
Abstract
Background
The acute: chronic workload ratio (ACWR) is an index of the acute workload relative to the cumulative chronic workloads. The monitoring of physical workloads using the ACWR has emerged and been hypothesized as a useful tool for coaches and athletes to optimize performance while aiming to reduce the risk of potentially preventable load-driven injuries.
Objectives
Our goal was to describe characteristics of the ACWR and investigate the association of the ACWR with the risk of time-loss injuries in adult elite team sport athletes.
Data sources
PubMed, EMBASE and grey literature databases; inception to May 2019.
Eligibility criteria
Longitudinal studies that assess the relationship of the ACWR and time-loss injury risk in adult professional or elite team sports.
Methods
We summarized the population characteristics, workload metrics and ACWR calculation methods. For each workload metric, we plotted the risk estimates for the ACWR in isolation, or when combined with chronic workloads. Methodological quality was assessed using a modified version of the Downs and Black scale.
Results
Twenty studies comprising 2375 injuries from 1234 athletes (all males and mean age of 24 years) from different sports were included. Internal (65%) and external loads (70%) were collected in more than half of the studies and the session-rating of perceived exertion and total distance were the most commonly collected metrics. The ACWR was commonly calculated using the coupled method (95%), 1:4 weekly blocks (95%) and subsequent week injury lag (80%). There were 14 different binning methods with almost none of the studies using the same binning categories.
Conclusion
The majority of studies suggest that athletes are at greater risk of sustaining a time-loss injury when the ACWR is higher relative to a lower or moderate ACWR. The heterogenous methodological approaches not only reflect the wide range of sports studied and the differing demands of these activities, but also limit the strength of recommendations.
PROSPERO registration number
CRD42017067585.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
A higher acute: chronic workload ratio in relation to a lower or moderate acute: chronic workload ratio suggests a greater risk of sustaining a time-loss injury. No clear association was observed for a low acute: chronic workload ratio in terms of injury risk. |
A low chronic load combined with a high acute: chronic workload ratio may increase the risk of injury, although the number of studies addressing these combinations is limited. |
The review highlighted a wide variation in methodologies, especially in regard to the definitions for workload categories. Researchers should clearly report and justify the methods they use for data structuring and analysis. Practitioners should be aware of the methodological divergence associated with research on acute: chronic workl oad ratio and injuries when interpreting published studies and adapting to their own context. |
1 Introduction
Sport injuries are complex and multifactorial. There is no linear causal relationship between a single risk factor and injury, but rather an interaction of a complex web of several different internal and external factors that act together to predispose an athlete to injury [1, 2]. While some risk factors are non-modifiable (e.g. history of previous injury, age, sex and genetic predisposition), there are also modifiable risk factors (e.g. aerobic fitness, strength and exposure to workloads) that can be manipulated to reduce injury risk [3].
Workloads involve the cumulation of physical and psychological stress from training and match exposures over a period of time [4] and can be regarded as a “vehicle” that can either drive the athlete towards or away from sports injury [5]. Workload monitoring has been widely implemented in sports teams to identify athletes at higher risk of injury, or training practices that have the potential to enhance performance or decrease the risk of injury [6,7,8,9,10]. Numerous studies have investigated the association of workloads and risk of sports injuries [4, 11,12,13,14,15,16]. While absolute workloads explore the association of cumulative loads with injury, relative loads compare the load an athlete is currently undergoing (the acute load) to what the athlete is prepared for (the chronic load). The acute:chronic workload ratio (ACWR) is used as an index of the current workload (acute) relative to the workload that the athlete is prepared for (cumulative chronic workload) [17]. From a biological perspective, if the athlete does not recover sufficiently after a training stimulus to allow the affected structures to adapt, they may move towards fatigue, injury and/or illness rather than improved performance [18]. Recent evidence suggests that higher ACWR combined with low cumulative chronic workloads [19,20,21,22] and rapid increases in player load (week-to-week changes, i.e. a “spike” in workload [19, 23]) expose the athlete to load that they may not be prepared for, predisposing the athlete to a higher risk of injury.
Understanding the workload–injury relationship is fundamental for coaches, sports scientists and sports medicine clinicians to optimize performance while reducing the risk of potentially preventable load-driven injuries. The ACWR is a modelling approach that is used to monitor the relative changes in workload in which the athlete has been exposed over time and examine workload incidents (rapid increases or decreases) that may suggest increased risk of injury. Despite the growing body of scientific evidence pinpointing the role of load changes in injury risk, we must ask ourselves: (1) Is the concept that the load applied relative to the load an athlete is prepared for a biologically plausible model to explain workload-related injuries? And (2) does the magnitude of change in load increase injury risk? Our goal was to investigate the relationship between changes in workloads (using the ACWR) and the risk of injuries in team sport athletes. We performed a systematic review that describes the characteristics of the ACWR calculation and its association with time-loss injuries in adult competitive team sports.
2 Methods
The systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [24]. The protocol for this systematic review was a priori registered at the International Prospective Register of Systematic Reviews (PROSPERO) with the number CRD42017067585.
2.1 Search Strategy
We conducted a comprehensive database search using PubMed and EMBASE to search for longitudinal studies that assessed the relation of ACWR and injury risk in the athletic population. We also used the OpenGrey database to search for grey literature. The search strategy can be seen in Electronic Supplementary Material Appendix S1. All searches were performed from database inception up to 31 May 2019. The reference lists of the most relevant reviews and consensus statements were scanned for additional studies.
2.2 Study Selection
We exported all references to EndNote X7 (Thomson and Reuters) and removed duplicates using the software command ‘find duplicates’ and by manually checking all references. Two authors (R. A. and A. R. M.) screened all non-duplicated titles and abstracts for relevant articles according to inclusion and exclusion criteria and retrieved the full text of relevant studies for further analysis. Any disagreement was resolved by a third reviewer (T. G.). The inclusion criteria comprised: (1) assessment of the ratio between acute and chronic volume- or intensity-based physical workloads (ACWR) and association with risk and/or incidence of primary sports injury; (2) includes professional or elite athletes; (3) adult population (age over 18 years); (4) applied a longitudinal study design with prospective collection of workload and injury data; (5) assesses only time-loss injuries; (6) entails at least a full playing season. Time-loss injuries were defined as physical complaints that resulted in a player missing a training session and/or match. No language restrictions were applied. We applied the following exclusion criteria: (1) other reviews or meta-analyses; (2) editorials, clinical commentaries, expert opinions or letters to the editor; (3) single case studies or case series under ten participants; (4) children and adolescents (under 18 years old); (5) studies that include overlapping samples. In the case of overlapping samples, the study first published was included.
