
Abstract
Return to play (RTP) criteria after hamstring strain injuries (HSIs) help clinicians in deciding whether an athlete is ready to safely resume previous sport activities. Today, functional and sport-specific training tests are the gold standard in the decision-making process. These criteria lead to an average RTP time between 11 and 25 days after a grade 1 or 2 HSI. However, the high re-injury rates indicate a possible inadequacy of the current RTP criteria. A possible explanation for this could be the neglect of biological healing time. The present review shows that studies indicating time as a possible factor within the RTP-decision are very scarce. However, studies on biological muscle healing showed immature scar tissue and incomplete muscle healing at the average moment of RTP. Twenty-five percent of the re-injuries occur in the first week after RTP and at the exact same location as the index injury. This review supports the statement that functional recovery precedes the biological healing of the muscle. Based on basic science studies on biological muscle healing, we recommend a minimum period of 4 weeks before RTP after a grade 1 or 2 HSI. In conclusion, we advise a comprehensive RTP functional test battery with respect for the natural healing process. Before deciding RTP readiness, clinicians should reflect whether or not it is biologically possible for the injured tissue to have regained enough strength to withstand the sport-specific forces. In an attempt to reduce the detrimental injury–reinjury cycle, it is time to start considering (biological healing) time.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
For hamstring muscle injuries (grade 1 and 2), the average return to play (RTP) is denoted between 11 and 25 days while the muscle regeneration process is ongoing and scar tissue is still immature. |
Athletes are allowed to RTP when the healing hamstring muscle tissue is not ready. The biological healing of the muscle tissue after injury is often not respected, leading to unremittingly high occurrences of re-injuries. |
Before RTP clearance, we recommend a comprehensive RTP functional test battery with adherence to the natural healing process of the injured tissue. As a first step in the attempt to reduce the detrimental injury–reinjury cycle, it is time to consider (the biological healing) time. Before deciding RTP readiness of the athlete, clinicians should reflect whether or not it is biologically possible for the injured tissue to have regained enough strength to withstand the sport-specific forces (despite good function shown on the current RTP criteria). |
As a general guideline, the authors of the present review suggest a minimum period of 4 weeks before RTP after a grade 1 and 2 hamstring strain injury. The presented timeframe could be a mainstay for clinicians and other stakeholders when making a RTP decision. |
1 Introduction
Hamstring strain injuries (HSIs) are abundantly prevalent across sports encompassing high-speed running such as football [1,2,3,4,5,6,7,8]. Comprising 12% of all football-related injuries, HSIs remain a substantial burden for football players and their clubs [3]. The hamstring injury problem manifests itself both at amateur and elite levels, with incidence rates up to 16 and 22% per season, respectively [3, 4, 9]. After the occurrence of an index HSI, approximately 30% reoccur within the same season after return to play (RTP) [8, 10, 11]. These HSIs do not only come with high expenses in health care for diagnosis and treatment, they also cause substantial financial losses in elite football. As the average annual cost of injuries in a first division English team is calculated around 45 million British pounds [12], and the mean time loss after a HSI is approximately 20 days [8, 13,14,15], (re)injury prevention is of utmost importance to both the individual player and the club. However, despite the growing evidence-based knowledge and countless scientific efforts to reduce the unremittingly high incidence of HSIs by providing prevention strategies [16,17,18], (re)occurrence rates are still extensive [15]. The high number of re-injuries could be associated with either an insufficient prevention or rehabilitation program and/or inadequate RTP criteria. A number of attempts have been made to reach an evidence-based consensus on the RTP criteria after muscle injuries in sport [19,20,21]. To date, no conclusive evidence is available to clinicians on how to return athletes to sport in the best or safest way possible. Most literature recommends functional tests when deciding the readiness of athletes to RTP. Consequently, this is traditionally used by clinicians today [22]. Pain-free completion of sport-specific field tests (e.g. full speed sprinting) is omnipresent within RTP test batteries [22]. However, does a perfect score on these functional tests reflect an athlete that is completely ready to safely return to his/her previous sport activities? Does successful completion of respective functional tasks perfectly reflect to what extent the previously injured structure can safely withstand the sport-specific forces? The current re-injury rates highlight a possible inadequacy of these RTP testing batteries. However, it should be mentioned that it is unclear whether these test batteries are fully adopted and used within practice. Despite the availability of these functional RTP screening protocols, previous studies have shown that 25% of the re-injuries occur in the first week after RTP and at the exact same location as the index injury, indicating RTP clearance occurring prematurely [23]. Strikingly, natural healing time is almost never specifically mentioned as part of the RTP batteries in the current literature. Therefore, the aim of this review is to answer the question if natural healing time should be a key factor within the RTP decision-making process after a HSI.
2 Methodological Considerations
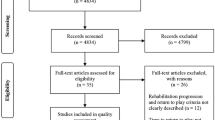
This review article is based on previous literature concerning two major topics, (1) RTP after HSIs and (2) biological muscle healing. By merging the scientific input gathered in the articles addressing these main domains, the authors attempted to answer the following research question: “Should biological healing time be included within the RTP criteria after a HSI?” We included previous review articles and consensus statements, and performed a hand search on the reference lists of these articles [19,20,21,22, 24,25,26,27,28]. In addition, the electronic database PubMed was searched (August 2020) by inserting domain-specific terms (Table 1). The search strategy concerning RTP after HSIs yielded 110 results. Within this domain only English language articles concerning human adults (19+ years) were included for further analysis. By applying these criteria, 48 studies remained for manual screening. Of these 48 studies, 32 were not eligible based on the topic discussed, leaving 16 extra studies for review. In the domain of biological muscle healing we limited the search to (systematic) reviews with the purpose of retrieving a structured overview of suitable studies in the current state of the art. The search strategy yielded 294 review articles of which 10 fully addressed the topic of interest. In conclusion, the search strategies in both domains resulted together in 26 additional studies retrieved from the PubMed database.
