
Abstract
Maximum oxygen consumption (\(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\)) is not only an indicator of endurance performance, but also a strong predictor of cardiovascular disease and mortality. This physiological parameter is known to decrease with aging. In turn, physical exercise might attenuate the rate of aging-related decline in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\), which in light of the global population aging is of major clinical relevance, especially at advanced ages. In this narrative review, we summarize the evidence available from masters athletes about the role of lifelong endurance exercise on aging-related \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) decline, with examples of the highest \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) values reported in the scientific literature for athletes across different ages (e.g., 35 ml·kg−1·min−1 in a centenarian cyclist). These data suggest that a linear decrease in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) might be possible if physical exercise loads are kept consistently high through the entire life span, with \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) values remaining higher than those of the general population across all ages. We also summarize the main physiological changes that occur with inactive aging at different system levels—pulmonary and cardiovascular function, blood O2 carrying capacity, skeletal muscle capillary density and oxidative capacity—and negatively influence \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\), and review how lifelong exercise can attenuate or even prevent most—but apparently not all (e.g., maximum heart rate decline)—of them. In summary, although aging seems to be invariably associated with a progressive decline in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\), maintaining high levels of physical exercise along the life span slows the multi-systemic deterioration that is commonly observed in inactive individuals, thereby attenuating age-related \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) decline.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Masters athletes are considered a paradigm of healthy aging because they are able to maintain high levels of exercise at advanced ages and show remarkable physical/physiological function compared to their inactive peers. |
Maximum oxygen consumption (\(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\)) decreases with aging, but lifelong physical exercise exerts a myriad of benefits (i.e., enhanced or at least preserved levels of pulmonary/cardiovascular function, blood O2 carrying capacity, skeletal muscle capillary density and oxidative capacity) which in turn seem to attenuate the rate of aging-related \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) decline. |
Given the role of \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) as a strong predictor of cardiovascular disease and mortality, these findings support the need to perform high levels of physical exercise across all ages. |
1 Introduction
Maximum oxygen consumption (\(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\)), that is, the maximum integrative ability of the organism to transfer oxygen (O2) from the atmosphere to be utilized by the mitochondria of working muscles [1], is widely considered the gold standard measurement of cardiorespiratory fitness [2]. \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) is well known to decrease with aging [3], and the rate of decline further accelerates at advanced ages [4]. Besides being a main limiting factor of endurance performance [1], \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) is a strong cardiovascular and all-cause mortality predictor [5,6,7]. Moreover, the exponential decline of physical fitness—including \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\)—that occurs with aging is a major contributor to loss of functionality and frailty [8], with the latter condition affecting one to two of every four individuals aged ≥ 85 years and thus being considered a major health problem [9]. Thus, attenuation of aging-related \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) decline is of clinical relevance.
The age-related decrease in physical/physiological function is currently exacerbated by the growing epidemic of inactivity, with at least one of every four individuals performing less than the minimum WHO-recommended amount of physical activity (PA) (≥ 150 min per week of moderate–vigorous PA, such as walking/brisk walking) [10]. Maintaining high levels of PA through the life span seems to be a necessary condition to attenuate the age- and inactivity-related decline in physiological function [11, 12]. Regular endurance exercise (e.g., running) is probably the most effective strategy for enhancing or preserving \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) levels over time, and there is evidence that this strategy can be beneficial even at the most advanced ages [13]. In this regard, masters endurance athletes (i.e., individuals > 40 years old who still actively participate in sports competitions) have been proposed as a paradigm of healthy aging because most are able to maintain high levels of endurance exercise and show a remarkable physical and physiological function compared to their sedentary peers [14,15,16].
In this narrative review, we summarize the evidence available on the impact of lifelong endurance exercise as a countermeasure against age-related \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) decline, supporting these benefits with cross-sectional data of the highest \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) values reported in athletes across different ages compared to the age-matched general population. We also review the main physiological mechanisms underlying lifelong endurance exercise benefits on age-related \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) decline.
2 Lifelong Endurance Exercise as a Countermeasure Against \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) Decline: Epidemiological Evidence in Masters Athletes
There are data supporting that endurance exercise levels might modulate the relationship between aging and \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) [17]. A classic study by Dehn and Bruce [18] reported that trained individuals present with an attenuated age-related decline in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) compared to their untrained peers. There is, however, controversy on this topic, with meta-analytical evidence showing either no differences in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) decline between endurance-trained and inactive men [19], or even a greater decline in the former [20]. Other studies reported that, although endurance-trained older adults had a higher absolute (l·min−1) and relative \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) (ml·kg−1·min−1) than their inactive peers at any age, the rate of \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) decline with aging (expressed in ml·kg−1·min−1·year−1, but not as a %) was also greater in the former [21, 22]. However, inactive individuals presented with a progressive reduction in VO2max across all ages, whereas endurance-trained athletes did not show this decline until a more advanced age (~ 50 years) [22].
The relative reduction in PA levels with aging is greater in trained than in untrained individuals, and this has been proposed as one of the main factors underlying the differences in the rate of \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) decline [14]. Several studies have proposed that the decrease in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) with aging is modulated by age-related decreases in training levels [21,22,23,24]. For instance, in a longitudinal study of individuals aged ~ 64 years, Katzel et al. [24] observed that those participants who stopped training during the following ~ 9 years lost on average 4.6% of \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) per year, whereas those who maintained high levels of exercise during this period only lost 0.3% per year. These findings are in line with classical longitudinal studies reporting a greater \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) decline in inactive older adults compared to masters endurance athletes who had maintained their training levels during a follow-up period [25, 26]. Thus, although performing physical exercise during youth and adulthood might help to reach older ages with a remarkable \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) level compared to sedentary individuals, keeping exercise levels high later in life—including at the most advanced ages—seems to be a necessary condition to attenuate the usual age-related \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) decline.
Confirming the benefits of exercise on \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) at advanced ages, a recent study reported that individuals aged ~ 72 to 74 years who had exercised regularly (~ 5 days/week) over the past ~ 52 years had a 44% higher \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) than their inactive peers [27]. Trappe et al. [28] showed that even at the most advanced ages (> 80 years) lifelong exercisers (> 50 years of endurance exercise) presented with a markedly higher \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) than their inactive counterparts (~ 38 vs ~21 ml·kg−1·min−1, respectively). The research group of Levine and co-workers has also consistently demonstrated that older adults (> 65 years) who maintain high levels of endurance exercise during 20–25 years or more attenuate or even prevent the age-related \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) decline compared to those who remain inactive during an equivalent time period [29,30,31,32,33]. Meta-analytical evidence has confirmed that masters athletes (mean age > 55 years) have higher \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) values than their inactive counterparts and similar values to those of untrained healthy young controls [34, 35]. In this regard, there seems to be a dose–response relationship between the levels of lifelong physical exercise (i.e., in terms of intensity, volume, or frequency [number of weekly sessions] of training) and the benefits on \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\). Carrick-Ranson et al. [32] and Hieda et al. [33] found that those individuals (mean age 68–71 years) who performed physical exercise more frequently during the past 25 years (≥ 4 to 5 sessions per week) had the highest \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) values, whereas no differences in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) were found between inactive individuals and those who performed 2 to 3 sessions of exercise per week. Thus, increasing training levels by manipulating either training frequency or particularly training volume (distance or time completed in each session) and/or intensity (e.g., watts, speed) might be factors modulating the benefits of lifelong exercise on VO2max [36, 37].
3 VO2max Records in Masters Athletes
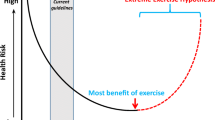
Masters athletes of different ages present with a higher \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) than age-matched inactive individuals, which supports the beneficial role of lifelong physical exercise to attenuate the age-related VO2max decline at advanced ages, particularly if physical training levels are kept consistently high. As shown in Fig. 1, which displays the highest \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) values found in the scientific literature for athletes of different ages, lifelong endurance exercise can result in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) values 20–40% higher than the 95th percentile of the age-reference values provided by the American College of Sports Medicine [38]. Levels of \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) > 90 ml·kg−1·min−1 have been reported for some young male elite athletes [39, 40], who probably present with the highest \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) values ever reported. In turn, \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) levels well above the average reference values for younger healthy individuals [38] have been reported for runners aged 47–62 years (63–76 ml·kg−1·min−1) [41,42,43] and markedly high \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) levels can still be present in older adults, as reflected by several studies reporting values between 50 and 59 ml·kg−1·min−1 for individuals aged 70–80 years [41, 42, 44, 45]. Of note, a remarkably high \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) value of 42.3 ml·kg−1·min−1 has been recently reported in an 83-year old female masters athlete, the highest value ever recorded for women older than 80 years [46]. Moreover, \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) values of 37 ml·kg−1·min−1 and 35 ml·kg−1·min−1, which correspond to the expected value for individuals aged 35–45 years [38], have been reported during cycle-ergometer testing in endurance athletes aged 91 and 103 years, respectively [28, 47].

