
Abstract
Parental influence in child development in children with autism spectrum disorder is increasingly recognized as important. The primary aim of this systematic mixed method review was to systematically examine the psychological constructs of competence, control, and self-efficacy in the autism literature to assess their relevance for understanding self-perceptions of parents of children with autism. This review illustrates that self-efficacy can be merged into competence and the emergence of the coherence construct. Competence, control, and coherence are vitally important core concepts for understanding parents of children with autism. A unified nomenclature based upon the overarching concept of self-perception would organize the most pivotal constructs much more clearly and reduce redundancies. Specifically, the concept of “parental self-perception” is the most promising candidate for this superordinate concept.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Autism spectrum disorders (ASDs) are a collection of pervasive developmental disorders characterized by difficulties with social interaction, communication, and stereotyped repetitive behaviors. The prevalence of ASD has been rising in recent decades and is approximately 0.6–1 % (Elsabbagh et al. 2012). Previous research has examined the parental challenges related to raising a child with ASD (Hastings and Johnson 2001; Dunn et al. 2001; Hastings et al. 2005; Matson et al. 2013; Larson 2010; Myers et al. 2009; Goin-Kochel et al. 2007). Regardless of the specific ASD diagnosis, child development is heavily influenced by parental emotional well-being, parenting beliefs, and intrapersonal resources (Dawson 2008; Fombonne 2009; Siller and Sigman 2002). Previous research has characterized children with ASD and their parents with respect to these challenges (Shu 2009; Larson 2010; Patten et al. 2013; Gray and Holden 1993; Gray 2002).
Recent research highlights an increasing need for ASD treatment individualization (Strauss et al. 2015). Predictors of treatment individualization have mostly been related to child factors such as age, cognitive functioning, and adaptive and communicative abilities (Eldevik et al. 2010; Reichow 2012). However, treatment individualization can also be based on parental aspects, and therefore, parental factors potentially important for treatment individualization need further and detailed exploration. Previous investigators already have established that parents of children with ASD are particularly vulnerable to experience stress, anxiety, depression, and social isolation (Dunn et al. 2001; Hastings et al. 2005). Parental psychological factors, e.g., stress, coping, depression, anxiety, and anger, appear to have considerable influence on child development for two reasons: (a) Parental well-being affects the child’s well-being, and (b) parents are primary mediators of their child’s development (Dunn et al. 2001; Fombonne 2009; Gray and Holden 1993; Gray 2002; Osborne et al. 2008). Recent work on parents as mediators of treatment response or outcomes concludes that it is critical to determine which parental aspects are most important (Fombonne 2009). Despite the potentially increased level of parental vulnerability, information about how parental characteristics facilitate a positive impact on treatment needs clarification (Strauss et al. 2015).
With regard to ASD treatment, previous research suggests various parental psychological constructs to be of importance to parental treatment preferences for their children (Goin-Kochel and Myers 2005; MacKintosh et al. 2012) For example, parents play a key role in integrating and generalizing ASD treatment strategies into family life (Bernheimer and Weisner 2007). Because each major intervention requires high consistency between the strategies used in school (or daycare) and in the home of the child with ASD, treatment success may depend upon how well the intervention fits with the home environment and family’s beliefs (Bernheimer and Weisner 2007). A final consideration is how the psychological constructs can inform treatment selection for children with ASD.
Based on clinical experiences of the authors, different parental behaviors, attitudes, needs, and expectations relative to treatment were observed. Diverse patterns of behavior that parents displayed related to levels of confidence, degrees of control, and different sources of satisfaction in relation to their role as parents of a child with ASD. Parental attitudes seem interrelated and mostly based on parents’ perceptions of themselves. Therefore, in order to clarify if parental self-perception should be included in treatment individualization strategies, the logical next step is to examine literature about parental self-perception in the ASD literature.
Competence, self-efficacy, and control are three psychological constructs of parental self-perception that could explain differences in parental attitudes and behaviors. Therefore, (a) competence, (b) self-efficacy, and (c) control were selected as the primary focus of this systematic mixed studies review (below referred to as SMSR). Each was selected based on clinical experience and an exploratory literature search that strongly suggested that these constructs might influence parents’ treatment preferences and ASD treatment adherence. The construct of parental competence is defined as an aspect of parenting behaviors, skills, and strategies that promote positive child development (Johnston and Mash 1989; Jones 2005). The construct of self-efficacy is defined as one’s capabilities to organize and execute specific courses of action adequately (Bandura 1997; Bandura et al. 2001). Parental self-efficacy is linked to adjustment of the parenting role, parental well-being, parental depression, social support, attachment, and temperamental qualities of the child (Bandura 1997). Competence and self-efficacy are closely related as both cover parental proficiency. One key difference between the two constructs is framed by who holds the perception (Montigny et al. 2005). Where self-efficacy refers to the parents’ own perception of their capabilities, competence entails the judgments that others hold on parents’ abilities (Montigny et al. 2005). The construct of control is defined further by internal or external locus of control (Rotter 1975). As two opposites, high internal control indicates a strong belief that circumstances are related to one’s own actions, while external control indicates a strong belief that circumstances are not or are on only a limited basis related to one’s own actions (Rotter 1966). Therefore, control indicates a person’s belief in either high or low control over her/his life (Campis et al. 1986). The clinical significance of these psychological constructs is based on their potential to clinically assess parental comprehension of treatment in relation to their child with ASD.
Despite the extensive literature on competence, control, and self-efficacy in ASD, assessment of these factors relevance specifically for understanding parental self-perception has been lacking. Hence, the primary aim of this SMSR is to systematically examine competence, self-efficacy, and control in the ASD literature to assess their relevance for understanding self-perceptions of parents of children with ASD and to understand the relationship between these constructs and to determine if a more unified construct could be developed that incorporates the core elements of each, eliminates overlap, and includes other relevant constructs that emerge. A secondary aim is to understand what specific instruments have been used for measuring competence, self-efficacy, and control in ASD, and the relative frequency of use of these instruments. This aim is important as it provides an overview of availability and application of self-report instruments.
Method
This SMSR was conducted by searching PubMed, PsycINFO, and Embase databases for articles concerning the psychological constructs competence, self-efficacy, and locus of control as well as associated parental self-report measures. Quantitative, qualitative, and mixed method articles specific to ASD were included to gain a multidimensional and comprehensive understanding of all extant literature (Miles et al. 2014; Pluye and Nha Hong 2014). In this review, treatment is used as a general term including intervention, therapy, teaching, or learning without restriction by treatment method or philosophy of treatment.
Identification of Relevant Literature
The search was performed in collaboration with a research librarian between November 2010 and February 2011 (PsycINFO 11.09.10, Embase 11.19.10, and PubMed 02.01.11) and then updated in May 2013 and April 2014 (all databases 05.23.13 and 04.01.2014). There were no constraints upon year of publication. The search strategy (see Table 1) consisted of three separate blocks, and the first consisted of ASD-specific keywords. The second block contained keywords related to the three psychological constructs central to this SMSR (“competence”, “self-efficacy”, and “locus of control”) as well as “stress” and “coping” to ensure that key-related literature was detected. The third block consisted of parent-related keywords such as “values”, “beliefs”, “culture”, “involvement”, “burden”, “attitude”, and “quality of life.” As with stress and coping, these terms were included in the search to help capture valuable information about parental psychological factors that could relate plausibly to competence, self-efficacy, and locus of control. Keywords within each block were combined with “OR,” and the subsequent total search between the blocks was combined with “AND,” to obtain the overall joint result of the three search blocks.
