
Abstract
Background
Current evidence suggests sodium bicarbonate (NaHCO3) should be ingested based upon the individualised alkalotic peak of either blood pH or bicarbonate (HCO3 −) because of large inter-individual variations (10–180 min). If such a strategy is to be practical, the blood analyte response needs to be reproducible.
Objective
This study aimed to evaluate the degree of reproducibility of both time to peak (TTP) and absolute change in blood pH, HCO3 − and sodium (Na+) following acute NaHCO3 ingestion.
Methods
Male participants (n = 15) with backgrounds in rugby, football or sprinting completed six randomised treatments entailing ingestion of two doses of 0.2 g·kg−1 body mass (BM) NaHCO3 (SBC2a and b), two doses of 0.3 g·kg−1 BM NaHCO3 (SBC3a and b) or two control treatments (CON1a and b) on separate days. Blood analysis included pH, HCO3 − and Na+ prior to and at regular time points following NaHCO3 ingestion over a 3-h period.
Results
HCO3 − displayed greater reproducibility than pH in intraclass correlation coefficient (ICC) analysis for both TTP (HCO3 − SBC2 r = 0.77, P = 0.003; SBC3 r = 0.94, P < 0.001; pH SBC2 r = 0.62, P = 0.044; SBC3 r = 0.71, P = 0.016) and absolute change (HCO3 − SBC2 r = 0.89, P < 0.001; SBC3 r = 0.76, P = 0.008; pH SBC2 r = 0.84, P = 0.001; SBC3 r = 0.62, P = 0.041).
Conclusion
Our results indicate that both TTP and absolute change in HCO3 − is more reliable than pH. As such, these data provide support for an individualised NaHCO3 ingestion strategy to consistently elicit peak alkalosis before exercise. Future work should utilise an individualised NaHCO3 ingestion strategy based on HCO3 − responses and evaluate effects on exercise performance.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Although both the blood pH and bicarbonate (HCO3 −) response following ingestion of sodium bicarbonate (NaHCO3) displays good test–retest reliability, the HCO3 − response is more reproducible. Therefore, an individualised NaHCO3 ingestion strategy should be based on time to peak HCO3 −. |
Large inter-individual variations in achieving both peak pH and HCO3 − suggest an individualised NaHCO3 ingestion strategy based on time to peak HCO3 − would be most appropriate to increase potential ergogenic effects on performance. |
Within the first 60 min following ingestion of 0.2 or 0.3 g·kg−1 body mass NaHCO3, the acid–base balance kinetics are similar, meaning smaller doses of NaHCO3 may be appropriate when <60 min is available, particularly for individuals who experience gastrointestinal discomfort. |
1 Introduction
Nutritional ergogenic aids that delay metabolic acidosis during high-intensity exercise have been widely investigated [5, 16, 38]. In particular, exogenous enhancement of the bicarbonate buffering systems is thought to have an important role in offsetting the metabolite fatigue process by dampening critical rises in hydrogen cations (H+) [17]. Ingestion of a known alkalotic buffer, sodium bicarbonate (NaHCO3), can achieve ergogenic effects by increasing blood bicarbonate concentration [HCO3 −] within extracellular fluid by 4–8 mmol·L−1 [34], which typically relates to peak alkalosis [32]. The most common ingestion practices include doses of 0.2–0.3 g·kg−1 body mass (BM) NaHCO3; lower amounts are considered insufficient to induce a level of peak alkalosis that would improve performance [34]. Doses above this concentration exacerbate the incidence and severity of gastrointestinal (GI) discomfort [16].
Multiple studies using group mean data have reported wide variations in time to peak (TTP) alkalosis (i.e. HCO3 − or pH ) following various doses of NaHCO3 [7, 28, 31, 32]. Peak HCO3 − has been observed at 40 and 60 min following 0.2 and 0.3 g·kg−1 BM NaHCO3, respectively [31], whereas others have observed peaks at 90 [28], 120 [7] and 180 min [32]. Differences may be due to either sampling rate (20–60 min) or inter-individual variations since it is possible that individual blood pH and HCO3 − absorption characteristics were overlooked [7, 28, 31, 32]. Consequently, this generic approach has led to potential reductions or variations in ergogenic effects [8, 30]. More specifically, Froio de Araujo Dias et al. [8] reported inconsistent performance responses following ingestion of NaHCO3 during 110% peak power output cycling time to exhaustion (TTE). Recreationally active participants (n = 15) consumed 0.3 g·kg−1 BM NaHCO3 on four occasions or a placebo on two occasions. Only one participant experienced ergogenic effects with all NaHCO3 treatments, and five did not improve with any treatment. This suggests some degree of intra-individual variation, which may be a result of intra-individual blood responses, although this is difficult to define because only group mean blood responses were reported.