Highest maximum oxygen consumption (\(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\)) values reported in the scientific literature for athletes of different ages (black circles). The solid line represents the 50th percentile of \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) according to the normative values provided by the American College of Sports Medicine [38], and the dotted lines represent the 5th and 95th percentiles. As reference values were only available up to the age of 65–75 years, reference values from that age were estimated through linear extrapolation. \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) individual data were obtained from the following references [28, 39,40,41,42,43,44,45, 47, 136]
It is traditionally believed that an exponential decline in physical/physiological function occurs with aging, particularly after 70–80 years of age (known as ‘break point’) [15]. For instance, longitudinal data from the masters athlete Ed Whitlock (first person > 70 years old to run a sub 3-h marathon) suggests that despite having an estimated VO2max value of ~ 50 ml·kg−1·min−1 at 80 years, he showed an accelerated decline in running performance after age 80 (he died at age 86 from prostate cancer) [48]. However, the values presented in Fig. 1 suggest that a linear decline in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) with aging is theoretically possible even at the most advanced ages (e.g., 100 years). Indeed, when trying to fit these \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) values to an exponential and a linear function, the resulting fit is worse for the former (R2 = 0.96 vs 0.99, respectively). The possible existence of a linear decline in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) with aging has also been inferred by the authors of a cross-sectional study performed in highly active individuals (cyclists) aged up to 79 years [49]. Interestingly, if our data were fitted with an exponential equation the results would suggest a greater decline at younger ages than at advanced ones, which is in contrast to what is traditionally thought [15]. In this line, cross-sectional \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) values from more than 4000 individuals aged between 20 and 79 years showed a \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) decline of 10% per decade [50], which would result in an exponential decline in this parameter when expressed in absolute values (l·min−1). Further research is, however, needed to confirm if the aforementioned rate of decline is observed in later years of life (i.e., above age 80). The trend observed in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) records reported here also suggests a faster decline in masters athletes than in the general population (at least when compared with normative values). It remains to be elucidated whether an eventual faster aging-related \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) decline in masters athletes compared to inactive people is caused by greater relative reductions in exercise levels over time in the former—as some longitudinal studies have proposed [21, 23, 24] —or alternatively, to a greater relative physiological deterioration independent of training status.
It must be noted that our analysis has some limitations, as it is cross-sectional, based on a thorough but not systematic search, and does not take into account several potential confounding factors (e.g., socio-economic status, or presence of diseases that aggravate physiological decline). Although \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) levels might show a theoretical linear decline with aging, there is no evidence from longitudinal studies to support that the occurrence of an age-related ‘break point’ in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) can be actually prevented with regular exercise, particularly at the most advanced ages. Moreover, the paucity of longitudinal studies hinders drawing solid conclusions on how does lifelong exercise actually modulate the inherent age-related decline in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\). In this regard, it may be hypothesized that masters athletes already had high \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) values at baseline (i.e., before engaging in training), or that they have a higher responsiveness or lower sensitivity to training and inactivity, respectively, compared to the general population. In this context, a recent case study showed that a 59-year-old world record marathon holder for his age group (and former Olympic-class runner) had retained a very high \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) value, 65.4 ml·kg−1·min−1—which is in fact, the highest known for his age—despite a 16-year break in training after he retired from competition at 32 years old [43]. It has been however reported that keeping exercise levels high is overall necessary to reduce the rate of age-related \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) decline [21, 23, 24]. Also noteworthy is that, even in the case of a linear decline in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) with aging, a more abrupt decline might still be found in other variables (e.g., muscle mass or strength) at advanced ages, which would lead to an exponential decline in overall physical performance. Notwithstanding, the present results suggest that the ‘break point’ in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) might be, at least partly, delayed if physical exercise loads are kept high across all ages, thereby reducing the risk of having very poor \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) levels at the end of the life span.
Besides the controversial issue of the actual influence of genetics on VO2max trainability [51,52,53], there are several ‘modifiable’ physiological mechanisms by which lifelong physical exercise might attenuate the normal age-related \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) decline. As reviewed by Wagner [54], the O2 pathway from the atmosphere to the mitochondria includes several steps (known as the ‘oxygen transport cascade’): convective O2 transport from air to lung, diffusive O2 transport from lung to blood, convective O2 transport in blood from lungs to muscle, and O2 diffusion from the microcirculation to the tissues and particularly to the mitochondria. In the following section, we will briefly discuss the main physiological systems/factors involved in the different steps of the O2 transport cascade and thus ultimately influencing \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\), how they are affected by the aging process, and the beneficial effects of lifelong exercise (Fig. 2).

Effects of aging on the factors affecting maximal oxygen consumption in lifelong exercisers and in untrained individuals. Images in circles represent increased fibrosis at the cardiac level and reduced hemoglobin levels, muscle capillary density and oxidative capacity in untrained individuals, all of which are at least partly attenuated by lifelong endurance exercise. a-v O2diff arteriovenous oxygen difference, HRmax maximum heart rate, FEV1 forced expiratory volume in 1 s. Arrows indicate increments (↑) or reductions (↓) with lifelong exercise or sedentary behaviors. ? indicates that no consistent benefits of lifelong exercise have been reported
4 Physiological Factors Mediating Lifelong Exercise Benefits on \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\)
4.1 Pulmonary Function
4.1.1 Aging Effects
The convective transport of O2 from the atmosphere to the lung is mostly mediated by pulmonary function. The latter becomes progressively compromised with aging [55, 56]. An increase in chest wall stiffness together with an impaired strength of ventilatory muscles result in decreased dynamic lung volumes (e.g., as assessed through the forced expiratory volume in one second [FEV1]) [57]. Aging also results in a progressive decline in the arterial partial pressure of O2 due to age-induced ventilation-perfusion mismatch [58], with the alveolar surface area decreasing due to alterations in the lung internal geometry [59]. The aforementioned age-induced changes impair maximal ventilatory capacity and pulmonary gas exchange, and thus can also affect \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) [60]. Although pulmonary function is not widely considered a major limiting factor of \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) in healthy young individuals, a compromised pulmonary function seems to be associated, at least partly, with an impaired \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\). Some authors have reported a relationship between \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) and pulmonary function—as measured by FEV1—but just until a given threshold value above which pulmonary function does not seem to limit \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) anymore [61]. It is important to note, however, that the identified threshold values were within the normal limits of lung function for elders, which suggests that pulmonary function might be a limiting factor of \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) in healthy older adults. A recent study reported that FEV1 values might affect \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) even in healthy young and middle-aged individuals, with both variables being positively associated in subjects with FEV1 values above the lower limit of normality [62]. Of note, the reason why an aging-related reduction in FEV1 might partly contribute to also reduce \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) values could be that it can reflect mechanical constraints—i.e., the lungs lose elastic recoil, the thorax wall gets stiffer and more restricted—to maximal ventilation capacity during exertion [62]. In turn, because maximal pulmonary ventilation, together with the difference between inspired and expired fractional O2, is the main factor in the computation of \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) by metabolic carts, even small changes in this variable can affect the final \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) value.
Some studies have used oxygen–helium mixture (HeO2 or ‘heliox’) to reduce the resistive load against ventilation during exercise, which could potentially enhance pulmonary function—and thus theoretically improve \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\). In sedentary older adults, breathing heliox increased the ventilatory response to maximal exercise and tidal volume compared to breathing room air, and this was accompanied by a slight increase in performance (time to exhaustion) during incremental exercise [63]. The same ventilatory responses have been observed in trained older adults and young individuals, but without performance benefits [64, 65]. It must be noted, however, that none of the aforementioned studies assessed changes in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) and thus it remains unknown whether reductions in pulmonary resistive loads can eventually improve \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\). However, evidence to date overall suggests that pulmonary function might be a limiting factor of \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\), at least in those individuals in which the former is compromised.
4.1.2 Training Effects
Although there is scarce evidence on the effectiveness of exercise training interventions to prevent the age-related decline in pulmonary function [66], some studies have shown that high levels of endurance exercise can partly attenuate this decline. A recent study in two monozygotic twins aged 52 years found that, although one of them had performed endurance training for more than 30 years and had a \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) ~ 30% higher compared to his inactive brother, no differences were found in pulmonary function [67]. However, it can be argued that these individuals were not old enough to show age-related deteriorations in pulmonary function. Johnson et al. [68] observed that fit older adults aged 63–77 years (\(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) of ~ 44 ml·kg−1·min−1 and a training frequency ≥ 2 times per week) presented with values of vital capacity, total lung capacity, and maximal voluntary ventilation that were 110% of those predicted for their age and height. Yet, a longitudinal study performed in highly active individuals aged 67–73 years found that lifelong exercise training did not prevent the decline in resting lung volumes and FEV1 that accompany the normal aging process [69]. However, the latter data were not compared with those of a control group of age-matched inactive subjects.