2.3 Data Extraction
Two independent authors (R. A. and E. H. W.) performed all the data extraction and collection and a third author (T. G.) was consulted if a decision could not be reached. Corresponding authors from included studies were contacted to resolve any unclear or missing data. We extracted and summarized the characteristics of population (number of athletes and athletes per season, sex and age), sports participation (type of sport, level of competition and number of teams and seasons), injury characteristics (type, number and who diagnosed and recorded injuries), workload metrics (methods for recording and which internal and external workload metrics were used). Internal loads comprise the athlete physiological status (e.g. heart rate or blood lactate concentration) and/or their perceived responses to workload measured by the 10-point modified-Borg session-rating of perceived exertion (sRPE). The product of sRPE and duration (min) provides a measure of “internal load”. External loads involve physical workloads (frequency, intensity and volume) performed by the athlete that can be measured by the amount of repetitive sport-specific activities (e.g., number of throws or pitches) or running-related metrics (e.g., total distance covered, accelerations and decelerations, distances covered at high-intensity) that can be tracked by global positioning systems (GPS) and inertial measurement sensors (e.g. wearable accelerometer devices). To date, there is no consensus in the literature on definitions of sprinting, or low, moderate, and high-intensity running as measured from GPS devices [25]. To allow for comparison and harmonize the metrics that measured the distance covered under specific running intensities, we standardized according to low-intensity running (< 6 km/h), moderate-intensity running (6–18 km/h), high-intensity running (18–24 km/h) and sprinting (> 24 km/h).
The ACWR calculation characteristics, risk estimates of ACWR and injury and statistical methods for calculating the risk estimates were also collected. We considered the ACWR data structure (coupled vs. uncoupled methods and weekly vs. daily blocks), the acute and chronic windows (in weeks or days), the binning methods and reference category of the ACWR, and the injury lag period used for calculation. The ACWR data structure was also registered according to the calculation method used: rolling averages and/or exponentially weighted moving averages (EWMA). The rolling averages model is calculated by dividing the absolute ("rolling") acute workload divided by the average chronic workload, which suggests that the workload in acute and chronic periods is equal and the association with injury is linear. The EWMA model assigns an increasing weighting to the more recent daily workload values to compensate the latency effects, assuming a non-linear relationship with injury [26]. The binning method refers to the method used to group the workload categories (standard increases in load, z scores, percentiles, tertiles/quintiles/quantiles or arbitrary bins) and the reference category (if any) is the workload category that serves as reference to which the other categories will be compared. We extracted the binning methods and reference category exactly as reported in the included studies. We extracted the findings of association of ACWR with injury risk according to the injury risk estimates reported in the included studies (relative risk, odds ratio, incidence risk ratio or hazard ratio) and sub-grouped according to the ACWR in isolation, or in combination with low/high chronic workloads. We scored the findings according to their statistical significance (if P < 0.05 and the 90% or 95% confidence intervals did not include the value 1) for each workload metric and according to ACWR reference categories. Scoring was based on the direction of result and coded as “↑” if representing a statistically increased risk condition, “↓” if representing a statistically decreased risk condition and “ ↔ ” if no statistical association was found.
2.4 Methodological Quality Assessment
The methodological quality of all included articles was assessed using a modified version of the Downs and Black methodological scale. The Downs and Black scale is supported by the Cochrane Handbook as a useful tool to appraise the methodological quality of nonrandomized healthcare studies [27]. We chose this checklist because it was validated for use with observational study designs [28] and has been previously used to assess the methodological quality in systematic reviews of longitudinal studies of workloads [10]. The number and appraisal of items from the original checklist was tailored to the scope of this systematic review (Table 1). A total of 16 items were used to assess 4 domains including reporting (7 items), external validity (3 items), internal validity (5 items) and study power (1 item). Each item was scored as “Y” if criterion was fulfilled (1 point), “N” if not fulfilled (0 points) or “U” if unable to determine (0 points). The scoring for each study was summed and converted into percentages to provide the total quality score. Two authors (R. A. and E. H. W.) independently rated each of the included studies and a third author (A. R. M.) was consulted if a decision could not be reached.
2.5 Synthesis of Results
We did not pursue quantitative data synthesis (meta-analysis) due to the heterogeneous characteristics of the included studies which would result in spurious pooling of injury risk estimates. Heterogeneity was evident by the different sports included, ACWR calculation (daily versus weekly blocks, acute and chronic windows, binning categories and injury lag) and statistical analyses performed (different approaches and varying time-to-event analyses).
We plotted a figure for each workload metric (if reported in ≥ 3 studies) to combine the association of the ACWR and injury risk estimates from the different studies. The figure comprised the sport analysed, the direction (increased or decreased risk) and estimate of injury, the risk situation (ACWR categories), the injury lag and the acute:chronic window used for each study. We plotted as dark red the areas of the ACWR continuum where the risk estimate pointed to an increased risk when compared to a lower risk area, highlighted as light green. Conversely, areas with decreased risk were highlighted as dark green when compared to areas with higher risk identified as light red. When the risk estimate was not statistically significant, the graph was represented by a grey colour. For ACWR combined with low or high chronic loads, we plotted the increased risk area of the ACWR (as dark red) and identified the amount of chronic load accumulated for each workload metric used. Row height was adjusted so every study in the same workload metric category represented the same overall row size, i.e. when a study was used more than once for the same workload metric, we divided the row by the number of times that study was being used. We prioritized the subsequent week injury lag when creating the figures to allow comparison between studies. We used the ColorADD identification system to enable all readers to distinguish between colours regardless of red-green colour-blindness [29].
3 Results
3.1 Study Selection
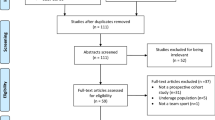
The database and hand-search yielded 4242 titles and abstracts. Duplicate articles were removed and 2961 articles were screened based on their title and abstract. A total of 117 full-text articles were screened for eligibility and 20 met the eligibility criteria and were included in our systematic review (Fig. 1) [19,20,21,22,23, 30,31,32,33,34,35,36,37,38,39,40,41,42,43,44]. Studies were published between 2014 and 2019, but mostly since 2016 (90%).

Preferred Reporting Items for Systematic reviews and Meta Analyses (PRISMA) flow chart of included and excluded studies. ACWR acute: chronic workload ratio
3.2 Population Characteristics
A total of 2375 injuries from 1234 athletes (all male and mean age of 24.0 ± 1.2 years) were included in this systematic review. Studies comprised an average of 62 ± 44 participants, ranging from 25 to 173 athletes. Football (35%), Australian Football (30%) and rugby (25%; of which 80% league and 20% union) were the most common sports studied. Gaelic Football and cricket (fast bowlers) were examined in one study each. The data were collected during 1 season (45%), 2 seasons (25%), and 3 or more seasons (30%). Table 2 presents the study and population characteristics of individual studies.
3.3 Methodological Quality
The ratings from the quality appraisal for each included study are presented in Table 3. The mean total score was 68.4% (range 56–81%) and 11.0 ± 1.0 (range 9–12) out of 16 possible points. We found major methodological concerns from the six criteria: reporting (85% and 75% of studies failed to report how they handled the players’ transferring between teams and missing data points); external validity (85% of studies only used one team); internal validity (90% of the studies failed to adjust the risk estimates for confounding factors); and 75% did not perform a power sample size calculation.
3.4 Workload Metrics and ACWR Analysis
More than half of the studies measured the internal (65%) and external loads (70%). Only seven studies (35%) collected both internal and external loads. The sRPE was the metric collected as internal load in all cases. Methods for recording external loads were mostly GPS and accelerometer monitoring of training sessions and matches (93% and 36% of studies that collected external loads, respectively). Other methods used were semi-automated camera system during competitive matches (1 study) and number of balls bowled per week in training and competition (1 study). The total distance covered (70%) and total distance covered within determined running-intensity zones (60%) were the most common metrics collected as external load measures. Electronic Supplementary Material Appendix S2 summarizes the workload metrics monitored.
