
Abstract
Background
Resistance training is well known to increase strength and lean body mass, and plays a key role in many female athletic and recreational training programs. Most females train throughout their reproductive years when they are exposed to continuously changing female steroid hormone profiles due to the menstrual cycle or contraceptive use. Therefore, it is important to focus on how female hormones may affect resistance training responses.
Objective
The aim of this systematic review is to identify and critically appraise current studies on the effect of the menstrual cycle and oral contraceptives on responses to resistance training.
Methods
The electronic databases Embase, PubMed, SPORTDiscus and Web of Science were searched using a comprehensive list of relevant terms. Studies that investigated the effect of the menstrual cycle phase or oral contraceptive cycle on resistance training responses were included. Studies were also included if they compared resistance training responses between the natural menstrual cycle and oral contraceptive use, or if resistance training was adapted to the menstrual cycle phase or oral contraceptive phase. Studies were critically appraised with the McMasters Universities Critical Review Form for Quantitative Studies and relevant data were extracted.
Results
Of 2007 articles found, 17 studies met the criteria and were included in this systematic review. The 17 included studies had a total of 418 participants with an age range of 18–38 years. One of the 17 studies found no significant differences in acute responses to a resistance training session over the natural menstrual cycle, while four studies did find changes. When assessing the differences in acute responses between the oral contraceptive and menstrual cycle groups, two studies reported oral contraceptives to have a positive influence, whilst four studies reported that oral contraceptive users had a delayed recovery, higher levels of markers of muscle damage, or both. For the responses to a resistance training program, three studies reported follicular phase-based training to be superior to luteal phase-based training or regular training, while one study reported no differences. In addition, one study reported no differences in strength development between oral contraceptive and menstrual cycle groups. One further study reported a greater increase in type I muscle fibre area and a trend toward a greater increase in muscle mass within low-androgenic oral contraceptive users compared with participants not taking hormonal contraceptives. Finally, one study investigated androgenicity of oral contraceptives and showed greater strength developments with high androgenic compared with anti-androgenic oral contraceptive use.
Conclusions
The reviewed articles reported conflicting findings, and were often limited by small participant numbers and methodological issues, but do appear to suggest female hormones may affect resistance training responses. The findings of this review highlight the need for further experimental studies on the effects of the menstrual cycle and oral contraceptives on acute and chronic responses to resistance training.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The effects of both the menstrual cycle and oral contraceptive use on acute responses to resistance training remain unclear. |
Follicular phase-based resistance training programs appear to result in better responses than luteal phase-based and regular training programs. |
Further research is needed in this area, including a focus on different types of oral contraceptives. |
1 Background
Resistance training is well established as a method for increasing strength and lean body mass. Many female athletes perform resistance training to improve sport performance and in the general population resistance training is popular as a form of recreational exercise for health-related benefits [1]. Despite the increase in female participation in resistance training, research in the area is often still performed on males or post-menopausal females with the results generalised to other populations. However, due to the completely different hormonal profiles of females of reproductive age, it is not possible to conclusively apply these results to this population.
In eumenorrhoeic females, the steroid hormones estrogen and progesterone fluctuate throughout the phases of the menstrual cycle. Three distinct hormonal environments have been identified: the early follicular phase characterised by low estrogen and progesterone concentrations, the late follicular (or peri-ovulatory) phase characterised by high estrogen and low progesterone concentrations, and the luteal phase where high levels of estrogen and progesterone are present [2]. However, many reproductive-aged females do not experience the expected fluctuations in endogenous hormones due to menstrual irregularities or the use of hormonal contraceptives. Oral contraceptives are a common form of birth control both in the general community and amongst female athletes [3]. With the use of oral contraceptives, the production of endogenous estrogen and progesterone is suppressed [4]. There are many different types of oral contraceptives. The combined multiphasic oral contraceptives (biphasic or triphasic) aim to mimic the normal physiological hormone fluctuations of the menstrual cycle by varying the doses of synthetic female sex hormones, such as ethinyl-estradiol and progestin, in each phase [5]. Progestin-only oral contraceptives are available for those who do not wish to take exogenous estrogen, such as lactating women and those who have a high cardiovascular risk [6]. However, the most commonly prescribed oral contraceptives are combined monophasic oral contraceptives, which deliver synthetic estrogen and progestin, in a uniform daily dose in all active pills [1]. The typical oral contraceptive regime consists of 21 active pills followed by seven non-active pills to induce cyclic withdrawal bleeding to mimic the natural menstrual cycle [7]. Therefore, most females of reproductive age are exposed to fluctuations in either endogenous or exogenous female steroid hormones. Apart from reproductive roles, both estrogen and progesterone have numerous physiological effects outside of the reproductive system by acting on receptor sites in target tissues [8]. As estrogen and progesterone receptors have been identified in skeletal muscles [9], variations in hormonal concentrations due to the menstrual cycle or oral contraceptive use may influence resistance training outcomes.
