
Abstract
Background
Repetitive head impacts in young athletes are potentially detrimental to later life (e.g., age 50 + years) neurological function; however, it is unknown what the short-term effects (e.g., age 20 years) are in collegiate student-athletes.
Objective
The purpose of this study was to determine the effect of the estimated age of first exposure to American tackle football participation on neurocognitive performance and symptom severity scores in collegiate student-athletes.
Methods
We used a cohort study in which neurocognitive performance was assessed using the Immediate Post-Concussion Assessment and Cognitive Testing (ImPACT) test in 4376 male athletes (age 19.3 ± 1.5 years, mass 96.3 ± 20.3 kg, height 185.0 ± 7.4 cm). Athletes were grouped by sport participation [American football (n = 3462) or non-contact (n = 914)] and estimated age of first exposure [< 12 years (n = 3022) or ≥ 12 years (n = 1354)]. The outcome measures were the four primary cognitive scores and the symptom severity score from ImPACT. We assessed primary outcomes across groups, controlling for age, learning accommodations, and concussion history.
Results
Neurocognitive performance was not associated with the estimated age of first exposure-by-group interaction.
Conclusion
Our findings indicate that participation in American tackle football before age 12 years does not result in neurocognitive deficits in college. Therefore, we suggest the following: the consequences of early exposure to repetitive head impacts do not manifest by college, the ImPACT test was not sensitive enough to identify the effects of an earlier estimated age of first exposure, or there is no association between an earlier estimated age of first exposure and neurocognitive functioning. Future longitudinal studies are warranted.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
We defined the estimated age of first exposure (eAFE) as the participant’s age at the time of assessment minus the number of years the participant reported playing his primary sport. |
Neurocognitive performance was not associated with the eAFE-by-group interaction. |
Our findings indicate that participation in American tackle football before age 12 years does not result in neurocognitive deficits in college. |
We suggest the consequences of early exposure to repetitive head impacts do not manifest by college, the Immediate Post-Concussion Assessment and Cognitive Testing (ImPACT) test was not sensitive enough to identify the effects of earlier eAFE, or there is no association between earlier eAFE and neurocognitive functioning. |
1 Introduction
Nearly 5 million athletes participate in organized tackle football each year [1,2,3], and head impacts are an inherent risk in tackle football. While the acute effects of concussion have been identified [4], the long-term effects are still being elucidated [5]. More recently, there has been concern that exposure to repetitive head impacts, which do not result in clinically identifiable concussion, may also be associated with short- and long-term neurological impairments [6,7,8]. Exposure to repetitive head impacts in tackle football is frequent, ranging from hundreds to thousands depending on the position and level of play [1, 9,10,11,12,13]. For example, a defensive lineman who begins tackle football at age 10 years may experience up to 5000 head impacts by the end of high school and, should they continue to play in college, over 8000 head impacts by the end of college [14]. Montenigro et al. proposed that as few as 2723 head impacts have been associated with an increased risk of impaired later life executive function [14]. This suggests that by the end of high school, football players who begin playing before age 12 years may already have experienced enough head impacts to cause long-term neurological impairments.
The literature on the long-term consequences of repetitive head impact exposure is inconsistent, as evidenced by the controversy surrounding the etiology of chronic traumatic encephalopathy (CTE) [15]. Yet, some have suggested that CTE may be associated with exposure to repetitive head impacts, whereby the severity of CTE pathology increases with the level and duration of play [16]. Others, however, have suggested no association between football participation and later life neurodegenerative syndromes or suicidality [17,18,19]. Ultimately, a cause-and-effect relationship has not yet been demonstrated between CTE and sport-related concussions or exposure to contact sports [15]. As such, there is much to learn about the potential consequences of repetitive head-impact exposure and concussions, as well as other risk factors/modifying factors [i.e., genetic, environmental, age of first exposure (AFE)] [15]. For example, several studies have suggested that earlier AFE, that is, exposure to tackle football prior to age 12 years, may result in greater cognitive and neuropsychiatric impairments later in life [20,21,22,23], although these findings have been challenged [24]. Ages 10–12 are years of rapid brain growth and maturation, including increased myelination and cerebral blood flow [25,26,27,28,29,30], and some have speculated that repetitive head impacts during this critical period of neurodevelopment may have both short- and long-term consequences [20,21,22,23]. However, studies examining AFE have been limited to later life, long-term outcomes across small sample sizes, and to a single institution. These findings may not be generalizable to all football players as they largely included former National Football League players and lack a control group to examine the effects of early exposure to repetitive head impacts compared to early exposure to sport participation more broadly.