A contemporary approach is to individualise the ingestion strategy; Stannard et al. [34] reported large inter-individual variations in TTP HCO3 − (0.2 g·kg−1 BM = 40–165 min; 0.3 g·kg−1 BM = 75–180 min). These findings challenge the results of the aforementioned studies, which reported group-level analysis following NaHCO3 supplementation at a fixed timeframe [17, 30, 31]. Furthermore, variations in TTP HCO3 − arguably provide insight into the commonly reported inter- and intra-individual variations in performance following NaHCO3 ingestion [8, 30], as participants may not have reached peak alkalosis before commencing exercise [17]. Recent work by Miller et al. [18] supports this claim. These authors found that total work done (TWD) during repeated sprint cycling (10 × 6 s) improved by 11% with an individualised ingestion strategy [18], a response greater than the 5% improvement in a similar study employing a standardised ingestion strategy [3].
Further research is necessary to identify individualised NaHCO3 ergogenic strategies that elicit peak alkalosis. Equally important for practical application in the field is a better understanding of the reproducibility of blood analytes (pH and HCO3 −) following acute ingestion of NaHCO3. Daily biological variations, either short term or long term, may occur in response to changes in nutritional practices and therefore effect daily acid load fluxes (potential renal acid load [PRAL]) [22, 26, 27] with the potential to affect the reproducibility of TTP alkalosis. This may then negatively affect the efficacy and consistency of an individualised NaHCO3 ingestion strategy intended to improve exercise performance. Therefore, the aim of this study was to assess the reproducibility of the individual blood pH, HCO3 − and Na+ response following acute ingestion of 0.2 or 0.3 g·kg−1 BM doses of NaHCO3.
2 Materials and Methods
2.1 Participants
Participants were recruited on the basis that they may gain a performance benefit from enhancing their buffering capacity [17]. In total, 16 participants in team or individual sports with backgrounds in rugby, football or running volunteered for this single-blind randomised crossover study. One participant withdrew from the study because of GI upset (vomiting) after the first dose of NaHCO3 0.3 g·kg−1 BM; therefore, 15 males (n = 5 rugby, n = 7 football, n = 3 sprinting) completed the study (height 1.81 ± 0.06 m, BM 84 ± 8 kg, age 21 ± 2 years, maximal oxygen uptake [VO2max] 52.1 ± 2.2 ml.kg−1.min−1). Participants habitually completed four (±1) exercise bouts per week lasting 2 (±0) h per session and had 10 (±3) years’ training experience within their respective sports. Ethical approval was obtained from the Departmental Research Ethics Committee (SPA-REC-2015-325), and each participant provided written informed consent and completed a health screening procedure prior to data collection. The research was conducted in accordance with the Helsinki declaration. Participants were verbally screened to ensure no NaHCO3 or similar intracellular or extracellular buffers such as beta alanine had been ingested during the 6 months prior to, or outside of, the experimental conditions.
2.2 Pre-Experimental Procedures
Participants visited the laboratory on seven occasions 4 h after eating and at the same time of day to minimise the effects of circadian rhythms [25]. Participants were required to avoid alcohol and any strenuous/unaccustomed exercise during the 24-h period before the experimental treatment [29]. Caffeine and spicy foods were also prohibited 12 h before experimental treatments to avoid any influence on metabolic regulation [15, 39]. Compliance with the above procedures was checked via a written log of nutritional intake 24 h prior to each experimental treatment, which was replicated for each visit (adherence = 100%) and later analysed for reproducibility. Treatments were conducted at least 7 days apart to allow for washout of residual NaHCO3 [3]. The NaHCO3 used in this study was purchased from the manufacturer and stored safely according to laboratory guidelines to avoid contamination by other stimulants.