During menopause, a period classified by decreasing levels of estrogen and progesterone, a marked decline in muscle strength has been reported [10]. Results from a meta-analysis have determined that hormone replacement therapy and particularly estrogen replacement can reverse these initial declines in strength [11]. There are very few studies available regarding the specific influence of progesterone on muscle strength and function. However, menstrual cycle research has reported greater amino acid oxidation and protein degradation in the luteal phase when compared to the follicular phase both at rest [12, 13] and during exercise [14, 15]. Thus, it has been suggested that progesterone increases protein catabolism, while estrogen may have an anabolic effect on muscle [16]. Based on the strengthening effect of estrogen on muscle during HRT, it could be suggested that oral contraceptive use may also provide benefits for muscle strength and function. However, it is unclear if the synthetic forms of hormones in oral contraceptives, some of which are derived from testosterone [6], have any effect on muscle strength and repair. Therefore, variations in endogenous and exogenous estrogen and progesterone may influence resistance training responses differently between the phases of the menstrual cycle or oral contraceptive cycle and between oral contraceptive users and females with a natural menstrual cycle.
The difficulties surrounding timing of testing to coincide with hormone fluctuations and measuring hormones to ensure the correct phase is being examined may be some of the reasons for the lack of research on resistance training in premenopausal females [2]. However, given the increase in resistance training participation in females, research that explores the effect of endogenous and exogenous female sex hormones on resistance training responses may enhance training outcomes in this population. Therefore, the objective of this manuscript was to investigate, by way of systematic review of the literature, the effect of the menstrual cycle phase and oral contraceptive use on responses to resistance training exercise in females of reproductive age.
2 Methods
2.1 Data Sources and Searches
An electronic database search of title and abstract in Embase, PubMed, SPORTDiscus and Web of Science was conducted on 15 September 2019. Search terms used were resistance training, weight training, strength training, resistive exercise, concentric exercise, eccentric exercise, phase-based training, menstrual cycle, oral contraceptives, endogenous hormones, exogenous hormones, luteal phase, follicular phase, estrogen, progesterone, progestin and estradiol (Electronic Supplementary Material Table S1). The search was restricted to the English language; however, no date restrictions were used. A manual search of the reference lists of included articles was also performed.
2.2 Study Selection
Only published full-text articles that investigated the effect of the menstrual cycle phase or oral contraceptives on resistance training responses were included. Studies were also included if they compared resistance training responses between the natural menstrual cycle and oral contraceptive use, or if resistance training was adapted to the menstrual cycle phase or oral contraceptive phase. Studies were excluded where no comparison was made between the phases of the menstrual cycle or oral contraceptive cycle or if there was no comparison of resistance training outcomes between oral contraceptive use and the natural menstrual cycle. Studies were also excluded where the responses to resistance training were not examined or where other interventions were used in conjunction with a resistance training protocol. Studies with a male or amenorrhoeic group were included if there was still a comparison between menstrual cycle or oral contraceptive phases, or where a comparison was made between menstrual cycle and oral contraceptive groups. In this case, the male or amenorrhoeic group was not included in this review.
2.3 Data Extraction and Quality Assessment
The electronic searches were performed by one reviewer (BT). Titles and abstracts were assessed independently by two reviewers (BT and AA). Any disagreement about the inclusion of trials was resolved by consensus or a third reviewer (XJ) where necessary. Two reviewers (BT and AA) independently extracted data using a standardised data extraction form. Population characteristics, trial inclusion and exclusion criteria and intervention details were extracted together with baseline data and resistance training responses.
The methodological quality of the included articles was assessed with the McMaster University Guidelines and Critical Review Form for Quantitative Studies [17]. This assessment tool has previously been used in exercise and sport science systematic reviews [18] and was deemed the most appropriate as all articles used quantitative methods. Two reviewers (BT and AA) performed the assessment independently. Scores were compared and any disagreements were resolved by a third reviewer (XJ). A numerical scoring system devised in previous reviews was used to enable comparison across trials [19]. Scores from 7 to 9 were considered moderate quality and scores of 10 or more were considered good quality [18].
3 Results
3.1 Study Selection
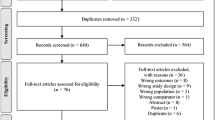
The initial database search produced a total of 2007 articles. After removing 353 duplicate articles, the remaining 1654 articles were screened, of which 23 were deemed potentially eligible based on title and abstract (Fig. 1). After a full-text review, six articles were excluded (Electronic Supplementary Material Table S2). A total of 17 studies remained for inclusion in the qualitative analysis. Due to the large variation in study design and outcomes, quantitative analysis was not deemed appropriate and, therefore, the results have been presented in a narrative form.

Flowchart showing screening process and search results
3.2 Methodological Quality
The critical appraisal scores for methodological quality ranged from 6 to 13 with a mean score of 10.5 out of a possible 15 points (Table 1). Overall the methodological quality was moderate to high with 11 of the 17 included studies scoring 10 or greater. Only one study scored below 7 and was considered to be of lesser quality. Although none of the studies were randomised controlled trials, 13 of the 17 included articles were deemed to have appropriate design for the study being reported. Sixteen of the included studies described the participant sample in detail; however, only two of these justified the sample size. One of the greatest areas of bias occurred in intervention where reporting on avoidance of co-intervention and contamination was inadequate in the majority of the studies.
3.3 Study Characteristics
The characteristics of the included studies are summarised in Table 2. The 17 studies examining the effect of the natural menstrual cycle or oral contraceptive cycle on resistance training responses included a total of 418 female participants with an age range of 18–38 years. The duration of each study spanned between one and four menstrual or oral contraceptive cycles. Studies examining acute resistance training responses investigated the effect of the menstrual cycle phase (n = 3), the effect of oral contraceptives compared with the menstrual cycle (n = 6), or the combined effects of the menstrual cycle phase and oral contraceptive phase (n = 1). Studies that examined responses to a training program investigated menstrual cycle phase-based resistance training (n = 3), menstrual cycle/oral contraceptive phase-based resistance training (n = 1), the effect of oral contraceptives compared with the menstrual cycle on strength development (n = 2), or the effect of anti-androgenic oral contraceptives compared with high androgenic oral contraceptives on strength development (n = 1).
