
Abstract
Aim
To investigate the severity of and contributing factors of early childhood caries (ECC) in preschool children presented to a paediatric dentistry department in Al-Ain Dental Centre, United Arab Emirates; to study the level of any previous dental care provided to these children and to establish a baseline database for further research and the resources required for serving preschool children in Al-Ain (UAE).
Study design
Cross-sectional prospective.
Methods
The sample consisted of all healthy children below 5 years of age who presented for their initial visits to the Department of Paediatric Dentistry during a 3-month period. A structured questionnaire was used to obtain information regarding demographic data, feeding history and dietary habits, and oral hygiene practices. The dental examination of children was conducted by the investigator with the help of a mouth mirror and Sirona dental unit light source.
Results
One hundred and seventy six children with a mean age of 3.7 years were included in the study and 78 (44 %) children were still bottle-fed on demand at the time of examination. More than half of the children consumed sweets more than once/day and 58 % either never or rarely brushed their teeth. Only one child was given fluoride. Two-thirds of children had never visited a dentist before and 63 % had poor oral hygiene. The mean dmft and dmfs scores were 10.9 and 32.1, respectively. The care index was very low (6.4 %).
Conclusion
The high level of dental decay could be attributed to on-demand bottle feeding, high sweet consumption, poor oral hygiene, lack of use of fluoride prevention and lack of regular dental visits. There is a great need for prospective studies and community preventive programmes to solve the continuing problem of ECC.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Early childhood caries (ECC) has been defined as “the presence of one or more decayed (noncavitated or cavitated lesions), missing (due to caries), or filled tooth surfaces” in any primary tooth in a child 71 months of age or younger” (Drury et al. 1999). It is a chronic, transmissible infectious disease affecting the primary teeth. The aetiology of the condition is a combination of frequent consumption of fermentable carbohydrates as drinks, especially when a baby is sleeping, with on-demand breast or bottle feeding, oral colonisation by cariogenic bacteria (especially mutans streptococci), poor oral hygiene and poor parenting (O’Keefe 2013). In most cases, the aetiology will be a combination of several of these factors.
The prevalence of ECC varies greatly between different studies which may be due to several factors such as (1) children studied: their age and the accessibility for examination; (2) socio-economic status; (3) ethnic and cultural factors and (4) criteria used for diagnosis. Moreover, the prevalence of ECC in one country usually cannot be compared with another and even results from one ethnic group cannot be extrapolated beyond that group, even within the same country (Richardson et al. 1981). In western societies, approximately 80 % of caries is present in 20 % of the population commonly in children from low socio-economic groups, certain immigrants, patients with learning difficulties and those with physical and medical disabilities. The dental survey of children aged one and a half to four years in Great Britain (O’Brien 1994) showed that the proportion of children affected increased with age; 4 % of one and a half to two and a half year olds, 14 % of two and half to three and half year olds and 30 % of those aged three and a half to four and a half years had some experience of dental caries. In contrast, ECC is the most common childhood disease in the United Arab Emirates (UAE). In Abu Dhabi, children aged 2, 4 and 5 years, the prevalence was 35.5, 85.7 and 93.8 %, respectively, and in Al-Ain city in the same age groups, it was 45.2, 73.8 and 90.4 %, respectively (Al-Hosani and Rugg-Gunn 1998).
ECC can result in considerable suffering, pain, disfigurement, reduction of quality of life of affected children and frequently compromises their future dentitions. Prevention of ECC can be achieved firstly, by the education of prospective and new parents and secondly, by the identification of ‘high risk’ children (Lee et al. 1994). Strategies have focused on the individual mother and child, by preventing transfer of cariogenic bacteria from mother to her infant, using preventive agents such as fluoride and teaching good oral hygiene practices (Kohler et al. 1983). Community-based approaches have been attempted. An example of a successful programme through home visits to mother of at-risk young children in Leeds, UK was reported by Kowash et al. (2000). The treatment of ECC is very costly, time consuming, and in most cases it requires full dental rehabilitation under general anaesthesia by a paediatric dentist. However, following restoration of decayed teeth, recurrence of decay and its complications are very common in the absence of adequate prevention programme and follow-up visits (O’Sullivan and Curzon 1991) (Fig. 1).

