
Abstract
Aims
To clinically evaluate the retention rates and caries-prevention effect of a resin-based, non-etch and rinse, self-etch primed pit and fissure sealant containing Sealant Pre-reacted Glass Ionomer Cement (S-PRG) fillers, in comparison to a conventional resin-based sealant over an 18-month period.
Methods
There were 81 children, aged 6–12 years old, who were randomly assigned to one of two sealant-groups, either the self-etch primed sealant (Beautisealant, Shofu) or the conventional etch and rinse sealant (Seal it, Spident). A total of 218 sealants of both groups were placed on first permanent molars with either sound surfaces (The International Caries Detection and Assessment System [ICDAS], code 0) or incipient enamel caries lesions (ICDAS code 1) according to the manufacturers’ instructions. Each sealant restoration was independently evaluated in terms of retention and caries status at 6, 12 and 18 months. The data were statistically analysed with the Chi-squared test and z-test and the level of significance was preset at α = 0.05.
Results
The differences between the complete retention rates of the two sealant groups were statistically significant in all periods of evaluation (p < 0.01). Survival rates of each sealant-group were comparable on sound (ICDAS 0) and enamel caries lesions (ICDAS1). Caries prevention effect of the two sealant groups was similar at the end of the evaluation period.
Conclusions
The clinical performance of the S-PRG filler-containing dental sealant placed with a self-etching primer was poor regarding its retention. Its significantly higher loss did not lead to more carious occlusal surfaces at the 18-month recall.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The occlusal surfaces of newly erupted posterior teeth are considered to be highly vulnerable to caries formation. It has been reported that almost 90% of the carious lesions in children occur in the pits and fissures of permanent posterior teeth, which can be explained by the anatomical complexity of these surfaces that favours plaque stagnation (Beauchamp et al. 2008).
The use of pit and fissure sealants has been widely recognised as an effective preventive treatment for managing occlusal dental caries (Beauchamp et al. 2008; Ahovuo-Saloranta et al. 2013). Sealants prevent the development of caries, or its progression, by preserving the pit and fissure system from the effects of dental plaque (Ahovuo-Saloranta et al. 2013). It has been proposed that sealants should be placed on both sound teeth and incipient non-cavitated carious lesions on permanent teeth of high caries risk patients in order to prevent the onset of caries and its progression (Griffin et al. 2008). The International Caries Detection and Assessment System (ICDAS) has been developed to assess the severity of carious lesions, from the earliest stages of visual demineralisation to obvious cavitations. According to the American Dental Association Guidelines for the use of pit and fissure sealants, ICDAS II codes 0, 1 and 2 are recommended for sealant application (Beauchamp et al. 2008).
A variety of dental materials have been used as sealants using different application techniques. Resin-based fissure sealants are the materials of choice and the standard clinical procedure involves acid-etching of the enamel (Feigal and Donly 2006; Beauchamp et al. 2008). Their effectiveness depends on the formation of a complete seal and is increased by correct technique and moisture control, appropriate follow-up and resealing as necessary. However, the isolation procedure may frequently be extremely challenging due to the state of eruption of the tooth or the patient’s non-compliance with treatment (Welbury et al. 2004).
Several studies report that the use of adhesive systems before sealant application on enamel may enhance the longevity of pit and fissure sealants and increase their shear bond strength, especially in situations predisposing to moisture contamination (Hebling and Feigal 2000; Hitt and Feigal 1992; Tulunoğlu et al. 1999). Improved mechanical retention is based on the adhesive properties of the bonding agent mediating between the etched enamel and the resin sealant (Peutzfeldt and Nielsen 2004).
