
Abstract
Background
Lower extremity overuse injuries are common in athletes participating in sports with repeated bouts of landing manoeuvres. Biomechanical alterations during landing may be associated with these types of injuries. The objective of this systematic review with meta-analysis was to summarise and determine the relationship between kinematic alterations during a landing task and the development of lower extremity overuse injuries in physically active populations.
Methods
PubMed, Embase, Web of Science, CINAHL, and SPORTDiscus were consulted up to and including February 2020. Cohort, cross-sectional or case–control studies were included if they investigated the relationship between three-dimensional (3D) landing kinematics in physically active populations and either new incidence or a history of lower extremity overuse injuries.
Results
Twenty-three studies that investigated 3D landing kinematics in subjects with either patellar tendinopathy (PT), patellofemoral pain (PFP), exertional medial tibial pain (EMTP) or groin overuse injury met the inclusion criteria. Based on this systematic review, there is evidence for decreased knee flexion range of motion (ROM) and increased knee abduction ROM during landing as risk factors for PFP. For PT, risk factors are poorly understood. Furthermore, the meta-analysis demonstrated significantly greater hip adduction at initial contact (IC) (p = 0.02), greater knee internal rotation at IC (p < 0.001), greater peak knee external rotation (p = 0.05) and less ankle dorsiflexion at peak vertical ground reaction force (vGRF) (p = 0.05) in subjects with knee overuse injuries compared to healthy controls. There is evidence of increased trunk, hip and knee transversal ROM as risk factors for EMTP. Groin injuries are associated with greater pelvic and hip frontal and transversal plane ROM in the injured group compared to the healthy controls.
Conclusion
The results of this systematic review and meta-analysis provide preliminary evidence for impaired landing kinematics associated with lower extremity overuse injuries. Excessive frontal and transversal plane movements during landing manoeuvres might increase impact and tensile forces resulting in lower extremity overuse injuries.
Registration
This systematic review was registered in the PROSPERO international prospective register of systematic reviews (ID = CRD42019135602).
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Excessive movement in the frontal and transversal plane during landing can be located locally and/or non-locally to the injury site in subjects with lower extremity overuse injuries. |
The meta-analysis demonstrated greater hip adduction and knee internal rotation at initial contact (IC), greater peak knee external rotation, and less ankle dorsiflexion at peak vertical ground reaction force (vGRF) in subjects with knee overuse injuries. |
Decreased knee sagittal range of motion (ROM) and increased knee frontal ROM are considered as risk factors for patellofemoral pain (PFP); whereas, increased trunk, hip and knee transversal ROM are risk factors for exertional medial tibial pain (EMTP). |
1 Introduction
Although the benefits of sports participation are well known, physical activity may also cause sports injuries in elite and recreational athletes which might lead to sports discontinuation [1]. The lower extremity is affected in 47–54% of all sports injuries [2, 3] Acute injuries usually implicate short-term disabilities [4]; whereas, overuse injuries may result in chronic, long-lasting disabilities and are three- to sixfold more frequent [2]. Lower extremity overuse injuries are defined as injuries that occur with gradual onset, without a single identifiable responsible event, and are thought to be the result of micro-trauma caused by repetitive similar movement patterns [5,6,7]. Because of the repetitive nature of running, lower extremity overuse injuries are common in running populations [8]. Furthermore, in sports with repetitive jump-landing manoeuvres, there is a high prevalence of PT and PFP, which might be the result of the accumulated impact forces associated with repetitive movements like single- or double-leg landings [5, 9, 10].
Due to the high prevalence and consequences of these sport-related overuse injuries, the determination of injury mechanisms and risk factors is crucial to provide adequate injury prevention [11, 12]. The majority of sports overuse injuries have a multifactorial origin, and several extrinsic and intrinsic risk factors for these injuries have already been determined in jumping and landing sports [13]. Concerning the intrinsic risk factors, kinematics are essential in understanding injury mechanisms during landing [14]. Previous research showed that joint kinematics are essential in quantifying the capability of the body to modify and absorb high impact forces during landing tasks that might lead to the development of injuries [15, 16]. A multitude of research has been performed to study the association between impaired landing kinematics and acute lower extremity injuries [17, 18]. For example, a stiff landing strategy and increased knee abduction angles and knee abduction moments during landing have been proposed as risk factors for anterior cruciate ligament (ACL) injuries in a female population [17]. Moreover, impaired landing kinematics may also predispose the athlete to overuse injuries due to the accumulation of high impact forces and needs consideration as well [16].
Taking into account these landing kinematics in lower extremity overuse injuries, previous literature often used a local approach to determine risk factors [19,20,21]. Despite the relevance of assessing local kinematic alterations during landing, the determination of non-local kinematic risk factors, which can be located distally or proximally to the site of injury, seems to be essential too. Impairments in these proximal and distal links of the kinetic chain have been found to be important contributors to lower extremity overuse injuries [22,23,24]. For example, trunk position alters lower extremity load through altered lower extremity kinematics [25,26,27], and reduced ankle mobility limits efficient function of the ankle plantar flexion muscles near end-range which transfers loads proximally to the knee [13, 28, 29]. Based on the currently available scientific evidence, it is still unclear whether or not impaired landing kinematics are associated with lower extremity overuse injuries. Therefore, identifying the relationship between impaired landing kinematics and overuse injuries is warranted and could have an added value in the process of injury prevention and injury treatment.
To this date, a recent systematic overview of evidence on the relationship between full-body landing kinematics and lower extremity overuse injuries is lacking. Therefore, the aim of this systematic review and the meta-analysis is twofold: (1) to give a summary of the current evidence regarding impaired local and non-local landing kinematics associated with and/or predictive for lower extremity overuse injuries in a physically active population, and (2) to compare the kinematic data between injured and non-injured physically active people with the meta-analysis if possible.
2 Methods
2.1 Search Strategy and Information Sources
This systematic review was registered in the PROSPERO international prospective register of systematic reviews (ID = CRD42019135602) and conducted by following the Preferred Reporting Items for Systematic reviews and Meta-analyses (PRISMA) guidelines. The database search, literature screening, data extraction, and quality assessment were performed independently by two researchers (CaDB and SV) of the Ghent University. A PICO question was designed to answer the following research question: “What is the relationship between kinematics during a landing task (I) and lower extremity overuse injuries (O) in physically active populations (P)?” There is no comparison (C) determined in this research question since there is no relevant comparator for landing task (I).
