
Abstract
Purpose
Chest x-ray (CXR) is the standard imaging used to evaluate children in acute respiratory distress and failure. Our objective was to compare the lung-imaging techniques of CXR and lung ultrasound (LUS) in the evaluation of children with acute respiratory failure (ARF) to quantify agreement and to determine which technique identified a higher frequency of pulmonary abnormalities.
Methods
This was a secondary analysis of a prospective observational study evaluating the sensitivity and specificity of LUS in children with ARF from 12/2018 to 02/2020 completed at the University of Wisconsin-Madison (USA). Children > 37.0 weeks corrected gestational age and ≤ 18 years of age admitted to the PICU with ARF were evaluated with LUS. We compared CXR and LUS completed within 6 h of each other. Kappa statistics (k) adjusted for maximum attainable agreement (k/kmax) were used to quantify agreement between imaging techniques and descriptive statistics were used to describe the frequency of abnormalities.
Results
Eighty-eight children had LUS completed, 32 with concomitant imaging completed within 6 h are included. There was fair agreement between LUS and CXR derived diagnoses with 58% agreement (k/kmax = 0.36). Evaluation of imaging patterns included: normal, 57% agreement (k = 0.032); interstitial pattern, 47% agreement (k = 0.003); and consolidation, 65% agreement (k = 0.29). CXR identified more imaging abnormalities than LUS.
Conclusions
There is fair agreement between CXR and LUS-derived diagnoses in children with ARF. Given this, clinicians should consider the benefits and limitations of specific imaging modalities when evaluating children with ARF. Additional studies are necessary to further define the role of LUS in pediatric ARF given the small sample size of our study.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Chest x-ray (CXR) is among the most commonly utilized tools in the assessment pediatric respiratory diseases and is a standard imaging technique to evaluate children in acute respiratory distress and failure [1]. Respiratory illness accounts for between 20 and 30% of pediatric intensive care unit (PICU) and ward admissions [2]. CXR is estimated to be obtained in 50% of PICU admissions [3]. Despite ubiquitous usage, CXRs accuracy and reliability has never been rigorously evaluated (i.e., compared to chest computerized tomography (CT)) [4]. While chest CT is considered the gold standard pulmonary imaging modality, CXR is the standard against which newer imaging techniques, such as lung ultrasound (LUS), are evaluated in pediatrics to limit exposure to the high ionizing radiation of CT [5,6,7].
Few studies have evaluated the diagnostic accuracy of CXR compared with CT and have demonstrated low to modest sensitivity (range 40–79%) and specificity (range 39–92%) in identifying pulmonary pathology [8,9,10,11]. Clinicians still highly value CXRs despite their low accuracy and continue to regularly utilize them in clinical practice [12]. Recently published guidelines support the use of LUS in pediatric respiratory diseases, yet cited studies include few children with acute respiratory failure (ARF), such as children requiring ancillary respiratory therapies, high supplemental oxygen support (hypoxemic respiratory failure), invasive or non-invasive mechanical support (hypercapnic respiratory failure), or an escalation from baseline respiratory support (acute on chronic respiratory failure) [13]. Many studies of specific disease processes have found LUS has high sensitivity (range 89–97%) and specificity (range 56–99%) identifying findings consistent with the underlying disease process; however, it has also been consistently described that children with a worse clinical course (defined by the requirement of more hospital resources) demonstrate more ultrasound abnormalities [14,15,16,17]. Therefore, our study objective was to compare lung imaging techniques (CXR and LUS) in the evaluation of children with undifferentiated ARF to quantify imaging agreement and determine which technique identifies a higher frequency of pulmonary abnormalities. We hypothesized that LUS would identify substantially more abnormalities than CXR in children with ARF. If borne out, clinicians may be able to reduce the financial cost and radiation exposure associated with CXR utilization while affording a better understanding of pulmonary pathophysiology and allowing for more specific treatments.
Methods
The Institutional Review Board at the University of Wisconsin-Madison (USA) approved this pre-designed secondary analysis of a prospective observational study evaluating the sensitivity and specificity of LUS in children admitted to the pediatric intensive care unit (PICU) with ARF (IRB 2018-071) [18]. ARF for the study was defined by the clinical needed for PICU admission and at least one of the following: (1) non-invasive (high flow nasal cannula (HFNC) ≥ 1 L/kg/min; continuous positive airway pressure; or bilevel positive airway pressure delivered by nasal cannula, nasal mask, or full face mask) or invasive respiratory support; (2) supplemental oxygen with FiO2 > 35% while on HFNC < 1 L/kg/min or nonrebreather/oxymask to maintain saturation ≥ 90%; (3) continuous nebulized therapy; or (4) chronic oxygen or ventilatory support and any increase in baseline support [18, 19]. Children > 37.0 weeks corrected gestational age and ≤ 18 years of age from whom signed, informed parent/guardian consent, and assent when appropriate, were enrolled from December 2018 to February 2020.