In turn, a cross-sectional association between PA levels and pulmonary function—as measured by FEV1—has been found in individuals aged 45–74 years [70]. Moreover, higher levels of vigorous PA were associated with a lower annual relative decline in FEV1 during a subsequent follow-up [70]. Pelkonen et al. [71] observed in individuals aged 40–59 years that those who performed the highest levels of PA during a 25-year follow-up lost less pulmonary function than those who remained less active. More recent research has shown that, although age was inversely associated with pulmonary function in both masters athletes (35–86 years) and age-matched inactive controls, the former had a 9% higher FEV1 [72]. However, these results were not explained by differences in maximal ventilatory pressure (i.e., ventilatory muscle strength), which suggests that other ‘non-muscular’ factors might account for the better pulmonary function observed in masters athletes. Thus, maintaining high levels of physical exercise in the long-term appears to overall attenuate—albeit not prevent—the expected age-related decline in pulmonary function, which in turn would have a beneficial effect on \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\). In this regard, however, it must be noted that exercise-induced arterial hypoxemia (EIAH), which is overall rare in older adults [73], is quite prevalent among not only elite masters athletes [74] but also older adults with very high cardiorespiratory fitness [69]. Together with other factors (such as aging-induced reduction in capillary blood volume or perfusion heterogeneity), relative alveolar hypoventilation is a potential contributing factor for very fit old individuals [73, 74].
4.1.3 Key Areas Where More Information is Needed
The relationship between pulmonary function and \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) in healthy individuals remains unclear, and future studies should confirm if the reductions observed with aging in the former can negatively influence \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\), especially in those in whom pulmonary function deterioration does not reach pathological limits. Assessing the effects of specific ventilatory muscle training—which has been proven to increase inspiratory muscle function in older adults [75] —on EIAH and \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) could shed some light on this topic. Evidence is also still warranted to elucidate the effects of lifelong physical exercise on pulmonary function, particularly at the most advanced ages. In this regard, even centenarian athletes might improve their pulmonary function (maximal ventilation, respiratory frequency and tidal volume) and \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) with proper training [47]. Thus, although previous studies have suggested that some degree of deterioration in pulmonary function is inevitable with aging, future research should assess if factors such as training frequency or intensity can influence the benefits of physical exercise on pulmonary function, with higher training loads potentially preventing pulmonary functional decline.
4.2 Cardiovascular System
4.2.1 Aging Effects
Together with pulmonary function, the cardiovascular system and particularly maximal cardiac output (\(\dot{Q}_{ \hbox{max} }\)) has been traditionally proposed as one of the major limiting factors of \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) [76]. The two factors that determine \(\dot{Q}_{ \hbox{max} }\) are maximum stroke volume (SVmax) and heart rate (HRmax), and although some controversy exists, SVmax is usually viewed as the main limiting factor of \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\), at least in healthy young individuals [77].
Several age-related changes at the cardiovascular level can explain, at least partly, the aging decline in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) [55, 78]. With regard to cardiac structural changes, aging is associated with increases in left ventricular (LV) wall thickness, which results from an accumulation of interstitial connective tissue and amyloid deposits as well as from myocyte hypertrophy (albeit there is also a progressive loss in their number, particularly in the sinoatrial node) [78]. These changes result in lower LV compliance and end-diastolic filling compared to younger individuals, which in turn reduce SVmax [29, 79]. On the other hand, aging is associated with a reduction in HRmax, which seems to be the consequence of an impaired β-adrenergic responsiveness and neurodegeneration [80]. Although as mentioned above SVmax is usually identified as the main limiting factor of \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) at the heart level, a reduction in HRmax could also potentially reduce \(\dot{Q}_{ \hbox{max} }\) and consequently \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) [3]. Aging is also associated with increases in fibrosis and calcification of the cardiac valves, stiffness of peripheral and central arteries, and the number of sites for lipid deposition at the vascular level, which leads to a reduced laminar blood flow and thus to a lower O2 supply to other tissues (e.g., contracting muscles) [78, 81]. Moreover, in young individuals the increased sympathetic vasoconstrictor activity that occurs with exercise is counteracted (a phenomenon known as functional ‘sympatholysis’) to redistribute blood flow to contracting muscles [82]. By contrast, older adults have a reduced vasodilatory capacity and an impaired functional sympatholysis during exercise, which might compromise O2 supply and reduce \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) [83]. It has been recently reported that the impaired vasodilatory capacity and functional sympatholysis observed in the older people might be due, at least partly, to a reduction in the deformability of red blood cells, which is associated with an impaired release of ATP—a vasoactive molecule that stimulates vasodilatation—in response to hemoglobin deoxygenation [84].
4.2.2 Training Effects
There is strong evidence that lifelong exercise can attenuate the age-related deterioration of many of the cardiovascular properties that influence \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\). Meta-analytical evidence shows that masters athletes (mean age > 55 years) present with \(\dot{Q}_{ \hbox{max} }\) values that are higher than those of non-athletes of similar age and similar to those of young healthy controls [35]. Some authors have reported that masters athletes aged 68–70 years present with a preserved LV compliance, diastolic function (i.e., myocardial filling and relaxation) and SV compared to age-matched inactive peers, with these variables being similar to those of young healthy controls [29, 30]. Howden et al. [85] recently reported that, although there were no age- or training-related differences in LV ejection fraction, older adults (~ 68 years) who had performed lifelong endurance exercise showed a preserved LV systolic longitudinal strain (a marker of systolic function) compared to their inactive peers. Interestingly, these differences disappeared when variations in LV end-diastolic volume were taken into account, which suggests that lifelong exercise prevents the normal age-related reduction in LV systolic function by improving LV diastolic filling [85].
Although lifelong endurance exercise is overall beneficial to attenuate the decline in LV compliance and diastolic function, research has demonstrated that there is a dose–response relationship—and a threshold—for these benefits. Bhella et al. [31] observed that those older adults (> 64 years) who had exercised more frequently during the past 25 years (i.e., ≥ 4 to 5 sessions/week) showed a higher LV compliance and distensibility than their inactive peers. Interestingly, no differences in LV compliance and distensibility were found between individuals who had exercised less frequently (≤ 3 sessions per week) and the inactive group, but \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) values rose linearly with increasing exercise frequency [31]. The same research group showed that those who had performed 4–5 sessions/week during the past 25 years—but not those who had exercised ≤ 3 times per week—presented with a more favorable ventricular-arterial coupling (i.e., dynamic Starling mechanism) and a higher LV end-diastolic volume, SVmax and \(\dot{Q}_{ \hbox{max} }\) than those who had remained inactive [32, 33]. Following the same trend, only those subjects who had exercised ≥ 4 times per week showed a higher \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) than their sedentary counterparts [32].
In contrast to its aforementioned benefits on LV compliance, lifelong exercise does not appear to counteract the decline in HRmax that typically accompanies the aging process. For instance, Heath et al. [42] suggested that age-related reductions in HRmax were the factor mediating the differences in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) between trained endurance masters athletes and young athletes; indeed, both groups presented with similar values of LV volume and mass (both being larger than in untrained individuals) but an age-related reduction in HRmax was observed in the former. Similarly, Hagberg et al. [86] found that although trained masters athletes presented with a preserved SVmax compared to young competitive athletes, the \(\dot{Q}_{ \hbox{max} }\) and thus the \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) of the former were lower due to a reduced HRmax (with a reduction rate similar to that of their inactive counterparts). Research in masters athletes has shown that HRmax decreases with aging regardless of training volume, although this reduction does not seem to be related to the change in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) [87]. Carrick-Ranson et al. [32] also observed no differences in HRmax between masters athletes who had performed lifelong exercise (> 25 years with 4–5 sessions/week) and inactive individuals. Nybo et al. [88] observed a yearly reduction in HRmax of ~ 1 beat·min−1 in an Olympic athlete who was followed for 20 years since he was a 19-year-old. However, this reduction in HRmax was compensated for by a proportional increase in O2 pulse (i.e., the ratio of \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) (mL·min−1) to HRmax (beats·min−1) which expresses the volume of O2 ejected from the ventricles with each cardiac beat) at maximal intensities, resulting in a steady \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) and performance level [88]. Thus, exercise does not seem to exert an influence on the HRmax decrease that commonly occurs with aging.
