
Abstract
Background
Physical exercise is beneficial to reduce the risk of several conditions associated with advanced age, but to our knowledge, no previous study has examined the association of long-term exercise interventions (≥ 1 year) with the occurrence of dropouts due to health issues and mortality, or the effectiveness of physical exercise versus usual primary care interventions on health-related outcomes in older adults (≥ 65 years old).
Objective
To analyze the safety and effectiveness of long-term exercise interventions in older adults.
Methods
We conducted a systematic review with meta-analysis examining the association of long-term exercise interventions (≥ 1 year) with dropouts from the corresponding study due to health issues and mortality (primary endpoint), and the effects of these interventions on health-related outcomes (falls and fall-associated injuries, fractures, physical function, quality of life, and cognition) (secondary endpoints).
Results
Ninety-three RCTs and six secondary studies met the inclusion criteria and were included in the analyses (n = 28,523 participants, mean age 74.2 years). No differences were found between the exercise and control groups for the risk of dropouts due to health issues (RR = 1.05, 95% CI 0.95–1.17) or mortality (RR = 0.93, 95% CI 0.83–1.04), although a lower mortality risk was observed in the former group when separately analyzing clinical populations (RR = 0.67, 95% CI 0.48–0.95). Exercise significantly reduced the number of falls and fall-associated injuries, and improved physical function and cognition. These results seemed independent of participants’ baseline characteristics (age, physical function, and cognitive status) and exercise frequency.
Conclusions
Long-term exercise training does not overall influence the risk of dropouts due to health issues or mortality in older adults, and results in a reduced mortality risk in clinical populations. Moreover, exercise reduces the number of falls and fall-associated injuries, and improves physical function and cognition in this population.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Long-term exercise does not influence the risk of dropouts due to health issues or mortality in older adults and results in a reduced mortality risk in clinical populations. |
Exercise reduces the number of falls and fall-associated injuries and improves physical function and cognition in this population. |
Long-term exercise training interventions are an effective and beneficial strategy in older adults for the prevention falls and fall-associated injuries and improvement of physical function and cognition. |
1 Introduction
The growing prevalence of physical inactivity among older adults represents an important public health problem in light of global population aging [1, 2]. For instance, only 27–44% of older U.S. adults meet international physical activity recommendations (≥ 150 min per week of moderate-to-vigorous physical activity) [3]. In this respect, regular exercise has multi-system anti-aging effects [4], and can attenuate the deleterious effects of inactivity while increasing healthy lifespan [5].
Recent systematic reviews and meta-analyses have concluded that physical exercise is beneficial to reduce the risk of several conditions associated with an advanced age, such as frailty [6], cognitive decline [7], low muscle power, or poor functional capacity [8]. There is also evidence that exercise intervention programs can prevent falls in older people with minor concomitant adverse effects [9,10,11]. To the best of our knowledge, however, no study has specifically analyzed the risk of dropouts from an exercise program due to health issues (adverse events, medical problems) in older persons, or the effect of this type of intervention on risk of mortality, with both outcomes being indicators of the safety and practical applicability of this type of lifestyle intervention in this population segment. It also remains to be determined whether the type of participant (age, health status) or intervention influences the risk of dropouts or mortality.
It was, therefore, the aim of our study to systematically review and meta-analyze (i) the association of long-term exercise programs (≥ 1 year) with dropouts due to health issues and risk of mortality in older adults (primary endpoints), and (ii) the effects of this type of intervention on health-related outcomes, including physical function, cognition status, health-related quality of life, risk of hospitalization, falls and fall-associated injuries, and fractures (secondary endpoints).
2 Methods
2.1 Protocol and Registration
This study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement checklist [12] and is registered in the International Prospective Register of Systematic Reviews (PROSPERO) (Registration number: CRD42020139614) (Electronic Supplementary Material Appendix S1).
2.2 Information Sources and Search
Searches in PubMed, Cochrane Controlled Trials Registry, and SPORTDiscus combined with manual searches of existing literature were done from inception to September 16, 2019. The search strategy applied is available in Electronic Supplementary Material Appendix S2. In addition, the reference list of each of the included studies was reviewed to find potential studies that could be used in this review.
2.3 Eligibility Criteria and Study Selection
The criteria for a study to be included in the systematic review were the following: (i) adults aged ≥ 65 years assessed at baseline; (ii) a randomized controlled trial (RCT) design, where the control group received usual care combined or not with a nutritional or educational intervention, but no structured physical exercise intervention; (iii) the study assessed the occurrence of dropouts due to health issues and/or mortality; and (iv) the exercise intervention lasted ≥ 1 year. Regarding exercise programs, no restrictions were made in terms of combination or not with a concomitant nutritional intervention, supervision or structure (e.g., supervised group based, unsupervised home based or a combination thereof), setting (e.g., community dwellers or institutionalized), or exercise modality, frequency or intensity (i.e., whether focusing only on either muscle strength [‘resistance’] or aerobic exercises, including multicomponent exercise training [combined aerobic, muscle strength, and balance exercises], or using Tai Chi). However, when the study included a nutritional intervention (e.g., health education), both the control and exercise groups had to participate in this intervention.
We excluded those studies with the following characteristics: (i) the exercise intervention was not well defined; (ii) included subjects aged < 65 years; and (iii) did not include a control (non-exercise) group for comparison. Titles, abstracts and full texts were assessed for eligibility independently by two authors (AG-H and RR-V) for potential inclusion. If necessary, a third researcher (MI) was consulted. Finally, only those papers written in the English language were included.
2.4 Data Collection Process
For each study, the following data were extracted (i) first author’s last name; (ii) year of publication; (iii) country; (iv) study setting; (v) sample size, participants’ characteristics and mean age; and (vi) characteristics of the exercise (exercise modality, frequency, and duration) and control intervention.
2.5 Endpoints
Primary endpoints were dropouts (defined as the number of randomized participants having no post-intervention measurements available due to health issues [medical problems, adverse events]), and mortality. Secondary endpoints were the following: physical function, cognition status, health-related quality of life, risk of hospitalization (inpatient hospitalization ≥ 24 h), falls (people who fell at least once) and fall-associated injuries, and fractures (number of people who sustained a fracture). When there was insufficient information, the corresponding author of the study in question was contacted.