Sixteen studies included participants who were not taking hormonal contraception and were experiencing a natural menstrual cycle. As potential effects of the menstrual cycle on resistance training responses are expected to be related to the secondary effects of female steroid hormone fluctuations, the measurement of estrogen and progesterone concentrations to confirm menstrual cycle phase is considered the gold standard for research purposes. Only five studies measured both estrogen and progesterone levels [20,21,22,23,24], while a further seven studies measured estrogen levels only [25,26,27,28,29,30,31]. Of the 11 studies which included participants who were taking oral contraceptives, 10 gave some information about the type of oral contraceptive taken by the participants, while one study did not include any information about the type of oral contraceptive used [28].
3.4 Reported Findings on the Effect of Menstrual Cycle Phase or Oral Contraceptives on Acute Resistance Training Responses
Ten studies examined the effect of menstrual cycle phase or oral contraceptives on responses to a single resistance training session. Two of these studies compared the response of anabolic hormones to a single resistance training session in the early follicular and mid-luteal phases in naturally menstruating females. These two high-quality studies observed a greater growth hormone response during the mid-luteal phase when compared with the early follicular phase [20, 21] and a greater androstenedione response in the mid-luteal phase compared with the early follicular phase [20]. No difference was reported between menstrual cycle phases for lactate, DHEAS, IGF-1, cortisol [21] or testosterone [20, 21]. One study examined whether estrogen receptor (ER) activation and subsequent effects on myogenic-related genes in response to eccentric exercise were different between the mid-follicular and mid-luteal phases [25]. This high-quality study reported skeletal muscle ER-α mRNA and protein expression, as well as skeletal muscle cyclin D1 mRNA expression to be greater during mid-follicular phase compared with the mid-luteal phase.
Six of the 10 studies compared acute responses between the menstrual cycle and oral contraceptive cycle. In a high-quality study, Kraemer et al. [32] observed a greater growth hormone response following a single heavy resistance training session in triphasic oral contraceptive users tested during the non-active pill phase compared to the early follicular phase of participants who were not taking oral contraceptives. Five studies compared exercise-induced muscle damage and recovery between participants using oral contraceptives and those who were not [26, 27, 29,30,31]. Of these, one high-quality study reported no difference in post-exercise creatine kinase (CK) between groups; however, a delayed recovery in the form of maximal isometric strength was observed for the participants who were taking oral contraceptives [31]. Minahan et al. [29], Roth et al. [30] and Hicks et al. [27] all reported significantly higher post-exercise levels of CK in the oral contraceptive groups compared with the naturally menstruating groups. Minahan et al. [29] also reported higher post-exercise levels of myoglobin and fatty acid-binding protein, and a greater decline in peak isometric strength in the oral contraceptive group. In contrast, Hayward et al. [26] reported significantly higher post-exercise levels of serum CK in participants who were not taking oral contraceptives compared with those who were.
To be able to compare findings of the five studies above, it is important to note differences in the timing of testing, as this will affect hormone concentrations. Three of these studies performed the eccentric exercise bout during the early follicular phase or non-active pill phase: on day 2 of menses for both the menstrual cycle and oral contraceptive groups [26], on days 2–6 of the menstrual cycle and oral contraceptive cycle [29] and on day 3 for the menstrual cycle group and days 3–6 for the oral contraceptive group [31]. One study performed the eccentric exercise mid-cycle on day 14 for both groups [27], while another study performed the eccentric exercise during the last week of the active pill for the oral contraceptive group (8–2 days prior to menses) and during menses for the menstrual cycle group (days 2–3) [30]. Therefore, both the endogenous and exogenous levels of hormones would have been very different between the various studies. In all five studies, estrogen was measured prior to the eccentric exercise bout and CK was measured daily for between 48 and 120 h after the eccentric exercise was performed. In four studies, endogenous estrogen at the time of testing was lower in the oral contraceptive group than the menstrual cycle group. One study reported higher levels of endogenous estrogen in the oral contraceptive group than the menstrual cycle group [26], and this study was also the only one to report higher post-exercise levels of CK in the menstrual cycle group. Therefore, four of the five studies reported a higher level of post-exercise CK when endogenous estrogen levels were lower at the time that the eccentric exercise was performed [26, 27, 29, 30] and one study found no significant difference [31].
One of the 10 studies combined menstrual cycle and oral contraceptive participants and randomly allocated them to follicular or luteal groups [28]. The follicular phase group was tested on day two or three of the follicular phase, while the luteal phase group was tested on day two or three of the luteal phase. The authors reported a greater decrement in strength and higher concentrations of CK in the luteal group (which included oral contraceptive users) in response to a single eccentric resistance training session.
