
Abstract
Purpose of Review
This review summarizes findings from quantitative research studies published between 2010 and 2022 providing insight on sociodemographic differences and disparities in ageism among US adults ages 50 and older.
Recent Findings
Across 21 studies, disparities in ageism were more consistently found such that those who were older (57% of studies), with less education (64%), and of lower socioeconomic status (100%) reported more ageism than their counterparts. Amount of ageism did not differ by sex in the majority (71%) of studies. Findings regarding race/ethnicity were mixed. Other possible differences in ageism, assessed in a small number of studies, were patterned by employment characteristics, geographic residence, religiosity, and political affiliation but not by marital or employment status.
Summary
Given that ageism is both common and associated with poor health outcomes, identifying disproportionately affected segments of the older adult population is a necessary prerequisite for developing targeted interventions to reduce negative outcomes linked to ageism and associated health disparities. Evidence within this review suggests that the patterning of ageism may deviate from that typically documented for other social and structural disadvantages. Some groups traditionally considered to be socially marginalized were found to report more ageism while others did not.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Ageism targeting older adults may be the most common and socially acceptable form of discrimination in the USA [1, 2••, 3, 4]. Estimates suggest that between 77 and 93% of older adults report experiences with ageism [2••, 5]. Ageism is defined as discrimination, prejudice, and narrow stereotypes related to aging processes, old age, and older adults [6]. While inextricably linked to chronological age and biological aging processes, ageism is a socially constructed phenomenon rooted in dominant beliefs, attitudes, and expectations about life at different ages and stages within the life course. While people of any age may be discriminated against because of their age, older adults are believed to be more negatively affected by ageism because they are systematically disempowered, devalued, and excluded across multiple life domains [7]. While definitions of “older adults” vary, age discrimination is commonly reported among those ages 50 and older [8] and is most often identified as beginning when people are in their 50s [9].
Ageism is deeply entrenched in contemporary society. It is embedded in major life events, such as being forced out of the workforce or one’s home primarily due to factors related to age [10–12]. It can also be present in routine aspects of older adults’ day-to-day lives, which is referred to as everyday ageism [2••, 13•]. Ageism manifests and affects the lives of older adults in a variety of ways: commonplace beliefs and prejudices about aging and older adults; the ubiquity of social and environmental cues reinforcing these messages; internalization of ageist stereotypes; older adults’ concerns about how ageism may shape others’ judgements and behaviors; the ways in which all of these affect older adults’ health and heath behaviors; and being the target of age-based discrimination in interpersonal interactions, institutions, and policies [14–16].
Although the literature is relatively scant, several systematic reviews have found consistent associations between ageism and health [7, 17, 18]. Linkages between ageism and health have been less frequently investigated when compared to the potential health ramifications of other types of discrimination [1]. For example, a PubMed keyword search of literature published since 2000 generated 5.5 times as many articles on racism than ageism and twice as many articles on sexism. Health outcomes that have been linked to ageism include poor mental health and lower overall well-being, impairments in physical and cognitive functioning, a variety of medical conditions and diseases, and premature mortality [7, 17, 18]. While it is probable that relationships between ageism and health are reciprocal, both theoretical [1, 14–16] and empirical [19, 20] research suggest that the effect of ageism on health is more substantial than the converse.
One important but understudied characteristic of ageism is that, like other social and structural disadvantages, it likely affects some segments of the population more than others. Some groups of older adults are posited to experience ageism at higher rates, more frequent and severe forms, and to be at increased risk for adverse health outcomes linked to ageism. In the USA, social, economic, and political disadvantages with implications for health are generally patterned such that they are disproportionately experienced by socially marginalized groups. Commonly identified marginalized sociodemographic groups include women, racial and ethnic minorities, those with less formal education and lower socioeconomic status, and older adults. Other sociodemographic characteristics less consistently associated with disadvantage include marital status, family and household composition, geographic location, religion, and political affiliation. Further, sociodemographic characteristics intersect to differentially shape the lived experiences, advantages, disadvantages, and health outcomes of groups within our population. For example, older African American women may be multiply marginalized, such that they experience ageism, racism, sexism, but also distinct discrimination related to the intersection of these characteristics (e.g., gendered ageism) [21].
This review article seeks to summarize the findings of recent research providing insight on sociodemographic differences and disparities in ageism among US adults ages 50 and older. In this paper we use the terms differences and disparities to emphasize that differences refer to things that distinguish one group from another, while disparities refer to the persistent, inequitably distribution of disadvantages that disproportionately harm the health and well-being of socially marginalized groups. Given the premise that ageism is a disadvantage that is unlikely to be experienced equally by all older adults, combined with its prevalence and the growing body of evidence implicating ageism in adverse health and other outcomes, identifying groups at increased risk for experiencing ageism and associated harms can inform strategies to promote older adult health. Further, identifying differences and disparities in ageism may advance our understanding and potential for intervening upon mechanisms generating the persistent health disparities documented within the older adult population [22]. Since it has not yet been clearly established which sociodemographic groups experience ageism more than others, this study addresses this gap in the literature.