2.6 Risk of Bias of Individual Studies
The risk of bias was evaluated using the Physiotherapy Evidence Database (PEDro) criteria [13], using an 11-item scale designed for measuring the methodological quality of RCT.
2.7 Statistical Analyses
All analyses were carried out using Comprehensive Meta-analysis Software (2nd version, Biostat; Englewood, NJ, USA) to calculate (i) the risk ratio (RR) for dichotomous outcomes, that is, dropouts due to health issues, mortality, hospitalization, falls, and fractures; or (ii) the standardized mean difference (SMD) for continuous data (i.e., physical function parameters, cognition and health-related quality of life parameters) [14]. The RR or SMD of each parameter (from baseline to follow-up) between groups [15] was calculated and pooled using a random-effects model (DerSimonian–Laird approach). For continuous outcomes, the pooled effect size for SMD was classified as small (0 ≤ SMD ≤ 0.50), moderate (0.50 < SMD ≤ 0.80) or large (SMD > 0.80) [16].
The percentage of total variation across studies due to heterogeneity (Cochran’s Q test) was used to calculate the I2 statistic [17], considering I2 values < 25%, 25–75%, and > 75% as indicators of small, moderate, and high heterogeneity, respectively [18]. Each study was removed once from the model to analyze its individual influence on the overall results. Egger’s regression tests and funnel plots were performed to detect small study effects and possible publication bias [19]. Data were pooled if outcomes were reported in at least 10 studies, because the power of the tests for funnel plot asymmetry is too low to distinguish chance from real asymmetry when fewer studies are evaluated [14].
When possible, a subgroup analysis for the primary endpoint was conducted taking into account the following potential moderators: type of exercise intervention, participants’ health status (apparently healthy vs clinical population), intervention structure (supervised group based, unsupervised home based, or a combination thereof), primary mode of exercise intervention (muscle strength [or ‘resistance’]-based, aerobic-based, multicomponent exercise training, or Tai Chi), study setting (community dwellers vs institutionalized), and risk of bias (PEDro Scale score < 7 or ≥ 7) [10]. Additionally, random-effects meta-regression analyses were used to evaluate the influence of age, physical function and cognition characteristics at baseline and the frequency of exercise (number of sessions per week) in the primary endpoints (dropouts due to health issues, and risk of mortality).
3 Results
3.1 Study Selection
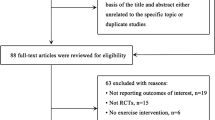
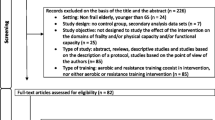
From the retrieved articles, 93 RCTs [1, 20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111] and 6 [112,113,114,115,116,117] secondary studies met the inclusion criteria and were included in the analyses (with secondary studies being only included to pool the secondary outcomes) (Fig. 1). However, due to missing data, we have included only 90 RCTs in the quantity analysis (meta-analysis).

PRISMA flow diagram
3.2 Study Characteristics
The characteristics of the included studies are summarized in Electronic Supplementary Material Table S1. The final analysis included 28,523 participants (mean age 74.2 years). Most studies included apparently healthy older adults, but 25 RCTs were conducted in clinical populations (i.e., individuals with cancer [n = 3 studies], mild cognitive impairment, Parkinson, Alzheimer or dementia [n = 11], or cardiorespiratory [n = 4], renal [n = 1], musculoskeletal [n = 3], or metabolic [n = 3] disease). Participants enrolled in the different studies were predominantly from the U.S. (n = 23 articles), with other studies from Australia (n = 15), Belgium (n = 2), Brazil (n = 2), Canada (n = 5), Chile (n = 2), Denmark (n = 2), Finland (n = 8), France (n = 3), Germany (n = 5), Hong Kong (n = 4), Hungary (n = 2), Japan (n = 2), The Netherlands (n = 1), New Zealand (n = 4), South Korea (n = 1), Spain (n = 2), Sweden (n = 2), Taiwan (n = 1), Thailand (n = 2), or the UK (n = 5). Most studies included men and women except four [78, 81, 90, 118] that included only men, and 19 studies with women only [30, 33, 34, 42, 44, 49, 61, 62, 68, 69, 72, 83, 88, 89, 93, 95, 99, 103, 108]. Sample sizes across studies ranged from 20 [23, 56] to 6420 [54] participants.
The primary mode of exercise intervention was multicomponent exercise training (n = 47), followed by muscle strength (n = 24) and aerobic training (e.g., walking, dancing) (n = 19), and Tai Chi (n = 4). Most studies used group-based supervised exercise training alone (n = 56) or combined with home-based unsupervised training (n = 21). The duration of the interventions ranged from 52 (in most studies) to 208 [85] weeks, and training frequency ranged from 1 to 7 sessions per week, with a duration of 10–90 min per session. Most control groups were instructed to maintain usual activity levels with or without an additional non-exercise intervention (e.g., health education, social visits, or telephone calls).
3.3 Risk of Bias Within Studies
The average total score was 6.1 with a range of 1–8. Thirty-six studies scored 7 or higher. Low scores corresponded to studies that failed to conceal allocation (40.2%), or to blind subjects (0%), or had researchers in charge of endpoint assessment and/or exercise supervision (1.0%) (Electronic Supplementary Material Table S2).
3.4 Synthesis of Results
3.4.1 Primary Endpoints
Dropouts due to health issues Forty-nine studies provided information on dropouts due to medical problems for 21,292 participants. Overall, 16.9% (1638 older adults) and 19.0% (2207 older adults) of participants dropped out of the corresponding study due to health issues in the exercise and control group, respectively (Electronic Supplementary Material Table S3). Exercise and control groups did not differ in terms of dropouts due to medical problems (RR = 1.05, 95% confidence interval [CI] 0.95–1.17), with low heterogeneity for this result (I2 = 14.07%).
All subgroup analyses provided similar results independent of the study setting, type of exercise training, or risk of bias (Table 1). The meta-regression analyses showed that participants’ age, physical function or cognition at baseline, or exercise frequency (number of exercise sessions per week) was not related to risk of mortality (ß = − 0.13–0.03) (Table 2 and Electronic Supplementary Material Figure S1–S5).