On the other hand, lifelong physical exercise can prevent the age-related decline in endothelial function. Some authors have found that trained older adults had an impaired endothelial function compared to their younger counterparts. Proctor et al. [89] observed a lower leg blood flow and vascular conductance during exercise in trained older adults (55–68 years) with ~ 18 years of experience in endurance exercise (~ 6 h per week) compared to young trained individuals. However, the authors did not assess an additional group of inactive older adults. In this regard, several studies have found that although aging is associated with an increased arterial stiffness, those individuals who perform lifelong exercise present with a lower arterial stiffness and a more preserved endothelium flow-mediated dilation compared to their inactive peers, both being markers related to \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) [81, 90]. The aforementioned benefits are supported by meta-analytical evidence that masters athletes present with an increased flow-mediated dilation compared to age-matched controls [91]. Shibata et al. [92] recently reported in individuals aged > 60 years that those who had trained ≥ 4 to 5 sessions/week at high intensities during the last > 25 years—but not those who had trained less—had a lower central arterial stiffness than their inactive counterparts, although lower training doses (2–3 sessions/week) were enough to observe benefits in carotid artery stiffness and central blood pressure [92]. Moreover, Mortensen et al. [83] showed that lifelong endurance exercise (> 5 h of training per week during the last 30 years in individuals aged ~ 66 years) preserved functional sympatholysis and attenuated the age-related deterioration in endothelial function and vasodilatory capacity, which could result in an improved blood flow and O2 supply to working muscles. Groot et al. [93] observed that older adults (mean age of 71–72 years) who performed more than either 30 or 60 min/day of moderate-vigorous PA, respectively, had a preserved vasodilatory capacity compared with their sedentary age-matched controls. Moreover, the \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) of both active groups was higher compared not only to their sedentary age-matched peers but also to a group of sedentary young subjects [93]. In line with these benefits on vasodilatory capacity, it has been reported that the bioavailability of nitric oxide is reduced in inactive older adults whereas lifelong exercise prevents this aging-induced change [94]. In summary, lifelong exercise attenuates the degeneration that occurs in inactive people with aging at both cardiac and vascular level, with subsequent benefits in O2 supply and \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\). However, lifelong exercise does not seem to attenuate the normal age-reduction in HRmax.
4.2.3 Key Areas Where More Information is Needed
Evidence on the benefits of lifelong endurance training on SVmax and vascular health is quite clear, suggesting that it may attenuate or even prevent the deterioration in LV diastolic filling, LV systolic function, and endothelial function provided a sufficient training frequency/load is applied. There is, however, scarce evidence on whether these beneficial effects are also present at advanced ages (e.g., in those aged 80–85 years and above). There is also controversy on the influence of HRmax on \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\), with some studies in young subjects suggesting that the former is not a limiting factor [95] while others conducted in older individuals suggesting that the age-related reduction in HRmax is the main factor mediating the corresponding \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) decline [42, 86]. In this regard, by replicating the protocol of Munch et al. in older adults [95] it could be analyzed whether increasing HRmax above physiological values via atrial pacing could help to increase \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\), which would shed some light on the actual role of HRmax on \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) in this population.
4.3 Blood Characteristics and Oxygen Carrying Capacity
4.3.1 Aging Effects
Convective O2 transport in blood from lungs to muscles is another major step in the oxygen transport cascade. The ability to carry O2 to working muscles, which is mostly mediated by the hemoglobin concentration of the blood, plays a major role in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\). Reductions (e.g., in blood donors or anemic patients) or increases (e.g., blood transfusion) in hemoglobin concentration result in an almost proportional change in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) [96, 97]. Changes in total hemoglobin mass have been suggested to influence \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) through an increase in the O2 carrying capacity of the blood, but also through the associated rise in blood volume and subsequent increase in \(\dot{Q}_{ \hbox{max} }\) [97]. On the other hand, aging is inversely associated with hemoglobin levels [98], and indeed there is a high prevalence (> 20%) of anemia among older adults, particularly in the ‘oldest old’ [99]. Although the causes of anemia are multifactorial, iron deficiency, renal insufficiency, chronic inflammation and drug interactions have been proposed as potential factors for impaired erythropoiesis with aging [99].
4.3.2 Training Effects
Controversy exists regarding the effects of exercise training on blood O2 carrying capacity, and the evidence available on its effects in older adults is scarce. However, considering the existing evidence in healthy younger adults, physical exercise might also improve O2 carrying capacity at advanced ages. Exercise training interventions have been reported to stimulate erythropoiesis, reticulocytosis and blood volume expansion in young individuals—mainly because of an increased plasma volume—and although hemoglobin concentration decreases during training due to hemodilution, total hemoglobin mass increases [100]. Later studies have also reported increases in total hemoglobin mass, red blood cell count and total blood volume with endurance training both at sea level and at altitude in young subjects [101].
On the other hand, it can be hypothesized that lifelong physical exercise might be indirectly beneficial for O2 supply in older adults by virtue of its protective effects against chronic inflammation and oxidative stress, both of which are prevalent among inactive older adults (a phenomenon known as ‘inflammaging’) [102] and can negatively affect erythropoiesis [99]. Chronic physical exercise has indeed been proven to attenuate systemic inflammation in older adults, as reflected by decreases in pro-inflammatory markers such as interleukin-6 and C-reactive protein [103]. Although the mechanisms underlying the relationship between inflammation and anemia remain to be elucidated, it has been proposed that excessive levels of inflammation might reduce erythropoietin release, the sensitivity to this hormone, and consequently the proliferation and differentiation of erythroid precursors, also promoting hepcidin synthesis (which reduces iron absorption) and decreasing erythrocyte survival [104, 105].
4.3.3 Key Areas Where More Information is Needed
Although there is biological rationale to support a potential beneficial effect of lifelong endurance training on O2 carrying capacity, longitudinal studies similar to those analyzing the effects at the cardiovascular level are needed. The documented benefits of endurance exercise training on the hemoglobin mass of young healthy subjects must be corroborated in older people, and particularly in the oldest old, who have an increased risk of anemia [99].
4.4 Muscle Capillary Density and Aerobic Enzyme Activity
4.4.1 Aging Effects
Once in the muscle, the ability to extract O2 (i.e., diffusive O2 transport from blood to mitochondria) and to be utilized by mitochondria has been suggested to be the last but essential step for an optimal cardiorespiratory capacity [106]. In this respect, aging is associated with a reduced muscle capillary density [107] as well as with an impaired mitochondrial biogenesis and function [108]. Coley et al. [109] observed that the reduction in muscle oxidative capacity—as reflected by an impaired recovery of muscle creatine phosphate content after exercise—in older adults occurred along with a reduction in the muscle mitochondrial content and oxidative capacity. A reduced local blood flow to contracting muscles was also observed in older adults compared to their younger counterparts, which seems to be partly due to functional impairments in microvascularization [110, 111]. Classical studies reported a relationship between muscle capillary density, mitochondrial density and ‘relative’ \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) (i.e., expressed relative to body mass, in ml·kg−1·min−1) [112, 113], with increases in the latter occurring along with an enhanced capillary density and oxidative enzyme activity [113, 114]. More recently there has been debate on whether the diffusion rate of O2 from micro-vessels into skeletal muscle is actually a limiting factor of \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) [115, 116]. Gifford et al. [117] suggested that among untrained individuals \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) would be limited by mitochondrial O2 demand whereas among trained individuals \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) would be limited by O2 supply despite the presence of a larger mitochondrial respiratory reserve capacity [117]. It has been however recently reported that muscle oxidative capacity was strongly related to relative \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) in individuals with a wide range of \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) values (from 9.8 to 79.0 ml·kg−1·min−1), including both trained individuals and patients with chronic heart failure [118]. In the same line, Esposito et al. observed that improvements in muscle capillary density and mitochondrial density lead to an increased \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) in patients with low physical fitness even in the absence of changes in \(\dot{Q}_{ \hbox{max} }\). [119]. Other authors have found a relationship between muscle oxidative capacity—as assessed through the determination of mitochondrial volume density and citrate synthase activity-, and relative (ml·kg−1·min−1) but not ‘absolute’ (l·min−1) \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) [120, 121]. Thus, the delivery of O2 to skeletal muscle and its utilization by muscle mitochondria should perhaps be viewed as an integrated system, with changes in any step potentially affecting the function of the others [122]. For instance, it has been recently reported that the reductions in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) observed with aging are associated with a reduction in muscle oxidative capacity, but this association seemed to be mediated by the level of resting muscle perfusion [123]. Layec et al. observed that in sedentary older adults ischemic exercise-induced reactive hyperemia resulted in a greater muscle capillary blood flow and convective O2 delivery, which led to an improved tissue oxygenation and mitochondrial function [124]. These findings were in line with those reported by Wray et al., who observed that increasing muscle perfusion in elderly subjects through the ingestion of an antioxidant cocktail led to a concomitant increase in muscle oxidative capacity [125]. Of note, no improvements in muscle perfusion or muscle oxidative capacity were observed in young subjects [125]. Thus, impairments in both muscle oxidative capacity and muscle perfusion together with a potential deterioration of previous steps in the O2 transport cascade seem to play a role in age-related \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) reductions [123]. Particularly, these impairments at the muscle level would result in a reduced arteriovenous O2 difference (a-vO2diff) with aging and consequently a lower extraction and utilization of O2 by the muscle tissue [126, 127].