Despite all the progress in improving adhesion, the sealant application procedure would be easier if the preparatory etch, rinse and drying steps could be eliminated, as they can be unpleasant for the patient, or difficult to achieve in some patients, especially children. To overcome this problem, sealants employing self-etch adhesive systems have been introduced to simplify the procedure, reduce chair time and patient technique sensitivity. Fewer operative steps are required when these materials are employed and they offer a better potential to traditional etch and rinse application techniques when treating paediatric patients (Peutzfeldt and Nielsen 2004; Feigal and Donly 2006). However, their bonding ability to previously unprepared enamel presents a challenge (Pashley and Tay 2001). There is limited documentation in the existing literature regarding their effectiveness when used as pit and fissure sealants (Burbridge et al. 2006).
The ability of these materials to release fluoride is cited as an advantage and resin sealants containing the so-called ‘giomers’ have appeared on the market. These contain pre-reacted glass ionomer cement (PRG) particles as inorganic fillers, which are prepared by the acid-base reaction of a fluoroaluminosilicate glass with polyalkenoic acid in water prior to inclusion into the urethane resin (Ikemura et al. 2008). Beautisealant (Shofu, Kyoto, Japan) is one such pit and fissure sealant that uses a self-etching primer. In vitro studies have concluded that it releases fluoride ions and is alleged to offer anti-caries properties (Dionysopoulos et al. 2016; Kaga et al. 2014). However, there are no studies in the literature as yet testing this material under clinical conditions.
Therefore, the aim of the present study was to clinically evaluate the retention rates and anti-cariogenic properties of a resin-based, S-PRG filler-containing pit and fissure sealant placed with a self-etching adhesive on either the sound or incipiently carious (ICDAS code 0 or 1) occlusal surfaces of first permanent molars. The null hypotheses were: (1) there is no difference in retention between a resin sealant placed with a conventional acid-etch bonding procedure, and one placed with a non-rinsing self-etch technique, (2) there is no difference in sealant retention by sound or incipiently carious occlusal enamel, and, (3) there is no difference in occlusal caries prevention between a fluoride releasing, S-PRG filler-containing resin sealant and a conventional resin sealant.
Materials and methods
The study was carried out at the Department of Paediatric Dentistry, School of Dentistry, Aristotle University of Thessaloniki (AUTh) in Greece. Ethical approval was granted by the School’s Research Ethics Committee (Id no. 12/18-2-2015). Signed informed consent was obtained from the parent or guardian of every participant.
Subjects were recruited from the patients seeking routine dental treatment at the postgraduate Paediatric Dental Clinic. Eligible patients were healthy children, aged 6–12 years, exhibiting minimal or no disruptive behaviour (positive or definitely positive on Frankl’s scale) and having at least one first permanent molar either clinically sound or with incipient enamel caries (ICDAS code 0 or 1). The tooth had to be in a fully erupted state, with no history of previous restorations or any enamel defects including hypomineralisation opacities. The candidates were clinically assessed by the principal investigator (SN), who had been previously trained and calibrated to diagnose caries using the ICDAS II system. A data recording form for each participant was filled in to provide details on which teeth were eligible to receive sealants, their initial ICDAS code diagnosis, together with the sealant group each participant was assigned to. Using a table of random numbers, a total of 81 patients were randomly assigned to either sealant group: the self-etch sealant (Beautisealant, Shofu, Japan) or the conventional etch and rinse sealant (Seal it, Spident Co Ltd, Korea). A total of 218 sealants of both groups were placed on first permanent molars with either sound surfaces (ICDAS code 0) or incipient enamel caries lesions (ICDAS code 1) by two operators. The operators were second-year postgraduate students in Paediatric dentistry with similar years of previous clinical experience, who had received written and oral instruction on the two fissure sealant techniques from the principal researcher (SN). The prophylaxis of each molar tooth was completed with a thin pointed brush operated by a slow speed hand-piece, prior to sealant placement. Isolation was undertaken with cotton-rolls and high volume suction. Sealant placement was completed in a four-handed application technique, according to manufacturers’ instructions.
Test group
In the test group, an adequate amount of primer was applied onto the enamel surface with a microbrush, left undisturbed for 5 s and then air-dried gently to avoid blowing it away. Beautisealant was applied directly from the syringe into pits and fissures and light-cured (Mini L.E.D. Satelec Acteon, France) for 10 s, according to the manufacturer’s instructions.