There was no evidence of publication bias in the analysis of dropouts due to medical problems (p = 0.618), and the results remained the same in the sensitivity analysis. The funnel plot is presented in Electronic Supplementary Material Figure S6.
Mortality Fifty-six RCTs provided information on death for 26,017 participants. Of these, 19 reported no deaths during the trial [26, 28, 36, 38, 44, 48, 49, 55, 56, 78, 79, 81, 86, 92, 93, 103, 107, 108, 119]. Exercise intervention had no effects on mortality (RR = 0.93, 95% CI 0.83–1.04), with low heterogeneity between studies (I2= 0%). Specifically, 5.5% (664 older adults) and 5.8% (820 older adults) of participants died in the exercise and control groups, respectively (Electronic Supplementary Material Table S3). All subgroup analyses provided similar results (Table 1), except for the analysis restricted to clinical populations, which showed that exercise significantly (p = 0.024) reduced the risk of mortality (RR = 0.67, 95% CI 0.48–0.95; I2= 0%) (Table 1).
The meta-regression analyses showed that neither age nor physical function nor cognition at baseline was associated with risk of mortality (ß = − 0.20– 0.09) (Table 2 and Electronic Supplementary Material Figure S7–S11).
There was no evidence of publication bias in the analysis of mortality (p = 0.097), and the results remained the same in the sensitivity analysis. The funnel plot is presented in Electronic Supplementary Material Figure S12.
3.4.2 Secondary Endpoints
The secondary endpoint measures (which were pooled when there were ≥ 10 studies per endpoint) were: physical function (assessed with balance tests, gait speed, knee-extension strength, timed get-up-and-go test, sit-to-stand test, and the short physical fitness battery [SPPB]), cognition status (assessed with the mini-mental state examination [MMSE]), health-related quality of life (assessed with the Short Form Health Survey [SF]-36 or SF-12), and risk of hospitalization, falls, fall-associated injuries, and fractures.
Compared with the control group, exercise interventions were associated with a significantly lower number of falls and fall-associated injuries, as well as with improvements in all analyzed physical function parameters (balance, gait speed knee-extension strength, SPPB, sit-to-stand and timed get-up-and-go tests) and cognition (MMSE) (Table 3). The forest plots are shown in Electronic Supplementary Material Figure S13–S25.
Finally, Fig. 2 illustrates how long-term physical exercise programs are safe and effective among older adults.

This figure illustrates how long-term physical exercise programs are safe and effective among older adults. Green arrows represent significant results and blue equal signs depict non-negative effects. Numbers in brackets represent data results for each parameter. RR risk ratio, SMD standardized mean difference. *The results are shown in Table 3
4 Discussion
The present meta-analysis found that long-term (≥ 1 year) exercise training interventions in older adults do not cause more dropouts due to health issues and do not affect mortality compared with a control (usual care) group. Similar results were found for risk of hospitalization and fractures. Importantly, however, these types of interventions are associated with a lower risk of falls and fall-induced injuries, and with improvements in muscle strength, balance, physical function, and cognition. Moreover, a lower risk of mortality was found in a separate analysis for patient populations only. Therefore, long-term physical exercise is overall safe and effective in older adults, and its benefits appear to be independent of participants’ age, physical function or cognition status at baseline.
To determine the safety of exercise training, we registered the number of dropouts per group due to health issues, and the pooled analysis suggests that physical exercise does not increase the risk of dropouts compared with the control group, and thus, compliance to this type of intervention does not seem to be compromised by health issues related to the intervention itself. In the same line, a recent systematic review reported only minor harms of exercise interventions aiming at preventing falls in community-dwelling older adults [11]. Therefore, our results, together with the aforementioned study [11], suggest that, beyond its practical benefits, exercise does not cause more harm among older adults than maintaining usual activity levels or usual care. Similar to the conclusions of our review, recent meta-analyses have reported that long-term exercise training does not increase the overall risk of mortality in older adults [9, 11]. The magnitude of the association for the risk of mortality in our review in patients and healthy individuals combined (56 RCTs, RR = 0.93, 95% CI 0.83–1.04) is in general agreement with the results reported by Barreto et al. [9] (RR = 0.96, 95% CI 0.85–1.09) and Guirguis-Blakeet al. [11] (RR = 0.96, 95% CI 0.79–1.17). In line with recent research [9], the risk of mortality in the general population of older adults is unlikely to be affected by exercise interventions alone. However, an important finding of our review is that long-term exercise decreases mortality risk specifically in clinical populations of older adults (16 RCTs; RR = 0.67, 95% CI 0.48–0.95). In this respect, a recent population-based cohort study reported significantly lower risk of mortality if becoming physically active among middle-aged and older patients with cardiovascular disease and cancer, which reinforces the role of physical exercise as a core therapeutic element for treating prevalent diseases [120].
Subgroup analyses revealed that type of physical exercise training, setting of the study, and risk of bias do not appear to influence the effect of exercise on the primary endpoint; that is, dropouts due to medical problems and mortality. We also evaluated the influence of age, cognition, physical function and exercise frequency on these results. With regard to age, although one could expect a priori that older participants are at greater risk of having adverse events when enrolling in an exercise program, this hypothesis was not corroborated by our results. In this respect, Hewitt et al. [41] showed a lower risk of dropouts due to health issues (RR = 0.35, 95% CI 0.15–0.91) in the exercise group, in individuals with low physical function level (SPPB score < 9) [121]. However, the results of the present meta-regression analysis should be interpreted with caution because the low number of studies might have affected the results.
With regard to secondary endpoints, our findings corroborate the results of a recent meta-analysis showing that exercise decreased the risk of falls and fall-associated injuries [9], and similar results were reported by Guirguis-Blake et al. for the US Preventive Services Task Force [11]. Thus, there seems to be compelling evidence to support the positive effects of exercise against fall-related outcomes in older adults. Furthermore, our review extends this literature by examining, for the first time, the association of long-term exercise training with several health outcomes in an elderly population, showing significant improvements in physical function and cognition parameters, and providing further support to the notion that regular exercise is necessary for healthy aging and offers multi-systemic health benefits [122].