To understand the manifestation or progression of the later life neurological impairments associated with exposure to repetitive head impacts, particularly with respect to tackle football during critical stages of neurodevelopment (i.e., ages 10–12 years) [25,26,27,28,29,30], we must assess neurological function across varying levels of sport participation and throughout the lifespan. Considering that, by the end of high school, football players may already have experienced enough head impacts to cause long-term neurological impairments, it is feasible that athletes exposed to tackle football participation before age 12 years (AFE < 12) have observable neurocognitive impairments in college relative to those with AFE ≥ age 12 years (AFE ≥ 12). Because neurodevelopment does not taper off toward adult levels until about age 20 years [26,27,28,29,30,31], observable neurocognitive impairments in college may inhibit cognitive tasks, such as planning, integrative information, abstract thinking, problem solving, judgment, and reasoning that develop during later stages of adolescent neurodevelopment [31]. Therefore, we aimed to determine the effects of estimated AFE (eAFE) to sport participation (i.e., eAFE < 12 vs. eAFE ≥ 12), the effects of collision-sport participation (i.e., football vs. control), and the interaction of eAFE-by-sport (i.e., eAFE < 12, football vs. eAFE ≥ 12, football vs. eAFE < 12, non-contact vs. eAFE ≥ 12, non-contact) on Immediate Post-Concussion Assessment and Cognitive Testing (ImPACT) composite scores in National Collegiate Athletic Association (NCAA) collegiate athletes. We defined eAFE as the participant’s age at the time of assessment minus the number of years the participant reported playing his primary sport. Although the predictive validity and diagnostic accuracy of the ImPACT test have been questioned, the ImPACT test is still the most widely used neurocognitive assessment by athletic trainers and physicians in sport-related concussion evaluation [32,33,34,35]. We hypothesized that ImPACT scores would be worse among those athletes exposed to tackle football participation before age 12 years (eAFE < 12).
2 Methods
This study was part of the NCAA-Department of Defense Concussion Assessment, Research and Education (CARE) Consortium, an ongoing study on the effects of concussion in collegiate athletes and US military service academy members that began in Autumn 2014 and has enrolled over 37,000 student-athletes and military service academy students across 30 colleges/universities [36]. We only used the baseline ImPACT test (used at 25 colleges/universities) and demographic information, collected as part of ‘Level A’ testing in this study. Because some athletes participated in the CARE Consortium study during more than one season, only the first season’s baseline data were included in analyses.
2.1 Participants
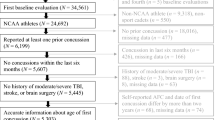
Participants included current NCAA collegiate athletes (n = 4376, age 19.3 ± 1.5 years, mass 96.3 ± 20.3 kg, height 185.0 ± 7.4 cm) that met inclusion/exclusion criteria and were enrolled in the CARE Consortium between June 2014 and August 2018. Inclusion criteria for the experimental group were male football players while the control group consisted of non-contact sport athletes (i.e., baseball, cross country/track, fencing, field events, gymnastics, volleyball, golf, rifle, rowing/crew, sailing, swimming, and tennis) [37]. Exclusion criteria included female athletes and non-contact sport athletes with a history of collision/contact sport participation (i.e., basketball, diving, field hockey, football, ice hockey, lacrosse, martial arts, rugby, soccer, water polo, and wrestling), or non-contact sport athletes who were also US military service academy members, as they may experience repetitive head impacts because of their military training (Fig. 1) [37,38,39,40,41]. The University of Michigan Institutional Review Board, the US Army Medical Research and Materiel Command Human Research Protection Office, as well as the local institutional review board at each of the performance sites reviewed all study procedures. Participants provided written informed consent prior to participation. The study was performed in accordance with the standards of ethics outlined in the Declaration of Helsinki.

Inclusion/exclusion sequence
2.2 Estimated Age of First Exposure
We defined the eAFE as the participant’s age at the time of assessment minus the number of years the participant reported playing his primary sport. The eAFE was used to divide participants into two cohorts: eAFE < 12 and eAFE ≥ 12 [20,21,22,23]. Of the 5136 participants who potentially met inclusion/exclusion criteria, 714 did not provide enough information to calculate eAFE, or provided inaccurate information (Fig. 1). The minimum eAFE for this study was 5 years as this is the youngest age for Pop Warner football and any participant indicating eAFE prior to age 5 years was excluded.
2.3 Outcome Measures
The ImPACT (ImPACT Applications Inc., Pittsburgh, PA, USA) is a computerized neurocognitive assessment designed specifically for the assessment and management of sport-related concussions and tests attention, memory, reaction time, and information-processing speed [42]. It consists of eight modules: immediate and delayed word recall, immediate and delayed design recall, a symbol-match test, a three-letter recall, the X’s and O’s test, and a color-match test. From these eight modules, five composite scores are calculated: visual memory, verbal memory, visual motor speed, and reaction time, and impulse control. The impulse control composite score is used to determine if the participant provided a good effort (impulse control < 30) [42]. Finally, the ImPACT test provides the Post-Concussion Symptom Scale (PCSS), which is a 22-item self-report, symptom checklist, including common concussion symptoms such as headache, dizziness, nausea, difficulty concentrating, and fatigue. The PCSS yields a total symptom severity composite score ranging from 0 to 132 [42]. The reliability and validity of the ImPACT test have been assessed in the literature [34, 43,44,45,46,47,48,49,50,51,52,53,54,55,56,57]. Despite limitations, including a susceptibility to false-positives in concussion assessment, poorer scores with group testing, a learning effect with repeated administration, and moderate-to-low test–retest reliability [33, 34, 46, 58], the cognitive domains represented by ImPACT have good construct validity with standard paper and pencil neurocognitive tests that are sensitive to cognitive functions associated with sport-related concussion [52, 53]. For example, the ImPACT Visual Memory composite score was correlated (r = 0.590, p < 0.001) with the Brief Visuospatial Memory Test-Revised, a neuropsychological test of visual memory [53]. Moreover, the ImPACT test is the most widely used neurocognitive assessment by athletic trainers and physicians in sport-related concussion evaluation [32,33,34,35]. The five ImPACT composite scores used as outcome measures in this study include visual memory, verbal memory, visual motor speed, reaction time, and symptom severity. Only participants with valid baseline ImPACT composite scores were included in the database.