3 Return to Play After Hamstring Injuries
The criteria for deciding an athlete’s readiness to RTP after a muscle injury has evolved substantially over the last decades. At present, a battery comprising functional tests is considered the gold standard within the RTP decision-making process [20]. This battery most frequently contains the following variables: pain reproducible by palpation, (eccentric) strength, flexibility, and functional, sport-specific capacity [22]. These state of the art RTP criteria, most commonly used in the context of HSI, are depicted in Fig. 1 (based on a systematic review from van der Horst et al.,). These functional RTP criteria have been developed with the sole purpose of providing a safe RTP after injury. However, the unremittingly high re-injury rate of HSIs (12–34%) indicates current RTP criteria to be inadequate [11, 29]. Using these RTP criteria, an average RTP is reported to be between 11 and 25 days for grade 1 and 2 hamstring muscle injuries, which comprise more than 80% of all HSI [29, 30]. A possible explanation for the ever-increasing re-injury rates could be the abandonment of biological healing time of muscle tissue. In the current literature, it is striking that time is rarely included within the RTP criteria. Of the 25 studies included in the review of van der Horst et al. [22], only one explicitly mentioned time as a criterion [31]. In that latter survey report, the criterion ‘respect of a theoretical period of competition break’ was ranked 6th (of the 14 criteria) in order of importance [31]. However, it should be mentioned that some authors tend to incorporate convalescence time within the criterion of pain. For example, Delvaux et al. [31] stated that a complete relief of pain is the most important criterion, as it is assumed that the presence of pain would indicate an incomplete healing. However, is it really safe to say that the opposite is also true? Is it warranted to state that the absence of pain depicts completed healing of the injured muscle tissue? Silder et al. [32] showed that despite a normal clinical examination, clinicians should be aware of the ongoing muscle healing process. In that study, 25 subjects with a HSI underwent both a MRI assessment and a physical examination before and after the rehabilitation period. At RTP, despite the fact that all subjects showed a resolution of pain and restoration of muscle strength, no athlete showed a complete resolution of the HSI on MRI assessment [32]. Previous studies showed that the recovery parameters, measured within a physical examination, do not represent a complete muscle healing assessed on MRI, leading to the assumption that the functional recovery of the athlete precedes the structural recovery of the injured tissue [24, 32,33,34]. Therefore, even when an athlete feels completely healed (e.g. absence of pain), this will most likely not be the case for the injured muscle tissue in many cases. This conclusion raises another important question that should be faced. Namely, is a complete and thus terminated muscle healing necessary for a successful RTP? According to a previous study of Vermeulen et al. [35], this does not seem to be the case. First, it should be mentioned that the study of Vermeulen et al. agrees with the previously stated fact that at the moment of RTP (the moment that the athlete seems clinically recovered), MRI does not depict a complete resolution of the hamstring injury [32, 35]. However, the authors reported that the group of athletes that obtained a re-injury showed the same tissue discontinuities on MRI as the group of athletes that had a successful, (re)injury-free RTP [35]. Therefore, it seems that a complete resolution of the hamstring injury and thus a complete terminated biological healing is not necessary for an athlete to safely RTP [35]. This discussion inevitably leads to the million dollar question: “At what point is the hamstring muscle biologically and functionally ready to withstand the required sport-specific forces?”.

Criteria used for evaluating the return to play decision after hamstring injuries (based on data from van der Horst et al. [22])
To explain the high-reoccurrence rates of HSI by possible inadequate RTP criteria, it is imperative to know whether the RTP criteria used in sport science literature are being translated into the practical field. Via a worldwide survey, Dunlop et al. [36] assessed the RTP criteria used by the medical staff of 131 premier league football teams. The authors found that (1) absence of pain, (2) hamstring strength, (3) training load and (4) functional performance tests were the most commonly used criteria to decide whether an athlete is ready to resume his/her sport activities. A very small number (1–2%) of the respondents indicated the category ‘other’ (including e.g. medical imaging and time) as an important criterion at the moment of RTP. It is clear that both in science and in practice, time is rarely incorporated as an additional criterion within the RTP decision-making process. This raises the question whether or not the biological healing time is important to consider. Previous studies showed that muscle re-injuries are often more severe and therefore in need of a longer convalescence time, compared to the index injury [1, 3, 37]. It should be mentioned that is not clear whether more time is required for the biological healing or for other aspects (e.g. neuromuscular function). However, this inevitably entails detrimental effects on the athlete’s performance and overall physical health. At club level, this means that the number of days (and thus matches played) without full availability of the player for the team is at least doubled in case of a re-injury. Moreover, due to the unremittingly high reoccurrences, hamstring injuries continue to entail high annual expenses in health care (doctor consults, medical imaging, rehabilitation) [38]. Therefore, it is in everyone’s interest (athlete, sport club and society) to further investigate the current available RTP criteria and how to ameliorate them, in order to address the unremittingly high reoccurrences of HSIs. This analysis will further review if there is a need for the incorporation of biological healing time as an additional criterion within the current RTP test batteries. In doing so, the authors of this review adopted a synergistic approach to targeting this discussion. Thereby, it is important to state that the goal of this review is not to degrade and erase the current RTP criteria but to look for additional criteria that, hopefully, will make the future RTP clearance more safe.
4 Biological Healing of Muscle Tissue
When treating an injury of any possible kind, it is important for the clinician to bear in mind the healing process of the injured tissue. For example, in case of a bone fracture, the clinician will provide a cast for a period of 3–4 weeks. This is generally accepted because it has been shown that the bone healing is mature after 3–4 weeks (depending on the type of fracture). In case of muscle injuries, it seems that (based on the current RTP criteria) the duration of healing is considered less when evaluating the readiness of the player and thus the maturation status of the injured tissue. In contrast to bone tissue, which heals by a regeneration process, muscle tissue heals via the combination of a regeneration and repair process [28]. This type of healing is characterized by the regeneration of damaged muscle tissue together with the formation of scar tissue (repair) that replaces the original (injured) tissue [28] and comprises of three overlapping phases [25, 26, 28], depicted in Fig. 2. These phases are: (1) muscle degeneration and inflammation, (2) muscle regeneration, and (3) scar tissue formation [25, 26]. It should be mentioned that these phases are denominated differently in literature. For example, Järvinen et al. [28] intitles the three overlapping phases as (1) the destruction phase, (2) the repair phase, and (3) the remodeling phase. Nevertheless, every muscle injury consistently follows the same steps during the healing process. At the moment the muscle gets injured, a retraction of the ruptured myofibers occurs, leaving a gap between the myofiber stumps. As a result of the simultaneous blood vessel rupture, the gap becomes filled with hematoma [28, 39, 40]. A degeneration or necrotization of the ruptured myofibers occurs, controlled and contained by the so called contraction band (condensation of cytoskeletal material) [28, 39, 40]. This degeneration of injured muscle tissue induces, on its turn, an inflammatory response via the release of substances that serve as chemoattractants for the extravasation of inflammatory cells [28, 40,41,42]. In the first week after injury, once the degeneration or destruction phase is decreasing, the muscle repair begins with two simultaneous processes, (1) the regeneration of the ruptured myofibers (and nerves) and (2) the formation of connective tissue scar that acts as a bridge between the myofiber stumps [28, 40]. The muscle starts regenerating due to the activation and subsequent differentiation of quiescent satellite cells, which lay underneath the basement membrane, into myoblasts [28, 40, 43, 44]. Subsequently, these myoblasts fuse with each other to form multinucleated myotubes, which on its turn fuse with the preserved myofiber [43]. This process leads to the formation of newly formed myofibers. Muscle regeneration has shown to peak at 2 weeks and then decelerates 4 weeks after injury [25, 26].