Some limitations of our review should be acknowledged. First, health issues were recorded through dropouts and we cannot determine whether they were directly associated with physical exercise. In this regard, however, most RCTs reported only minor harms associated with exercise interventions. Second, the included RCTs were heterogeneous with respect to exercise training protocols and study population (healthy vs clinical population); however, we performed subgroup analyses to account for heterogeneity among studies. Third, most of the analyzed studies included community-dwelling older adults, and the small number of studies with institutionalized elderly people (n = 9) prevented us from performing a separate subgroup analysis, thereby limiting the generalizability of our results. On the other hand, a main strength of our meta-analysis is that it is, to our knowledge, the first to determine both the safety and effectiveness of long-term physical exercise interventions among older adults. Our meta-analysis provides an update and extension of the evidence reported in an earlier reviews [9], including more studies and other health outcomes. Furthermore, according to the Cochrane Handbook, and to avoid publication bias, we pooled only the results of those outcomes that were reported by at least 10 studies [14], thereby avoiding any loss of statistical power.
5 Conclusion
Compared with usual care, long-term (≥ 1 year) exercise training interventions in older adults do not increase the risk of dropouts due to health issues, mortality, hospitalization, or fractures, but do decrease the risk of falls and fall-associated injuries and mortality (although the latter only in clinical populations), while improving physical function and cognition. Therefore, health care professionals have an important role to play in reducing the prevalence of inactivity and fostering regular exercise among older adults.
Data Availability Statement
The data that support the findings of this review are available on request from the corresponding author (Mikel Izquierdo).
References
Pahor M, Guralnik JM, Ambrosius WT, Blair S, Bonds DE, Church TS, et al. Effect of structured physical activity on prevention of major mobility disability in older adults: the LIFE study randomized clinical trial. JAMA [Internet]. 2014;311:2387–96 (cited 2019 Aug 4).
He W, Goodkind D, Kowal P. International population reports. P95/16-1, An aging world: 2015. US Census Bureau, editors. Washington, DC: US Government Publishing Office, 2016.
Keadle SK, McKinnon R, Graubard BI, Troiano RP. Prevalence and trends in physical activity among older adults in the United States: a comparison across three national surveys. Prev Med (Baltim). 2016;89:37–43.
Garatachea N, Pareja-Galeano H, Sanchis-Gomar F, Santos-Lozano A, Fiuza-Luces C, Morán M, et al. Exercise attenuates the major hallmarks of aging. Rejuvenation Res. 2015;18:57–89.
Chodzko-Zajko WJ, Proctor DN, Fiatarone Singh MA, Minson CT, Nigg CR, Salem GJ, et al. Exercise and physical activity for older adults. Med Sci Sport Exerc. 2009;41:1510–30.
Silva RB, Aldoradin-Cabeza H, Eslick GD, Phu S, Duque G. The effect of physical exercise on frail older oersons: a systematic review. J Frailty Aging. 2017;6:91–6.
Zheng G, Xia R, Zhou W, Tao J, Chen L. Aerobic exercise ameliorates cognitive function in older adults with mild cognitive impairment: a systematic review and meta-analysis of randomised controlled trials. Br J Sports Med. 2016;50:1443–50.
Chase J-AD, Phillips LJ, Brown M. Physical activity intervention effects on physical function among community-dwelling older adults: a systematic review and meta-analysis. J Aging Phys Act. 2017;25:149–70.
De Souto Barreto P, Rolland Y, Vellas B, Maltais M. Association of long-term exercise training with risk of falls, fractures, hospitalizations, and mortality in older adults: a systematic review and meta-analysis. JAMA Intern Med. 2019;179:394–405.
Sherrington C, Michaleff ZA, Fairhall N, Paul SS, Tiedemann A, Whitney J, et al. Exercise to prevent falls in older adults: an updated systematic review and meta-analysis. Br J Sports Med. 2017;51:1750–8.
Guirguis-Blake JM, Michael YL, Perdue LA, Coppola EL, Beil TL. Interventions prevent falls in older adults: updated evidence report and systematic review for the US preventive services task force. JAMA. 2018;319:1705–16.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009;6:e1000100.
Maher C, Sherrington C, Herbert RD, et al. Reliability of the PEDro scale for rating quality of randomized controlled trials. academic.oup.com. https://academic.oup.com/ptj/article-abstract/83/8/713/2805287. Accessed 29 June 2019.
Higgins JP, Green S, editors. Cochrane handbook for systematic reviews of interventions. Chichester: Wiley; 2008.
Morris S-18th annual conference of the S, 2003 U. Estimating effect size from the pretest-posttest-control design. http://faculty.cas.usf.edu/mbrannick/papers/conf/esppcsiop03.pdf. Accessed 29 June 2019.
Cohen J. Statistical power analysis for the behavioral sciences. 2013.
Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21:1539–58.
Higgins J, Thompson S, Deeks J, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60.
Egger M, Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34.
Arrieta H, Astrugue C, Regueme S, Durrieu J, Maillard A, Rieger A, et al. Effects of a physical activity programme to prevent physical performance decline in onco-geriatric patients: a randomized multicentre trial. J Cachexia Sarcopenia Muscle. 2019;10:287–97.
Barnett A. Community-based group exercise improves balance and reduces falls in at-risk older people: a randomised controlled trial. Age Ageing. 2003;32:407–14.
Batchelor FA, Hill KD, Mackintosh SF, Said CM, Whitehead CH. Effects of a multifactorial falls prevention program for people with stroke returning home after rehabilitation: a randomized controlled trial. Arch Phys Med Rehabil. 2012;93:1648–55.
Baum EE, Jarjoura D, Polen AE, Faur D, Rutecki G. Effectiveness of a group exercise program in a long-term care facility: a randomized pilot trial. J Am Med Dir Assoc. 2003;4:74–80.
Becker C, Kron M, Lindemann U, Sturm E, Eichner B, Walter-Jung B, et al. Effectiveness of a multifaceted intervention on falls in nursing home residents. J Am Geriatr Soc. 2003;51:306–13.
Blumenthal JA, Emery CF, Madden DJ, Coleman RE, Riddle MW, Schniebolk S, et al. Effects of exercise training on cardiorespiratory function in men and women older than 60 years of age. Am J Cardiol. 1991;67:633–9.
Bogaerts A, Verschueren S, Delecluse C, Claessens AL, Boonen S. Effects of whole body vibration training on postural control in older individuals: a 1 year randomized controlled trial. Gait Posture. 2007;26:309–16.