2.3 Maximal Oxygen Uptake Protocol
An incremental ramp VO2max test on an electromagnetically braked cycle ergometer (Lode Excalibur, Germany) was initially conducted. After a 5-min warm-up (70 W), participants began cycling at their respective self-selected cadence at a power output of 75 W (ten participants at 80 r.min−1; five participants at 90 r.min−1). This then increased by 1 W every 2 s (30 W.min−1) until volitional exhaustion. Samples were continuously analysed using a gas analyser (Cosmed, K5, Italy) for oxygen consumption (VO2), carbon dioxide expired (VCO2) and respiratory exchange ratio (RER). Data were averaged over the last 30 s of exercise to determine the VO2max.
2.4 Main Treatment Arms
The subsequent six treatments were administered in a block randomised manner and involved two treatment arms of no treatment (CON1a, CON1b) to assess daily variations in blood analytes, two treatment arms requiring ingestion of NaHCO3 0.2 g·kg−1 (SBC2a, SBC2b), and two treatment arms requiring ingestion of NaHCO3 0.3 g·kg−1 BM (SBC3a, SBC3b). Solutions were prepared by a laboratory technician not involved with the research: 400 ml of water was mixed with 50 ml of flavoured sugar-free drink concentrate and refrigerated to enhance palatability [18]. Treatments were administered single blind, and participants consumed the drink within the first 10 mins of the 180 min experimental procedures [34].
An arterialised finger prick capillary blood sample was obtained from participants in a rested and seated state prior to NaHCO3 ingestion. Arterialisation was achieved by warming the hand with a heated blanket (45 °C) for 5 min prior to taking each individual sample [13]. After ingestion of NaHCO3, a further 15 blood samples were obtained over a 180-min period in each treatment (Table 1). At multiple time points, a GI questionnaire (visual analogue scale [VAS] where 0 = no instance and 10 = most severe) that included a range of symptoms was completed as per previous research [18] (Table 2). Participants remained seated throughout, with only toilet breaks permitted. No food was allowed to be consumed during this period, and water was consumed ab libitum, with total volume replicated in subsequent treatment arms. Blood samples were collected in 100-µl heparin-coated clinitubes (Radiometer Medical Ltd, Denmark) and subsequently analysed for blood pH, HCO3 − and Na+ (ABL800 BASIC, Radiometer Medical Ltd). This radiometer has demonstrated a low bias in pH, PCO2 and Na+ [24] and a correlation coefficient of r > 0.98 for both HCO3 − and pH against other commercially available blood gas analysers [35]. Moreover, a small pilot study (n = 8) in our laboratory also revealed high test–retest reliability for both HCO3 − (16 samples: coefficient of variation [CV] 3.0–4.9%) and pH (16 samples: CV 0.17–0.20%) at both resting levels and following NaHCO3 ingestion.
2.5 Statistical Analysis
We conducted an a priori power calculation using the statistical software package SPSS Sample Power 3 (IBM, Chicago, IL, USA). Based upon the expected population correlation of r = 0.80 between both NaHCO3 conditions (SBC2 and SBC3), a minimum of 11 participants was required to achieve 80% power (P < 0.05).
Assessed variables were initially analysed for normality (Shapiro–Wilks and Q–Q plots) and homogeneity of variance/sphericity (Mauchly). To assess the differences between conditions, t tests were used. For non-normally distributed data, a Mann–Whitney U test was used with Z score and significance reported (e.g. GI data). Likewise, the appropriate correction was applied (Greenhouse Geisser) for violations of sphericity. Both one-way (treatment) and two-way (treatment × time) repeated measured analysis of variation (ANOVA) was used to analyse differences in blood parameters with Bonferroni corrections applied. Tukey’s honestly significant difference (HSD) post hoc analysis was carried out to assess interactions by calculating the minimal difference required between means to confirm significance had been achieved [37]. Statistical significance was set at P > 0.05.
Limits of agreement (LOA) with 95% limits and Bland–Altman plots were utilised for within-subject variance and to determine whether data were heteroscedastic [4]. This method is widely used [19, 33] and accounts for bias between the mean differences [9]. Intraclass correlation coefficients (ICCs) were displayed with r value and significance level, as per previous recommendations [1]. CV is reported using standard deviation (SD)/mean × 100. Correlation between TTP HCO3 − and pH was calculated using Pearson’s correlation, from Hopkins’ spreadsheet [12]. Statistical procedures were completed using SPSS version 22, and calculations were carried out using Microsoft® Excel 2013 (Microsoft Inc., Redmond, WA, USA).
