
Abstract
Aim
Estimate the prevalence of developmental defects of enamel (DDE) in the primary dentition, describe the distribution among tooth groups and investigate the association with birth weight.
Methods
A cross-sectional study was conducted with a sample of 827 children aged 2–5 years representative of the city of Canela in southern Brazil. Demographic characteristics (gender and age) and birth weight were collected from vaccination cards. The diagnosis of DDE was performed by six trained examiners following the criteria of the Federation Dentaire International. DDE were described both jointly and separately as opacity and hypoplasia. Statistical analysis involved the Chi square test, Mann–Whitney test and Poisson regression with robust variance.
Results
The prevalence of DDE was 55.1% (95% CI 51.6–58.5%), with a mean of 3.0 ± 2.2 teeth affected. Opacity was the more frequent defect (50.4%), followed by hypoplasia (15.5%). Distribution of the defects was uneven, with opacity predominant on second molars and hypoplasia predominant on canines and second molars. Children with a low birth weight did not have a greater probability of opacity (PR: 1.13; 95% CI 0.91–1.41), hypoplasia (PR: 1.33; 95% CI 0.80–2.22) or DDE (PR: 1.11; 95% CI 0.91–1.37).
Conclusion
The prevalence of DDE was high, predominant on second molars and not associated with birth weight. These findings indicate directions for future examination/diagnosis protocols and specific orientations.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Developmental defects of enamel (DDE) appear in the form of variations in the translucence of tooth enamel (opacity) or a reduction in the thickness of visible enamel (hypoplasia) (FDI 1992; Elfrink et al. 2013). DDE are clinically relevant because such defects potentiate the accumulation of biofilm and contribute to both the occurrence and progression of dental caries (Li et al. 1996; Oliveira et al. 2006; Hong et al. 2009; Targino et al. 2011; Côrrea-Faria et al. 2015; Massignan et al. 2016; Costa et al. 2017). DDE have also been associated with tooth sensitivity and unpleasing dental aesthetics (Oliveira et al. 2006; Hong et al. 2009; Targino et al. 2011; Vargas-Ferreira et al. 2014).
Knowledge on the prevalence and distribution of DDE in the primary dentition is fundamental to the establishment of examination protocols, early diagnosis and treatment, and specific counseling at different ages. Moreover, the relationship with dental caries underscores the importance of recognising the teeth and arches most affected by opacity and hypoplasia in children. However, population-based studies on DDE in the primary dentition are scarce and offer inconsistent results, with prevalence rates ranging from 24 to 81.3% (Lunardelli and Peres 2005; Hoffmann et al. 2007; Farsi 2010; Côrrea-Faria et al. 2013; Massumo et al. 2013; Alkhtib et al. 2016).
Studies that address the network of causality of DDE are also scarce and there is no scientific basis for the explanation of the occurrence of such defects. Although the influence of socio-economic factors as well as hereditary or acquired (systemic or local) characteristics of the child has been suggested (Rugg-Gunn et al. 1998; Chaves et al. 2007; Massoni et al. 2009; Targino et al. 2011; Côrrea-Faria et al. 2013; Salanitri and Seow 2013), there is no evidence that can contribute to the planning of prevention strategies or at least predict which children may develop DDE.
Primary teeth have a precise chronology, with formation beginning during pregnancy and ending after the birth of the child, making these teeth subject to formation and calcification disorders in the prenatal and postnatal periods (Sarnat and Schour 1941). It is therefore plausible that DDE are associated with birth weight. However, studies that have evaluated the influence of prenatal and postnatal factors, such as low birth weight and prematurity, offer conflicting findings (Rugg-Gunn et al. 1998; Lunardelli and Peres 2006; Massoni et al. 2009; Côrrea-Faria et al. 2013; Jacobsen et al. 2014). As low birth weight affects less than 10% of children, studies with a small sample size do not have the power to detect its effect on different conditions of child health. Clarifying the role of birth weight in the occurrence of DDE in studies with a representative sample of adequate size could contribute to the definition of whether children with a low birth weight should be prioritised or whether preventive measures should be taken for all parents and caregivers. Moreover, identifying teeth with a greater prevalence rate of DDE may assist dentists in advising parents/caregivers more effectively during the eruption of different tooth groups.