Phases of muscle healing depicted in time (gray bars, based on Huard et al. [25, 26]), average return to play after a hamstring injury (dotted line box), recommended optimal moment of return to play (striped line box) and terminal endpoint of the muscle healing in time (arrow). The dotted bars depict the overlapping character of the healing stages. The three dots between the dotted bars of the regeneration and scar formation stage represent a long period of time
In addition to the regeneration process, scar tissue is gradually formed between the stumps [25, 28, 39, 40]. In the beginning, the blood clot that filled the gap between the ruptured myofibers starts to be disposed of by phagocytes that invade the hematoma [28, 39, 40]. Then, granulation tissue is formed by the cross-linking of blood-derived fibrin and fibronectin [28, 39, 40]. This early granulation tissue, that can be seen as a primary extracellular matrix (ECM), acts as an anchorage site for fibroblasts and provides the injured tissue with some early tensile strength to withstand applied contraction forces [28, 39, 40]. Later on, ECM proteins, such as tenascin-C (TN-C) and fibronectin, are synthesized by the fibroblasts [28, 39, 40, 45]. These elastic proteins simultaneously enhance the strength of the early scar tissue [45]. The deposition of TN-C is then followed by, among others, the synthesis of type III collagen [28, 40]. The formation of type I collagen starts later within the healing process and will play an important part in the tensile strength enhancement [46]. From day 5 after injury, multiple branches at ends of the regenerating myofiber stumps try to pierce through both sides of the scar tissue [28, 39, 40]. Until day 10–14, these stumps are not able to form a stable terminal connection with the intermediate scar tissue. Therefore, a reinforced lateral adhesion of the myofibers to the ECM is formed. Due to this lateral adhesion, stump movement and thus strain on the still fragile scar tissue is reduced [28, 39, 40]. Beginning at day 14, various new and small MTJs (so called mini-MTJs) are formed between the ends of the myofibers and the scar tissue [28, 39, 40]. With the clustering of integrin (among others) at these new MTJs, a terminal adhesion between the regenerated myofibers and the scar tissue is established [28, 39, 40, 45, 47]. From day 21, the scar tissue starts diminishing in size, bringing the myofiber stumps closer to each other which makes it possible for the myofibers to become interlaced [28, 40, 48]. From that moment on, the regenerating myofibers need to further mature until they reach a normal cross-striated appearance [40]. This means healing muscle acquires a mature form primarily after day 21, and thus after the player is usually sent back on the pitch. The maturation or remodeling phase is described by Järvinen et al. as the period in which the newly formed myofibers and scar tissue mature into fully regenerated muscle fibers together with well-organized, mature scar tissue [23, 24]. It is previously stated that this phase can continue until several months after the injury onset [49]. However, it is important to know that scar tissue is likely to permanently divide the muscle into two parts [28, 40].
An important goal of this review is to investigate when the injured tissue has regained enough strength to withstand high loads during sport participation. Therefore, it is imperative to highlight the evolution (during the healing process) of the tensile strength of the connective scar tissue and its newly formed connection with the regenerated myofibers (mini-MTJs). The strength of the scar tissue and adjacent mini-MTJs is mainly defined by two important biological phenomena, (1) cross-links between collagen type I fibers and (2) the expression of adhesion proteins/receptors [45,46,47]. The ratio of types III and type I collagen changes considerably during the healing process, with great implications for the scar tissue tensile strength [46]. In the early phase of healing, there is a significant increase in the formation of type III collagen [46]. This type of collagen fibrils has a much smaller diameter and thus lower tensile strength compared to type I fibrils, which results in inferior loading capacities compared to healthy muscle tissue (predominantly composed of type I collagen) [50, 51]. At this stage, the granulation tissue is predominantly composed of type III collagen and therefore the weakest point of the muscle [39]. The deposition of type III collagen persists to at least 2 weeks following injury and remains the dominant collagen type at 2 or 3 weeks after injury [52]. Therefore, in the beginning of the scar formation or repair phase, scar tissue is still disorganized as it matures over time (up to four weeks post-injury) [25, 26]. With time, the proportion of type I collagen fibers and thus the tensile strength of the scar tissue significantly increases [28, 46, 52]. In order to provide mechanical support and form a stress-bearing fiber, the collagen fibers must be highly cross-linked [46]. The formation of intermolecular cross-links is indispensable during the maturation of the scar tissue [46]. This is a late biological feature as it can solely take place after the production of strong collagen type I and thus after granulation tissue (rich of collagen type III) is replaced by stronger collagen type I fibers [46]. It is not sooner than 3 weeks after injury that ratio of type III/I collagen gradually shifts to a similar level seen in normal tissue [46]. Once the turnover of type III collagen reduces, type I collagen fibers can increase in size and form mature cross-links, and therefore start restoring the mechanical strength of the muscle tissue [46]. The moment when the newly formed scar tissue has gained enough strength (due to cross-link formation) to withstand the contraction force, the biomechanical weakest link shifts towards the interface between regenerating skeletal muscle fibers and the scar tissue (myofibers adjacent to the newly formed mini-MTJs) [28, 48]. This is also the location were most re-injuries take place after RTP [23]. This means that a strong connection between scar and muscle tissue needs to be formed. Therefore, the expression of strong adhesion proteins and receptors is required at the location of these mini-MTJs. The elastic protein TN-C and integrin α7β1 are abundantly expressed during the formation of granulation tissue but also during the regeneration of myofibers [45, 47]. From day 14, they play an important role in providing tensile strength at the side of the newly formed MTJs [45, 47]. This gradually increasing expression is imperative for ensuring a stable and inextensible connection between scare and muscle tissue, and thus for ensuring a good transmission of mechanical forces during heavy muscle contractions [28, 40, 45, 47]. A firm attachment cannot be formed until day 21, when integrin α7β1 is abundantly developed at the newly formed mini-MTJs [47].