Methods
We conducted a review of literature on sociodemographic differences and disparities in ageism among older US adults. For the current study, differences and disparities in ageism were conceptualized as including sociodemographic differences in (1) amount of ageism experienced and (2) relationships between ageism and health (e.g., moderation analyses indicating that some sociodemographic groups may be more vulnerable to outcomes associated with ageism than others). In line with the limited research on this topic to date, this study emphasizes general patterns of sociodemographic group differences in ageism including identification of the presence/absence of differences and disproportionately affected groups. It does not seek to quantify the magnitude of sociodemographic differences in ageism.
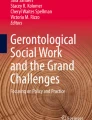
A multiphase, systematic process was used to identify relevant publications between June and August 2022 for inclusion. Figure 1 shows the study search flowchart. The article search occurred in three phases. First, the PubMed database was used to identify published articles assigned the Medical Subject Heading (MESH) term of “ageism” published between 2010 and 2022 in English. This search was further refined by excluding articles assigned MESH terms denoting various age groups (e.g., adolescents), geographic regions (e.g., Germany), and article types (e.g., qualitative research, review, and meta-analysis) not relevant to the current study. Next, keywords related to ageism were used to identify PubMed articles overlooked in the first search phase. Relevant articles may not have been assigned the “ageism” MESH term, either because their subject or terminology diverged from the criteria used for the “ageism” MESH term or because they were not assigned any MESH terms, which is the case for approximately 9% of PubMed articles including newly indexed papers. Key words used were ageism, ageist, age discrimination, self-perceptions of aging, age prejudice, age stereotypes, age identity, and unequal aging, which were applied in conjunction with the same constraints and exclusions used the first search. Finally, additional articles were identified through manual searches of relevant bibliographies.

Flowchart of literature search and screening. Search criteria: quantitative studies published in English between 2010 and 2022 providing insight on sociodemographic differences and disparities in ageism among US adults ages 50 + . Database searches were conducted in PubMed with the “ageism” MESH term and keywords of ageism, ageist, age discrimination, self-perceptions of aging, age prejudice, age stereotypes, age identity, and unequal aging
The list of articles identified for inclusion in the study was narrowed down through two screening phases. In the preliminary screening phase, article titles, abstracts, and easily accessible full-text articles were evaluated for potential inclusion based on the study eligibility criteria. Article eligibility criteria were (1) published in English; (2) published since 2010; (3) empirical studies utilizing quantitative methods; (4) studies with older adult samples, defined as exclusively or predominantly (> 50%) adults ages 50 years and older, or in which data were provided so as to allow for analysis exclusively among older adults; (5) sample sizes of ≥ 30 older adults; (6) studies with exclusively or predominantly US samples; and (7) comparison of the amount of ageism and/or nature of the relationship between ageism and health for two or more groups differentiated by sociodemographic characteristic (e.g., age or age group, sex, race, ethnicity, marital status, family and household characteristics, education, income, employment status, place of residence, migration background, language, religion, political affiliation, sexual orientation, and/or gender identity). Articles incompatible with these criteria were excluded immediately. Articles consistent with these criteria or for which it was indeterminate were retained. Full-text versions were obtained of all remaining articles, which were comprehensively screened for eligibility. The most common reasons for excluding articles during the second phase of screening were non-US sample and/or absence of a comparison of ageism by sociodemographic characteristic.
For each article, we abstracted information on the data source, study design, sampling methods, sample characteristics, ageism measure(s) used and types assessed, groups compared (e.g., sociodemographic characteristic(s) serving as a basis for comparison), and a summary of relevant findings. When possible, we included information missing from the articles that was obtained from the authors via email. In most cases, we relied on author-reported statistical test results. When statistical comparisons of interest to the review were not reported and sufficient data were available, we assessed group-based statistical differences ourselves. For the purpose of this review, the threshold for statistical significance was set at p < 0.05 for all analyses. Given the limited research conducted on this topic to date, we did not evaluate study quality or assess potential publication bias but instead summarized key findings.