3.5 Reported Findings on the Effect of the Menstrual Cycle or Oral Contraceptives on Chronic Adaptations in Response to a Resistance Training Program
Four of the included studies examined phase-based training, in which training is planned to coincide with hormonal phases. For example, follicular phase-based training has more sessions during the follicular phase than during the luteal phase. Three of these four studies investigated menstrual cycle phase-based training [22, 23, 33]. Reis et al. [22] compared regular training consisting of one resistance training session every third day over the entire cycle with phase-based training of equal total volume per menstrual cycle consisting of a resistance training session every second day in the follicular phase and one session per week in the luteal phase. The participants served as their own control by performing regular training on one leg and phase-based training on the other leg for two menstrual cycles (8 weeks). The authors confirmed menstrual cycle phases through hormone testing and reported higher strength adaptations by performing follicular phase-based training when compared to the regular training protocol [22]. Sung et al. [23] compared follicular phase-based training with luteal phase-based training over three menstrual cycles (12 weeks). The participants in this study also served as their own control by performing a higher volume of training on one leg in the follicular phase versus a higher volume of training on the other leg in the luteal phase. These authors also confirmed menstrual cycle phases with hormone testing and reported higher gains in muscle strength and muscle diameter in response to follicular phase-based training compared with luteal phase-based training [23]. Sakamaki-Sunaga et al. [33] also compared follicular phase-based training with luteal phase-based training over three menstrual cycles (12 weeks). Participants in this study served as their own control by exercising each arm separately, but this study did not use hormone testing to confirm menstrual cycle phases. In contrast to the above studies, no differences in muscle hypertrophy or strength between the training protocols were reported [33]. One study combined menstrual cycle and oral contraceptive cycle phase-based training over four menstrual cycles (16 weeks) [34]. The three groups were a follicular phase-based group, a luteal phase-based group, and a group that performed regular training as the control group. All three groups included a combination of oral contraceptive users and participants with a regular menstrual cycle, and no hormonal verification of the menstrual cycle phases was performed. Significant increases in lean mass were reported for follicular/early oral contraceptive cycle phase-based training compared with luteal/late oral contraceptive cycle phase-based or regular training, and significant gains in strength and power for follicular/early oral contraceptive cycle phase-based training compared with luteal/late oral contraceptive cycle phase-based training [34].
Three studies examined the effect of oral contraceptives on strength development. Nichols et al. [35] reported no significant difference in strength development between participants who used combined oral contraceptives and those who were not using hormonal contraceptives in response to a 12-week resistance training program. In the only study scoring low quality (Table 1), Ruzic et al. [36] reported significantly greater gains in muscle strength and lean mass in response to a 16-week resistance training program in participants who used a combined oral contraceptive compared with participants who used an oral contraceptive containing anti-androgens. Dalgaard et al. [24] reported a significant increase in type I muscle fibre area in response to a 10-week resistance training program in participants using a low-androgenic oral contraceptive, while participants with a natural menstrual cycle showed no significant increase. No differences in strength development were observed between the two groups; however, a trend towards a greater increase in muscle mass in oral contraceptive users was observed. Sub-analysis of the oral contraceptive group indicated that a greater increase in muscle mass occurred in participants taking an oral contraceptive containing 30 mg of ethinyl-estradiol, whereas the response in participants taking an oral contraceptive with only 20 mg ethinyl-estradiol did not differ from the natural menstrual cycle group.
4 Discussion
Many females participate in resistance training to improve athletic performance or for general health benefits. Previous research suggests that endogenous and exogenous female steroid hormones may affect resistance training outcomes. The aim of this systematic review was to investigate the effect of the menstrual cycle or oral contraceptives on resistance training responses. Only 17 studies met the inclusion criteria for this review. These studies addressed a range of different research questions, measured different responses to resistance training, and often reported conflicting results.
4.1 The Effect of Menstrual Cycle Phase or Oral Contraceptives on Acute Resistance Training Responses
Growth hormone response to a single resistance training session was greater in the mid-luteal phase when compared to the early follicular phase [20, 21], suggesting a more anabolic environment in the luteal phase. It should be noted, however, that these two studies only tested when estrogen and progesterone were low (early follicular phase) and when estrogen and progesterone were high (mid-luteal phase). It has been previously demonstrated that estrogen enhances circulating levels of growth hormone and that this estrogen-associated effect may be blunted by progesterone [37]. Furthermore, previous studies examining the effect of the menstrual cycle phase on growth hormone response following exercise on a bicycle ergometer reported a greater growth hormone response to exercise during the late follicular phase (high estrogen, low progesterone) when compared to the early follicular phase [38, 39]. It may be that the growth hormone response following resistance training is also greater in the late follicular phase than in either the early follicular or mid-luteal phases. Therefore, further research which compares the growth hormone response to a resistance training session should include testing in the late follicular phase when estrogen is high and progesterone is low. Testing at this additional time point may lead to a better understanding of the effect of the female sex hormones on acute anabolic hormone responses to resistance training.
Kraemer et al. [32] reported exercise-induced increase in growth hormone to be greater for triphasic oral contraceptive users compared with non-oral contraceptive users, suggesting that oral contraceptives may positively influence the physiological adaptations to resistance training. However, as previously demonstrated, growth hormone response to exercise is lower in the early follicular phase of the natural menstrual cycle compared with the mid-luteal [20, 21] and late follicular phases [38, 39]. Therefore, although the growth hormone response may be greater during the non-active triphasic oral contraceptive phase than in the early follicular menstrual cycle phase, it is not known whether a greater growth hormone response would be observed with triphasic oral contraceptive use during the active pill phases compared with the phases of the natural menstrual cycle. As the oral contraceptive group participants were only tested while taking the non-active pill, it can be assumed that the hormonal environment for this group would be very different had they been tested at different time points while they were taking the active hormonal pill. Further research that tests during the different menstrual cycle phases and while oral contraceptive users are taking the active hormonal pill is required to determine if the different hormonal environments result in different growth hormone responses to a resistance training session.