The electronic databases Pubmed, Web of Science, Embase, CINAHL, and SPORTDiscus were consulted up to and including February 2020. Free text words, search terms, and corresponding MeSH terms (for PubMed) and EMTREE terms (for Embase) were combined with Boolean operators to answer the research question. Furthermore, the reference lists of included studies were hand-searched to identify other relevant articles. The search strategy is shown in Online Resource 1.
2.2 Eligibility Criteria
Studies were included if they met the following inclusion criteria: (1) written in the English language, (2) a prospective cohort, cross-sectional or case–control study design, (3) investigated a physically active population (regular participation in sports during leisure time, work or education programmes), (4) included individuals with a recent/previous overuse injury of the lower extremity, and (5) extracted 3D landing kinematics during jump manoeuvres in an upright position.
Studies were excluded if they met the following exclusion criteria: (1) investigated a population with acute injuries, (2) measured another movement task than jump-landings, (3) extracted kinematics of other phases during jumping (e.g. take-off), (4) used a qualitative method to obtain the kinematic parameters, and (5) investigated the effects of interventions (e.g. modifying landing kinematics by feedback).
2.3 Study Selection
First, CaDB and SV screened for potential eligible studies on title and abstract. Second, the full texts of the articles that remained after screening on title and abstract were retrieved and assessed by the same researchers. Any discrepancies between the two researchers were resolved with a consensus meeting. RDR was consulted if no agreement could be reached. Inter-rater agreement for screening was calculated and expressed as percentage of agreement (PoA) and k-statistics.
2.4 Quality Assessment (Risk of Bias)
The methodological quality of each study was evaluated independently by two researchers using a modified form of the Downs and Black checklist as provided in the Online Resource 2 [30]. This modified checklist has been previously used in other systematic reviews investigating the relationship between biomechanics and injuries [31,32,33]. Fifteen items (items 1, 2, 3, 5, 6, 7, 9, 10, 11, 12, 16, 18, 20, 25, 26) with a combined maximum score of 16 points were applicable for the included prospective cohort studies. For the case–control studies, the questions regarding follow-up (9 and 26) were not scored resulting in a combined maximum score of 14. Each item could be rewarded with a maximum score of 1 point (1 = “yes”, 0 = “no”, 0 = “not able to determine”). Only the fifth item of the checklist could be rewarded with a maximum score of 2 points (2 = “yes”, 1 = “partially”, 0 = “no”). For the prospective cohort studies, a quality score of 11 or more was considered as high quality, 6–10 was considered as moderate quality, and ≤ 5 was considered as low quality [31]. For the case–control studies, a comparable cut-off was used. A quality score of 10 or more was considered as high quality, 5–9 was considered as moderate quality and ≤ 4 was considered as low quality. After individual quality assessment, consensus between authors was made. K-statistics and PoA were calculated to check agreement between researchers. Individual quality scores were used afterwards to compare the results of the selected studies.
The 2005 classification system of the Dutch Institute for Healthcare Improvement CBO was used to allocate a level of evidence for each included study, based on the study design and methodological quality [34]. Finally, a level of conclusion was made when clustering results of different studies with comparable methodological quality. The levels of conclusion ranged from 1 to 4 and corresponded with a (1) high, (2) moderate, (3) low strength of conclusion or (4) no strength of conclusion at all [34]. The clarification of the levels of evidence and levels of conclusion is shown in Online Resource 3.
2.5 Data Collection and Data Items
A table of evidence was made to summarise the main results for included studies. For each article, the following topics are reported in Table 1: (1) study design, (2) injury type, (3) population, (4) group information, (5) follow-up and injury rate, (6) type of jump, (7) phase of landing, (8) plane of movement, and (9) main results.
Review Manager version 5.3 was used for the meta-analysis. Kinematic results at discrete points during landing were meta-analysed if two or more studies reported the same kinematic outcomes with comparable methodology. As such, only the cross-sectional, case–control, and prospective cohort studies of knee overuse injuries were included for the meta-analysis. The heterogeneity was determined by I2 and associated p values (p < 0.05). The results with an I2 of less than 75% were reported [35]. Mean differences and a confidence interval of 95% were calculated using an inverse variance with random-effect model and were reported in forest plots.
3 Results
3.1 Study Selection
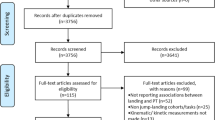
The database searches of PubMed, Web of Science, Embase, CINAHL and SPORTDiscus yielded a total of 2850 citations. Screening on title and abstract resulted in 58 studies, of which 23 articles fulfilled the eligibility criteria after full-text screening (Fig. 1). Fourteen articles, out of the 23 included articles, were used for the meta-analysis.

PRISMA flowchart of study selection process
The PoA between researchers for screening the articles on title and abstract was excellent (99.2%) with a k-score of 80.8%. (p < 0.001). For screening on full-text, reproducibility revealed an excellent PoA of 90.6% and a k-score of 80.6% (p < 0.001).
3.2 Study Characteristics
Fourteen studies with a case–control or cross-sectional study design were included [20, 29, 36,37,38,39,40,41,42,43,44,45,46,47]. The other nine studies had a prospective cohort design [13, 19, 21, 24, 48,49,50,51,52].
Four studies evaluated landing kinematics in volleyball athletes [20, 36, 37, 40], two studies in basketball players [21, 39], two studies in a combination of volleyball, basketball and korfball athletes [13, 52], one study in a combination of volleyball and basketball athletes [29], two studies in a military cohort [48, 49], one study in ballet dancers [38], three studies in physical education students [24, 50, 51], and eight studies in a general physical active population [19, 41,42,43,44,45,46,47]. The mean age in three studies was below 18 years [19, 21, 39].