Vicious circle of treatment and re-treatment of ECC and its’ complications in the absence of an effective preventive strategy
The severity and contributing factors of ECC in Al-Ain preschool children have not been adequately studied. In addition, there have been few preventive programmes implemented in the UAE and only for school-age children. Therefore, this study was carried out to investigate the severity and contributing factors of early childhood caries (ECC) in preschool children presented to a paediatric dentistry department in Al-Ain, United Arab Emirates, to study the level of any previous dental care provided to these children and to establish a baseline data for further research and the resources required for serving Al-Ain’s preschool children.
Materials and methods
Subjects
The sample consisted of all healthy children below 5 years of age who presented for their screening visits to the Department of Paediatric Dentistry, Tawam Dental Centre in Al-Ain city, UAE during a 3-month period. Tawam dental centre is the largest dental centre in Al-Ain and provides free dental treatment to Emirati nationals. The children were all Emirati nationals and accompanied by their mothers who had given their consent to be interviewed and for their children to be included in the study. Children with medical or behavioural problems who could not be persuaded to sit still for oral examination were excluded. The research protocol was approved by the research committee at Tawam dental centre.
Questionnaire interview
A structured questionnaire similar to that used by the National Diet and Nutrition Survey of the UK preschool children (Hinds and Gregory 1995) was used. Information was obtained regarding demographic data, feeding history and dietary habits, dental health and oral hygiene practices. The questionnaire was tested and used by the investigator in a previous study (Kowash et al. 2000).
Clinical examination
The oral examination of children was conducted by the principal investigator with the help of a mouth mirror and Sirona dental unit light source.
The investigator was trained and calibrated in the use of BASCD criteria (Palmer et al. 1984) which was used for caries diagnosis. The examiner was trained and calibrated by staff in Child dental Health of the university of Leeds (UK) (Kappa score = 0.82). No attempt was made to probe the teeth and dental radiographs were not used in any of the examinations. A tooth was considered present when any of its part was visible through the oral mucosa. Initial caries was defined as a demineralised area with loss of translucency and manifested caries as the presence of actual cavitation.
The oral hygiene status was examined by scoring debris (plaque, materia alba) and calculus using the same diagnostic criteria of the Children’s Dental Health Survey in the UK (Todd and Dodd 1985). Each jaw was divided into three segments: the right and left segments extending backwards from the distal surfaces of the canines to the distal surfaces of the most posterior teeth present and the middle segment extending forwards from the distal surface of canine on one side around to the distal surface of the canine on the other side. Each segment was examined both bucally and lingually and the presence of debris was recorded according to the following categories:
-
0 = The teeth are clean with no debris evident
-
1 = There is a small amount of debris of recent origin
-
2 = There is a considerable amount of long standing debris
Calculus presence was recorded according to the following categories:
-
0 = No calculus
-
1 = Calculus present
The restorative index (RI) was calculated, as described by Jackson (1973), by determining the ratio of filled teeth (f) to filled plus decayed teeth (f + d) and expressed as a percentage. The care index (CI) was measured using the ratio of the mean filled teeth (f) to mean decayed, missing and filled teeth (dmf). Only descriptive statistics were used. Results of caries risk factors were presented using histograms. The dental caries data were presented as mean dmft/dmfs.
Results
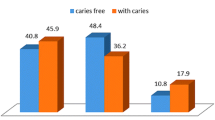
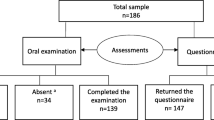
One hundred-seventy six children met the inclusion criteria and were included in the study (75 females and 101 males). The age of children ranged between 1.5 and 5 years with a mean age of 3.7 years and 78 (44 %) children were still bottle-fed on demand at the time of examination and 56 % stopped bottle feeding at the mean age of 2.4 years. More than half (52 %) consumed sweets more than once/day (Fig. 2) and 58 % either never or rarely brushed their teeth (Fig. 3). Two-thirds of children examined had never visited the dentist before and only one child was given fluoride supplement.

Frequency of children’s sweet consumption in preschool children in Al-Ain (UAE)

Frequency of children’s toothbrushing in preschool children in Al-Ain (UAE)
The results of oral examinations revealed that a high proportion of children (63 %) had poor oral hygiene and only 37 % had optimal/good oral hygiene (Table 1). The level of dental decay into dentine (initial caries without cavitation was excluded) was very high. The mean dmft and dmfs scores were 10.9 and 32.1 respectively. The CI, which is the proportion of filled teeth in relation to overall dmft and the RI, which is ratio of filled to filled plus decayed teeth were very low and both had an equal value of 6.4 % because in this study the children had no missing teeth (Table 1).