2.4 Statistical Analysis
Generalized linear modeling was used for the prediction of each cognitive domain score and the symptom severity score. Predictor variables were entered in the following order: a dichotomous variable for the group (football vs. non-contact), a dichotomous variable for the eAFE (eAFE < 12 vs. eAFE ≥ 12), an interaction term, group-by-eAFE, and covariates for learning accommodation status, number of previous concussions, and age [24]. The self-reported learning accommodation status, i.e., Individualized Education Program, 504 Plan (i.e., a plan developed to ensure that a child who has a disability identified under the law and is attending an elementary or secondary educational institution receives accommodations that will ensure their academic success and access to the learning environment), or other learning accommodations, was input as a dichotomous variable, and the number of previous concussions and age were input as continuous variables (Table 1). We initially fitted generalized linear models for each cognitive domain score based on a normal (Gaussian) distribution and identity link functions but then considered models with alternative distributions and link functions and selected the model with the lowest Akaike information criterion value (i.e., best fit). Reaction time scores were positively skewed; an inverse Gaussian distribution with a power link function best fit these data. For the symptom score, which has a high zero count and extreme positive skewing, a negative binomial distribution with a log link achieved the lowest Akaike information criterion value. Significance was defined a priori as p < 0.05. All analyses were conducted using SPSS Version 24 (IBM, Armonk, NY, USA).
3 Results
There were 4376 male athletes included in the final analysis (Table 1). One participant had an outlier (more than three standard deviations from the mean) for reaction time and was removed from analyses. The results of the generalized linear modeling for each ImPACT score are presented in Table 2.
In these models, the interaction term, group-by-eAFE, was only a significant predictor of symptom severity scores; pairwise comparisons suggested that football, eAFE < 12 interaction reported lower severity scores than all other groups (non-contact, eAFE < 12: mean difference = − 0.97, p < 0.001, Cohen’s d = 0.11; non-contact, eAFE ≥ 12: mean difference = − 0.92, p < 0.001, Cohen’s d = 0.11; football, eAFE ≥ 12: mean difference = − 0.56, p < 0.001, Cohen’s d = 0.08), and that football, eAFE ≥ 12 interaction reported lower symptom severity scores than non-contact, eAFE < 12 (mean difference = − 0.41, p < 0.044, Cohen’s d = 0.02). Considering the small effect sizes, these findings suggest that outcomes did not differ across groups.
The main effect for the group was only a significant predictor of visual motor speed (mean difference = − 1.25, p < 0.001, Cohen’s d = 0.13) and reaction time (mean difference = 0.02 s, p < 0.001, Cohen’s d = 0.18), whereby football participants had lower visual motor speed and slower reaction time than non-contact participants, but considering the small effect sizes, these findings are likely of minimal clinical significance. Finally, the few but small significant eAFE differences among participants in verbal memory (mean difference = 0.40, p = 0.049, Cohen’s d = 0.08), visual motor speed (mean difference = 0.29, p = 0.026, Cohen’s d = 0.07), and symptom severity score (mean difference = 0.29, p < 0.001, Cohen’s d = 0.07) are likely of minimal clinical significance, though they suggest that eAFE < 12 has higher verbal memory and visual motor speed and lower symptom severity than eAFE ≥ 12.
4 Discussion
Some studies have reported that repetitive head impacts in young athletes may potentially be detrimental to later life neurological function; however, it is unknown what the short-term effects (e.g., at age 20 years) are in collegiate student-athletes [20,21,22,23]. Our goal was to determine the effect of the eAFE to repetitive head impacts on neurocognitive performance and symptom severity scores in football and non-contact collegiate student-athletes. Our findings suggest that participation in tackle football before age 12 years, when evaluated by the ImPACT test, did not result in neurocognitive deficits in college. Participation in tackle football before age 12 years did, however, result in lower (better) symptom severity scores than all other groups (i.e., non-contact, eAFE < 12; non-contact, eAFE > 12; football, eAFE > 12), although the differences between groups were within the established reliable change index (10), and had small effect sizes, suggesting that these findings are not clinically meaningful [59]. While we did observe lower (worse) visual motor speed and slower (worse) reaction time in football participants than non-contact participants, regardless of eAFE, these differences had small effect sizes and were within the established reliable change indices (visual motor speed = 3; reaction time = 0.06 s) [59]. We also observed higher (better) verbal memory and visual motor speed and lower (better) symptom severity in participants, both football and non-contact, who participated in sport before age 12 years, but again these differences were within the established reliable change indices (verbal memory = 9; visual motor speed = 3; symptom severity = 10) and had small effect sizes [59]. Finally, learning disabilities and previous concussion history were significant covariates in the model suggesting that they were modifiers for the neurocognitive test outcomes. Taken together, these findings suggest that we identified several statistically significant differences in sport and eAFE in a large cohort of collegiate student-athletes, but these findings are likely of minimal clinical significance.