Various lower extremity overuse injuries were described across the different studies. Nine studies reported on patellar tendinopathy (PT), [13, 20, 29, 36,37,38,39,40, 43] nine studies reported on patellofemoral pain (PFP) [19, 21, 41, 42, 44,45,46, 48, 49], one study reported on general knee overuse injuries (without further specification) [52], one study reported on groin injury [47] and three studies reported exertional medial tibial pain (EMTP) [24, 50, 51]. Three studies included participants with previous symptoms of PT (n = 21) [20, 36, 37], seven studies included participants with a recent PT (n = 72) [20, 29, 36, 38,39,40, 43], one study included participants who developed PT during follow-up (n = 3/49) [13], five studies included participants with PFP (n = 67) [41, 42, 44,45,46], three studies included participants who developed PFP during follow-up (n = 242/5357) [21, 48, 49], one study included participants who developed a general knee overuse injury (n = 25/74) [52], one study analysed 10 participants with a groin injury [47] and three studies included participants who developed EMTP (n = 22/79) [24, 50, 51].
The different studies analysed sport-specific jumps like ballet specific landing [38], block and spike jumps [20, 37, 40]. Also more standardised jumps like double- [21, 29, 36, 48, 49] and single-leg drop jumps [24, 47, 50, 51], double- [13, 19, 21, 41, 43] and single-leg drop vertical jumps [42], maximal single-leg jumps [44,45,46], vertical stop jumps [39] and countermovement jumps [52].
3.3 Quality Assessment (Risk of Bias)
The scores of the modified Downs and Black checklist ranged from 8 to 14 out of 16 (50–87.5%) for the prospective studies and from 7 to 14 out of 14 (50%–100%) for the case-control studies. Eleven studies were of high methodological quality and twelve of moderate methodological quality. Complete information on the quality assessment is presented in Table 2.
Twenty studies out of the twenty-three included studies received a level of evidence B; whereas, two articles obtained a level of evidence A2 [50, 51]; and one study, a level of evidence C [20].
A good reproducibility between researchers was observed with a k-score of 71.9% (p < 0.001), and an excellent 90% PoA for determining risk of bias was calculated.
3.4 Synthesis of the Results
Kinematics are presented per clusters of lower extremity overuse injury as 3D joint angles (degrees). The following points throughout the landing phase are used: initial contact (IC), peak vertical ground reaction force (vGRF), peak knee extension moment (KEM), and peak angle. ROMvGRF represents the trajectory from IC to peak vGRF, \({\text{ROM}}_{\text{KEM}}\) from IC to peak KEM and total ROM is the trajectory from IC to peak angle. Flexion/dorsiflexion in the sagittal plane, adduction/inversion in the frontal plane and internal rotation in the transversal plane are represented as positive values. Extension/plantar flexion in the sagittal plane, abduction/eversion in the frontal plane and external rotation in the transversal plane are shown as negative values. A summary of the results is presented in Fig. 2.

Graphical abstract of the landing kinematics in subjects with lower extremity overuse injuries. ABD abduction, ADD adduction, DF dorsiflexion, EMTP exertional medial tibial pain, EXT ROT external rotation, IC Initial contact, INT ROT internal rotation, PT patellar tendinopathy, PFP patellofemoral pain syndrome, ROM Range of motion from angle at IC to peak angle, vGRF Vertical ground reaction force
3.4.1 Knee Overuse Injuries
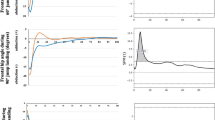
For the knee overuse injuries (PT and PFP), the evidence for differences in kinematics between the control group and injury group is summarised as well as the evidence for altered kinematics as a risk factor for knee overuse injuries is presented. Furthermore, mean differences between the injured and non-injured groups calculated in the meta-analysis are discussed and are added as forest plots in Fig. 3.



Forest plots of the meta-analysis. IC Initial contact, PT patellar tendinopathy, PFP patellofemoral pain syndrome, vGRF Vertical ground reaction force, ROM Range of motion from angle at IC to peak angle, ROM_vGRF Range of motion from angle at IC to peak vGRF. *Significant difference compared with healthy subjects
3.4.1.1 Sagittal Plane Kinematics
There is moderate strength of conclusion for similar trunk sagittal plane kinematics at IC and at peak trunk angle during landing for subjects with PT compared to healthy controls. [29, 39] There is low strength of conclusion for an equal amount of trunk flexion angle at peak vGRF when comparing the PT group with healthy controls [39]. The meta-analysis in subjects with PT shows no effect of trunk flexion at IC (mean 0.08°, 95% CI [− 9.28°, 9.45°]) and at peak angle (mean 1.67°, 95% CI [− 4.55°, 7.88°]).
There is low strength of conclusion for similar pelvic sagittal plane kinematics at IC, peak vGRF and peak angle when subjects with PT are compared to healthy controls [39].
There is moderate strength of conclusion for similar hip sagittal plane kinematics at IC during landing for subjects with PT compared to the healthy controls. [36, 38,39,40, 43] For peak hip flexion, one study showed significantly less flexion (p = 0.03) in the PT group [43]; whereas, three studies found no differences between PT group and non-injured groups [29, 39, 40]. There is moderate strength of conclusion for no differences at peak vGRF when comparing subjects with PT to healthy controls [36, 39]. There is low strength of conclusion for similar hip \({\text{ROM}}_{\text{vGRF}}\) between subjects with PT and healthy controls [36]. There is low strength of conclusion for significantly less total hip flexion ROM in subjects with PFP (p = 0.02) [42]. The meta-analysis in subjects with general knee overuse injuries shows no effect of hip flexion at IC (mean −1.37°, 95% CI [− 2.88°, 0.15°]), at peak vGRF (mean − 0.81°, 95% CI [− 4.88°, 3.27°]), at peak angle (mean −0.11°, 95% CI [− 7.36°, 7.14]) and no effect of total ROM (mean − 3.07°, 95% CI [− 11.40°, 5.25°]).