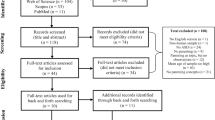
The first stage of article evaluation and selection was conducted using abstracts alone. After deleting duplicates, articles were included and excluded based on the criteria presented in Fig. 1. The second stage of inclusion and exclusion was conducted using the “Introduction” and “Methods” sections. Articles concerning parents, family, and psychological themes were included for a full-text examination and analysis. The third stage of evaluation and selection was conducted on the entire article. All articles containing any reference to parental self-evaluation was included in this study. Articles containing only psychological aspects not related to self-evaluation were excluded. Articles were also classified as primarily quantitative or primarily qualitative in methodology. The first stage was conducted by the first author (KKF) alone, while the second and third stages were also cross-checked by a second reviewer (MBL). During the cross-checking process, the decision was made to include articles that used the term “family” as well as “parents.” Although this was unconstrained, it led to the inclusion of several articles that contained parent-oriented self-report measures or concerned “control” or “coherence” as they related to parents and to the specific aim of this SMSR.

Inclusion and exclusion criteria stages 1–3 for assessment of relevant literature
Inclusion and Exclusion of Articles
Articles included in this review cover all diagnostic categories related to autism (ASD, autism, childhood autism, autistic disorder, Asperger’s syndrome or disorder, PDD-NOS, autism condition, etc.). Furthermore, this review did not include information about the presence of comorbidity in the included articles.
Based on the purpose of examining psychological constructs to assess their relevance in relation to parental self-perception, articles were included if they mentioned and referred to any of the selected constructs; competence, self-efficacy, locus of control, “sense of coherence,” or “self-esteem” (Fig. 1). Since only a few of the qualitative articles directly concerned competence, or self-efficacy, locus of control, a thematic analysis was conducted to identify the most relevant themes to use as a basis for including qualitative articles (Boyatzis 1998). Themes used for including qualitative articles are listed in Table 2. Articles that did not contain aspects of ASD and/or parents of children with ASD, and also articles that referred only to peripheral concepts such as stress, coping, depression, anxiety, anger, well-being, and neuroticism were excluded because these concepts are not the focus of this SMSR. Also excluded were articles that focused primarily upon any of the following topics: family systems theory, caregiver burden, marital relationships, ASD treatment and outcomes, parenting, and parental concordance or collaboration and/or relationship with professionals, relationship between parents and staff/professional, staff/professional-perspectives alone, and treatment outcomes.
Quality Appraisal
The articles were assessed using the Mixed Methods Appraisal Tool (MMAT) (Pluye et al. 2011) which is a tool in SMSR to assess the quality of studies eligible for inclusion. Quality appraisal was conducted in collaboration between first author (KKF), last author (MB), and second author (MBL). The quality assessment for both the qualitative and quantitative articles was first completed independently and subsequently compared with the second reviewer. Due to the priorities and the explorative nature of this review, no articles were excluded on the basis of the quality appraisal, as they all were significant in relation to the aim of the review (Pope et al. 2007). The quality appraisal of the included studies also makes it possible to conduct a sensitivity analysis between all included studies and high-quality studies if relevant.
Method of Analysis
The analytic approach leveraged meta-integration of the convergent qualitative (QUAL) synthesis type (Frantzen and Fetters 2015). Results from all included studies (both quantitative and qualitative and mixed method) were transformed into qualitative findings in order to present relevant themes, concepts, and patterns (Pluye and Nha Hong 2014). The thematic analysis was a hybrid deductive-inductive approach (Boyatzis 1998, pp. 51) in which the predefined themes from the quantitative articles through mindful comparison, the process of contemplating the evolving outcomes during the analysis from both data sources, connected the quantitative and qualitative data (Fig. 2).

Convergent QUAL synthesis
Analysis of the Psychological Constructs
Analysis of the psychological constructs rigorously followed the methodological procedures illustrated in Fig. 2 (Frantzen and Fetters 2015). The thematic analysis identified not only all the constructs of relevance but also the factors influencing the constructs. The thematic analysis was initially conducted deductively and focused on the framework from the quantitative articles. Subsequently, this was followed by an inductive data-driven analysis to determine whether any additional constructs existed. This analysis was based on all the included articles.
Analysis of the Key Self-Report Measures
The analysis of the actual self-report measures was conducted as an a priori research-driven analysis (deductive) in which the initially identified psychological constructs formed the basis for the analysis of the articles (Boyatzis 1998). The analysis of the self-report measures was performed by first establishing an overview of what specific measure(s) a given study applied, as presented in Table 3. To find the most useful measurement for each psychological construct, the analysis focused on determining whether the same measures were used in other included studies. This analysis was based on the articles using self-report measures.
Results
Search Results
The search strategy identified 911 articles published from 1972 to 2014, as presented in Fig. 1. The first stage of inclusion and exclusion identified 389 articles. In the second stage, the number was reduced to 219 articles, and of these, 170 were excluded by the third stage. This resulted in a final set of 53 included articles. Of the 911 articles, 531 were identified in the first search from 2010 to 2011, while the updated searches in May 2013 and April 2014 added 275 and 105 additional articles. Of the 53 included articles, 29 were from the 2010/2011 search, while the updated searches in May 2013 and April 2014 included 14 and 10 additional articles, respectively.
The first author (KKF) and the second author (MBL) independently assessed articles for inclusion and exclusion. Of 11 eligible articles, two were included and nine were excluded on the basis of no focus on the psychological constructs of interest in this SMSR. The quality appraisal procedure revealed minor differences in the quality scoring of the articles.
Psychological Constructs
Thematic analysis of the psychological constructs of competence, self-efficacy, and control revealed three important outcomes.
First, three additional constructs—“coherence,” “self,” and “self-esteem”—were identified. The construct of coherence was found to be important in several articles (Kaniel and Siman-Tov 2011; Siman-Tov and Kaniel 2011; Sivberg 2002a; Sivberg 2002b; Manor-Binyamini 2011; Pozo et al. 2014; Pisula and Kossakowska 2010; Olsson and Hwang 2008) and therefore included as a separate construct. Coherence covers a person’s confidence in perceiving one’s internal and external environments as predictable, comprehensible, manageable, and meaningful (Antonovsky 1979). A second psychological construct not initially part of the search strategy was the concept of self. The sense of self seems to be affected, changed, or altered partly as a consequence of having a child with ASD (Altiere and von Kluge 2009; Cashin 2004; Shu et al. 2006). Since the construct of self is already included as part of the overall goal of this SMSR (parental self-perception), it was not handled as a separate construct but served as an overall construct. The psychological construct self-esteem was not included in the search because there is overlap with the construct of competence and only a limited number of articles were about self-esteem.
Second, self-efficacy, like self-esteem, is closely related to competence and therefore insufficient as an independent construct of its own. This judgment was based partially on the fact that competence and self-efficacy are very closely related concepts.
Third, thematic analysis of the psychological constructs reveals that competence, control, and coherence were influenced by several important factors related to being parents of children with ASD. Below, the results of the detailed thematic analysis of related factors are presented separately under each construct.
Competence
Regarding competence, detailed analysis of the included articles reveals several interesting trends (Table 4). In the quantitative articles, competence is a relatively stable psychological construct, especially at higher levels of competence (Keen et al. 2007; Keen et al. 2009; Sofronoff et al. 2011; Solish and Perry 2008). The level of competence affects the parents’ benefit from intervention with a tendency of the self-efficacy dimension being improved, while the satisfaction dimension remains unaffected (Dunn et al. 2012; Hesse et al. 2013; Reitzel et al. 2013; Estes et al. 2014; Raj and Salagame 2010; Weiss et al. 2012).