Discussion
The main limitation in this study was that the study children consisted of those presenting for their screening visits in a paediatric dentistry department in Al-Ain Tawam Dental Centre (i.e. convenient sample). The main aims were to explore the severity of dental decay and level of dental care provided to Al-Ain preschool children presented to the paediatric dentistry department. The results found in this study represent a baseline for further research and the resources required to serve Al-Ain’s preschool children.
The structured questionnaire used in this study was similar to that used in the diet and nutrition survey of preschool children in the UK (Hinds and Gregory 1995). It has been tested and used by the author in a previous study (Kowash et al. 2000). The questionnaire consisted of simple questions and was conducted through interviews by the investigator. This helped to overcome the problems that are usually encountered with mailed questionnaires which include refusal or delay in replying and difficulty in understanding the questions (Abramson 1990). A high proportion (44 %) of children was still bottle-fed on demand and 56 % had stopped bottle feeding at the mean age of 2.4 years. The Committee on medical aspects of food (COMA) in Britain (COMA 1989) recommended the early substitution of bottle with cup. The American Academy of Pediatric Dentistry (AAPD) recommended that infants should not be put to sleep with a bottle after the first primary tooth begins to erupt. Parents should be encouraged to have their infants drink from a cup after one year of age. Repetitive consumption of any liquid containing fermentable carbohydrates from a bottle should be avoided (AAPD 2012).
Night-time bottle feeding with juice, repeated use of a no-spill cup and frequent in-between meal consumption of sugar-containing snacks or drinks (e.g., juice, formula, soda) increases the risk of caries (Lo et al. 1998). More than half (52 %) of the children in this study consumed sweets more than once/day. A significant positive relationship between frequency of sugar consumption and dental caries has been reported (Hinds and Gregory 1995). Another study, however, failed to demonstrate the existence of a consistent correlation (Sundin et al. 1983). The reasons for these contradictory results are most likely due to the following: the dietary data are unreliable because they were collected by questionnaire from memory and not by records made in a diary as the food was eaten; the data were not incremental but, related to life-long accumulation of caries to dietary information for, in some studies, as little as one day (Jenkins 1982); other factors which are difficult to control include salivary factors and oral hygiene practice.
The mean age of children in this study was 3.7 years; however, two-thirds had not visited a dentist before. The AAPD has recommend an initial dental consultation visit no later than 1 year of age, to educate parents and provide anticipating guidance for prevention of dental diseases. The initial visit should include thorough medical (infant) and dental (parent and infant) histories, a thorough oral examination, performance of an age-appropriate tooth brushing demonstration, and prophylaxis and fluoride varnish treatment if indicated (American Academy of Pediatric Dentistry 2012). More than half (58 %) either never or rarely brushed their teeth. According to AAPD, oral hygiene measures should be implemented no later than the time of eruption of the first primary tooth. Twice-daily use of fluoridated toothpaste with a soft toothbrush of appropriate size is recommended. Parents should assess and supervise their preschool-age child tooth brushing. An infant’s newly erupted teeth may be cleaned using a cloth. Flossing of a child’s teeth is recommended where there are tight contacts (American Academy of Pediatric Dentistry 2012).
Optimal exposure to fluoride is important to all dentate infants and children (Garcia et al. 2001). Although the UAE drinking water is not optimally fluoridated, in this study only one child was given a fluoride supplement. Decisions concerning the administration of fluoride are based on the unique needs of each patient, and the use of fluoride for the prevention and control of caries is documented to be both safe and effective especially in at-risk populations (Chu et al. 2012).