Results
Characteristics of Included Studies
Twenty-one articles met the criteria for inclusion in this review. The list of included studies and their characteristics are reported in Table 1. Ten studies analyzed data from large social and health research datasets, and most of these utilized dataset-specific recommended techniques for generating estimates that were nationally representative of older adults living in the USA. Six studies used the Health and Retirement Study (HRS), and two used data from the National Poll on Healthy Aging (NPHA), resulting in duplicate participants across studies. One study each used data from the Panel Study of Income Dynamics (PSID) and the Midlife in the US (MIDUS) study. Eleven studies analyzed data collected from different convenience samples. The majority of included studies (18) were observational survey studies in which participants self-reported their experiences with ageism. The Chopik and Giasson [23•] study included both an experimental component and self-report on ageism survey items. The study by Smith and colleagues [24••] was solely experimental, and the Wilson and Roscigno [25••] study used records of occupational trends as a proxy for workplace ageism.
Study sample sizes ranged from 101 to 61,732, with nine relatively small samples comprised 100–400 participants, seven moderate-sized samples of approximately 1000–2000, and five large samples exceeding 4000. The mean sample size was 4940 and median was 1416. Nineteen studies included exclusively older adults (ages ≥ 50). Of these, the majority used approximately age 50 as the lower limit of the age range, though the youngest participants in five studies were in their 60s. Study upper age limits varied, with some sample ages spanning 10 years and others > 50 years and including adults over age 100. Across studies, the mean participant age was 66.3, unweighted, or 61.3, weighted by sample size.
Assessment of Ageism
Included studies assessed older adults’ experiences with and internalization of ageism using a variety of self-report survey scales and items, some of which are widely used and psychometrically validated [26], and some of which were novel [2••, 13•] or ageism-specific modifications to existing instruments [27•]; a minority of studies used experimental protocols or proxy measures in lieu of [24••, 25••] or in combination with [23•] survey scales (Table 1). The most frequently used ageism measures were Healthcare Stereotype Threat attributed to age [28•] (3 studies), the Attitude Toward Own Aging subscale from the Philadelphia Geriatric Center Morale Scale [29] (3 studies), the Everyday Discrimination Scale attributed to age [26] (3 studies), and the Everyday Ageism Scale (2 studies) [13•]. Four studies measured ageism with multiple scales and/or strategies. Across studies, amount of ageism was operationalized as either a binary variable indicating any ageism (yes/no) or continuously with scales capturing some combination of ageism frequency, severity, and/or different examples experienced.
Types of ageism assessed in included studies were classified in four categories: age stereotypes, internalized ageism, concern about ageist stereotypes/discrimination, and age discrimination. Age stereotypes refer to general beliefs, stereotypes, and prejudices related to old age, aging processes, and older adults that participants encounter and were assessed in three studies. Internalized ageism refers to when older adults believe ageist stereotypes, themselves, and was assessed in 11 studies. Concern about ageist stereotypes/discrimination includes scales tapping into concern and anxiety about how other people’s ageist assumptions and stereotypes may shape those people’s perceptions, judgment, or behavior when interacting with older adults such as themselves and was assessed in five studies. Age discrimination refers to a self-report of discrimination due to age or age in combination with other reasons and was assessed in nine studies.
Differences and Disparities in Ageism
Of the 21 included studies, five articulated study objectives of identifying sociodemographic differences in amounts of ageism [2••, 23•, 25••, 30••, 31••], and two articulated objectives of identifying whether sociodemographic characteristics moderated associations between ageism and health outcomes [24••, 32•] (Table 1). For the remaining studies, we extracted insight on sociodemographic differences in ageism provided as part of background or supplementary information generated in the pursuit of other objectives.
Included studies assessed differences and disparities in ageism experienced by older adults by the sociodemographic characteristics of age, sex, race/ethnicity, marital status, household composition, education, finances, employment, geography, religion, and political affiliation (Tables 1 and 2). All reported differences were statistically significant with p < 0.05, unless indicated otherwise. Information about differences in ageism by age, sex, race/ethnicity, and education was provided in more than half the studies. Other sociodemographic differences were less frequently assessed.
Disparities in ageism were most consistently reported by education and chronological age. More ageism was associated with lower levels of education in 64% of the 11 studies assessing this characteristic and older age in 57% of 14 studies. A mix of small, moderate, and large studies reported differences in ageism by education and age, while small studies with less statistical power to detect group-based differences were overrepresented among studies reporting no differences.
Findings regarding ageism differences by race/ethnicity were mixed. Of the 12 studies assessing differences by race and/or ethnicity, 42% reported more ageism among racial/ethnic minority groups. Seventeen percent reported more ageism among majority groups, and 75% reported no racial/ethnic differences at all or for some pairwise comparisons. There was not a clear pattern of findings regarding race/ethnicity related to study sample size.
Sex differences were absent in 71% of the 14 studies with relevant information. Studies reflecting a range of sample sizes reported no sex differences.
Socioeconomic status was assessed in four studies. Low socioeconomic status was associated with more ageism without exception. Differences in ageism by employment status were mixed, with no difference in 3 out of 5 studies. Experiences with ageism differed by some, but not all, other employment characteristics examined.