There is moderate strength of conclusion for similar knee sagittal plane kinematics at IC during landing for subjects with PT compared to healthy controls. [36,37,38,39,40, 43] There is low strength of conclusion for similar knee flexion at peak vGRF between subjects with PT and healthy controls [36, 37, 39]. For peak knee flexion, one study demonstrated significantly less flexion (p = 0.01) in the PT group [43] and three studies did not found differences between the PT group and healthy controls [29, 39, 40]. There is low strength of conclusion for significantly less knee flexion \({\text{ROM}}_{\text{vGRF}}\) (p = 0.04) for an asymptomatic group with a history of PT and no differences for the symptomatic PT group compared to the healthy group [36, 37, 39]. Finally, there is low strength of conclusion for an increased peak knee flexion angle as a significant risk factor (p = 0.02) for PT compared to healthy controls [20]. In subjects with PFP, there is low strength of conclusion for significantly less total knee flexion ROM (p < 0.01) [42]. Low strength of conclusion suggests decreased peak knee flexion as a significant risk factor (p = 0.02) in developing PFP [49]. The meta-analysis of knee sagittal plane kinematics in subjects with general knee overuse injuries demonstrates no effect of knee flexion angle at IC (mean − 0.66°, 95% CI [− 2.44°, 1.13°]), at peak vGRF (mean − 1.44°, 95% CI [− 6.11°, 3.23°]) and no effect of total ROM (mean − 3.72°, 95% CI [− 8.86°, 1.41°]) and total \({\text{ROM}}_{\text{vGRF}}\) (mean − 4.61, 95% CI [− 11.12°, 1.90°]).
There is moderate strength of conclusion for similar ankle sagittal plane kinematics at IC during landing for subjects with PT compared to healthy controls [36, 38,39,40, 43]. In an asymptomatic group with a history of PT, there is low strength of conclusion for significantly less plantar flexion (p = 0.05) at IC [37]. There is low strength of conclusion for a similar amount of ankle ROM at peak vGRF in the asymptomatic group with a history of PT. For the symptomatic group with PT, one study demonstrated significantly less ankle dorsiflexion (p < 0.01); whereas, another study showed no differences when this group was compared to healthy controls [36, 37]. There is low strength of conclusion for no differences for ankle \({\text{ROM}}_{\text{vGRF}}\) between the asymptomatic group with a history of PT and non-injured athletes [37]. For peak ankle dorsiflexion in subjects with PT, one study demonstrated significantly less peak ankle dorsiflexion (p = 0.01) [40]; whereas, three studies showed no differences for peak dorsiflexion angle during landing between these subjects and healthy controls [29, 39, 43]. Regarding ankle sagittal plane kinematics in subjects with PFP, there is low strength of conclusion for no differences in total ankle ROM [42]. The meta-analysis of ankle sagittal plane kinematics in subjects with general knee overuse injuries shows significantly less ankle dorsiflexion at peak vGRF (mean − 3.26°, 95% CI [− 6.44°, − 0.07°]; p = 0.05) and no effect of ankle dorsiflexion at IC (mean − 0.48°, 95% CI [− 3.95°, 2.98°]), at peak angle (mean 0.43°, 95% CI [− 2.04°, 2.91°]) and no effect of total ankle ROM (mean − 3.05°, 95% CI [− 6.32°, 0.22°]) and \({\text{ROM}}_{\text{vGRF}}\) (mean − 4.48°, 95% CI [− 10.69°, 1.74°]).
Two studies investigated the lower extremity contact angle (LECA) in subjects with PT, which represents the angle between the floor and the line connecting the L5-S1 marker to the centre of pressure at IC [38, 40]. One study demonstrated a significantly lower LECA during landing in subjects with PT compared to healthy controls [40]; whereas, another study found no differences [38].
3.4.1.2 Frontal plane kinematics
For pelvic frontal plane kinematics in subjects with PFP, there is low strength of conclusion for similar contralateral pelvic tilt during a single-leg drop landing in subjects with PFP compared to healthy controls. [44, 45].
Regarding the hip frontal plane kinematics in subjects with PFP, there is low strength of conclusion for a significantly greater adduction \({\text{ROM}}_{\text{KEM}}\) when compared to healthy controls (p = 0.012–0.05) [44, 45]. For subjects with general knee overuse injuries, there is low strength of conclusion for no differences at IC, at peak angle and for total ROM when compared to healthy controls [41,42,43]. The meta-analysis of hip frontal kinematics in subjects with general knee overuse injuries shows significantly less hip abduction angle at IC (mean 1.04°, 95% CI [0.17°, 1.91°]; p = 0.02) and no differences for peak hip adduction (mean 0.37°, 95% CI [− 2.18°, 2.92°]).
In reference to the knee frontal plane kinematics in subjects with PFP, there is low strength of conclusion for increased knee abduction ROM as a significant risk factor (p = 0.002) [19]. For knee kinematics in subjects with general knee overuse injuries, there is low strength of conclusion for no differences at IC, peak angle and for total ROM when compared to healthy controls [42, 43]. The meta-analysis of knee frontal plane kinematics in subjects with general knee overuse injuries shows no effect of knee abduction at IC (mean − 0.18°, 95% CI [− 0.70°, 0.34°]) and at peak angle (mean − 1.61°, 0.55°, 95% CI [− 6.54°, 3.31°]).
There is low strength of conclusion for similar ankle frontal plane kinematics at IC, peak angle and for total ROM during landing in subjects with PFP compared to healthy controls. [42, 43].
3.4.1.3 Transversal plane kinematics
There is low strength of conclusion for similar hip external rotation at IC and peak angle during landing in subjects with PT compared to healthy controls [43]. In subjects with PFP, one study demonstrated a significantly lower internal rotation \({\text{ROM}}_{\text{KEM}}\)(p = 0.01) when compared to healthy controls [45]; whereas, another study found no differences [44]. For peak angle, there is low strength of conclusion for significantly more internal rotation (p < 0.01) in the PFP-group [41]. There is low strength of conclusion for a similar hip internal rotation angle between subjects with PFP and healthy controls [49]. For hip kinematic parameters, the meta-analysis of hip transversal plane kinematics in subjects with general knee overuse injuries shows no effect of hip external rotation at IC (mean − 0.61°, 95% CI [− 1.71°, 0.49°]).
There is low strength of conclusion for similar knee internal and external rotation angles at IC and peak angle during landing in subjects with PT compared to healthy controls [43]. In subjects with PFP, there is low strength of conclusion for significantly lower knee internal rotation \({\text{ROM}}_{\text{KEM}}\)(p = 0.05) in subjects with PFP compared to healthy controls [45, 46]. The meta-analysis of knee transversal plane kinematics in general shows significantly more internal rotation at IC (mean 1.99°, 95% CI [0.92°, 3.05°]; p < 0.001) and significantly more peak external rotation (mean − 2.37°, 95% CI [− 4.75°, 0.01°]; p = 0.05) in subjects with knee overuse injuries compared to healthy controls.