The aim of the present study was to estimate the prevalence of DDE in the primary dentition, describe the distribution among tooth groups and investigate the association with birth weight in children in southern Brazil.
Methods
Participants and study design
A cross-sectional study was conducted with a representative sample of children aged 2–5 years who participated in the National Multi-Vaccination Campaign in the city of Canela in southern Brazil, which has 39,229 inhabitants and vaccine coverage reaches more than 90% of children aged 0–5 years. This study received approval from the Human Research Ethics Committee of the Lutheran University of Brazil (process: CEP ULBRA 200.403.2H). Guardians signed a statement of informed consent authorising the oral examination of the children.
The calculation of the sample size necessary to investigate the association between birth weight and DDE considered a 95% confidence level, 80% power, 9:1 ratio of non-exposed (adequate birth weight) to exposed (low birth weight) and prevalence of DDE of 13% and 27% among non-exposed and exposed individuals, respectively (Seow et al. 1987). The required sample size (n = 650) was increased by 20% for the multivariate analysis, leading to the need to examine 780 children. The Municipal Secretary of Health established 12 vaccination posts. Considering the number of children expected for National Vaccination Day (approximately 3000), possible refusals and the possibility of inclement weather reducing the turnout at the health units, six of the 12 vaccination sites were randomly selected to reach the predetermined sample size.
All children who attended the selected health units for vaccination were invited to participate in the study, regardless of their health condition or any previous medical or dental treatment. Thus, no exclusion criterion was used to ensure maximum external validity.
Data collection
The independent variables (birth weight, gender and age) were collected from vaccination cards, which contained information recorded at the time of birth. Birth weight was categorised dichotomously (< 2500 g = low weight; ≥ 2500 g = adequate weight) as well as in deciles. Age was collected quantitatively (complete years) and subsequently dichotomised (2–3 years/4–5 years).
The clinical examination was performed by six examiners who had undergone training and calibration exercises. The teeth were cleaned with a toothbrush and dried with gauze. The Modified Developmental Defects of Enamel Index proposed by the Federation Dentaire International (FDI 1992) was used, which defines opacity (“defect involving an alteration in the translucency of the enamel, variable in degree; the defective enamel is of normal thickness with a smooth surface”) and hypoplasia (“defect involving the surface of the enamel and associated with a reduced localised thickness of enamel”). Based on these criteria, demarcated opacity, diffuse opacity and demarcated/diffuse opacity were designated opacity; hypoplasia, demarcated opacity/hypoplasia, diffuse opacity/hypoplasia and all three conditions combined were identified as hypoplasia. Each tooth was categorised as normal (absence of enamel defect) or with DDE (presence of opacity or hypoplasia).
For the training and calibration exercises, 20 children at a public preschool in the same age group were examined. These children did not participate in the main study. The examiners were trained by an experienced researcher for the diagnosis of DDE. Intra-examiner Kappa coefficients ranged from 0.78 to 0.92 and inter-examiner coefficients ranged from 0.81 to 0.92.
Data analysis
The data were entered and analysed using the Statistical Package for the Social Sciences (SPSS 20.0 for Windows). Prevalence ratios (PR) and 95% confidence intervals (CI) were calculated using Poisson regression with robust variance to investigate associations between birth weight and DDE, opacity and hypoplasia. The variables child’s gender, age and number of teeth were incorporated into the model as potential confounding factors and maintained in the multivariate model independently of the level of significance. The linear trend Chi square test was used to analyse the association between birth weight (categorised in deciles) and the presence of opacity, hypoplasia and DDE. The Mann–Whitney test was used to determine the existence of significant differences among the categories of the exposure variables with regard to the number of teeth with DDE. The level of significance was set to 5% (p < 0.05).