Control group
In the control group, orthophosphoric acid gel 37% (Fine Etch, Spident Co Ltd, Korea) was applied to the occlusal surface of the selected molars for 30 s. The teeth were rinsed, air-dried and checked for appropriate etching. The Seal-it light-curing fissure sealant was applied directly from the syringe to all fissures and then light-cured with the above dental-curing unit for 30 s, according to the manufacturer’s instructions.
Two calibrated and blinded assessors (A.A., N.K.) evaluated the sealant restorations. Prior to the start of this clinical trial, in vivo and in vitro training sessions were conducted in order to standardise and calibrate the two evaluators participating in the study. The evaluation was blind, as treatment allocation details of each participant were not given to the assessors and both the materials are similarly coloured.
All sealant restorations were evaluated at 6, 12 and 18 months following placement. Only the occlusal surfaces of the teeth were evaluated with the aid of a dental mirror and explorer in terms of caries formation based on ICDAS II and sealant retention according to the following criteria:
-
1.
Total retention (TR): all pits and fissures of the occlusal surface are covered and no ledge of material is present.
-
2.
Partial loss (PL): fracture and/or some loss of material is present.
-
3.
Total loss (TL): absence of material from the occlusal surface.
Formerly sealed teeth were not resealed at the review appointments unless they presented with caries progression. If caries progression had occurred, the teeth were withdrawn from the study at this stage and restored appropriately. Patients failing to show up in 6-monthly reviews were considered as drop-outs. At the end of the 18-month evaluation period, all lost sealants were replaced or repaired according to the extent of their loss.
In the present study, the tooth was the experimental unit, taking into account that each individual participant might have both sound and incipiently carious molars included in the study. A total sample of a minimum of 186 teeth (93 teeth per material) was adequate to achieve a power of 80% in order to detect (with a two-sided z-test, at significance level a = 0.05) a difference in complete retention rates of 20% (conservative anticipation) between the two examined materials at the 6 months follow-up appointment. A priori Power Analysis was performed with the GPower v3.1.2 software. A difference of 20% was considered as a conservative biologically significant difference in the light of other studies having found greater differences. For example, Aman et al. (2015) indicated a difference of 30% between the totally retained sealants placed with the self-etch and the total etch approach. In another study Karaman et al. (2013) concluded there was a difference of 70% between the two groups mentioned above. Finally, a total of 81 patients were included in the study with a total of 218 teeth, an approximately 20% greater number than the estimated minimum sample size from power analysis in order to provide for possible dropouts.
Statistical analysis
Comparisons of independent percentages (%) were performed with the Chi-squared test and z-test. In all the hypothesis testing procedures, the observed significance level (p-value) was computed where appropriate, either with the Monte-Carlo simulation method or with Fisher’s Exact Method. By using these approaches, the inferential conclusions were safe, even in cases where the methodological assumptions of χ2 and z-tests were not fulfilled (e.g. random samples, independent observations). Data analysis was Performed with the SPSS V.20 statistical software. The significance level was predetermined at a = 0.05 (p ≤ 0.05). Kappa (κ) values were determined for intra-examiner and inter-examiner reproducibility.
Results
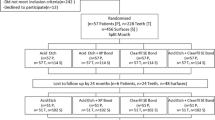
The study sample was selected within 4 months (October 2014–January 2015) and the evaluation period lasted until July 2016. The intra-examiner and inter-examiner reproducibility for the sealant retention scores were calculated by re-examining 10% of the sample a week apart. Intra-examiner k-value was 0.87 and 0.90 for examiners A.A. and N.K., respectively. Inter-examiner k-value was 0.90, indicating almost perfect agreement between the two examiners. As for ICDAS scoring, this was determined by the prime author alone (S.N.) after being familiarised during preparatory theoretical and bench seminars. Details of the 81 subjects with 218 teeth participating in the study appear in Fig. 1. Out of this number of participants, 16 subjects had 1 first permanent molar (FPM) restored with sealant, 24 subjects received 2 sealants on their FPMs, 10 participants had 3 FPMs restored with sealants and 31 participants had all 4 FPMs sealed.