Findings from the few studies examining ageism differences by other sociodemographic characteristics suggested possible differences such that more ageism may be reported by those living in rural areas, in the Midwest, with lower religiosity, and who identify politically as Republican and Independent. Ageism was not found to consistently differ by marital status or household composition.
Discussion
This narrative review adds to the scant literature on sociodemographic differences and disparities in ageism among contemporary US adults ages 50 and older. Findings indicated that ageism is not experienced equally by all older adults. Rather, it disproportionately affects some groups and potentially puts them at increased risk for negative health and other outcomes associated with ageism. We found differences in ageism within the older adult population that generally mapped onto chronological age, which was anticipated given that age is a fundamental element embedded in the conceptualization and expressions of ageism in society. We also found that amount of ageism experienced also differed by other sociodemographic characteristics that are not directly related to the definition of ageism, such as education and socioeconomic status. Findings add to the evidence in support of an intersectional approach to examining social determinants of health; in that, certain segments within the population are multiply marginalized [21]. Collectively, findings suggest that the patterning of ageism may deviate somewhat from the typical patterning of social and structural disadvantages, which are disproportionately experienced by members of socially marginalized groups. Some socially marginalized groups were generally found to report more ageism (older, less educated, and lower socioeconomic status) while others did not (racial/ethnic minorities, women, not employed).
There are several possible explanations for why we documented trends in the published literature suggesting that ageism may be more commonly experienced by groups with less education and lower socioeconomic status. Groups with more education and wealth may have more knowledge, financial resources, and other advantages at their disposal to disguise appearance-related indicators of aging, cope with aging-related physical changes, and support healthy aging. As a result, these groups may have fewer negative experiences of aging, including both ageism in interpersonal interactions and reinforcement of internalized ageist beliefs and attitudes. These may result in lower report of ageism. In addition, these same advantages may enable some older adults with more education and wealth, particularly those at the younger end of the older adult age range, to not self-identify as older adults and not find ageist beliefs and stereotypes self-relevant [33–35]. These individuals may report lower levels of ageism either because they do not experience it or because they do not attribute age-based discrimination they experience to their age. Alternatively, or perhaps in combination, older adults with less education and lower socioeconomic status may be more likely to look and/or act stereotypically older. This may result in them experiencing more ageism in interpersonal interactions, since appearance is an important determinant of others’ perceptions of age. Older adults with lower education levels and socioeconomic status are more likely to experience harsher living and working conditions, have greater exposure to chronic sources of stress, and engage in unhealthy behaviors such as smoking across the life course, all of which contribute to premature aging in appearance and physical deterioration.
The mixed findings regarding differences in ageism by race/ethnicity were unanticipated. Numerous social and structural disadvantages, (e.g., other forms of discrimination, residence in resource-poor communities, poverty, poor access to quality healthcare) are patterned by race in the USA. Racial and ethnic minority groups experience more disadvantages of many kinds and greater social marginalization when compared to their non-Hispanic White counterparts, who benefit from affiliation with the dominant racial/ethnic group possessing disproportionate political, economic, and social advantages [36]. For this reason, we had anticipated that ageism, as an example of a socially constructed disadvantage, would also be more commonly experienced by racial and ethnic minority groups. It is plausible that the mixed findings reflected methodological issues across and within studies. The racial and ethnic categories used in the included studies were inconsistent, which made summarizing and synthesizing findings across studies challenging. In addition, many studies combined the data of distinct racial and ethnic groups together for analysis (e.g., non-White and Other categories). This approach inhibited detection of potential differences between those groups and may have biased the results of the racial/ethnic group comparisons that were conducted, particularly increasing the risk that differences in ageism were underestimated or concealed. Indicative of this, the two studies that included comparisons between more than three racial/ethnic groups [2••, 31••] reported that among those racial and ethnic minority groups often grouped together in other studies, some reported more ageism (Asian American and Hispanic) while others reported less (Black).
Alternatively, the mixed findings for race/ethnicity, as well as the general absence of differences in ageism by sex, may be due to variations in how different racial and ethnic groups and men and women respond to ageism survey items (the predominant strategy for collecting ageism data in included studies), perceive ageism, and/or experience ageism. For example, stigmatized groups have been shown to avoid acknowledging and reporting discrimination; researchers argue that this may be motivated by internal factors, such as preserving self-esteem and perceived control, or external reasons, such as avoiding associated social costs [37]. Alternatively, people that have experienced racism and/or sexism throughout life may be more habituated to discrimination or more likely to attribute discrimination to their race/ethnicity or sex rather than their age [2••]. Either of these circumstances would cause racial and ethnic minorities and women to underestimate self-reported experiences with ageism. Finally, experiences of ageism may be qualitatively different for members of different racial/ethnic groups and/or for men and women. Researchers have explored the notion of gendered ageism [21, 38], with a particular emphasis on how age and gender ideologies intersect to uniquely influence older women’s experiences and social status. Women experience more ageism related to their appearance than men [21] and may be more likely to internalize ageist beliefs and values related to youthful beauty given lifelong socialization and social rewards linked to female appearance. Men, on the other hand, may be more affected by ageism when their capacity to perform key social and cultural roles is insulted, restricted, or altered, as role fulfillment has been identified as a central tenet of males’ identities [39].