Results
The sample was composed of 827 children [405 boys (49%) and 422 girls (51%)]. Age was distributed as follows: 270 (32.6%) were 2 years of age; 275 (33.3%) were 3 years of age; 256 (31.0%) were 4 years of age; and 26 (3.1%) were 5 years of age. A total of 90.4% of the children had fully erupted primary dentitions. Birth weight ranged from 1495 to 4900 g [mean and standard deviation (SD) 3140 ± 525.3 g]. Seventy children (8.9%) had low birth weight and one had very low birth weight (< 1500 g).
The prevalence of DDE was 55.1% (456/827; 95% CI 51.6–58.5%). The number of teeth with DDE ranged from 0 to 13 [mean (SD) 1.67 ± 2.2; median 1]. Among the children with DDE, the mean (SD) number of teeth affected was 3.0 ± 2.2 (median 2). Regarding the type of DDE, the prevalence of opacity and hypoplasia was 50.4% (417/827; 95% CI 46.9–53.8%) and 15.5% (128/827; 95% CI 13.0–18.1%), respectively.
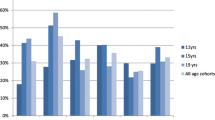
The prevalence of DDE in the maxilla and mandible was 41.5 and 39.3%, respectively. Considerable heterogeneity was found regarding the distribution of opacity and hypoplasia according to tooth group (Figs. 1, 2). DDE was more prevalent on primary second molars (21.2%), followed by primary canines (10.4%), first molars (10.1%), central incisors (2.0%) and lateral incisors (1.4%). Opacity was more prevalent on primary second molars (18.8%), followed by primary first molars (8.9%), canines (7.9%), central incisors (1.2%) and lateral incisors (1.1%). Hypolasia was more prevalent on primary canines (2.5%), followed by primary second molars (2.4%), first molars (1.2%), central incisors (0.8%) and lateral incisors (0.3%).

Prevalence of enamel opacity according to tooth examined

Prevalence of enamel hypoplasia according to tooth examined
No difference in the prevalence of DDE was found between genders. The prevalence was slightly higher among children with a low birth weight (60.0%) than those with adequate birth weight (54.9%) (Table 1). After adjusting for confounding variables, however, children with a low birth weight did not have a greater probability of the outcome (PR = 1.11; 95% CI 0.91–1.37). The prevalence of opacity also did not differ significantly in relation to gender, age or birth weight. The small difference in the prevalence of opacity between children with a low birth weight (55.7%) and those with adequate birth weight (50.1%) was not statistically significant after controlling for confounding factors (PR = 1.13; 95% CI 0.91–1.41). Likewise, no associations were found between hypoplasia and gender, age or birth weight. The prevalence of hypoplasia among children with a low birth weight and those with an adequate birth weight was 20.0 and 15.4%, respectively, but this difference did not achieve statistical significance (PR = 1.33; 95% CI 0.80–2.22) (Table 1). Moreover, no differences in the number of teeth with DDE were found in relation to gender (p = 0.423), age group (p = 0.062) or birth weight (p = 0.190) (Table 2).
Table 3 displays the prevalence rates of DDE, opacity and hypoplasia according to birth weight categorised in deciles. The frequencies of the three conditions were higher among children in the first decile (weight < 2511 g) than those in the last decile (weight > 3800 g). However, no tendency toward a reduction in prevalence was found with the increase in birth weight (p > 0.05 for all conditions).
Discussion
The most important findings of the present study involving children in southern Brazil were a high prevalence rate of DDE in the primary dentition, the uneven distribution among tooth groups and the absence of an association with birth weight.
Population-based studies using the same index for the evaluation of DDE describe considerable variation in the prevalence, but none report defects in less than 20% of children, which demonstrates the magnitude of the problem (Lunardelli and Peres 2005; Hoffmann et al. 2007; Farsi 2010; Côrrea-Faria et al. 2013). Although characteristics related to the population may partially explain the divergence in the estimates (Farsi 2010; Jacobsen et al. 2014), methodological aspects of the examinations, such as the type of lighting, cleaning and drying of the teeth, must also contribute in this respect. Moreover, the differentiation between demarcated opacity and diffuse opacity is not a simple task and could lead to some degree of measurement bias. However, differences in the classification criteria of DDE are likely to be the main reason for the differences among studies.