Data characteristics provided at baseline
At the 6-month follow-up appointment, 198 teeth were evaluated for sealant retention and caries incidence. The teeth available for evaluation decreased to 189 and 176 at the 12 and 18-month recall appointments, respectively. The most common reasons the participants did not return throughout the follow-up period were: parents’ lack of time, children missing school hours and family relocation.
At the 6-month recall appointment, the complete retention rates were 82.2% for the control group as opposed to 16.5% for the experimental group, the difference being statistically significant (p < 0.001). After 12 months, the respective rates were 72.2% and 8.7% (p < 0.001). While at the end of 18 months, the overall retention rates for Seal it and Beautisealant were 69.7% and 6.9%, respectively (p < 0.001) (Table 1). Five sealants from the Seal it group and 55 from the Beautisealant group were totally lost in the course of the study.
The comparisons between the survival rates of each sealant group on sound and incipiently carious teeth are shown in Table 2. The differences were not statistically significant for either material over the 18-month evaluation period.
The results regarding caries incidence for the Seal it and the Beautisealant group throughout the 18-month evaluation period are shown in Table 3. Six molars in the Seal it group and 13 molars in the Beautisealant group presented with caries progression at the 18-month recall appointment. The overall caries incidence for the control and the experimental groups were 6.7% and 14.9%, respectively. The differences among those percentages were not statistically significant at the end of the evaluation period (χ2 = 3.073, df = 1, p = 0.093).
Discussion
The effectiveness of pit and fissure sealants regarding caries prevention in children and adolescents has been well documented in a Cochrane systematic review of 16 clinical trials (Ahovuo-Saloranta et al. 2013) and their use is indicated for patients who are at high risk of experiencing caries, as well as for caries management when ‘demineralisation appears confined to enamel’ (Welbury et al. 2004; Beauchamp et al. 2008). In the present study, molars with code 2 in ICDAS were not included because demineralisation in these surfaces may histologically extend into the dentine. Further diagnostic investigation would be required concerning those surfaces and, depending on the results of these, the suggested therapeutic approach could include a sealant or caries biopsy.
Different types of pit and fissure sealants have been evaluated in several clinical and laboratory studies using a variety of application techniques. In the present 18-month randomised control clinical trial, a non-rinse, resin based, SPR-G filler-containing dental sealant was clinically assessed in terms of retention and caries prevention on sound and incipiently carious first permanent molars. Beautisealant was selected as a fluoride releasing sealant that requires very little time for its application (30 s) and possibly exhibits some cariostatic effects.
However, the overall survival rates of Beautisealant were statistically significantly poorer compared to the conventional sealant group over the 18-month evaluation period. This refutes the first null hypothesis. The current study reported complete retention rates of 16.5% for the Beautisealant group in comparison with the conventionally sealed molars which produced a retention rate of 82.2% at the 6-month follow-up appointment. These percentages declined further to 6.9% and 69.7%, respectively, at the final 18-month evaluation.
The observed results could be explained by possible deficiencies in the etching capacity of the Beautisealant self-etching primer. It is well known that bonding to enamel is achieved by the formation of resin tags in the etched enamel and the length of these tags correlates with the bond strength (dos Santos et al. 2008). The bond effectiveness of self-etch adhesives is disputed, as most of them are not as acidic as phosphoric acid (Swift et al. 1995). There are several studies supporting the theory that the enamel etching potential of self-etching primers depends on their pH (Kanemura et al. 1999; Pashley and Tay 2001). A SEM study assessing the etching pattern of phosphoric acid etchants versus self-etch adhesives concluded that the etching effects of the latter were inferior on intact enamel surfaces (Shinohara et al. 2006). In another study by dos Santos et al. (2008), it was found that the penetration of adhesive materials was significantly greater when applied on enamel etched with phosphoric acid than with self-etching adhesives, prior to the application of a pit and fissure sealant.