The results of dental examinations in this study showed very severe ECC in terms of dmft and dmfs scores (10.9 and 32.1, respectively). These results cannot be compared with the two main previous studies conducted in the UAE because the study population in this study consisted of children presenting for their screening visits in a paediatric dentistry department (i.e. a convenience sample). Hashim et al. (2006) in Ajman, UAE studied caries prevalence and severity of ECC in 5–6-year-old children. They reported high caries prevalence (76.1 %) and an average dmfs score of 10.2 and that the Emirati (local) children had higher caries severity than other children. Severity of ECC was higher in this study (dmft = 10.9) than that reported by Al-Hosani and Rugg-Gunn (1998) in 5-year-old children of the same city (dmft = 8.6). The results of this study in terms of mean dmfs (32.1) is clearly a cause of concern for this continuing problem in the UAE especially when comparing it with the internationally accepted definition of severe ECC (S-ECC), which states that in children younger than 3 years of age, any sign of smooth-surface caries is indicative of S-ECC. From ages three to five years, one or more cavitated, missing (due to caries) or filled smooth surfaces in primary maxillary anterior teeth or a decayed, missing or filled score of ≥4 (age 3), ≥5 (age 4) or ≥6 (age 5) surfaces constitutes S-ECC (Ismail and Sohn 1999). An additional continued problem in Al-Ain children is that few decayed teeth were restored (Al-Hosani and Rugg-Gunn 1998). Also in this study, the filled component of dmft was very low (ft = 0.7). This clearly demonstrated the lack of dental care provided to Al-Ain preschool children with very low care and restorative indices (4.6 %) (Table 1). A high proportion of children (63 %) had poor oral hygiene. A positive correlation has been reported between plaque accumulation on primary teeth and ECC risk (Kowash et al. 2000).
The high level of dental decay in Al-Ain preschool children in this study could be attributed to on-demand prolonged bottle feeding, high sweet consumption, poor oral hygiene, lack of fluoride and lack of regular dental visits. Therefore, prevention seems to be the solution for the continuing problem of ECC because although it is an infectious and transmissible disease, it is preventable. There are two main preventive programmes: individual-based intervention and community-based intervention.
Individual-based intervention
This approach is used for high-risk populations because it is simple and does not require much effort from the parent or caregiver. However, it has two main disadvantages. Firstly, it requires identification of at-risk children and secondly, it can be costly as it requires professional or auxiliary personnel. Studies have used this approach by treating either the mother or child. In the case of mother, this can be done by counselling, toothbrushing and the use of fluoride to reduce the number of maternal micro-organisms transmitted to her child. Restoration of a mother’s open cavities and the use of anti-microbial agents can prevent or delay bacterial transmission to her infant. In the case of a child, this is done by the application of fluoride varnish and xylitol (Kohler et al. 1983; Lee et al. 1994; American Academy of Pediatric Dentistry 2012).
Community-based interventions
To effectively solve the problem of ECC, there should be collaboration between parents or caregivers, health personnel and the community. Community dental health programmes have been generally reported to be more important and effective than individual-based dental health programmes (Weinstraub 1998). However, to be effective, community-based initiatives should take into consideration the social belief, culture and level of education of parents or caregivers. Moreover, the dental personnel should be informed and trained to deliver evidence-based and effective dental health messages. Infants and young children are unable to effectively perform their daily dietary and oral hygiene practices and are dependent on their parents. Therefore, it is important that the dental health messages should focus on educating and changing the behaviour of parents or caregivers and should be practical by giving alternatives, for example, substituting milk with water in baby bottle at night for those who find it difficult to stop night-time bottle feeding. They should also consider the socioeconomic status of the parents and be culturally sensitive (Kowash et al. 2000). The benefit-cost (B/C) and cost-effectiveness (C/E) of a long-term dental health education programme to mothers of young children through repeated home visits were evaluated (Kowash et al. 2006). Comparisons were made for B/C and C/E with results from a clinical trial of a slow releasing fluoride device (Toumba and Curzon 2005), community water fluoridation and a school-based fissure sealant programme. The results showed that dental health education for mothers of young children starting at 8 months of age gave better B/C and C/E ratios than other preventive programmes.
Conclusion
The results of this study cannot be generalised because the study sample was not representative of all Al-Ain preschool children. However, having looked at children from the main dental centre, the alarmingly high level of dental decay may be attributed to on-demand prolonged bottle feeding, high sweet consumption, poor oral hygiene, lack of fluoride and lack of regular dental visits. The care index was very low; therefore, preschool children with active carious lesions should be given priority. The management of ECC should take into consideration the biology of the caries process and salivary protective mechanisms. The restorations placed should be of high standard and monitored through regular follow-up visits and long-term preventive strategy. There is a great need for prospective long-term studies and community-based preventive programmes to solve the continuing problem of ECC in the UAE. It is important that the dental health programmes should focus on educating and changing the behaviour of parents or caregivers. Moreover, the dental health messages should be practical and culturally sensitive.
References
Abramson JH. Interview and self-administered questionnaire. In: Survey methods in community medicine (4th edition). Edinburgh: Churchill Livingstone; 1990. p. 165–176.
Al-Hosani E, Rugg-Gunn A. Combination of low parental educational attainment and high parental income related to high caries experience in pre-school children in Abu Dhabi. Community Dent Oral Epidemiol. 1998;26(1):31–6.