3 Results
3.1 Nutritional Intake
Total daily calorie (r = 0.78, P < 0.001; mean ± SD 2283 ± 75), carbohydrate (r = 0.97, P < 0.001; 253 ± 4 g), protein (r = 0.98, P < 0.001; 85 ± 2 g) and fat (r = 0.97, P < 0.001; 126 ± 3 g) intake were all highly reproducible for all treatments.
3.2 Gastrointestinal Upset
Both the severity and the TTP GI upset displayed excellent reproducibility in SBC2 and SBC3 (severity: SBC2 r = 0.92, P < 0.001; LOA: B –0.5, −3.1, +2.2; TTP: SBC2 r = 0.91, P < 0.001; LOA: B 5, −38, +47 vs. severity SBC3 r = 0.90, P < 0.001; LOA: B −0.4, −4.7, +3.8; TTP SBC3 r = 0.78, P = 0.005; LOA: B 7, −64, 77). In total, 10 of the 15 participants reported symptoms of GI upset in both SBC2 and SBC3; the specific symptoms are depicted in Table 2. The severity of upset was lower in SBC2 than in SBC3 (mean 2.0 vs. 3.6), but the difference was not significant (Z = 0.922, P = 0.356). In SBC2 TTP GI upset was established ealier compared to SBC3 (mean 29 vs. 36 min), but this was also not significant (Z = 0.439, P = 0.661).
3.3 Reproducibility of Blood pH, Bicarbonate and Sodium
Baseline measures for both HCO3 − (r = 0.83, P < 0.001) and Na+ (Na+ r = 0.86, P < 0.001) displayed excellent reproducibility and pH displayed good reproducibility (r = 0.66, P = 0.002). Values for ICCs across the 3-h sampling period ranged from fair to excellent (r = 0.530–0.914) for pH in SBC2 and from good to excellent (r = 0.76–0.92) in SBC3 upon excluding two poor values at 80 (r = 0.05) and 85 min (r = 0.01). Reproducibility for HCO3 − in SBC2 demonstrated excellent reproducibility (r = 0.76–0.87) and SBC3 displayed good to excellent (r = 0.65–0.87) reproducibility across all time points (Table 1).
Greater reproducibility of TTP HCO3 − was demonstrated for SBC3 (ICC: r = 0.94, P < 0.001; LOA: B 2.3, −15.9, +20.5) compared to SBC2 (ICC: r = 0.77, P = 0.003; LOA: B −6, −36, +24). Likewise, TTP pH demonstrated a greater reproducibility for SBC3 (ICC: r = 0.71, P = 0.016; LOA: B 2.3, −37.3, +42) than for SBC2 (ICC: r = 0.62, P = 0.044; LOA: B 2.3, −39.3, +42). The correlation between TTP pH and TTP HCO3 − was greater in SBC2 (r = 0.61 and r = 0.66, respectively) than in SBC3 (r = 0.26 and r = 0.17, respectively). The relationship between TTP Na+ was greater for SBC2 (ICC: r = 0.75, P = 0.838; LOA: B 8.7, +41.8, −73.2) than for SBC3 (ICC: r = 0.56, P = 0.061; LOA: B 15, +44.4, −71.9), but neither were significant in ICCs and displayed considerable bias in LOA analysis.
Absolute change (peak change from baseline) for HCO3 − displayed high reproducibility for SBC2 (ICC: r = 0.90, P < 0.001; LOA: B 0.1, −0.9, +1.1) compared with SBC3 (ICC: r = 0.76, P = 0.008; LOA: B 0.1, −1.9, +2.0). The absolute change in pH was highly reproducible in SBC2 (ICC: r = 0.84, P = 0.001; LOA: B −0.1, −0.04, +0.03) compared with SBC3 (ICC: r = 0.62, P = 0.041; LOA: B 0.01, −0.04, +0.05). In contrast, the absolute change in Na+ displayed no relationship in either SBC2 (ICC: r = 0.10, P = 0.562; LOA: B 0.1, −4.9, +5.1) or SBC3 (ICC: r = 0.10, P = 0.425; LOA: B 1.3, −6.2, +8.7).
3.4 Differences Between Treatments
There was no significant difference in TTP HCO3 − between SBC2 and SBC3 (all P > 0.05) (Table 3). Conversely, TTP pH occurred significantly later in SBC3a than in SBC2a (+17 min; P < 0.026) but non-significantly later in SBC3b than in SBC2b (+8 min; P = 0.392) (Table 3). In SBC3a, TTP Na+ occured significantly later than in SBC2a (+32 min; P = 0.027) and 25 min later in SBC3b than in SBC2b (P = 0.061). A large inter-individual variation in TTP pH, HCO3 − and Na+ was observed in both SBC treatments (Table 3).