We hypothesized that ImPACT composite scores would be worse among those athletes exposed to tackle football participation before age 12 years (eAFE < 12). However, this hypothesis was not supported; there was no significant eAFE-by-sport interaction suggesting that early participation in football did not result in neurocognitive performance deficits in our population of current collegiate student-athletes. When compared to normative data for the ImPACT test, both football and non-contact athletes had “average” composite scores for sex and age across all domains [37, 60]. Studies by Stamm et al. and Alosco et al. reported differences between AFE < 12 and AFE ≥ 12 in later life (i.e., largely over 50 years) cognitive function (i.e., the Wisconsin Card Sort Test, the Neuropsychological Assessment Battery List Learning test, and the Wide Range Achievement Test, Fourth Edition performance), white matter microstructure, neuropsychiatric outcomes, thalamic volumes, and age of neurobehavioral symptom onset in retired professional and amateur football players, whereby those athletes who participated in tackle football prior to age 12 years had greater neurological impairments and a younger age of neurobehavioral symptom onset [20,21,22,23, 61], although younger AFE to tackle football was not associated with CTE pathological severity [61].
Our studies differed from those by Stamm et al. in several key areas—our cohorts were different: the average age of our participants was 19 years, including college freshmen through seniors, who played tackle football for an average of 10 years, and were apparently healthy; whereas, their cohort included retired athletes, who were largely aged over 50 years, reported an average of 19 years of participation in tackle football, and reported a worsening of cognitive, behavioral, and mood symptoms for at least the previous 6 months [20,21,22,23]. Although we did not observe differences between football, eAFE < 12 and football, eAFE ≥ 12 in neurocognitive performance, it is possible that symptoms of early exposure to repetitive head impacts will not manifest until later in life. For example, the neuroprotective effect of exercise is well documented, and aerobic exercise training is associated with modest improvements in attention and processing speed, executive function, and memory [62]. Perhaps throughout college, when student-athletes are young and still actively participating in sport, they have sufficient cognitive reserves or compensatory neurocognitive capabilities to adapt and overcome potential degradation. However, as athletes age and become less active, they may no longer able to compensate and only then present with neurological impairments. In addition, it is possible that symptoms of neurological impairment will progress with increased exposure to repetitive head impacts (e.g., throughout college and professional play). For example, Montenigro et al. suggested that beyond 2723 head impacts, there is a worsening dose–response relationship between the number of head impacts and neurological impairments [14]. We expect that many participants captured in this study were just beyond a cumulative repetitive head impact exposure of 3000 impacts [14]. If we were to capture all participants at the end of their college career or beyond collegiate play, perhaps these findings may differ.
Our findings agree with Solomon and colleagues who reported no correlations between pre-high school years of exposure to tackle football and neurological outcomes across three domains of neuroradiological, neurobehavioral, and neuropsychological testing, including the ImPACT test, in retired National Football League players [24]. Like our findings, their ImPACT composite scores were not related to pre-high school years of exposure to tackle football. While there are known limitations to the ImPACT test, Solomon et al. also reported no statistically significant relationship between paper-and-pencil neurocognitive test scores and pre-high school years of exposure to tackle football. Unlike the studies by Stamm and colleagues, Solomon et al. did not recruit exclusively former National Football League players who were experiencing a worsening of cognitive, behavioral, and mood symptoms. In addition, Solomon et al. used multiple regression models with “number of years of pre-high school football” utilized as the predictor variable, as opposed to a cut-off age [24]. The cut-off age was selected by Stamm and colleagues because ages 10–12 are years of rapid brain growth and maturation, including increased myelination and cerebral blood flow [25,26,27,28,29,30], and some have speculated that repetitive head impacts during this critical period of neurodevelopment may have both short- and long-term consequences [20,21,22,23].
Our findings, taken with those of Solomon et al. do not support the presence of a relationship between AFE to tackle football and neurological impairments in samples of apparently healthy current and former football players, but do not rule out the possibility that a relationship may present in those former athletes who later experience a worsening of cognitive, behavioral, and mood symptoms [20,21,22,23]. Thus, prospective longitudinal studies are required to more thoroughly investigate the effects of repetitive head impacts on neurological health [36].
Although time allocated to academic study sometimes shows a corresponding reduction in sport participation, sport participation during youth results in better grade point averages and cognitive function, and positive influences on concentration, memory, and classroom behavior [63]. It would be conceivable then that participation in sport, football or non-contact, would positively affect neurocognitive performance during these critical neurodevelopmental phases through high school and college. There was an effect for eAFE, whereby athletes, both football and non-contact, who participated in sport before age 12 years, had higher (better) verbal memory, visual motor speed, and lower (better) symptom severity scores. However, these differences also had small effect sizes and were within the reliable change indices, suggesting that these findings are not clinically meaningful.
We observed that participation in tackle football before age 12 years, when evaluated by the ImPACT test, did not result in neurocognitive deficits in collegiate student-athletes. Though this is not a study of “retired” athletes, such as those conducted by Solomon et al., Stamm et al., and Alosco et al., and thus we cannot discern the effect of long-term neurocognitive impairment later in life, these results lend empirical evidence to the notion that AFE is not associated with neurocognitive functioning. However, to gain a more comprehensive understanding of the manifestation and progression of long-term neurological impairments in former football players, future research should prospectively examine neuroradiological, neurobehavioral, and neuropsychological tests across varying levels of sport participation and across the lifespan.
