
Abstract
Purpose
Verify the acute responses of static stretching (SS) on the rectus femoris (RF), vastus medialis (VM), and vastus lateralis (VL) elasticity and knee/hip range of motion (ROM). Additionally, to investigate if there are consistency among quadriceps muscle elasticity after SS.
Methods
Acute effect of SS on pre-post-intervention design. Thirtheen healthy participants (both genders) proposed for a pre-post experimental design. RF, VM, and VL elasticity (strain ratio, SR) was evaluated bilaterally by ultrasound with quasi-static elastography. Higher SR values refer to more rigid tissues. A SS protocol of 3 series of 30 s was applied at right lower limb. The left lower limb was considered as control group. Also, photogrammetry evaluated the knee/hip ROM.
Results
For SR muscle comparisons, VM was lower (less stiff) than VL and RF at pre- and post-SS. For time comparisons, no differences were observed for SR and ROM at pre- and post-SS. However, the effect size of the quadriceps SR at SS lower limb was higher than control.
Conclusion
Acute effects of SS did not change the quadriceps SR or knee/hip ROM in healthy and active subjects. Non-uniform quadriceps SR are observed (VM < VL and RF) independently of SS. Future studies should consider different protocols, muscles, and populations.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Static stretching (SS) involves the application of a maintained and controlled joint movement up to its maximum range of motion (ROM) [1]. Stress could be promoted by active contraction of the agonist muscles or using external forces. Stretching protocols are often prescribed in sports activity warm-ups and injury prevention [2], rehabilitation programs [3, 4], and indicated to improve patient or athlete performance [5].
ROM is an outcome frequently measured in SS studies [4, 6,7,8] due to its important relationship with muscle function and feasibility of measurement. The mechanisms involved to explain the ROM increase after SS could be associated with an expansion in stretching tolerance [9] and changes in mechanical properties [10]. The evaluation of these properties represents a more objective and specific analysis of these mechanisms.
This way, elastography technique allows the evaluation of the mechanical properties of musculoskeletal tissue [11] in a non-invasive [12] and safe way [13], producing information in real-time. The application of elastography in musculoskeletal tissue has made it possible to identify mechanical alterations in the myotendinous unit, especially in adaptations related to interventions, such as stretching [6, 14, 15]. Furthermore, it allows the regional and individualized evaluation [16], which allows comparisons in specific regions of the same group of muscles.
Some recent studies have shown regional differences in stiffness of hamstrings of athletes [17] and healthy individuals [16] by elastography. It was verified that the greater stiffness in the distal region of the semimembranous muscle remained unchanged after the application of acute SS [16]. Static stretching response in hamstring and plantiflexors are often studied [15, 18,19,20], however, few studies [20, 21] evaluated the quadriceps.
Quadriceps muscle architecture differs regionally which can generate distinct patterns of strength production, ROM, and speed of contraction in each muscle [22]. In addition, the quadriceps is constituted by uni and biarticular muscles that are involved in stretch shortening cycle, such as jumping and running, which makes it susceptible to injuries, especially considering the rectus femoris (RF) [20]. In this way, the understanding of quadriceps mechanical properties and its responses to exercise is clinically relevant.
Like so, the aim of present study was to verify the acute responses of SS on the RF, vastus medialis (VM), and vastus lateralis (VL) elasticity and knee/hip ROM. Additionally, to investigate if there are uniformity among quadriceps muscle elasticity after static stretching protocol. The main hypothesis is that the application of a short duration stretching protocol promotes an increase of muscle elasticity on the stretching side and no effects on the control side.
Methods
We examined the acute effect of SS on pre-post-intervention design.
Participants
Thirteen young, physically active, and healthy individuals (both genders) were included in the study. Those with previous osteoarticular injuries such as trauma, inflammation, autoimmune and oncologic diseases, wounds or immediate postoperative, systemic diseases such as diabetes mellitus, hypertension, heart diseases, and malignant tumors were excluded of this study. The sample was selected in a non-probabilistic way, for convenience. They were asked to refrain from strenuous exercise 24 h before the experiments.