In the present investigation, demarcated and diffuse opacities were included in the same category. This decision was made during the planning of the study, considering the two conditions together to be more informative than separate descriptions, which increases the possibility of measurement bias. However, the present findings unmistakably demonstrate that DDE constitute a highly prevalent condition in the primary dentition. It should also be stressed that the examiners underwent an exhaustive training and calibration process and that the sample size was the largest among the studies that have used the FDI index, which indicates a high degree of precision in the estimates.
The uneven distribution with regard to tooth groups has been reported previously for both opacity and hypoplasia (Seow et al. 1987; Lunardelli and Peres 2005; Hoffmann et al. 2007; Farsi 2010; Côrrea-Faria et al. 2013; Vargas-Ferreira et al. 2015; Wagner 2017). The higher prevalence of opacity on primary second and first molars and the higher prevalence of hypoplasia on primary canines and second molars may be related to the time and duration of tooth formation, which could make these teeth more exposed to the development of defects. Interestingly, the prevalence of DDE is inversely proportional to the amount of tissue formed at the time of birth and directly proportional to the duration of the complete mineralisation of the crown. Evidence of the calcification of the primary second molars and canines is observed only around the fifth month of intrauterine life and the crowns of these teeth are completed around ten months of age (Lunt and Law 1974). Thus, complications, especially in the postnatal period, seem to exert a direct influence on the formation of DDE.
Opacity on primary second molars was the most frequent enamel defect. This condition has recently been renamed hypomineralised second primary molars (HSPM) from deciduous molar hypomineralisation (DMH) (Elfrink et al. 2008, 2012, 2014). Studies have demonstrated that the prevalence of DMH ranges from 4.6 to 9% (Elfrink et al. 2014; Temilola et al. 2015) and this defect is suggested to be a predictor of molar-incisor hypomineralisation (Elfrink et al. 2012, 2014; Ghanim et al. 2013). Common aetiological factors (peri-natal problems and infection) may be associated with both conditions (Elfrink et al. 2012, 2014), since primary second molars undergo calcification in a period close to that of the permanent first molars (Butler 1967).
The aetiology of DDE has been attributed to hereditary or acquired (systemic or local) factors (Salanitri and Seow 2013), including prematurity and low birth weight (Rugg-Gunn 1998; Lunardelli and Peres 2006; Côrrea-Faria et al. 2013; Jacobsen et al. 2014; Wagner 2017), which are considered preventable public health problems that exert a negative impact on child morbidity and mortality rates (Gallo et al. 2011). In the present study, however, low birth weight was not associated with opacity or hypoplasia, regardless of how this variable was categorised (dichotomised or in deciles). Moreover, the number of teeth with DDE did not differ according to birth weight. Previous studies report a greater occurrence of DDE among children with low birth weight (Rugg-Gunn 1998; Massoni et al. 2009; Velló et al. 2010), whereas others have not found such an association (Lunardelli and Peres 2006; Massumo et al. 2013). Low birth weight reflects the health status of the child and family, socioeconomic level and quality of prenatal care (Sclowitz and Santos Ida 2006) and can be a marker of numerous conditions with the potential to impair enamel development, resulting in DDE in the primary dentition (Salanitri and Seow 2013), such as maternal vitamin D deficiency during pregnancy, cardiovascular defects, haematological problems and kidney defects (Seow 1997). However, some of these conditions are rare and may not affect a reasonable number of children with low birth weight, which would explain the lack of an association with DDE. If DDE are actually caused by multiple health conditions that individually have low prevalence rates, the identification of this effect for each condition will be problematic in future studies, since it would require a sample size that would be very difficult or even impossible to obtain.