The five studies investigating the influence of oral contraceptive use compared with the natural menstrual cycle on exercise-induced muscle damage and recovery have provided varying results. One study reported no difference between the oral contraceptive group and menstrual cycle group in CK response [31], three reported a higher CK response in their oral contraceptive group [27, 29, 30], while one reported a lower CK response in the oral contraceptive group [26]. These conflicting findings may be due in part to the timing of the testing and the different hormonal environments between the studies. For example, in contrast to the other studies, Hayward et al. [26] reported a lower CK response in their oral contraceptive group. Hayward et al. [26] were also the only authors to find an unexpectedly higher endogenous estrogen concentration in the oral contraceptive group compared to the menstrual cycle group. These findings may be explained by the timing of their testing (day 2 of menses for both groups). Day 2 of menses in the menstrual cycle group is likely to be at the lowest point of endogenous estrogen. In the oral contraceptive group, however, withdrawal bleeding generally commences after 2–3 days of taking the non-active pills; therefore, it is possible that at day 2 of withdrawal bleeding, endogenous estrogen had increased in this oral contraceptive group without the suppressing effect of the exogenous hormones [40]. It is important to note that four of the five studies reported a higher level of post-exercise CK when endogenous estrogen levels were lower at the time that the eccentric exercise was performed [26, 27, 29, 30]. Therefore, it appears that endogenous estrogen may be protective against exercise-induced muscle damage. If this is the case, it could be speculated that endogenous estrogen may play a role in enhancing recovery from exercise-induced muscle damage. Two of the studies also reported a delayed recovery in the form of maximal strength for the oral contraceptive group [29, 31]. The protective role of estrogen against exercise-induced muscle damage is also supported by studies comparing males with females, with higher concentrations of markers of muscle damage reported in males [29].
Markofski et al. [28] examined the effect of the menstrual cycle phase on markers of exercise-induced muscle damage following a single session of high-volume eccentric exercise. However, eight of the eighteen participants were oral contraceptive users, who were divided evenly between the two groups. The problem with pooling oral contraceptive and menstrual cycle participants is that their hormonal environments are likely to be very different, especially in the luteal phase with high endogenous hormones for menstrual cycle participants and suppressed endogenous hormones for oral contraceptive participants. Combining these participants into one group will, therefore, not provide specific information regarding the effect of endogenous or exogenous hormones. In addition, two of the oral contraceptive participants who were in the luteal group dropped out, leaving an uneven number of oral contraceptive participants in the two groups. Furthermore, no information was provided about the type of oral contraceptive used and only serum estrogen was measured. In contrast to the above studies, these authors reported a higher CK response to exercise and a reduced strength recovery in the luteal phase when endogenous estrogen was higher at the time of the damaging exercise bout. However, as participants with a natural menstrual cycle and those taking oral contraceptives were pooled, it is difficult to draw conclusions regarding the effect of the menstrual cycle/oral contraceptive phase on exercise-induced muscle damage from this study. Further research that separates menstrual cycle and oral contraceptive participants into different groups based on their different hormonal environments is recommended.
Haines et al. [25] reported skeletal muscle ER-α mRNA and protein expression, as well as skeletal muscle cyclin D1 mRNA expression, to be greater during the mid-follicular phase compared with the mid-luteal phase following a single eccentric resistance training session. This was despite lower serum estrogen levels in the mid-follicular phase compared with the mid-luteal phase. ER-α is an important receptor for optimal contractile function of muscles [41], and activation of ER-α is thought to play a primary role in increasing satellite cell proliferation and activation following eccentric exercise [42]. In addition, cyclin D1 mRNA is also associated with the activation and proliferation of skeletal muscle satellite cells [43]. Therefore, the results of this study indicate an enhanced ability for skeletal muscle strength, growth and regeneration during the mid-follicular phase compared with the luteal phase.
4.2 The Effect of the Menstrual Cycle or Oral Contraceptives on Chronic Adaptations in Response to a Resistance Training Program
The theory that estrogen induces anabolic effects and progesterone induces catabolic effects on skeletal muscle suggests that timing training based on hormone concentrations may affect adaptations to resistance training. Phase-based training is, therefore, designed to vary training volume according to the phases of the menstrual cycle. Two studies examining phase-based training [22, 23] suggest that performing a higher volume of training in the follicular phase is superior to regular training or luteal phase-based training. In contrast to these findings, Sakamaki-Sunaga et al. [33] reported no differences in muscle hypertrophy or strength between follicular phase- and luteal phase-based training. However, the two studies that supported menstrual cycle phase-based training [22, 23] performed hormonal analysis to confirm that their participants were in the correct phase at the time of training. Hormonal analysis also ensures that participants are not included if they have anovulatory or luteal-deficient cycles, which are both characterised by lower follicular phase estrogen levels and reduced luteal phase progesterone levels [44]. There is a high prevalence of anovulation and luteal phase deficiency (30%) in physically active females, which often occurs in apparently normal cycles [45]. Therefore, it appears likely that Sakamaki-Sunaga et al. [33] who did not perform hormonal analysis on their physically active participants may have included participants who were not experiencing the expected hormonal fluctuations and/or may not have timed the phase-based training correctly. This would likely impact the results and may help explain the conflicting findings in the above studies. Furthermore, the participants in all three studies served as their own control by training their right and left limbs differently. However, it is not known whether the systemic release of anabolic hormones in response to each training session would have a confounding effect on the outcomes regardless of which limb is being trained.