The ACWR was calculated mostly using the coupled method (95% of studies) and weekly blocks (75% of studies). The acute window was generally 1 week or 7 days (95% of studies) and chronic window was 4 weeks or 28 days (95% of studies). All studies used rolling averages (100% of studies) and two studies (10%) also calculated the EWMA. Binning categorization varied between studies and injury lag period was most commonly the subsequent week (80% of studies). Electronic Supplementary Material Appendix S3 summarizes the ACWR calculation methods.
Statistical analysis was performed mostly using logistic regression analysis or generalized estimating equation (GEE) modelling (45% of studies each). Electronic Supplementary Material Appendix S4 summarizes the statistical analysis methods.
3.5 Risk Estimates for ACWR
The results of risk estimates for ACWR in isolation or in combination with low or high chronic workloads for each individual study are reported in Electronic Supplementary Material Appendix S5. Figures 2, 3, 4, 5, 6, 7 and 8 display the risk estimates and ACWR circumstances for sRPE (n = 834 and 1527 injuries for a combined 23 seasons), total distance (n = 436 and 857 injuries for a combined 19 seasons), moderate-intensity running (n = 229 and 343 injuries for a combined 9 seasons), high-intensity running (n = 410 and 593 injuries for a combined 17 seasons), sprinting (n = 238 and 417 injuries for a combined 9 seasons), accelerations and decelerations (n = 116 and 232 injuries for a combined 6 seasons), and player load (n = 215 and 319 injuries for a combined 7 seasons). Figures 9, 10 and 11 show the risk estimates and circumstances for high ACWR combined with low chronic loads (n = 226 and 567 injuries for a combined 13 seasons), low ACWR combined with low chronic loads (n = 140 and 230 injuries for a combined 8 seasons) and high ACWR combined with high chronic loads (n = 156 and 434 injuries for a combined 9 seasons). As only one study reported the risk estimates of low ACWR combined with high chronic loads [21], we did not plot the results into a figure.

Risk estimates and ACWR circumstances (categories, injury lag and A: C windows) for sRPE. ↑—significant increased risk, ↓—significant decreased risk; ↔—no significant differences;  —football (soccer);
—football (soccer);  —Australian Football;
—Australian Football;  —rugby;
—rugby;  —fast bowlers (cricket);
—fast bowlers (cricket);  —Gaelic Football; *—90% confidence intervals. RR relative risk, OR odds ratio, HR hazard ratio, ACWR acute: chronic workload ratio, EWMA exponentially weighted moving averages
—Gaelic Football; *—90% confidence intervals. RR relative risk, OR odds ratio, HR hazard ratio, ACWR acute: chronic workload ratio, EWMA exponentially weighted moving averages

Risk estimates and ACWR circumstances (categories, injury lag and A: C windows) for total distance. ↑—significant increased risk; ↔—no significant differences;
—football (soccer);
—Australian Football;
—rugby; *—90% confidence intervals; †—non-contact injuries. RR relative risk, HR hazard ratio, ACWR acute: chronic workload ratio, EWMA exponentially weighted moving averages

Risk estimates and ACWR circumstances (categories, injury lag and A: C windows) for moderate-intensity running. ↑—significant increased risk; ↔—no significant differences;
—football (soccer);
—Australian Football; *—90% confidence intervals; †—non-contact injuries. RR relative risk, HR hazard ratio, ACWR acute: chronic workload ratio, EWMA exponentially weighted moving averages

Risk estimates and ACWR circumstances (categories, injury lag and A: C windows) for high-intensity running. ↑—significant increased risk; ↓—significant decreased risk; ↔—no significant differences;
—football (soccer);
—Australian Football;
—rugby; *—90% confidence intervals; †—non-contact injuries. RR relative risk, IRR incidence risk ratio, ACWR acute: chronic workload ratio

Risk estimates and ACWR circumstances (categories, injury lag and A: C windows) for sprint. ↑—significant increased risk; ↔—no significant differences;
—football (soccer);
—Australian Football;
—rugby; †—non-contact injuries. RR relative risk, OR odds ratio, ACWR acute: chronic workload ratio

Risk estimates and ACWR circumstances (categories, injury lag and A:C windows) for a acceleration and b decelerations. ↑—significant increased risk; ↔—no significant differences;
—football (soccer);
—rugby; *—90% confidence intervals; †—non-contact injuries. RR relative risk, OR odds ratio; ACWR acute: chronic workload ratio

Risk estimates and ACWR circumstances (categories, injury lag and A: C windows) for player load. ↑—significant increased risk;
—Australian Football;
—rugby; *—90% confidence intervals. RR relative risk, HR hazard ratio, OR odds ratio, ACWR acute: chronic workload ratio, EWMA exponentially weighted moving averages

Risk estimates and ACWR circumstances (categories, injury lag and A: C windows) for high ACWR combined with low chronic workloads. ↑—significant increased risk; ↔—no significant differences;
—football (soccer);
—Australian Football;
—rugby; *—90% confidence intervals; †—non-contact injuries. RR relative risk, IRR incidence risk ratio, adj-IRR adjusted incidence risk ratio, ACWR acute: chronic workload ratio, sRPE session-rating of perceived exertion, TD total distance, MIR moderate-intensity running, HIR high-intensity running, ACC accelerations, DEC decelerations

Risk estimates and ACWR circumstances (categories, injury lag and A:C windows) for low ACWR combined with low chronic workloads. ↑—significant increased risk; ↔—no significant differences;
—Australian Football. IRR – incidence risk ratio; adj-IRR – adjusted incidence risk ratio; ACWR – acute:chronic workload ratio; sRPE—session-rating of perceived exertion; TD – total distance; HIR – high-intensity running

Risk estimates and ACWR circumstances (categories, injury lag and A:C windows) for high ACWR combined with high chronic workloads. ↑—significant increased risk; ↔—no significant differences;
—football (soccer);
—Australian Football;
—rugby; †—non-contact injuries. RR relative risk, ACWR acute: chronic workload ratio; sRPE session-rating of perceived exertion, TD total distance, MIR moderate-intensity running, HIR high-intensity running, ACC accelerations, DEC decelerations
4 Discussion
4.1 Is the ACWR Associated with Sports Injury?
This review included 20 studies that assessed the association of ACWR and time-loss injury risk across multiple team sports. Ninety percent of studies showed a positive association between higher ACWR (relative to a low or moderate ACWR) and higher risk of injury. There were two studies [31, 44] not identifying any significant associations and no studies indicated a decreased injury risk with high ACWR. PlayerLoad and sRPE were the two metrics showing the most consistent findings. PlayerLoad is a variable offered by the software provider of a commercially available wearable inertial measurement unit. The combined vectors of the anterio-posterior, medio-lateral, and longitudinal accelerometers have been used to provide a measure of accelerometer load [45]. Both the PlayerLoad and sRPE are time-dependent metrics that measure the overall physical and/or psycho-physical loads and therefore may be suited to monitor injury risk. There was a wide variation in methodological approaches to calculate the ACWR. Almost all studies tested their hypothesis using different methods of data structuring and analysis which was especially apparent in terms of creating ACWR cut-offs (binning). Practitioners are advised to take these considerations into account when interpreting the results.