The absolute change in blood analytes HCO3 − and pH can be observed in Table 3. Absolute change in HCO3 − was greater in SBC3 than in SBC2 (P < 0.001). Absolute pH change was significantly greater in SBC3a than in SBC2a (+0.2; P = 0.018) but not in SBC2b and SBC3b (+0.1; P = 0.242). Absolute change in Na+ was significantly greater in SBC3 than in SBC2 (P > 0.05; Fig. 1). A large inter-individual variation in absolute change of pH, HCO3 − and Na+ was observed in both SBC2 and SBC3 (Table 3). Lastly, up to 60 min post NaHCO3 ingestion, neither HCO3 − nor pH were significantly different between SBC2 and SBC3 (both P > 0.05; Fig. 1).

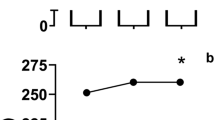
Mean blood analyte responses for blood bicarbonate, pH and sodium following control treatments (solid squares), ingestion of sodium bicarbonate 0.2 g·kg−1 body mass (SBC2; solid triangles) and 0.3 g·kg−1 body mass (SBC3; solid circles). Some error bars and timepoints (5-min interval samples) are omitted for clarity
4 Discussion
This is the first study to investigate the reproducibility of individual blood analytes pH, HCO3 − and Na+ following acute induced metabolic alkalosis. Our findings suggest blood pH and HCO3 − are highly reproducible in most participants (13 of 15), whereas Na+ displays poor reproducibility. Given that TTP and absolute change reflected greater reproducibility for HCO3 − and correlation was lacking between pH and HCO3 − (no to moderate correlation; Sect. 3.2), prior knowledge of HCO3 − absorption characteristics following NaHCO3 ingestion is essential. As such, practitioners and athletes should develop their respective NaHCO3 dosing strategies based on TTP HCO3 −.
These results challenge the common ingestion strategy of NaHCO3 0.3 g·kg−1 BM 1–4 h before exercise [16, 28, 32] because a large inter-individual variation in TTP alkalosis is evident (Table 3). For instance, the absolute changes in HCO3 − observed in this study for SBC2 (~5.7 mmol·L−1) and SBC3 (~7.1 mmol·L−1) (Table 3) were greater than the typical change with standardised ingestion strategies [31]. This is also within the range of absolute change that is suggested to be required to potentially produce ergogenic effects (>5 mmol·L−1 [6]). Moreover, in light of similar reports of inter-individual variations [18, 32, 34], a standardised ingestion strategy is not suitable to heighten the potential ergogenic effects from alkalotic substances (i.e. NaHCO3 and sodium citrate). Rather, an individualised ingestion strategy is more relevant to optimise peak alkalosis and, therefore, individuals should identify their respective alkalotic peak.
TTP HCO3 − was achieved considerably earlier in the present study (<90 min) than in previous work (>95 min) that adopted the same ingestion window (10 min) [34]. Both studies controlled nutritional intake and employed the same 4-h post-prandial strategy; however, as 10% of food is suggested to be present in the stomach even after a 4-h fast [34], small contributions from meal volume, composition and texture may have produced equivocal timeframes. However, it is more plausible that the differences in NaHCO3 administration (solution vs. capsule) between studies explains the discrepancies in TTP given the differential rapid emptying of liquids versus the slower emptying of solids [11]. In support, TTP HCO3 − has occurred earlier in other studies that administered NaHCO3 via solution [6, 18, 23, 28, 30] compared with capsules [6, 30, 34]. In future, individuals should consider the time until competition/exercise and the palatability of NaHCO3 as a solution versus the large number of capsules (~20) required within their respective ingestion strategies.
In some participants, the absolute HCO3 − change lacked reproducibility (SBC3 n = 6; SBC2 n = 2), with differences >1 mmol·L−1 observed (Table 3). For instance, participant 1 elicited a 6.9 mmol·L−1 change in HCO3 − in SCB3a compared with a 5.6 mmol·L−1 change in SBC3b. Furthermore, two participants did not reproduce a similar TTP HCO3 −, with over 15 min difference between SBC2 and SBC3 (Table 3). It is unclear why this occurred given that participants replicated nutritional intake. Nonetheless, some individuals may require a test–retest to evaluate the reproducibility of the absolute change in HCO3 −, which presents a logistical limitation to the practitioner/athlete. Whether such discrepancies would translate to a lack of consistency in the performance response is unknown; however, McNaughton [16] demonstrated that differences of around 1 mmol·L−1 in HCO3 − elicited different performance responses. Future work should assess whether discrepancies in either TTP or absolute change within such individuals affects performance responses.