It is clear that these two biological features (cross-linking and the expression of adhesive proteins) are imperative events during the tissue healing process and that they occur at a later stage in time. Therefore, it seems impossible that a stable, firm and mature muscle tissue (MTJs) is formed at the time players usually return to the pitch. Because these biological phenomena take place around day 21, a safe RTP cannot (biologically speaking) be guaranteed before week 4 after injury.
In conclusion, when considering the timeframe of the above-mentioned phases and biological features, it seems that the muscle healing process is slower than the average RTP (Fig. 2) [53]. Studies on biological muscle healing have shown that at 2 and 3 weeks post injury, which is the average moment of RTP after grade 1 and 2 hamstring injuries, the muscle regeneration and repair is still ongoing and both the new muscle fibers and scar tissue are still immature [25, 26, 28, 52]. Bearing this in mind, the high re-injury rates documented in the context of muscle injury are certainly not surprising given athletes are allowed to return to full-on competition after only 2–3 weeks of rehabilitation. At that point in time, the sport-specific forces may exceed those of the immature muscle and scar tissue. This is further supported by previous literature. Indeed, Wagensteen et al. [23] showed that, within the first 6 weeks after index injury, all re-injuries occur at the exact same location as the index injury and frequently (25%) within the first week after RTP. Interestingly, Askling et al. [54] found no re-injuries when players were allowed to RTP not earlier than an average time of 49–86 days. It should, however, be noticed that the population in the latter study included also grade 3 injuries, which has an impact on the average RTP time. So, when we allow a RTP after a hamstring injury at 2 or 3 weeks, we allow RTP in a time frame athletes are just not (biologically) ready to re-participate at pre-injury level. As a result, these premature RTP decisions continue to favor the ineluctable re-injury rates and their detrimental effects on the athlete’s level of performance, overall physical health and psychosocial wellbeing [55].
When determining the point of biological readiness of the newly formed tissue, it is important to define the term ‘biological readiness’. This term could be interpreted in two different ways: (1) the terminal endpoint of the active healing process of the injured tissue or (2) the moment (within the healing process) when the injured tissue is functionally healed to the extent that it can withstand the required sport-specific forces. As previously mentioned, the healing process could take months to reach its final endpoint [49]. No doctor or physiotherapist can sideline a player for months after a (grade 1 or 2) muscle injury, especially not when the player shows good function. However, we need to bear in mind that the goal of a successful RTP is to avoid re-injuries. Thus, the primary requirement is a tissue that is structurally capable of doing its duty without failing, regardless of whether or not the healing endpoint has been reached. As the strength of the newly formed tissue is defined by the stability and stress-bearing capacity of the scar tissue and the newly formed MTJs (the place where re-injuries take place), provided by the formation of cross-links between collagen type I fibers and the expression of adhesive proteins, the point in time where enough tensile strength is obtained seems primarily based on the timing of these two biological features [4, 28, 40, 45,46,47]. As these processes take place around day 21, a strong inextensible (pre-injury resembling) tissue cannot be formed before a period of 4 weeks [45, 47]. Therefore, we suggest a shift from the current average RTP moment (between 2 and 3 weeks) to a new moment of RTP that respects the minimal biological healing time of 4 weeks, reflecting a strong newly formed muscle tissue (Fig. 2).
5 Towards a New Mindset for Return to Play
As a first step in the attempt to reduce the detrimental injury–reinjury cycle, it is time to consider (biological healing) time. We advocate the incorporation of the natural healing time within the existing functional RTP testing batteries. Based on the tissue biological healing process, we recommend a minimum rehabilitation period of 4 weeks before considering RTP clearance in case of a grade 1 and 2 hamstring muscle injury. It is important to mention that the size or severity of the strain is correlated with the convalescence time of the muscle injury [33]. The most common HSIs are grade 1 and 2 lesions [56]. A distinction in biological healing time should be made as the extent of the injury is larger in grade 2 injuries (fiber disruption of less than 5 cm) compared to grade 1 injuries (fiber disruption of less than 1 cm) [57]. The fact that grade 2 injuries will need more time to form a strong and firm muscle tissue seems logical as the initial gap formed between the ruptured myofibers will be larger and more scar tissue needs to formed, requiring a larger formation of strong (highly cross-linked) collagen fibers and a more extensive expression of adhesive proteins. As the size of the scar tissue will be larger in grade 2 injuries, the process of scar tissue size reduction and synchronized progression of myofibril interlacing will take significantly more time. Therefore, it seems logical to state that the greater the extent of the lesion, the longer the time needed to heal and thus the longer the time needed to RTP. This is in line with a recent study that emphasized the fact that it is primarily the amount of damage caused to the connective tissue that defines the length of the RTP time [58]. However, biological studies regarding the healing process of the different grades of muscle injuries are scarce. This means that it is not clear how much longer it takes for a grade 2 injury (compared to a grade 1 injury) to reach the point of scar and muscle tissue maturity. Therefore, we recommend a minimum period of 4 weeks before considering RTP after both grade 1 and 2 HSIs. We acknowledge the fact that this could mean that for some players with a grade 1 injury, this period is perhaps somewhat longer than strictly needed. However, we think it is better to wait a little longer than to increase the risk of a premature RTP.