A higher ACWR (relative to a low or moderate ACWR) was commonly associated with increased injury risk [19,20,21, 23, 30, 32,33,34,35, 37,38,39,40,41,42], regardless of the metric monitored. A low ACWR has also been suggested as a potential risk factor for injuries in team sports [22, 30, 33, 34]. Only a few studies found a significant association of low ACWR and higher risk of injury [20, 30, 33, 34] and there is currently insufficient scientific evidence (many non-significant findings) to conclude that a low ACWR is associated with increased risk of injury. When combined with low chronic loads, a high or low ACWR was associated with increased risk of injury [19,20,21,22]. These findings suggest that consistently low workloads leave the athlete unprepared and more susceptible to injury. In turn, athletes with higher aerobic fitness, lower body strength, speed, and repeated-sprint ability can better tolerate higher ACWRs and have reduced risk of injury [37,38,39, 46]. High chronic loads combined with either low or high ACWRs did not consistently show significant associations with reduced or increased risk of injury [19,20,21]. Taken together, these findings suggest that the ACWR should not be used alone to assess the risk of injury, but rather placed in context and balanced with other predisposing risk factors to allow a more informed decision.
4.2 How to Best Calculate the ACWR? The Decision Requires Context
There has been considerable debate on the best methods to calculate the ACWR and the most appropriate statistical models to use when ascertaining risk. Some of these methodological issues have been tested in the real world and others remain in the domain of proposed methodological improvements that have yet to be explored [47].
4.2.1 Rolling or EWMA, Which Model Fits Best?
The rolling average ACWR assigns the same level of importance to all observations in the aggregated chronic time window. Williams et al. [26] proposed a non-linear model—the EWMA [48]—that sets an increasing weighting to the more recent daily workload values to compensate for these latency effects. Only two studies [34, 42] included in this review used the EWMA model and suggested that the EWMA model was a better alternative to rolling averages for assessing injury risk. Some studies show that while both models demonstrate significant associations between ACWR and injury risk [49,50,51], rolling ACWRs may underestimate the injury risk at higher ACWR ranges [49, 50, 52, 53], while others suggest that there are no differences between the rolling averages and the EWMA methods [51]. Studies included in this review support both methods, but when directly compared, the EWMA model shows greater sensitivity. However, one model may not be a perfect fit for all purposes. Coaches and sports scientists should adapt their ACWR calculation method to the realities of their sport, i.e. based on the different physical demands among sports, training environments and games schedules [54]. Consider an example from a Major League Baseball pitcher. Although teams generally play a game every day, starting pitchers will typically compete on a 5-day rotation. A 7-day acute loading cycle, along with a 28-day chronic window (reflecting ~ 25–26 games) may not fit the periodization model for this athlete. In this example, baseball teams will likely adjust the acute and chronic loading periods to suit the game schedule and periodization strategy of the sport and athlete.
4.2.2 To Couple or Not to Couple?
All but one study [19] employed a coupled strategy to calculate the ACWR. This means that these studies used the acute workload in both the numerator and denominator. Conversely, the uncoupled method excludes the acute workload from the denominator (chronic workloads). Mathematical coupling of ACWR is controversial [55,56,57,58] as it influences the chronic workloads and therefore the ACWR itself. While the coupled method never exceeds an ACWR of 4, the uncoupled method has no maximum bound [57]. The controversy was first introduced in an editorial by Lolli et al. [56], where using simulated data from 1000 Australian Football players [49], they concluded that using the coupled method resulted in a spurious correlation between acute and chronic workloads and decreased the variability of load between athletes. In contrast, using the uncoupled method the correlation was close to zero (r = 0.01). Real-world data demonstrate that there is a nearly perfect correlation (r = 0.99) with similar injury likelihoods between coupled and uncoupled methods [55], and that the mathematical coupling has little effect on the ACWR injury relationship [55]. While some authors [56] suggest using the uncoupled method, other authors [57] advocate that regardless of the method used, researchers should clearly detail how they calculated the ACWR to allow a better interpretation of the results and that practitioners should select the approach that best fit their context. We cannot settle this question with the current literature and need further studies to investigate whether there is an advantage in using the uncoupled ACWR.
4.2.3 Acute and Chronic Time Windows, Which Best Represent the Risk?
Regardless of the model used to calculate the ACWR, the acute and chronic timeframes influence the injury risk [30]. Across the included studies, more than fifty combinations of acute: chronic windows were tested, with 1:4 weeks (or 7:28 days) being the most common. Three studies [33, 35, 40] compared 1:2, 1:3 and 1:4 weeks sRPE ACWR in football (soccer) and found that although the three ratios were associated with significant injury risks [33, 35], the 1:3 and 1:4 weeks ACWRs better identified the risk of injury [40]. Carey et al. [30] tested several different acute and chronic day-based time frames in Australian Football players and found that the 3:21 days (which included the training workloads) or 6:28 days (which included both the last game and training workloads) best explained injury risk. The 3:21 days ACWR also showed an association with injury risk in football as the 3-day acute periods reflect the main training sessions prior to games and the 21-days the football-specific mesocycle [39]. Stares et al. [22] tested different acute (1 and 2 weeks) and chronic windows (2 to 8 weeks) for ACWR in combination with chronic loads and found no significant differences among the different timeframes for injury prediction. Both the 3:21 days and the 1:3 or 1:4 weeks ACWRs provide significant associations with injury risk, but coaches and sports scientists should adapt their model to cover the timeframes that most suit their sport.
4.2.4 Do Injury Latency Periods Matter When Calculating Injury Risk?
Several injury lag periods were tested across the ACWR studies—same day [30, 34, 43], 2 or 5 days [30], current week [21, 23, 41, 42, 44], subsequent week [19,20,21, 23, 31, 32, 35,36,37,38,39,40,41,42, 44], and across periods of 7, 14, 21 and 28 days [22]—but the most commonly employed was the subsequent week (80% of the studies). The use of a latent period is important to allow directional inferences between spikes in workloads and injury [59]. For instance, a spike in training or match loads can predispose the athlete to higher risk of injury for up to 3–4 weeks [22], which highlights how important it is to monitor the athlete in the latent period after a workload spike. Making a clear distinction between the measurement period and the risk period also decreases the chances of spurious findings of overlapping windows where low training is associated with injury, which could be equally explained by an injured athlete being unable to accrue training load. Cumulative workloads and ACWR can also have a different effect depending on the tissue type that is injured, reflecting different injury latency periods, including a more acute (e.g. muscle injury), medium-term (e.g. bone stress fractures) or long-term (e.g. joint cartilage) injury lag [60]. Injury lag period seems to have an effect on the injury risk [30] and can be adapted to address the specificities of each sport (can comprise the last game or both last game and training sessions).