Recent systematic reviews of ageism research [17, 40] have identified several issues that may account, in part, for the modest number and quality of studies providing insight on the patterning of ageism within the older adult population. These include a lack of consensus on the best way to measure ageism and a dearth of high quality, validated measures that capture the many different types of ageism that older adults may experience. Consistent with this, documenting sociodemographic differences and disparities in ageism was not an identified research objective for the majority of the studies included in this review. These conditions made quantifying the magnitude of group-based differences in ageism across studies problematic. Therefore, we elected focus on the qualitative nature of group-based differences (e.g., presence/absence and direction of sociodemographic differences), which were posited to be more consistently detected across studies with diverse designs, measurement instruments, and objectives. Given the limited research in this area, we also opted to evaluate literature published over a longer timeframe (2010–2022) than what is typically used in review articles covering timely topics. While this means that our review covered a time period during which practices, policies, and awareness of ageism have changed, it provides a larger literature upon which to generate robust findings. This timeframe also coincided with an increase in the amount of published ageism research in PubMed beginning in 2010 and continuing to today.
Implications for Intervention and Future Research
This review summarizes current research knowledge on differences and disparities in ageism within the older US adult population, which is a necessary prerequisite for developing targeted interventions to reduce ageism for those most affected. Further, given that ageism is both common and associated with a variety of negative health outcomes, efforts to combat ageism focused on sociodemographic groups identified as disproportionately affected have potential to both improve health and diminish health disparities within the older adult population. Rigorous, population-level research is needed to confirm the general findings produced in this review and quantify the magnitude of sociodemographic differences in ageism. This would benefit from attention to several issues hindering current research identified in this review including the lack of investigating group-based differences in ageism as a research objective; absence of widely used, validated, comprehensive ageism survey instruments; and need for consistent and distinct sociodemographic categories (especially for race and ethnicity). Other strategies that could be advantageous for building on this line of research include longitudinal study designs for further investigation of causality, methodology for investigating the consequences of sociocultural and structurally embedded ageism, research assessing the generalizability of mechanisms linking ageism and health identified in experimental research, and studies investigating whether objective indicators of ageism match self-report.
Limitations
First, despite our systematic and extensive process, we may have overlooked relevant articles. We also did not review research reported in books or the grey literature. Second, given the few studies that adopted examining sociodemographic differences and disparities in ageism as an objective, the nature of data provided by some studies incorporated into this review is subject to critique. We also did not perform study quality assessments, weight findings by study sample size, or conduct a meta-analysis, as these activities are premature given the current state of the literature. Finally, the majority of included studies used measures of self-reported ageism that may be affected by social desirability, inaccurate recall, and other factors, thereby resulting in biased estimates of ageism. If self-report biases differentially affect some sociodemographic groups more than others, this could prevent accurate detection of differences.
Conclusions
The presence of sociodemographic differences and disparities in ageism across studies included in this narrative review support the growing body of evidence that disadvantages are unevenly distributed within society. This review found suggestive evidence of disparities in ageism within the older US adult population patterned by age, education, and socioeconomic status; mixed findings related to race and ethnicity; and no differences in ageism by sex. It also identified other potential associations between sociodemographic characteristics and ageism warranting further study.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Allen JO. Ageism as a risk factor for chronic disease. Gerontologist. 2016. https://doi.org/10.1093/geront/gnu158.
Allen JO, Solway E, Kirch M, Singer D, Kullgren JT, Moïse V, Malani PN. Experiences of everyday ageism and the health of older US adults. JAMA Netw Open. 2022. https://doi.org/10.1001/jamanetworkopen.2022.17240.
Angus J, Reeve P. Ageism: a threat to “aging well” in the 21st century. J Appl Gerontol. 2006. https://doi.org/10.1177/0733464805285745.
Hagestad GO, Uhlenberg P. The social separation of old and young: a root of ageism. J Soc Issues. 2005. https://doi.org/10.1111/j.1540-4560.2005.00409.x.
Wilson DM, Errasti-Ibarrondo B, Low G. Where are we now in relation to determining the prevalence of ageism in this era of escalating population ageing? Ageing Res Rev. 2019. https://doi.org/10.1016/j.arr.2019.03.001.