All the individuals who participated in the research read and signed the term of informed consent. The research was approved by the local Ethics and Research Committee on Human Beings (approval number 2.620.2040).
Primary outcome
Elastography
The volunteers answered a questionnaire containing personal information, anthropometric data, and physical activity level. Later, in the orthostatic position, they were guided to maintain the equivalent weight discharge between the members. The thigh length (distance between the greater trochanter and fibula head) was measured with a tape measure and the anterior region of 50% of this length was marked on the skin.
The participants laidy in the supine position and were orientated to keep their lower limbs at rest during the test. RF, VL, and VM were evaluated bilaterally. B-mode and elastographic images were acquired by LOGIQTM Expert ultrasound (S7, Massachusetts, USA), coupled to a linear transducer (6–15 MHz) of 50 mm at an operating frequency of 8 MHz. An experienced ultrasound examiner (9 years) was responsible for all acquisition. A clinical water-based gel layer (RMC, São Paulo, Brazil) was used for the acoustic coupling between the transducer and the tissue.
To acquire the images, the examiner scanned the marked region of the left and right anterior thighs with the transducer placed transversally to the limb. Approximately in the middle region of the cross-sectional area of the RF, VL, and VM muscles, the transducer was repositioned longitudinally to the fibers (Fig. 1). When the fascicles were well visualized in the ultrasound image, the elastographic mode was activated. In this mode, the examiner performed approximately ten cycles of compressions with moderate pressure level, as guided by the pressure feedback shown in the display (Fig. 1). The elastographic images were displayed by a color map within a rectangular area (elastogram) superimposed on the B-mode image (Fig. 1). The color scale varies from red (highest strain or lowest stiffness) to blue (lowest strain or highest stiffness).

Elastographic (upper) and B-mode (bottom) images of the rectus femoris (RF), vastus lateralis (VL) and vastus medialis (VM) muscles. The strain ratio was determined by the ratio of muscle strain (green ROI) by reference tissue strain (fat, yellow ROI). Note that color map varies from the largest strain (red color) to the smallest strain (blue color)
A video of approximately 20 s contained cycles of compressions was recorded to each muscle, totaling six videos per individual. Two circular regions of interest (ROI) of 0.5 and 0.1 cm diameter were selected in the central region of the muscle and fat image, respectively (Fig. 1), by the ultrasound display. A semi-quantitative analysis was performed by the strain ratio (SR), which represents the ratio between the muscle and the reference region (fat) strain. The SR varies from 0.0 to 10.0, which means that higher values refer to more stiff tissues. Data containing all the SR were evaluated on a graph of SR x time exhibited on the ultrasound display and, subsequently, exported in text format.
Photogrammetry
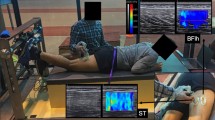
Photogrammetry is a method that presents high intra and interrater reliability (ICC 0.95) for angular measurements [35]. This way, it was applied for verification of knee flexion and hip extension ROM. Six reflex markers were positioned bilaterally, being the knee flexion angle formed by the lateral malleolus, fibula head, and greater trochanter markers, and the hip extension angle formed by the fibula head and greater trochanter markers (Fig. 2).

Photo of a volunteer with reflective markers and self-reported maximum range of motion. A Knee flexion angle and B Hip extension angle
In the orthostatic position, the participant flexed one knee at a time until reaching a sufficient amplitude to promote mild discomfort in the anterior region of the thigh. If knee flexion did not induce slight discomfort, an extension of the hip on the same side was allowed. The abdomen was supported on the wall to control possible trunk compensations. The camera was positioned 1 m from the participant, and two photos were acquired bilaterally before and immediately after the SS program, totaling eight photos per individual. After the acquisitions, the images were transferred to a computer and analyzed through the SAPO posture assessment software (v. 0.69). This software is available for free download at http://pesquisa.ufabc.edu.br/bmclab/sapo/.