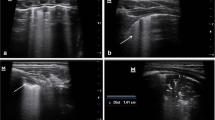
A 3-region per hemithorax LUS was completed using a modified BLUE (Bedside Lung Ultrasound in Emergency) protocol within 14 h of PICU admission by one of three pediatric intensivists with point-of-care ultrasound training and clinical LUS experience [20, 21]. The three lung regions were defined by: (1) the anterior chest wall between the anterior axillary line and sternum; (2) the lateral chest wall between the anterior and posterior axillary lines; and (3) the posterolateral chest wall between the posterior axillary line and the spine (Fig. 1A). For each region, the most abnormal ultrasound pattern was identified and a representative 4-s video recorded and uploaded to Q-path imaging system (Telexy Healthcare; British Columbia, Canada). In Q-path, an assessment of ultrasound artifacts was made for each individual region and an overall diagnosis determined (e-Table 1A). For comparison with CXR, A lines were considered a normal ultrasound pattern; multiple B lines and confluent B lines were considered an interstitial disease pattern; and sub-pleural consolidation and lobar consolidation were considered consolidation patterns [21, 22]. All patients/images were examined by a senior intensivist with extensive experience in LUS acquisition and interpretation and blinded to patient historical and clinical information. A second physician (ultrasound fellowship-trained emergency medicine physician) independently reviewed all images to determine an ultrasound diagnosis, but did not document individual ultrasound artifact findings due to loss of documented lung region location during a Q-path system upgrade. Differences in diagnoses between the two were resolved by consensus.

Lung ultrasound (A) and chest radiograph (B) regions. LA left anterior, LL left lateral, LLL left lower lobe, LP left posterior, LU left upper lobe, RA right anterior, RLL right lower (right middle lobe and right lower lobe), RP right posterior, RU right upper lobe
Clinical CXRs completed within 6 h of LUS were evaluated concurrently by two pediatric radiologists who were blinded to patient historical, clinical, and LUS information. CXRs were evaluated for the presence of interstitial lung disease, atelectasis, consolidations, pleural effusions, and pneumothoraces across four lung regions and a radiographic diagnosis was determined [22]. Differences in CXR interpretation were resolved in real-time by consensus (Fig. 1B; e-Table 1B). The six LUS regions were combined into four to correspond with the four CXR regions, approximating the five lung lobes (e-Table 2) [22]. A LUS sub-pleural consolidation (SPC) artifact was considered a consolidation for the primary study analysis [22]. A separate analysis was conducted that did not include SPC as a consolidation, as small consolidations may not be identified on CXR. A CXR finding of atelectasis was considered a consolidation for comparisons. Given the relatively long duration between imaging studies, sub-analyses of studies completed within 4 h and within 2 h of each other were additionally performed.
All LUS exams were performed using a Philips Sparq ultrasound machine (Koninklijke Philips N.V; Amsterdam, Netherlands) with a L12-4 linear probe (frequency 12–4 MHz) or S4-2 phased array probe (frequency 4–2 MHz) with children in a recumbent or semi-recumbent position and (when clinically feasible) rolled onto their side or placed into a sitting position to optimize posterior lung field scanning according to the previously published protocol [18]. In the PICU, a portable single view anterior–posterior (AP) CXR was obtained using a Fujifilm FDR Go Mobile radiograph machine (Fujifilm Medical Systems; Connecticut, USA). In the Emergency Department either a portable single view AP CXR was obtained using a Philips MobileDiagnost wDR 2.2 (Philips Healthcare; Massachusetts, USA) or a two-view AP and lateral CXR was obtained using Samsung GC85 radiograph machine (Samsung/Neurologica Corporation; Massachusetts, USA). All CXR imaging was obtained according to standard hospital thoracic imaging protocols, as requested for clinical care by the clinicians caring for the patient. The reference standard for the final patient diagnosis was an independent, standardized review of the medical record following hospital discharge by a physician not involved in the care of the patient (final diagnosis) and incorporated the history, clinical findings, laboratory tests, radiographic (including CXR) data, patient management, and course to determine the etiology of the ARF [18].