Disagreement about if and how intervention influences competence is found as some studies show improved competence, while others show no improvement (Dunn et al. 2012; Reitzel et al. 2013; Estes et al. 2014; Raj and Salagame 2010; Weiss et al. 2012). Duration of intervention and number of interventions may explain these differences (Estes et al. 2014). Moreover, improvements in parental competence may affect not only the child with ASD but also his/her non-affected siblings (Hesse et al. 2013; Meirsschaut et al. 2010). There is considerable disagreement among the articles as to whether competence is related to either type of disorder or the presence/absence of disorder (Rodrigue et al. 1992; Donenberg and Baker 1993; Al-Kandari and Al-Qashan 2010). Furthermore, competence functions differently for mothers and fathers. That is, competence acts as a mediating factor for mothers and as a moderating, protective factor for fathers (Sofronoff and Farbotko 2002; Hastings and Brown 2002). In relation to attachment, there is a correlation between parental attachment to child and parental sense of competence, while there is no correlation between parental perception of child attachment to parents and sense of competence (Goodman and Glenwick 2012; Rutgers et al. 2007). Time also seems to be a factor for parents gaining confidence (Dunn et al. 2012; Raj and Salagame 2010; Hodgetts et al. 2013). Time here refers to several aspects: time to feel less distressed and more confident (Dunn et al. 2012), time to practice strategies related to ASD intervention (Sofronoff et al. 2011), time to process child progress (Dunn et al. 2012), time to regain physical energy to engage in parenting again (Giallo et al. 2013), time to perceive important contextual factors (Dunn et al. 2012), and time to cope with their own reactions to child behavior (Dunn et al. 2012). An important note is that the terminology from the original articles (confidence) is applied here. Even though the definition of confidence and competence is different, they represent some of the same aspects. Therefore, in this review, confidence is organized alongside competence (Pakenham et al. 2004; Hodgetts et al. 2013).
Competence is associated with a wide variety of other variables such as stress (Pakenham et al. 2004; Lerner et al. 2012; Kuhn and Carter 2006; Meirsschaut et al. 2010; Hastings and Brown 2002; Rutgers et al. 2007; Keen et al. 2009; Giallo et al. 2013; Hesse et al. 2013; Reitzel et al. 2013; Estes et al. 2014; Weiss et al. 2013a, b; Weiss et al. 2012; Dunn et al. 2012; Goodman and Glenwick 2012; Malow et al. 2014), depression (Giallo et al. 2013; Kuhn and Carter 2006; Weiss et al. 2012; Lerner et al. 2012; Benson and Kersh 2011; Malow et al. 2014), guilt (Kuhn and Carter 2006), agency (Kuhn and Carter 2006), maternal cognition (Meirsschaut et al. 2010; Kuhn and Carter 2006; Weiss et al. 2013a, b; Bourke-Taylor et al. 2012; Raj and Salagame 2010), severity of disorder (Hesse et al. 2013; Hastings and Symes 2002), self-esteem (Werner and Shulman 2013; Higgins et al. 2005), fatigue (Giallo et al. 2013; Malow et al. 2014), treatment support (Bourke-Taylor et al. 2012), social support (Dunn et al. 2012; Giallo et al. 2013; Hastings and Brown 2002; Weiss et al. 2012; Werner and Shulman 2013), family hardiness (Weiss et al. 2013a, b), intervention (Keen et al. 2009; Sofronoff and Farbotko 2002; Estes et al. 2014; Solish and Perry 2008; Hodgetts et al. 2013), sleep education (Malow et al. 2014; Giallo et al. 2013), parenting style (Hesse et al. 2013; Rutgers et al. 2007), ASD meaning (Pakenham et al. 2004; Werner and Shulman 2013), treatment involvement (Solish and Perry 2008; Raj and Salagame 2010; Hesse et al. 2013), quality of marriage (Higgins et al. 2005; Benson and Kersh 2011), acceptance and empowerment (Bourke-Taylor et al. 2012; Weiss et al. 2012; Weiss et al. 2013a, b; Werner and Shulman 2013; Malow et al. 2014; Hodgetts et al. 2013), consonance between parent and child views of social functioning (Lerner et al. 2012), and negative life events (Estes et al. 2014; Weiss et al. 2012).
The analysis of the qualitative articles focuses on different aspects than the quantitative articles. The qualitative studies conclude that competence is directly influenced by the following six different factors. Competence is a question of time and timing (Meirsschaut et al. 2010; Larson 2010; Cashin 2004; Myers et al. 2009; Shu et al. 2006; Gray 2001). It implies that not only must the parents give the right amount of assistance in a given situation but they must also give the assistance at exactly the moment when it is needed.
Knowledge is described as related to confidence (Pakenham et al. 2004; Hodgetts et al. 2013; King et al. 2006; Cashin 2004; Altiere and von Kluge 2009). ASD-specific knowledge emerges as a key element for parental feeling of competence. In the process of exploring how they could improve their child’s situation, parents become effective advocates and gain much knowledge. As knowledge increases, so does their confidence (Altiere and von Kluge 2009). Parental knowledge and beliefs about ASD based on their experiences alter their self-identities as caregivers (Hines et al. 2012; Shu et al. 2006).
A clear sense of values and priorities not only improves the feeling of competence (King et al. 2006; Shu et al. 2006) but might prevent parents from “second-guessing” themselves and hence having feelings of guilt (Cashin 2004). Competence is also linked to the perceived ability to find the best treatment for their specific child—not necessarily knowing the presumptive “right” treatment in general (Cashin 2004; Altiere and von Kluge 2009; Myers et al. 2009). Competence also appears to be related to being able to differentiate one’s parenting cognitions relevant to the situation and thereby being able to adapt using the most appropriate skills at a given moment (Meirsschaut et al. 2010). Parents’ feelings of competence are influenced by the misinformed judgment they sometimes meet from others (Cashin 2004; Meirsschaut et al. 2010). This is especially the case if the child with ASD behaves in an antisocial or maladapted way in a social situation among strangers that do not know anything about the disorder. Judgment from strangers thus impacts parental feelings of competence (Cashin 2004).
Control
Similar to the stability of measures found for competence, the quantitative articles generally indicate that parental feelings of control are fairly stable across time (Table 5) (Lloyd and Hastings 2009). Similar to the findings for competence, there are questions about how control relates to different disorders as well as the importance of either presence or absence of a childhood disorder (Hamlyn-Wright et al. 2007; DeVellis 1985). Both control and ASD severity are found to affect parental beliefs about how much they could influence their child’s recovery (DeVellis 1985). As with competence, the studies also concur that control correlates with numerous other variables such as maternal perception (Cappe et al. 2011), maternal distress (Lloyd and Hastings 2009), depression (Hamlyn-Wright et al. 2007), anxiety (Hamlyn-Wright et al. 2007), stress (Hamlyn-Wright et al. 2007; Lloyd and Hastings 2009; Siman-Tov and Kaniel 2011; Kaniel and Siman-Tov 2011; Cappe et al. 2011), coping (Siman-Tov and Kaniel 2011; Kaniel and Siman-Tov 2011; Cappe et al. 2011), well-being (Lloyd and Hastings 2009), family adjustment (Henderson and Vandenberg 1992), parental perception of effectiveness in parenting role (Lloyd and Hastings 2009), and outcome and experiences (Siman-Tov and Kaniel 2011; Cappe et al. 2011).
The analysis of the qualitative articles likewise indicates that sense of control is influenced by five factors. Parents’ ability to manage their own time and timetable (Shu et al. 2006; Cashin 2004; Gray 2001), parents’ timing in relation to intervention (Larson 2010), parents’ experience of judgment from others, and their lack of control over the environment are all found as key factors influencing control (Cashin 2004). Another trend is that parents’ are attentive about their ability to actively change their focus and worldviews and try focusing on positive rather than negative factors (Pakenham et al. 2004; King et al. 2006; Altiere and von Kluge 2009; Shu et al. 2006; Foster et al. 2013).
Insight and worldviews are found as impacting control. Lastly, both social support from the parent’s family and social network as well as social services are another important component influencing parents’ feelings of control (Meirsschaut et al. 2010; Larson 2010; Altiere and von Kluge 2009; Myers et al. 2009).