4.4.2 Training Effects
Endurance exercise has been reported to increase muscle capillary density and oxidative enzymatic activity [114]. Although there are many overlapping pathways involved in these benefits, a key player is the peroxisome proliferator activated receptor γ coactivator 1α (commonly abbreviated as ‘PGC-1α’), which promotes mitochondrial biogenesis [128, 129], together with increases in the levels of vascular endothelial growth factor, a signal protein that stimulates angiogenesis [130]. Moreover, lifelong exercise can help to prevent the reduction in muscle capillary density and oxidative capacity that occurs with aging in inactive people. Iversen et al. [131] observed that trained older adults aged 65–75 years who had been engaged in endurance sports for the last 20–50 years had a 40% higher muscle oxidative enzymatic activity and 27% higher muscle capillarization than their untrained counterparts. In line with the aforementioned findings, a recent study [27] showed that older adults aged ~ 72 to 74 years who had performed lifelong exercise (~ 5 days/week during the previous ~ 52 years) had similar levels of muscle capillarization and aerobic enzyme activity in the vastus lateralis to trained individuals aged ~ 25 years (which in turn were 20–90% greater than those of inactive older adults). Other authors also reported a very minor degree of age-related decline in muscle properties (including mitochondrial protein content) in cyclists aged 55–79 years who had been training for the last ~ 26 years, although a small inverse relationship was found between aging and capillary density in male, but not female, subjects [132]; of note, capillary density was related to training volume in both female and male participants. The benefits of lifelong physical exercise on muscle oxidative capacity seem to be present even at the most advanced ages, as reflected by the 42–54% higher activity of muscle oxidative enzymes found in octogenarian athletes who had performed endurance exercise for > 50 years compared to an age-matched group of inactive individuals [28].
The abovementioned training benefits on muscle capillary density and muscle oxidative capacity would overall result in an attenuated decline of a-vO2diff with aging. Some studies have indeed reported a higher a-vO2diff in endurance-trained older adults than in their sedentary counterparts, with the former in fact presenting similar values to those of young individuals [32, 127]. For instance, Carrick-Ranson et al. observed that subjects aged ~ 68 years who had performed endurance exercise regularly during the previous 25 years—and in fact even those doing less than 3 sessions/week—showed a higher a-vO2diff than those who had remained inactive during an equivalent time period [32]. Thus, lifelong exercise helps to prevent the age-related deterioration in skeletal muscle capillary density and oxidative capacity, which would result in an enhanced extraction and utilization of O2, and consequently in an improved VO2max.
4.4.3 Key Areas Where More Information is Needed
Lifelong endurance exercise seems effective to prevent or at least attenuate the age-related decline in muscle capillary density and oxidative capacity. However, as with other factors affecting \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\), evidence is lacking on whether these benefits are also present at the most advanced ages. Moreover, despite the potential important role of capillary density and oxidative capacity in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) as the last step of the oxygen transport cascade, some debate has been raised on the actual influence of these factors [115]. In this respect, a systematic review of 70 studies found that relative increases in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) with training were overall associated with the changes observed in muscle oxidative capacity [121]. This association, however, was not significant when analyzing older subjects separately, which suggests that there might be other confounding factors (e.g., impairments in previous steps of the O2 transport cascade) affecting \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) in old people [121].
5 Limitations and Perspectives
The evidence about the benefits of exercise at the most advanced ages (> 80 years) is rather scarce. Although anecdotal data in very old masters athletes would indicate that it is possible to retain a remarkable physical function with proper physical training, these preliminary findings should be confirmed in adequately-powered studies with large cohorts—including also non-athletes in order to assess generalizability to the general population. On the other hand, further research is needed to elucidate the main training-related variables driving exercise benefits on \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\). Indeed, most reports refer to training frequency (i.e., days per week) as a modulator of these benefits, but other less studied variables such as training volume or intensity are likely to play a major role. Of note is also the fact that we have consistently used the term \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) throughout our review even though a less valid surrogate, peak oxygen uptake (\(\dot{V}{\text{O}}_{{ 2 {\text{peak}}}}\), that is, the peak value of \(\dot{V}{\text{O}}_{2}\) recorded during maximal exercise testing even when an actual plateau in \(\dot{V}{\text{O}}_{2}\) values or other criteria of maximality were not fulfilled) was the parameter that was actually reported in numerous studies discussed here. Using \(\dot{V}{\text{O}}_{{ 2 {\text{peak}}}}\) might lead to an underestimation of actual \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) values in some individuals, particularly those who are naïve to the test, less motivated, or who are less fit (such as, e.g., patient populations) [133]. Future studies should optimize methodological procedures to ensure an appropriate assessment of VO2max.
Finally, the bulk of scientific evidence in the field comes from studies conducted in men only. Preliminary evidence suggests that oldest old women can also retain high \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) levels with lifelong exercise training [46]. Women usually present with lower values of relative and absolute \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) than men [134], and although they might also show some different physiological adaptations (e.g., lower rates of increase in cardiac mass, SVmax, or \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) after one year of endurance training) [135], evidence suggests that the age-related reduction in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) observed in women is also modulated by reductions in training volume [21]. Research is nevertheless warranted to determine potential between-sex differences in the effects of lifelong exercise on the age-related \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) decline.
6 Conclusions
Although aging has been traditionally associated with an exponential decline in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) and overall physical function, this association might be confounded by many factors, notably the increasingly inactive lifestyle that often accompanies the aging process in the general population. Although more longitudinal studies are needed, particularly in non-athletes, current data from masters athletes suggest that the rate of age-related decline in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) might be modulated by the amount of physical exercise performed over life, with higher levels exerting a marked protective function against the ultimately inevitable aging-induced deterioration in most of the physiological mechanisms that influence \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) (i.e., pulmonary and cardiovascular function, blood oxygen transport capacity, skeletal muscle capillary density and oxidative capacity) (Fig. 2). Future longitudinal studies should, however, confirm this hypothesis as well as the actual role of age-related, non-pathological reductions in some physiological factors (e.g., pulmonary function and HRmax) in \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) decline. Overall, given the clinical importance of reaching an advanced age with a preserved functional capacity, the evidence available supports the need for maintaining high levels of physical exercise across all ages, including at an advanced age.
References
Joyner MJ, Coyle EF. Endurance exercise performance: the physiology of champions. J Physiol. 2008;586:35–44.
Ross R, Blair SN, Arena R, Church TS, Després JP, Franklin BA, et al. Importance of assessing cardiorespiratory fitness in clinical practice: a case for fitness as a clinical vital sign: a scientific statement from the American heart Association. Circulation. 2016;134:e653–99.
Astrand I, Astrand P, Hallback I, Kilbom A. Reduction in maximal oxygen uptake with age. J Appl Physiol. 1973;35:649–54.
Fleg J, Morrell C, Bos A, Brant L, Talbot L, Wright J, et al. Accelerated longitudinal decline of aerobic capacity in healthy older adults. Circulation. 2005;112:674–82.
Myers J, Prakash M, Froelicher V, Do D, Partington S, Atwood J. Exercise capacity and mortality among men referred for exercise testing. N Engl J Med. 2002;346:793–801.
Mandsager K, Harb S, Cremer P, Phelan D, Nissen SE, Jaber W. Association of cardiorespiratory fitness with long-term mortality among adults undergoing exercise treadmill testing. JAMA Netw Open. 2018;1:e183605.
Kodama S, Saito K, Tanaka S, Maki M, Yachi Y, Asumi M, et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events. J Am Med Assoc. 2009;301:2024–35.
Lazarus NR, Izquierdo M, Higginson IJ, Harridge SDR. Exercise deiciency diseases of ageing: the primacy of exercise and muscle strengthening as irst line therapeutic agents to combat frailty. J Am Med Dir Assoc. 2018;19:741–3.
Clegg A, Young J, Iliffe S, Olde Rikkert M, Rockwood K. Frailty in elderly people. Lancet. 2013;381:752–62.
Guthold R, Stevens GA, Riley LM, Bull FC. Worldwide trends in insuicient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob. Health. 2018;6:e1077–86.