4.2.5 How can Binning Hamper Injury Risk Association?
Discretization of workloads has been questioned because it implies that two different ACWRs within the same binning category have equal risk [61]. Discretization removes variation in workloads and ACWR which hampers the statistical power and the ability to detect true relationships [62, 63]. Workloads use repeated measures (from the same athlete) which means that they are correlated within-individual and are not independent [61]. Despite this apparent pitfall, discretizing the ACWR can be useful in the real-world context as it provides a discrete range of workloads (low, moderate or high)—rather than relying on exact amounts of workloads—that athletes may be prepared to endure (based on their chronic workloads) and thus guide coaches in formulating their training plans [47]. Almost all studies binned the ACWR into discrete categories, but using heterogeneous binning methods and even the number of categories varied for the studies that used the same binning method. Binning methods ranged from standard deviation increases [31, 44], 0.5 increments [23], z scores [19, 21, 33], percentiles [35, 40], tertiles [32, 36], quintiles [20], quantiles [30, 34] and arbitrary bins [22, 37,38,39, 41, 42]. Carey et al. [61] compared discrete (binned using 7 z score categories, 5 quantiles or 5 arbitrary cut-offs) to continuous models (restricted cubic splines and fractional polynomials) using simulation data from samples of 1000 and 5000 observations. Their findings showed that transforming workloads into discrete categories and assuming independence, results in a higher risk of false discovery rates (type-I error) and false rejection rates (type-II error). This leads to an unrealistic and discontinuous model that is not suited for modelling the continuous U-shaped risk profile of the association between ACWR and injury. Based on the lack of support for increased injury risk at low ACWRs from the studies included in our systematic review, a non-linear risk such as a J-shaped curve seems to better describe the risk profile. Future studies should avoid discretization of workloads and employ continuous multivariate models that are better suited to fit non-linear trends (U-shaped and S-shaped). We suggest that more useful information may be gathered from data when curve-fitting is based on either previous positive results or some biologically plausible association rather than convenience or overfitting [64].
4.2.6 Do Studies Implement Suitable Statistical Modelling for Longitudinal Data?
Included studies mostly used logistic regression or GEE models to calculate the injury risk. Logistic regression models assume the same exposure (training and match loads) across athletes [5] and have a higher risk of false rejection rates [61]. As such, GEE models are considered preferable. A previous review has highlighted that logistic regression models are not suited to address the multifactorial aetiology of sports injury and between- and within-athlete differences, as well as the temporal design of intensive longitudinal data challenges [59]. The authors suggested using time-to-event (Cox proportional hazards and frailty models) and multilevel modelling. Others have suggested the use of advanced causal inference-based methods [47]. None of the included studies in this review used time-to-event analyses and only two employed multilevel modelling. Future studies using the ACWR should consider statistical methods that address both time-to-event and multilevel modelling. For further information on this topic, the reader is referred to several useful reviews in this area [59, 65,66,67].
4.3 Higher Risk Does Not Mean Injuries Can be Predicted
Although ACWRs were commonly associated with increased injury risk, injury risk is not equal to injury rate, i.e. when athlete workloads spike (e.g. ACWR > 2.0) they are at higher risk of injury, but this does not imply that they will definitely experience an injury. For instance, Murray et al. [41] reported a fivefold increased risk of injury for a high ACWR (> 2.0) in total distance covered corresponding to a 4% likelihood of injury. In comparison to a moderate ACWR (1.0–1.49) which had a 1% likelihood of injury, the absolute increased risk was ~ 3%. A few studies tested the predictive ability of the ACWR models and reported that in isolation, it had poor or no predictive ability to detect individuals that would suffer a sports-related injury [33, 35, 40], resulting in a high number of false-positive predictions [35, 40]. This is not surprising as baseline risks are typically objectively low, so relative risks can be large, yet still associated with a somewhat low absolute injury risk. For example, if an athlete has their injury risk more than doubled from, say, 5–20%, they still have an 80% chance of not being injured [23]. Using multivariate models that consider the interaction between multiple risk factors [1, 68] it is possible to increase the predictive accuracy of ACWR models [20]. As with other isolated screening measures [69,70,71], the ACWR is unlikely to predict future injuries, but in combination with other monitoring and screening systems can identify athletes or training practices that may be at higher risk of injury and help coaches to manage the athlete training and match workload exposures to decrease the risk of injury [72]. Recently, “differential loads”—which measure the smoothed rate of week-to-week changes in workloads [53]—have been proposed to predict the likelihood of injury; however, this method still requires further investigation.
4.4 Cracks in the Armour. How Can We Move Forward?
Injury risk is a complex phenomenon. Considering the multiple risk factors playing a role and the proportion of chance and luck involved in team sport injuries, it is unlikely that a review like this, addressing a single risk factor, will provide a clear and consistent answer.
The number of studies examining the relationship between the ACWR and injuries has grown rapidly over the last few years. No clear consensus on the most appropriate approach has been achieved and several different methods to calculate the ACWR are being proposed (coupled versus uncoupled, rolling vs EWMA, different acute and chronic timeframes, binning categories and injury lag periods). While we need to appreciate the research that has been conducted, with the benefit of hindsight, we can now identify some areas which can be improved and implemented in future research. To reach more definitive conclusions we need future studies to pre-register [73], accurately report the ACWR calculation methods, describe how they handled transferring players’ data, apply statistical models that can handle missing data, and compare ACWR calculation approaches in large samples [66] of players across different sports. While this is especially challenging in a competitive team sport environment, it is necessary to secure the scientific integrity of each published article and allow for informed methodological recommendations.
There are other factors that still need clarification. Further studies are required to establish the interaction between workloads and other moderators in the multivariate risk of sports injuries [5, 68, 74, 75]. While some moderators (history of previous injury [34], level of experience [34], strength [34, 46], aerobic fitness [37, 38], repeated-sprint ability and maximal speed [46]) have shown a significant interaction with the ACWR and injury risk, the interaction of other moderators with ACWR—such as sleep (quality and duration) and psychological factors (mood, stress and fatigue) which are also linked to injury [76,77,78]—is poorly investigated and reported in only a single study [34]. Other research priorities include identifying the long-term response of different tissue types to varying loading patterns [60]. A recent study of professional football players competing at elite European level showed that there were no significant differences in the ACWR among different tissue types (muscle, ligament, and tendon) for the incidence and severity of injury [79]. Given the lack of statistical rigour in this study, these findings should be interpreted with caution. Most studies use arbitrary workload metrics (e.g. sRPE and PlayerLoad) and broad definitions of injury (all time-loss injuries). Future studies should focus on workload metrics that are structure-specific with potentially a better association with each specific injured tissue type (e.g. distance covered sprinting and risk of muscle injuries) for each sport (e.g. running distance for runners or number of throws for overhead athletes) [80, 81].
Finally, theoretical causal frameworks [47, 53] that account for time-dependencies of load and confounders [65, 66] have recently been proposed. Research using actual data is warranted to investigate the effect and applicability of this framework to the “real-world” context.
4.5 How Can we Translate These Findings into Real-World Situations? Some Practical Applications
The results of the systematic review point towards greater risk of injury at higher ACWRs. The ACWR can be used as a planning tool to minimize spikes in workload during the season, as well as when returning athletes to competition following injury and off-season break.
The principle of progressive overload states that load must slightly exceed load capacity (i.e. the load that the athlete is prepared for) in order for improvements in load capacity to occur [75]. However, if the increases in load are excessive, and greatly exceed load capacity, injury risk is heightened [82]. While other methods of progressing load have been proposed (e.g. week-to-week changes), no other method considers the athlete’s current capacity when progressing training. The ACWR offers an important practical advantage over other methods of progressing training load, by not only considering “load” but also the load that the athlete is ready to tolerate.
While this review has focused on a single variable (i.e. ACWR), it is important to recognize that training is designed to develop the physical qualities that allow athletes to tolerate the week-to-week demands of competition. In this respect, the development of chronic load, and the moderators that help protect against spikes in workload (e.g. strength, aerobic fitness), are critical [37, 46, 74]. Within the debate surrounding the predictive ability of the ACWR, and whether more suitable statistical models should be used, the importance of building chronic load to enhance injury resilience and performance appears to have been lost. We encourage practitioners to develop greater chronic loads in their athletes in order to tolerate the acute loads associated with competition.