Descriptive statistics were used to define the frequency of imaging abnormalities. Kappa statistics (k) adjusted for maximum attainable agreement (kmax) were used to quantify agreement between techniques [23,24,25]. The 95% confidence intervals (95% CI) for k and kmax were computed by bootstrap replications (B = 5000) [26]. The k/kmax was used when the sparsity of diagnoses made the default maximum of one unattainable, as the upper and lower limits of k are a function of the frequency [24]. Kappa statistical agreement (for both k and k/kmax) was considered: k ≤ 0.00, less than chance agreement; k > 0.00–0.20, slight agreement; k > 0.20–0.40, fair agreement; k > 0.40–0.60, moderate agreement; k > 0.60–0.80, substantial agreement; and k ≥ 0.80, near perfect agreement [25]. Statistical analysis was performed using R version 3.6.3 (R Project for Statistical Computing; Vienna, Austria). The study was registered with ClinicalTrials.gov and data are reported using Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Results
Eighty-eight children had LUS completed for the primary study [18]; 32 of these 88 (36%) had LUS and CXR completed within 6 h of each other and are included in this study (e-Fig. 1). The study cohort includes 2 (6%) patients with status asthmaticus, 17 (53%) with bronchiolitis/viral pneumonitis, 12 (37%) with pneumonia, and 1 (3%) patient with multiple concurrent final diagnoses. CXR was completed a median of 1.25 h (IQR − 2.0 to 5.81) following PICU admission while LUS was completed a median of 4.67 h (IQR 2.70–7.63) following PICU admission and a median of 3.64 h (IQR 1.85–5.88) from CXR. Demographics of the study cohort are presented in Table 1.
There was fair agreement between LUS and CXR derived diagnoses with 58% agreement (k/kmax = 0.36, 95% CI − 0.01 to 0.80) (Table 2A). CXR identified more abnormalities (104 abnormal lung regions across 123 examined regions) compared with LUS (71 abnormal regions) (Table 3A; e-Table 3). Evaluation of specific imaging patterns included: normal, 57% agreement (k = 0.032, 95% CI − 0.11 to 0.17); interstitial pattern, 47% agreement (k = 0.003, 95% CI − 0.20 to 0.20); consolidation, 65% agreement (k = 0.294, 95% CI 0.13–0.46); pleural effusion, 94% agreement (k = NA; one imaging modality did not find an effusion); and pneumothorax, 99% agreement (k = NA; one imaging modality did not find a pneumothorax) (Table 3B).
When comparing LUS and CXR with the final patient diagnosis, LUS demonstrated moderate agreement (k/kmax = 0.43, 95% CI 0.12–0.84) while CXR demonstrated slight agreement (k/kmax = 0.18, 95% CI − 0.21 to 0.65) (Table 2B). Additional analyses evaluating agreement between LUS and CXR when SPCs were not considered LUS determined consolidations and when comparing imaging obtained within 4 h and 2 h of each other, did not significantly increase agreement (Table 4).
There was substantial agreement between the intensivist and emergency medicine physician-derived ultrasound diagnoses with 67% observed agreement (k/kmax = 0.61, 95% CI 0.49–0.78) [27]. Agreement in CXR interpretation between radiologists was not determined as interpretations were performed concurrently with differences resolved in real-time.
Discussion
Acute respiratory distress and failure are among the most common indications for pediatric hospitalization [2]. As such, there is great interest in improving diagnostic accuracy and treatment specificity given the high disease burden and associated costs [2]. Given frequent diagnostic uncertainty, many children presenting with respiratory concerns, especially when on the severe end of the disease spectrum, are initially treated with a multi-therapy approach until the underlying etiology becomes better defined, after which therapeutic de-escalation may occur [28,29,30]. LUS has proven useful in adult medicine where it demonstrates improved sensitivity and specificity in determining the etiology of ARF when compared with standard clinical evaluation (history, physical, and CXR imaging) [21, 22, 31, 32]. The few studies evaluating the ability of LUS to determine the underlying etiology in undifferentiated pediatric respiratory distress and failure have been less convincing [16, 18, 20, 33, 34]; though when evaluating a single suspected disease entity, LUS appears to have favorable operating characteristics [5, 6, 14, 17, 35]. Most pediatric studies use CXR as the standard against which LUS is compared [5,6,7] and most use children with a known or suspected disease process (and thus high pre-test probability). In a blinded assessment of temporally related imaging studies, we found only fair agreement between imaging derived diagnoses and fair to slight agreement in identifying specific imaging abnormality patterns. CXR detected more interstitial disease and pleural effusions while LUS detected more consolidations and pneumothoraces, though neither of these were statistically more than CXR.