4.1 Limitations
We addressed some methodological limitations of previous studies. For example, Stamm and colleagues were critiqued for a small homogenous sample, lack of a control group of participants from non-contact sports, an abnormally high total number of concussions, and use of inappropriate neurocognitive tests [64]. However, we used the ImPACT test and PCSS as the only outcome measures. The ImPACT test and PCSS have been components of sport-related concussion assessment and are recommended as core assessments in the recent National Institutes of Health/National Institute of Neurological Disorders and Stroke Sports Concussion Common Data Elements [65]. Further, the ImPACT test was created to assess neurocognitive function following sport-related concussion when cognitive function demonstrates the largest impairment (i.e., relative to repetitive head impacts and throughout recovery following sport-related concussion) [66]; therefore, perhaps it is not sensitive enough to identify more subtle deficits. Incorporating more sensitive measures of neuroradiological, neurobehavioral, and neuropsychological testing may result in a more comprehensive approach.
We also do not know the previous number of times each athlete has taken the ImPACT test, and with the known learning effect of the ImPACT test, this may confound results. Like prior studies, eAFE was based on self-reporting in which athletes were asked to report the number of years of participation in their primary sport. While there are numerous limitations with self-reporting, these data are essential to behavioral and medical research [67].
In the current study, exposure to repetitive head impacts was delimited to tackle football, but athletes in other sports, such as ice hockey, soccer, and lacrosse, may also experience repetitive head impacts at a young age, but the current findings may not extend to those populations. Moreover, repetitive head impacts were not directly assessed; thus, future research should not only consider AFE, but also the number and magnitude of impacts experienced throughout the lifespan.
Finally, we did not account for group or eAFE differences in socioeconomic status or the age of the first concussion. The socioeconomic status and race of student-athletes has independently predicted baseline ImPACT scores, when concussion history and years exposed to sport were not predictive [68]. The age at which an individual has his or her first concussion may be associated with the age at which an individual begins playing sports and may be an important factor in determining long-lasting cognitive effects [69]. Therefore, future studies should incorporate measures of socioeconomic status and demographic variables, and age of first concussion in addition to eAFE.
5 Conclusion
In summary, we found no statistically significant or clinically important association between eAFE < 12 in American football and neurocognitive performance in collegiate student-athletes after analyzing ImPACT data in a large cohort of NCAA student-athletes. Therefore, we suggest the following: the consequences of early exposure to repetitive head impacts do not manifest until later in life, symptoms of neurological impairment progress with increased exposure to repetitive head impacts throughout and beyond collegiate play, the ImPACT test was not sensitive enough to identify the effects of earlier eAFE, or there is no association between earlier eAFE and neurocognitive functioning. Ultimately, these athletes must be followed for years after college sport participation to determine future manifestation and progression of neurological disruption.
References
Daniel RW, Rowson S, Duma SM. Head impact exposure in youth football. Ann Biomed Eng. 2012;40(4):976–81.
Powell JW, Barber-Foss KD. Traumatic brain injury in high school athletes. JAMA. 1999;282(10):958–63.
Guskiewicz KM, Weaver NL, Padua DA, Garrett WE. Epidemiology of concussion in collegiate and high school football players. Am J Sports Med. 2000;28(5):643–50.
McCrea M, Guskiewicz KM, Marshall SW, Barr W, Randolph C, Cantu RC, et al. Acute effects and recovery time following concussion in collegiate football players: the NCAA Concussion Study. JAMA. 2003;290(19):2556–63.
Manley GT, Gardner AJ, Schneider KJ, Guskiewicz KM, Bailes J, Cantu RC, et al. A systematic review of potential long-term effects of sport-related concussion. Br J Sports Med. 2017;51(12):969–77.
Bailes JE, Petraglia AL, Omalu BI, Nauman E, Talavage T. Role of subconcussion in repetitive mild traumatic brain injury: a review. J Neurosurg. 2013;119(5):1235–45.
Belanger HG, Vanderploeg RD, McAllister T. Subconcussive blows to the head: a formative review of short-term clinical outcomes. J Head Trauma Rehabil. 2016;31(3):159–66.
Erlanger DM. Exposure to sub-concussive head injury in boxing and other sports. Brain Inj. 2015;29(2):171–4.
Broglio SP, Eckner JT, Martini D, Sosnoff JJ, Kutcher JS, Randolph C. Cumulative head impact burden in high school football. J Neurotrauma. 2011;28(10):2069–78.
Cobb BR, Urban JE, Davenport EM, Rowson S, Duma SM, Maldjian JA, et al. Head impact exposure in youth football: elementary school ages 9–12 years and the effect of practice structure. Ann Biomed Eng. 2013;41(12):2463–73.
Mihalik JP, Bell DR, Marshall SW, Guskiewicz KM. Measurement of head impacts in collegiate football players: a investigation of positional and event-type differences. Neurosurgery. 2007;61(6):1229–35.
Crisco JJ, Wilcox BJ, Beckwith JG, Chu JJ, Duhaime A, Rowson S, et al. Head impact exposure in collegiate football players. J Biomech. 2011;44(15):2673–8.
Crisco JJ, Fiore R, Beckwith JG, Chu JJ, Brolinson PG, Duma S, et al. Frequency and location of head impact exposures in individual collegiate football players. J Athl Train. 2010;45(6):549–59.
Montenigro PH, Alosco ML, Martin BM, Daneshvar DH, Mez J, Chaisson CE, et al. Cumulative head impact exposure predicts later-life depression, apathy, executive dysfunction, and cognitive impairment in former high school and college football players. J Neurotrauma. 2017;34(2):328–40.
