-monoxygenase (KMO) deletion or galantamine. Neuroscience. 2015;310:91–105.
Schroecksnadel K, Winkler C, Fuith LC, Fuchs D. Tryptophan degradation in patients with gynecological cancer correlates with immune activation. Cancer Lett. 2005;223:323–9.
Schröcksnadel K, Widner B, Bergant A, Neurauter G, Schennach H, Schröcksnadel H, et al. Longitudinal study of tryptophan degradation during and after pregnancy. Life Sci. 2003;72:785–93.
Heyes MP, Saito K, Lackner A, Wiley CA, Achim CL, Markey SP. Sources of the neurotoxin quinolinic acid in the brain of HIV-1-infected patients and retrovirus-infected macaques. FASEB J. 1998;12:881–96.
Huengsberg M, Winer JB, Gompels M, Round R, Ross J, Shahmanesh M. Serum kynurenine-to-tryptophan ratio increases with progressive disease in HIV-infected patients. Clin Chem. 1998;44:858–62.
Look MP, Altfeld M, Kreuzer KA, Riezler R, Stabler SP, Allen RH, et al. Parallel decrease in neurotoxin quinolinic acid and soluble tumor necrosis factor receptor p75 in serum during highly active antiretroviral therapy of HIV type 1 disease. AIDS Res Hum Retrovir. 2000;16:1215–21.
Murr C, Gerlach D, Widner B, Dierich MP, Fuchs D. Neopterin production and tryptophan degradation in humans infected by Streptococcus pyogenes. Med Microbiol Immunol. 2001;189:161–3.
Huang A, Fuchs D, Widner B, Glover C, Henderson DC, Allen-Mersh TG. Serum tryptophan decrease correlates with immune activation and impaired quality of life in colorectal cancer. Br J Cancer. 2002;86:1691–6.
Young SN, Joseph MH, Gauthier S. Studies on kynurenine in human cerebrospinal fluid: lowered levels in epilepsy. J Neural Transm. 1983;58:193–204.
Baig S, Halawa I, Qureshi GA. High performance liquid chromatography as a tool in the definition of abnormalities in monoamine and tryptophan metabolites in cerebrospinal fluid from patients with neurological disorders. Biomed Chromatogr. 1991;5:108–12.
Heyes MP, Saito K, Devinsky O, Nadi NS. Kynurenine pathway metabolites in cerebrospinal fluid and serum in complex partial seizures. Epilepsia. 1994;35:251–7.
Heyes MP, Saito K, Milstien S, Schiff SJ. Quinolinic acid in tumors, hemorrhage and bacterial infections of the central nervous system in children. J Neurol Sci. 1995;133:112–8.
Medana IM, Day NPJ, Salahifar-Sabet H, Stocker R, Smythe G, Bwanaisa L, et al. Metabolites of the kynurenine pathway of tryptophan metabolism in the cerebrospinal fluid of Malawian children with malaria. J Infect Dis. 2003;188:844–9.
Iłzecka J, Kocki T, Stelmasiak Z, Turski WA. Endogenous protectant kynurenic acid in amyotrophic lateral sclerosis. Acta Neurol Scand. 2003;107:412–8.
Theme 3 cognitive and psychological assessment and support. Amyotroph Lateral Scler Frontotemporal Degener. 2014;15(Suppl 1):81–92.
Rejdak K, Bartosik-Psujek H, Dobosz B, Kocki T, Grieb P, Giovannoni G, et al. Decreased level of kynurenic acid in cerebrospinal fluid of relapsing-onset multiple sclerosis patients. Neurosci Lett. 2002;331:63–5.
Orlikov AB, Prakhye IB, Ryzov IV. Kynurenine in blood plasma and DST in patients with endogenous anxiety and endogenous depression. Biol Psychiatry. 1994;36:97–102.
Beal MF, Matson WR, Storey E, Milbury P, Ryan EA, Ogawa T, et al. Kynurenic acid concentrations are reduced in Huntington’s disease cerebral cortex. J Neurol Sci. 1992;108:80–7.
Sardar AM, Bell JE, Reynolds GP. Increased concentrations of the neurotoxin 3-hydroxykynurenine in the frontal cortex of HIV-1-positive patients. J Neurochem. 1995;64:932–5.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Human and Animal Rights Informed Consent
This article does not contain any studies involving human or animal subjects performed by any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Neuropharmacology
Rights and permissions
About this article

Cite this article
Tutakhail, A., Boulet, L., Khabil, S. et al. Neuropathology of Kynurenine Pathway of Tryptophan Metabolism. Curr Pharmacol Rep 6, 8–23 (2020). https://doi.org/10.1007/s40495-019-00208-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40495-019-00208-2