Brandon LJ, Gaasch DA, Boyette LW, Lloyd AM. Effects of long-term resistive training on mobility and strength in older adults with diabetes. Journals Gerontol Ser A Biol Sci Med Sci. 2003;58:M740–5.
Brandon LJ, Boyette LW, Lloyd A, Gaasch DA. Resistive training and long-term function in older adults. J Aging Phys Act. 2004;12:10–28.
Bunout D, Barrera G, Avendaño M, de la Maza P, Gattas V, Leiva L, et al. Results of a community-based weight-bearing resistance training programme for healthy Chilean elderly subjects. Age Ageing. 2005;34:80–3.
Campbell AJ, Robertson MC, Gardner MM, Norton RN, Tilyard MW, Buchner DM. Randomised controlled trial of a general practice programme of home based exercise to prevent falls in elderly women. BMJ. 1997;315:1065–9.
Clemson L, Fiatarone Singh MA, Bundy A, Cumming RG, Manollaras K, O’Loughlin P, et al. Integration of balance and strength training into daily life activity to reduce rate of falls in older people (the LiFE study): randomised parallel trial. BMJ. 2012;345:e4547.
Dangour AD, Albala C, Allen E, Grundy E, Walker DG, Aedo C, et al. Effect of a nutrition supplement and physical activity program on pneumonia and walking capacity in Chilean older people: a factorial cluster randomized trial. PLoS Med. 2011;8:e1001023.
Ebrahim S, Thompson PW, Baskaran V, Evans K. Randomized placebo-controlled trial of brisk walking in the prevention of postmenopausal osteoporosis. Age Ageing. 1997;26:253–60.
El-Khoury F, Cassou B, Latouche A, Aegerter P, Charles M-A, Dargent-Molina P. Effectiveness of two year balance training programme on prevention of fall induced injuries in at risk women aged 75-85 living in community: ossébo randomised controlled trial. BMJ. 2015;351:h3830.
Elley CR, Robertson MC, Garrett S, Kerse NM, McKinlay E, Lawton B, et al. Effectiveness of a falls-and-fracture nurse coordinator to reduce falls: a randomized, controlled trial of at-risk older adults. J Am Geriatr Soc. 2008;56:1383–9.
Erickson KI, Voss MW, Prakash RS, Basak C, Szabo A, Chaddock L, et al. Exercise training increases size of hippocampus and improves memory. Proc Natl Acad Sci. 2011;108:3017–22.
Fairhall N, Sherrington C, Kurrle SE, Lord SR, Lockwood K, Cameron ID. Effect of a multifactorial interdisciplinary intervention on mobility-related disability in frail older people: randomised controlled trial. BMC Med. 2012;10:120.
Foster ER, Golden L, Duncan RP, Earhart GM. Community-based Argentine tango dance program is associated with increased activity participation among individuals with Parkinson’s disease. Arch Phys Med Rehabil. 2013;94:240–9.
Gianoudis J, Bailey CA, Ebeling PR, Nowson CA, Sanders KM, Hill K, et al. Effects of a targeted multimodal exercise program incorporating high-speed power training on falls and fracture risk factors in older adults: a community-based randomized controlled trial. J Bone Miner Res. 2014;29:182–91.
Graessel E, Stemmer R, Eichenseer B, Pickel S, Donath C, Kornhuber J, et al. Non-pharmacological, multicomponent group therapy in patients with degenerative dementia: a 12-month randomizied, controlled trial. BMC Med. 2011;9:129.
Hewitt J, Goodall S, Clemson L, Henwood T, Refshauge K. Progressive resistance and balance training for falls prevention in long-term residential aged care: a cluster randomized trial of the Sunbeam Program. J Am Med Dir Assoc. 2018;19:361–9.
Karinkanta S, Heinonen A, Sievänen H, Uusi-Rasi K, Pasanen M, Ojala K, et al. A multi-component exercise regimen to prevent functional decline and bone fragility in home-dwelling elderly women: randomized, controlled trial. Osteoporos Int. 2007;18:453–62.
King AC, Pruitt LA, Phillips W, Oka R, Rodenburg A, Haskell WL. Comparative effects of two physical activity programs on measured and perceived physical functioning and other health-related quality of life outcomes in older adults. J Gerontol A Biol Sci Med Sci. 2000;55:M74–83.
Liu-Ambrose T, Nagamatsu LS, Graf P, Beattie BL, Ashe MC, Handy TC. Resistance training and executive functions. Arch Intern Med. 2010;170:170.
Liu-Ambrose T, Davis JC, Best JR, Dian L, Madden K, Cook W, et al. Effect of a home-based exercise program on subsequent falls among community-dwelling high-risk older adults after a fall. JAMA. 2019;321:2092.
Lord SR, Castell S, Corcoran J, Dayhew J, Matters B, Shan A, et al. The effect of group exercise on physical functioning and falls in frail older people living in retirement villages: a randomized, controlled trial. J Am Geriatr Soc. 2003;51:1685–92.
Luukinen H, Lehtola S, Jokelainen J, Väänänen-Sainio R, Lotvonen S, Koistinen P. Pragmatic exercise-oriented prevention of falls among the elderly: a population-based, randomized, controlled trial. Prev Med (Baltim). 2007;44:265–71.
MacRae PG, Feltner ME, Reinsch S. A 1-year exercise program for older women: effects on falls, injuries, and physical performance. J Aging Phys Act. 1994;2:127–42.
Madureira MM, Takayama L, Gallinaro AL, Caparbo VF, Costa RA, Pereira RMR. Balance training program is highly effective in improving functional status and reducing the risk of falls in elderly women with osteoporosis: a randomized controlled trial. Osteoporos Int. 2007;18:419–25.
Merom D, Mathieu E, Cerin E, Morton RL, Simpson JM, Rissel C, et al. Social dancing and incidence of falls in older adults: a cluster randomised controlled trial. PLoS Med. 2016;13:e1002112.
Messier SP, Mihalko SL, Legault C, Miller GD, Nicklas BJ, DeVita P, et al. Effects of intensive diet and exercise on knee joint loads, inflammation, and clinical outcomes among overweight and obese adults with knee osteoarthritis: the IDEA randomized clinical trial. JAMA. 2013;310:1263–73.
