
Abstract
Background
Several studies have examined the effects of balance training in elderly individuals following total knee arthroplasty (TKA), although findings appear to be equivocal.
Objectives
This systematic review and meta-analysis examined the effects of balance training on walking capacity, balance-specific performance and other functional outcome measures in elderly individuals following TKA.
Methods
Data sources: Pubmed, PEDro, Cinahl, SportDiscus, Scopus. Eligibility criteria: Data were aggregated following the population-intervention-comparison-outcome (PICO) principles. Eligibility criteria included: (1) randomised controlled trials; (2) studies with comparative groups; (3) training interventions were incorporated post-TKA; and (4) outcome measures included walking capacity, balance-specific performance measures, subjective measures of physical function and pain and knee range-of-motion. Participants: Elderly individuals (65 + years) who underwent total knee arthroplasty. Interventions: Balance interventions that consisted of balance exercises, which were compared to control interventions that did not involve balance exercises, or to a lesser extent. Participants also undertook usual physiotherapy care in conjunction with either the balance and/or control intervention. The intervention duration ranged from 4 to 32 weeks with outcome measures reported immediately following the intervention. Of these, four studies also reported follow-up measures ranging from 6 to 12 months post-interventions. Study appraisal: PEDro scale.
Synthesis methods
Quantitative analysis was conducted by generating forest plots to report on standardised mean differences (SMD; i.e. effect size), test statistics for statistical significance (i.e. Z values) and inter-trial heterogeneity by inspecting I2. A meta-regression was also conducted to determine whether training duration predicted the magnitude of SMD.
Results
Balance training exhibited significantly greater improvement in walking capacity (SMD = 0.57; Z = 6.30; P < 0.001; I2 = 35%), balance-specific performance measures (SMD = 1.19; Z = 7.33; P < 0.001; I2 = 0%) and subjective measures of physical function (SMD = 0.46; Z = 4.19; P < 0.001; I2 = 0%) compared to conventional training immediately post-intervention. However, there were no differences in subjective measures of pain (SMD = 0.77; Z = 1.63; P > 0.05; I2 = 95%) and knee range-of-motion (SMD = 0.05; Z = 0.39; P > 0.05; I2 = 1%) between interventions. At the 6- to 12-month follow-up period, improvement in combined measures of walking capacity and balance performance (SMD = 041; Z = 3.55; P < 0.001; I2 = 0%) were significantly greater for balance training compared to conventional training, although no differences were observed for subjective measures of physical function and pain (SMD = 0.26; Z = 2.09; P > 0.05; I2 = 0%). Finally, the training duration significantly predicted subjective measures of pain and physical function (r2 = 0.85; standardised β = 0.92; P < 0.001), although this was not observed for walking capacity and balance-specific performance measures (r2 = 0.02; standardised β = 0.13; P = 0.48).
Limitations
A number of outcome measures indicated high inter-trial heterogeneity and only articles published in English were included.
Conclusion
Balance training improved walking capacity, balance-specific performance and functional outcome measures for elderly individuals following TKA. These findings may improve clinical decision-making for appropriate post-TKA exercise prescription to minimise falls risks and optimise physical function.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Knee osteoarthritis is the most common orthopaedic condition in developed countries and is the leading cause of functional impairment in the elderly population. |
Whilst elderly individuals typically undergo total knee arthroplasty to treat knee osteoarthritis, they are still at an increased risk of impaired physical function and fall compared to their healthy age-matched counterparts. |
Greater improvements in walking capacity and balance-specific performance measures are observed following rehabilitation programmes that have a greater emphasis on balance training when compared to conventional methods of rehabilitation. |
Balance training improves subjective measures of physical function and range-of-motion to a greater extent than conventional methods of rehabilitation. |
At 6- to 12-month follow-up, greater improvements are shown following balance training compared to conventional rehabilitation for combined measures of walking capacity and balance-specific performance measures. |
1 Introduction
Knee osteoarthritis is the most common type of arthritis and the leading cause of functional impairment among older adults in the developed world [1]. The common treatment of this condition is total knee arthroplasty (TKA) to reduce pain and stiffness, increase joint range of motion and improve overall physical function [2]. However, individuals following TKA experience greater postural sway, possibly due to reduced muscular strength and proprioception [3]. For example, it was reported that patients following TKA exhibited an average 80% more centre of pressure velocity in anteroposterior and lateral sway compared to controls [4]. Such physical limitations render difficulty in undertaking activities of daily living, compromise walking capacity and increase the risks of falls in patients following TKA compared to their healthy, age-matched counterparts [5]. Furthermore, falling in older individuals following TKA may result in fear and avoidance of movement, serious injuries or even mortality [6] and places considerable financial burden on the healthcare system [7]. Subsequently, interventions that minimise the risks of fall by improving walking capacity and balance are crucial determinants of post-TKA rehabilitation success.
Traditionally, post-TKA interventions consisted of more conventional exercises (e.g. range-of-motion, stretching, strengthening and endurance exercises). These interventions have shown minimal benefits in terms of pain and function [8,9,10]. However, recent studies have incorporated exercises that challenged the sensory systems for balance and have shown to improve balance-specific outcomes (e.g. walking capacity, single-leg stance time) [11,12,13,14]. These studies compared groups that completed several weeks of balance exercises (BLN group) against a control (CON) group that undertook exercises with no particular emphasis on training the sensory systems for balance following TKA [11,12,13,14,15,16]. Other studies have incorporated balance exercises in both BLN and CON groups, but with the BLN group having greater emphasis on training the balance sensory systems by incorporating a greater range of balance exercises [17, 18], or with greater volume of balance training [19]. Overall, the results demonstrate that post-TKA rehabilitation programmes consisting of balance exercises, or those with greater emphasis on training the balance sensory systems, improve balance-specific outcomes. Whilst these findings have important clinical implications for developing effective post-TKA rehabilitation programmes, there were substantial discrepancies in the methodological design, making global interpretations difficult. The major disparity in the methodological design identified included the type of outcome measures, statistical design and the timing of assessments relative to the duration of training intervention. Subsequently, a systematic exploration of the literature is warranted to address differences in the methodological approach used by previous studies to investigate the benefits of balance training following TKA.