Inadequate penetration of the adhesive material could also be dependent on the prophylaxis of the teeth that received sealants. Even though, in the present study, the prophylaxis of each tooth was performed with a thin pointed brush prior to sealant placement, organic remnants in the deepest aspect of the fissures may have been inadequately removed by the use of a self-etching primer, resulting in the poorer retention of Beautisealant (Burrow et al. 2003).
The findings of the present investigation are in accordance with those produced by a school-based retrospective study (Venker et al. 2004) that compared sealant placement with a self-etching primer system with the traditional acid-etch technique. The authors concluded that the retention of sealants placed with self-etch adhesives was significantly poorer compared to those placed with phosphoric-acid etching. Burbridge et al. (2006) reported on the clinical effectiveness of a one-step conditioning agent in sealant placement. In this clinical trial, sealants in the Xeno III group were more likely to fail compared with phosphoric-acid in conjunction with the Prime and Bond group that presented significantly superior retention. Contrary to these findings, and also to the results of the present study, Feigal and Quelhas (2003) found that Prompt L-Pop self-etching adhesive was as effective as phosphoric-acid alone for sealant placement evaluated over a 24-month period. These results could be explained by the particular aggressiveness of the self-etch adhesive used in this study, which is very similar to phosphoric acid, with a pH of 1 (Pashley and Tay 2001).
With regards to sealant retention rates on sound and incipiently carious molars, the differences found between the two subgroups (ICDAS 0 and ICDAS 1) were not statistically significant for either of the materials tested. Consequently, the second null hypothesis is accepted. The present study findings are in accordance with those of Handelman et al. (1987) who found almost identical sealant retention figures between sound tooth surfaces and surfaces with sticky fissures indicative of incipient caries. Similar to the present study, Soto-Rojas et al. (2012) investigated the retention of dental sealants on sound teeth and incipient caries lesions (ICDAS 1–3) as part of an in service-learning program in rural areas. The authors reported that sealant retention rates were almost identical in the above groups, irrespective of the ICDAS code.
Some studies however correlate fissure sealant success with the caries risk status of the patient (Bravo et al. 1996; Oulis and Berdouses 2009). In a study based on longitudinal data aggregated from children that received sealants in a private paediatric dental practice, it was concluded that high caries risk patients experienced more sealant losses resulting in higher caries prevalence, compared to those of low caries risk (Oulis and Berdouses 2009).These findings are in accordance with the study by Bravo et al. (1996) who reported that the number of sealant losses increased proportionately with the increase of the dft index. The authors’ explanation was that more questionable or incipiently carious fissures might have been sealed in those high caries risk children. Those surfaces differ from sound surfaces as they incorporate larger amounts of organic material that blocks acid penetration into the deeper surfaces of the fissure. Another in vitro study (Michalaki et al. 2010) investigated the microleakage of different sealant materials on sound (ICDAS II code 0) and questionable occlusal surfaces (ICDAS II codes 1 and 2). The findings of this study showed that fissure sealants placed on teeth with incipient enamel caries appeared to suffer statistically significantly higher microleakage in comparison with those applied on sound tooth surfaces. According to the authors, this is explained by the tissue characteristics of these surfaces that are different from sound surfaces, resulting in the poorer adaptation of fissure sealants.
The strength of evidence on the effectiveness of sealing over incipient enamel caries is weak, and more research is needed to clarify this grey area. The use of more standardised criteria to identify caries incidence, such as ICDAS, should be employed in all further studies in order to provide comparable conclusions regarding the retention of sealants on those surfaces. The existing evidence supports sealing over incipiently carious enamel lesions if those sealed surfaces can be maintained over time (Bader and Shugars 2006).