We should also bear in mind that the healing process of muscle tissue, or any kind of tissue for that matter, is inter-individually highly variable. Therefore, it is important to note that these are general guidelines and that the clinician should always adopt an individualized approach for each patient. This individual approach should be guided by the current RTP tests and criteria. When a player with a grade 1 or 2 HSI does not pass the current criteria (e.g. pain on palpation or strength deficits) after 4 weeks, it could be assumed that the injured muscle tissue has not reached the point of forming a mature stress-bearing tissue (despite the 4 weeks). However, as discussed before, the converse is equally important. When the player shows good function but the minimal time period of 4 weeks has not past yet, it could be stated that it is too early (biologically speaking) for RTP clearance. This highlights the need for a synergistic relationship between the current RTP criteria and the additional (biological) time criterion. Furthermore, the location of the injury has also some important implications with regard to the injury healing time. Pollock et al. [59] showed that the time needed to return to full training is significantly longer in intratendinous hamstring injuries, with an even longer duration in the more severe grades of tendon injuries. This seems intuitive as the tendon healing occurs in a different and slower way to muscle healing [59]. This was supported by van der Made et al. [60], who found that hamstring injuries with intramuscular tendon involvement had a delay in RTP of approximately a week. However, the authors of this study concluded that the clinical value of this finding is limited due to the great overlap in RTP between athletes with or without tendon involvement [60]. To date, the role of intramuscular tendon involvement and its impact on the RTP time is still controversial. Lastly, previous studies have shown that different injury mechanisms have a different prognosis [13, 61], also necessitating clinicians to take the exact injury mechanism into account in deciding when an athlete can be safely allowed to participate at the pre-injury level of competition. Askling et al. [61] defined two main types of hamstring injuries; the high-speed running and stretching type. It has been demonstrated that the high-speed running type requires a shorter rehabilitation time compared to the stretching type [62]. One of the possible explanations for this finding might be the fact that the injury location has been shown to have a significant association with the injury mechanism. The high-speed running type mostly involves the proximal muscle–tendon junction of the biceps femoris (long head), whereas the stretching type mainly involves tendon tissue of the semimembranosus [63, 64]. Thus, the longer convalescence time seen in the stretching type HSI, compared to the high-speed running type, seems attributable to the difference in tissue involvement (more tendon in stretching type, more muscle in high-speed running type), rather than the biomechanical circumstances in which the lesion occurred. Due to the inconsistencies in current literature regarding the impact of tendon involvement on RTP time and the scarcity of biological studies on the healing process of such injuries, it impossible to give specific and conclusive recommendations. Therefore, the evidence-based recommendations made in this review focus on the most common grade 1 and 2 HSIs.
The authors of this review propose a new approach for deciding RTP readiness of the athlete. Based on biological studies, it is clear that biological healing time should be respected and should therefore be incorporated within the current RTP criteria. As a clinical guideline we propose a flowchart that could help guide clinicians in the RTP decision-making process (Fig. 3). In the first step, the clinician must reflect whether the biological healing time is respected and thus if it is (biologically) possible that the injured tissue has regained enough strength to withstand the sport-specific forces. The second step depicts the current RTP practice, evaluating the functional readiness of the player based on the well-known test criteria [19, 20, 22]. Naturally, new clinical studies are needed to further refine and complete this approach.

Flowchart: new approach for deciding return to play readiness
6 (How) Can We Monitor the Muscle Healing Process?
Time should play a crucial role within the RTP criteria. However, in clinical practice we notice that the healing process, and thus convalescence time, shows some variability between athletes. This raises an important question: can serial assessment via medical imaging help clinicians to evaluate if the newly formed tissue has gained enough strength to withstand the sport-specific forces? Physicians from elite teams tend to use MR imaging of the injured muscle to evaluate the rehabilitation and guide its progress [24]. However, this technique is practically and financially not feasible to use, especially within the non-elite athlete population. More importantly, a recent study from Vermeulen et al. [35] showed that a MRI-scan at the moment of RTP has limited benefit, as a complete resolution of an intratendinous hamstring injury does not necessarily predict a successful RTP. Based on previous studies [65, 66], MRI assessment has already been excluded as a potential criterion within the RTP decision making process by a panel of international experts [20]. Previous studies indicated that MRI-scans tend to show abnormalities for a substantial period after the injury occurred [33, 64]. This is in line with the previously mentioned fact that the muscle healing process could take months to reach its final endpoint. Naturally, it is not possible (for a player or clinician) to wait until MRI shows no abnormalities at all before considering RTP. A clinician should be able to pinpoint the exact moment in time where the newly formed tissue has regained enough strength to withstand the high sport-specific forces. However, it appears that this could be problematic for the currently used imaging techniques. It seems that (with currently used imaging techniques such as MRI) we cannot get a quantitative measurement that tells us whether or not this crucial point has been reached (because in most cases, there will be abnormalities on MRI at the moment of RTP). In addition, some biological features that take place during the muscle healing process (e.g. the formation of type I collagen fibers, cross-linking between collagen fibers and the expression of adhesive proteins) are imperative for the formation of strong and mature muscle and scar tissue. These processes cannot be detected via MRI assessment but are imperative for a safe RTP. Therefore, is seems that MRI is not able to pinpoint the exact moment in time when the newly formed tissue is properly matured and capable of withstanding the sport-specific requirements. Another frequently used imaging tool to diagnose acute muscle injuries is sonography. While the sonographic technique is less expensive than MRI, it is also has some shortcomings for the follow-up of the healing process of the injured muscle [33]. For example, abnormalities tend to resolve faster on sonographic assessment than on MRI. At 2 and 6 weeks after injury, sonography detected fewer abnormalities than MRI [33]. Whereas the identification of muscle tears during healing requires the illustration of subtle alterations in echotexture, sonography has lower contrast resolution than MRI [33]. In conclusion, it seems that current medical imaging methods used for the diagnosis and prognosis in the context of muscle injury lack sensitivity to provide conclusive evidence and quantitative information regarding the tissue’s stress-bearing capacities, and are therefore not able to identify the exact point in time when the muscle tissue is ready to safely RTP. At RTP, medical imaging has indeed been shown to fail to add value to the decision-making process [66]. Therefore, we advocate the adherence to generic timeframes for grade 1 and 2 injuries. We acknowledge that when keeping the individual variation of the tissue healing rate in mind, these generic time frames could mean that some athletes stay ‘ashore’ too long. However, clinicians must ultimately protect the health of the athletes above all. That is why it seems justified to state that it is better to wait a little longer to send a player back on the pitch, than to increase the re-injury risk allowing premature RTP. Interestingly, new technologies are being developed and tested as we write. A promising upcoming tool for the evaluation of (scar) tissue maturation could be shear wave elastography (SWE). This ultrasound-based technique can measure soft tissue stiffness that changes during healing processes, and can be measured in real time [67,68,69,70]. Therefore, it could be used to diagnose and monitor musculoskeletal injuries [67]. Indeed, Yoshida et al. [71] successfully used SWE for objectifying the healing process of a gastrocnemius muscle injury. It seems that SWE could be used as a quantitative measurement of the changes in stiffness during the muscle healing process (with the healthy side as reference). This could be important as the stiffness at the site of previous injury (site of scar tissue formation) is assumed to be related to the risk of injury reoccurrence. However, due to the scarcity of studies in the current literature, further research is needed to verify whether or not SWE might be a valuable tool to monitor the healing process of the injured muscle tissue. This could provide clinicians with the possibility to evaluate both the athlete’s and the muscle tissue’s readiness to return to pre-injury-level sports activities and therefore finally enable evidence-based justification of RTP.