There is low strength of conclusion for similar ankle internal and external rotation at IC and peak angle when compared to controls [43]. In subjects with PFP, there is low strength of conclusion for similar external rotation \({\text{ROM}}_{\text{KEM}}\) [45].
3.4.2 Exertional Medial Tibial Pain (EMTP)
There is moderate strength of conclusion for significantly increased trunk, hip and knee rotation ROM in subjects with EMTP [24, 50, 51]. More specifically, one study found significantly increased transversal trunk ROM (p = 0.026) [24], two studies found significantly increased transversal ROM of the ipsilateral hip (p = 0.002–0.01) [24, 50] and two studies found significantly increased transversal ROM of the contralateral knee (p = 0.012–0.023) as risk factors for developing EMTP [50, 51].
3.4.3 Groin Pain
There is only low strength of conclusion for significantly greater pelvic and hip frontal and transversal plane joint angles in subjects with chronic groin pain compared to healthy controls [47]. This study demonstrated significantly greater lateral pelvic tilt (p = 0.01), hip abduction (p < 0.001), and external rotation at IC (p = 0.03) in the injured group in comparison to the control group. A significantly greater lateral pelvic tilt (p = 0.05) and internal rotation (p = 0.02) at the lowest point and significantly greater total hip rotation ROM (p = 0.05) was found in the injured group.
4 Discussion
4.1 Summary of Evidence
To the authors’ knowledge, this is the first systematic review that provides an overview of the current existing literature regarding the association between local and non-local landing kinematics for lower extremity overuse injuries and which pooled these results for knee overuse injuries with the meta-analysis.
The results of this systematic review and the meta-analysis clearly associate impaired landing kinematics with PT, PFP, EMTP, and groin injuries. For subjects with knee overuse injuries, some kinematic risk factors during landing could be identified. Based on the moderate- to high-quality studies, there is low strength of conclusion for decreased knee flexion and increased knee abduction as risk factors for PFP [19, 48]. In contrast to PFP, kinematic risk factors for the development of PT are poorly understood. Only one prospective study with moderate study quality demonstrated high lower extremity stiffness during landing as a potential risk factor for the development of PT [13]. However, this study reported a low incidence of PT and, therefore, used descriptive data [13].
A meta-analysis was performed to clarify the association between knee overuse injuries and landing kinematics. The results of the meta-analysis also showed a trend to a stiff sagittal landing strategy in subjects with knee overuse injuries, with a significantly reduced ROM located at the ankle joint. Furthermore, excessive movements in the frontal and transversal plane of, respectively, the hip and knee are found. More specifically, less ankle dorsiflexion at peak vGRF, greater hip adduction at IC, greater knee internal rotation at IC, and greater peak knee external rotation are observed in subjects with knee overuse injuries. These specific local and non-local landing kinematics in subjects with a recent and/or a new incidence of a knee overuse injury may be associated with the accumulation of impact and tensile forces.
For example, higher impact forces and loading rates during drop jumps were shown in asymptomatic subjects with a history of PT; whereas, comparable magnitudes of the peak vGRF were observed in players with symptomatic PT [36, 39]. Furthermore, the study of Bisseling et al. (2007) correlated high magnitudes of peak vGRF in subjects with a history of PT to a stiff landing pattern, specially landing with less knee flexion [36]. As such, it has been hypothesised that smaller knee flexion angles during landing together with increasing loads might increase patellofemoral joint pressure and, therefore, the risk for developing PFP. In addition, reduced ankle dorsiflexion may result in less absorption of landing impact forces, resulting in more stress being transferred to the knee joint which might increase injury risk [13, 28, 29, 37].
Higher tensile forces acting on the patellar tendon and increased patellofemoral joint contact pressure could be induced by inadequate activation of the hip musculature, resulting in excessive hip and knee frontal and transversal movements during landing [53, 54]. Excessive knee abduction and knee internal rotation might increase loads acting on the medial part and midsection of the patellar tendon [55]; whereas, higher hip adduction and knee abduction might result in, respectively, greater iliotibial band tensile forces together with greater lateral force acting on a decreased patellofemoral contact area [45, 49, 56]. In summary, repeated bouts of impaired landing patterns may result in the accumulation of both compression and tensile forces, and may predispose the athlete to the development of knee overuse injuries.
The only kinematic risk factors that were identified in subjects developing EMTP were non-local to the injury site and were limited to the transversal plane of movement. The combination of impaired single-leg landing kinematics at the trunk, ipsilateral hip, and contralateral knee was hypothesised to be related to higher eccentric lower leg muscle tensile forces to control motion, which might result in the development of EMTP [50]. These conclusions have moderate strength and are supported by three high-quality studies of the same research group [24, 50, 51].
Finally, only one high-quality study investigated the association between impaired landing kinematics and groin injuries which makes it difficult to draw strong conclusions. However, comparable results to the other types of overuse injuries are found, specifically excessive frontal and transversal movements situated locally at pelvis and hip. Inadequate functioning of the stabilising muscles of the trunk and pelvis might increase uncontrolled movements throughout the kinetic chain and therefore increase the workload of the peripheral muscles (e.g. adductor muscles) [50, 51, 57].
To conclude, impaired local and/or non-local landing kinematics can play an important role in developing different types of lower extremity overuse injuries. More specifically, our results indicate that excessive movements in the frontal and transversal plane might accumulate impact and tensile forces acting on lower extremity musculoskeletal structures.
4.2 Methodological considerations and research implications
First, most of the included studies have a cross-sectional or case–control study design. As such, it is currently not clear whether the kinematic alterations can be interpreted as load-avoiding strategy to limit pain and maintain jump performance or as a causal mechanism which transfers loads proximally or distally to the knee [13, 20, 28, 29, 36]. Longitudinal prospective study designs are needed to gain insight into the causality of this relationship. Furthermore, landing kinematics of subjects with PT and PFP, that were retrieved from the case–control and prospective studies, were combined into one study group for the meta-analysis, which makes subsequent interpretation debatable. Correction of these limitations would imply that reduced ankle dorsiflexion at peak vGRF would only serve as an associative factor for the symptomatic PT group (mean − 3.91°, 95% CI [− 7.88°, − 0.05°]. p = 0.05); whereas, no effect would be shown in the asymptomatic PT group (mean − 2.85, 95% CI [− 6.44, 0.73], p = 0.12), which reflects the impact of pain.