Butler RN. Ageism: another form of bigotry. Gerontologist. 1969. https://doi.org/10.1093/geront/9.4_Part_1.243.
Chang ES, Kannoth S, Levy S, Wang SY, Lee JE, Levy BR. Global reach of ageism on older persons’ health: a systematic review. PLoS ONE. 2020. https://doi.org/10.1371/journal.pone.0220857.
Allen JO, Solway E, Kirch M, Singer D, Kullgren J, Malani P. Everyday ageism and health. University of Michigan National Poll on Healthy Aging. 2020. https://www.healthyagingpoll.org/report/everyday-ageism-and-health.
Perron R. The value of experience: age discrimination against older workers persists. AARP Research. 2018. https://doi.org/10.26419/res.00177.002.
Abecassis M, Bridges ND, Clancy CJ, Dew MA, Eldadah B, Englesbe MJ, Flessner MF, Frank JC, Friedewald J, Gill J, Gries C, Halter JB, Hartmann EL, Hazzard WR, Horne FM, Hosenpud J, Jacobson P, Kasiske BL, Lake J, Loomba R, Malani PN, Moore TM, Murray A, Nguyen M-H, Powe NR, Reese PP, Reynolds H, Samaniego MD, Schmader KE, Segev DL, Shah AS, Singer LG, Sosa JA, Stewart ZA, Tan JC, Williams WW, Zaas DW, High KP. Solid-organ transplantation in older adults: current status and future research. Am J Transplant. 2012. https://doi.org/10.1111/j.1600-6143.2012.04245.x.
Bender KA. An analysis of well-being in retirement: the role of pensions, health, and ‘voluntariness’ of retirement. J Socio Econ. 2012. https://doi.org/10.1016/j.socec.2011.05.010.
Kydd A, Fleming A. Ageism and age discrimination in health care: fact or fiction? A narrative review of the literature. Maturitas. 2015. https://doi.org/10.1016/j.maturitas.2015.05.002.
Allen JO, Solway E, Kirch M, Singer D, Kullgren JT, Malani PN. The everyday ageism scale: development and evaluation. J Aging Health. 2022. https://doi.org/10.1177/08982643211036131.
Iversen TN, Larsen L, Solem PE. A conceptual analysis of ageism. Nordic Psychol. 2009. https://doi.org/10.1027/1901-2276.61.3.4.
Levy B. Stereotype embodiment. Curr Dir Psychol Sci. 2009. https://doi.org/10.1111/j.1467-8721.2009.01662.x.
Swift HJ, Abrams D, Lamont RA, Drury L. The risks of ageism model: how ageism and negative attitudes toward age can be a barrier to active aging. Soc Issues Policy Rev. 2017. https://doi.org/10.1111/sipr.12031.
Hu RX, Luo M, Zhang A, Li LW. Associations of ageism and health: a systematic review of quantitative Observational study studies. Res Aging. 2021. https://doi.org/10.1177/0164027520980130.
Warmoth K, Tarrant M, Abraham C, Lang IA. Older adults’ perceptions of ageing and their health and functioning: a systematic review of observational study studies. Psychol Health Med. 2016; https://doi.org/10.1080/13548506.2015.1096946
Levy BR, Banaji MR. Implicit ageism. In: Nelson T, editor. Ageism: Stereotyping and Prejudice Against Older Persons. Cambridge, MA: MIT Press; 2002. 49–75. https://doi.org/10.7551/mitpress/1157.001.0001.
Sargent-Cox KA, Anstey KJ, Luszcz MA. The relationship between change in self-perceptions of aging and physical functioning in older adults. Psychol Aging. 2012. https://doi.org/10.1037/a0027578.
Krekula C, Nikander P, Wilińska M. Multiple marginalizations based on age: gendered ageism and beyond. In: Ayalon L, Tesch-Romer C, editors. Contemporary Perspectives on Ageism. Cham, Switzerland: Springer; 2018. 33–50. https://doi.org/10.1007/978-3-319-73820-8.
Herd P, Robert SA, House JS. Health disparities among older adults: life course influences and policy solutions. In: Binstock RH, George LK, editors. Handbook of Aging and the Social Sciences. Amsterdam: Academic Press; 2011. 121–134. https://doi.org/10.1016/B978-0-12-380880-6.00009-5.
Chopik WJ, Giasson HL. Age differences in explicit and implicit age attitudes across the life span. Gerontologist. 2017. https://doi.org/10.1093/geront/gnx058.
Smith AM, Gallo DA, Barber SJ, Maddox KB, Thomas AK. Stereotypes, warnings, and identity-related variables influence older adults’ susceptibility to associative false memory errors. Gerontologist. 2017. https://doi.org/10.1093/geront/gnx057.