Coherence
The pool of quantitative articles contains some consistent as well as conflicting indications of gender differences. In some studies (Kaniel and Siman-Tov 2011; Sivberg 2002b), fathers are found to have a higher sense of coherence than mothers though another study reports no differences (Pisula and Kossakowska 2010) (Table 6). A further gender difference is that while coherence is linked to quality of marriage for mothers, it is linked to mental health for fathers. Existing research illustrates an association between the severity of parents’ life stress and their desire to find meaning in their child’s ASD (Sivberg 2002a; Pozo et al. 2014). The parents’ “expertise” about their own life emerges as an important factor in sense of coherence, primarily because they understand their current life situation having a child with ASD through the filter of their prior experiences. Parents of children with ASD showed lower level of meaningfulness and manageability compared to parents of typically developing children, suggesting that they were experiencing a sense of helplessness influenced by the level of behavioral problems the child with ASD displayed (Pozo et al. 2014; Pisula and Kossakowska 2010; Manor-Binyamini 2011) and parents had a weaker central coherence and a stronger tendency to detail-focused processing of information (Pisula and Kossakowska 2010). Parents with a higher level of sense of coherence perceived stressors as comprehensible, controllable, predictable, and manageable (Manor-Binyamini 2011; Pozo et al. 2014). Coherence is linked to mental health (Siman-Tov and Kaniel 2011; Kaniel and Siman-Tov 2011), well-being (Siman-Tov and Kaniel 2011; Olsson and Hwang 2008; Pozo et al. 2014), adjustment (Siman-Tov and Kaniel 2011), stress (Sivberg 2002a; Pisula and Kossakowska 2010; Pozo et al. 2014; Kaniel and Siman-Tov 2011), psychological protective factors (Olsson and Hwang 2008), contextual risk factors (Olsson and Hwang 2008), social support (Pisula and Kossakowska 2010; Kaniel and Siman-Tov 2011), self-control (Pisula and Kossakowska 2010), and quality of marriage (Kaniel and Siman-Tov 2011).
In the qualitative articles, coherence is described as being under the influence of time, because parents seem to scan past situations to create an overview and understanding (Larson 2010; Cashin 2004; Altiere and von Kluge 2009; Shu et al. 2006). Coherence is affected by hope and frustration (King et al. 2006; Cashin 2004; Altiere and von Kluge 2009) and can lead to changes in world views, values, priorities, and the need to “have things in place” (Pakenham et al. 2004; King et al. 2006; Cashin 2004; Altiere and von Kluge 2009; Shu et al. 2006). As a consequence, parents’ experience changes in their relationship both to their partner (Cashin 2004; Shu et al. 2006), their near and extended relatives (Altiere and von Kluge 2009; Larson 2010), and their broader social network (Altiere and von Kluge 2009; Shu et al. 2006). Finally, coherence is tightly connected to the needs of parents’ for a causal explanation and clear understanding of the ASD diagnosis (Pakenham et al. 2004; Meirsschaut et al. 2010; Hodgetts et al. 2013; Altiere and von Kluge 2009; Gray 2001; Hines et al. 2012; Foster et al. 2013) and some parents use the ability of objectifying the disability as something distinct (Hines et al. 2012).
Self-Report Measures
Table 3 lists the pool of quantitative articles concerning the self-report measures that appeared to be important with respect to the aim for this SMSR. None of the qualitative articles mentioned any self-report measures. Within the construct competence (n = 12), all studies used the Parenting Sense of Competence scale, while the construct control (n = 7) used 6 different scales and self-efficacy (n = 17) used 10 different scales. Two additional psychological constructs also emerged: Coherence (n = 8), using three different versions of the Antonovsky Sense of Coherence scale, and Self-esteem (n = 2) both using the Rosenberg self-esteem scale.
Within the construct competence, the articles apparently had a high degree of agreement as to the preferred measurement, insofar as all included articles used the Parenting Sense of Competence scale (Johnston and Mash 1989). Conversely, for locus of control and self-efficacy, a variety of different types of scales were represented. With regard to locus of control, closer evaluation of the different measures in Table 3 reveals that only one of the measures used was developed specifically to elucidate parents’ perception of locus of control in their parental role. Consequently, the Parental Locus of Control scale (Campis et al. 1986) emerges as the most appropriate instrument for measuring parental locus of control. The search revealed no consistent approach to measuring self-efficacy. However, the Parenting Sense of Competence scale is a superordinate label that includes both a dimension of self-efficacy and of satisfaction (Johnston and Mash 1989), and therefore, this scale is deemed suitable as a measurement covering the construct of self-efficacy. In addition to the psychological constructs intentionally included in the search, the extended search strategy revealed two additional constructs that seemed potentially important to parental treatment preferences: sense of coherence and self-esteem. Looking into the scales used to measure sense of coherence, the term is very clearly defined by Antonovsky, and there is an identical concept underlying the different versions of the scale. The Sense of Coherence scale is available in a short 13-item version measuring the same aspects of coherence as the longer 29-item version, so the 13-item version was deemed appropriate for use. The Rosenberg Self-Esteem Scale (Rosenberg 1965; Rosenberg 1979) measures general self-esteem (as opposed to self-esteem specific to parenting) making it a poor fit for research on parental self-esteem and competence. The Parenting Sense of Competence scale and the Parental Locus of Control scale emerge as the best fit for measuring self-esteem in relation to the parental role.
In summary, the examination of the self-report scales used in the included articles shows that the primary scales relevant to review parents’ psychological constructs that may affect their treatment preferences are Parenting Sense of Competence (PSOC) (Johnston and Mash 1989), Parental Locus of Control (PLOC) (Campis et al. 1986), and Sense of Coherence (SOC) (Antonovsky 1993). An important outcome of the SMSR is dropping self-efficacy and self-esteem as measures, and substituting a more robust measure, Sense of Coherence. Table 7 illustrates that PSOC with 42 % of the articles is the most frequently used self-report measure covering competence, self-efficacy, and self-esteem.
Discussion
This SMSR has provided new key information about the psychological constructs of competence, control, and coherence. The new information relates to the constructs importance for parental perceptions and to the extent of overlap between the three constructs. Some of these findings relate to commonalities across the constructs, while other findings are specific for one of the constructs or specifically related to parents of children with ASD. The integration of data in this SMSR is an expansion where the various results from the quantitative, qualitative, and mixed methods papers are addressing different aspects of the three constructs and expanding understanding of these constructs (Fetters et al. 2013).
General Findings
Based on an extensive thematic analysis and conceptual mapping of the included articles, the most prominent finding is that the construct of competence overlapped the constructs of self-efficacy and self-esteem to such an extent that—at least in this context—they seem functionally the same construct. Another finding is the discovery of coherence, which was not initially included in the search strategy, emerged as a potential influence upon parental treatment preferences. While it was relatively straightforward to identify the key self-report measures of these constructs, these findings prompt further consideration about the parents’ self-reflections.
The papers included in this review revealed that the scales and constructs used to describe parental psychological characteristics are highly diverse and includes several concepts and designations that are interconnected, comparable, and overlapping. It was not possible to designate any single construct as being more unique than other constructs, and therefore, they are equally essential. Not only did concept mapping indicate that the three constructs overlap (see Fig. 3), but different names and terminologies are sometimes used to refer to psychological constructs containing the same elements. This suggests a need for a systematic uniform nomenclature about parents’ psychological constructs. However, the most important question now becomes: “Should researchers distinguish between otherwise similar constructs?”

Concept mapping of the psychological constructs competence, control, and coherence. Figure 3 illustrates the distribution of themes in either specific themes for each psychological construct or mutual themes relevant for all the three psychological constructs. As the number of mutual themes exceeds a possible visual presentation in the figure, these themes are presented as linked findings and in a box. The highlighted words are headlines for some of the themes that are closely related. The bulleted items are the actual themes mentioned in the included articles. These themes were identified through the thematic analysis described in the method section of this paper
One the one hand, it can be argued that competence control and coherence are merely facets of a superordinate concept such as parental self-perception. This conception would seem more comprehensive because it could furthermore include several additional constructs such as self-efficacy, self-esteem, empowerment, and resilience, thereby subsuming all conceivable aspects of parental self-evaluations, self-reflections, and self-assessment. Because use of the self-perception construct could embrace all relevant psychological constructs related to parental belief and behavior, its adoption may reduce confusion, clarify similarities and differences between constructs, and increase comparability. On the other hand, the downside of merging different psychological constructs into one single concept like parental self-perception would be that the distinctive characteristics and specificities in the terminology of the specific constructs potentially could vanish, and thus important differences of nuance could be lost. However, the current use of terminologies is questionable as the evidence established in this review indicates a substantial overlap between the constructs. Maintaining a division of the terminology in the existing terms requires not only a clear demarcation of the constructs but also a more focused and systematic application of the terminology to avoid any ambiguity. Therefore, clear and unambiguous definitions clarifying similarities and differences between the constructs are needed to maintain the current differentiation in terminology.