7 Conclusion
The current state of the art shows that the criterion of biological healing time is disregarded within the RTP decision after a hamstring strain injury. Basic science studies on muscle healing affirm that athletes are allowed to return to play when the injured structures are not yet mature. At the average moment of RTP, the muscle healing process is ongoing and scar tissue is still immature, leading to unremittingly high reoccurrences of re-injuries. We recommend a comprehensive RTP functional test battery, as described in literature and used commonly by most clinicians, with adherence to the natural healing process of the injured tissue. As a first step in the attempt to reduce the detrimental injury–reinjury cycle, it is time to consider (the biological healing) time. Before deciding RTP readiness of the athlete, clinicians should reflect whether or not it is biologically possible for the injured tissue to have regained enough strength to withstand the sport-specific forces (despite good function according to the current RTP criteria). As a general guideline, the authors of the present review suggest a minimum period of 4 weeks before RTP after a grade 1 and 2 hamstring injury. The presented timeframe could be a mainstay for clinicians and other stakeholders when making a RTP decision.
References
Brooks JH, Fuller CW, Kemp SP, Reddin DB. Incidence, risk, and prevention of hamstring muscle injuries in professional rugby union. Am J Sports Med. 2006;34(8):1297–306.
Carling C, Orhant E, LeGall F. Match injuries in professional soccer: inter-seasonal variation and effects of competition type, match congestion and positional role. Int J Sports Med. 2010;31(4):271–6.
Ekstrand J, Hagglund M, Walden M. Epidemiology of muscle injuries in professional football (soccer). Am J Sports Med. 2011;39(6):1226–32.
Ekstrand J, Hagglund M, Walden M. Injury incidence and injury patterns in professional football: the UEFA injury study. Br J Sports Med. 2011;45(7):553–8.
Hagglund M, Walden M, Ekstrand J. Injury incidence and distribution in elite football—a prospective study of the Danish and the Swedish top divisions. Scand J Med Sci Sports. 2005;15(1):21–8.
Opar DA, Williams MD, Shield AJ. Hamstring strain injuries: factors that lead to injury and re-injury. Sports Med. 2012;42(3):209–26.
Walden M, Hagglund M, Ekstrand J. UEFA Champions League study: a prospective study of injuries in professional football during the 2001–2002 season. Br J Sports Med. 2005;39(8):542–6.
Woods C, Hawkins RD, Maltby S, Hulse M, Thomas A, Hodson A, et al. The Football Association Medical Research Programme: an audit of injuries in professional football–analysis of hamstring injuries. Br J Sports Med. 2004;38(1):36–41.
van Beijsterveldt AMC, van de Port IGL, Krist MR, Schmikli SL, Stubbe JH, Frederiks JE, et al. Effectiveness of an injury prevention programme for adult male amateur soccer players: a cluster-randomised controlled trial. Br J Sport Med. 2012;46(16):1114.
Orchard J, Best TM. The management of muscle strain injuries: an early return versus the risk of recurrence. Clin J Sport Med. 2002;12(1):3–5.
Orchard J, Seward H. Epidemiology of injuries in the Australian Football League, seasons 1997–2000. Br J Sports Med. 2002;36(1):39–44.
Eliakim E, Morgulev E, Lidor R, Meckel Y. Estimation of injury costs: financial damage of English Premier League teams’ underachievement due to injuries. BMJ Open Sport Exerc Med. 2020;6(1):e000675.
Askling CM, Tengvar M, Thorstensson A. Acute hamstring injuries in Swedish elite football: a prospective randomised controlled clinical trial comparing two rehabilitation protocols. Br J Sports Med. 2013;47(15):953–9.
Ekstrand J, Krutsch W, Spreco A, van Zoest W, Roberts C, Meyer T, et al. Time before return to play for the most common injuries in professional football: a 16-year follow-up of the UEFA Elite Club Injury Study. Br J Sports Med. 2020;54(7):421–6.
Ekstrand J, Walden M, Hagglund M. Hamstring injuries have increased by 4% annually in men’s professional football, since 2001: a 13-year longitudinal analysis of the UEFA Elite Club injury study. Br J Sports Med. 2016;50(12):731–7.
Bourne MN, Timmins RG, Opar DA, Pizzari T, Ruddy JD, Sims C, et al. An evidence-based framework for strengthening exercises to prevent hamstring injury. Sports Med. 2018;48(2):251–67.
Brukner P. Hamstring injuries: prevention and treatment-an update. Br J Sports Med. 2015;49(19):1241–4.
van Dyk N, Behan FP, Whiteley R. Including the Nordic hamstring exercise in injury prevention programmes halves the rate of hamstring injuries: a systematic review and meta-analysis of 8459 athletes. Br J Sports Med. 2019;53(21):1362–70.