Wikstrom-Frisen et al. [34] examined the effect of menstrual cycle/oral contraceptive cycle phase-based training on power, strength and lean body mass using three separate groups to avoid the problem of the systemic effect of anabolic hormones during training when participants serve as their own controls. However, both oral contraceptive and non-oral contraceptive users were blended within each group. As previously mentioned, the problem with combining participants who are using oral contraceptives with participants with a natural menstrual cycle is that the hormonal environment in each phase is likely to be very different within the one group, which may confound the results. When pooling the data from oral contraceptive and non-oral contraceptive users, significantly greater improvements in lean body mass, and peak torque of the quadriceps and hamstrings were found in favour of follicular phase-based training over luteal phase-based training. However, as no hormonal analysis was performed to confirm menstrual cycle phase, and as oral contraceptive users and those not taking hormonal contraception were pooled within each group, care should be taken when interpreting these findings.
Nichols et al. [35] compared female student athletes who were taking a combined oral contraceptive with those who were not taking any form of hormonal contraception. Following a 12-week resistance training program, there were no differences observed between groups for isokinetic torque production or repetition maximum strength gains, which suggests that oral contraceptive use does not positively or negatively influence strength gains. Information was provided on the types of progestin in the combined oral contraceptives used by the oral contraceptive group. It could be determined that some participants were taking a low-androgenicity pill, while others in the same group were using a high-androgenicity pill. Androgenicity (androgenic relative binding affinity) refers to the ability of the progestin in the oral contraceptive to produce masculine characteristics and is determined by the progestin type and dosage [3]. It has been proposed that the level of androgenicity in oral contraceptives may influence resistance training responses; however, only one of the included studies divided their oral contraceptive participants into groups according to the level of androgenicity. Ruzic et al. [36] reported a significantly greater gain in lean body mass together with a greater gain in muscle strength following a 16-week resistance training program in the participants who were taking an oral contraceptive with a higher level of androgenicity when compared to the participants who were using an anti-androgenic oral contraceptive. The authors concluded that the use of anti-androgenic oral contraceptives should be avoided in athletes where possible. A main limitation of this low-quality study was the absence of hormonal concentration measurements, which may have provided a deeper understanding of the mechanisms behind the androgen effect. Furthermore, as there was no menstrual cycle group in this study, it is not known whether participants taking a high androgenic oral contraceptive would demonstrate greater strength gains compared to participants who are not taking oral contraceptives. Dalgaard et al. [24] limited their oral contraceptive group to participants who were taking a low-androgenic oral contraceptive with either 20 or 30 mg ethinyl-estradiol. Although no differences in strength development over a 10-week training program were observed between the oral contraceptive and menstrual cycle groups, a significant increase in Type I muscle fibre area was only found in the oral contraceptive group. Furthermore, a trend towards a greater increase in muscle CSA in oral contraceptive users was found compared to the menstrual cycle group. Sub-analysis of the oral contraceptive group revealed that the participants taking 30 mg ethinyl-estradiol had greater gains in muscle mass than the menstrual cycle group and the participants in the oral contraceptive group who were only taking 20 mg ethinyl-estradiol. This suggests that the level of exogenous estrogen in oral contraceptives may influence resistance training adaptations and this warrants further investigation.
5 Conclusion
This systematic review highlights the lack of research examining the effect of endogenous female hormones and oral contraceptive use on resistance training outcomes. Most of the included studies reported some differences in outcomes between females with a natural menstrual cycle and females taking oral contraceptives, or between phases of the menstrual cycle. However, it is difficult to draw clear conclusions regarding the effect of female hormones on resistance training outcomes in women of reproductive age due to the many different study designs. Furthermore, small participant numbers, failure to measure estrogen and especially progesterone to confirm menstrual cycle phase, pooling of participants experiencing a natural menstrual cycle with those taking oral contraceptives, and combining different types of oral contraceptives often without considering androgenicity adds to the confusion surrounding female hormones and resistance training outcomes. To improve the quality of future menstrual cycle research, it is recommended to measure hormones to confirm that each participant has ovulated and that the correct phase is being measured. For further detail on methodological recommendations for menstrual cycle research, please refer to Janse de Jonge et al. [2].
Two studies provided evidence that higher endogenous estrogen concentrations result in a higher growth hormone response to exercise. A further four studies showed support for the protective role of endogenous estrogen against exercise-induced muscle damage. The effect of progesterone remains unclear. There is some evidence from moderate- to high-quality studies suggesting that follicular phase-based training is superior to both regular training and luteal phase-based training for developing strength and muscle mass in eumenorrheic participants. One further high-quality study demonstrated a greater potential for muscle strength and regeneration during the follicular phase when compared with the luteal phase. Together, these studies provide support for follicular phase-based training for enhancing resistance training outcomes in eumenorrheic females. Therefore, it is recommended that in their overall training plan, when possible, athletes with an ovulatory menstrual cycle aim to focus on resistance training during the follicular phase of the menstrual cycle.