Wilson G, Roscigno VJ. Race, ageism and the slide from privileged occupations. Soc Sci Res. 2018. https://doi.org/10.1016/j.ssresearch.2017.09.009.
Williams DR, Yan Y, Jackson JS, Anderson NB. Racial differences in physical and mental health: socio-economic status, stress and discrimination. J Health Psychol. 1997. https://doi.org/10.1177/135910539700200305.
Sabik NJ. Ageism and body esteem: associations with psychological well-being among late middle-aged African American and European American women. J Gerontol B Sci Soc Sci. 2015. https://doi.org/10.1093/geronb/gbt080.
Abdou CM, Fingerhut AW, Jackson JS, Wheaton F. Healthcare stereotype threat in older adults in the Health and Retirement Study. Am J Prev Med. 2016. https://doi.org/10.1016/j.amepre.2015.07.034.
Lawton MP. The Philadelphia geriatric center morale scale: a revision. J Gerontol. 1975. https://doi.org/10.1093/geronj/30.1.85.
Giasson HL, Queen TL, Larkina M, Smith J. Age group differences in perceived age discrimination: associations with self-perceptions of aging. Gerontologist. 2017. https://doi.org/10.1093/geront/gnx070.
Menkin JA, Guan SS, Araiza D, Reyes CE, Trejo L, Choi SE, Willis P, Kotick J, Jimenez E, Ma S, McCreath HE. Racial/ethnic differences in expectations regarding aging among older adults. Gerontologist. 2017. https://doi.org/10.1093/geront/gnx078.
Syme ML, Cohn TJ. Aging sexual stereotypes and sexual expression in mid-and later life: examining the stereotype matching effect. Aging Ment Health. 2021; https://doi.org/10.1080/13607863.2020.1758909.
Calasanti T. Ageism, gravity, and gender: experiences of aging bodies. Generations. 2005;29(3):8–12.
Chonody JM, Teater B. Why do I dread looking old? A test of social identity theory, terror management theory, and the double standard of aging. J Women Aging. 2015. https://doi.org/10.1080/08952841.2014.950533.
Fishman JR, Settersten RA, Flatt MA. In the vanguard of biomedicine? The curious and contradictory case of anti-aging medicine. Sociol Health Illn. 2010. https://doi.org/10.1111/j.1467-9566.2009.01212.x.
Geronimus AT, Thompson JP. To denigrate, ignore, or disrupt: racial inequality in health and the impact of a policy-induced breakdown of African American communities. Du Bois Rev. 2004. https://doi.org/10.1017/S1742058X04042031.
Kaiser CR, Miller CT. Stop complaining! The social costs of making attributions to discrimination. Pers Soc Psychol Bull. 2001. https://doi.org/10.1177/0146167201272010.
Itzin C, Phillipson C. Gendered ageism: a double jeopardy for women in organizations. In: Gender Culture, Change Organizational, editors. Itzin C, Phillipson C. Putting Theory into Practice. London: Routledge; 1995. p. 84–94.
Griffith DM, Gunter K, Allen JO. Male gender role strain as a barrier to African American men’s physical activity. Health Educ Behav. 2011. https://doi.org/10.1177/1090198110383660.
Ayalon L, Dolberg P, Mikulioniene S, Perek-Białas J, Rapoliene G, Stypinska J, Willinska M, de la Fuente-Nunez V. A systematic review of existing ageism scales. Ageing Res Rev. 2019. https://doi.org/10.1016/j.arr.2019.100919.
Choi EY, Kim Y, Chipalo E, Lee HY. Does perceived ageism widen the digital divide? And does it vary by gender? Gerontologist. 2020. https://doi.org/10.1093/geront/gnaa066.
Greenwald AG, Banaji MR, Rudman LA, Farnham SD, Nosek BA, Mellott DS. A unified theory of implicit attitudes, stereotypes, self-esteem, and self-concept. Psychol Rev. 2002. https://doi.org/10.1037/0033-295X.109.1.3.
Nosek BA, Banaji M, Greenwald AG. Harvesting implicit group attitudes and beliefs from a demonstration web site. Group Dyn. 2002. https://doi.org/10.1037/1089-2699.6.1.101.
Halpin SN, Dillard RL, Idler E, Clevenger C, Rothschild E, Blanton S, Wilson J, Flacker JM. The benefits of being a senior mentor: cultivating resilience through the mentorship of health professions students. Gerontol Geriatr Educ. 2017; https://doi.org/10.1080/02701960.2015.1079707.
Kang SK, Chasteen AL. The development and validation of the age-based rejection sensitivity questionnaire. Gerontologist. 2009. https://doi.org/10.1093/geront/gnp035.
Hooker K, Mejía ST, Phibbs S, Tan EJ, Stevens J. Effects of age discrimination on self-perceptions of aging and cancer risk behaviors. Gerontologist. 2019. https://doi.org/10.1093/geront/gny183.