A systematic review published in 2011 by Pritchett et al. identified 107 self-report measures describing different aspects of family functioning (Pritchett et al. 2011), which were divided into six domains based on specific aspects of family functioning being measured. This has important implications for determining when self-report measures are most suitable and emphasizes the need for a holistic measurement approach that incorporates data from multiple informants. Thus, the present review is in agreement with Pritchett et al. (2011) conclusion that the psychological constructs targeting parents need to be simplified through the use of some superordinate concept (e.g., parental self-perception) that incorporates all aspects of parental beliefs and self-perception. Future research on these constructs should emphasize the analysis of content, application, and understanding in order to clearly address the boundaries and overlaps across these constructs.
Autism-Specific Findings
The results in the present study enable certain firm conclusions about competence, control, and coherence in parents of children with ASD. It is important to measure all three constructs insofar as they are each associated with better parental functioning. Moreover, all three constructs appear to be relatively stable in the short term (Keen et al. 2007; Keen et al. 2009; Sofronoff et al. 2011; Solish and Perry 2008; Lloyd and Hastings 2009). However, their long-term stability remains unclear due to the lack of longitudinal evidence. Nonetheless, parents’ baseline levels of competence, control, and coherence are important reference points for understanding their stressful situation. A review by Bekhet et al. (2012) had the aim to find indicators of resilience in parents of children with ASD and concluded that competence, control, and coherence act as protective factors and therefore promote resilience (Bekhet et al. 2012). Thus, a review that does not have competence, control, and coherence as objective or search terms revealed that these constructs are important for parents of children with ASD.
The results also demonstrate that the constructs are influenced by several environmental factors such as presence of child’s disorder, type and severity of disorder, and child behavior and functioning (Rodrigue et al. 1992; Donenberg and Baker 1993; Al-Kandari and Al-Qashan 2010; Sivberg 2002a; Pozo et al. 2014; DeVellis 1985; Hamlyn-Wright et al. 2007). Additionally, higher levels of competence are associated with maternal empowerment and that the benefits could affect not only child with ASD but also unaffected siblings (Hesse et al. 2013; Meirsschaut et al. 2010). Attachment also plays an important but complex role (Goodman and Glenwick 2012; Rutgers et al. 2007). While parental competence is associated with parents’ attachment to their children, it is seemingly not associated with children’s attachment to their parents. This suggests that parents are aware that their child’s disorder influences the child’s ability to attach and that many parents can adjust their reciprocity expectations based upon their child’s limitations. This may be undergirded by the fact that some parents objectify (i.e., separate the ASD symptoms from the child) with the goal of achieving coherence (Hines et al. 2012). Parents of children with ASD also display an overall ability to differentiate and distinguish between their views on parental skills and the difficulties and challenges caused by having a child with ASD (Meirsschaut et al. 2010).
This SMSR also elucidates that knowledge, priorities, values, beliefs, and worldviews are important factors in relation to competence, control, and coherence (Pakenham et al. 2004; Hodgetts et al. 2013; King et al. 2006; Cashin 2004; Myers et al. 2009: Altiere and von Kluge 2009; Shu et al. 2006; Foster et al. 2013). Knowledge is related to competence (confidence), and clear values and priorities are important (Altiere and von Kluge 2009). The control construct is intimately linked to insight and worldview (Pakenham et al. 2004; King et al. 2006; Altiere and von Kluge 2009; Shu et al. 2006; Foster et al. 2013), and the coherence is related to worldview, values, priorities, and explanation and understanding the diagnosis (Pakenham et al. 2004; King et al. 2006; Cashin 2004; Altiere and von Kluge 2009; Gray 2001). Parents function as their own experience-based expert (Pisula and Kossakowska 2010), suggesting that parental competence, control, and coherence evolve through an iterative, self-reinforcing process. While some parents might experience a sense of empowerment, others experience a far-reaching vulnerability perhaps after experiencing others as judgmental of their parenting skills (Meirsschaut et al. 2010; Cashin 2004). This probably influences not only their competence but also their sense of control. Parental values, beliefs, and worldviews particularly focus on aspects in their daily life. Regarding treatment parental values, beliefs and worldviews influence their attitudes toward treatment content and treatment priorities. Values, beliefs, and worldviews also affect’ parents’ awareness about their life situation and prompt a greater attention to possibilities rather than limitations and on positive experiences rather than negative experiences.
Another prominent finding revealed by the thematic analysis is the extent to which parenting demands restrict parents’ sense of personal freedom to control their schedules (Hodgetts et al. 2013; Cashin 2004; Gray 2001). Parents’ feelings and views on chronological time and timing are largely governed by their efforts made to keep the child functioning at the day-to-day level (Larson 2010; Gray 2001). They must vigilantly oversee both social and physical environments, scan all situations to understand the big picture, determine the best amount of assistance only when necessary, accept limitations on controlling their own personal schedule, and cope with reduced socializing and even isolation (Meirsschaut et al. 2010; Larson 2010; Cashin 2004; Myers et al. 2009; Shu et al. 2006; Gray 2001).
One rather unexpected finding is the very limited information available on how the three constructs relate to treatment preferences. Treatment preferences may be related to competence, in the sense that parents are aware of differences between treatments (Cashin 2004; Altiere and von Kluge 2009; Myers et al. 2009). Additionally, the link between the three constructs and support is only presented briefly in this SMSR. While treatment preferences are related to competence (Dunn et al. 2012; Hesse et al. 2013; Reitzel et al. 2013; Estes et al. 2014; Raj and Salagame 2010; Weiss et al. 2012), support tends to be described as being related to control (Meirsschaut et al. 2010; Larson 2010; Altiere and von Kluge 2009; Myers et al. 2009), perhaps because the amount of available support is frequently insufficient in time and quality to be meaningful to parents.
A final implication of the present review is that there are differences by parental gender in two of the three constructs. Competence and coherence have different meanings and effects for mothers and fathers of children with ASD. Competence can be perceived as either a mediator for mothers or a moderator for fathers (Hastings and Brown 2002; Sofronoff and Farbotko 2002), while coherence is related to either quality of marriage for mothers or mental health for fathers (Kaniel and Siman-Tov 2011; Sivberg 2002a; Pisula and Kossakowska 2010). Intervention might improve competence and coherence in mothers, while it has no or limited effect in fathers (Dunn et al. 2012; Hesse et al. 2013; Reitzel et al. 2013; Estes et al. 2014; Raj and Salagame 2010; Weiss et al. 2012; Kaniel and Siman-Tov 2011; Sivberg 2002a; Pisula and Kossakowska 2010). Thus, competence and coherence can only be understood and interpreted within the context of parental gender. These gender differences also play a role in how these constructs impact parenting behavior, motivations, and treatment preferences.
In summary the systematic examination of the three psychological constructs examined in this review suggests that parents’ psychological resources can have a substantial impact on major decisions parents makes about their child with ASD. This review contributes new insight for ASD professionals about attentiveness to competence, control and coherence beyond the usual focus on resources, stress, coping, anger, anxiety, and depression. Future research needs to clarify if there is a relation between competence, control, and coherence that can be correlated with specific parental treatment preferences. Furthermore, research is needed on whether the three psychological constructs exhibit unique properties or a high level of concordance.