Static stretching protocol
Passive static stretching consisted of three series of 30 s with 30 s rest. SS was applied only in the right quadriceps. As the left quadriceps did not receive any stimulus, it was considered a control group. The participant remained in left lateral decubitus with the limb relaxed while the same examiner, responsible for the application in all the volunteers, performed the stretching, supporting one hand on the knee and another stabilizing the pelvis. The border joint amplitude of knee flexion and thigh extension used for muscle stretching was determined by the report of the discomfort of the subject, preceding the pain threshold [7]. The SS protocol was performed between the SR and ROM evaluations. The time interval between the end of SS and the beginning of the post-test was approximately 1 min.
Statistical analysis
The data were analyzed through the Statistical Package for the Social Sciences (SPSS). The normality of the data was verified by the Shapiro–Wilk test. However, although the SR values were classified as nonparametric, the univariate multifactorial analysis of variance (ANOVA) test 2 × 2 × 3 (left and right side; pre and post stretching; RF, VM, and VL muscles) was used due to its robustness in relation to the nonparametric tests [23]. Tukey’s Post Hoc test was applied to verify the muscles that showed significant differences. The t test for dependent samples was used to compare the data obtained by photogrammetry.
In addition, effect size (ES) was calculated accordingly to Cliif (δ) and 95% CI using a tool available online https://www.biorxiv.org/content/10.1101/073999v2.supplementary-material). Cliff's ES (δ) was interpreted as: negligible (< 0.147), small (0.148–0.32), medium (0.33–0.474) and strong (> 0.474) [24]. Photogrammetry and elastography reliability was analyzed among 78 images on the left side only (control) by the intraclass correlation coefficient (ICC), whose values below 0.50 represent low reliability, 0.50 to 0.75 represents moderate reliability, 0.75 to 0.90 indicates good reliability and values equal to or above 0.90 indicate excellent reliability [25]. Also, to detect minimal changes after SS protocol, the standard error of measurement (SEM) and minimal detectable change (MDC) were calculated [26].
Results
The descriptive data of the participants were 26.30 ± 3.40 years; 1.72 ± 0.11 m and 75.50 ± 13.90 kg.
Elastography
For SR muscle comparisons, we observed lower values for VM compared to VL (p = 0.00) and RF (p = 0.01), as we can see in Fig. 3. There was no difference for SR between the VL and RF (p = 0.148).

Box plots of the rectus femoris (RF), vastus lateralis (VL), and vastus medialis (VM) strain ratio in the A left lower limbs (LLL) and B right lower limbs (RLL), at pre- and post-stretching. *p < 0.05 for muscles comparinsons
In addition, there was no difference for the SR values between the pre and post-stretching moments (p > 0.05) in each of the three muscles analyzed. Comparing quadriceps SR in the SS and control sides, right (R) and left (L) respectively, no differences were observed (p > 0.05). There was no interaction (p > 0.05) between the muscle, time and side factors.
Regarding the ES between pre and post-stretching, RF R was 0.76. The ES of the VM R, VL R, RF L, VM L, and VL L were respectively: 0.27; 0.36; 0.28; 0.12, and 0.07.
Considering the reliability, the intra-rater and intra-session ICC values were: 0.77, 0.39, and 0.61 for the RF, VM, and VL muscles, respectively. The SEM and MDC for the left lower limb muscles were: 0.06, and 0.17 (RF), 0.06, and 0.17 (VM), and 0.09, and 0.26 (VL). For the right lower limb were: 0.10 and 0.26 (RF), 0.09, and 0.24 (VM), 0.06, and 0.15 (VL).
Photogrammetry
Photogrammetry analysis indicated that there was no difference for knee flexion and hip extension ROM between left and right sides for the pre- and post-stretching moments (p > 0.05), as shown in Fig. 4.

Box plots for A knee flexion range of motion (ROM) and B hip extension in the left lower limbs (LLL) and right lower limbs (RLL), at pre- and post-stretching
The intra-rater ICC of ROM measurements varied from 0.98 to 0.99 and inter-rater, from 0.94 to 0.99. Regarding ES between pre- and post-stretching, flexion R, flexion L, extension R and extension L were respectively: 0.15; 0.29; 0.08, and 0.11.