Chest CT is considered the preeminent pulmonary imaging modality but in contrast to adult medicine, in which CT is considered very early in the disease course, it is hardly ever used for diagnosis of acute pediatric respiratory diseases because of the high ionizing radiation, difficulty in patient cooperation, and high cost [5, 6]. Instead, clinical examination and CXR remain standard of care despite relatively low sensitivity and specificity [5, 8, 9, 36]. In a study of 56 children being evaluated for complicated pneumonia that were unresponsive to therapy, CXR missed 110 CT findings, including parenchymal, pleural, and consolidative findings [36]. In another study of 949 children with suspected pneumonia who underwent CT, CXR demonstrated only 79% sensitivity and 60% specificity [8] and in a study of 36 children with suspected pneumonia who underwent CT, CXR demonstrated 62% sensitivity (specificity not reported) [9]. These two studies additionally evaluated LUS with CT and found that LUS demonstrated slightly improved sensitivity and similar or worse specificity when compared with CXR [8, 9]. Still, meta-analyses comparing LUS to CXR demonstrate pooled estimates of the area under the receiver operating curve of 98% [5, 6]. However, the utility of evaluating LUS compared with an imaging modality with known modest operating characteristics is unclear. A large (413 patients with 1002 CXR/LUS comparisons) recently published study similarly comparing imaging patterns in children with concomitantly obtained CXR and LUS found k agreement ranging from 0.51 (moderate agreement) in the detection of left sided pleural effusion to 0.98 (near perfect agreement) in the detection of right sided pneumothorax [37]; though agreement did differ significantly based on imaged region/location and only 19% of patients had underlying respiratory pathology. Another study of 81 children comparing LUS with CXR found k agreement of 0.64 (substantial agreement) for the diagnosis of pneumonia [38], though agreement for other disease processes are not specifically provided. Newer LUS studies are evaluating temporal trends and changes over time including using the lung ultrasound score to evaluate children with bronchiolitis [14, 39, 40] and pediatric acute respiratory distress syndrome [41], and to evaluate changes in lung aeration over time [42].
Pediatric researchers are also beginning to utilize alternative ultrasound modes (i.e., non-B mode) to more thoroughly define LUS specific patterns for individual disease processes [43]. M-mode has classically been utilized to detect pleural motion (or lack thereof) over time; now doppler ultrasound is being used to describe consolidation characteristics [43]. Color and pulsed wave doppler have been used to identify the presence and type of vessels within consolidations [44], helping to differentiate fluid or mucus filled bronchograms, lung necrosis, and abscesses [43]. Incorporation of lesion characteristics including size, number, and distribution of consolidations, position and motion of bronchograms, as well as pleural effusion characteristics and the distribution, movement, and characteristics of vertical artifacts can all significantly complement LUS evaluation [45, 46]. Contrast-enhanced ultrasound and microvascular flow imaging are additional techniques being studied which may provide benefit in LUS [47, 48]. Inclusion of real-time ultrasound during therapeutic trials and inclusion of clinical information may further inform LUS examination [33, 49].
LUS also has proposed benefits outside of its diagnostic abilities, including its ubiquity in patient care units, it does not rely on another provider for performance (it is interpreted by a provider with clinical knowledge of the patient), it promotes provider time spent at the bedside, it is readily repeatable, that allows immediate integration into treatment plans, and that it has a rapid time to acquisition (typically < 10–15 min but shorter with a directed clinical question) [13, 18, 33, 50]; though in certain instances or circumstances these may not be considered beneficial. LUS has additionally been used to guide therapeutic intervention and patient reassessment including in guiding fluid administration/diuresis, lung recruitment, and chest tube insertion [13, 51]; in emergent or time-sensitive situations such as determination of the presence of a pneumothorax [13, 51, 52]; it has been combined with point-of-care cardiac exams to evaluate for reversible causes of cardiopulmonary arrest [51]; and it may be helpful in rapid assessment of reflux/aspiration risk [53]. Our data and similar recently published studies [37,38,39, 41, 42] suggest that it is likely that LUS plays a complimentary role to CXR in children with respiratory distress and ARF given differences in strengths and weaknesses [54], though our study was not specifically designed to test this. CXR provides an overall picture of the patient at a moment in time, is well established in clinical care, and is completed by another provider allowing for quick examination of multiple patients, while LUS provides more regionalized information, is performed by providers caring for the patient, and can readily be repeated following changes in therapeutic intervention or patient pathophysiology.