Limitations
While this SMSR reveals important patterns and trends for further exploration, the results must be interpreted cautiously, given the types of articles included within each subcategory. The set of reviewed articles is highly heterogeneous with respect to the number of different psychological constructs and terminologies, and the boundaries assumed between them. Less restrictive search criteria and/or in combination with a chain search (in the references used in the included articles) could possibly have increased the number of included articles, and an adequate quantitative SMSR could potentially have been conducted. A literature search on the three constructs in a general population of parents would have allowed a comparative analysis highlighting similarities and differences to parents of children with ASD. Utilizing a greater number of data analysts may have reduced the risk of subjective judgment though this is unlikely to undermine the overall validity of our results. As for any under-researched topic, publication bias could affect the findings. Finally, this SMSR only included a very limited number of articles using mixed method.
Conclusion
In conclusion, competence, control, and coherence are core concepts for understanding parents of children with ASD. These three constructs underlie several key aspects of these parents’ lives. A unified, more elegant conception and nomenclature based upon the overarching concept of self-perception could organize these pivotal constructs more clearly and reduce redundancies in psychological terms, labels, and constructs. The concept of “parental self-perception” is the most promising candidate for this superordinate concept. Future studies should aim to confirm these associations and reduce their complexity by elucidating the unique and common aspects of competence, control, and coherence and related constructs.
References
Al-Kandari, H. Y., & Al-Qashan, H. (2010). Maternal self-efficacy of mothers of children with intellectual developmental disabilities, down syndrome, and autism in Kuwait. Child and Adolescent Social Work Journal, 27(1), 21–39.
Altiere, M. J., & von Kluge, S. (2009). Searching for acceptance: challenges encountered while raising a child with autism. Journal of Intellectual and Developmental Disability, 34(2), 142–152.
Antonovsky, A. (1979). Health, stress and coping (p. 1979). San Francisco: Jossey-Bass.
Antonovsky, A. (1987). Unraveling the mystery of health: how people manage stress and stay well. San Francisco: Jossey-Bass.
Antonovsky, A. (1991). Hälsans mysterium [Unraveling the mystery of health] (Vol. 1). Stockholm: Natur och Kultur.
Antonovsky, A. (1993). The structure and properties of the sense of coherence scale. Social Science & Medicine (1982), 36(6), 725–733.
Bandura A. (1997). Self-efficacy: the exercise of control. New York: W.H. Freeman.
Bandura, A., Barbaranelli, C., Caprara, G. V., & Pastorelli, C. (2001). Self-efficacy beliefs as shapers of children’s aspirations and career trajectories. Child Development, 72(1), 187–206.
Bekhet, A. K., Johnson, N. L., & Zauszniewski, J. A. (2012). Resilience in family members of persons with autism spectrum disorder: a review of the literature. Issues in Mental Health Nursing, 33(10), 650–656.
Benson, P. R., & Kersh, J. (2011). Marital quality and psychological adjustment among mothers of children with ASD: cross-sectional and longitudinal relationships. Journal of Autism and Developmental Disorders, 41(12), 1675–1685.
Bernheimer, L. P., & Weisner, T. S. (2007). “Let me just tell you what I do all day…”: the family story at the center of intervention research and practice. Infants and Young Children, 20(3), 192–201.
Bourke-Taylor, H., Pallant, J. F., Law, M., & Howie, L. (2012). Predicting mental health among mothers of school-aged children with developmental disabilities: the relative contribution of child, maternal and environmental factors. Research in Developmental Disabilities, 33(6), 1732–1740.
Boyatzis, R. E. (1998). Transforming qualitative information: thematic analysis and code development. London: Sage.
Campis, L. K., Lyman, R. D., & Prentice-Dunn, S. (1986). The parental locus of control scale: development and validation. Journal of Clinical Child Psychology, 15(3), 260–267.
Cappe, E., Wolff, M., Bobet, R., & Adrien, J. L. (2011). Quality of life: a key variable to consider in the evaluation of adjustment in parents of children with autism spectrum disorders and in the development of relevant support and assistance programmes. Quality of Life Research: an International Journal of Quality of Life Aspects of Treatment, Care and Rehabilitation, 20(8), 1279–1294.
Caprara, G. V., Scabini, E., Barbaranelli, C., Pastorelli, C., Regalia, C., & Bandura, A. (1998). Impact of adolescents’ perceived self-regulatory efficacy on familial communication and antisocial conduct. European Psychologist, 3(2), 125–132.
Cashin, A. (2004). Painting the vortex: the existential structure of the experience of parenting a child with autism. International Forum of Psychoanalysis, 13(3), 164–174.
Cousson-Gélie, F., Irachabal, S., Bruchon-Schweitzer, M., Dilhuydy, J. M., & Lakdja, F. (2005). Dimensions of cancer locus of control scale as predictors of psychological adjustment and survival in breast cancer patients. Psychological Reports, 97(3), 699–711.
Dawson, G. (2008). Early behavioral intervention, brain plasticity, and the prevention of autism spectrum disorder. Development and Psychopathology, 20(3), 775–803.
de Montigny, F., Lacharité, C. (2005). Perceived parental efficacy: concept analysis. Journal of Advance Nursing, 49(4), 387–396.
DeVellis, R. F. (1985). Development and validation of the child improvement locus of control (CILC) scales. Journal of Social and Clinical Psychology, 3(3), 307–324.
Donenberg, G., & Baker, B. L. (1993). The impact of young children with externalizing behaviors on their families. Journal of Abnormal Child Psychology, 21(2), 179–198.
Dunn, M. E., Burbine, T., Bowers, C. A., & Tantleff-Dunn, S. (2001). Moderators of stress in parents of children with autism. Community Mental Health Journal, 37(1), 39–52.
Dunn, W., Cox, J., Foster, L., Mische-Lawson, L., & Tanquary, J. (2012). Impact of a contextual intervention on child participation and parent competence among children with autism spectrum disorders: a pretest-posttest repeated-measures design. American Journal of Occupational Therapy, 66(5), 520–528.
Eldevik, S., Hastings, R. P., Hughes, J. C., Jahr, C., Eikeseth, E., & Cross, S. (2010). Using participant data to extend the evidence base for intensive behavioral intervention for children with autism. American Journal of Intellectual and Developmental Disability, 115, 381–405.
Elsabbagh, M., Divan, G., Koh, Y. J., Kim, Y. S., Kauchali, S., Marcin, C., & Fombonne, E. (2012). Global prevalence of autism and other pervasive developmental disorders. Autism Research: Official Journal of the International Society for Autism Research, 5(3), 160–179.
Estes, A., Vismara, L., Mercado, C., Fitzpatrick, A., Elder, L., Greenson, J., & Rogers, S. (2014). The impact of parent-delivered intervention on parents of very young children with autism. Journal of Autism and Developmental Disorders, 44(2), 353–365.
Fetters, M. D., Curry, L. A., & Creswell, J. W. (2013). Achieving integration in mixed methods designs-principles and practices. Health Services Research, 48(6 Pt 2), 2134–56.
Fombonne, E. (2009). A wrinkle in time: from early signs to a diagnosis of autism. Journal of the American Academy of Child and Adolescent Psychiatry, 48(5), 463–464.
Foster, L., Dunn, W., & Lawson, L. M. (2013). Coaching mothers of children with autism: a qualitative study for occupational therapy practice. Physical & Occupational Therapy in Pediatrics, 33(2), 253–263.
Frantzen, K. K., & Fetters, M. D. (2015). Meta-integration for synthesizing data in a systematic mixed studies review: insights from research on autism spectrum disorder. Quality and Quantity, online access. doi:10.1007/s11135-015-0261-6.
Giallo, R., Wood, C. E., Jellett, R., & Porter, R. (2013). Fatigue, wellbeing and parental self-efficacy in mothers of children with an autism spectrum disorder. Autism: The International Journal of Research and Practice, 17(4), 465–480.