Noakes T, Spedding M. Olympics: run for your life. Nature. 2012;487:295–6.
Harridge SDR, Lazarus NR. Physical activity, aging, and physiological function. Physiology. 2017;32:152–61.
Valenzuela P, Castillo-García A, Morales J, Izquierdo M, Serra-Rexach J, Santos-Lozano A, et al. Physical exercise in the oldest old. Compr Physiol. 2019;9:1281–304.
Tanaka H, Seals DR. Dynamic exercise performance in Masters athletes: insight into the effects of primary human aging on physiological functional capacity. J Appl Physiol. 2003;95:2152–62.
Lazarus NR, Harridge SDR. Declining performance of master athletes: silhouettes of the trajectory of healthy human ageing? J Physiol. 2017;595:2941–8.
Lepers R, Stapley PJ. Master athletes are extending the limits of human endurance. Front Physiol. 2016;7:1–8.
Tanaka H, Seals DR. Endurance exercise performance in Masters athletes: age-associated changes and underlying physiological mechanisms. J Physiol. 2008;586:55–63.
Dehn MM, Bruce RA. Longitudinal variations in maximal oxygen intake with age and activity. J Appl Physiol. 1972;33:805–7.
Wilson TM, Tanaka H. Meta-analysis of the age-associated decline in maximal aerobic capacity in men: relation to training status. Am J Physiol Circ Physiol. 2000;278:H829–34.
Fitzgerald MD, Tanaka H, Tran ZV, Seals DR. Age-related declines in maximal aerobic capacity in regularly exercising vs. sedentary women: a meta-analysis. J Appl Physiol. 1997;83:160–5.
Eskurza I, Donato AJ, Moreau KL, Seals DR, Tanaka H. Changes in maximal aerobic capacity with age in endurance-trained women: 7-yr follow-up. J Appl Physiol. 2002;92:2303–8.
Pimentel AE, Gentile CL, Tanaka H, Seals DR, Gates PE. Greater rate of decline in maximal aerobic capacity with age in endurance-trained than in sedentary men. J Appl Physiol. 2003;94:2406–13.
Trappe SW, Costill DL, Vukovich MD, Jones J, Melham T. Aging among elite distance runners: a 22-yr longitudinal study. J Appl Physiol. 1996;80:285–90.
Katzel LI, Sorkin JD, Fleg JL. A comparison of longitudinal changes in aerobic fitness in older endurance athletes and sedentary men. J Am Geriatr Soc. 2001;49:1657–64.
Kasch FW, Van Camp S, Nettl F, Wallace JP. Cardiovascular changes with age and exercise: a 28-year longitudinal study. Scand J Med Sci Sports. 1995;5:147–51.
Rogers MA, Hagberg JM, Martin WH, Ehsani AA, Holloszy JO. Decline in VO2max with aging in master athletes and sedentary men. J Appl Physiol. 1990;68:2195–9.
Gries KJ, Raue U, Perkins RK, Lavin KM, Overstreet BS, D’Acquisto LJ, et al. Cardiovascular and skeletal muscle health with lifelong exercise. J Appl Physiol. 2018;125:1636–45.
Trappe S, Hayes E, Galpin A, Jemiolo B, Fink W, Trappe T, et al. New records in aerobic power among octogenarian lifelong endurance athletes. J Appl Physiol. 2013;114:3–10.
Arbab-Zadeh A, Dijk E, Prasad A, Fu Q, Torres P, Zhang R, et al. Effect of aging and physical activity on left ventricular compliance. Circulation. 2004;110:1799–805.
Prasad A, Popovic ZB, Arbab-Zadeh A, Fu Q, Palmer D, Dijk E, et al. The effects of aging and physical activity on doppler measures of diastolic function. Am J Cardiol. 2007;99:1629–36.
Bhella PS, Hastings JL, Fujimoto N, Shibata S, Carrick-Ranson G, Palmer MD, et al. Impact of lifelong exercise “dose” on left ventricular compliance and distensibility. J Am Coll Cardiol. 2014;64:1257–66.
Carrick-Ranson G, Hastings JL, Bhella PS, Fujimoto N, Shibata S, Palmer MD, et al. The effect of lifelong exercise dose on cardiovascular function during exercise. J Appl Physiol. 2014;116:736–45.
Hieda M, Howden E, Sarma S, Tarumi T, Palmer D, Lawley J, et al. Impact of lifelong exercise training “dose” on ventricular-arterial coupling. Circulation. 2018;138:2638–47.
Mckendry J, Breen L, Shad BJ, Greig CA. Muscle morphology and performance in master athletes: a systematic review and meta-analyses. Ageing Res Rev. 2018;45:62–82.
Montero D, Díaz-Cañestro C. Maximal cardiac output in athletes: Influence of age. Eur J Prev Cardiol. 2015;22:1588–600.
Bacon AP, Carter RE, Ogle EA, Joyner MJ. VO2max trainability and high Intensity interval training in humans: a meta-analysis. PLoS ONE. 2013;8:e73182.
MacInnis MJ, Gibala MJ. Physiological adaptations to interval training and the role of exercise intensity. J Physiol. 2017;595:2915–30.
ACSM. ACSM’s guidelines for exercise testing and prescription. 10th ed. Philadelphia: Lippincott Williams & Wilkins; 2010.
Burtscher M, Nachbauer W, Wilber R. The upper limit of aerobic power in humans. Eur J Appl Physiol. 2011;111:2625–8.
Ronnestad BR, Hansen J, Stenlokken L, Joyner M, Lundby C. Case studies in physiology: temporal changes in determinants of aerobic performance in individual going from alpine skier to world champion time trial cyclist. J Appl Physiol. 2019;127:306–11.
Everman S, Farris JW, Bay RC, Daniels JT. Elite distance runners: a 45-year follow-up. Med Sci Sports Exerc. 2018;50:73–8.
Heath GW, Hagberg JM, Ehsani AA, Holloszy JO. A physiological comparison of young and older endurance athletes. J Appl Physiol. 1981;51:634–40.
Lepers R, Bontemps B, Louis J. Physiological profile of a 59-year-old male world record holder marathoner. Med Sci Sports Exerc. 2019. https://doi.org/10.1249/MSS.0000000000002181.
Maud PJ, Pollock ML, Foster C, Anholm JD, Guten G, Al-Nouri M, et al. Fifty years of training and competition in the marathon: Wally Hayward, age 70—a physiological profile. S Afr Med J. 1981;59:153–7.
Karlsen T, Leinan IM, Bækkerud FH, Lundgren KM, Tari A, Steinshamn SL, et al. How to be 80 year old and have a VO2max of a 35 year old. Case Rep Med. 2015;2015:1–6.
Cattagni T, Gremeaux V, Lepers R. The physiological characteristics of an 83-year-old champion female master runner. Int J Sports Physiol Perform. 2019. https://doi.org/10.1123/ijspp.2018-0879.
Billat V, Dhonneur G, Mille-Hamard L, Le Moyec L, Momken I, Launay T, et al. Maximal oxygen consumption and performance in a centenarian cyclist. J Appl Physiol. 2017;122:430–4.
Lepers R, Cattagni T. Age-related decline in endurance running performance—an example of a multiple World records holder. Appl Physiol Nutr Metab. 2018;43:98–100.
Pollock RD, Carter S, Velloso CP, Duggal NA, Lord JM, Lazarus NR, et al. An investigation into the relationship between age and physiological function in highly active older adults. J Physiol. 2015;593:657–80.
Kaminsky LA, Imboden MT, Arena R, Myers J. Reference standards for cardiorespiratory fitness measured with cardiopulmonary exercise testing using cycle ergometry: Data from the Fitness Registry and the importance of Exercise National Database (FRIEND) Registry. Mayo Clin Proc. 2017;92:228–33.
Williams CJ, Williams MG, Eynon N, Ashton KJ, Little JP, Wisloff U, et al. Genes to predict VO2max trainability: a systematic review. BMC Genomics. 2017;18:831.
Bouchard C. DNA sequence variations contribute to variability in fitness and trainability. Med Sci Sports Exerc. 2019;51:1781–5.
Joyner MJ. Limits to the evidence that DNA sequence diferences contribute to the variability in fitness and trainability. Med Sci Sports Exerc. 2019;51:1786–9.
Wagner PD. Determinants of maximal oxygen transport and utilization. Annu Rev Physiol. 1996;58:21–50.
Aalami O, Fang T, Song H, Nacamuli R. Physiological features of aging persons. Arch Surg. 2003;138:1068–76.
Lowery EM, Brubaker AL, Kuhlmann E, Kovacs EJ. The aging lung. Clin Interv Aging. 2013;8:1489–96.