McCrory P, Meeuwisse W, Dvorak J, Aubry M, Bailes J, Broglio S, et al. Consensus statement on concussion in sport: the 5th International Conference on Concussion in Sport held in Berlin, October 2016. Br J Sports Med. 2017;51:838–47.
Mez J, Daneshvar DH, Kiernan PT, Abdolmohammadi B, Alvarez VE, Huber BR, et al. Clinicopathological evaluation of chronic traumatic encephalopathy in players of American football. JAMA. 2017;318(4):360–70.
Lehman EJ, Hein MJ, Gersic CM. Suicide mortality among retired national football league players who played 5 or more seasons. Am J Sports Med. 2016;44(10):2486–91.
Janssen PH, Mandrekar J, Mielke MM, Ahlskog JE, Boeve BF, Josephs K, et al. High school football and late-life risk of neurodegenerative syndromes, 1956–1970. Mayo Clin Proc. 2017;92(1):66–71.
Kuhn AW, Zuckerman SL, Solomon GS, Casson IR, Viano DC. Interrelationships among neuroimaging biomarkers, neuropsychological test data, and symptom reporting in a cohort of retired national football league players. Sports Health. 2017;9(1):30–40.
Stamm JM, Koerte IK, Muehlmann M, Pasternak O, Bourlas AP, Baugh CM, et al. Age at first exposure to football is associated with altered corpus callosum white matter microstructure in former professional football players. J Neurotrauma. 2015;32(22):1768–76.
Schultz V, Stern RA, Tripodis Y, Stamm JM, Wrobel P, Lepage C, et al. Age at first exposure to repetitive head impacts is associated with smaller thalamic volumes in former professional American football players. J Neurotrauma. 2017;35(2):278–85.
Stamm JM, Bourlas AP, Baugh CM, Fritts NG, Daneshvar DH, Martin BM, et al. Age of first exposure to football and later-life cognitive impairment in former NFL players. Neurology. 2015;84(11):1114–20.
Alosco ML, Kasimis AB, Stamm JM, Chua AS, Baugh CM, Daneshvar DH, et al. Age of first exposure to American football and long-term neuropsychiatric and cognitive outcomes. Transl Psychiatry. 2017;7(9):e1236.
Solomon GS, Kuhn AW, Zuckerman SL, Casson IR, Viano DC, Lovell MR, et al. Participation in pre-high school football and neurological, neuroradiological, and neuropsychological findings in later life: a study of 45 retired National Football League players. Am J Sports Med. 2016;44(5):1106–15.
Epstein HT. Stages of increased cerebral blood flow accompany stages of rapid brain growth. Brain Dev. 1999;21(8):535–9.
Giedd JN, Blumenthal J, Jeffries NO, Castellanos FX, Liu H, Zijdenbos A, et al. Brain development during childhood and adolescence: a longitudinal MRI study. Nat Neurosci. 1999;2(10):861–3.
Lebel C, Walker L, Leemans A, Phillips L, Beaulieu C. Microstructural maturation of the human brain from childhood to adulthood. Neuroimage. 2008;40(3):1044–55.
Uematsu A, Matsui M, Tanaka C, Takahashi T, Noguchi K, Suzuki M, et al. Developmental trajectories of amygdala and hippocampus from infancy to early adulthood in healthy individuals. PLoS One. 2012;7(10):e46970.
Chugani HT, Phelps ME, Mazziotta JC. Positron emission tomography study of human brain functional development. Ann Neurol. 1987;22(4):487–97.
Shaw P, Greenstein D, Lerch J, Clasen L, Lenroot R, Gogtay N, et al. Intellectual ability and cortical development in children and adolescents. Nature. 2006;440(7084):676–9.
Zeigler DW, Wang CC, Yoast RA, Dickinson BD, McCaffree MA, Robinowitz CB, et al. The neurocognitive effects of alcohol on adolescents and college students. Prev Med. 2005;40(1):23–32.
Kelly KC, Jordan EM, Joyner AB, Burdette GT, Buckley TA. National collegiate athletic association division I athletic trainers’ concussion-management practice patterns. J Ath Train. 2014;49(5):665–73.
Alsalaheen B, Stockdale K, Pechumer D, Broglio SP. Validity of the Immediate Post Concussion Assessment and Cognitive Testing (ImPACT). Sports Med. 2016;46(10):1487–501.
Broglio SP, Katz BP, Zhao S, McCrea M, McAllister T, CARE Consortium Investigators. Test–retest reliability and interpretation of common concussion assessment tools: findings from the NCAA-DoD CARE consortium. Sports Med. 2017;48(5):1255–68.
Buckley TA, Burdette G, Kelly K. Concussion-management practice patterns of national collegiate athletic association division II and III athletic trainers: how the other half lives. J Athl Train. 2015;50(8):879–88.
Broglio SP, McCrea M, McAllister T, Harezlak J, Katz B, Hack D, et al. A national study on the effects of concussion in collegiate athletes and US military service academy members: the NCAA-DoD Concussion Assessment, Research and Education (CARE) Consortium structure and methods. Sports Med. 2017;47(7):1437–51.