A recent systematic review [20] investigated the effect of balance training on balance performance measures in individuals following TKA. The results demonstrated that a range of rehabilitation protocols were utilised to improve proprioception, postural control, balance and coordination, with reports qualitatively indicating improvement in functional ability and balance when compared to controls. Whilst these findings may provide insight on the usability of balance training for individuals post-TKA, the results were not examined via meta-analytical methods, which neither enables statistical comparisons nor critically evaluates comparable studies with limited interpretation of quantitative data. Furthermore, given that studies that have incorporated balance training prior to TKA with those following TKA were combined [20], it is difficult to ascertain, with confidence, whether balance training is beneficial specifically for post-TKA rehabilitation. The purpose of the current review was therefore twofold. First, to systematically and critically evaluate studies that have examined balance training during post-TKA rehabilitation. Second, to determine whether post-TKA balance training improves walking capacity, balance-specific performance and other functional outcome measures compared to programmes with exercises with no balance exercises, or those with a lesser emphasis on balance exercises in patients following TKA.
2 Methods
The methodology and reporting of data in this systematic review and meta-analysis were conducted in accordance with the PRISMA guidelines [21] and followed a population, intervention/exposure, comparison and outcome (PICO) approach.
2.1 Inclusion/Exclusion Criteria
Studies were considered eligible and included into this review that met the following PICO criteria:
-
1.
Population Elderly individuals (65 + years) who had undergone TKA due to osteoarthritis.
-
2.
Intervention or exposure Randomised controlled trials (RCTs) and pilot RCTs examining the effect of balance training implemented following TKA. Training interventions were considered to include balance exercises based on description from included studies, or when referred to training interventions as “sensori-motor training” as described by Taube et al. [22]. When such classification was not given by authors, then these were defined as “balance exercises” as they appeared to challenge the primary sensory systems for balance (i.e. visual, vestibule and/or prioprioceptive) [23], or to restore neuromuscular function and motor efficiency, as explained by Taube et al. [22]. In addition, the balance training interventions were either classified as static/dynamic steady-state (maintaining steady position during standing or walking), proactive balance (anticipating a predetermined perturbation) and/or reactive balance (re-establishing balance from an unpredicted perturbation), depending on the nature of the exercises.
-
3.
Comparison Groups were compared between those that undertook balance training in conjunction with conventional rehabilitative training versus those that completed conventional rehabilitative training only, or groups were compared between those that undertook balance training only versus those that completed conventional rehabilitative training only.
-
4.
Outcomes Outcome measures included balance-specific performance measures, walking capacity measures, agility performance, muscular function and/or subjective measures of physical function and pain (further description on outcome measures are outlined under Outcome Measures, Sect. 2.2 below).
Studies were excluded if: (1) no comparative group was incorporated; (2) they combined patients with various orthopaedic procedures, such as TKA and total hip arthroplasty; (3) exercises were included as pre-surgical interventions; (4) they were published in a non-English language; and (5) they were reported as abstracts, reviews or case reports.
2.2 Outcome Measures
The primary outcome measures for the current review were walking capacity and balance-specific performance measures as these parameters have been reported as strong predictors for future falls [24] and are commonly utilised to assess falls risks amongst the elderly population [25]. Measures of walking capacity may include protocols with walking time-trial of a given distance (e.g. 6-min walk test, timed up-and-go [TUG] test) and/or gait speed by dividing the distance by the time taken to completion. Balance-specific performance measures may consist of assessments that measure stance time (e.g. single-leg stance or standing on unstable surfaces), chair sit-to-stand (CSTS) time and/or standing reach distance. These balance-specific protocols have been identified as effective falls risk screening instruments in the elderly population (65 + years) [26,27,28]. Similar to the training intervention methods mentioned earlier, both walking capacity and balance-specific performance measures were either classified as static/dynamic steady-state, proactive balance and/or reactive balance. Knee range-of-motion (ROM) and subjective scores of physical function and pain level are commonly reported to assess the success of post-TKA rehabilitation and have been associated with balance ability [29]. The subjective measures of physical function are derived from questionnaires [e.g. Wester Ontario and McMaster Universities Osteoarthritis Index (WOMAC) or the Knee Injury and Osteoarthritis Outcome Score (KOOS)] that determine the difficulty of undertaking activities of daily living (e.g. ascending/descending stairs, picking objects from floors, going shopping, etc.). However, these measures were reported as secondary outcomes as these assessments are not typically administered specifically for falls risk, but rather for overall functional assessment [30]. Outcome measures were extracted from included studies when reported immediately after the balance interventions and control interventions and at 6- to 12-month follow-up.
2.3 Search Strategy
A literature search was performed on 1 June 2018 across five major electronic data bases (Medline, Cinahl, PEDro, Scopus and SportDiscus) appropriate for rehabilitation and orthopaedics. A supplementary search was also conducted by screening the reference lists of included studies. For the Medline search, four groupings of mesh terms were utilised in combination: (1) humans; (2) orthopaedic condition (osteoarthritis, knee OR arthroplasty, replacement, knee OR knee/pathology OR knee/surgery OR knee/therapy); (3) Interventions (physical therapy modalities OR exercise therapy); and (4) outcome measures (postural balance OR proprioception). Free text search was also conducted in Medline during the last year (January 2016-current) for studies that were ‘in press’, with the following: osteoarthrit* OR arthroplasty OR replacement) and (knee) and (exercise OR therapy OR vibration) and (postural OR balance OR propriocep*). Equivalent free text search was also conducted on Scopus during the last 10 years. For the Pedro search, the advanced function was used with the combination of the following text: arthrop*, replacement, fitness testing, lower leg or knee and clinical trial.
2.4 Selection Process
Two independent reviewers (AG and JM), with expert knowledge in orthopaedics and exercise, undertook the stepwise computed literature search. Firstly, all abstracts that met the inclusion criteria were classified as either meeting the criteria (i.e. ‘yes’), possibly meeting the criteria (i.e. ‘maybe’) or not meeting the criteria (i.e. ‘no’). Following screening of the abstract list, a random sample (40%) of these abstracts was examined to establish the inter-rater reliability between both reviewers. According to the Weighted Kappa statistic, a value of 0.82 (95% confidence interval: 0.75–0.89) was obtained, which was considered acceptable for inter-rater reliability [31]. Upon completion of the abstract screening process, corresponding full text articles were retrieved and further screened based on the inclusion/exclusion criteria.