As most of the studies examining the effects of oral contraceptive use on acute resistance training outcomes tested while the participants were not taking the active hormone pills, it remains unclear what effect the exogenous hormones administered during oral contraceptive consumption and the simultaneous suppression of endogenous hormones have on resistance training responses. Furthermore, only one study examined the effect of anti-androgenic oral contraceptives compared with high androgenic oral contraceptives and found greater gains in strength and lean mass in the high androgenic oral contraceptive group. One further study provided some evidence to support the role of exogenous estrogen in enhancing muscle gains in response to a resistance training program. The effect of the level of androgenicity as well as estrogen dosage in oral contraceptives, therefore, warrants further investigation. Future research including participants who are taking oral contraceptives should report the type of oral contraceptive used by the participants and should test during both the active hormone and non-active pill phases. This lack of clear resolution on the influence of exogenous hormones on resistance training responses contributes to the confusion females, and especially athletes, face when trying to make an educated decision on whether or not to use an oral contraceptive agent, and if so, which type. Further high-quality research on the potential effects of exogenous hormones on responses to resistance training is clearly needed before practical recommendations can be made.
Data Availability Statement
All data generated for this review are included in the manuscript and/or the supplementary files.
References
Hurley KS, Flippin KJ, Blom LC, Bolin JE, Hoover DL, Judge LW. Practices, perceived benefits, and barriers to resistance training among women enrolled in college. Int J Exerc Sci. 2018;11(5):226–38.
Janse de Jonge X, Thompson B, Han A. Methodological recommendations for menstrual cycle research in sports and exercise. Med Sci Sports Exerc. 2019. https://doi.org/10.1249/mss.0000000000002073(Epub ahead of print).
Burrows M, Peters CE. The influence of oral contraceptives on athletic performance in female athletes. Sports Med. 2007;37(7):557–74.
Schaumberg MA, Emmerton LM, Jenkins DG, Burton NW, Janse de Jonge XAK, Skinner TL. Use of oral contraceptives to manipulate menstruation in young, physically active women. Int J Sports Physiol Perform. 2018;13(1):82–7.
Dragoman MV. The combined oral contraceptive pill—recent developments, risks and benefits. Best Pract Res Clin Obstet Gynaecol. 2014;28(6):825–34.
Regidor PA. The clinical relevance of progestogens in hormonal contraception: present status and future developments. Oncotarget. 2018;9(77):34628–38.
Stewart M, Black K. Choosing a combined oral contraceptive pill. Aust Prescr. 2015;38(1):6–11.
Janse de Jonge XA. Effects of the menstrual cycle on exercise performance. Sports Med. 2003;33(11):833–51.
Kim YJ, Tamadon A, Park HT, Kim H, Ku SY. The role of sex steroid hormones in the pathophysiology and treatment of sarcopenia. Osteoporos Sarcopenia. 2016;2(3):140–55.
Lowe DA, Baltgalvis KA, Greising SM. Mechanisms behind estrogens’ beneficial effect on muscle strength in females. Exerc Sport Sci Rev. 2010;38(2):61–7.
Greising SM, Baltgalvis KA, Lowe DA, Warren GL. Hormone therapy and skeletal muscle strength: a meta-analysis. J Gerontol A Biol Sci Med Sci. 2009;64A(10):1071–81.
Kriengsinyos W, Wykes LJ, Goonewardene LA, Ball RO, Pencharz PB. Phase of menstrual cycle affects lysine requirement in healthy women. Am J Physiol Endocrinol Metab. 2004;287(3):E489–96.
Lariviere F, Moussalli R, Garrel DR. Increased leucine flux and leucine oxidation during the luteal phase of the menstrual cycle in women. Am J Physiol. 1994;267(3 Pt 1):E422–8.
Bailey SP, Zacher CM, Mittleman KD. Effect of menstrual cycle phase on carbohydrate supplementation during prolonged exercise to fatigue. J Appl Physiol. 2000;88(2):690–7.
Lamont LS, Lemon PW, Bruot BC. Menstrual cycle and exercise effects on protein catabolism. Med Sci Sports Exerc. 1987;19(2):106–10.
Oosthuyse T, Bosch AN. The effect of the menstrual cycle on exercise metabolism: implications for exercise performance in eumenorrhoeic women. Sports Med. 2010;40(3):207–27.
Law M, Stewart D, Pollock N, Letts L, Bosch J, Westmorland M. Guidelines for critical review of the literature: quantitative studies. Hamilton: McMasters University; 1998.
Pressick EL, Gray MA, Cole RL, Burkett BJ. A systematic review on research into the effectiveness of group-based sport and exercise programs designed for indigenous adults. J Sci Med Sport. 2016;19(9):726–32.
Anaf S, Sheppard LA. Physiotherapy as a clinical service in emergency departments: a narrative review. Physiotherapy. 2007;93(4):243–52.
Kraemer RR, Heleniak RJ, Tryniecki JL, Kraemer GR, Okazaki NJ, Castracane VD. Follicular and luteal phase hormonal responses to low-volume resistive exercise. Med Sci Sports Exerc. 1995;27(6):809–17.
Nakamura Y, Aizawa K, Imai T, Kono I, Mesaki N. Hormonal responses to resistance exercise during different menstrual cycle states. Med Sci Sports Exerc. 2011;43(6):967–73.
Reis E, Frick U, Schmidtbleicher D. Frequency variations of strength training sessions triggered by the phases of the menstrual cycle. Int J Sports Med. 1995;16(8):545–50.
Sung E, Han A, Hinrichs T, Vorgerd M, Manchado C, Platen P. Effects of follicular versus luteal phase-based strength training in young women. SpringerPlus. 2014;3:668.
Dalgaard LB, Dalgas U, Andersen JL, Rossen NB, Møller AB, Stødkilde-Jørgensen H, et al. Influence of oral contraceptive use on adaptations to resistance training. Front Physiol. 2019;10:824.