A major limitation in the use of LUS is in its inability to detect peri-hilar lesions which are especially common in pediatrics, as it requires findings which extend to the pleural surface [49, 50]. Additional limitations specific to our study include: failure to evaluate LUS and CXR operating characteristics with CT (the gold standard pulmonary imaging modality); evaluation of only the most abnormal LUS pattern in each lung region which may have decreased agreement; evaluation of only 3 LUS regions per hemithorax and inclusion of single view AP CXR which likely decreased the number of identified pathology and thus imaging sensitivity, though chosen for the study design given its clinically pragmatic approach; utilization of approximate lung anatomy (lobes) and corresponding imaging location which may not have correlated with actual anatomy; imaging interpretation being blinded to the patient’s history (and interpretation by different providers) which likewise may have decreased agreement (and is different from clinical practice, though chosen for our study design to reduce confirmation bias and maximize reliability); inability to use a LUS expert consensus of ultrasound artifact findings (due to loss of documented lung region location during a Q-path system upgrade) which may have increased or decreased lesion and location specific agreement; failure to compare agreement in lesion size which may influence a patient’s clinical presentation and course; failure to include patients with pulmonary edema, pneumothorax, or pleural effusion which may have increased agreement; utilization of standard clinical imaging (CXR) in the final diagnosis; and the 6-h duration between imaging which may have been sufficient for changes in pulmonary pathophysiology (either due to progression or improvement with treatment) so as to change imaging patterns (though sub-analyses completed at shorter intervals did not significantly increase agreement). Though chest CT is considered the “gold standard” lung imaging modality, given its limitations, it is not the “standard of [clinical] care” used in pediatrics; future studies should consider evaluating imaging modalities in the context of clinical care (rather than using a blinded interpretation as in this study), as well as evaluating how image acquisition and interpretation influences clinical management.
Conclusion
There is fair agreement between CXR and LUS-derived imaging diagnoses in children with ARF when imaging is completed within 6 h of each other. Given this, clinicians should consider the benefits and limitations of specific imaging modalities when evaluating children with ARF. Additional studies are necessary to further define the role of LUS in children with ARF given the small sample size of our study.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
- AP:
-
Anterior–posterior
- ARF:
-
Acute respiratory failure
- BLUE:
-
Bedside lung ultrasound in emergency protocol
- CT:
-
Computerized tomography
- CXR:
-
Chest x-ray
- HFNC:
-
High flow nasal cannula
- LUS:
-
Lung ultrasound
- PICU:
-
Pediatric intensive care unit
- SPC:
-
Subpleural consolidation
References
Price MB, Grant MJ, Welkie K (1999) Financial impact of elimination of routine chest radiographs in a pediatric intensive care unit. Crit Care Med 27:1588–1593. https://doi.org/10.1097/00003246-199908000-00033
Leyenaar JK, Ralston SL, Shieh M-S et al (2016) Epidemiology of pediatric hospitalizations at general hospitals and freestanding children’s hospitals in the United States. J Hosp Med 11:743–749. https://doi.org/10.1002/jhm.2624
Gupta R, Nallasamy K, Williams V et al (2021) Prescription practice and clinical utility of chest radiographs in a pediatric intensive care unit: a prospective observational study. BMC Med Imaging 21:44. https://doi.org/10.1186/s12880-021-00576-6
Gurney JW (1995) Why chest radiography became routine. Radiology 195:245–246. https://doi.org/10.1148/radiology.195.1.7892479
Pereda MA, Chavez MA, Hooper-Miele CC et al (2015) Lung ultrasound for the diagnosis of pneumonia in children: a meta-analysis. Pediatrics 135:714–722. https://doi.org/10.1542/peds.2014-2833
Orso D, Ban A, Guglielmo N (2018) Lung ultrasound in diagnosing pneumonia in childhood: a systematic review and meta-analysis. J Ultrasound 21:183–195. https://doi.org/10.1007/s40477-018-0306-5