Second, it should be noted that a modified version of the Downs and Black checklist, which has not been validated in the past, is used to determine the methodological quality of the studies. However, this modified checklist has already been used in other systematic reviews concerning biomechanics and injuries [31,32,33].
Furthermore, heterogeneity was substantial for population and injury definition across the selected studies. In addition, recreational as well as (sub)elite athletes were included. It should be noted that ball sports like basketball and volleyball players develop more specific skills regarding landing and jumping compared to other sports. Moreover, no conclusion about more game specific unanticipated landings could be drawn due to the investigation of only planned landings. Furthermore, gender could have an impact on landing kinematics as one prospective study demonstrated some gender-specific risk factors for PFP [48]. Finally, age could also play a role in landing biomechanics. One included study with a population of adolescent athletes with PFP demonstrated no differences for knee abduction ROM [21], which is comparable to studies with adult athletes with knee overuse injuries examining this outcome parameter [42, 43]. On the other hand, another included study showed more knee abduction as a risk factor for PFP in an adolescent population [19]. The effect of age on biomechanics only seems to be an important confounding variable in case of early sport specialisation as knee abduction ROM during a drop vertical jump was only significantly higher post-pubertal in the group participating in sport-specific training [58].
Caution should be applied when comparing studies with different types of jump-landings as conflicting results can be attributed to context-specific inconsistencies (horizontal vs vertical tasks, double- vs single-leg tasks, etc.). As the majority of included studies investigated kinematic parameters at discrete points during landing, it is impossible to make conclusions during the entire landing phase. Despite the importance of the first part of impact and the peak values at the final part of landing [37], it might be interesting to investigate the kinematic behaviour between those temporal events to provide more profound information regarding energy storage and load transmission during the whole landing phase. To achieve this, future studies should use specialised statistical methods (e.g. Statistical Parametric Mapping (SPM) analysis) to analyse the whole kinematic landing curve including all three motion planes. These methods may be valuable since they avoid focus bias, implement curve smoothness and correct for multiple comparisons. [15, 59] The different landing tasks made it also difficult to compare the results. Some researchers focused on sport specific performance, while others investigated laboratory-based landing.
Finally, three studies used a local approach in describing joint kinematics and neglected whole body kinematics [19,20,21]. However, kinematic non-local behaviour at joints located proximally or distally to the site of injury might be important to evaluate [23]. In this systematic review, two included studies introduced the LECA as a kinematic measure of the whole body’s interaction with the ground during landing [38, 40]. Eight studies incorporated pelvic and/or trunk kinematics during landing [24, 29, 39, 44, 45, 47, 50, 51]. Consequently, future prospective studies should focus on full-body 3D landing kinematics. As the development of overuse injuries is multifactorial in nature, future research should explore the multifactorial approach of these injuries [12].
4.3 Clinical implications
This systematic review and the meta-analysis provide preliminary evidence of the association between an impaired landing pattern and the development of lower extremity overuse injuries in physically active populations. More specifically, excessive frontal and transversal plane movements during repetitive landings may lead to overuse injuries and, therefore, need to be considered when screening athletes. Since two-dimensional video analysis has been found valid for 3D knee valgus displacement in subjects with a risk for PFP [19], these analyses may have an added value in rehabilitation programmes and screening tools to detect and correct impaired landing patterns with the aim of preventing (re)injuries.
5 Conclusion
There is preliminary evidence of an association between local and non-local impaired landing kinematics and lower extremity overuse injuries. More specific, excessive frontal and transversal plane movements during repeated bouts of jumping and landing manoeuvres might increase impact and tensile force acting on lower extremity musculoskeletal structures. However, strong conclusions are difficult to make due to the methodological differences between studies and the moderate study quality of the included studies. In consequence of the inclusion of cross-sectional as well as cohort studies in this systematic review, more insight has been delivered into, respectively, the kinematic consequences and risk factors of lower extremity overuse injuries. In addition, the meta-analysis confirmed these impaired landing kinematics seen in subjects with a history or new incidence of lower extremity overuse injuries.
Data Availability Statement
The authors declare that data supporting the findings of this study are available within the article and its supplementary information files.
References
Merkel DL. Youth sport: positive and negative impact on young athletes. Open Access J Sports Med. 2013;4:151–60. https://doi.org/10.2147/oajsm.S33556.
Cassel M, Muller J, Moser O, et al. Orthopedic injury profiles in adolescent elite athletes: a retrospective analysis from a sports medicine department. Front Physiol. 2019;10:544. https://doi.org/10.3389/fphys.2019.00544.
Seil R, Rupp S, Tempelhof S, et al. Sports injuries in team handball. A one-year prospective study of sixteen men’s senior teams of a superior nonprofessional level. Am J Sports Med. 1998;26(5):681–7. https://doi.org/10.1177/03635465980260051401.
Hewett TE, Myer GD, Ford KR, et al. Mechanisms, prediction, and prevention of ACL injuries: cut risk with three sharpened and validated tools. J Orthop Res. 2016;34(11):1843–55. https://doi.org/10.1002/jor.23414.
Lian ØB, Engebretsen L, Bahr R. Prevalence of jumper’s knee among elite athletes from different sports: a cross-sectional study. Am J Sports Med. 2005;33(4):561–7. https://doi.org/10.1177/0363546504270454.
Fuller CW, Ekstrand J, Junge A, et al. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Clin J Sport Med. 2006;16(2):97–106.
Bahr R. No injuries, but plenty of pain? On the methodology for recording overuse symptoms in sports. Br J Sports Med. 2009;43(13):966–72. https://doi.org/10.1136/bjsm.2009.066936.
Hein T, Janssen P, Wagner-Fritz U, et al. Prospective analysis of intrinsic and extrinsic risk factors on the development of Achilles tendon pain in runners. Scand J Med Sci Sports. 2014;24(3):E201–12. https://doi.org/10.1111/sms.12137.
Barber Foss KD, Myer GD, Chen SS, et al. Expected prevalence from the differential diagnosis of anterior knee pain in adolescent female athletes during preparticipation screening. J Athl Train. 2012;47(5):519–24. https://doi.org/10.4085/1062-6050-47.5.01.