Katz BP, Kudela M, Harezlak J, McCrea M, McAllister T, Broglio SP, CARE Consortium Investigators. Baseline performance of NCAA athletes on a concussion assessment battery: a report from the CARE consortium. Sports Med. 2018;48(8):1971–85.
Catenaccio E, Caccese J, Wakschlag N, Fleysher R, Kim N, Kim M, et al. Validation and calibration of HeadCount, a self-report measure for quantifying heading exposure in soccer players. Res Sports Med. 2016;24(4):416–25.
Caccese JB, Lamond LC, Buckley TA, Kaminski TW. Reducing purposeful headers from goal kicks and punts may reduce cumulative exposure to head acceleration. Res Sports Med. 2016;24(4):407–15.
Caccese JB, Kaminski TW. Minimizing head acceleration in soccer: a review of the literature. Sports Med. 2016;46(11):1591–604.
Caccese JB, Kaminski TW. Neurocognitive changes in men’s and women’s soccer players across a collegiate career. In: Favero T, Drust B, Dawson B, editors. International research in science and soccer II. New York: Routledge; 2015. p. 133–44.
Lovell M. ImPACT 2007 (6.0) clinical interpretation manual. Pittsburgh: ImPACT Applications; 2007.
Bruce J, Echemendia R, Meeuwisse W, Comper P, Sisco A. 1 year test–retest reliability of ImPACT in professional ice hockey players. Clin Neuropsychol. 2014;28(1):14–25.
Elbin RJ, Schatz P, Covassin T. One-year test–retest reliability of the online version of ImPACT in high school athletes. Am J Sports Med. 2011;39(11):2319–24.
Iverson GL, Lovell MR, Collins MW. Validity of ImPACT for measuring processing speed following sports-related concussion. J Clin Exp Neuropsychol. 2005;27(6):683–9.
Resch J, Driscoll A, McCaffrey N, Brown C, Ferrara MS, Macciocchi S, et al. ImPact test–retest reliability: reliably unreliable? J Athl Train. 2013;48(4):506–11.
Schatz P, Sandel N. Sensitivity and specificity of the online version of ImPACT in high school and collegiate athletes. Am J Sports Med. 2013;41(2):321–6.
Schatz P, Pardini JE, Lovell MR, Collins MW, Podell K. Sensitivity and specificity of the ImPACT test battery for concussion in athletes. Arch Clin Neuropsychol. 2006;21(1):91–9.
Schatz P, Ferris CS. One-month test–retest reliability of the ImPACT test battery. Arch Clin Neuropsychol. 2013;28(5):499–504.
Schatz P. Long-term test–retest reliability of baseline cognitive assessments using ImPACT. Am J Sports Med. 2010;38(1):47–53.
Nakayama Y, Covassin T, Schatz P, Nogle S, Kovan J. Examination of the test–retest reliability of a computerized neurocognitive test battery. Am J Sports Med. 2014;42(8):2000–5.
Maerlender A, Flashman L, Kessler A, Kumbhani S, Greenwald R, Tosteson T, et al. Discriminant construct validity of ImPACT™: a companion study. Clin Neuropsychol. 2013;27(2):290–9.
Maerlender A, Flashman L, Kessler A, Kumbhani S, Greenwald R, Tosteson T, et al. Examination of the construct validity of ImPACT™ computerized test, traditional, and experimental neuropsychological measures. Clin Neuropsychol. 2010;24(8):1309–25.
Lau BC, Collins MW, Lovell MR. Sensitivity and specificity of subacute computerized neurocognitive testing and symptom evaluation in predicting outcomes after sports-related concussion. Am J Sports Med. 2011;39(6):1209–16.
Broglio SP, Macciocchi SN, Ferrara MS. Sensitivity of the concussion assessment battery. Neurosurgery. 2007;60(6):1050–8.
Allen BJ, Gfeller JD. The immediate post-concussion assessment and cognitive testing battery and traditional neuropsychological measures: a construct and concurrent validity study. Brain Inj. 2011;25(2):179–91.
Broglio SP, Ferrara MS, Macciocchi SN, Baumgartner TA, Elliott R. Test–retest reliability of computerized concussion assessment programs. J Athl Train. 2007;42(4):509–14.
Erdal K. Neuropsychological testing for sports-related concussion: how athletes can sandbag their baseline testing without detection. Arch Clin Neuropsychol. 2012;27(5):473–9.
Iverson GL, Lovell MR, Collins MW. Interpreting change on ImPACT following sport concussion. Clin Neuropsychol. 2003;17(4):460–7.
Iverson GL, Lovell MR, Collins MW. Immediate post-concussion assessment and cognitive testing (ImPACT) normative data. University of British Columbia and Riverview Hospital; 2003. https://www.impacttest.com/ArticlesPage_images/Articles_Docs/7ImPACTNormativeDataversion%202.pdf. Accessed 2 Jan 2018.
Alosco ML, Mez J, Tripodis Y, Kiernan PT, Abdolmohammadi B, Murphy L, et al. Age of first exposure to tackle football and chronic traumatic encephalopathy. Ann Neurol. 2018;83:886–901.
Smith PJ, Blumenthal JA, Hoffman BM, Cooper H, Strauman TA, Welsh-Bohmer K, et al. Aerobic exercise and neurocognitive performance: a meta-analytic review of randomized controlled trials. Psychosom Med. 2010;72(3):239–52.