Xin H, Li J, Hu H-Y (2018) Is lung ultrasound useful for diagnosing pneumonia in children?: A meta-analysis and systematic review. Ultrasound Q 34:3–10. https://doi.org/10.1097/RUQ.0000000000000330
Yan C, Hui R, Lijuan Z, Zhou Y (2020) Lung ultrasound vs. chest X-ray in children with suspected pneumonia confirmed by chest computed tomography: a retrospective cohort study. Exp Ther Med 19:1363–1369. https://doi.org/10.3892/etm.2019.8333
Ambroggio L, Sucharew H, Rattan MS et al (2016) Lung ultrasonography: a viable alternative to chest radiography in children with suspected pneumonia? J Pediatr 176:93–98. https://doi.org/10.1016/j.jpeds.2016.05.033. (e7)
Maughan BC, Asselin N, Carey JL et al (2014) False-negative chest radiographs in emergency department diagnosis of pneumonia. R I Med J (2013) 97:20–23
Winkler MH, Touw HR, van de Ven PM et al (2018) Diagnostic accuracy of chest radiograph, and when concomitantly studied lung ultrasound, in critically Ill patients with respiratory symptoms: a systematic review and meta-analysis. Crit Care Med 46:e707–e714. https://doi.org/10.1097/CCM.0000000000003129
Tolsma M, van der Voort PHJ, van der Meer NJM (2015) Why intensivists want chest radiographs. Crit care 19:100
Singh Y, Tissot C, Fraga MV et al (2020) International evidence-based guidelines on Point of Care Ultrasound (POCUS) for critically ill neonates and children issued by the POCUS Working Group of the European Society of Paediatric and Neonatal Intensive Care (ESPNIC). Crit Care 24:65. https://doi.org/10.1186/s13054-020-2787-9
Basile V, Di Mauro A, Scalini E et al (2015) Lung ultrasound: a useful tool in diagnosis and management of bronchiolitis. BMC Pediatr 15:63. https://doi.org/10.1186/s12887-015-0380-1
Bueno-Campaña M, Sainz T, Alba M et al (2019) Lung ultrasound for prediction of respiratory support in infants with acute bronchiolitis: a cohort study. Pediatr Pulmonol 54:873–880. https://doi.org/10.1002/ppul.24287
Varshney T, Mok E, Shapiro AJ et al (2016) Point-of-care lung ultrasound in young children with respiratory tract infections and wheeze. Emerg Med J 33:603–610. https://doi.org/10.1136/emermed-2015-205302
Dankoff S, Li P, Shapiro AJ et al (2017) Point of care lung ultrasound of children with acute asthma exacerbations in the pediatric ED. Am J Emerg Med 35:615–622. https://doi.org/10.1016/j.ajem.2016.12.057
DeSanti RL, Al-Subu AM, Cowan EA et al (2021) Point-of-care lung ultrasound to diagnose the etiology of acute respiratory failure at admission to the PICU. Pediatr Crit Care Med 22:722–732. https://doi.org/10.1097/PCC.0000000000002716
Tynan M (2015) Pediatric respiratory failure: the need for specific definitions. Assoc Clin Doc Improv Spec 1–9. https://acdis.org/
Tripathi S, Ganatra H, Martinez E et al (2019) Accuracy and reliability of bedside thoracic ultrasound in detecting pulmonary pathology in a heterogeneous pediatric intensive care unit population. J Clin Ultrasound 47:63–70. https://doi.org/10.1002/jcu.22657
Lichtenstein DA, Mezière GA (2008) Relevance of lung ultrasound in the diagnosis of acute respiratory failure: the BLUE protocol. Chest 134:117–125. https://doi.org/10.1378/chest.07-2800
Tierney DM, Huelster JS, Overgaard JD et al (2020) Comparative performance of pulmonary ultrasound, chest radiograph, and CT among patients with acute respiratory failure. Crit Care Med 48:151–157. https://doi.org/10.1097/CCM.0000000000004124
Cohen J (1960) A coefficient of agreement for nominal scales. Educ Psychol Meas 20:37–46
Cook RJ (2005) Kappa. In: Armitage P, Colton T (eds) Encyclopedia of Biostatistics, 2nd edn. John Wiley & Sons, Hoboken
Viera AJ, Garrett JM (2005) Understanding interobserver agreement: the kappa statistic. Fam Med 37:360–363
Banjanovic ES, Osborne JW (2016) Confidence intervals for effect sizes: applying bootstrap resampling. Pract Assess Res Eval. https://doi.org/10.7275/dz3r-8n08
DeSanti RL, Cowan EA, Kory PD et al (2022) The inter-rater reliability of pediatric point-of-care lung ultrasound interpretation in children with acute respiratory failure. J Ultrasound Med 41:1159–1167. https://doi.org/10.1002/jum.15805
Florin TA, Byczkowski T, Ruddy RM et al (2014) Variation in the management of infants hospitalized for bronchiolitis persists after the 2006 American Academy of Pediatrics bronchiolitis guidelines. J Pediatr 165:786–792. https://doi.org/10.1016/j.jpeds.2014.05.057. (e1)