Discussion
This study aimed to investigate the acute effects of SS on the mechanical properties of quadriceps and if there are uniform response among quadriceps musculature. Our findings suggest that there is a significant strain difference between RF compared to VM and VL compared to VM in pre-stretching (Fig. 4), which was maintained in post-stretching. No differences were found in the quadriceps strain after stretching when compared to the control side (left limb).
Elastography stands out for allowing a regional and real-time evaluation in the myotendinous unit. Our results show that there is not uniformity at quadriceps strain (not related to SS protocol). Different levels of passive tension were found among VM, RF, and VL muscles during stretching (RF > VM and VL) [20]. The authors explain this finding by the biarticular characteristic of RF whose proximal insertion becomes tensioned in the supine position. The same supine position was adopted in the current study, which could also explain RF and VM differences. However, there was no difference between VL and RF strain, which indicates that other factors also contribute to generating these regional differences. These factors may be associated with the tasks performed by individuals, as level and modality of physical training, frequency of muscle activation in functional activities, specific tension, muscle anisotropy, curvature of aponeuroses, and muscle architecture [27,28,29].
VM muscle showed lower reliability compared to VL and RF. Available data from human cadavers show a similar VM, VL, and RF fascicle length (approximately 70 mm) but with differences in pennation angles (VM = 29.6°, VL = 18.4°, and RF = 13.9°) [30] and cross-sectional areas (VL > VM > RF) [31]. Higher pennation angles could generate higher anisotropy [28] which can make the acquisition more difficult. Moreover, the VM muscle architecture is more complex than the other evaluated muscles because it changes its angulation in more distal regions of insertion.
Acute responses
Understanding the acute effects of traditional SS protocols is important for sports and rehabilitation areas. Many studies have investigated the immediate effect of SS on myotendinous unit stiffness [8, 19, 21, 32]. However, the originality of this study comes from the use of the quasi-static elastography technique to investigate the quadriceps elasticity regionally in physically active subjects after a passive stretching protocol.
Some authors argue that the application of stretching promotes changes in length and stiffness of the muscle tendon unit [6, 15, 33]. However, Caliskan et al. [21] found no significant reduction in RF stiffness after 2 min of SS which corroborates with our study. When SS was applied during a longer time (5 min), RF stiffness reduced its values [21]. The protocol used in the present study (90 s) may have been insufficient to promote changes in the mechanical properties of the quadriceps. Another point, it is that the interval between the application of the stretching protocol and the start of the post-test may have exceeded the time of acute response to stretching, i.e., the strain may have returned to baseline values before the start of the post-test. However, this time was only 1 min, which is less than the duration of acute response described in the literature (approximately 20 min) [32]. Distinct ways of keeping the stress during SS also could influence the results observed because according to Hooke’s Law, elasticity is proportional to stress/strain relation. For example, the joint angle during SS could be maintained by the individual himself [32], while in the present study, by an experienced evaluator.
Although we did not observe a significant difference in SR values at pre- and post-stretching as well as MDC was larger than these differences, the effect size after SS was larger for the elongated side, mainly for RF (0.76). A study with larger samples and different populations may elucidate whether the stretching protocol can change the mechanical properties of the quadriceps.
Range of motion
For ROM assessment, we use the high reliability and reproducibility photogrammetry method [34, 35]. As elasticity analysis, we did not observe knee flexion and hip extension ROM changes post SS comparing to pre SS or control side, which suggests that the joint angle seems to be related to the mechanical properties of the muscle. The ROM effect size at pre- and post-stretching was considered small for both sides, suggesting that the ROM did not change after SS.
In our previous study, we observed that a traditional SS protocol (3 series of 30 s) applied on quadriceps did not modify the the hip extension and knee flexion ROM in young people [7]. The authors justify the fact that they considered in the sample volunteers physically active who used to perform stretching in their daily activities. Future studies should also evaluate different protocols as well as the role of other components such as tendon, fascia, and titin.