4.6 Limitations
As this is a fast-developing topic in the field of exercise and sports medicine, a few studies were recently published and were not included in this systematic review. We also excluded studies that included adolescents, recreational or amateur players, non-time-loss injuries and overlapping samples. These two factors may have excluded some potentially relevant studies for this review, but we analysed those studies and included them in the discussion where applicable. Although we only included time-loss injuries, the definition of “time-loss injuries” and type of injuries included can vary across studies [83, 84]. While some studies defined time-loss injury if the athlete missed a match, other studies considered when the athlete missed a match and/or a training session (or no participation for more than 24 h). When more than one type of injury was reported in the study (e.g. contact and non-contact injuries), we prioritized the non-contact injuries to allow a more reliable comparison across studies.
Our ultimate pursuit was to perform a meta-analysis but for that purpose we needed more studies within the same sport that used the same ACWR calculation methods and that employed statistical methods that were adequate to estimate the risk of repeated, longitudinal workload data. It would be clinically useful to have a prescribed cut-point beyond which injury risk clearly increased; however the wide heterogeneity in methods and results documented here as well as the issues associated with discretizing continuous variables [61] precluded us from defining specific cut-offs to classify low, moderate and high ACWRs. We advise use of a more standardized approach to binning the ACWR in future studies to allow for categorisation of the ACWR.
We did not employ a risk of bias assessment tool because the domains did not apply to this type of studies. We used the Downs and Black scale and, although not recommended [85, 86], we modified the scale to adapt to the type of studies included in our systematic review.
All included studies comprised male athletes; workload as a risk factor in female athletes is insufficiently investigated. Future research should also study the effect of the exposure of high and low workloads on injury risk of female athletes.
5 Conclusion
The methodological variations identified in the studies included in our systematic review precluded statistical pooling of results and warrant caution with any recommendations. All studies showed either increased risk or null findings and there were no studies showing protective association between high ACWR and injury. These findings suggest that a higher ACWR (relative to a lower or moderate ACWR) is associated with an increase in time-loss injury risk but requires further exploration. Future research should aim to address the methodological limitations identified before definitive statements can be made.
Data Availability
Additional data can be provided by reasonable request to authors.
References
Bittencourt NFN, Meeuwisse WH, Mendonça LD, Nettel-Aguirre A, Ocarino JM, Fonseca ST. Complex systems approach for sports injuries: moving from risk factor identification to injury pattern recognition—narrative review and new concept. Br J Sports Med. 2016;50(21):1309.
Hulme A, Finch CF. From monocausality to systems thinking: a complementary and alternative conceptual approach for better understanding the development and prevention of sports injury. Inj Epidemiol. 2015;2(1):31.
Meeuwisse WH, Tyreman H, Hagel B, Emery C. A dynamic model of etiology in sport injury: the recursive nature of risk and causation. Clin J Sport Med. 2007;17(3):215–9.
Gabbett TJ, Whyte DG, Hartwig TB, Wescombe H, Naughton GA. The relationship between workloads, physical performance, injury and illness in adolescent male football players. Sports Med. 2014;44(7):989–1003.
Windt J, Gabbett TJ. How do training and competition workloads relate to injury? The workload—injury aetiology model. Br J Sports Med. 2017;51(5):428.
Burgess DJ. The research doesn't always apply: practical solutions to evidence-based training-load monitoring in elite team sports. Int J Sports Physiol Perform. 2017;12(Suppl 2):S2136–S21412141.
Fox JL, Scanlan AT, Stanton R. A review of player monitoring approaches in basketball: current trends and future directions. J Strength Cond Res. 2017;31(7):2021–9.
Bourdon PC, Cardinale M, Murray A, Gastin P, Kellmann M, Varley MC, et al. Monitoring athlete training loads: consensus statement. Int J Sports Physiol Perform. 2017;12(Suppl 2):S2161–S21702170.
Quarrie KL, Raftery M, Blackie J, Cook CJ, Fuller CW, Gabbett TJ, et al. Managing player load in professional rugby union: a review of current knowledge and practices. Br J Sports Med. 2017;51(5):421–7.
Fox JL, Stanton R, Sargent C, Wintour SA, Scanlan AT. The association between training load and performance in team sports: a systematic review. Sports Med. 2018;48(12):2743–74.
Drew MK, Cook J, Finch CF. Sports-related workload and injury risk: simply knowing the risks will not prevent injuries: narrative review. Br J Sports Med. 2016;50(21):1306–8.
Damsted C, Glad S, Nielsen RO, Sorensen H, Malisoux L. Is there evidence for an association between changes in training load and running-related injuries? A systematic review. Int J Sports Phys Ther. 2018;13(6):931–42.
Griffin A, Kenny IC, Comyns TM, Lyons M. The association between the acute:chronic workload ratio and injury and its application in team sports: a systematic review. Sports Med. 2020;50(3):561–80.
Drew MK, Finch CF. The relationship between training load and injury, illness and soreness: a systematic and literature review. Sports Med. 2016;46(6):861–83.
Jones CM, Griffiths PC, Mellalieu SD. Training load and fatigue marker associations with injury and illness: a systematic review of longitudinal studies. Sports Med. 2017;47(5):943–74.
Maupin D, Schram B, Canetti E, Orr R. The relationship between acute: chronic workload ratios and injury risk in sports: a systematic review. Open Access J Sports Med. 2020;11:51–755.
Gabbett TJ. The training—injury prevention paradox: should athletes be training smarter and harder? Br J Sports Med. 2016;50(5):273–80.
Soligard T, Schwellnus M, Alonso JM, Bahr R, Clarsen B, Dijkstra HP, et al. How much is too much? (Part 1) International Olympic Committee consensus statement on load in sport and risk of injury. Br J Sports Med. 2016;50(17):1030–41.
Bowen L, Gross AS, Gimpel M, Bruce-Low S, Li FX. Spikes in acute: chronic workload ratio (ACWR) associated with a 5–7 times greater injury rate in English Premier League football players: a comprehensive 3-year study. Br J Sports Med. 2019. https://doi.org/10.1136/bjsports-2018-099422.
Colby MJ, Dawson B, Peeling P, Heasman J, Rogalski B, Drew MK, et al. Multivariate modelling of subjective and objective monitoring data improve the detection of non-contact injury risk in elite Australian footballers. J Sci Med Sport. 2017;20(12):1068–74.
Hulin BT, Gabbett TJ, Lawson DW, Caputi P, Sampson JA. The acute:chronic workload ratio predicts injury: high chronic workload may decrease injury risk in elite rugby league players. Br J Sports Med. 2016;50(4):231–6.
Stares J, Dawson B, Peeling P, Heasman J, Rogalski B, Drew M, et al. Identifying high risk loading conditions for in-season injury in elite Australian football players. J Sci Med Sport. 2018;21(1):46–51.
Hulin BT, Gabbett TJ, Blanch P, Chapman P, Bailey D, Orchard JW. Spikes in acute workload are associated with increased injury risk in elite cricket fast bowlers. Br J Sports Med. 2014;48(8):708–12.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535.
Dwyer DB, Gabbett TJ. Global positioning system data analysis: velocity ranges and a new definition of sprinting for field sport athletes. J Strength Cond Res. 2012;26(3):818–24.