Goin-Kochel, R. P., & Myers, B. J. (2005). Congenital versus regressive onset of autism spectrum disorders: parents’ beliefs about causes. Focus on Autism and Other Developmental Disabilities, 20(3), 169–179.
Goin-Kochel, R. P., Myers, B. J., & Mackintosh, V. H. (2007). Parental reports on the use of treatments and therapies for children with autism spectrum disorders. Research in Autism Spectrum Disorders, 1(3), 195–209.
Goldberg, L. R. (1999). A broad-bandwidth, public domain, personality inventory measuring the lower-level facets of several five-factor models. In I. Mervielde, F. Deary, F. De Fruyt, & F. Ostendorf (Eds.), Personality psychology in europe (Vol. 7, pp. 7–28). Tilburg: Tilburg Universities Press.
Goodman, S. J., & Glenwick, D. S. (2012). Correlates of attachment perceptions in parents of children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 42(10), 2056–2066.
Gray, D. E. (2001). Accommodation, resistance and transcendence: three narratives of autism. Social Science and Medicine, 53(9), 1247–1257.
Gray, D. E. (2002). Ten years on: a longitudinal study of families of children with autism. Journal of Intellectual and Developmental Disability, 27(3), 215–222.
Gray, D. E., & Holden, W. J. (1993). Psycho-social well-being among the parents of children with autism. Australia and New Zealand Journal of Developmental Disabilities, 18(2), 83–93.
Hamlyn-Wright, S., Draghi-Lorenz, R., & Ellis, J. (2007). Locus of control fails to mediate between stress and anxiety and depression in parents of children with a developmental disorder. Autism, 11(6), 489–501.
Hastings, R. P., & Brown, T. (2002). Behavior problems of children with autism, parental self-efficacy, and mental health. American Journal of Mental Retardation, 107(3), 222–232.
Hastings, R. P., & Johnson, E. (2001). Stress in UK families conducting intensive home-based behavioral intervention for their young child with autism. Journal of Autism and Developmental Disorders, 31(3), 327–336.
Hastings, R. P., & Symes, M. D. (2002). Early intensive behavioral intervention for children with autism: parental therapeutic self-efficacy. Research in Developmental Disabilities, 23(5), 332–341.
Hastings, R. P., Kovshoff, H., Brown, T., Ward, N. J., Espinosa, F. D., & Remington, B. (2005). Coping strategies in mothers and fathers of preschool and school-age children with autism. Autism, 9(4), 377–391.
Henderson, D., & Vandenberg, B. (1992). Factors influencing adjustment in the families of autistic children. Psychological Reports, 71(1), 167–171.
Hesse, T. L., Danko, C. M., & Budd, K. S. (2013). Siblings of children with autism: predictors of adjustment. Research in Autism Spectrum Disorders, 7(11), 1323–1331.
Higgins, D. J., Bailey, S. R., & Pearce, J. C. (2005). Factors associated with functioning style and coping strategies of families with a child with an autism spectrum disorder. Autism, 9(2), 125–137.
Hines, M., Balandin, S., & Togher, L. (2012). Buried by autism: older parents’ perceptions of autism. Autism, 16(1), 15–26.
Hodgetts, S., Savage, A., & McConnell, D. (2013). Experience and outcomes of stepping stones triple P for families of children with autism. Research in Developmental Disabilities, 34(9), 2572–2585. doi:10.1016/j.ridd.2013.05.005.
Johnston, C., & Mash, E. J. (1989). A measure of parenting satisfaction and efficacy. Journal of Clinical Child Psychology, 18(2), 167–175.
Jones T. L., Prinz, R. J. (2005). Potential roles of parental self-efficacy in parent and child adjustment: a review. Clinical Psychology Review, 25(3), 341–363.
Kandari, H. Y. (2005). Parenting stressors, needs for services, and caregiving self-efficacy among mothers of children with mild IDD in kuwait: assessing impact between variables. Boston: Simmons College. Unpublished Doctoral dissertation.
Kaniel, S., & Siman-Tov, A. (2011). Comparison between mothers and fathers in coping with autistic children: a multivariate model. European Journal of Special Needs Education, 26(4), 479–493.
Keen, D., Rodger, S., Doussin, K., & Braithwaite, M. (2007). A pilot study of the effects of a social-pragmatic intervention on the communication and symbolic play of children with autism. Autism, 11(1), 63–71.
Keen, D., Couzens, D., Muspratt, S., & Rodger, S. (2009). The effects of a parent-focused intervention for children with a recent diagnosis of autism spectrum disorder on parenting stress and competence. Research in Autism Spectrum Disorders, 4(2), 229–241.
King, G. A., Zwaigenbaum, L., King, S., Baxter, D., Rosenbaum, P., & Bates, A. (2006). A qualitative investigation of changes in the belief systems of families of children with autism or down syndrome. Child: Care, Health and Development, 32(3), 353–369.
Koren, P. E., DeChillo, N., & Friesen, B. J. (1992). Measuring empowerment in families whose children have emotional disabilities: a brief questionnaire. Rehabilitation Psychology, 37(4), 305–321.
Kuhn, J. C., & Carter, A. S. (2006). Maternal self-efficacy and associated parenting cognitions among mothers of children with autism. The American Journal of Orthopsychiatry, 76(4), 564–575.
Larson, E. (2010). Ever vigilant: maternal support of participation in daily life for boys with autism. Physical & Occupational Therapy in Pediatrics, 30(1), 16–27.
Lerner, M. D., Calhoun, C. D., Mikami, A. Y., & De Los Reyes, A. (2012). Understanding parent–child social informant discrepancy in youth with high functioning autism spectrum disorders. Journal of Autism and Developmental Disorders, 42(12), 1–13.
Lloyd, T., & Hastings, R. P. (2009). Parental locus of control and psychological well-being in mothers of children with intellectual disability. Journal of Intellectual & Developmental Disability, 34(2), 104–115.
MacKintosh, V. H., Goin-Kochel, R. P., & Myers, B. J. (2012). “What do you like/dislike about the treatments you’re currently using?”: a qualitative study of parents of children with autism spectrum disorders. Focus on Autism and Other Developmental Disabilities, 27(1), 51–60.
Malow, B. A., Adkins, K. W., Reynolds, A., Weiss, S. K., Loh, A., Fawkes, D., & Clemons, T. (2014). Parent-based sleep education for children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 44(1), 216–228.
Manor-Binyamini, I. (2011). Mothers of children with developmental disorders in the bedouin community in israel: family functioning, caregiver burden, and coping abilities. Journal of Autism and Developmental Disorders, 41(5), 610–617.
Matson, J. L., Adams, H. L., Williams, L. W., & Rieske, R. D. (2013). Why are there so many unsubstantiated treatments in autism? Research in Autism Spectrum Disorders, 7(3), 466–474.
Meirsschaut, M., Roeyers, H., & Warreyn, P. (2010). Parenting in families with a child with autism spectrum disorder and a typically developing child: mothers’ experiences and cognitions. Research in Autism Spectrum Disorders, 4(4), 661–669.
Miles, M. B., Huberman, A. M., & Saldaña, J. (2014). Qualitative data analysis: a methods sourcebook (3rd ed.). Thousand Oaks: SAGE Publications, Inc.
Myers, B. J., Mackintosh, V. H., & Goin-Kochel, R. P. (2009). “My greatest joy and my greatest heart ache:” parents’ own words on how having a child in the autism spectrum has affected their lives and their families’ lives. Research in Autism Spectrum Disorders, 3(3), 670–684.
Nowicki, S. J., & Duke, M. P. (1983). The Nowicki-Strickland life-span locus of control scales: construct validation. In H. M. Lefcourt (Ed.), Research with the locus of control construct (Vol. 2, pp. 9–51). New York: Academic.
Olsson, M. B., & Hwang, C. P. (2008). Socioeconomic and psychological variables as risk and protective factors for parental well-being in families of children with intellectual disabilities. Journal of Intellectual Disability Research, 52(12), 1102–1113.