For four of the participants, the absolute change in HCO3 − following SBC2 was not enhanced further following SBC3. For instance, participant 1 displayed a minimal improvement of 0.1 mmol·L−1 between SBC2 and SBC3. In comparison, participant 13 increased nearly twofold between SBC2 (+4.8 mmol·L−1) and SBC3 (+8.8 mmol·L−1). This suggests identification of the absolute HCO3 − change between different doses of NaHCO3 is required, as some do not display any further increase in HCO3 − from NaHCO3 doses >0.2 g·kg−1 BM. This indicates that ingestion of NaHCO3 >0.2 g·kg−1 BM may not be warranted in individuals who display small changes between NaHCO3 doses. This finding is of practical significance to individuals who experience GI upset from a dose of 0.3 g·kg−1 BM, given that the same acid–base response can be elicited from a smaller dose. Further research could evaluate whether both doses improve performance to a similar extent in individuals who respond this way.
This study found that HCO3 − and pH did not significantly differ between SBC2 and SBC3 up to 60 min, which supports previous findings [34]. This suggests it may be possible for individuals to ingest a smaller dose if limited time (<60 min) is available before exercise. This may be of significance to individuals who participate in two bouts of exercise with a small recovery time (e.g. track and field athletes) or who experience GI upset, as lower doses have been shown to reduce the severity and incidence of such occurrences [16].
Inconsistencies in pH reproducibility observed in this study could be explained by the breadth of factors that affect pH, including contributions from intracellular buffering such as carnosine, phosphocreatine and phosphates [10, 14]. Moreover, as ingestion of a NaHCO3 bolus will initially and directly increase HCO3 − concentration, the effect on pH is secondary and therefore may lead to increased variability [10]. Variable pH has also been observed in a recent study, even when HCO3 − was similar [8]. For instance, following NaHCO3 ingestion, pH increased by 0.045 ± 0.029 in one treatment but only by 0.027 ± 0.054 in another. Conversely, in the same treatments, HCO3 − increased by 6.1 ± 2.3 and 5.9 ± 2.7 mmol·L−1, but one of the limitations in this study was that data were analysed at the group level and only at two time points. Alternatively, the effect of nutritional intake may have caused pH to vary. It is well known that the acid/alkaline levels (PRAL) within nutritional intake may affect the acid base balance [26, 27]. Therefore, a limitation of this study is that participants completed a nutrition log for only 24 h. Further research could investigate the effects of PRAL and longitudinal nutritional practices on NaHCO3 absorption characteristics.
The Na+ response displayed high intra-individual variability following NaHCO3 (Sect. 3.2; Fig. 1). In this study, participants replicated nutritional practices prior to experiments, and analysis revealed this was highly reproducible (Sect. 3.1) but not specifically for Na+ ingestion. Therefore, small changes in total Na+ ingested may explain these findings. Moreover, whilst the volume of water was controlled during experimental treatments, a limitation of this study is that the frequency of ingestion was not measured, which may also have affected Na+ concentrations [20]. Nonetheless, whether small differences in total Na+ ingested or frequency of water consumption would account for a meaningful change is unclear. An alternative but speculative factor may be gastric emptying, as other work [2, 21, 36] has suggested intra-individual variability. Our analysis focused on blood Na+, so different quantities may or may not have reached the bloodstream by the second intake of the same NaHCO3 dose and consequently may have produced equivocal responses.
We propose that disturbances to the acid base balance of the stomach from high Na+ load accompanying NaHCO3 ingestion can cause the onset of GI upset [34]. When considering participants who experienced GI upset in this study, TTP GI upset broadly corresponded with peak Na+ in SBC2 (peak GI upset ~30 min, peak Na+ 41 min) but not as strongly in SBC3 (peak GI upset ~35 min, peak Na+ ~70 min). The absolute change in Na+ was significantly higher in SBC3 than in SBC2 (~2 vs. ~6 mmol·L−1); however, the incidence and severity of GI upset did not differ significantly. Therefore, whether the magnitude of change in Na+ is useful in predicting the onset of GI upset is unclear. Interestingly, the same severity of nausea in SBC2 and diarrhoea in SBC3 was observed in participant 8 (Table 2), with this theme apparent for seven participants in total. As such, these differences between doses will plausibly vary in the effects on the ability to perform exercise. It is therefore important to evaluate the severity of the specific symptom experienced in the GI upset and make judgements on the cost:benefit of NaHCO3 ingestion.