Knudson R, Lebowitz M, Holberg C, Burrows B. Changes in the normal maximal expiratory flow-volume curve with growth and aging. Am Rev Respir Dis. 1983;127:725–34.
Sorbini C, Grassi V, Solinas E, Muisan G. Arterial oxygen tension in relation to age in healthy subjects. Respiration. 1968;25:3–13.
Thurlbeck W, Angus G. Growth and aging of the normal human lung. Chest. 1975;67:3S–7S.
Bassett D, Howley E. Limiting factors for maximum oxygen uptake and determinants of endurance performance. Med Sci Sports Exerc. 2000;32:70–84.
Hassel E, Stensvold D, Halvorsen T, Wisløff U, Langhammer A, Steinshamn S. Association between pulmonary function and peak oxygen uptake in elderly: the Generation 100 study. Respir Res. 2015;16:1–8.
Rasch-Halvorsen Ø, Steinshamn S, Hassel E, Brumpton BM, Langhammer A. The association between dynamic lung function and peak oxygen uptake in a healthy general population. The HUNT Study. BMC Pulm Med. 2019;19:OA3190.
Babb TG. Ventilatory response to exercise in subjects breathing CO2 or HeO2. J Appl Physiol. 1997;82:746–54.
Babb TG, DeLorey DS, Wyrick BL. Ventilatory response to exercise in aged runners breathing He-O2 or inspired CO2. J Appl Physiol. 2003;94:685–93.
Babb TG. Ventilation and respiratory mechanics during exercise in younger subjects breathing CO2 or HeO2. Respir Physiol. 1997;109:15–28.
Roman MA, Rossiter HB, Casaburi R. Exercise, ageing and the lung. Eur Respir J. 2016;48:1471–86.
Bathgate KE, Bagley JR, Jo E, Talmadge RJ, Tobias IS, Brown LE, et al. Muscle health and performance in monozygotic twins with 30 years of discordant exercise habits. Eur J Appl Physiol. 2018;118:2097–110.
Johnson BD, Reddan WG, Seow KC, Dempsey JA. Mechanical constraints on exercise hyperpnea in a fit aging population. Am Rev Respir Dis. 1991;143:968–77.
McClaran SR, Babcock MA, Pegelow DF, Reddan WG, Dempsey JA. Longitudinal effects of aging on lung function at rest and exercise in healthy active fit elderly adults. J Appl Physiol. 1995;78:1957–68.
Jakes RW, Day NE, Patel B, Khaw KT, Oakes S, Luben R, et al. Physical inactivity is associated with lower forced expiratory volume in 1 second: European prospective investigation into cancer-Norfolk prospective population study. Am J Epidemiol. 2002;156:139–47.
Pelkonen M, Notkola IL, Lakka T, Tukiainen HO, Kivinen P, Nissinen A. Delaying decline in pulmonary function with physical activity: a 25-year follow-up. Am J Respir Crit Care Med. 2003;168:494–9.
Degens H, Maden-Wilkinson TM, Ireland A, Korhonen MT, Suominen H, Heinonen A, et al. Relationship between ventilatory function and age in master athletes and a sedentary reference population. Age. 2013;35:1007–15.
Taylor BJ, Johnson BD. The pulmonary circulation and exercise responses in the elderly. Semin Respir Crit Care Med. 2010;31:528–38.
Préfaut C, Anselme F, Caillaud C, Massé-Biron J. Exercise-induced hypoxemia in older athletes. J Appl Physiol. 1994;76:120–6.
Mills DE, Johnson MA, Barnett YA, Smith WHT, Sharpe GR. The effects of inspiratory muscle training in older adults. Med Sci Sports Exerc. 2015;47:691–7.
Hill A, Lupton H. Muscular exercise, lactic acid, and the supply and utilization of oxygen. Proc R Soc. 1924;97:135–71.
Levine BD. VO2max: what do we know, and what do we still need to know? J Physiol. 2008;586:25–34.
Lye M, Donnellan C. Heart disease in the elderly. Heart. 2000;84:560–6.
Fujimoto N, Hastings JL, Bhella PS, Shibata S, Gandhi NK, Carrick-Ranson G, et al. Effect of ageing on left ventricular compliance and distensibility in healthy sedentary humans. J Physiol. 2012;590:1871–80.
Francis Stuart SD, Wang L, Woodard WR, Ng GA, Habecker BA, Ripplinger CM. Age-related changes in cardiac electrophysiology and calcium handling in response to sympathetic nerve stimulation. J Physiol. 2018;596:3977–91.
Vaitkevicius PV, Fleg JL, Engel JH, O’Connor FC, Wright JG, Lakatta LE, et al. Effects of age and aerobic capacity on arterial stiffness in healthy adults. Circulation. 1993;88:1456–62.
Tschakovsky ME, Sujirattanawimol K, Ruble SB, Valic Z, Joyner MJ. Is sympathetic neural vasoconstriction blunted in the vascular bed of exercising human muscle? J Physiol. 2002;541:623–35.
Mortensen SP, Nyberg M, Winding K, Saltin B. Lifelong physical activity preserves functional sympatholysis and purinergic signalling in the ageing human leg. J Physiol. 2012;590:6227–36.
Racine M, Dinenno F. Reduced deformability contributes to impaired deoxygenation-induced ATP release from red blood cells of older adult humans. J Physiol. 2019;597:4503–19.
Howden EJ, Carrick-Ranson G, Sarma S, Hieda M, Fujimoto N, Levine BD. Effects of sedentary aging and lifelong exercise on left ventricular systolic function. Med Sci Sports Exerc. 2018;50:494–501.
Hagberg JM, Allen WK, Seals DR, Hurley BF, Ehsani AA, Holloszy JO. A hemodynamic comparison of young and older endurance athletes during exercise. J Appl Physiol. 1985;58:2041–6.
Hawkins SA, Marcell TJ, Jaque SV, et al. A longitudinal VO2max and maximal heart rate in master athletes. Med Sci Sports Exerc. 2001;33:7.
Nybo L, Schmidt JF, Fritzdorf S, Nordsborg NB. Physiological characteristics of an aging olympic athlete. Med Sci Sports Exerc. 2014;46:2132–8.
Proctor DN, Shen PH, Dietz NM, Eickhoff TJ, Lawler LA, Ebersold EJ, et al. Reduced leg blood flow during dynamic exercise in older endurance-trained men. J Appl Physiol. 1998;85:68–75.
Franzoni F, Ghiadoni L, Galetta F, Plantinga Y, Lubrano V, Huang Y, et al. Physical activity, plasma antioxidant capacity, and endothelium-dependent vasodilation in young and older men. Am J Hypertens. 2005;18:510–6.
Montero D, Padilla J, Diaz-Cañestro C, Muris DMJ, Pyke KE, Obert P, et al. Flow-mediated dilation in athletes: influence of aging. Med Sci Sports Exerc. 2014;46:2148–58.
Shibata S, Fujimoto N, Hastings JL, Carrick-Ranson G, Bhella PS, Hearon CM, et al. The effect of lifelong exercise frequency on arterial stiffness. J Physiol. 2018;596:2783–95.
Groot H, Rossman M, Garten R, Wang E, Hoff J, Helgerud J, et al. The effect of physical activity on passive leg movement-induced vasodilation with age. Med Sci Sports Exerc. 2016;48:1548–57.
Nyberg M, Blackwell JR, Damsgaard R, Jones AM, Hellsten Y, Mortensen SP. Lifelong physical activity prevents an age-related reduction in arterial and skeletal muscle nitric oxide bioavailability in humans. J Physiol. 2012;590:5361–70.
Munch GDW, Svendsen JH, Damsgaard R, Secher NH, González-Alonso J, Mortensen SP. Maximal heart rate does not limit cardiovascular capacity in healthy humans: insight from right atrial pacing during maximal exercise. J Physiol. 2014;592:377–90.
Calbet JAL, Lundby C, Koskolou M, Boushel R. Importance of hemoglobin concentration to exercise: acute manipulations. Respir Physiol Neurobiol. 2006;151:132–40.
Schmidt WF, Prommer N. Impact of alterations in total hemoglobin mass on VO2max. Exerc Sport Sci Rev. 2010;38:68–75.
Salive M, Cornoni-Huntley J, Guralnik J, Philips C, Wallace R, Ostfeld A, et al. Anemia and hemoglobin levels in older persons: relationship with age, gender, and health status. J Am Geriatr Soc. 1992;40:489–96.
Steensma DP, Tefferi A. Anemia in the elderly: how should we define it, when does it matter, and what can be done? Mayo Clin Proc. 2007;82:958–66.