Another important finding of the present study needing to be considered is the caries incidence in the two sealant groups. Despite the poor performance of Beautisealant in terms of retention, the caries prevalence of the S-PRG filler-containing sealant group was not statistically significantly different compared to the traditional phosphoric-acid sealant group at the end of the 18-month evaluation period. The caries prevention effect of the two sealant groups was similar, resulting in the acceptance of the third null hypothesis. These findings might be explained on the basis of in vitro studies indicating that sealants containing S-PRG fillers have enamel demineralisation-inhibiting and remineralisation-promoting properties (Shimazu et al. 2011; Dionysopoulos et al. 2016). It is possible that, although Beautisealant was poorly retained in the present study, small S-PRG particles remaining into the depth of the fissures offering a caries prevention benefit.
A limitation of the present clinical trial is that the randomisation of the two treatment interventions was between the participants and not within the participants of this study. A split-mouth design would have better control over patient related factors such as oral hygiene, diet, behaviour possibly affecting the sealant retention and caries rates. However, this change would have resulted in greatly restricting subject recruitment. Another possible limitation of the present study is the 18-month follow-up period. A longer follow-up period and/or a greater sample size could have led to more definite results regarding the sealant retention rates when sealing over incipient caries.
Conclusions
The clinical performance of the S-PRG filler-containing dental sealant placed with a self-etching primer was poor regarding its retention when compared with the traditional phosphoric acid approach. However, its significantly higher loss did not lead to more carious occlusal surfaces at 18-month recall.
References
Ahovuo-Saloranta A, Forss H, Walsh T, et al. Sealants for preventing dental decay in the permanent teeth. Cochrane Database Syst Rev. 2013;(3):CD001830.
Aman N, Khan FR, Salim A, Farid H. A randomized control clinical trial of fissure sealant retention: self etch adhesive versus total etch adhesive. J Conserv Dent. 2015;18(1):20–4.
Bader JD, Shugars DA. The evidence supporting alternative management strategies for early occlusal caries and suspected occlusal dentinal caries. J Evid Based Dent Pract. 2006;6(1):91–100.
Beauchamp J, Caufield PW, Crall JJ, et al. Evidence-based clinical recommendations for the use of pit-and-fissure sealants: a report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2008;139(3):257–68.
Bravo M, Osorio E, García-Anllo I, Llodra JC, Baca P. The influence of dft index on sealant success: a 48-month survival analysis. J Dent Res. 1996;75(2):768–74.
Burbridge L, Nugent Z, Deery C. A randomized controlled trial of the effectiveness of a one-step conditioning agent in sealant placement: 6-month results. Int J Paediatr Dent. 2006;16(6):424–30.
Burrow JF, Burrow MF, Makinson OF. Pits and fissures: relative space contribution in fissures from sealants, prophylaxis pastes and organic remnants. Aust Dent J. 2003;48(3):175–9.
Dionysopoulos D, Sfeikos T, Tolidis K. Fluoride release and recharging ability of new dental sealants. Eur Arch Paediatr Dent. 2016;17(1):45–51.
dos Santos KT, Sundfeld RH, Garbin CAS, et al. Length of resin tags in pit-and-fissure sealants: all-in-one self-etching adhesive vs phosphoric acid etching. Compend Contin Educ Dent. 2008;29(3):186–92.
Feigal RJ, Donly KJ. The use of pit and fissure sealants. Pediatr Dent. 2006;28(2):143–50.
Feigal RJ, Quelhas I. Clinical trial of a self-etching adhesive for sealant application: success at 24 months with Prompt L-Pop. Am J Dent. 2003;16(4):249–51.
Griffin SO, Oong E, Kohn W, et al. The effectiveness of sealants in managing caries lesions. J Dent Res. 2008;87(2):169–74.
Handelman SL, Leverett DH, Espeland M, Curzon J. Retention of sealants over carious and sound tooth surfaces. Community Dent Oral Epidemiol. 1987;15(1):1–5.