Ardern CL, Glasgow P, Schneiders A, Witvrouw E, Clarsen B, Cools A, et al. 2016 Consensus statement on return to sport from the first world congress in sports physical therapy. Bern Br J Sports Med. 2016;50(14):853–64.
van der Horst N, Backx F, Goedhart EA, Huisstede BM, Group HI-D. Return to play after hamstring injuries in football (soccer): a worldwide Delphi procedure regarding definition, medical criteria and decision-making. Br J Sports Med. 2017;51(22):1583–91.
Zambaldi M, Beasley I, Rushton A. Return to play criteria after hamstring muscle injury in professional football: a Delphi consensus study. Br J Sports Med. 2017;51(16):1221–6.
van der Horst N, van de Hoef S, Reurink G, Huisstede B, Backx F. Return to play after hamstring injuries: a qualitative systematic review of definitions and criteria. Sports Med. 2016;46(6):899–912.
Wangensteen A, Tol JL, Witvrouw E, Van Linschoten R, Almusa E, Hamilton B, et al. Hamstring reinjuries occur at the same location and early after return to sport: a descriptive study of MRI-confirmed reinjuries. Am J Sports Med. 2016;44(8):2112–21.
Flores DV, Mejia Gomez C, Estrada-Castrillon M, Smitaman E, Pathria MN. MR imaging of muscle trauma: anatomy, biomechanics, pathophysiology, and imaging appearance. Radiographics. 2018;38(1):124–48.
Huard J, Li Y, Fu FH. Muscle injuries and repair: current trends in research. J Bone Joint Surg Am. 2002;84(5):822–32.
Huard J, Lu A, Mu X, Guo P, Li Y. Muscle injuries and repair: what’s new on the horizon! Cells Tissues Organs. 2016;202(3–4):227–36.
Jarvinen TA, Jarvinen M, Kalimo H. Regeneration of injured skeletal muscle after the injury. Muscles Ligaments Tendons J. 2013;3(4):337–45.
Jarvinen TA, Jarvinen TL, Kaariainen M, Kalimo H, Jarvinen M. Muscle injuries: biology and treatment. Am J Sports Med. 2005;33(5):745–64.
Hallen A, Ekstrand J. Return to play following muscle injuries in professional footballers. J Sports Sci. 2014;32(13):1229–36.
Kilcoyne KG, Dickens JF, Keblish D, Rue JP, Chronister R. Outcome of grade I and II hamstring injuries in intercollegiate athletes: a novel rehabilitation protocol. Sports Health. 2011;3(6):528–33.
Delvaux F, Rochcongar P, Bruyere O, Bourlet G, Daniel C, Diverse P, et al. Return-to-play criteria after hamstring injury: actual medicine practice in professional soccer teams. J Sports Sci Med. 2014;13(3):721–3.
Silder A, Sherry MA, Sanfilippo J, Tuite MJ, Hetzel SJ, Heiderscheit BC. Clinical and morphological changes following 2 rehabilitation programs for acute hamstring strain injuries: a randomized clinical trial. J Orthop Sports Phys Ther. 2013;43(5):284–99.
Connell DA, Schneider-Kolsky ME, Hoving JL, Malara F, Buchbinder R, Koulouris G, et al. Longitudinal study comparing sonographic and MRI assessments of acute and healing hamstring injuries. AJR Am J Roentgenol. 2004;183(4):975–84.
Schneider-Kolsky ME, Hoving JL, Warren P, Connell DA. A comparison between clinical assessment and magnetic resonance imaging of acute hamstring injuries. Am J Sports Med. 2006;34(6):1008–15.
Vermeulen R, Almusa E, Buckens S, Six W, Whiteley R, Reurink G, et al. Complete resolution of a hamstring intramuscular tendon injury on MRI is not necessary for a clinically successful return to play. Br J Sports Med. 2020;2020:5.
Dunlop G, Ardern CL, Andersen TE, Lewin C, Dupont G, Ashworth B, et al. Return-to-play practices following hamstring injury: a worldwide survey of 131 premier league football teams. Sports Med. 2020;50(4):829–40.
Walden M, Hagglund M, Ekstrand J. Injuries in Swedish elite football–a prospective study on injury definitions, risk for injury and injury pattern during 2001. Scand J Med Sci Sports. 2005;15(2):118–25.
Hickey J, Shield AJ, Williams MD, Opar DA. The financial cost of hamstring strain injuries in the Australian Football League. Br J Sports Med. 2014;48(8):729–30.
Hurme T, Kalimo H, Lehto M, Jarvinen M. Healing of skeletal muscle injury: an ultrastructural and immunohistochemical study. Med Sci Sports Exerc. 1991;23(7):801–10.
Kaariainen M, Jarvinen T, Jarvinen M, Rantanen J, Kalimo H. Relation between myofibers and connective tissue during muscle injury repair. Scand J Med Sci Sports. 2000;10(6):332–7.
Chazaud B, Sonnet C, Lafuste P, Bassez G, Rimaniol AC, Poron F, et al. Satellite cells attract monocytes and use macrophages as a support to escape apoptosis and enhance muscle growth. J Cell Biol. 2003;163(5):1133–43.
Tidball JG. Inflammatory cell response to acute muscle injury. Med Sci Sports Exerc. 1995;27(7):1022–32.
Hurme T, Kalimo H. Activation of myogenic precursor cells after muscle injury. Med Sci Sports Exerc. 1992;24(2):197–205.
Rantanen J, Hurme T, Lukka R, Heino J, Kalimo H. Satellite cell proliferation and the expression of myogenin and desmin in regenerating skeletal muscle: evidence for two different populations of satellite cells. Lab Invest. 1995;72(3):341–7.
Jarvinen TA, Kannus P, Jarvinen TL, Jozsa L, Kalimo H, Jarvinen M. Tenascin-C in the pathobiology and healing process of musculoskeletal tissue injury. Scand J Med Sci Sports. 2000;10(6):376–82.
Lehto M, Sims TJ, Bailey AJ. Skeletal muscle injury–molecular changes in the collagen during healing. Res Exp Med (Berl). 1985;185(2):95–106.
Kaariainen M, Nissinen L, Kaufman S, Sonnenberg A, Jarvinen M, Heino J, et al. Expression of alpha7beta1 integrin splicing variants during skeletal muscle regeneration. Am J Pathol. 2002;161(3):1023–31.