Weiss AK, Hall M, Lee GE et al (2011) Adjunct corticosteroids in children hospitalized with community-acquired pneumonia. Pediatrics 127:e255–e263. https://doi.org/10.1542/peds.2010-0983
Baan EJ, Janssens HM, Kerckaert T et al (2018) Antibiotic use in children with asthma: cohort study in UK and Dutch primary care databases. BMJ Open 8:e022979. https://doi.org/10.1136/bmjopen-2018-022979
Xirouchaki N, Magkanas E, Vaporidi K et al (2011) Lung ultrasound in critically ill patients: comparison with bedside chest radiography. Intensive Care Med 37:1488–1493. https://doi.org/10.1007/s00134-011-2317-y
Lichtenstein D, Goldstein I, Mourgeon E et al (2004) Comparative diagnostic performances of auscultation, chest radiography, and lung ultrasonography in acute respiratory distress syndrome. Anesthesiology 100:9–15. https://doi.org/10.1097/00000542-200401000-00006
Özkaya AK, Başkan Vuralkan F, Ardıç Ş (2019) Point-of-care lung ultrasound in children with non-cardiac respiratory distress or tachypnea. Am J Emerg Med 37:2102–2106. https://doi.org/10.1016/j.ajem.2019.05.063
Hegazy LM, Rezk AR, Sakr HM, Ahmed AS (2020) Comparison of Efficacy of LUS and CXR in the Diagnosis of Children Presenting with Respiratory Distress to Emergency Department. Indian J Crit care Med Peer-Rev Off Publ Indian Soc Crit Care Med 24:459–464. https://doi.org/10.5005/jp-journals-10071-23459
Amatya Y, Russell FM, Rijal S et al (2023) Bedside lung ultrasound for the diagnosis of pneumonia in children presenting to an emergency department in a resource-limited setting. Int J Emerg Med 16:2. https://doi.org/10.1186/s12245-022-00474-w
Donnelly LF, Klosterman LA (1998) The yield of CT of children who have complicated pneumonia and noncontributory chest radiography. Am J Roentgenol 170:1627–1631. https://doi.org/10.2214/ajr.170.6.9609186
Sachdev A, Khatri A, Saxena KK et al (2021) Chest sonography versus chest radiograph in children admitted to paediatric intensive care—a prospective study. Trop Doct 51:296–301. https://doi.org/10.1177/00494755211016650
Phung NTN, Vo TTT, Hon KLE (2020) The role of lung ultrasonography in etiologic diagnosis of acute dyspnea in a resource limited setting. Bull Emerg Trauma 8:121–124. https://doi.org/10.30476/BEAT.2020.46453
Bobillo-Perez S, Sorribes C, Gebellí P et al (2021) Lung ultrasound to predict pediatric intensive care admission in infants with bronchiolitis (LUSBRO study). Eur J Pediatr 180:2065–2072. https://doi.org/10.1007/s00431-021-03978-4
Gori L, Amendolea A, Buonsenso D et al (2022) Prognostic role of lung ultrasound in children with bronchiolitis: multicentric prospective study. J Clin Med. https://doi.org/10.3390/jcm11144233
Zhang Y, Wang C, Wang F et al (2022) Lung ultrasound in pediatric acute respiratory distress syndrome received extracorporeal membrane oxygenation: a prospective cohort study. Front Pediatr 10:798855. https://doi.org/10.3389/fped.2022.798855
Fochi O, Bronco A, Nacoti M et al (2021) Modified pediatric lung ultrasound score compared with computed tomography for assessment of lung aeration in children. Minerva Anestesiol 87:675–683. https://doi.org/10.23736/S0375-9393.21.15155-7
Musolino AM, Tomà P, De Rose C et al (2021) Ten years of pediatric lung ultrasound: a narrative review. Front Physiol 12:721951. https://doi.org/10.3389/fphys.2021.721951
Acosta CM, Tusman G, Costantini M et al (2016) Doppler images of intra-pulmonary shunt within atelectasis in anesthetized children. Crit Ultrasound J 8:19. https://doi.org/10.1186/s13089-016-0055-7
Buonsenso D, Musolino A, Ferro V et al (2021) Role of lung ultrasound for the etiological diagnosis of acute lower respiratory tract infection (ALRTI) in children: a prospective study. J Ultrasound. https://doi.org/10.1007/s40477-021-00600-z
Buonsenso D, De Rose C, Ferro V et al (2022) Lung ultrasound to detect cardiopulmonary interactions in acutely ill children. Pediatr Pulmonol 57:483–497. https://doi.org/10.1002/ppul.25755
Rumolo M, Santarsiere M, Menna BF et al (2022) Color doppler and microvascular flow imaging to evaluate the degree of inflammation in a case of hidradenitis suppurativa. J Vasc Ultrasound 46:67–70. https://doi.org/10.1177/15443167211066491
Tufano A, Flammia RS, Antonelli L, et al (2021) The value of contrast-enhanced ultrasound (CEUS) in differentiating testicular masses: a systematic review and meta-analysis. Appl Sci 11: 8990. https://doi.org/10.3390/app11198990