Mian OS, Thom JM, Ardigò LP, Morse CI, Narici MV, Minetti AE. Effect of a 12-month physical conditioning programme on the metabolic cost of walking in healthy older adults. Eur J Appl Physiol. 2007;100:499–505.
Möller UO, Kristensson J, Midlöv P, Ekdahl C, Jakobsson U. Effects of a one-year home-based case management intervention on falls in older people: a randomized controlled trial. J Aging Phys Act. 2014;22:457–64.
Munro JF. Cost effectiveness of a community based exercise programme in over 65 year olds: cluster randomised trial. J Epidemiol Community Heal. 2004;58:1004–10.
Muscari A, Giannoni C, Pierpaoli L, Berzigotti A, Maietta P, Foschi E, et al. Chronic endurance exercise training prevents aging-related cognitive decline in healthy older adults: a randomized controlled trial. Int J Geriatr Psychiatry. 2010;25:1055–64.
Mustata S, Groeneveld S, Davidson W, Ford G, Kiland K, Manns B. Effects of exercise training on physical impairment, arterial stiffness and health-related quality of life in patients with chronic kidney disease: a pilot study. Int Urol Nephrol. 2011;43:1133–41.
Nowalk MP, Prendergast JM, Bayles CM, D’Amico FJ, Colvin GC. A randomized trial of exercise programs among older individuals living in two long-term care facilities: the FallsFREE program. J Am Geriatr Soc. 2001;49:859–65.
Olazarán J, Muñiz R, Reisberg B, Peña-Casanova J, del Ser T, Cruz-Jentoft AJ, et al. Benefits of cognitive-motor intervention in MCI and mild to moderate Alzheimer disease. Neurology. 2004;63:2348–53.
Pahor M, Blair SN, Espeland M, Fielding R, Gill TM, Guralnik JM, et al. Effects of a physical activity intervention on measures of physical performance: results of the Lifestyle Interventions and Independence for Elders Pilot (LIFE-P) Study. J Gerontol Ser A Biol Sci Med Sci. 2006;61:1157–65.
Pakkala I, Read S, Leinonen R, Hirvensalo M, Lintunen T, Rantanen T. The effects of physical activity counseling on mood among 75- to 81-year-old people: a randomized controlled trial. Prev Med (Baltim). 2008;46:412–8.
Park H, Kim KJ, Komatsu T, Park SK, Mutoh Y. Effect of combined exercise training on bone, body balance, and gait ability: a randomized controlled study in community-dwelling elderly women. J Bone Miner Metab. 2008;26:254–9.
Patil R, Uusi-Rasi K, Tokola K, Karinkanta S, Kannus P, Sievänen H. Effects of a multimodal exercise program on physical function, falls, and injuries in older women: a 2-year community-based, randomized controlled trial. J Am Geriatr Soc. 2015;63:1306–13.
Pérula LA, Varas-Fabra F, Rodríguez V, Ruiz-Moral R, Fernández JA, González J, et al. Effectiveness of a multifactorial intervention program to reduce falls incidence among community-living older adults: a randomized controlled trial. Arch Phys Med Rehabil. 2012;93:1677–84.
Petrella RJ, Koval JJ, Cunningham DA, Paterson DH. Can primary care doctors prescribe exercise to improve fitness? The Step Test Exercise Prescription (STEP) project. Am J Prev Med. 2003;24:316–22.
Pitkälä KH, Pöysti MM, Laakkonen M-L, Tilvis RS, Savikko N, Kautiainen H, et al. Effects of the Finnish Alzheimer Disease Exercise Trial (FINALEX). JAMA Intern Med. 2013;173:894.
Pothirat C, Chaiwong W, Phetsuk N, Liwsrisakun C, Bumroongkit C, Deesomchok A, et al. Long-term efficacy of intensive cycle ergometer exercise training program for advanced COPD patients. Int J Chron Obstruct Pulmon Dis. 2015;10:133–44.
Prescott E, Hjardem-Hansen R, Dela F, Ørkild B, Teisner AS, Nielsen H. Effects of a 14-month low-cost maintenance training program in patients with chronic systolic heart failure: a randomized study. Eur J Cardiovasc Prev Rehabil. 2009;16:430–7.
Pruitt LA, Taaffe DR, Marcus R. Effects of a one-year high-intensity versus low-intensity resistance training program on bone mineral density in older women. J Bone Miner Res. 1995;10:1788–95.
Raso V, Benard G, Silva DA, Duarte AJ, Natale VM. Effect of resistance training on immunological parameters of healthy elderly women. Med Sci Sport Exerc. 2007;39:2152–9.
Reinsch S, MacRae P, Lachenbruch PA, Tobis JS. Attempts to prevent falls and injury: a prospective community study. Gerontologist. 1992;32:450–6.
Rejeski WJ, Ambrosius WT, Burdette JH, Walkup MP, Marsh AP. Community weight loss to combat obesity and disability in at-risk older adults. J Gerontol A Biol Sci Med Sci. 2017;72:1547–53.
Rhodes EC, Martin AD, Taunton JE, Donnelly M, Warren J, Elliot J. Effects of one year of resistance training on the relation between muscular strength and bone density in elderly women. Br J Sports Med. 2000;34:18–22.
Robertson MC, Devlin N, Gardner MM, Campbell AJ. Effectiveness and economic evaluation of a nurse delivered home exercise programme to prevent falls 1: Randomised controlled trial. BMJ. 2001;322:697–701.
Rolland Y, Pillard F, Klapouszczak A, Reynish E, Thomas D, Andrieu S, et al. Exercise program for nursing home residents with Alzheimer’s disease: a 1-year randomized, controlled trial. J Am Geriatr Soc. 2007;55:158–65.
Sherrington C, Lord SR, Vogler CM, Close JCT, Howard K, Dean CM, et al. A post-hospital home exercise program improved mobility but increased falls in older people: a randomised controlled trial. Quinn TJ, editor. PLoS One. 2014;9:e104412.
Shumway-Cook A, Silver IF, LeMier M, York S, Cummings P, Koepsell TD. Effectiveness of a community-based multifactorial intervention on falls and fall risk factors in community-living older adults: a randomized, controlled trial. J Gerontol Ser A. 2007;62:1420–7.