Haines M, McKinley-Barnard SK, Andre TL, Gann JJ, Hwang PS, Willoughby DS. Skeletal muscle estrogen receptor activation in response to eccentric exercise up-regulates myogenic-related gene expression independent of differing serum estradiol levels occurring during the human menstrual cycle. J Sports Sci Med. 2018;17(1):31–9.
Hayward R, Dennehy CA, Rodearmel SJ, Schneider CM. Serum creatine kinase, CK-MB, and perceived soreness following eccentric exercise in oral contraceptive users. Sports Med Train Rehabil. 1998;8(2):193–207.
Hicks K, Onambélé-Pearson G, Winwood K, Morse C, Hicks KM, Morse CI. Oral contraceptive pill use and the susceptibility to markers of exercise-induced muscle damage. Eur J Appl Physiol. 2017;117(7):1393–402.
Markofski MM, Braun WA. Influence of menstrual cycle on indices of contraction-induced muscle damage. J Strength Cond Res. 2014;28(9):2649–56.
Minahan C, Joyce S, Bulmer AC, Cronin N, Sabapathy S. The influence of estradiol on muscle damage and leg strength after intense eccentric exercise. Eur J Appl Physiol. 2015;115(7):1493–500.
Roth SM, Gajdosik R, Ruby BC. Effects of circulating estradiol on exercise-induced creatine kinase activity. J Exerc Physiol Online. 2001;4(2):10–7.
Savage KJ, Clarkson PM. Oral contraceptive use and exercise-induced muscle damage and recovery. Contraception. 2002;66(1):67–71.
Kraemer WJ, Nindl BC, Volek JS, Marx JO, Gotshalk LA, Bush JA, et al. Influence of oral contraceptive use on growth hormone in vivo bioactivity following resistance exercise: responses of molecular mass variants. Growth Horm IGF Res. 2008;18(3):238–44.
Sakamaki-Sunaga M, Min S, Kamemoto K, Okamoto T. Effects of menstrual phase-dependent resistance training frequency on muscular hypertrophy and strength. J Strength Cond Res. 2016;30(6):1727–34.
Wikstrom-Frisen L, Boraxbekk CJ, Henriksson-Larsen K. Effects on power, strength and lean body mass of menstrual/oral contraceptive cycle based resistance training. J Sports Med Phys Fitness. 2017;57(1–2):43–52.
Nichols AW, Hetzler RK, Villanueva RJ, Stickley CD, Kimura IF. Effects of combination oral contraceptives on strength development in women athletes. J Strength Cond Res. 2008;22(5):1625–32.
Ruzic L, Matkovic BR, Leko G. Antiandrogens in hormonal contraception limit muscle strength gain in strength training: comparison study. CMJ. 2003;44(1):65–8.
Faria AC, Bekenstein LW, Booth RA Jr, Vaccaro VA, Asplin CM, Veldhuis JD, et al. Pulsatile growth hormone release in normal women during the menstrual cycle. Clin Endocrinol. 1992;36(6):591–6.
Hansen AP, Weeke J. Fasting serum growth hormone levels and growth hormone responses to exercise during normal menstrual cycles and cycles of oral contraceptives. Scand J Clin Lab Invest. 1974;34(3):199–205.
Hornum M, Cooper DM, Brasel JA, Bueno A, Sietsema KE. Exercise-induced changes in circulating growth factors with cyclic variation in plasma estradiol in women. J Appl Physiol. 1997;82(6):1946–51.
Vandever MA, Kuehl TJ, Sulak PJ, Witt I, Coffee A, Wincek TJ, Reape KZ. Evaluation of pituitary-ovarian axis suppression with three oral contraceptive regimens. Contraception. 2008;77(3):162–70.
Collins BC, Mader TL, Cabelka CA, Iñigo MR, Spangenburg EE, Lowe DA. Deletion of estrogen receptor α in skeletal muscle results in impaired contractility in female mice. J Appl Physiol. 2018;124(4):980–92.
Thomas A, Bunyan K, Tiidus PM. Oestrogen receptor-alpha activation augments post-exercise myoblast proliferation. Acta Physiol. 2010;198(1):81–9.
Kadi F, Schjerling P, Andersen LL, Charifi N, Madsen JL, Christensen LR, et al. The effects of heavy resistance training and detraining on satellite cells in human skeletal muscles. J Physiol. 2004;558(Pt 3):1005–12.
De Souza MJ. Menstrual disturbances in athletes: a focus on luteal phase defects. Med Sci Sports Exerc. 2003;35(9):1553–63.
Schaumberg MA, Jenkins DG, Janse de Jonge XAK, Emmerton LM, Skinner TL. Three-step method for menstrual and oral contraceptive cycle verification. J Sci Med Sport. 2017;20(11):965–9.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This research was supported by an Australian Government Research Training Program (RTP) Scholarship.
Conflict of Interest
Belinda Thompson, Ashley Almarjawi, Dean Sculley and Xanne Janse de Jonge declare that they have no conflicts of interest relevant to the content of this review.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Thompson, B., Almarjawi, A., Sculley, D. et al. The Effect of the Menstrual Cycle and Oral Contraceptives on Acute Responses and Chronic Adaptations to Resistance Training: A Systematic Review of the Literature. Sports Med 50, 171–185 (2020). https://doi.org/10.1007/s40279-019-01219-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-019-01219-1