5 Conclusion
The blood analyte response following acute NaHCO3 ingestion is highly reproducible. The practitioner and/or athlete should identify both the TTP and the absolute change in HCO3 − to determine both the time and the amount to ingest prior to using it in training or competition. However, caution should be taken with participants who displayed intra-individual variations in both TTP and absolute change in HCO3 −, as NaHCO3 ingestion is potentially unsuitable in these individuals. Future work should investigate why some participants do not reproduce a blood analyte response from NaHCO3 ingestion, including investigation into the role of PRAL and longitudinal nutritional practices. Lastly, given that both SBC2 and SBC3 elicited a change in HCO3 − that may improve performance, establishing the performance response utilising an individualised NaHCO3 strategy is required.
References
Atkinson G, Nevill AM. Statistical methods for assessing measurement error (reliability) in variables relevant to sports medicine. Sports Med. 1998;26:217–38.
Barnett C, Snel A, Omari T, Davidson G, Haslam R, Butler R. Reproducibility of the 13C-octanoic acid breath test for assessment of gastric emptying in healthy preterm infants. J Pediar Gastroenterol Nutr. 1999;29:26–30.
Bishop D, Edge J, Davis C, Goodman C. Induced metabolic alkalosis affects muscle metabolism and repeated-sprint ability. Med Sci Sports Exerc. 2004;36:807–13.
Bland JM, Altman GD. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1(8476):307–10.
Cairns SP. Lactic acid and exercise performance: culprit or friend? Sports Med. 2006;36:279–91.
Carr AJ, Hopkins WG, Gore CJ. Effects of acute alkalosis and acidosis on performance: a meta-analysis. Sports Med. 2011;41:801–14.
Carr AJ, Slater GJ, Gore CJ, Dawson B, Burke LM. Effect of sodium bicarbonate on [HCO3-], pH, and gastrointestinal symptoms. Int J Sport Nutr Exerc Metab. 2011;21:189–94.
Froio de Araujo Dias G, da Eira Silva V, de Salles Painelli V, Sale C, Giannini Artioli G, Gualano B, Saunders B. (In)Consistencies in responses to sodium bicarbonate supplementation: a randomised, repeated measures, counterbalanced and double blind study. PLOS One. 2015; 10(11):e0143086.
Giavarina D. Understanding bland altman analysis. Biochem Med (Zagreb). 2015;25:141–51.
Goel N, Calvert J. Understanding blood gases/acid-base balance. Paediatr Child Health. 2011;22:142–8.
Hellström PM, Grybäck P, Jacobsson H. The physiology of gastric emptying. Best Pract Res Clin Anaesthesiol. 2006;20:397–407.
Hopkins WG. Measures of reliability in sports medicine and science. Sports Med. 2000;30:1–15.
Johnston KR, Vickers MD, Mapleson WW. Comparison of arterialized venous with arterial blood propofol concentrations during sub-anaesthetic infusions in volunteers. Br J Anaesth. 1996;76:401–4.
MacLaren D, Morton J. Biochemistry for sport and exercise science. Champaign: Human Kinetics; 2012.
Maughan RJ, King DS, Lea T. Dietary supplements. J Sports Sci. 2004;22:95–113.
McNaughton LR. Bicarbonate ingestion: effects of dosage on 60 s cycle ergometry. J Sports Sci. 1992;10:415–23.
McNaughton LR, Gough L, Deb S, Bentley D, Sparks SA. Recent developments in the use of sodium bicarbonate as an ergogenic aid. Curr Sports Med Rep. 2016;15(4):233–44.
Miller P, Robinson AL, Sparks SA, Bridge CA, Bentley DJ, McNaughton LR. The effects of novel ingestion of sodium bicarbonate on repeated sprint ability. J Strength Cond Res. 2016;30:561–8.
Myles PS, Cui J. Using the bland-altman method to measure agreement with repeated measures. Br J Anaesth. 2007;99:309–11.