Sjösten NM, Vahlberg TJ, Kivelä S-L. The effects of multifactorial fall prevention on depressive symptoms among the aged at increased risk of falling. Int J Geriatr Psychiatry. 2008;23:504–10.
Sundstrup E, Jakobsen MD, Andersen LL, Andersen TR, Randers MB, Helge JW, et al. Positive effects of 1-year football and strength training on mechanical muscle function and functional capacity in elderly men. Eur J Appl Physiol. 2016;116:1127–38.
Suzuki T, Shimada H, Makizako H, Doi T, Yoshida D, Ito K, et al. A randomized controlled trial of multicomponent exercise in older adults with mild cognitive impairment. PLoS One. 2013;8:e61483.
Thomas GN, Hong AWL, Tomlinson B, Lau E, Lam CWK, Sanderson JE, et al. Effects of Tai Chi and resistance training on cardiovascular risk factors in elderly Chinese subjects: a 12-month longitudinal, randomized, controlled intervention study. Clin Endocrinol (Oxf). 2005;63:663–9.
Tsai C-L, Wang C-H, Pan C-Y, Chen F-C. The effects of long-term resistance exercise on the relationship between neurocognitive performance and GH, IGF-1, and homocysteine levels in the elderly. Front Behav Neurosci. 2015;9:23.
Underwood M, Lamb SE, Eldridge S, Sheehan B, Slowther A-M, Spencer A, et al. Exercise for depression in elderly residents of care homes: a cluster-randomised controlled trial. Lancet. 2013;382:41–9.
Uusi-Rasi K, Patil R, Karinkanta S, Kannus P, Tokola K, Lamberg-Allardt C, et al. Exercise and vitamin D in fall prevention among older women. JAMA Intern Med. 2015;175:703.
van Uffelen JGZ, Chinapaw MJM, van Mechelen W, Hopman-Rock M. Walking or vitamin B for cognition in older adults with mild cognitive impairment? A randomised controlled trial. Br J Sports Med. 2008;42:344–51.
Vetter NJ, Lewis PA, Ford D. Can health visitors prevent fractures in elderly people? BMJ. 1992;304:888–90.
Villareal DT, Chode S, Parimi N, Sinacore DR, Hilton T, Armamento-Villareal R, et al. Weight loss, exercise, or both and physical function in obese older adults. N Engl J Med. 2011;364:1218–29.
Voelcker-Rehage C, Godde B, Staudinger UM. Cardiovascular and coordination training differentially improve cognitive performance and neural processing in older adults. Front Hum Neurosci. 2011;5:26.
von Stengel S, Kemmler W, Engelke K, Kalender WA. Effects of whole body vibration on bone mineral density and falls: results of the randomized controlled ELVIS study with postmenopausal women. Osteoporos Int. 2011;22:317–25.
Williams P, Lord SR. Effects of group exercise on cognitive functioning and mood in older women. Aust N Z J Public Health. 1997;21:45–52.
Winters-Stone KM, Dobek JC, Bennett JA, Dieckmann NF, Maddalozzo GF, Ryan CW, et al. Resistance training reduces disability in prostate cancer survivors on androgen deprivation therapy: evidence from a randomized controlled trial. Arch Phys Med Rehabil. 2015;96:7–14.
Wolf SL, Sattin RW, Kutner M, O’Grady M, Greenspan AI, Gregor RJ. Intense tai chi exercise training and fall occurrences in older, transitionally frail adults: a randomized, controlled trial. J Am Geriatr Soc. 2003;51:1693–701.
Woo J, Hong A, Lau E, Lynn H. A randomised controlled trial of Tai Chi and resistance exercise on bone health, muscle strength and balance in community-living elderly people. Age Ageing. 2007;36:262–8.
Englund U, Littbrand H, Sondell A, Pettersson U, Bucht G. A 1-year combined weight-bearing training program is beneficial for bone mineral density and neuromuscular function in older women. Osteoporos Int. 2005;16:1117–23.
Fox KR, Stathi A, McKenna J, Davis MG. Physical activity and mental well-being in older people participating in the Better Ageing Project. Eur J Appl Physiol. 2007;100:591–602.
Kemmler W, von Stengel S, Engelke K, Häberle L, Kalender WA. Exercise effects on bone mineral density, falls, coronary risk factors, and health care costs in older women. Arch Intern Med. 2010;170:179.
Kennis E, Verschueren SM, Bogaerts A, Van Roie E, Boonen S, Delecluse C. Long-term impact of strength training on muscle strength characteristics in older adults. Arch Phys Med Rehabil. 2013;94:2054–60.
Kerr J, Rosenberg D, Millstein RA, Bolling K, Crist K, Takemoto M, et al. Cluster randomized controlled trial of a multilevel physical activity intervention for older adults. Int J Behav Nutr Phys Act. 2018;15:32.
Kerse N, Peri K, Robinson E, Wilkinson T, von Randow M, Kiata L, et al. Does a functional activity programme improve function, quality of life, and falls for residents in long term care? Cluster randomised controlled trial. BMJ. 2008;337:a1445.
Lord SR, Ward JA, Williams P, Strudwick M. The effect of a 12-month exercise trial on balance, strength, and falls in older women: a randomized controlled trial. J Am Geriatr Soc. 1995;43:1198–206.
Lam LCW, Chau RCM, Wong BML, Fung AWT, Lui VWC, Tam CCW, et al. Interim follow-up of a randomized controlled trial comparing Chinese style mind body (Tai Chi) and stretching exercises on cognitive function in subjects at risk of progressive cognitive decline. Int J Geriatr Psychiatry. 2011;26:733–40.
Lam LCW, Chan WC, Leung T, Fung AWT, Leung EMF. Would older adults with mild cognitive impairment adhere to and benefit from a structured lifestyle activity intervention to enhance cognition: a cluster randomized controlled trial. PLoS One. 2015;10:e0118173.
Sjösten NM, Salonoja M, Piirtola M, Vahlberg T, Isoaho R, Hyttinen H, et al. A multifactorial fall prevention programme in home-dwelling elderly people: a randomized-controlled trial. Public Health. 2007;121:308–18.