Osborne, L. A., McHugh, L., Saunders, J., & Reed, P. (2008). Parenting stress reduces the effectiveness of early teaching interventions for autistic spectrum disorders. Journal of Autism and Developmental Disorders, 38(6), 1092–1103.
Pakenham, K. I., Sofronoff, K., & Samios, C. (2004). Finding meaning in parenting a child with asperger syndrome: correlates of sense making and benefit finding. Research in Developmental Disabilities, 25(3), 245–264.
Patten, E., Baranek, G. T., Watson, L. R., & Schultz, B. (2013). Child and family characteristics influencing intervention choices in autism spectrum disorders. Focus on Autism and Other Developmental Disabilities, 28(3), 138–146.
Pisula, E., & Kossakowska, Z. (2010). Sense of coherence and coping with stress among mothers and fathers of children with autism. Journal of Autism and Developmental Disorders, 40(12), 1485–94.
Pluye, P., & Nha Hong, Q. (2014). Combining the power of stories and the power of numbers: mixed methods research and mixed studies reviews. Annual Review of Public Health, 35, 29–45.
Pluye, P., Robert, E., Cargo, M., Bartlett, G., O’Cathain, A., Griffiths, F., Rousseau, M. C. (2011). Proposal: a mixed methods appraisal tool for systematic mixed studies reviews. Retrieved from http://mixedmethodsappraisaltoolpublic.pbworks.com.
Pope, C., Mays, N., & Popay, J. (2007). Synthesizing qualitative and quantitative health evidence: a guide to methods. Maidenhead: Open University Press, McGraw Hill Education.
Pozo, P., Sarria, E., & Brioso, A. (2014). Family quality of life and psychological well-being in parents of children with autism spectrum disorders: a double ABCX model. Journal of Intellectual Disability Research, 58(5), 442–58.
Pritchett, R., Kemp, J., Wilson, P., Minnis, H., Bryce, G., & Gillberg, C. (2011). Quick, simple measures of family relationships for use in clinical practice and research. A systematic review. Family Practice, 28(2), 172–187.
Raj, A., & Salagame, K. K. (2010). Effect of sensitized coaching on self-efficacy of parents of children with autism. Journal on Developmental Disabilities, 16(2), 44–51.
Reichow, B. (2012). Overview of meta-analyses on early behavioral intervention for young children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 42(4), 512–520.
Reitzel, J., Summers, J., Lorv, B., Szatmari, P., Zwaigenbaum, L., Georgiades, S., & Duku, E. (2013). Pilot randomized controlled trial of a functional behavior skills training program for young children with autism spectrum disorder who have significant early learning skill impairments and their families. Research in Autism Spectrum Disorders, 7(11), 1418–1432.
Rodrigue, J. R., Morgan, S. B., & Geffken, G. R. (1992). Psychosocial adaptation of fathers of children with autism, down syndrome, and normal development. Journal of Autism and Developmental Disorders, 22(2), 249–263.
Rosenberg, M. (1965). Society and the adolescent self-image. Princeton: Princeton University Press.
Rosenberg, M. (1979). Conceiving the self. New York: Basic Books.
Rotter, J. B. (1966). Generalized expectancies for internal versus external control of reinforcement. Psychological Monographs, 80(1), 1.
Rotter, J. B. (1975). Some problems and misconceptions related to the construct of internal versus external control of reinforcement. Journal of Consulting and Clinical Psychology, 43(1), 56–67.
Rutgers, A. H., van Ijzendoorn, M. H., Bakermans-Kranenburg, M. J., Swinkels, S. H., van Daalen, E., Dietz, C., & van Engeland, H. (2007). Autism, attachment and parenting: a comparison of children with autism spectrum disorder, mental retardation, language disorder, and non-clinical children. Journal of Abnormal Child Psychology, 35(5), 859–870.
Shu, B. C. (2009). Quality of life of family caregivers of children with autism: the mother’s perspective. Autism, 13(1), 81–91.
Shu, B. C., Lo, L. H., Lin, L. L., Hsieh, S. C., Li, S. M., & Wu, S. C. (2006). Process of self-identity transformation in women with autistic adolescent. Journal of Nursing Research, 14(1), 55–64.
Siller, M., & Sigman, M. (2002). The behaviors of parents of children with autism predict the subsequent development of their children’s communication. Journal of Autism and Developmental Disorders, 32(2), 77–89.
Siman-Tov, A., & Kaniel, S. (2011). Stress and personal resource as predictors of the adjustment of parents to autistic children: a multivariate model. Journal of Autism and Developmental Disorders, 41, 879–890.
Sivberg, B. (2002a). Coping strategies and parental attitudes, a comparison of parents with children with autistic spectrum disorders and parents with non-autistic children. International Journal of Circumpolar Health, 61(2), 36–50.
Sivberg, B. (2002b). Family system and coping behaviors: a comparison between parents of children with autistic spectrum disorders and parents with non-autistic children. Autism, 6(4), 397–409.
Sofronoff, K., & Farbotko, M. (2002). The effectiveness of parent management training to increase self-efficacy in parents of children with asperger syndrome. Autism, 6(3), 271–286.
Sofronoff, K., Jahnel, D., & Sanders, M. (2011). Stepping stones triple P seminars for parents of a child with a disability: a randomized controlled trial. Research in Developmental Disabilities, 32(6), 2253–2262.
Solish, A., & Perry, A. (2008). Parents’ involvement in their children’s behavioral intervention programs: parent and therapist perspectives. Research in Autism Spectrum Disorders, 2(4), 728–738.
Strauss, K., Benvenuto, A., Battan, B., Siracusano, M., Terribili, M., Curatolo, P., & Fave, L. (2015). Promoting shared decision making to strengthen outcome of young children with autism spectrum disorders: the role of staff competence. Research in Developmental Disabilities, 38, 48–63.
Teti, D. M., & Gelfand, D. M. (1991). Behavioral competence among mothers of infants in the first year: the mediational role of maternal self-efficacy. Child Development, 62(5), 918–929.
Weiss, J. A., Cappadocia, M. C., MacMullin, J. A., Viecili, M., & Lunsky, Y. (2012). The impact of child problem behaviors of children with ASD on parent mental health: the mediating role of acceptance and empowerment. Autism, 16(3), 261–274.
Weiss, J. A., Viecili, M. A., Sloman, L., & Lunsky, Y. (2013a). Direct and indirect psychosocial outcomes for children with autism spectrum disorder and their parents following a parent-involved social skills group intervention. Journal of the Canadian Academy of Child and Adolescent Psychiatry = Journal De L’Academie Canadienne De Psychiatrie De L'Enfant Et De L’Adolescent, 22(4), 303–309.
Weiss, J. A., Robinson, S., Fung, S., Tint, A., Chalmers, P., & Lunsky, Y. (2013b). Family hardiness, social support, and self-efficacy in mothers of individuals with autism spectrum disorders. Research in Autism Spectrum Disorders, 7(11), 1310–1317.
Werner, S., & Shulman, C. (2013). Subjective well-being among family caregivers of individuals with developmental disabilities: the role of affiliate stigma and psychosocial moderating variables. Research in Developmental Disabilities, 34(11), 4103–4114.
Acknowledgments
This research was supported by the Tryg Foundation, the Family Hede Nielsen Foundation, and the Central Denmark Region. Hanne Munch Kristiansen and Helene Sognstrup, Aarhus University Library, Psychiatry, provided professional library support to conduct the systematic literature search to conduct this review.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
No financial disclosure for any of the above mentioned authors.
Rights and permissions
About this article

Cite this article
Frantzen, K.K., Lauritsen, M.B., Jørgensen, M. et al. Parental Self-perception in the Autism Spectrum Disorder Literature: a Systematic Mixed Studies Review. Rev J Autism Dev Disord 3, 18–36 (2016). https://doi.org/10.1007/s40489-015-0063-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40489-015-0063-8