Heebner NR, Rafferty DM, Wohleber MF, et al. Landing kinematics and kinetics at the knee during different landing tasks. J Athl Train. 2017;52(12):1101–8. https://doi.org/10.4085/1062-6050-52.11.25.
van Mechelen W, Hlobil H, Kemper HC. Incidence, severity, aetiology and prevention of sports injuries. A review of concepts. Sports Med (Auckland, NZ). 1992;14(2):82–99. https://doi.org/10.2165/00007256-199214020-00002.
Van Tiggelen D, Wickes S, Stevens V, et al. Effective prevention of sports injuries: a model integrating efficacy, efficiency, compliance and risk-taking behaviour. Br J Sports Med. 2008;42(8):648–52. https://doi.org/10.1136/bjsm.2008.046441.
van der Worp H, van der Does HTD, Brink MS, et al. Prospective Study of the Relation between Landing Biomechanics and Jumper’s Knee. Int J Sports Med. 2016;37(3):245–50.
Aerts I, Cumps E, Verhagen E, et al. A systematic review of different jump-landing variables in relation to injuries. J Sports Med Phys Fitn. 2013;53(5):509–19.
De Ridder R, Willems T, Vanrenterghem J, et al. Lower limb landing biomechanics in subjects with chronic ankle instability. Med Sci Sports Exerc. 2015;47(6):1225–31. https://doi.org/10.1249/mss.0000000000000525.
Zhang SN, Bates BT, Dufek JS. Contributions of lower extremity joints to energy dissipation during landings. Med Sci Sports Exerc. 2000;32(4):812–9. https://doi.org/10.1097/00005768-200004000-00014.
Hewett TE, Myer GD, Ford KR, et al. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med. 2005;33(4):492–501. https://doi.org/10.1177/0363546504269591.
Leppanen M, Pasanen K, Krosshaug T, et al. Sagittal plane hip, knee, and ankle biomechanics and the risk of anterior cruciate ligament injury: a prospective study. Orthop J Sports Med. 2017;5(12):2325967117745487. https://doi.org/10.1177/2325967117745487.
Holden S, Boreham C, Doherty C, et al. Two-dimensional knee valgus displacement as a predictor of patellofemoral pain in adolescent females. Scand J Med Sci Sports. 2017;27(2):188–94. https://doi.org/10.1111/sms.12633.
Richards DP, Ajemian SV, Wiley JP, et al. Knee joint dynamics predict patellar tendinitis in elite volleyball players. Am J Sports Med. 1996;24(5):676–83. https://doi.org/10.1177/036354659602400520.
Myer GD, Ford KR, Barber Foss KD, et al. The incidence and potential pathomechanics of patellofemoral pain in female athletes. Clin Biomech (Bristol, Avon). 2010;25(7):700–7. https://doi.org/10.1016/j.clinbiomech.2010.04.001.
De Blaiser C, Roosen P, Willems T, et al. Is core stability a risk factor for lower extremity injuries in an athletic population? A systematic review. Phys Ther Sport. 2018;30:48–56. https://doi.org/10.1016/j.ptsp.2017.08.076.
Chuter VH, de Jonge JXA. Proximal and distal contributions to lower extremity injury: a review of the literature. Gait Posture. 2012;36(1):7–15. https://doi.org/10.1016/j.gaitpost.2012.02.001.
Verrelst R, De Clercq D, Willems TM, et al. Contralateral risk factors associated with exertional medial tibial pain in women. Med Sci Sports Exerc. 2014;46(8):1546–53. https://doi.org/10.1249/MSS.0000000000000280.
Blackburn JT, Padua DA. Influence of trunk flexion on hip and knee joint kinematics during a controlled drop landing. Clin Biomech (Bristol, Avon). 2008;23(3):313–9. https://doi.org/10.1016/j.clinbiomech.2007.10.003.
Kulas A, Zalewski P, Hortobagyi T, et al. Effects of added trunk load and corresponding trunk position adaptations on lower extremity biomechanics during drop-landings. J Biomech. 2008;41(1):180–5. https://doi.org/10.1016/j.jbiomech.2007.06.027.
Powers CM. The influence of abnormal hip mechanics on knee injury: a biomechanical perspective. J Orthop Sports Phys Ther. 2010;40(2):42–51. https://doi.org/10.2519/jospt.2010.3337.
Siegmund JA, Huxel KC, Swanik CB. Compensatory mechanisms in basketball players with jumper’s knee. J Sport Rehabil. 2008;17(4):359–71.
Scattone Silva R, Purdam CR, Fearon AM, et al. Effects of altering trunk position during landings on patellar tendon force and pain. Med Sci Sports Exerc. 2017;49(12):2517–27. https://doi.org/10.1249/mss.0000000000001369.
Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377–84. https://doi.org/10.1136/jech.52.6.377.
Neal BS, Barton CJ, Gallie R, et al. Runners with patellofemoral pain have altered biomechanics which targeted interventions can modify: a systematic review and meta-analysis. Gait Posture. 2016;45:69–82. https://doi.org/10.1016/j.gaitpost.2015.11.018.
Barton CJ, Levinger P, Menz HB, et al. Kinematic gait characteristics associated with patellofemoral pain syndrome: a systematic review. Gait Posture. 2009;30(4):405–16. https://doi.org/10.1016/j.gaitpost.2009.07.109.
Ceyssens L, Vanelderen R, Barton C, et al. Biomechanical risk factors associated with running-related injuries: a systematic review. Sports Med (Auckland, NZ). 2019;49(7):1095–115. https://doi.org/10.1007/s40279-019-01110-z.
Meeus M GN. In: Literacy H, editor. From reference to review. Leuven (Belgium)/Den Haag (The Netherlands). 2016.
Guyatt GH, Oxman AD, Kunz R, et al. GRADE guidelines: 7. Rating the quality of evidence–inconsistency. J Clin Epidemiol. 2011;64(12):1294–302. https://doi.org/10.1016/j.jclinepi.2011.03.017.
Bisseling RW, Hof AL, Bredeweg SW, et al. Relationship between landing strategy and patellar tendinopathy in volleyball. Br J Sports Med. 2007;41(7):e8.
Bisseling RW, Hof AL, Bredeweg SW, et al. Are the take-off and landing phase dynamics of the volleyball spike jump related to patellar tendinopathy? Br J Sports Med. 2008;42(6):483–9. https://doi.org/10.1136/bjsm.2007.044057.