American Academy of Pediatric Dentistry. Guideline on infant oral health care. Ref Man. 2012;35(6):13–4.
Chu CH, Chau AM, Wong ZS, Hui BS, Lo EC. Oral health status and behaviours of children in myanmar—a pilot study in four villages in rural areas. Oral Health Prev Dent. 2012;10:365–71.
Committee on Medical Aspects of Food (COMA). Dietary sugars and human disease. Reports of panel on dietary sugars. Report in health and social subjects. London: HMSO;1989. p 37.
Drury TF, Horowitz AM, Ismail AI. Diagnosing and reporting early childhood caries for research purposes. J Public Health Dent. 1999;59(3):192–7.
Garcia MB, Nör JE, Schneider LG, Bretz WA. A model for clinical evaluation of the effect of antimicrobial agents on carious dentin. Am J Dent. 2001;14:119–22.
Hashim R, Thomson WM, Ayers KMS, Lewsey JD, Awad M. Dental caries experience and use of dental services among preschool children in Ajman UAE. Intern J Paediatr Dent. 2006;16(4):257–62.
Hinds K, Gregory T. National diet and nutrition survey: children aged 1.5 to 4.5 years. Report of the dental survey Volume 2. HMSO: London; 1995.
Ismail AI, Sohn W. A systematic review of clinical diagnos-tic criteria of early childhood caries. J Public Health Dent. 1999;59(3):171–91.
Jackson D. Measuring restorative dental care in communities. Br Dent J. 1973;134:385–8.
Jenkins GN. Review of food cariogenicity testing. In: Diet and dental caries, editor. Storey E. Melbourne: University of Melbourne; 1982. p. 47–55.
Kohler B, Bratthall D, Krasse B. Preventive measures in mothers influence the establishment of bacterium streptococcus mutans in their infants. Arch Oral Biol. 1983;28:225–31.
Kowash MB, Pinfield A, Smith J, Curzon MEJ. Effectiveness on oral health of a long-term health education programme for mothers with young children. Br Dent J. 2000;188:201–4.
Kowash MB, Toumba KJ, Curzon MEJ. Cost-effectiveness of a long-term dental health education programme for the prevention of early childhood caries. Eur Arch Paediatr Dent. 2006;7(3):130–5.
Lee C, Rezaiamiri N, Jeffcott E, Oberg D, Domoto P, Weinstein P. Teaching parents at WIC clinics to examine their high caries risk babies. J Dent Child. 1994;61:347–9.
Lo EC, Schwarz E, Wong MC. Arresting dentine caries in Chinese preschool children. Int J Paediatr Dent. 1998;8:253–60.
O’Brien JE. Children’s dental health in the United Kingdom 1993. London: HMSO School Survey Division; 1994.
O’Keefe E. Early Childhood caries. Evid Based Dent 2013;14:40–1.
O’Sullivan EA, Curzon MEJ. Efficacy of comprehensive dental care for children under general anaesthesia. Br Dent J 1991;171:56–8.
Palmer JD, Anderson RJ, Downer MC. Guidelines for prevalence studies of dental caries. Community Dent Oral Epidemiol. 1984;1:55–66.
Richardson BD, Cleaton-Jones PE, McInnes PM, Ranisho JM. Infant feeding practices and nursing bottle caries. J Dent Child. 1981;48:423–9.
Sundin B, Birkhed D, Granath L. Is there not a strong relationship nowadays between caries and consumption of sweet? Swed Dent J. 1983;7:103–8.
Todd JE, Dodd T. Children’s dental health in the UK 1983. London: OPCS Social Survey Division; 1985.
Toumba KJ, Curzon ME. A clinical trial of a slow-releasing fluoride device in children. Caries Res. 2005;39(3):195–200
Weinstraub JA. Prevention of early childhood caries: a public health perspective. Community Dent Oral Epidemiol. 1998;26:62–6.
Acknowledgments
The author wishes to express his great appreciation to the mothers of the children for their interest and cooperation in this study. The author would also like to thank professors David Wray and Dr. Iyad Hussein for their help in checking and editing the English language of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Kowash, M.B. Severity of early childhood caries in preschool children attending Al-Ain Dental Centre, United Arab Emirates. Eur Arch Paediatr Dent 16, 319–324 (2015). https://doi.org/10.1007/s40368-014-0164-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40368-014-0164-6