Among the clinical implications of the present study, the high prevalence of DDE observed and the results of previous studies in which such defects were identified as a risk factor for early childhood caries (Oliveira et al. 2006; Targino et al. 2011; Côrrea-Faria et al. 2015; Massignan et al. 2016) indicate the need for special attention and specific orientations during checkups. Enamel with defects has been described as more prone to retaining biofilm (Li et al. 1996; Hong et al. 2009; Caufield et al. 2012). Teeth with DDE are less resistant to acid; thus, carious lesions can progress more rapidly in comparison to areas without DDE (Salanitri and Seow 2013). Moreover, brushing in these areas could cause tooth sensitivity. Thus, early diagnosis of the condition can contribute to specific preventive orientations to avoid the initiation of caries, which could potentially assist in reducing the consequences of caries, such as dental pain and tooth loss (Hong et al. 2009; Boeira et al. 2012). The identification of the most affected teeth, especially the primary second molars, suggests that parents/caregivers should be warned of the possibility of such defects and be given specific oral hygiene instructions when the period of eruption of this tooth group approaches. The fact that low birth weight is not associated with the outcome indicates that this group of children does not need to be prioritised and such orientations should be directed in a broader manner to all families.
The present study has limitations that should be addressed. The cross-sectional design impedes the detection of causal relationships. However, the exposure used in the study (low birth weight) was collected at birth, prior to the eruption of any teeth. Thus, longitudinal studies would not represent a lower possibility of reverse causality bias regarding this specific issue. Nonetheless, longitudinal studies are needed due to the ability to detect DDE soon after the eruption of tooth groups, which would diminish the possibility of measurement bias, as the changes caused by tooth wear and the occurrence of caries can exert an influence on the diagnosis (Elfrink et al. 2012). Moreover, cross-sectional studies may underestimate the prevalence of DDE, since filled or missing teeth due to caries could previously have had DDE, especially hypoplasia. Although it is not possible to estimate the size of this bias, it is plausible that it is small, since untreated dental caries accounts for almost the entire dmft index among preschool children in southern Brazil (Chaffee et al. 2017). In addition, the training of the examiners, which included the diagnosis of DDE in teeth with carious lesions, demonstrated good reproducibility. It is also important to stress that dental caries does not satisfy the conditions of a confounding variable, especially since it is not plausible that this condition is associated with the exposure variable. Thus, its inclusion in the analysis would not have altered the results regarding the lack of an association between birth weight and DDE.
Another limitation is the small number of independent and control variables, which impeded the investigation of other relevant factors potentially associated with the outcome. Actually, the present study prioritised investigating a large, population-based sample, which was the greatest strength of the study, to achieve greater precision in the estimates of each of the conditions evaluated. For example, the prevalence of low birth weight in the present study was virtually the same as that for the southern region of Brazil (8.6%) (Brazil 2014). Moreover, the study had power to detect an association between birth weight and DDE. The findings can be generalised to similar populations with a predominantly low socio-economic status in developing countries.
Conclusion
The findings of the present study demonstrate a high prevalence rate of developmental defects of enamel in the primary dentition, uneven distribution with regard to the teeth affected and the absence of an association with birth weight. These findings underscore the need for early care and can contribute to the development of examination/diagnosis protocols and specific orientations for oral health promotion in childhood.
References
Alkhtib A, Ghanim A, Temple-Smith M, et al. Prevalence of early childhood caries and enamel defects in four and five-year old Qatari preschool children. BMC Oral Health. 2016;16:73.
Boeira GF, Correa MB, Peres K, et al. Caries is the main cause for dental pain in childhood: findings from a birth cohort. Caries Res. 2012;46(5):488–95.
Brazil, Health Ministry. Health Brazil 2013: an analysis of health situation and communicable diseases related to poverty. Brasília: Health Ministry, 2014 [document in Portuguese]. http://bvsms.saude.gov.br/bvs/publicacoes/saude_brasil_2013_analise_situacao_saude.pdf. Accessed 30 Apr 2017.
Butler PM. Comparison of the development of the second deciduous molar and first permanent molar in man. Arch Oral Biol. 1967;12(11):1245–60.