Trudeau F, Shephard RJ. Physical education, school physical activity, school sports and academic performance. Int J Behav Nutr Phys Act. 2008;5(1):10.
Maroon JC, Bailes J, Collins M, Lovell M, Mathyssek C, Andrikopoulos J, et al. Age of first exposure to football and later-life cognitive impairment in former NFL players. Neurology. 2015;85(11):1007–10.
Broglio SP, Kontos AP, Levin H, Schneider K, Wilde EA, Cantu RC, et al. The National Institute of Neurological Disorders and Stroke and Department of Defense Sport-Related Concussion Common Data Elements Version 1.0 recommendations. J Neurotrauma. 2018;35(23):2776–83.
Martini DN, Broglio SP. Long-term effects of sport concussion on cognitive and motor performance: a review. Int J Psychophysiol. 2018;132(Pt A):25–30.
Stone AA, Bachrach CA, Jobe JB, Kurtzman HS, Cain VS. The science of self-report: implications for research and practice. London: Psychology Press; 1999.
Houck Z, Asken B, Clugston J, Perlstein W, Bauer R. Socioeconomic status and race outperform concussion history and sport participation in predicting collegiate athlete baseline neurocognitive scores. J Int Neuropsychol Soc. 2018;24(1):1–10.
Taylor KM, Kioumourtzoglou MA, Clover J, Coull BA, Dennerlein JT, Bellinger DC, Weisskopf MG. Concussion history and cognitive function in a large cohort of adolescent athletes. Am J Sports Med. 2018;46(13):3262–70.
Acknowledgements
Contributing CARE Consortium Investigators include: April Marie (Reed) Hoy, MS, ATC (Azusa Pacific University); Joseph B. Hazzard Jr, EdD, ATC (Bloomsburg University); Louise A. Kelly, PhD (California Lutheran University); Justus D. Ortega, PhD (Humboldt State University); Nicholas Port, PhD (Indiana University); Margot Putukian MD (Princeton University); T. Dianne Langford, PhD (Temple University); Holly J. Benjamin MD (University of Chicago); James R. Clugston, MD, MS (University of Florida); Julianne D. Schmidt, PhD, ATC (University of Georgia); Luis A. Feigenbaum, DPT, ATC (University of Miami); James T. Eckner, MD, MS (University of Michigan); Jason P. Mihalik, PhD, CAT(C), ATC (University of North Carolina at Chapel Hill); Jessica Dysart Miles, PhD, ATC (University of North Georgia); Scott Anderson, ATC (University of Oklahoma); Christina L. Master, MD (University of Pennsylvania); Micky Collins, PhD, and Anthony P. Kontos, PhD (University of Pittsburgh Medical Center); Sara P.O. Chrisman, MD, MPH (University of Washington); Alison Brooks, MD, MPH (University of Wisconsin-Madison); Jonathan Jackson, MD, and Gerald McGinty, DPT (United States Air Force Academy); Kenneth Cameron, PhD, MPH, ATC (United States Military Academy); Adam Susmarski, MD (United States Naval Academy); Stefan Duma, PhD and Steve Rowson, PhD (Virginia Tech); Christopher M. Miles, MD (Wake Forest University); Brian H. Dykhuizen, MS, ATC (Wilmington College); Laura Lintner DO (Winston-Salem University). The authors also thank the research and medical staff at each of the participating sites.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Funding
This publication was made possible, in part, with support from the Grand Alliance CARE Consortium, funded by the National Collegiate Athletic Association and the Department of Defence. The United States Army Medical Research Acquisition Activity, Ford Detrick, MD, USA is the awarding and administering acquisition office. This work was supported by the Office of the Assistant Secretary of Defense for Health Affairs through the Psychological Health and Traumatic Brain Injury Program under Award No. W81XWH-14-2-0151. Opinions, interpretations, conclusions, and recommendations are those of the authors and are not necessarily endorsed by the Department of Defense (Defense Health Program funds).
Conflict of interest
Beyond the research grant received, in part for this work (described under funding), Jaclyn B. Caccese, Ryan M. DeWolf, Thomas W. Kaminski, Steven P. Broglio, Thomas W. McAllister, Michael McCrea, and Thomas A. Buckley have no conflicts of interest that are directly relevant to the content of this study.
Ethics approval
The study was performed in accordance with the standards of ethics outlined in the Declaration of Helsinki. All study procedures were reviewed by the University of Michigan Institutional Review Board, the US Army Medical Research and Materiel Command Human Research Protection Office, as well as the local institutional review board at each of the performance sites.
Consent to participate
Participants provided written informed consent prior to participation.
Data availability
The CARE Consortium datasets generated and analyzed during the current study will be available in the Federal Interagency Traumatic Brain Injury Research repository (https://fitbir.nih.gov/) by the end of 2019.
Additional information
This article is part of a Topical Collection on The NCAA-DoD Concussion Assessment, Research and Education (CARE) Consortium.
The members of the ‘CARE Consortium Investigators’ are listed in the Acknowledgements section.
Rights and permissions
About this article

Cite this article
Caccese, J.B., DeWolf, R.M., Kaminski, T.W. et al. Estimated Age of First Exposure to American Football and Neurocognitive Performance Amongst NCAA Male Student-Athletes: A Cohort Study. Sports Med 49, 477–487 (2019). https://doi.org/10.1007/s40279-019-01069-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-019-01069-x