2.5 Data Extraction, Quality Assessment and Risk of Bias
Following completion of full text screening, a customised form was utlilised to extract information regarding study design, participant details (e.g. age, height, weight, BMI, length of hospital stay, etc.), study aims, methodological design (e.g. intervention type, study duration, performance type, timing of performance assessment, etc.) and main findings. The results of pre- and post-intervention values of each group [i.e. BLN group and CON group] were then entered into Excel as mean ± standard deviation. Patients were considered as part of the BLN group if they undertook exercises that challenged their primary sensory systems for balance (e.g. walking over obstacles, stair walking, step-ups, vibration platforms, etc.). Contrarily, CON groups consisted of patients who either did not complete balance exercises (e.g. range-of-motion exercises and resistance exercises whilst seated only), or undertook balance exercises but with a substantially lesser emphasis than the BLN group. The data on the methodological quality of each included study was screened using the PEDro scale and pooled into a table with overall scores reported as a median. This critical appraisal tool assesses internal validity of each trial [32]. The quality ratings were interpreted as follows: 9–11 (excellent); 6–8 (good); 4–5 (fair); and < 4 (poor) [32]. Reporting bias was minimised by use of strict inclusion/exclusion criteria and acceptable agreement between reviewers during abstract screening and consensus of full-text screening. Publication bias was assessed via inspection of funnel plots generated from Reviewer Manager Software 5 (RevMan, Version 5.3, Copenhagen: The Nordic Cochrane Centre, 2014), which are simple scatter plots with the studies’ mean differences plotted on the x-axis and standard error on the y-axis [33]. Participant selection bias was inevitable in the current review given that participants following TKA were selectively included. However, this selection process was essential to align the conceptual approach to the purpose of the current review.
2.6 Statistical Methods
In the current systematic review, a meta-analysis was conducted using Reviewer Manager Software 5. All data from included studies were reported as mean ± standard deviation, and central tendencies originally reported as standard errors or confidence intervals were converted to standard deviations [34]. The heterogeneity among samples of included studies was assessed based on I2 statistic tests in conjunction with level of statistical significance. For I2 interpretation, values of 25, 50 and 75% were classified as low, moderate and high, respectively, with inspection of associated P-values for level of statistical significance [35]. The comparison of training intervention effect between BLN and CON groups were analysed according to the post-intervention data, or where accessible, the rate of pre-post improvement (i.e. mean differences or percentage change). Corresponding authors were also contacted where data were not available, and when retrieved, data were included into this review. Data pooling of the outcome measures was completed and reported via forest plots using a random effects model to account for between-trial heterogeneity. The magnitude of between-group differences (i.e. BLN vs. CON groups) was calculated based on standardised mean differences (i.e. effect size), with values of 0.2, 0.5 and 0.8 classified as small, medium and large, respectively [36]. The overall effect of between-group comparisons is reported as a Z-value derived from the forest plot, which is a test statistic resulting from the statistical test to determine the P value. The effect of the balance interventions was interpreted based on standardised mean differences and statistical significance between BLN and CON. All overall effect values were reported from the forest plot, although specific measures were reported separately if it involved three or more effect points. A sensitivity analysis was also performed on the following outcomes: walking capacity, balance performance, range-of-motion and subjective measures of physical function and pain to determine the impact of study quality on the effects of balance exercise interventions in patients following TKA. To determine the sensitivity of the measures, the primary meta-analysis was repeated, excluding studies that demonstrated a PEDro score of less than 8. Furthermore, a meta-regression was conducted to determine whether the effects of balance training on physical performance measures (i.e. walking capacity and balance-specific performance) and subjective measures (i.e. physical function and pain) were moderated by training duration reported in weeks using the Statistical Package of Social Sciences (SPSS, v25, IBM Corp., Armonk, NY, USA). If studies reported training duration as a range, the mid-point of this duration was utilised. For example, if a study reported a training duration of 6–8 weeks, then the predictor variable for this measure was included as 7 weeks. The alpha level was set at 0.05 for all analyses.
3 Results
3.1 Systematic Literature Search
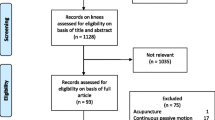
A total of 4253 abstracts were screened following removal of abstracts (n = 412) based on the inclusion criteria from Medline, PEDro and Scopus databases (Fig. 1). After review of abstracts, 4148 abstracts were excluded, which resulted in 105 remaining full-text articles. Consequently, these full-text articles were further screened with 12 original articles included for evaluation. All included studies consisted of a BLN training group and a CON training group.

Flowchart of the search strategy according to the PRISMA guidelines
3.2 Participants
Based on the 12 included studies, a total of 740 participants were analysed, of which 373 and 367 participants were included in the BLN and CON groups, respectively. The mean range for age and BMI of participants for the BLN group were between 64–75 years and 28.0–33.3 kg·m2, respectively, and between 66–73 years and 28.3–34.2 kg·m2, respectively, for the CON group, indicating that the physical characteristics were relatively evenly distributed between groups (Table 1). Furthermore, the majority of studies compared baseline outcome measures between BLN and CON groups. No significant between-group differences (P > 0.05) were observed in baseline measures, providing further support of homogeneity in all outcome measures for both groups.