Fietzer AL, Chang YJ, Kulig K. Dancers with patellar tendinopathy exhibit higher vertical and braking ground reaction forces during landing. J Sports Sci. 2012;30(11):1157–63. https://doi.org/10.1080/02640414.2012.695080.
Harris M, Schultz A, Drew MK, et al. Jump-landing mechanics in patellar tendinopathy in elite youth basketballers. Scand J Med Sci Sports. 2020;30(3):540–8. https://doi.org/10.1111/sms.13595.
Kulig K, Joiner DG, Chang YJ. Landing limb posture in volleyball athletes with patellar tendinopathy: a Pilot Study. Int J Sports Med. 2015;36(5):400–6.
Souza RB, Arya S, Pollard CD, et al. Patellar tendinopathy alters the distribution of lower extremity net joint moments during hopping. J Appl Biomech. 2010;26(3):249–55. https://doi.org/10.1123/jab.26.3.249.
Nunes GS, Barton CJ, Serrao FV. Females with patellofemoral pain have impaired impact absorption during a single-legged drop vertical jump. Gait Posture. 2019;68:346–51. https://doi.org/10.1016/j.gaitpost.2018.12.013.
Rosen AB, Ko J, Simpson KJ, et al. Lower extremity kinematics during a drop jump in individuals with patellar tendinopathy. Orthop J Sports Med. 2015;3(3):2325967115576100. https://doi.org/10.1177/2325967115576100.
Willson JD, Davis IS. Lower extremity strength and mechanics during jumping in women with patellofemoral pain. J Sport Rehabil. 2009;18(1):76–90.
Willson JD, Davis IS. Lower extremity mechanics of females with and without patellofemoral pain across activities with progressively greater task demands. Clin Biomech. 2008;23(2):203–11. https://doi.org/10.1016/j.clinbiomech.2007.08.025.
Willson JD, Davis IS. Utility of the frontal plane projection angle in females with patellofemoral pain. J Orthop Sports Phys Ther. 2008;38(10):606–15. https://doi.org/10.2519/jospt.2008.2706.
van Rensburg LJ, Dare M, Louw Q, et al. Pelvic and hip kinematics during single-leg drop-landing are altered in sports participants with long-standing groin pain: a cross-sectional study. Phys Ther Sport. 2017;26:20–6. https://doi.org/10.1016/j.ptsp.2017.05.003.
Boling MC, Nguyen AD, Padua DA, et al. Gender-specific risk factor profiles for patellofemoral pain. Clin J Sport Med. 2019. https://doi.org/10.1097/jsm.0000000000000719.
Boling MC, Padua DA, Marshall SW, et al. A prospective investigation of biomechanical risk factors for patellofemoral pain syndrome: the Joint Undertaking to Monitor and Prevent ACL Injury (JUMP-ACL) cohort. Am J Sports Med. 2009;37(11):2108–16. https://doi.org/10.1177/0363546509337934.
Verrelst R, De Clercq D, Vanrenterghem J, et al. The role of proximal dynamic joint stability in the development of exertional medial tibial pain: a prospective study. Br J Sports Med. 2014;48(5):388–93. https://doi.org/10.1136/bjsports-2012-092126.
Verrelst R, De Clercq D, Willems TM, et al. Contribution of a muscle fatigue protocol to a dynamic stability screening test for exertional medial tibial pain. Am J Sports Med. 2014;42(5):1219–25.
van der Does HT, Brink MS, Benjaminse A, et al. Jump landing characteristics predict lower extremity injuries in indoor team sports. Int J Sports Med. 2016;37(3):251–6. https://doi.org/10.1055/s-0035-1559688.
Cannon J, Cambridge EDJ, McGill SM. Anterior cruciate ligament injury mechanisms and the kinetic chain linkage: the effect of proximal joint stiffness on distal knee control during bilateral landings. J Orthop Sports Phys Ther. 2019;49(8):601–10. https://doi.org/10.2519/jospt.2019.8248.
Mirzaie GH, Rahimi A, Kajbafvala M, et al. Electromyographic activity of the hip and knee muscles during functional tasks in males with and without patellofemoral pain. J Bodyw Mov Ther. 2019;23(1):54–8. https://doi.org/10.1016/j.jbmt.2018.11.001.
Edwards S, Steele JR, McGhee DE, et al. Landing strategies of athletes with an asymptomatic patellar tendon abnormality. Med Sci Sports Exerc. 2010;42(11):2072–80. https://doi.org/10.1249/MSS.0b013e3181e0550b.
Huberti HH, Hayes WC. Patellofemoral contact pressures. The influence of q-angle and tendofemoral contact. J Bone Jt Surg Am Vol. 1984;66(5):715–24.
Maffey L, Emery C. What are the risk factors for groin strain injury in sport? A systematic review of the literature. Sports Med (Auckland, NZ). 2007;37(10):881–94. https://doi.org/10.2165/00007256-200737100-00004.
DiCesare CA, Montalvo A, Barber Foss KD, et al. Lower extremity biomechanics are altered across maturation in sport-specialized female adolescent athletes. Front Pediatr. 2019;7:268. https://doi.org/10.3389/fped.2019.00268.
Pataky TC, Robinson MA, Vanrenterghem J. Vector field statistical analysis of kinematic and force trajectories. J Biomech. 2013;46(14):2394–401. https://doi.org/10.1016/j.jbiomech.2013.07.031.
Author information
Authors and Affiliations
Contributions
CaDB and SV contributed equally to the design of the study, literature search, data screening and extraction and risk of bias assessment; conducted all statistical analyses and managed the aspects of the manuscript writing, editing and submission. All authors revised critically for important intellectual content and approved the final version to be submitted.
Corresponding author
Ethics declarations
Funding
The authors did not receive any specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing Interests
All of the authors declare that they have no competing interests.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
De Bleecker, C., Vermeulen, S., De Blaiser, C. et al. Relationship Between Jump-Landing Kinematics and Lower Extremity Overuse Injuries in Physically Active Populations: A Systematic Review and Meta-Analysis. Sports Med 50, 1515–1532 (2020). https://doi.org/10.1007/s40279-020-01296-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-020-01296-7