Tusman G, Acosta CM, Nicola M et al (2015) Real-time images of tidal recruitment using lung ultrasound. Crit Ultrasound J 7:19. https://doi.org/10.1186/s13089-015-0036-2
Conlon TW, Nishisaki A, Singh Y et al (2019) Moving beyond the stethoscope: diagnostic point-of-care ultrasound in pediatric practice. Pediatrics. https://doi.org/10.1542/peds.2019-1402
Volpicelli G, Elbarbary M, Blaivas M et al (2012) International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med 38:577–591. https://doi.org/10.1007/s00134-012-2513-4
Scialanga B, Buonsenso D, Scateni S et al (2022) Lung ultrasound to detect pneumothorax in children evaluated for acute chest pain in the emergency department: an observational pilot study. Front Pediatr 10:812246. https://doi.org/10.3389/fped.2022.812246
Minella R, Minelli R, Rossi E et al (2021) Gastroesophageal and gastric ultrasound in children: the state of the art. J Ultrasound 24:11–14. https://doi.org/10.1007/s40477-020-00471-w
Conlon T, Keim G (2021) Pathophysiology versus etiology using lung ultrasound: clinical correlation required. Pediatr Crit Care Med 22:761–763
Iuri D, De Candia A, Bazzocchi M (2009) Evaluation of the lung in children with suspected pneumonia: usefulness of ultrasonography. Radiol Med 114:321–330. https://doi.org/10.1007/s11547-008-0336-8
Acknowledgements
We would like to thank Drs. Hagen and Allen for their guidance in the production of this project, the nurses for their enthusiasm and support of this research, and the families and patients at the University of Wisconsin-Madison for their willingness to participate.
Prior presentation
Study data were presented at the Society of Critical Care Medicine (SCCM) Annual Congress (2022 April 18; virtual conference).
Funding
This project was supported by the Clinical and Translational Science Award (CTSA) program through the NIH National Center for Advancing Translational Sciences (NCATS), Grant UL1TR002373. The content of the work and manuscript are solely the responsibility of the authors and do not represent the views of the NIH. The funding source had no involvement in the study design; collection, analysis, or interpretation of data; in the writing of the manuscript; or in the decision to submit the article for publication. The authors have declared no other sources of funding related to this work.
Author information
Authors and Affiliations
Contributions
Ryan DeSanti, Awni Al-Subu, and Pierre Kory contributed to the conception of the study, data acquisition, analysis and interpretation, work drafting and gave final approval of the version to be published. Kara Gill; Jonathan Swanson, Jessica Schmidt, and Eileen Cowan contributed to data acquisition, work drafting and gave final approval of the version to be published. Michael Lasarev contributed to data analysis and interpretation, work drafting and gave final approval of the version to be published. Ryan DeSanti is the guarantor of the paper, had full access to all study data, and takes responsibility for the integrity of the data and accuracy of analysis, from inception to published article.
Corresponding author
Ethics declarations
Conflict of interest
Dr. Al-Subu has a consulting agreement with Edwards Lifesciences LLC. The remaining authors have declared no conflicts of interest related to this work.
Study location, ethical approval, and consent to participate
This study was completed at The American Family Children’s Hospital, University of Wisconsin School of Medicine and Public Health, Madison, Wisconsin, USA. The Institutional Review Board at the University of Wisconsin-Madison approved this study (IRB 2018-071). Signed, informed parent/guardian consent, and assent when appropriate was obtained for participants. The study was registered with ClinicalTrials.gov (NCT03744169).
Consent to publish
All study authors have reviewed the final manuscript and gave approval for the version to be published.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
DeSanti, R.L., Gill, K.G., Swanson, J.O. et al. Comparison of chest radiograph and lung ultrasound in children with acute respiratory failure. J Ultrasound 26, 861–870 (2023). https://doi.org/10.1007/s40477-023-00827-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40477-023-00827-y