Maxfield M, Peckham A, Guest MA, Pituch KA. Age-based healthcare stereotype threat during the COVID-19 pandemic. J Gerontol Soc Work. 2021; https://doi.org/10.1080/01634372.2021.1904080
McConatha JT, Kumar VK, Magnarelli J. Ageism, Job engagement, negative stereotypes, intergenerational climate, and life satisfaction among middle-aged and older employees in a university setting. Int J Environ Res Public Health. 2022. https://doi.org/10.3390/ijerph19137554.
Marchiondo LA, Gonzales E, Ran S. Development and validation of the workplace age discrimination scale. J Bus Psychol. 2016. https://doi.org/10.1007/s10869-015-9425-6.
King SP, Bryant FB. The Workplace Intergenerational Climate Scale (WICS): a self-report instrument measuring ageism in the workplace. J Organ Behav. 2017. https://doi.org/10.1002/job.2118.
Bal PM, De Lange AH, Van Der Heijden B, Zacher H, Oderkerk FA, Otten S. Young at heart, old at work? Relations between age, (meta) stereotypes, self-categorization, and retirement attitudes. J Vocat Behav. 2015. https://doi.org/10.1016/j.jvb.2015.09.002.
Sarkisian CA, Prohaska TR, Wong MD, Hirsch S, Mangione CM. The relationship between expectations for aging and physical activity among older adults. J Gen Int Med. 2005. https://doi.org/10.1111/j.1525-1497.2005.0204.x.
Phibbs S, Hooker K. An exploration of factors associated with ageist stereotype threat in a medical setting. J Gerontol B Sci Soc Sci. 2018. https://doi.org/10.1093/geronb/gbx034.
Steward A, Hasche L. Exploring lifestyle activities to reduce internalized ageism: self-efficacy as a mediator between exercise, volunteering, computer use, and self-perceptions of aging. Int J Aging Hum Dev. 2022. https://doi.org/10.1177/00914150211024175.
Kotter-Grühn D, Kleinspehn-Ammerlahn A, Gerstorf D, Smith J. Self-perceptions of aging predict mortality and change with approaching death: 16-year longitudinal results from the Berlin Aging Study. Psychol Aging. 2009. https://doi.org/10.1037/a0016510.
Steward AT, Hasche L, Laser JA. Do internalized age stereotypes mediate the relationship between volunteering and social connectedness for adults 50+? J Aging Stud. 2022. https://doi.org/10.1016/j.jaging.2022.101031.
Fernandez-Ballesteros R, Olmos R, Santacreu M, Bustillos A, Schettini R, Huici C, Rivera JM. Assessing aging stereotypes: personal stereotypes, self-stereotypes and self-perception of aging. Psicothema. 2017. https://doi.org/10.7334/psicothema2016.314.
White CB. A scale for the assessment of attitudes and knowledge regarding sexuality in the aged. Arch Sex Behav. 1982. https://doi.org/10.1007/BF01542474.
Templeton K, Nilsen KM, Walling A. Issues faced by senior women physicians: a national survey. J Womens Health. 2020. https://doi.org/10.1089/jwh.2019.7910.
Vale MT, Stanley JT, Houston ML, Villalba AA, Turner JR. Ageism and behavior change during a health pandemic: a preregistered study. Front Psychol. 2020. https://doi.org/10.3389/fpsyg.2020.587911.
Cary LA, Chasteen AL, Remedios J. The Ambivalent Ageism Scale: developing and validating a scale to measure benevolent and hostile ageism. Gerontologist. 2017. https://doi.org/10.1093/geront/gnw118.
Weiss D, Weiss M. The interplay of subjective social status and essentialist beliefs about cognitive aging on cortisol reactivity to challenge in older adults. Psychophysiol. 2016. https://doi.org/10.1111/psyp.12667.
Lachman ME, Baltes P, Nesselroade JR, Willis SL. Examination of personality-ability relationships in the elderly: the role of the contextual (interface) assessment mode. J Res Pers. 1982. https://doi.org/10.1016/0092-6566(82)90007-1.
Funding
This work was supported, in part, by the Michigan Integrative Wellbeing and Inequality Training Program (National Center for Complementary and Integrative Health (R25-AT010664).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception, design, and methodology. Literature searches and data collection were conducted by Lauren Elias and Josie Greenwood. Julie Ober Allen conducted the data analysis and took the lead role in drafting the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Topical Collection on Epidemiology of Aging.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Allen, J.O., Elias, L.K. & Greenwood, J.C. Differences and Disparities in Ageism Affecting Older US Adults: a Review. Curr Epidemiol Rep 10, 17–32 (2023). https://doi.org/10.1007/s40471-022-00316-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40471-022-00316-6