Hebling J, Feigal RJ. Use of one-bottle adhesive as an intermediate bonding layer to reduce sealant microleakage on saliva-contaminated enamel. Am J Dent. 2000;13(4):187–91.
Hitt JC, Feigal RJ. Use of a bonding agent to reduce sealant sensitivity to moisture contamination: an in vitro study. Pediatr Dent. 1992;14(1):41–6.
Ikemura K, Tay FR, Endo T, Pashley DH. A review of chemical-approach and ultramorphological studies on the development of fluoride-releasing dental adhesives comprising new pre-reacted glass ionomer (PRG) fillers. Dent Mater J. 2008;27(3):315–39.
Kaga M, Kakuda S, Ida Y, et al. Inhibition of enamel demineralization by buffering effect of S-PRG filler-containing dental sealant. Eur J Oral Sci. 2014;122(1):78–83.
Kanemura N, Sano H, Tagami J. Tensile bond strength to and SEM evaluation of ground and intact enamel surfaces. J Dent. 1999;27(7):523–30.
Karaman E, Yazici A, Tuncer D, et al. A 48-month clinical evaluation of fissure sealants placed with different adhesive systems. Oper Dent. 2013;38(4):369–75.
Michalaki MG, Oulis CJ, Lagouvardos P. Microleakage of three different sealants on sound and questionable occlusal surfaces of permanent molars: an in vitro study. Eur Arch Paediatr Dent. 2010;11(1):26–31.
Oulis CJ, Berdouses ED. Fissure sealant retention and caries development after resealing on first permanent molars of children with low, moderate and high caries risk. Eur Arch Paediatr Dent. 2009;10(4):211–7.
Pashley DH, Tay FR. Aggressiveness of contemporary self-etching adhesives. Part II: etching effects on unground enamel. Dent Mater. 2001;17(5):430–44.
Peutzfeldt A, Nielsen LA. Bond strength of a sealant to primary and permanent enamel: phosphoric acid versus self-etching adhesive. Pediatr Dent. 2004;26(3):240–4.
Shimazu K, Ogata K, Karibe H. Evaluation of the ion-releasing and recharging abilities of a resin-based fissure sealant containing S-PRG filler. Dent Mater J. 2011;30(6):923–7.
Shinohara MS, de Oliveira MT, Di Hipólito V, Giannini M, de Goes MF. SEM analysis of the acid-etched enamel patterns promoted by acidic monomers and phosphoric acids. J Appl Oral Sci. 2006;14(6):427–35.
Soto-Rojas AE, Escoffié-Ramírez M, Pérez-Ferrera G, et al. Retention of dental sealants placed on sound teeth and incipient caries lesions as part of a service-learning programme in rural areas in Mexico. Int J Paediatr Dent. 2012;22(6):451–8.
Swift EJ, Perdigão J, Heymann HO. Bonding to enamel and dentin: a brief history and state of the art, 1995. Quintessence Int. 1995;26(2):95–110.
Tulunoğlu O, Bodur H, Uçtaşli M, Alaçam A. The effect of bonding agents on the microleakage and bond strength of sealant in primary teeth. J Oral Rehabil. 1999;26(5):436–41.
Venker DJ, Kuthy RA, Qian F, Kanellis MJ. Twelve-month sealant retention in a school-based program using a self-etching primer/adhesive. J Public Health Dent. 2004;64(4):191–7.
Welbury R, Raadal M, Lygidakis NA. European Academy of Paediatric Dentistry. EAPD guidelines for the use of pit and fissure sealants. Eur J Paediatr Dent. 2004;5(3):179–84.
Author information
Authors and Affiliations
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Rights and permissions
About this article

Cite this article
Ntaoutidou, S., Arhakis, A., Tolidis, K. et al. Clinical evaluation of a surface pre-reacted glass (S-PRG) filler-containing dental sealant placed with a self-etching primer/adhesive. Eur Arch Paediatr Dent 19, 431–437 (2018). https://doi.org/10.1007/s40368-018-0379-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40368-018-0379-z