Kaariainen M, Kaariainen J, Jarvinen TL, Sievanen H, Kalimo H, Jarvinen M. Correlation between biomechanical and structural changes during the regeneration of skeletal muscle after laceration injury. J Orthop Res. 1998;16(2):197–206.
Delos D, Maak TG, Rodeo SA. Muscle injuries in athletes: enhancing recovery through scientific understanding and novel therapies. Sports Health. 2013;5(4):346–52.
Stauber WT, Knack KK, Miller GR, Grimmett JG. Fibrosis and intercellular collagen connections from four weeks of muscle strains. Muscle Nerve. 1996;19(4):423–30.
Wiedemann H, Chung E, Fujii T, Miller EJ, Kuhn K. Comparative electron-microscope studies on type-III and type-I collagens. Eur J Biochem. 1975;51(2):363–8.
Best TM, Shehadeh SE, Leverson G, Michel JT, Corr DT, Aeschlimann D. Analysis of changes in mRNA levels of myoblast- and fibroblast-derived gene products in healing skeletal muscle using quantitative reverse transcription-polymerase chain reaction. J Orthop Res. 2001;19(4):565–72.
McCall A, Carling C, Nedelec M, Davison M, Le Gall F, Berthoin S, et al. Risk factors, testing and preventative strategies for non-contact injuries in professional football: current perceptions and practices of 44 teams from various premier leagues. Br J Sports Med. 2014;48(18):1352–7.
Askling CM, Tengvar M, Tarassova O, Thorstensson A. Acute hamstring injuries in Swedish elite sprinters and jumpers: a prospective randomised controlled clinical trial comparing two rehabilitation protocols. Br J Sports Med. 2014;48(7):532–9.
Hagglund M, Walden M, Magnusson H, Kristenson K, Bengtsson H, Ekstrand J. Injuries affect team performance negatively in professional football: an 11-year follow-up of the UEFA Champions League injury study. Br J Sports Med. 2013;47(12):738–42.
Liu H, Garrett WE, Moorman CT, Yu B. Injury rate, mechanism, and risk factors of hamstring strain injuries in sports: a review of the literature. J Sport Health Sci. 2012;1(2):92–101.
Pollock N, James SL, Lee JC, Chakraverty R. British athletics muscle injury classification: a new grading system. Br J Sports Med. 2014;48(18):1347–51.
Study Group of the Muscle and Tendon System from the Spanish Society of Sports Traumatology, Balius R, Blasi M, Pedret C, Alomar X, et al. A histoarchitectural approach to skeletal muscle injury: searching for a common nomenclature. Orthop J Sports Med. 2020;8(3):2325967120909090.
Pollock N, Patel A, Chakraverty J, Suokas A, James SL, Chakraverty R. Time to return to full training is delayed and recurrence rate is higher in intratendinous ('c’) acute hamstring injury in elite track and field athletes: clinical application of the British Athletics Muscle Injury Classification. Br J Sports Med. 2016;50(5):305–10.
van der Made AD, Almusa E, Whiteley R, Hamilton B, Eirale C, van Hellemondt F, et al. Intramuscular tendon involvement on MRI has limited value for predicting time to return to play following acute hamstring injury. Br J Sports Med. 2018;52(2):83–8.
Askling CM, Malliaropoulos N, Karlsson J. High-speed running type or stretching-type of hamstring injuries makes a difference to treatment and prognosis. Br J Sports Med. 2012;46(2):86–7.
Askling C, Saartok T, Thorstensson A. Type of acute hamstring strain affects flexibility, strength, and time to return to pre-injury level. Br J Sports Med. 2006;40(1):40–4.
Askling CM, Tengvar M, Saartok T, Thorstensson A. Acute first-time hamstring strains during slow-speed stretching: clinical, magnetic resonance imaging, and recovery characteristics. Am J Sports Med. 2007;35(10):1716–24.
Askling CM, Tengvar M, Saartok T, Thorstensson A. Acute first-time hamstring strains during high-speed running: a longitudinal study including clinical and magnetic resonance imaging findings. Am J Sports Med. 2007;35(2):197–206.
De Vos RJ, Reurink G, Goudswaard GJ, Moen MH, Weir A, Tol JL. Clinical findings just after return to play predict hamstring re-injury, but baseline MRI findings do not. Br J Sports Med. 2014;48(18):1377–84.
Reurink G, Whiteley R, Tol JL. Hamstring injuries and predicting return to play: “bye-bye MRI?” Br J Sports Med. 2015;49(18):1162–3.
Brandenburg JE, Eby SF, Song P, Zhao H, Brault JS, Chen S, et al. Ultrasound elastography: the new frontier in direct measurement of muscle stiffness. Arch Phys Med Rehabil. 2014;95(11):2207–19.
Eby SF, Song P, Chen S, Chen Q, Greenleaf JF, An KN. Validation of shear wave elastography in skeletal muscle. J Biomech. 2013;46(14):2381–7.
Schmalzl J, Fenwick A, Boehm D, Gilbert F. The application of ultrasound elastography in the shoulder. J Shoulder Elbow Surg. 2017;26(12):2236–46.
Sigrist RMS, Liau J, Kaffas AE, Chammas MC, Willmann JK. Ultrasound elastography: review of techniques and clinical applications. Theranostics. 2017;7(5):1303–29.
Yoshida K, Itoigawa Y, Maruyama Y, Kaneko K. Healing process of gastrocnemius muscle injury on ultrasonography using B-mode imaging, power Doppler imaging, and shear wave elastography. J Ultrasound Med. 2019;38(12):3239–46.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No sources of funding were used to assist in the preparation of this article.
Conflicts of interest/competing interests
Dries Pieters, Evi Wezenbeek, Joke Schuermans and Erik Witvrouw declare that they have no conflicts of interest relevant to the content of this review.
Availability of data and material
Not applicable.
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Authors' contributions
All authors had a substantial role in writing this manuscript and approved the final version to be submitted.
Rights and permissions
About this article

Cite this article
Pieters, D., Wezenbeek, E., Schuermans, J. et al. Return to Play After a Hamstring Strain Injury: It is Time to Consider Natural Healing. Sports Med 51, 2067–2077 (2021). https://doi.org/10.1007/s40279-021-01494-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-021-01494-x