3.3 Methodological Descriptions
With respect to the method of exercise implementation, five studies incorporated balance training intervention as an additional component of the rehabilitation programme for BLN groups with identical conventional rehabilitation programmes completed by both the BLN and CON groups [11, 15, 16, 18, 19] (Table 2). Conversely, seven studies incorporated training interventions for the CON group, which were separate to and were not undertaken by the BLN group [12,13,14, 17, 37,38,39]. Participants in each study also undertook usual physiotherapy care in conjunction with either the balance and/or control intervention. All included studies reported progression of exercise for both groups with training frequencies ranging from two sessions/week to three sessions/day, with longer durations (~ 60–90 min) typically having fewer training frequencies compared to those with shorter durations (~ 5–10 min). Most participants commenced their rehabilitation programme within 6 weeks following TKA, except for one study where the intervention was initiated 32 weeks post-TKA [11]. All included studies reported outcome measures immediately following the balance and conventional interventions, and of these, four studies also reported follow-up measures ranging from 6 to 12 months post-interventions. Amongst the studies that reported follow-up measures, two studies [13, 16] had patients continue with their rehabilitation programme under unsupervised conditions during the follow-up period, one study [37] reported that patients did not continue their rehabilitative activities (i.e. passive) and one study [12] did not report patient’s activities during follow-up. For the primary outcome measures, walking capacity was reported in the form of 2- and 6-min walk tests (6MWT) [12, 17, 37, 39], gait speed [11, 13, 16, 39] and TUG [11, 12, 14, 15, 19]. Balance-specific parameters were reported as Berg Balance Scale (BBS) test [18, 19], single-leg stand time on the operated leg with eyes open (SLSTKR-EO) [11, 15] and eyes closed (SLSTKR-EC) [11, 15], single-leg stance time on the non-operated leg with eyes open (SLSNon-TKR-EO) [11, 15] and eyes closed (SLSNon-TKR-EC) [11, 15], reach distance [11, 19] and CSTS times [11, 15, 16, 39]. For the secondary outcome measures, subjective scores of physical function [11, 12, 16,17,18, 39] and pain [11,12,13,14, 16,17,18, 38] and knee range of motion of the operated leg [12,13,14, 17] were reported.
3.4 Methodological Quality
The PEDro scores for included studies ranged from good to excellent quality (Table 3). All included studies consisted of the following: eligibility criteria; randomisation of participants into BLN and CON groups; standardisation of baseline values; outcome measures reported from more than 85% of participants initially allocated to groups; similar treatment of data irrespective of group allocation; and analyses for between-group comparisons. A double-blinded approach was utilised by six studies (i.e. blinding of assessors and participants) and a single-blinded approach by four studies (i.e. blinding of assessors), although none of the studies blinded the therapists who supervised the exercise sessions and only three studies concealed participant allocation.
3.5 Quantitative Analyses
For the walking capacity and balance-specific performance analyses, a total of 32 effect points were incorporated from 11 studies. According to the overall between-group comparison, significantly greater improvement in walking capacity measures was observed for the BLN group compared to the CON group (SMD = 0.57; Z = 6.8; P < 0.01; Fig. 2) with low inter-study heterogeneity (I2 = 30%; P = 0.13). Furthermore, significantly greater improvement in 6-min walk test (SMD = 0.35; Z = 2.61; P < 0.01), gait speed (SMD = 0.50; Z = 3.77; P < 0.01) and TUG (SMD = 0.70; Z = 4.53; P < 0.01) were found for the BLN group compared to the CON group, all with low inter-study heterogeneity (I2 = 0–41%; P > 0.05). According to the overall between-group comparisons, a significant improvement was shown for balance-specific performance measures (SMD = 1.19; Z = 6.48; P < 0.01; Fig. 3). Whilst only two effect points were reported for BBS, SLSTKR-EC, SLSNon-TKR-EC, SLSNon-TKR-EO and thus sub-totals are not reported, significantly greater improvement was found with the BLN compared to the CON group for reach distance (SMD = 1.48; Z = 3.53; P < 0.01). However, differences in CSTS were not significant between the BLN and CON groups (SMD = 0.45; Z = 1.81; P = 0.07). Large inter-study heterogeneity was noted for the overall effect (I2 = 90%), reach distance (I2 = 87%) and CSTS (I2 = 80%). Based on visual inspection, the funnel plot was relatively symmetrical and evenly distributed for the walking capacity measures (Online resource 1), the follow-up walking capacity and balance measures (Online resource 2) and follow-up subjective measures (Online resource 3). However, the funnel plot for the balance-performance (Online resource 4) and secondary outcome measures (i.e. subjective measures of pain, physical function and ROM; Online resource 5) appeared deviated.

Forest plot of the walking capacity measures with standardised (Std.) mean differences and associated 95% confidence intervals (CI). 6MWT 6-min walk test, 2MWT 2-min walk test, TUG timed up and go

Forest plot of the balance measures with standardised (Std.) mean differences and associated 95% confidence intervals (CI). BBS Berg Balance Scale, SLS TKR EO single leg stance time for limb with total knee replacement with eyes open, SLS TKR EC single leg stance time for limb with total knee replacement with eyes closed, SLS Non-TR EO Single leg stance time for limb without total knee replacement with eyes open, SLS Non-TR EC Single leg stance time for limb without total knee replacement with eyes closed, RD reach distance, RD-Ratio Reach distance as a ratio to limb length, TCS timed chair stands
According to the forest plot of the secondary outcome measures, a total of 21 effect points were incorporated from nine studies. Using standardised mean differences (Fig. 4), subjective measures of function exhibited significantly greater improvement for the BLN group compared to the CON group (Z = 4.19; P < 0.01), with low inter-study heterogeneity (I2 = 0%; P > 0.05). However, no differences were noted for subjective measures of pain (Z = 1.63; P = 0.10) with high inter-study heterogeneity (I2 = 95%; P < 0.01) and for ROM (Z = 0.39; P = 0.70) which demonstrated low inter-study heterogeneity (I2 = 1%; P > 0.05).

Forest plot of the subjective measures of function and pain with standardised (Std.) mean differences and associated 95% confidence intervals (CI). ROM range-of-motion
For the 6- to 12-month follow-up measures, six effect points based on four studies were reported for the combined meta-analytical calculations of walking capacity and balance (i.e. 6MWT, gait speed and CSTS; Fig. 5). The results demonstrated an overall significant improvement for the BLN group compared to the CON group (SMD = 0.41; Z = 3.55; P < 0.05), with low heterogeneity (I2 = 0%; P = 0.71). The subjective measures during the 6- to 12-month follow-up consisted of five effect points with three studies (Fig. 6). The overall test statistic demonstrated significantly greater improvement for the BLN group compared to the CON group (SMD = 0.26; Z = 2.09; P < 0.05) with low inter-study heterogeneity (I2 = 0%; P = 0.84), although isolated measures of subjective pain (SMD = 0.28; Z = 1.83; P = 0.07) exhibited no differences between groups with low inter-study heterogeneity (I2 = 0%; P < 0.05).