Schmidt W, Maassen N, Trost F, Böning D. Training induced effects on blood volume, erythrocyte turnover and haemoglobin oxygen binding properties. Eur J Appl Physiol Occup Physiol. 1988;57:490–8.
Schmidt W, Heinicke K, Rojas J, Gomez JM, Serrato M, Mora M, et al. Blood volume and hemoglobin mass in endurance athletes from moderate altitude. Med Sci Sports Exerc. 2002;34:1934–40.
Rea IM, Gibson DS, McGilligan V, McNerlan SE, Denis Alexander H, Ross OA. Age and age-related diseases: role of inflammation triggers and cytokines. Front Immunol. 2018;9:1–28.
Monteiro Junior RS, de Tarso Maciel-Pinheiro P, da Matta M Portugal E, da Silva Figueiredo LF, Terra R, Carneiro LSF, et al. Effect of exercise on inflammatory profile of older persons: systematic review and meta-analyses. J Phys Act Health. 2018;15:65–71.
Macciò A, Madeddu C. Management of anemia of inflammation in the elderly. Anemia. 2012;2012:1–20.
Nemeth E, Ganz T. Anemia of inflammation. Hematol Oncol Clin N Am. 2014;28:671–81.
di Prampero P. Metabolic and circulatory limitations to VO2max at the whole animal level. J Exp Biol. 1985;115:319–31.
Groen B, Hamer HM, Snijders T, van Kranenburg J, Frijns D, Vink H, et al. Skeletal muscle capillary density and microvascular function are compromised with aging and type 2 diabetes. J Appl Physiol. 2014;116:998–1005.
Chistiakov DA, Sobenin IA, Revin VV, Orekhov AN, Bobryshev YV. Mitochondrial aging and age-related dysfunction of mitochondria. Biomed Res Int. 2014;2014:238463.
Conley KE, Jubrias SA, Esselman PC. Oxidative capacity and ageing in human muscle. J Physiol. 2000;526(Pt 1):203–10.
Proctor DN, Parker BA. Vasodilation and vascular control in contracting muscle of the aging human. Microcirculation. 2006;13:325–37.
Hildebrandt W, Schwarzbach H, Pardun A, Hannemann L, Bogs B, König AM, et al. Age-related differences in skeletal muscle microvascular response to exercise as detected by contrast-enhanced ultrasound (CEUS). PLoS ONE. 2017;12:1–25.
Ingjer F. Maximal aerobic power related to the capillary supply of the quadriceps femoris muscle in man. Acta Physiol Scand. 1978;104:238–40.
Hoppeler H, Howald H, Conley K, Lindstedt SL, Claassen H, Vock P, et al. Endurance training in humans: aerobic capacity and structure of skeletal muscle. J Appl Physiol. 1985;59:320–7.
Andersen P, Henriksson J. Capillary supply of the quadriceps femoris muscle of man: adaptive response to exercise. J Physiol. 1977;270:677–90.
Lundby C, Montero D. CrossTalk opposing view: diffusion limitation of O2 from microvessels into muscle does not contribute to the limitation of VO2max. J Physiol. 2015;593:3759–61.
Wagner PD. CrossTalk proposal: diffusion limitation of O2 from microvessels into muscle does contribute to the limitation of VO2max. J Physiol. 2015;593:3757–8.
Gifford JR, Garten RS, Nelson AD, Trinity JD, Layec G, Witman MAH, et al. Symmorphosis and skeletal muscle VO2max: in vivo and in vitro measures reveal differing constraints in the exercise-trained and untrained human. J Physiol. 2016;594:1741–51.
van der Zwaard S, de Ruiter CJ, Noordhof DA, Sterrenburg R, Bloemers FW, de Koning JJ, et al. Maximal oxygen uptake is proportional to muscle fiber oxidative capacity, from chronic heart failure patients to professional cyclists. J Appl Physiol. 2016;121:636–45.
Esposito F, Reese V, Shabetai R, Wagner P, Richardson R. Isolated quadriceps training increases maximal exercise capacity in chronic heart failure: the role of skeletal muscle convective and diffusive oxygen transport. J Am Coll Cardiol. 2011;58:1353–62.
Lundby C, Jacobs RA. Adaptations of skeletal muscle mitochondria to exercise training. Exp Physiol. 2016;101:17–22.
Vigelsø A, Andersen NB, Dela F. The relationship between skeletal muscle mitochondrial citrate synthase activity and whole body oxygen uptake adaptations in response to exercise training. Int J Physiol Pathophysiol Pharmacol. 2014;6:84–101.
Wagner PD. Modeling O2 transport as an integrated system limiting VO2max. Comput Methods Programs Biomed. 2011;101:109–14.
Adelnia F, Cameron D, Bergeron C, Fishbein K, Spencer R, Reiter D, et al. The role of perfusion in the age-associated decline of mitochondrial function with aging in healthy individuals. Front Physiol. 2019;10:427.
Layec G, Trinity JD, Hart CR, Le Fur Y, Sorensen JR, Jeong EK, et al. Evidence of a metabolic reserve in the skeletal muscle of elderly people. Aging. 2017;9:52–67.
Wray DW, Nishiyama SK, Monnet A, Wary C, Duteil SS, Carlier PG, et al. Antioxidants and aging: NMR-based evidence of improved skeletal muscle perfusion and energetics. Am J Physiol Heart Circ Physiol. 2009;297:1870–5.
Carrick-Ranson G, Hastings JL, Bhella PS, Shibata S, Fujimoto N, Palmer D, et al. The effect of age-related differences in body size and composition on cardiovascular determinants of VO2max. J Gerontol Ser A Biol Sci Med Sci. 2013;68:608–16.
Ogawa T, Spina RJ, Martin WH, Kohrt WM, Schechtman KB, Holloszy JO, et al. Effects of aging, sex, and physical training on cardiovascular responses to exercise. Circulation. 1992;86:494–503.
Irrcher I, Adhihetty PJ, Joseph AM, Ljubicic V, Hood DA. Regulation of mitochondrial biogenesis in muscle by endurance exercise. Sports Med. 2003;33:783–93.
Kang C, Ji LL. Role of PGC-1α in muscle function and aging. J Sports Health Sci. 2013;2:81–6.
Gavin TP, Ruster RS, Carrithers JA, Zwetsloot KA, Kraus RM, Evans CA, et al. No difference in the skeletal muscle angiogenic response to aerobic exercise training between young and aged men. J Physiol. 2007;585:231–9.
Iversen N, Krustrup P, Rasmussen HN, Rasmussen UF, Saltin B, Pilegaard H. Mitochondrial biogenesis and angiogenesis in skeletal muscle of the elderly. Exp Gerontol. 2011;46:670–8.
Pollock RD, O’Brien KA, Daniels LJ, Nielsen KB, Rowlerson A, Duggal NA, et al. Properties of the vastus lateralis muscle in relation to age and physiological function in master cyclists aged 55–79 years. Aging Cell. 2018;17:e12735.
Poole DC, Jones AM. Measurement of the maximum oxygen uptake VO2max: VO2peak is no longer acceptable. J Appl Physiol. 2017;122:997–1002.
Joyner MJ. Physiological limits to endurance exercise performance: influence of sex. J Physiol. 2017;595:2949–54.
Howden EJ, Perhonen M, Peshock RM, Zhang R, Arbab-Zadeh A, Adams-Huet B, et al. Females have a blunted cardiovascular response to one year of intensive supervised endurance training. J Appl Physiol. 2015;119:37–46.
Ingjer F. Maximal oxygen uptake as a predictor of performance ability in women and men elite cross-country skiers. Scand J Med Sci Sports. 1991;1:25–30.
Acknowledgements
We sincerely thank Adrián Castillo García (http://www.fissac.com) for designing the figures included in this work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The work of Pedro Valenzuela is supported by University of Acalá (FPI2016) and the research by Alejandro Lucia on aging is funded by the Fondo de Investigaciones Sanitarias, Instituto de Salud Carlos III (FIS, Grant PI15/00558) and cofunded by ‘Fondos FEDER’. No other specific sources of funding were used to assist in the preparation of this article.
Conflict of interest
Pedro L. Valenzuela, Nicola A. Maffiuletti, Michael J. Joyner, Alejandro Lucia and Romuald Lepers declare that they have no conflicts of interest relevant to the content of this review.
Rights and permissions
About this article

Cite this article
Valenzuela, P.L., Maffiuletti, N.A., Joyner, M.J. et al. Lifelong Endurance Exercise as a Countermeasure Against Age-Related \(\dot{V}{\text{O}}_{{ 2 {\text{max}}}}\) Decline: Physiological Overview and Insights from Masters Athletes. Sports Med 50, 703–716 (2020). https://doi.org/10.1007/s40279-019-01252-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-019-01252-0