Nose H, Sugimoto E, Okuno T, Morimoto T. Changes in blood volume and plasma sodium concentration after water intake in rats. Am J Physiol. 1987;253:15–9.
Paintaud G, Thibault P, Queneau PE, Magnette J, Berard M, Rumbach L, Bechtel PR, Carayon P. Intraindividual variability of paracetamol absorption absorption kinetics after a semisolid meal in healthy. Eur J Clin Pharmacol. 1998;53:355–9.
Poupin N, Calvez J, Lassale C, Chesneau C, Tomé D. Impact of the diet on net endogenous acid production and acid-base balance. Clin Nutr. 2012;31:313–21.
Price MJ, Singh M. Time course of blood bicarbonate and pH three hours after sodium bicarbonate ingestion. Int J Sports Physiol Perform. 2008;3:240–2.
Radiometer Medical. 2015. ABL 800 Reference Manual. http://www.radiometer.com. Accessed 2015.
Reilly T. Human circadian rhythms and exercise. Crit Rev Biomed Eng. 1990;18:165–80.
Remer T. Influence of nutrition on acid-base balance—metabolic aspects. Eur J Nutr. 2001;40:214.
Remer T, Manz F. Potential renal acid load and its influence on urine pH. J Am Diet Assoc. 1995;95:791–7.
Renfree A. The time course of changes in plasma [H+] after sodium bicarbonate ingestion. Int J Sports Physiol Perform. 2007;2:323–6.
Rosenberg K, Durnin JV. The effect of alcohol on resting metabolic rate. Br J Nutr. 1978;40:293–8.
Saunders B, Sale C, Harris RC, Sunderland C. Sodium bicarbonate and high-intensity-cycling capacity: variability in responses. Int J Sports Physiol Perform. 2014;9:627–32.
Siegler JC, Marshall PW, Bray J, Towlson C. Sodium bicarbonate supplementation and ingestion timing: does it matter? J Strength Cond Res. 2012;26:1953–8.
Siegler JC, Midgley AW, Polman RC, Lever R. Effects of various sodium bicarbonate loading protocols on the time-dependent extracellular buffering profile. J Strength Cond Res. 2010;24:2551–7.
Sparks SA, Close GL. Validity of a portable urine refractometer: the effects of sample freezing. J Sports Sci. 2013;31:745–9.
Stannard RL, Stellingwerff T, Artioli GG, Saunders B, Cooper S, Sale C. Dose-response of sodium bicarbonate ingestion highlights individuality in time course of blood analyte responses. Int J Sport Nutr Exerc Metab. 2016;26(5):445–53.
Stadlbauer V, Wallner S, Stojakovic T, Smolle KH. Comparison of 3 different multianalyte point-of-care devices during clinical routine on a medical intensive care unit. J Crit Care. 2011;26:433.
Tougas G, Eaker EY, Abell TL, Abrahamsson H, Boivin M, Chen J, Hocking MP, Quigley EM, Koch KL, Tokayer AZ, Stanghellini V, Chen Y, Huizinga JD, Ryden J, Bourgeois L, McCallum RW. Assessment of gastric emptying using a low fat meal: establishment of international control values. Am J Gastroenterol. 2000;95:1456–62.
Vincent W, Weir J. Statistics in Kinesiology. 4th ed. Champaign: Human Kinetics; 2012.
Westerblad H, Allen DG, Lännergren J. Muscle fatigue: lactic acid or inorganic phosphate the major cause? News Physiol Sci. 2002;17:17–21.
Westerterp-Platenga M, Diepvens K, Joosen AM, Bérubé-Parent S, Tremblay A. Metabolic effects of spices, teas and caffeine. Physiol Behav. 2006;89:85–91.
Acknowledgements
The authors are grateful for the technical assistance received during data collection and thank fellow colleagues who provided laboratory space, even during busy times.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No sources of funding were used to conduct this study or prepare this manuscript.
Conflicts of interest
LA Gough, SK Deb, SA Sparks, and LR McNaughton have no conflicts of interest that are directly relevant to the content of this article.
Rights and permissions
About this article

Cite this article
Gough, L.A., Deb, S.K., Sparks, A.S. et al. The Reproducibility of Blood Acid Base Responses in Male Collegiate Athletes Following Individualised Doses of Sodium Bicarbonate: A Randomised Controlled Crossover Study. Sports Med 47, 2117–2127 (2017). https://doi.org/10.1007/s40279-017-0699-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-017-0699-x