Forest plot of the walking capacity and balance measures during the 6- to 12-month follow-up period with standardised (Std.) mean differences and associated 95% confidence intervals (CI). 6MWT 6-min walk test, TCS timed chair stand

Forest plot of the subjective measures of function and pain during the 6- to 12-month follow-up period with standardised (Std.) mean differences and associated 95% confidence intervals (CI)
3.6 Sensitivity Analysis
The sensitivity analysis showed no differences in the overall standardised mean differences for 6-min walk test (Z = 2.59; P < 0.01) when studies [14, 17] with lower PEDro scores were excluded. Similarly, excluding a study with lower PEDro scores [18] for balance performance showed no differences in the overall standardised mean differences (Z = 7.33; P < 0.01). Excluding studies with lower PEDro scores for subjective measures of physical function [17, 18] and range-of-motion [14, 17] exhibited no changes in the overall standardised mean differences (Z = 3.43; P < 0.01 and Z = 0.47; P > 0.05, respectively). However, subjective measures of pain approached significance (Z = 1.81; P = 0.07) when excluding studies with lower PEDro scores [14, 17, 18].
3.7 Meta-Regression Analysis of Balance Training Duration
According to the meta-regression, balance training duration in weeks significantly predicted (r2 = 0.48; standardised β = 0.70; P < 0.01) the effect of the intervention on overall performance (i.e. walking capacity, balance performance, subjective measures of function and subjective measures of pain). When meta-regression analysis was separated between physical performance (i.e. walking capacity and balance-specific performance measures) and subjective measures (i.e. pain and physical function), training duration was not a significant predictor for physical performance (r2 = 0.02; standardised β = 0.13; P = 0.48). However, the proportion of the variance in training duration predicting subjective measures of pain and function was significant (r2 = 0.85; standardised β = 0.92; P < 0.001), and greater than the combined measures as well as physical function measures alone.
4 Discussion
The current systematic review meta-analytically explored the literature to determine the benefits of balance training on balance performance and other relevant functional and subjective outcome measures on elderly individuals post-TKA. Based on strict inclusion criteria, 12 studies were included which: (1) utilised a randomised controlled approach; (2) incorporated an even sampling distribution between BLN and CON groups; and (3) demonstrated good to excellent quality ratings. The meta-analyses showed that balance-specific training improved walking capacity and balance performance compared to conventional rehabilitation. Similarly, significantly greater improvements were shown in subjective measures of physical function for the BLN group compared to the CON group, although no between-group differences were found for subjective measures of pain and ROM. During the 6- to 12-month follow-up, significantly greater improvements were found for the BLN group compared to the CON group when walking capacity and balance-specific performance measures as well as subjective measures of physical function and pain were combined. Finally, the training duration significantly predicted the magnitude of the subjective pain and physical function, suggesting a possible dose–response relationship of balance training on subjective measures.
According to consensus in the literature, traditional rehabilitation programmes alone are sufficient to enhance balance [40]. However, the current meta-analyses demonstrated that those who undertook approximately 6 weeks of balance training, as an adjunct to or distinct from typical rehabilitative exercises, showed significantly greater improvement in balance-specific tasks than those who performed typical ROM and muscular strength exercises with lesser emphasis on balance. Comparing these findings to previous review papers is at present difficult as the current review is the first to meta-analytically examine the effects of balance training where specifically implemented following TKA. Moutzouri and colleagues [20] conducted a systematic review of six studies and reported an improvement in functional ability and balance of post-TKA patients following rehabilitative exercises that targeted proprioception, postural control and coordination. However, their work did not statistically compare the pooled data of BLN and CON groups, nor did their inclusion criteria include restriction to randomised controlled trials of rehabilitation exercises implemented post-TKA only. Nonetheless, the similarity in findings between the current review and those by Moutzouri et al. [20] support the inclusion of balance training in post-TKA rehabilitation protocols.
Exercises specifically designed to cause instability at the base of the feet, and/or occluding the vision, have been suggested to compensate for proprioceptive impairment in the knee by enhancing proprioception of the ankles and hips [41], stimulate neuromuscular feedback control, and eventually improve balance and postural stabilisation [15]. Studies included in the current review incorporated these types of exercises, by positioning participants in unstable conditions (e.g. single-leg stance), using equipment that induced instability at the base of the feet (e.g. foam, balance boards and balance beams) and exercising with eyes closed, all of which activate visual, proprioceptive and vestibular systems essential for optimising balance capabilities [23]. As a result of these balance exercises, most of the included studies reported significantly greater improvement in balance-specific tasks for the BLN group compared to the CON group. These findings have substantial clinical implications for individuals post-TKA, given that TKA procedures cause lower extremity pain, impair proprioception and cause fear of falls [2, 18], all of which may increase risks of falls [40]. Subsequently, incorporating rehabilitation programmes that include balance training has the potential to accelerate recovery and minimise the risks of falls in the elderly post-TKA.
Similar to the balance performance measures, the current meta-analyses showed significantly greater improvement in walking capacity. Given that walking performance is highly dependent on balance capabilities [42], it is not surprising that studies that reported improvement in balance also showed enhanced walking capacity. In fact, walking assessments are utilised as strong predictors of falls among older individuals [43]. For example, it has been suggested that the probability of falling will increase from 69 to 83% as TUG time-trial increases from 13 to 14 s [43]. According to the results of the studies included in the current review [11, 15], time-trial for TUG was reduced by an average of 3.3 s with an average of 14.2% greater improvement for the BLN group compared to the CON group. Gait velocity was also shown to increase by 16.2% for the BLN group compared to the CON group [11], which is an important prognosis, given that every 0.1 m·s−1 decrease in gait velocity has been associated with a 10% reduction in physical function [44]. Consequently, balance training post-TKA may assist in improving balance reactivity, accelerate functional recovery and reduce risks of disability.