Limitations
The present study has some limitations. The sample for this study consisted of recreationally trained subjects which results cannot be straightforwardly transferred to sedentary or elite-athletes. Also, we did not evaluate different site portions within each muscle which could identify intra-regional stretching effects on quadriceps stiffness. We did not measure eletromiography activity to ensure that the muscle was relaxed, but the voluntaries were well orientated to keep the muscle relaxed. Additionally, the “maximal” ROM was based on the own pain threshold of subjects. A dynamometer was not used because we would like to simulate the stretching performed in clinical and sport environments. Also, we did not measure the follow-up of static stretching. However, we conducted a series of reliability and confidence statistical tests to ensure all presented data.
Conclusion
Static stretching applied does not change the quadriceps strain ratio. Non-uniform quadriceps strain ratios (vastus medialis less stiff than vastus lateralis or rectus femoris) were found independently of the stretching protocol applied. Additionally, stretching did not promote a range of motion increase as expected which can be associated with elasticity findings.
References
Behm DG, Blazevich AJ, Kay AD, McHugh M (2016) Acute effects of muscle stretching on physical performance, range of motion, and injury incidence in healthy active individuals: a systematic review. Appl Physiol Nutr Metab 41:1–11
Behm DG, Chaouachi A (2011) A review of the acute effects of static and dynamic stretching on performance. Eur J Appl Physiol 111:2633–2651
Fasen JM et al (2009) A randomized controlled trial of hamstring stretching: comparison of four techniques. J strength Cond Res 23:660–667
Lempke L, Wilkinson R, Murray C, Stanek J (2018) The effectiveness of PNF versus static stretching on increasing hip-flexion range of motion. J Sport Rehabil 27:289–294
Opar DA, Williams MD, Shield AJ (2012) Hamstring strain injuries: factors that lead to injury and re-injury. Sports Med 42:209–226
Akagi R, Takahashi H (2013) Acute effect of static stretching on hardness of the gastrocnemius muscle. Med Sci Sports Exerc 45:1348–1354
Lima KMM, Carneiro SP, Alves DDS, Peixinho CC, de Oliveira LF (2015) Assessment of muscle architecture of the biceps femoris and vastus lateralis by ultrasound after a chronic stretching program. Clin J Sport Med 25:55–60
Zhou J, Liu C, Zhang Z (2019) Non-uniform stiffness within gastrocnemius-achilles tendon complex observed after static stretching. J Sports Sci Med 18:454–461
Magnusson SP et al (1996) Mechanical and physical responses to stretching with and without preisometric contraction in human skeletal muscle. Arch Phys Med Rehabil 77:373–378
Morse CI, Degens H, Seynnes OR, Maganaris CN, Jones DA (2008) The acute effect of stretching on the passive stiffness of the human gastrocnemius muscle tendon unit. J Physiol 586:97–106
Demirel A, Baykara M, Koca TT, Berk E (2018) Ultrasound elastography findings in piriformis muscle syndrome. Indian J Radiol Imaging 28:412–418
DeJong HM et al (2017) The validity and reliability of using ultrasound elastography to measure cutaneous stiffness, a systematic review. Int J Burns Trauma 7:124–141
Li G, Cao Y (2017) Mechanics of ultrasound elastography. Proc Math Phys Eng Sci 473:20160841
Akagi R, Takahashi H (2014) Effect of a 5-week static stretching program on hardness of the gastrocnemius muscle. Scand J Med Sci Sports 24:950–957
Sato S et al (2020) The acute and prolonged effects of 20-s static stretching on muscle strength and shear elastic modulus. PLoS ONE 15:e0228583
Miyamoto N, Kimura N, Hirata K (2020) Non-uniform distribution of passive muscle stiffness within hamstring. Scand J Med Sci Sports 30:1729–1738
Avrillon S et al (2020) Hamstring muscle elasticity differs in specialized high-performance athletes. Scand J Med Sci Sports 30:83–91
Hirata K, Kanehisa H, Miyamoto N (2017) Acute effect of static stretching on passive stiffness of the human gastrocnemius fascicle measured by ultrasound shear wave elastography. Eur J Appl Physiol 117:493–499