Caufield PW, Li Y, Bromage TG. Hypoplasia-associated severe early childhood caries—a proposed definition. J Dent Res. 2012;91(6):544–50.
Chaffee BW, Rodrigues PH, Kramer PF, Vítolo MR, Feldens CA. Oral health-related quality-of-life scores differ by socioeconomic status and caries experience. Community Dent Oral Epidemiol. 2017. https://doi.org/10.1111/cdoe12279.
Chaves AMB, Rosenblatt A, Oliveira OFB. Enamel defects and its relation to life course events in primary dentition of Brazilian children: a longitudinal study. Community Dent Health. 2007;24(1):31–6.
Corrêa-Faria P, Martins-Júnior PA, Vieira-Andrade RG, et al. Developmental defects of enamel in primary teeth: prevalence and associated factors. Int J Paediatr Dent. 2013;23(3):173–9.
Corrêa-Faria P, Paixão-Gonçalves S, Paiva SM, et al. Association between developmental defects of enamel and early childhood caries: a cross-sectional study. Int J Paediatr Dent. 2015;25(2):103–9.
Costa FS, Silveira ER, Pinto GS, et al. Developmental defects of enamel and dental caries in the primary dentition: a systematic review and meta-analysis. J Dent. 2017. https://doi.org/10.1016/j.jdent.2017.03.006.
Elfrink MEC, Schuller AA, Weerheijm KL, Veerkamp JSJ. Hypomineralized second primary molars: prevalence data in Dutch 5-year-olds. Caries Res. 2008;42(4):282–5.
Elfrink MEC, Ten Cate JM, Jaddoe VWV, et al. Deciduous molar hypomineralization and molar incisor hypomineralization. J Dent Res. 2012;91(6):551–5.
Elfrink ME, Ten Cate JM, van Ruijven LJ, Veerkamp JS. Mineral content in teeth with deciduous molar hypomineralisation (DMH). J Dent. 2013;41(11):974–8.
Elfrink MEC, Moll HA, Kiefte-de Jong JC, et al. Pre-and postnatal determinants of deciduous molar hypomineralisation in 6-year-old children. The Generation R Study. PLoS One. 2014;9:e91057.
Farsi N. Developmental enamel defects and their association with dental caries in preschoolers in Jeddah, Saudi Arabia. Oral Health Prev Dent. 2010;8(1):85–92.
Federation Dentaire Internationale-Commission on Oral Health, Research and Epidemiology. A review of the developmental defects of dental index (DDE index). Int Dent J. 1992;42(6):411–26.
Gallo EAG, Anselmi L, Dumith S, et al. Size at birth and mental health problems at 11 years of age in a Brazilian birth cohort. Cad Saúde Pública. 2011;27(6):1622–32.
Ghanim A, Manton D, Marino R, Morgan M, Bailey D. Prevalence of demarcated hypomineralisation defects in second primary molars in Iraqi children. Int J Paed Dent. 2013;23(1):48–55.
Hoffmann RH, de Sousa ML, Cypriano S. Prevalence of enamel defects and the relationship to dental caries in deciduous and permanent dentition in Indaiatuba, São Paulo, Brasil. Cad Saúde Pública. 2007;23(2):435–44.
Hong L, Levy SM, Warren JJ, Brofitt B. Association between enamel hypoplasia and dental caries in primary second molars: a cohort study. Caries Res. 2009;43(5):345–53.
Jacobsen PE, Haubek D, Henriksen TB, Østergaard JR, Poulsen S. Developmental enamel defects in children born preterm: a systematic review. Eur J Oral Sci. 2014;122(1):7–14.
Li Y, Navia JM, Bian JY. Caries experience in deciduous dentition of rural Chinese children 3–5 years old in relation to the presence or absence of enamel hypoplasia. Caries Res. 1996;30(1):8–15.
Lunardelli SE, Peres MA. Prevalence and distribution of developmental enamel defects in the primary dentition of pre-school children. Braz Oral Res. 2005;19(2):144–9.