In addition to changes in walking capacity and balance, significantly greater improvement in subjective measures of physical function were found for the BLN group compared to the CON group. These findings are expected, given that the self-report instruments utilised by included studies consisted of questions regarding function of daily living and sport and recreation, which requires balance and walking capabilities [45]. Interestingly, Fung et al. [17] reported a notably greater improvement (14.1%) in scores from the Activity-specific Balance Confidence Scale for the BLN group compared to the CON group, suggesting that participants that undertook balance training were more confident in their balance capabilities. Improvement in subjective measures of physical function observed in the current review and the confidence scale reported by Fung et al. [17] indicate that balance training may enhance individual’s confidence to perform functional tasks, minimise fear of fall and assist in returning to activities of daily living. Whilst changes were shown in subjective measures of physical function, no changes were observed in subjective measures of pain and ROM measures. Since balance interventions are specifically designed to stimulate the sensory systems for balance [11], it is possible that adaptations induced by such exercises do not provide further improvement in pain levels and ROM compared to CON protocols. However, it is also important to note that balance training did cause sub-optimal changes in pain and ROM measures compared to conventional methods of rehabilitation. Therefore, balance training appears to optimise walking capacity, balance and subjective measures of physical function to a greater degree than conventional protocols without compromising pain level and ROM measures.
During the 6- to 12-month follow-up period, combined measures of walking capacity (i.e. 6-min walk test and gait speed) and balance (i.e. TUG) exhibited significantly greater improvement for individuals undertaking BLN training than those that completed CON rehabilitation. These findings suggest that improved balance capabilities developed as a result of balance training are retained for several months post-training. In addition, when compared to their healthy aged-matched counterparts, elderly individuals that have undergone TKA have an increased falls risks for several months post-surgery due to reduced kinaesthetic awareness [46], with walking and balance capabilities as strong predictors of falls in the elderly [24, 43]. Thus, in addition to immediate improvements in outcomes, balance training may minimise the risk of falls for several months post-intervention when incorporated as part of a post-TKA rehabilitation programme. Similarly, when combining subjective measures of physical function and pain, the overall effect was significant with results favouring the BLN group over the CON group. These data support the additional effects of balance intervention on subjective measures of physical function and pain during follow-up assessments several months post-TKA.
According to the meta-regression, balance training duration did not predict physical performance (i.e. walking capacity and balance-specific performance), although significantly predicted subject measures (i.e. physical function and pain). Thus, there is a larger improvement on subjective measures of physical function and pain with a longer duration (i.e. 8 or more weeks) of balance training, suggesting a dose–response relationship for these types of measures. The discrepancy in regression findings between physical performance and subjective measures may be due to the variation in assessment protocols utilised for the physical performance measures. Given that the sensitivity of an assessment to detect intervention-induced changes is highly dependent on the nature of the protocol, it is possible that the variety of assessment protocols incorporated for walking capacity and balance-specific performance measures precluded training duration to predict the magnitude of change in physical performance measures. Conversely, the subjective measures of physical function and pain were primarily derived by the same questionnaires (i.e. WOMAC and KOOS), or visual analogue scales. Interestingly, in a systematic review and meta-analysis, Lesinski et al. [47] reported that a longer training duration of balance training improved balance-specific performance measures to a greater extent in older adults. Comparing these findings to the current review is difficult at present given that Lesinski et al. [47] did not conduct a meta-regression and studies were not specific to patients following TKA. Nonetheless, irrespective of the variables measured and the statistical analyses employed, the similarity in trend between the current review and that by Lesinski et al. [47] demonstrates that balance training duration influences the magnitude of improvement in performance measures. As the majority of studies included in the current review incorporated balance interventions ranging from 4 to 8 weeks, clinicians should consider extending the duration of post-TKA rehabilitation for at least 8 weeks.
In line with most review papers, a number of limitations should be addressed. Firstly, the I2 values for some outcome measures was large (> 75%; P < 0.05). Whilst these findings suggest large inter-study heterogeneity, every effort was made to ensure that the purpose of the primary (i.e. walking capacity and balance) and secondary (i.e. subjective measures of physical function and pain and ROM) outcome measures were standardised with similar experimental design using strict inclusion criteria. Furthermore, the majority of the reported measures had low I2 values with no statistically significant effects. Secondly, the included studies were limited to articles in English, thus excluding studies published in other languages that would otherwise have contributed to the pool of data. To minimise language-selection bias, two databases considered appropriate for rehabilitation and orthopaedics [32, 48] were used, in conjunction with manual selection of study inclusion via reference lists.
5 Conclusion
In conclusion, the current systematic review and meta-analyses demonstrates that a rehabilitation programme heavily emphasised on balance exercises significantly improves walking capacity, balance-specific and functional outcome measures for elderly patients following TKA to a greater extent than an intervention with a lesser focus on balance training. Thus, clinicians should consider implementing rehabilitation programmes for elderly post-TKA patients with a strong emphasis on exercises that target the balance sensory systems. These include exercises using equipment that induce unstable surfaces (e.g. foam pads or balance boards), assuming positions with single-leg stance, non-assisted gait training and exercises with visual occlusion. In addition, the duration of rehabilitation prescription should be set for 8 or more weeks to optimise the benefits of balance training. These findings may assist in guiding clinical decision-making regarding appropriate post-TKA exercise prescription to minimise falls risks and optimise physical function.
References
Litwic A, Edwards MH, Dennison EM, Cooper C. Epidemiology and burden of osteoarthritis. Br Med Bull. 2013;105:185–99. https://doi.org/10.1093/bmb/lds038.
Mont MA, Banerjee S, Jauregui JJ, Cherian JJ, Kapadia BH. What outcome metrics do the various knee rating systems for assessment of outcomes following total kknee athroplasty measure? A systematic review of literature. Surg Tehnol Int. 2015;26:267–74.
Moutzouri M, Gleeson N, Billis E, Tsepis E, Panoutsopoulou I, Gliatis J. The effect of total knee arthroplasty on patients’ balance and incidence of falls: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2017;25(11):3439–51. https://doi.org/10.1007/s00167-016-4355-z.
Tjon SS, Geurts AC, van’t Pad Bosch P, Laan RF, Mulder T. Postural control in rheumatoid arthritis patients scheduled for total knee arthroplasty. Arch Phys Med Rehabil. 2000;81(11):1489–93.