Nakao G, Taniguchi K, Katayose M (2018) Acute effect of active and passive static stretching on elastic modulus of the hamstrings. Sport Med Int open 2:E163–E170
Xu J, Hug F, Fu SN (2018) Stiffness of individual quadriceps muscle assessed using ultrasound shear wave elastography during passive stretching. J Sport Heal Sci 7:245–249
Caliskan E et al (2019) Effects of static stretching duration on muscle stiffness and blood flow in the rectus femoris in adolescents. Med Ultrason 21:136–143
Blazevich AJ, Gill ND, Zhou S (2006) Intra- and intermuscular variation in human quadriceps femoris architecture assessed in vivo. J Anat 209:289–310
Blanca MJ, Alarcón R, Arnau J, Bono R, Bendayan R (2017) Non-normal data: is ANOVA still a valid option? Psicothema 29:552–557
Romano J, Kromrey JD, Coraggio J, Skowronek J (2006) Appropriate statistics for ordinal level data : Should we really be using t-test and Cohen’s d for evaluating group differences on the NSSE and other surveys? Florida Assoc Inst Res Annu Meet 13:1–33
Koo TK, Li MY (2016) A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med 15:155–163
Furlan L, Sterr A (2018) The applicability of standard error of measurement and minimal detectable change to motor learning research-a behavioral study. Front Hum Neurosci 12:95
Wiesinger H-P, Rieder F, Kösters A, Müller E, Seynnes OR (2016) Are sport-specific profiles of tendon stiffness and cross-sectional area determined by structural or functional integrity? PLoS ONE 11:e0158441
Lima K, Rouffaud R, Pereira W, Oliveira LF (2019) Supersonic shear imaging elastography in skeletal muscles: relationship between in vivo and synthetic fiber angles and shear modulus. J Ultrasound Med 38:81–90
Noorkoiv M, Stavnsbo A, Aagaard P, Blazevich AJ (2010) In vivo assessment of muscle fascicle length by extended field-of-view ultrasonography. J Appl Physiol 109:1974–1979
Ward SR, Eng CM, Smallwood LH, Lieber RL (2009) Are current measurements of lower extremity muscle architecture accurate? Clin Orthop Relat Res 467:1074–1082
Lieber RL, Bodine-Fowler SC (1993) Skeletal muscle mechanics: implications for rehabilitation. Phys Ther 73:844–856
Taniguchi K, Shinohara M, Nozaki S, Katayose M (2015) Acute decrease in the stiffness of resting muscle belly due to static stretching. Scand J Med Sci Sports 25:32–40
Nakamura M et al (2017) Acute effects of static stretching on the shear elastic moduli of the medial and lateral gastrocnemius muscles in young and elderly women. Musculoskelet Sci Pract 32:98–103
Crasto JA, Sayari AJ, Gray RR, Askari M (2015) Comparative analysis of photograph-based clinical goniometry to standard techniques. Am Assoc Hand Surg 10:248–253
Zonnenberg AJJ, Van Maanen CJ, Elvers JWH, Oostendorp RAB (1996) Intra/Interrater reliability of measurements on body posture photographs. Cranio 14:326–331
Acknowledgements
The authors thank the National Council of Scientific Research (CNPq) Brazil for the provision of scholarships and Research and Innovation Funder (FINEP) for infrastructure. Additionally, Dr. Leticia Martins Raposo for statistics helps.
Funding
Funding not received.
Author information
Authors and Affiliations
Contributions
CHN and IN participated in study design, data analysis, interpretation of results, and writing the manuscript. FD assisted in the writing and critical review of the content. KMML and BMM designed the study and participated in data collection, writing and coordination of the manuscript. All authors have read and approved the final version of the manuscript, and agree with the order of presentation of the authors.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Nonnenmacher, C.H., Nunes, I., de Moura, B.M. et al. Does static stretching change uniformly the quadriceps elasticity in physically actives subjects?. J Ultrasound 25, 915–921 (2022). https://doi.org/10.1007/s40477-021-00649-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40477-021-00649-w