Korpelainen R, Keinänen-Kiukaanniemi S, Heikkinen J, Väänänen K, Korpelainen J. Effect of impact exercise on bone mineral density in elderly women with low BMD: a population-based randomized controlled 30-month intervention. Osteoporos Int. 2006;17:109–18.
Kruse RL, LeMaster JW, Madsen RW. Fall and balance outcomes after an intervention to promote leg strength, balance, and walking in people with diabetic peripheral neuropathy: “Feet First” randomized controlled trial. Phys Ther. 2010;90:1568–79.
Dean CM, Rissel C, Sherrington C, Sharkey M, Cumming RG, Lord SR, et al. Exercise to enhance mobility and prevent falls after stroke: the community stroke club randomized trial. Neurorehabil Neural Repair. 2012;26:1046–57.
Morey MC, Peterson MJ, Pieper CF, Sloane R, Crowley GM, Cowper PA, et al. The veterans learning to improve fitness and function in elders study: a randomized trial of primary care-based physical activity counseling for older men. J Am Geriatr Soc. 2009;57:1166–74.
Kim H, Yoshida H, Suzuki T. Falls and fractures in participants and excluded non-participants of a fall prevention exercise program for elderly women with a history of falls: 1-year follow-up study. Geriatr Gerontol Int. 2014;14:285–92.
Mikó I, Szerb I, Szerb A, Poor G. Effectiveness of balance training programme in reducing the frequency of falling in established osteoporotic women: a randomized controlled trial. Clin Rehabil. 2017;31:217–24.
Boongird C, Keesukphan P, Phiphadthakusolkul S, Rattanasiri S, Thakkinstian A. Effects of a simple home-based exercise program on fall prevention in older adults: a 12-month primary care setting, randomized controlled trial. Geriatr Gerontol Int. 2017;17:2157–63.
Day L, Hill KD, Stathakis VZ, Flicker L, Segal L, Cicuttini F, et al. Impact of tai-chi on falls among preclinically disabled older people. A randomized controlled trial. J Am Med Dir Assoc. 2015;16:420–6.
Voukelatos A, Merom D, Sherrington C, Rissel C, Cumming RG, Lord SR. The impact of a home-based walking programme on falls in older people: the Easy Steps randomised controlled trial. Age Ageing. 2015;44:377–83.
Öhman H, Savikko N, Strandberg TE, Kautiainen H, Raivio MM, Laakkonen M-L, et al. Effects of exercise on cognition: the Finnish Alzheimer Disease Exercise Trial: a randomized, controlled trial. J Am Geriatr Soc. 2016;64:731–8.
Wang X, Hsu F-C, Isom S, Walkup MP, Kritchevsky SB, Goodpaster BH, et al. Effects of a 12-month physical activity intervention on prevalence of metabolic syndrome in elderly men and women. J Gerontol A Biol Sci Med Sci. 2012;67:417–24.
Lam LCW, Chau RCM, Wong BML, Fung AWT, Tam CWC, Leung GTY, et al. A 1-year randomized controlled trial comparing mind body exercise (Tai Chi) with stretching and toning exercise on cognitive function in older chinese adults at risk of cognitive decline. J Am Med Dir Assoc. 2012;13:568.e15–20.
Fairhall N, Sherrington C, Lord SR, Kurrle SE, Langron C, Lockwood K, et al. Effect of a multifactorial, interdisciplinary intervention on risk factors for falls and fall rate in frail older people: a randomised controlled trial. Age Ageing. 2014;43:616–22.
Bouchonville M, Armamento-Villareal R, Shah K, Napoli N, Sinacore DR, Qualls C, et al. Weight loss, exercise or both and cardiometabolic risk factors in obese older adults: results of a randomized controlled trial. Int J Obes. 2014;38:423–31.
Williamson JD, Espeland M, Kritchevsky SB, Newman AB, King AC, Pahor M, et al. Changes in cognitive function in a randomized trial of physical activity: results of the lifestyle interventions and independence for elders pilot study. J Gerontol A Biol Sci Med Sci. 2009;64:688–94.
Morse CI, Thom JM, Mian OS, Muirhead A, Birch KM, Narici MV. Muscle strength, volume and activation following 12-month resistance training in 70-year-old males. Eur J Appl Physiol. 2005;95:197–204.
Morey MC, Snyder DC, Sloane R, Cohen HJ, Peterson B, Hartman TJ, et al. Effects of home-based diet and exercise on functional outcomes among older, overweight long-term cancer survivors. JAMA. 2009;301:1883.
Mok A, Khaw K-T, Luben R, Wareham N, Brage S. Physical activity trajectories and mortality: population based cohort study. BMJ. 2019;365:l2323.
Pavasini R, Guralnik J, Brown JC, di Bari M, Cesari M, Landi F, et al. Short physical performance battery and all-cause mortality: systematic review and meta-analysis. BMC Med. 2016;14:215.
Fiuza-Luces C, Santos-Lozano A, Joyner M, Carrera-Bastos P, Picazo O, Zugaza JL, et al. Exercise benefits in cardiovascular disease: beyond attenuation of traditional risk factors. Nat Rev Cardiol. 2018;15:731–43.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This work was supported by the Biomedical Research Networking Center on Frailty and Healthy Aging (CIBERFES) and FEDER funds from the European Union. It was further funded by a grant from the Spanish Ministry of Economy, “Ministerio de Economía y Competitividad,” Instituto de Salud Carlos III, FEDER, (PI17/01814). AGH is a Miguel Servet Fellow (Instituto de Salud Carlos III-CP18/0150). NM-V received funding from “la Caixa” Foundation (ID 100010434), under agreement LCF/PR/PR15/51100006.
Conflicts of Interest
Antonio García-Hermoso, Robinson Ramirez-Vélez, Mikel López Sáez de Asteasu, Nicolás Martínez-Velilla, Fabricio Zambom-Ferraresi, Pedro Valenzuela, Alejandro Lucia and Mikel Izquierdo declare that they have no conflicts of interest relevant to the content of this review.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
García-Hermoso, A., Ramirez-Vélez, R., Sáez de Asteasu, M.L. et al. Safety and Effectiveness of Long-Term Exercise Interventions in Older Adults: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Sports Med 50, 1095–1106 (2020). https://doi.org/10.1007/s40279-020-01259-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-020-01259-y