Matsumoto H, Okuno M, Nakamura T, Yamamoto K, Hagino H. Fall incidence and risk factors in patients after total knee arthroplasty. Arch Orthop Trauma Surg. 2012;132(4):555–63. https://doi.org/10.1007/s00402-011-1418-y.
Matsumoto T, Kubo S, Sasaki K, Kawakami Y, Oka S, Sasaki H, et al. Acceleration of tendon-bone healing of anterior cruciate ligament graft using autologous ruptured tissue. Am J Sports Med. 2012;40(6):1296–302. https://doi.org/10.1177/0363546512439026.
Takura T, Miki K. The future of medical reimbursement for orthopedic surgery in Japan from the viewpoint of the health economy. J Orthop Sci. 2016;21(3):273–81. https://doi.org/10.1016/j.jos.2016.02.007.
Kramer JF, Speechley M, Bourne R, Rorabeck C, Vaz M. Comparison of clinic- and home-based rehabilitation programs after total knee arthroplasty. Clin Orthop Relat Res. 2003;410:225–34. https://doi.org/10.1097/01.blo.0000063600.67412.11.
Shepperd S, Harwood D, Jenkinson C, Gray A, Vessey M, Morgan P. Randomised controlled trial comparing hospital at home care with inpatient hospital care. I: three month follow up of health outcomes. BMJ. 1998;316(7147):1786–91.
Walsh MB, Herbold J. Outcome after rehabilitation for total joint replacement at IRF and SNF: a case-controlled comparison. Am J Phys Med Rehabil. 2006;85(1):1–5.
Liao CD, Lin LF, Huang YC, Huang SW, Chou LC, Liou TH. Functional outcomes of outpatient balance training following total knee replacement in patients with knee osteoarthritis: a randomized controlled trial. Clin Rehabil. 2015;29(9):855–67. https://doi.org/10.1177/0269215514564086.
Bruun-Olsen V, Heiberg KE, Wahl AK, Mengshoel AM. The immediate and long-term effects of a walking-skill program compared to usual physiotherapy care in patients who have undergone total knee arthroplasty (TKA): a randomized controlled trial. Disabil Rehabil. 2013;35(23):2008–15. https://doi.org/10.3109/09638288.2013.770084.
Frost H, Lamb SE, Robertson S. A ranodmized controlled trial of exercise to improve mobility and function after elective knee arthroplasty. Feasibility, results and methodological difficulties. Clin Rehabil. 2002;16:200–9.
Johnson AW, Myrer JW, Hunter I, Feland JB, Hopkins JT, Draper DO, et al. Whole-body vibration strengthening compared to traditional strengthening during physical therapy in individuals with total knee arthroplasty. Physiother Theory Pract. 2010;26(4):215–25. https://doi.org/10.3109/09593980902967196.
Liao CD, Liou TH, Huang YY, Huang YC. Effects of balance training on functional outcome after total knee replacement in patients with knee osteoarthritis: a randomized controlled trial. Clin Rehabil. 2013;27(8):697–709. https://doi.org/10.1177/0269215513476722.
Piva SR, Gil AB, Almeida GJ, DiGioia AM 3rd, Levison TJ, Fitzgerald GK. A balance exercise program appears to improve function for patients with total knee arthroplasty: a randomized clinical trial. Phys Ther. 2010;90(6):880–94. https://doi.org/10.2522/ptj.20090150.
Fung V, Ho A, Shaffer J, Chung E, Gomez M. Use of Nintendo Wii FitTM in the rehabilitation of outpatients following total knee replacement: a preliminary randomised controlled trial. Physiotherapy. 2012;98(3):183–8.
Karaman A, Yuksel I, Kinikli GI, Caglar O. Do Pilates-based exercises following total knee arthroplasty improve postural control and quality of life? Physiother Theory Pract. 2017;33(4):289–95.
Roig-Casasus S, Maria Blasco J, Lopez-Bueno L, Blasco-Igual MC. Balance training with a dynamometric platform following total knee replacement: a randomized controlled trial. J Geriatr Phys Ther. 2017. https://doi.org/10.1519/JPT.0000000000000121.
Moutzouri M, Gleeson N, Billis E, Panoutsopoulou I, Gliatis J. What is the effect of sensori-motor training on functional outcome and balance performance of patients’ undergoing TKR? A systematic review. Physiotherapy. 2016;102(2):136–44.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Ann Intern Med. 2009;151(4):W65–94.
Taube W, Gruber M, Beck S, Faist M, Gollhofer A, Schubert M. Cortical and spinal adaptations induced by balance training: correlation between stance stability and corticospinal activation. Acta Physiol (Oxf). 2007;189(4):347–58. https://doi.org/10.1111/j.1365-201X.2007.01665.x.
Kuo AD. An optimal state estimation model of sensory integration in human postural balance. J Neural Eng. 2005;2(3):S235–49. https://doi.org/10.1088/1741-2560/2/3/S07.
Lusardi MM, Fritz S, Middleton A, Allison L, Wingood M, Phillips E, et al. Determining risk of falls in community dwelling older adults: a systematic review and meta-analysis using posttest probability. J Geriatr Phys Ther. 2017;40(1):1–36. https://doi.org/10.1519/JPT.0000000000000099.
Runge M, Hunter G. Determinants of musculoskeletal frailty and the risk of falls in old age. J Musculoskelet Neuronal Interact. 2006;6(2):167–73.
Reider N, Gaul C. Fall risk screening in the elderly: a comparison of the minimal chair height standing ability test and 5-repetition sit-to-stand test. Arch Gerontol Geriatr. 2016;65:133–9. https://doi.org/10.1016/j.archger.2016.03.004.
Komatsu T, Kim KJ, Kaminai T, Okuizumi H, Kamioka H, Okada S, et al. Clinical factors as predictors of the risk of falls and subsequent bone fractures due to osteoporosis in postmenopausal women. J Bone Miner Metab. 2006;24(5):419–24. https://doi.org/10.1007/s00774-006-0704-1.
Alenazi AM, Alshehri MM, Alothman S, Rucker J, Dunning K, D’Silva L, et al. Functional reach, depression scores, and number of medications are associated with number of falls in people with chronic stroke. PM R. 2017. https://doi.org/10.1016/j.pmrj.2017.12.005.