Lunardelli SE, Peres MA. Breast-feeding and other mother-child factors associated with developmental enamel defects in the primary teeth of Brazilian children. J Dent Child. 2006;73(2):70–8.
Lunt RC, Law DB. A review of the chronology of eruption of deciduous teeth. J Am Dent Assoc. 1974;89(4):872–9.
Massignan C, Ximenes M, da Silva Pereira C, et al. Prevalence of enamel defects and association with dental caries in preschool children. Eur Arch Paediatr Dent. 2016;17(6):461–6.
Massoni AC, Chaves AM, Rosenblatt A, Sampaio FC, Oliveira AF. Prevalence of enamel defects related to pre-, peri-and postnatal factors in a Brazilian children. Community Dent Health. 2009;26(3):143–9.
Massumo R, Bardsen A, Astrom AN. Developmental defects of enamel in primary teeth and association with early life course events: a study of 6–36 month old children in Manyara, Tanzania. BMC Oral Health. 2013;13:21.
Oliveira AFB, Chaves AMB, Rosenblatt A. The influence of enamel defects on the development of early childhood caries in a population with low socioeconomic status: a longitudinal study. Caries Res. 2006;40(4):296–302.
Rugg-Gunn AJ, Al-Mohammadi SM, Butler TJ. Malnutrition and developmental defects of enamel in 2-to 6-year-old Saudi boys. Caries Res. 1998;32(3):181–92.
Salanitri S, Seow WK. Developmental enamel defects in the primary dentition: aetiology and clinical management. Aust Dent J. 2013;58(2):133–40.
Sarnat BG, Schour I. Enamel hypoplasia (chronologic enamel aplasia) in relation to systemic disease: a chronologic, morphologic and etiologic classification. J Am Dent Assoc. 1941;28(12):1989–2000.
Sclowitz IK, Santos Ida S. Risk factors for repetition of low birth weight, intrauterine growth retardation, and prematurity in subsequent pregnancies: a systematic review. Cad Saúde Pública. 2006;22(6):1129–36.
Seow WK. Effects of preterm birth on oral growth and development. Aust Dent J. 1997;42(2):85–91.
Seow WK, Humphrys C, Tudehope DI. Increased prevalence of developmental dental defects in low birth-weight, prematurely born children: a controlled study. Pediatr Dent. 1987;9(3):221–5.
Targino AGR, Rosenblatt A, Oliveira AF, Chaves AMB, Santos VE. The relationship of enamel defects and caries: a cohort study. Oral Dis. 2011;17(4):420–6.
Temilola OD, Folayan MO, Oyedele T. The prevalence and pattern of deciduous molar hypomineralization and molar-incisor hypomineralization in children from a suburban population in Nigeria. BMC Oral Health. 2015;15:73.
Vargas-Ferreira F, Zeng J, Thomson WM, Peres MA, Demarco FF. Association between developmental defects of enamel and dental caries in schoolchildren. J Dent. 2014;42(5):540–6.
Vargas-Ferreira F, Salas MM, Nascimento GG, et al. Association between developmental defects of enamel and dental caries: a systematic review and meta-analysis. J Dent. 2015;43(6):619–28.
Velló MA, Martínez-Costa C, Catala M, Fons J, Guijarro-Martínez R. Prenatal and neonatal risk factors for the development of enamel defects in low birth weight children. Oral Dis. 2010;16:257–62.
Wagner Y. Developmental defects of enamel in primary teeth—findings of a regional German birth cohort study. BMC Oral Health. 2017;17:10.
Funding
No funding was received.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflict of interest.
Research involving human participants and/or animals
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
All the participants (respondents) filled a term to participate of the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ruschel, H.C., Vargas-Ferreira, F., Tovo, M.F. et al. Developmental defects of enamel in primary teeth: highly prevalent, unevenly distributed in the oral cavity and not associated with birth weight. Eur Arch Paediatr Dent 20, 241–248 (2019). https://doi.org/10.1007/s40368-018-0402-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40368-018-0402-4