Williams S, West S, Cross MJ, Stokes KA. Better way to determine the acute: chronic workload ratio? Br J Sports Med. 2017;51(3):209–10.
Higgins JP, Green S. Section 13.5. 2.3. Tools for assessing methodological quality or risk of bias in non-randomized studies. Cochrane handbook for systematic reviews of interventions, version 5 1. 2011. https://handbook-5-1.cochrane.org/chapter_13/13_5_2_3_tools_for_assessing_methodological_quality_or_risk_of.htm
Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377–84.
Neiva M. ColorADD: color identification system for color-blind people. In: Espregueira-Mendes J, van Dijk CN, Neyret P, Cohen M, Della Villa S, Pereira H, et al., editors. Injuries and health problems in football: what everyone should know. Berlin: Springer; 2017. p. 303–304.
Carey DL, Blanch P, Ong KL, Crossley KM, Crow J, Morris ME. Training loads and injury risk in Australian football-differing acute: chronic workload ratios influence match injury risk. Br J Sports Med. 2017;51(16):1215–20.
Cross MJ, Williams S, Trewartha G, Kemp SP, Stokes KA. The influence of in-season training loads on injury risk in professional rugby union. Int J Sports Physiol Perform. 2016;11(3):350–5.
Cummins C, Welch M, Inkster B, Cupples B, Weaving D, Jones B, et al. Modelling the relationships between volume, intensity and injury-risk in professional rugby league players. J Sci Med Sport. 2019;22(6):653–60.
Delecroix B, McCall A, Dawson B, Berthoin S, Dupont G. Workload and non-contact injury incidence in elite football players competing in European leagues. Eur J Sport Sci. 2018;18(9):1280–7.
Esmaeili A, Hopkins WG, Stewart AM, Elias GP, Lazarus BH, Aughey RJ. The individual and combined effects of multiple factors on the risk of soft tissue non-contact injuries in elite team sport athletes. Front Physiol. 2018;9:1280.
Fanchini M, Rampinini E, Riggio M, Coutts AJ, Pecci C, McCall A. Despite association, the acute: chronic work load ratio does not predict non-contact injury in elite footballers. Sci Med Foot. 2018;2(2):108–14.
Jaspers A, Kuyvenhoven JP, Staes F, Frencken WGP, Helsen WF, Brink MS. Examination of the external and internal load indicators' association with overuse injuries in professional soccer players. J Sci Med Sport. 2018;21(6):579–85.
Malone S, Roe M, Doran DA, Gabbett TJ, Collins KD. Protection against spikes in workload with aerobic fitness and playing experience: the role of the acute: chronic workload ratio on injury risk in elite Gaelic football. Int J Sports Physiol Perform. 2017;12(3):393–401.
Malone S, Owen A, Newton M, Mendes B, Collins KD, Gabbett TJ. The acute: chonic workload ratio in relation to injury risk in professional soccer. J Sci Med Sport. 2017;20(6):561–5.
Malone S, Owen A, Mendes B, Hughes B, Collins K, Gabbett TJ. High-speed running and sprinting as an injury risk factor in soccer: can well-developed physical qualities reduce the risk? J Sci Med Sport. 2018;21(3):257–62.
McCall A, Dupont G, Ekstrand J. Internal workload and non-contact injury: a one-season study of five teams from the UEFA Elite Club Injury Study. Br J Sports Med. 2018;52(23):1517–22.
Murray NB, Gabbett TJ, Townshend AD, Hulin BT, McLellan CP. Individual and combined effects of acute and chronic running loads on injury risk in elite Australian footballers. Scand J Med Sci Sports. 2017;27(9):990–8.
Murray NB, Gabbett TJ, Townshend AD. The use of relative speed zones in Australian football: are we really measuring what we think we are? Int J Sports Physiol Perform. 2018;13(4):442–51.
Thornton HR, Delaney JA, Duthie GM, Dascombe BJ. Importance of various training-load measures in injury incidence of professional rugby league athletes. Int J Sports Physiol Perform. 2017;12(6):819–24.
Windt J, Gabbett TJ, Ferris D, Khan KM. Training load-injury paradox: is greater preseason participation associated with lower in-season injury risk in elite rugby league players? Br J Sports Med. 2017;51(8):645–50.
Boyd LJ, Ball K, Aughey RJ. The reliability of MinimaxX accelerometers for measuring physical activity in Australian football. Int J Sports Physiol Perform. 2011;6(3):311–21.
Malone S, Hughes B, Doran DA, Collins K, Gabbett TJ. Can the workload-injury relationship be moderated by improved strength, speed and repeated-sprint qualities? J Sci Med Sport. 2019;22(1):29–34.
Wang C, Vargas JT, Stokes T, Steele R, Shrier I. Analyzing activity and injury: lessons learned from the acute: chronic workload ratio. Sports Med. 2020. https://doi.org/10.1007/s40279-020-01280-1.
Hunter JS. The exponentially weighted moving average. J Qual Technol. 1986;18(4):203–10.
Murray NB, Gabbett TJ, Townshend AD, Blanch P. Calculating acute: chronic workload ratios using exponentially weighted moving averages provides a more sensitive indicator of injury likelihood than rolling averages. Br J Sports Med. 2017;51(9):749–54.
Sampson JA, Murray A, Williams S, Halseth T, Hanisch J, Golden G, et al. Injury risk-workload associations in NCAA American college football. J Sci Med Sport. 2018;21(12):1215–20.
Hulin BT, Gabbett TJ, Pickworth NJ, Johnston RD, Jenkins DG. Relationships among PlayerLoad, high-intensity intermittent running ability, and injury risk in professional rugby league players. Int J Sports Physiol Perform. 2020;15(3):423–9.
Cousins BEW, Morris JG, Sunderland C, Bennett AM, Shahtahmassebi G, Cooper SB. match and training load exposure and time-loss incidence in elite Rugby Union players. Front Physiol. 2019;10:1413.
Tysoe A, Moore IS, Ranson C, McCaig S, Williams S. Bowling loads and injury risk in male first class county cricket: is ‘differential load’ an alternative to the acute-to-chronic workload ratio? J Sci Med Sport. 2020. https://doi.org/10.1016/j.jsams.2020.01.004.
Sampson JA, Fullagar HH, Murray A. Evidence is needed to determine if there is a better way to determine the acute: chronic workload. Br J Sports Med. 2017;51(7):621–2.
Gabbett TJ, Hulin B, Blanch P, Chapman P, Bailey D. To couple or not to couple? For acute: chronic workload ratios and injury risk, does it really matter? Int J Sports Med. 2019;40(9):597–600.
Lolli L, Batterham AM, Hawkins R, Kelly DM, Strudwick AJ, Thorpe R, et al. Mathematical coupling causes spurious correlation within the conventional acute-to-chronic workload ratio calculations. Br J Sports Med. 2019;53(15):921–2.
Windt J, Gabbett TJ. Is it all for naught? What does mathematical coupling mean for acute: chronic workload ratios? Br J Sports Med. 2019;53(16):988–90.
Coyne JOC, Nimphius S, Newton RU, Haff GG. Does mathematical coupling matter to the acute to chronic workload ratio? A case study from elite sport. Int J Sports Physiol Perform. 2019. https://doi.org/10.1123/ijspp.2018-0874.
Windt J, Ardern CL, Gabbett TJ, Khan KM, Cook CE, Sporer BC, et al. Getting the most out of intensive longitudinal data: a methodological review of workload-injury studies. BMJ Open. 2018;8(10):e022626.