Bello AI, Ababio E, Antwi-Baffoe S, Seidu MA, Adjei DN. Pain, range of motion and activity level as correlates of dynamic balance among elderly people with musculoskeletal disorder. Ghana Med J. 2014;48(4):214–8.
Miner AL, Lingard EA, Wright EA, Sledge CB, Katz JN, Kinemax Outcomes G. Knee range of motion after total knee arthroplasty: how important is this as an outcome measure? J Arthroplasty. 2003;18(3):286–94. https://doi.org/10.1054/arth.2003.50046.
Cicchetti DV. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol Assess. 1994;6:284–90.
de Morton NA. The PEDro scale is a valid measure of the methodological quality of clinical trials: a demographic study. Aust J Physiother. 2009;55(2):129–33.
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–34.
Deeks J, Higgins JPT. Cochrane handbook for systematic reviews of interventions. Analysing data and undertaking meta-analyses. New Jersey: Wiley-Blackwell; 2008.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60. https://doi.org/10.1136/bmj.327.7414.557.
Cohen J. Statistical power analysis for the behavioral sciences. Hillsdale: Erlbaum; 1988.
Moffet H, Collet JP, Shapiro SH, Paradis G, Marquis F, Roy L. Effectiveness of intensive rehabilitation on functional ability and quality of life after first total knee arthroplasty: a single-blind randomized controlled trial. Arch Phys Med Rehabil. 2004;85(4):546–56.
Monticone M, Ferrante S, Rocca B, Salvaderi S, Fiorentini R, Restelli M, et al. Home-based functional exercises aimed at managing kinesiophobia contribute to improving disability and quality of life of patients undergoing total knee arthroplasty: a randomized controlled trial. Arch Phys Med Rehabil. 2013;94(2):231–9. https://doi.org/10.1016/j.apmr.2012.10.003.
Piva SR, Almeida GJ, Gil AB, DiGioia AM, Helsel DL, Sowa GA. A comprehensive behavioral and exercise intervention improves physical function and activity participation after total knee replacement—a pilot randomized study. Arthritis Care Res (Hoboken). 2017. https://doi.org/10.1002/acr.23227.
Mistry JB, Elmallah RD, Bhave A, Chughtai M, Cherian JJ, McGinn T, et al. Rehabilitative guidelines after total knee arthroplasty: a review. J Knee Surg. 2016;29(3):201–17. https://doi.org/10.1055/s-0036-1579670.
Bunton EE, Pitney WA, Cappaert TA, Kane AW. The role of limb torque, muscle action and proprioception during closed kinetic chain rehabilitation of the lower extremity. J Athl Train. 1993;28(1):10–20.
Nadeau S, Arsenault AB, Gravel D, Bourbonnais D. Analysis of the clinical factors determining natural and maximal gait speeds in adults with a stroke. Am J Phys Med Rehabil. 1999;78(2):123–30.
Shumway-Cook A, Brauer S, Woollacott M. Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test. Phys Ther. 2000;80(9):896–903.
Judge JO, Schechtman K, Cress E. The relationship between physical performance measures and independence in instrumental activities of daily living. The FICSIT Group. Frailty and Injury: cooperative studies of intervention trials. J Am Geriatr Soc. 1996;44(11):1332–41.
Hagovska M, Olekszyova Z. Relationships between balance control and cognitive functions, gait speed, and activities of daily living. Z Gerontol Geriatr. 2016;49(5):379–85. https://doi.org/10.1007/s00391-015-0955-3.
Swinkels A, Allain TJ. Physical performance tests, self-reported outcomes, and accidental falls before and after total knee arthroplasty: an exploratory study. Physiother Theory Pract. 2013;29(6):432–42. https://doi.org/10.3109/09593985.2012.755590.
Lesinski M, Hortobagyi T, Muehlbauer T, Gollhofer A, Granacher U. Effects of balance training on balance performance in healthy older adults: a systematic review and meta-analysis. Sports Med. 2015;45(12):1721–38. https://doi.org/10.1007/s40279-015-0375-y.
Rahman M, Sakamoto J, Fukui T. Japan’s share of articles in orthopedics. J Orthop Sci. 2002;7(6):607–9. https://doi.org/10.1007/s007760200109.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Data Availability Statement
The mean and standard deviation measures for each effect point is presented in the forest plot. Thus, to avoid repetition, the data set for this review has not been included as a separate file.
Conflict of Interest
Kenji Doma, Jodie Morris and Andrea Grant declare that they have no conflicts of interest.
Study Funding
No financial support was received for the conduct of this study or preparation of this manuscript.
Electronic supplementary material
Below is the link to the electronic supplementary material.
40279_2018_964_MOESM1_ESM.pdf
Online resource 1. Funnel plot of the walk capacity measures. 2MWT – two minute walk test; 6MWT – six minute walk test (PDF 142 kb)
40279_2018_964_MOESM2_ESM.pdf
Online resource 2. Funnel plot of the walking capacity and balance measures during the 6-12 month follow-up period. 6MWT – six minute walk test (PDF 140 kb)
40279_2018_964_MOESM3_ESM.pdf
Online resource 3. Funnel plot of the subjective measures of function and pain during the 6-12 month follow-up period (PDF 186 kb)
40279_2018_964_MOESM4_ESM.pdf
Online resource 4. Funnel plot of the balance measures. BBS – Berg balance scale; SLS TKR EC – single leg stance time for the total knee replacement limb with eyes closed; SLS Non-TKR EC – single leg stance time for the limb without total knee replacement with eyes closed; CSTS – chair sit-to-stand; SLS TKR EO – single leg stance time for the total knee replacement limb with eyes open; SLS Non-TKR EO – single leg stance time for the limb without total knee replacement with eyes opened (PDF 192 kb)
40279_2018_964_MOESM5_ESM.pdf
Online resource 5. Funnel plot of the subjective measures of function and pain and range-of-motion measures (PDF 194 kb)
Rights and permissions
About this article

Cite this article
Doma, K., Grant, A. & Morris, J. The Effects of Balance Training on Balance Performance and Functional Outcome Measures Following Total Knee Arthroplasty: A Systematic Review and Meta-Analysis. Sports Med 48, 2367–2385 (2018). https://doi.org/10.1007/s40279-018-0964-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-018-0964-7