Orchard JW, Blanch P, Paoloni J, Kountouris A, Sims K, Orchard JJ, et al. Cricket fast bowling workload patterns as risk factors for tendon, muscle, bone and joint injuries. Br J Sports Med. 2015;49(16):1064–8.
Carey DL, Crossley KM, Whiteley R, Mosler A, Ong KL, Crow J, et al. Modeling training loads and injuries: the dangers of discretization. Med Sci Sports Exerc. 2018;50(11):2267–76.
Bennette C, Vickers A. Against quantiles: categorization of continuous variables in epidemiologic research, and its discontents. BMC Med Res Methodol. 2012;12:21.
Altman DG, Royston P. The cost of dichotomising continuous variables. BMJ. 2006;332(7549):1080.
Babyak MA. What you see may not be what you get: a brief, nontechnical introduction to overfitting in regression-type models. Psychosom Med. 2004;66(3):411–21.
Nielsen RO, Bertelsen ML, Ramskov D, Møller M, Hulme A, Theisen D, et al. Time-to-event analysis for sports injury research part 1: time-varying exposures. Br J Sports Med. 2019;53(1):61–8.
Nielsen RO, Bertelsen ML, Ramskov D, Møller M, Hulme A, Theisen D, et al. Time-to-event analysis for sports injury research part 2: time-varying outcomes. Br J Sports Med. 2019;53(1):70–8.
Hulme A, Thompson J, Nielsen RO, Read GJM, Salmon PM. Towards a complex systems approach in sports injury research: simulating running-related injury development with agent-based modelling. Br J Sports Med. 2019;53(9):560–9.
Gabbett TJ, Nielsen RO, Bertelsen ML, Bittencourt NFN, Fonseca ST, Malone S, et al. In pursuit of the ‘unbreakable’ athlete: what is the role of moderating factors and circular causation? Br J Sports Med. 2019;53(7):394–5.
Mørtvedt AI, Krosshaug T, Bahr R, Petushek E. I spy with my little eye … a knee about to go ‘pop’? Can coaches and sports medicine professionals predict who is at greater risk of ACL rupture? Br J Sports Med. 2020;54(3):154–8.
Bahr R. Why screening tests to predict injury do not work—and probably never will…: a critical review. Br J Sports Med. 2016;50(13):776–80.
Verhagen E, van Dyk N, Clark N, Shrier I. Do not throw the baby out with the bathwater; screening can identify meaningful risk factors for sports injuries. Br J Sports Med. 2018;52(19):1223–4.
Hulin BT, Gabbett TJ. Indeed association does not equal prediction: the never-ending search for the perfect acute: chronic workload ratio. Br J Sports Med. 2019;53(3):144–5.
Impellizzeri FM, McCall A, Meyer T. Registered reports coming soon: our contribution to better science in football research. Sci Med Footb. 2019;3(2):87–8.
Windt J, Zumbo BD, Sporer B, MacDonald K, Gabbett TJ. Why do workload spikes cause injuries, and which athletes are at higher risk? Mediators and moderators in workload-injury investigations. Br J Sports Med. 2017;51(13):993–4.
Verhagen E, Gabbett T. Load, capacity and health: critical pieces of the holistic performance puzzle. Br J Sports Med. 2019;53(1):5–6.
Charest J, Grandner MA. Sleep and athletic performance: impacts on physical performance, mental performance, injury risk and recovery, and mental health. Sleep Med Clin. 2020;15(1):41–57.
Galambos SA, Terry PC, Moyle GM, Locke SA, Lane AM. Psychological predictors of injury among elite athletes. Br J Sports Med. 2005;39(6):351–4.
Lathlean TJH, Gastin PB, Newstead SV, Finch CF. A prospective cohort study of load and wellness (sleep, fatigue, soreness, stress, and mood) in elite junior australian football players. Int J Sports Physiol Perform. 2019;14(6):829–40.
Enright K, Green M, Hay G, Malone JJ. Workload and injury in professional soccer players: role of injury tissue type and injury severity. Int J Sports Med. 2020;41(2):89–97.
Nielsen RO, Bertelsen ML, Moller M, Hulme A, Windt J, Verhagen E, et al. Training load and structure-specific load: applications for sport injury causality and data analyses. Br J Sports Med. 2018;52(16):1016–7.
Verheul J, Nedergaard NJ, Vanrenterghem J, Robinson MA. Measuring biomechanical loads in team sports—from lab to field. Sci Med Footb. 2020. https://doi.org/10.1080/24733938.2019.1709654.
Stovitz SD, Johnson RJ. “Underuse” as a cause for musculoskeletal injuries: is it time that we started reframing our message? Br J Sports Med. 2006;40(9):738–9.
Clarsen B, Bahr R. Matching the choice of injury/illness definition to study setting, purpose and design: one size does not fit all! Br J Sports Med. 2014;48(7):510–2.
Hulin BT. The never-ending search for the perfect acute:chronic workload ratio: what role injury definition? Br J Sports Med. 2017;51(13):991–2.
Büttner F, Winters M, Delahunt E, Elbers R, Lura CB, Khan KM, et al. Identifying the ‘incredible’! Part 1: assessing the risk of bias in outcomes included in systematic reviews. Br J Sports Med. 2019. https://doi.org/10.1136/bjsports-2019-100806.
Büttner F, Winters M, Delahunt E, Elbers R, Lura CB, Khan KM, et al. Identifying the ‘incredible’! Part 2: spot the difference—a rigorous risk of bias assessment can alter the main findings of a systematic review. Br J Sports Med. 2019. https://doi.org/10.1136/bjsports-2019-101675.
Acknowledgements
The authors would like thank Dr. for their courtesy in authorizing the use and implementation of the ColorADD® colour system for our figures. The authors would also like to thank Cristina Valente for her valuable help in building and finetuning all the figures in this article.
Author information
Authors and Affiliations
Contributions
RA and ARM performed the database searches. RA and EHW performed the data extraction, methodological quality assessment and initial interpretation of results. TG provided advice throughout the interpretation of data and manuscript drafting. RA was responsible for initial drafting of the article, which was reviewed and edited by all authors. All authors were involved in the conception, design and interpretation of data. All authors read and reviewed the manuscript critically for important intellectual content and approved the final version to be submitted.
Corresponding author
Ethics declarations
Funding
No sources of funding were used to assist in the preparation of this article.
Conflict of interest
Tim Gabbett works as a consultant to several high-performance organisations, including sporting teams, industry, military and higher education institutions. He also conducts training load workshops for health practitioners—in these workshops, among other topics, the strengths and limitations of the acute:chronic workload ratio are discussed. Peter Blanch is currently employed by a sporting organization which has been involved in the production of ACWR research. Renato Andrade, Eirik Halvorsen Wik, Alexandre Rebelo-Marques, Rodney Whiteley and João Espregueira-Mendes declare that they have no conflicts of interest relevant to the content of this review.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Andrade, R., Wik, E.H., Rebelo-Marques, A. et al. Is the Acute: Chronic Workload Ratio (ACWR) Associated with Risk of Time-Loss Injury in Professional Team Sports? A Systematic Review of Methodology, Variables and Injury Risk in Practical Situations. Sports Med 50, 1613–1635 (2020). https://doi.org/10.1007/s40279-020-01308-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-020-01308-6